mayo clinic - rochester, mn 55905 - usa arthroscopy.pdf · synovectomy may provoke anxiety. ......
TRANSCRIPT

ELBOW ARTHROSCOPY
Shawn W. O'DRISCOLL Mayo Clinic - Rochester, MN 55905 - USA
INTRODUCTION
The field of arthroscopy has experienced remarkable growth and advance in the treatment of elbow disorders in recent years. It is now being performed by an ever increasing number of surgeons for a wide variety of conditions (3, 4, 7, 12, 17, 22, 24, 27, 34, 39, 41, 52). Useful both for diagnosis and treatment, arthroscopic techniques are demanding, and potentially devastating neurovascular injuries are a concern (4, 12, 24, 39, 49). As elbow arthroscopy assumes a greater role in the diagnosis and
management of elbow problems, new indications continue to emerge.
INDICATIONS / CONTRE-INDICATIONS
The indications for elbow arthroscopy include: removal of osteophytes due to impingement or osteoarthritis (2, 32, 33, 37), synovectomy in patients with inflammatory arthritis(2, 12, 13, 52), removal of adhesions and capsular release in patients with contractures(5, 18, 19, 28, 50), resection of symptomatic plicae(7, 8), removal of loose bodies(4, 10, 23, 27, 31, 38), and evaluation of patients with
chronic elbow pain.(34) In addition, elbow arthroscopy has been used to treat patients with osteochondritis dissecans(12, 17, 43, 52), septic arthritis(34, 47), epicondylitis(11), and elbow fractures.(2,
34, 52)
GENERAL TECHNIQUES
The operative techniques in general have been well described elsewhere.(27, 34-36) I prefer the
lateral decubitus position with the forearm allowed to swing free. A soft elastic bandage is then wrapped around the hand and forearm to within ten centimeters of the olecranon. The tourniquet, which is used routinely, is inflated to 250 mm/Hg. The elastic bandage is left on until the end of the procedure to limit the periarticular swelling to the elbow area. When the bandage and tourniquet were removed, any accumulated edema rapidly dissipated into the tissues of the forearm and arm.
With the increasing complexity of the procedures performed, the number of portals used has increased (Figure 1). In addition, more of an emphasis has been placed on utilizing the more proximal portals (proximal anterolateral and anteromedial) portals.

Figure 1 : Graph showing the increasing trend in the average number of portals utilized in elbow arthroscopy over time.
The method and sequence of portal placement varied and evolved over the years. Currently, we
generally start in the direct midlateral portal and establish access through the posterior portals
immediately as well. Open drainage outflow through one or more sites is immediately instituted and maintained throughout the procedure. The posterior compartment is usually treated first and then the anterior portals established for correction of anterior compartment pathology. Portal
placement is determined by careful palpation of the underlying bony structures and we do not rely on skin markings, as the skin markings do not correctly indicate the underlying structures after swelling occurs. We now rely on the use of retractors to permit visualization in the anterior compartment, rather than pressurization to accomplish joint distention. This reduces the risk of edema and even more greatly expands the complexity of surgical procedures that can be performed inside the elbow.
Anterior portal placement has been accomplished using both the outside-in and inside-out techniques, but over time the outside-in technique has become the preferred one. Initially, we believed that edema could be minimized by placing a cannula in each portal and keeping it there
throughout the duration of the procedure, but our practice has been changed. Currently, cannulae
are used only in one or two of the anterior portals. The proximal anterolateral portal is usually used for a retractor and the anterolateral and proximal anteromedial portals for the scope and working instruments. The bulkiness of the cannulae can outweigh their advantages except in the working instrument portal. In more complicated procedures such as those in which extensive bone and capsular work are required, the cannulae may be discarded as periarticular edema develops. This edema actually permits retention of the portal pathway and permits instruments to be readily moved in and out of the elbow, which is usually required.
A previously described system for pressurized irrigation was routinely used and recommended.(36)
The system is a modified pulsatile lavage system that is used to lavage the canal during joint replacement and for the irrigation of open fractures. The spray nozzle is cut off from its connecting tubing, which is then connected to the arthroscope via a standard intravenous line. The driving pressure is set at fifty mm/Hg and flow is controlled by the assistant using the intravenous flow control knob. The auditory feedback (“putt-putt”) of the pulsatile lavage system is invaluable in permitting the surgeon to monitor the fluid flow into the joint without having to consult others or a
display panel. Edema is controlled by always maintaining direct outflow through one or more
portals and also through the shaver device. No drainage tubings are connected to the outflow cannulas or shaver, so that the flow can simply drain to the floor where it is collected by suction.

Entry into a contracted joint is best accomplished using a custom made switching stick that has
been machined to a taper-point at the end. This is machined from a Steinmann pin such that the point is blunt enough so that it will not cut into tissues, yet tapered enough so that it can be used to penetrate the capsule without deflecting off it. Once this blunted Steinmann pin has been placed, the arthroscope sheath is slid into the joint over the pin and the pin withdrawn. We believe this to be easier, safer, and more effective than trying to place the arthroscope sheath containing an obturator into the joint. It also obviates the problem of not being able to distend the capsule in stiff elbows, a step that moves the radial nerve away from the instruments in a normal elbow (Figure 2).
Figure 2 : Importance of capsular distention. The anterior neurovascular structures are very close to the instruments placed in the anterior portals. The radial nerve, which can lie right on the capsule, is an average of only 4 mm from the arthroscope sheath and trocar as it enters the undistended joint (24). With joint distention and the elbow in 90o of flexion, the neurovascular structures are displaced anteriorly and protected. The distance between the radial nerve and the scope increases to about 11 mm with joint distention, making portal establishment much safer. In stiff elbows this distension is not possible.
For a period of time, I routinely established the anterolateral portal first and placed plastic
cannulae in them so as to maximize joint distention and therefore protect the deep radial nerve. Currently, that is no longer done routinely due to accumulated experience with establishing these anterior portals later in the procedure and the fact that the cannula tends to slip out into the soft tissues (which actually permits increased swelling in the anterior soft tissues) while working on the back of the elbow. Thus, there are both advantages and disadvantages of routinely establishing the anterior portals first. It is not clear that the balance favors one or the other approach.
LOOSE BODY REMOVAL
Loose body removal has been considered the prime indication for elbow arthroscopy. Success rates have been consistently reported in the 90% range or better (4, 25, 29, 31, 38).
Loose bodies are removed with various sized graspers that have teeth. ThoseGraspers that are smooth on their outside surface, without irregular surfaces or corners, work best as they do not catch on the soft tissues as they exit the elbow. Always grasp loose bodies so that they can be

pulled out longitudinally, rather than obliquely or transversely, which often requires that they be
rotated into position for the grapser. Grasp them very firmly. Rotate them fully so as to confirm they are not still attached to soft tissue prior to extraction. Observe the fragment until it exits the capsule so that it can be recovered if lost from the jaws of the grasper. Check each one after extraction, to confirm a fragment has not broken off in the soft tissues. Rotate the loose body in the soft tissues to "work it out". Large loose bodies in the anterior elbow can be pushed out with the sheath of the scope (uncouple and back the scope itself out of the sheath a few millimeters to avoid damaging the lens) while pulling it with the grasper. Finally, don't hesitate to enlarge the portal somewhat rather than risk loosing the fragment in the soft tissues.
Synovectomy
Synovectomy is a challenging operation. The very idea of attempting a total arthroscopic synovectomy may provoke anxiety. First, the radial nerve lies right against, or within a few millimters of, the anterolateral joint capsule. Second, the ulnar nerve lies adjacent to the capsule in
the posteromedial gutter. Add to these perils the fact that diffuse proliferative synovitis such as that seen in rheumatoid arthritis can obliterate one's view of the joint.
First, let us consider the problem of visualization. This is a purely technical challenge and can be overcome in a predictable manner. Start working in an area that does not place structures at risk, for example the olecranon fossa, and clear it out. The initial work can be done with poor visualization if both the scope and the shaver are in the fossa. Then work toward the medial gutter. Small pituitary rongeurs are useful for beginning to clear the gutter. The synovium is grasped without fully closing the jaws, so as not to pull out the capsule or ulnar nerve. As the view
enlarges, a 3.5 shaver can be used, with the side cutting opening facing away from the nerve (toward the scope) and gravity outflow without suction. In the anterior elbow, one must use a third portal, such as the proximal anterolateral portal, to place a retractor. A Howarth blunt periosteal
elevator with is easy to place and broad enough to be effective in retracting the anterior capsule. Start working with the shaver against the distal humerus and progress from proximal to distal, and medial to lateral. Again, by having the shaver connected only to gravity outflow and with the opening facing away from the capsule (Figure 3), one can sweep across the capsule and remove
the synovium without perforating the capsule. Capsular release is usually required not just to restore motion, but to eliminate the pain at the limits of motion.
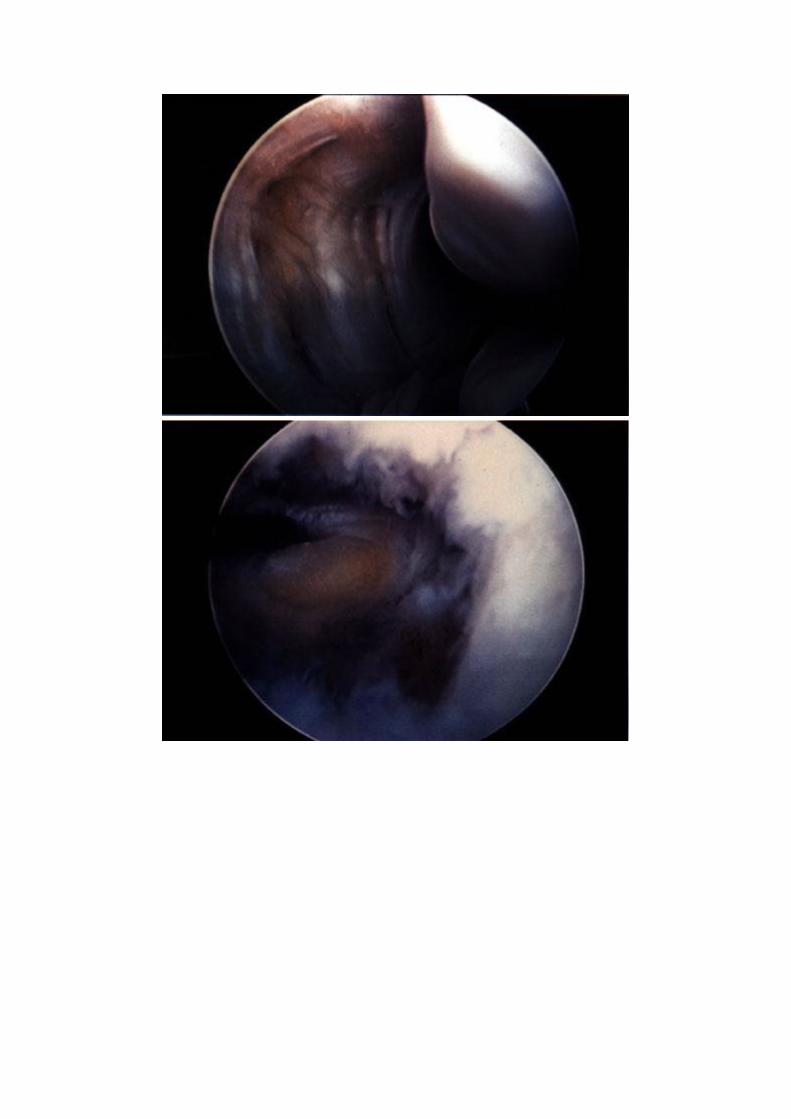

Figure 3 : Synovectomy and clearing of posteromedial gutter plus posteromedial capsular release (A) with extensive synovitis and filling of medial gutter, anatomic landmarks are difficult or impossible to see. A small pituitary grasping instrument can be used to gently tease out loose synovium (without fully closing the jaws of the grasper) until a small shaver can be used to clean it. (B). The capsule should be retained intact until all the synovium is cleared of it. (C, D, & E). On occasion, it may be necessary to expose the ulnar nerve and visualize it in order to safely release the posteromedial capsule. In this case, with significant loss of flexion, a complete posteromedial capsulotomy was required and the ulnar nerve had to be exposed extensively in order to safely do that. Complicating this particular case, the patient also had a small amount of heterotopic ossification beneath the medial epicondyle (top of figure) that required removal.
CAPSULAR RELEASE
The performance of a contracture release in our experience has beenis best conducted in a stepwise manner as follows: The first step involves synovectomy and removal of any soft tissue
that may block motion due to its bulk, such as scar tissue in the olecranon fossa. The second step involves removal of osteophytes from the olecranon and coronoid as well as restoration of the normal depth and contour of the fossae for the( olecranon, coronoid, and radial head). If motion is still limited, as is almost always the case, the final stage is capsular release, which is described

above..
The nerves can be visualized arthroscopically from inside the joint to permit safe resection of the capsule while observing the nerves under direct vision a safe distance from the cutting instrument. A full description of the technique of arthroscopic nerve exploration is not possible in this paper. The location of the nerve behind the capsule is first based on the knowledge of three-dimensional anatomy of the elbow and then the capsule is incised with a wide duckbill basket punch biopsy. In the case of the ulnar nerve, the nerve is also palpated with a blunt probe through the capsule before the capsule is opened (Figure 3). The soft tissue behind the capsule is dissected away to
create a plane for safe incision of the capsule. The nerve is then gently palpated through the opening of the capsule and the dissection continued until the fat around the nerve is visualized. The nerve itself is then visualized and once under direct vision the rest of the capsule is incised or excised.
Figure 4 (A & B) : Capsular stripping. The anterior capsule can be stripped off the humerus with a blunt periosteal elevator.

Capsular release can be performed in one of three sequential stages. Blunt stripping of the capsule
off the humerus can be performed with a periosteal elevator (Figure 4). It is probably associated with minimal risk. However, it does not seem to be as effective as capsulotomy or capsulectomy. The next stage would be capsulotomy, or division of the capsule (Figure 5). This is best and most safely performed with a hand instrument such a wide duck-billed basket punch biopsy. The anterior capsule is most safely cut across its midsection, starting from medial and working toward the lateral side. The plane of dissection between the capsule/scar and brachialis is more obvious medially than laterally. Finally, capsulectomy (excision of the capsule) can be performed after the
previous two stages have been completed (Figure 5). This is best performed with a shaver using no suction, but the outflow on the shaver simply left open to let drainage fall to the floor. One should progress from proximal medial to distal medial, then proximal lateral to distal lateral. This last region is the site of greatest risk of nerve injury.

Figure 5 : Capuslotomy/capsulectomy. (A). The capsulotomy is performed with a hand instrument such as a duckbill basket punch forceps. (B). If capsulectomy is performed, the shaver should be directed away from the brachialis and the nerves. No section is used. (C). In some cases, the radial nerve may need to be identified in order to safely remove the capsule with certainty that the nerve is not being damaged.
Capsulectomy is a procedure that requires the highest level of arthroscopic expertise and
experience in open elbow surgery as well. Under no other circumstances should it be performed, for the risk of injury to a major nerve would be unacceptably high.
OSTEOCAPSULAR ARTHROPLASTY
Figure 6 : Radiographic findings in osteoarthritis of the elbow. (A). Anteroposterior radiograph

reveals loss of definition of the coronoid and olecranon fossae due to thickening of the bone in this region and osteophyte formation. (B). Lateral radiograph demonstrates the osteophytes on the olecranon (arrow). The anterior osteophytes are sometimes more difficult to distinguish. (C). Lateral tomograms are the imaging study of choice to visualize the osteophytes on the olecranon and coronoid (solid arrows) as well as those in and around the olecranon and coronoid fossae (hollow arrows).
One of the most rewarding arthroscopic interventions is osteocapsular arthroplasty for
osteoarthritis (32, 37). This procedure involves four components to treat the characteristic pathological changes (Figure 6): (1) removal of all loose bodies, including those that are not loose, but stuck in the synovium, (2) removal of all osteophytes in the ulnohumeral articulation including those on the olecranon, coronoid, medial trochlea, and in the 3 fossae – olecranon, coronoid, and
radial, (3) total synovectomy, and (4) anterior and posterior capsulectomy, with posteromedial and posterolateral capsulectomy for those patients lacking significant degrees of flexion. In patients with preexistant ulnar neuritis or neuropathy, and those with severe loss of flexion, the ulnar nerve is transposed subcutaneously as well (Figure 7).
Figure 7 : In cases of arthritis (primary or posttraumatic) with significant loss of flexion, it may be necessary to transpose the ulnar nerve anteriorly in the subcutaneous position to prevent postoperative stretch induced ulnar neuropathy. In those cases, the transposition is performed first and then the open incision is used for some of the portal access. The ulnar nerve is kept under direct visualization the whole time.
There are three option for capsular release, with increasing difficulty and increasing efficacy
(Figures 4 & 5). The safest technique, but least effective is blunt stripping of the capsule off the humerus with a periosteal elevator. The next stage is capsulotomy, or division of the capsule. Finally, capsulectomy (excision of the capsule) involves complete removal of the capsule and associated scar tissue. Capsular release (in my experience, capsulectomy) is an integral component of osteocapsular arthroplasty.
Osteocapsular arthroplasty is an extensive operation, requiring substantial skill and experience. The respective loose body and synovectomy components of the operation are as described above. The osteophyte removal is accomplished with a combination of instruments, principally burrs. Osteotomes can be useful, but removal of the osteotomized fragment can be tedious due to sharp edges and soft tissue attachments. The shaver (rather than burr) can be used once the bone has been cut into and trabecular bone exposed. A shaver is less likely to wrap up soft tissue, which puts nerves at risk, than is a burr.

Figure 8 : (A) In osteoarthritis the anterior compartment often has numerous loose bodies as well. Five are seen here in obscuring the coronoid (C) and trochlea (T). (B) After removing the loose bodies, the coronoid osteophyte is removed with a burr or osteotome. (C/D). The coronoid fossa is usually filled in with bone in osteoarthritis. The fossa must be recreated with a burr.
To most effectively and safely perform these more complex osteocapsular procedures, one should proceed in a logical manner. First establish the view and place one or two retractors into the joint.
Second, clean up the joint by removing loose bodies and performing a synovectomy. Debride the capsule of any loose scar tissue so that it has the appearance and texture of a structure. Remove the osteophytes and clean up the bone debris (Figures 8 & 9). Strip the capsule off the humerus if not already done (it is useful to do this earlier if the joint is quite tight) (Figure 4). Cut the capsule with the duck-bill basket biopsy punch (Figure 5). Excise the capsule with the shaver. Then incise and resect the capsule just anterior to the medial and lateral collateral ligaments. By following this stepwise sequence, one can progress within the limits of one’s skill with the least likelihood of complications.

Figure 9 : (A) Multiple loose bodies were removed from this patient, ranging in size from a few millimeters to 2 centimeters. Different size graspers were needed. On the right hand side of the picture are the osteophyte fragments that were removed using the osteotome and graspers illustrated. (B). Preoperative radiograph of the same patient. Multiple loose bodies are seen anteriorly and posteriorly. In addition, osteophytes (dark arrows) are seen on the olecranon and coronoid. The trochlea has osteophytes at the bottom of the olecranon and coronoid fossae (hollow arrows), so that the trochlea has become "U-shaped" rather than "O-shaped". These must be removed to eliminate impingement and gain motion. (C). Postoperatively, the osteophytes and loose bodies are not seen.
POSTOPERATIVE MANAGEMENT
A compressive dressing is wrapped around the elbow and the patient instructed to start using the
elbow as tolerated. It is kept elevated when not in use for the first day to decrease swelling. If the procedure was performed for improving motion or for the treatment of arthritis, an indwelling catheter is inserted for brachial plexus block anesthetic if the neurologic exam is normal in the recovery room, and the patient started on a full range of motion on a CPM machine the same day.
All circumferential dressings must be removed to avoid skin damage during CPM. Only an elastic
sleeve is used to hold the absorbent dressing in place.
RESULTS
During the past decade the complexity and extent of the procedures has increased dramatically. Figure 10 shows that the average complexity of the arthroscopic procedures increased exponentially from 1980 to 1998 with the greatest increases in the last six years (R2 = 0.96; p < 0.0001). Figure 1 shows the increased number of portals used per procedure. From 1980 to 1992, the average number of portals used was less than three. However, from 1993 to 1998, the average number of portals used increased from three to five per procedure.

Figure 10 : Graph showing the exponential increase in the complexity of elbow arthroscopy procedures over time.
While there has been a dramatic increase in the average complexity of procedures performed, our
experience has demonstrated a much lesser increase in the total complications (R2 = 0.13; p <
0.05; Figure 11). More importantly, however, Figure 12 shows that the rate of neurologic complications did not increase as the complexity of the procedures did (R2 = 0.002; p = 0.48). In fact, the rate of nerve palsies declined slightly during the same time period.
Figure 11 : Graph showing the slight increase in the average annual rate of complications following elbow arthroscopy.

Diagnostic Benefits. O'Driscoll and Morrey evaluated the diagnostic and therapeutic usefulness of
arthroscopy (34). A diagnostic arthroscopy was considered beneficial if a patient's outcome was positively influenced by the procedure, i.e. the correct final diagnosis was (a) changed from that of the preoperative diagnosis, which was proved to be incorrect; (b) established when the diagnosis could not be made preoperatively; or (c) expanded or confirmed when the preoperative diagnosis was incomplete or uncertain. The procedure was said to be of therapeutic benefit to the patient if it was (a) completely successful and obviated the need for any further surgery, (b) partially successful in that the patient was clinically improved and needed no further surgery, or (c)
adjunctive in that an important part of the operation was performed arthroscopically and the arthroscopy directed the surgical intervention in an important manner. Of the 71 consecutive arthroscopies in that series, approximately three quarters of the patients who undergo arthroscopy of the elbow benefit (34). The distribution according to type of benefits were 31% diagnostic benefit, 24% both diagnostic and therapeutic, and 17% therapeutic benefit only.
Figure 12 : Graph showing the decrease in the average annual rate of transient nerve palsies following elbow arthroscopy.
Until recently the ideal indication for operative arthroscopy has been considered to be removal of
loose bodies, with greater than 90% success rates reported (4, 31, 34). Currently, it has become our impression that treatment of osteoarthritis by osteocapsular arthroplasty, which includes excision
of loose bodies and osteophytes from the olecranon and coronoid, as well as from each respective fossa, and capsular release may be one of the most gratifying procedures, as it is usually so predictably effective and beneficial in terms of both pain relief and restoration of motion.
Redden and Stanley reported 12 of 12 patients with osteoarthritis and loose bodies to benefit from arthroscopic removal of osteophytes and loose bodies (42). They performed a fenestration of the distal humerus through the olecranon fossa to the coronoid fossa. They did not notice any improvement in elbow range of motion, presumably because they did not release the capsular contractures. Successful arthroscopic treatment of symptomatic lateral synovial plicae has been reported (7). This
condition, which may be suggestive of loose bodies or recalcitrant tennis elbow, can be diagnosed arthroscopically and treated by excision of the plica.
Little data exist regarding arthroscopic synovectomy. This is due to the fact that not until recently did we become comfortable with the technical challenges and execution of the procedure.

Satisfactory pain relief is obtained in about 75% – 90% of cases. Range of motion is improved,
particularly if one is careful to remove the contracted capsule and scar tissue around the elbow.
The role of radial head excision is not clear. Theoretically, the risk of late deterioration to increased
biomechanical loading of the ulnohumeral articulation will occur if the radial head is excised. The radial head should probably be left in unless the indications above are present, as its role in stability would be greater in a rheumatoid elbow, which has already suffered bone loss and soft tissue damage.
Lee and Morrey reported on 14 synovectomies in 11 patients with rheumatoid arthritis (21). They had a 93% early success, which declined to 57% by 3.5 years, but concluded that the decline might have been due to limitations of the arthroscopic technique. Those procedures were not total synovectomies and did not include capsular releases. Current experience in our institution suggests that both of these factors are important. Further follow-up will be necessary to ascertain the long-
term benefit. Also, the role of arthroscopic synovectomy in more advanced stages of disease and
joint destruction remain to be determined. Our experience indicates that there are a percentage of patients who will benefit regardless of the stage of disease. Arthroscopic capsular release for contracture of the elbow is being performed more frequently now. It has been shown be several authors to be effective (18, 40), but complications such nerve transection have been reported (14, 18). Although the safety of this procedure remains to be confirmed, it seems likely that the decreased morbidity and increased surgical access to remove all
contracted tissue may bring this procedure into the mainstay of treatment of the stiff elbow (30). My anecdotal impression, after treating a large number of stiff elbows by both open and arthroscopic capsulectomy, is that arthroscopic release is as effective as open release, if not more so (Figure 13). The relative importance of capsulotomy versus capsulectomy is yet to be clarified.


Figure 13 (A, B, C, D) : Clinical preoperative and postoperative photographs of the left arm of patient with a severe posttraumatic contracture with near ankylosis of the elbow preoperatively as a result of a severe open fracture treated with three surgeries including a prior attempt at open capsular release. Two months following an arthroscopic total capsulectomy, his motion is almost full. He returned to full active use of that arm in physical labor.
COMPLICATIONS
In a review of almost 500 consecutive elbow arthroscopies by Kelly et al, complications occurred in 11%. They include the following:
Persistent drainage from the portals. Deep infection
Minor contractures, usually related to nature of the underlying condition (such as
inflammatory arthritis). Transient palsies caused by extravasation of local anesthetic, direct blunt trauma,
compression by the tourniquet or forearm wrapping, or the use of the indwelling catheter postoperatively.
Permanent nerve injury.
The reported prevalence of neurologic complications after elbow arthroscopy has ranged from 0 to 14 percent.(2, 12, 19, 34, 45-48, 51) In the report of our patients by Kelly et al, there were no permanent
neurologic injuries, while ten of the 473 (2.5 percent) patients did suffer transient nerve palsies. The nerve-to-portal distances increase with joint distension although the nerve does not move further away from the capsule.(1, 2, 24, 26) Also, capsular distension is often not possible in elbows with contractures, as they have a loss of intracapsular capacity to an average of six milliliters.(9) Nerve injuries associated with elbow arthroscopy have been reported to result from compression(24,
39), local anesthetic(2, 27), or direct trauma(6, 24, 44, 49), intra-articular local anesthetic injection,
prolonged tourniquet compression, and forearm compression from wrapping it too tightly. Cutting only through the skin can protect the superficial nerves with the knife blade, making certain to drag the skin across the blade rather than making a stab incision. Permanent nerve injury. Although we have not experienced any permanent nerve or vascular
injuries, the risk of injury to these structures is real and transections of all three major nerves have been reported. The anterolateral and the anteromedial portals are most likely to be associated with nerve injury due to the proximities of the radial, posterior interosseous, ulnar, and median nerves
to these portals (3, 22, 24, 39). These injuries are best avoided by careful technique and constant

vigilance. The distances between these nerves and all of the portals are increased substantially by
flexing the elbow to 90o and distending the joint with saline (39). Displacement of the nerves anteriorly away from the portals is accomplished by capsular distention with 15 to 25 ml of saline, but the average intracapsular capacity of stiff elbows is only 6 ml (Figure 2). Thus, the capsule cannot be distended away from the instruments in stiff elbows.
DISCUSSION
In considering the future of elbow arthroscopy, two issues dominate. First, arthroscopy appears to
be highly useful for the treatment of arthritis and contractures. Second, the ultimate role that this technology will play in our patients will be determined principally by how successful we are in avoiding nerve injuries.
The reported prevalence of neurologic complications after elbow arthroscopy has ranged from 0 to 14 percent.(2, 14, 27, 40, 50-52, 54, 61) In our series, there were no permanent neurologic injuries, while ten of the 473 (2.5 percent) patients did suffer transient nerve palsies. The The nerve-to-portal
distances increase with joint distension although the nerve does not move further away from the capsule.(1, 2, 31, 34) Also, capsular distension is often not possible in elbows with contractures, as they have a loss of intracapsular capacity to an average of six milliliters.(11) Nerve injuries associated with elbow arthroscopy have been reported to result from compression(31,
45), local anesthetic(2, 35), or direct trauma(9 31, 48, 58), , intra-articular local anesthetic injection, prolonged tourniquet compression, and forearm compression from wrapping it too tightly. Cutting only through the skin can protect the superficial nerves with the knife blade, making certain to
drag the skin across the blade rather than making a stab incision. For a period of time, I routinely established the anterolateral portal first and placed plastic cannulae in them so as to maximize joint distention and therefore protect the deep radial nerve. Currently, that is no longer done routinely due to accumulated experience with establishing these anterior portals later in the procedure and the fact that the cannula tends to slip out into the soft
tissues (which actually permits increased swelling in the anterior soft tissues) while working on the back of the elbow. Thus, there are both advantages and disadvantages of routinely establishing the
anterior portals first. It is not clear that the balance favors one or the other approach. Entry into a contracted joint is best accomplished using a custom made switching stick that has been machined to a taper-point at the end. This is machined from a Steinmann pin such that the point is blunt enough so that it will not cut into tissues, yet tapered enough so that it can be used to penetrate the capsule without deflecting off it. Once this blunted Steinmann pin has been placed, the arthroscope sheath is slid into the joint over the pin and the pin withdrawn. We believe this to
be easier, safer, and more effective than trying to place the arthroscope sheath containing an obturator into the joint. It is likely that nerve injuries are related more to the use, than selection, of instruments. In general, we used a 4.0-millimeter arthroscope and motorized shavers ranging from 3.5 to 5.5 millimeters are used. Suction is avoided near the nerves and motorized instruments are directed away from the nerves rather than towards them. Despite the lack of a direct relationship between nerve injury and elbow contracture in our series,
we A believe a loss of capsular space contracture increases the difficulty of the procedure. Kim and coworkers reported two transient median nerve palsies after arthroscopic capsulectomy in patients with contractures.(19) Jones and Savoie also reported a posterior interosseous nerve transection in a patient with an elbow contracture who had a capsulectomy performed.(18) Haapaniemi and colleagues reported a case of complete transection of the median and radial nerves in a patient with post-traumatic elbow cContracture treated by arthroscopic capsular release.(14) The literature reports at least two complete nerve transections have occurred during synovectomy
in patients with rheumatoid arthritis who are believed to be at increased risk for nerve injury during elbow arthroscopy.(44) Ruch and Poehling noted that patients with rheumatoid arthritis have a “thin and filmy capsule.” We agree, and would add that the altered bony architecture impairs the surgeon from predicting the nerve location, due to loss of normal intra-articular landmarks. In our series, seven of the ten patients with nerve complications had rheumatoid arthritis, although rheumatoid arthritis was present in only seventy-five of the 449 patients. However, no patient
sustained a complete nerve injury or evidence of a nerve laceration in our series of these complex procedures.
It has now become our my routine practice to release the capsule in rheumatoid patients with significant elbow contractures. Thus, the indications for contracture release in the rheumatoid population are the same as those in the general population (i.e. loss of motion impeding functional activities of daily living). Based on substantial further experience with these types of procedures,

we attribute the relative absence of a serious nerve injury to a determined attempt to identify the
nerves prior to resecting tissue in close proximity to them. Injury to the ulnar nerve for example, can perhaps best be avoided by completing the synovectomy and osteophyte removal prior to incising the posteromedial capsule. Exceptions to the rule include patients with severe synovitis and thinning of the capsule, or revision cases in which the capsule has already been excised. During the years that we have been performing arthroscopy, the complexities of the procedures we perform has increased markedly and continues to do so (Figure 10). Figure 11 shows the slight increase in the overall complication rate seen in elbow arthroscopy patients over time. More
importantly, Figure 12 demonstrates that the incidence of nerve complications did not increase as the complexity did, but in fact decreased slightly over time. More importantly, none of these were permanent motor deficits. These findings indicate that as a surgeon becomes more skilled and knowledgeable in a given surgical procedure, procedures that are technically more challenging can be performed without necessarily increasing the risk of complications. In other words, the risk of nerve injury is determined not just by the procedure, but also by the operating surgeon, amongst
other factors. It is our belief that substantial experience with open elbow surgery and anatomy,
combined with a very cautious attitude towards adopting or starting new techniques, permitted the more complicated surgeries to be performed without serious permanent complications. It has been well established in the medical literature that complication rates vary by surgeon and center following procedures varying from total hip arthroplasty(20) to coronary angiography.(15, 16) The single most important technical factor that we I believe can prevented serious nerve injuries was is the use of retractors. We I now routinely use one or two retractors in the anterior elbow
when performing synovectomy, or capsulectomy, or other complex procedures. This greatly facilitates exposure in addition to reducing the risk. Currently, it is my opinion (which I believe reflects the opinion of other experts) that anterior or posterior capsulectomy should be performed only by surgeons who are experienced in the performance of such procedures using open techniques, and also have substantial expertise in arthroscopy. The operating surgeon must either be able to identify the radial and ulnar nerves at the time of anterior or posteromedial capsulectomy respectively, or have sufficient experience with
this procedure, and knowledge of the neural anatomy in relation to the capsule and intra-articular structures, that such visualization of the nerves is simply not necessary in his/her hands. This
would be an example of a procedure that should not, at the present time, be carried out by an occasional elbow arthroscopist. However, with time, significant advances will accrue in surgeons’ familiarity with the normal and abnormal elbow anatomy as well as with both open and arthroscopic procedures around the elbow. It could reasonably be expected that with such
advances in this area, capsulectomy could become standard practice. A thorough understanding of the three-dimensional anatomy of the elbow and surrounding nerves, effects of joint distention, correct portal placement, recognition of “at risk” procedures and strong arthroscopic skills are necessary to prevent serious complications, particularly as more complicated procedures are performed. The individual surgeon should not only recognize and acknowledge what is beyond the limits of his or her experience and skill, but also exercise judgment so as to ensure an adequate margin of safety in applying arthroscopic techniques to this joint. Of the various
factors to which we attribute the absence of any serious nerve injuries in our experience to date, we feel that none bears more significance that the concept of maintaining a margin of safety at the limits of one’s capabilities. By so doing, and by realizing that what one can do and what can be done are not always the same, the risks of serious complications may be kept to a minimum.
References
1. ADOLFSSON L. Arthroscopy of the elbow joint: a cadaveric study of
portal placement. J Shoulder Elbow Surg. 3: 53-61, 1994.
2. ANDREWS JR, CARSON WG. Arthroscopy of the elbow. Arthroscopy. 1: 97-107, 1985.
3. ANDREWS JR, ST. PIERRE RK, CARSON WG. Arthroscopy of the elbow. Clinics Sport Med. 5: 653-662, 1986.
4. BOE S. Arthroscopy of the elbow. Diagnosis and extraction of loose

bodies. Acta Orthop Scand. 57: 52-53, 1986.
5. BYRD JW. Elbow arthroscopy for arthrofibrosis after type I radial head fractures. Arthroscopy. 10: 162-165, 1994.
6. CASSCELLS SW. Editor's Comment. Neurovascular anatomy and elbow arthroscopy: Inherent risks. Arthroscopy. 2: 190, 1986.
7. CLARKE R. Symptomatic, lateral synovial fringe (plica) of the elbow
joint. Arthroscopy. 4: 112-116, 1988.
8. COMMANDRE F, TAILLAN B, BENEZIS C, FOLLACCI F, HAMMOU
J. Plica synovialis (synovial fold) of the elbow. Report on one case. J Sports Med Phys Fit. 28: 209-210, 1988.
9. GALLAY SH, RICHARDS RR, O'DRISCOLL SW. Intraarticular
capacity and compliance of stiff and normal elbows. Arthroscopy. 9: 9-
13, 1993.
10. GREIS PE, HALBRECHT J, PLANCHER KD. Arthroscopic removal of loose bodies of the elbow. Orthop Clin North Am. 26: 679-89., 1995.
11. GRIFKA J, BOENKE S, KRAMER J. Endoscopic therapy in epicondylitis radialis humeri. Arthroscopy. 11: 743-8., 1995.
12. GUHL J. Arthroscopy and arthroscopic surgery of the elbow. Orthopedics. 8: 1290-1296, 1985.
13. GUHL J. "Arthroscopic surgery of the elbow." Arthroscopic Surgery. Parisien J ed. 1988 McGraw-Hill. New York: 249-258.
14. HAAPANIEMI T, BERGGREN M, ADOLFSSON L. Complete
transection of the median and radial nerves during arthroscopic release of post-traumatic elbow contracture. Arthroscopy. 15: 784-7, 1999.
15. HANNAN EL, O'DONNELL JF, KILBURN H, JR., BERNARD HR,
YAZICI A. Investigation of the relationship between volume and
mortality for surgical procedures performed in New York State hospitals.
Jama. 262: 503-10., 1989.
16. HANNAN EL, RACZ M, RYAN TJ, McCALLISTER BD, JOHNSON
LW, ARANI DT, GUERCI AD, SOSA J, TOPOL EJ. Coronary angioplasty
volume-outcome relationships for hospitals and cardiologists. JAMA. 277:
892-898, 1997.
17. JACKSON D, SILVINO N, REIMAN P. Osteochondritis in the female
gymnast's elbow. Arthroscopy. 5: 129-136, 1989.
18. JONES GS, SAVOIE FH, III. Arthroscopic capsular release of
flexion contractures (arthrofibrosis) of the elbow. Arthroscopy. 9: 277-283, 1993.
19. KIM SJ, KIM HK, LEE JW. Arthroscopy for limitation of motion of

the elbow. Arthroscopy. 11: 680-3., 1995.
20. KREDER HJ, DEYO RA, KOEPSELL T, SWIONTKOWSKI MF,
KREUTER W. Relationship between the volume of total hip replacements
performed by providers and the rates of postoperative complications in
the state of Washington. J Bone Joint Surg. 79A: 485-494, 1997.
21. LEE BPH, MORREY BF. Arthroscopic synovectomy of the elbow for rheumatoid arthritis. J Bone Joint Surg. 79: 770-772, 1997.
22. LINDENFELD TN. Medial approach in elbow arthroscopy. Am J Sports Med. 18: 413-417, 1990.
23. LOKIETEK JC, DE CLOEDT P, LEGAYE J, LOKIETEK W.
[Extraction of a foreign body from the elbow using arthroscopy]. Rev Chir
Orthop Reparatrice Appar Mot. 74: 93-8, 1988.
24. LYNCH G, MEYERS J, WHIPPLE T, CASPARI R. Neurovascular
anatomy and elbow arthroscopy: Inherent risks. Arthroscopy. 2: 191-197, 1986.
25. McGINTY J. Arthroscopic removal of loose bodies. Orthop Clin N Amer. 13: 313-328, 1982.
26. MILLER C, JOBE C, WRIGHT M. Neuroanatomy in elbow
arthroscopy. J Shoulder Elbow Surg. 4: 168-74, 1995.
27. MORREY BF. Arthroscopy of the elbow. Instructional Course Lec. 35: 102-107, 1986.
28. NOWICKI KD, SHALL LM. Arthroscopic release of a posttraumatic
flexion contracture in the elbow: a case report and review of the literature. Arthroscopy. 8: 544-547, 1992.
29. O'DRISCOLL S. "Elbow arthroscopy: loose bodies." The Elbow and
its Disorders. Morrey B ed. 2000 W.B. Saunders Company. Philadelphia: 510-514.
30. O'DRISCOLL S. "Elbow arthroscopy: the future." The Elbow and its
Disorders. Morrey B ed. 2000 W.B. Saunders Company. Philadelphia: 522.
31. O'DRISCOLL SW. Elbow arthroscopy for loose bodies. Orthopedics.
15: 855-859, 1992.
32. O'DRISCOLL SW. Arthroscopic treatment for osteoarthritis of the
elbow. Orthop Clin North Am. 26: 691-706, 1995.
33. O'DRISCOLL SW. Operative treatment of elbow arthritis. Curr Opin Rheum. 7: 103-106, 1995.
34. O'DRISCOLL SW, MORREY BF. Arthroscopy of the elbow:
Diagnostic and therapeutic benefits and hazards. J Bone Joint Surg. 74-

A: 84-94, 1992.
35. O'DRISCOLL SW, MORREY BF. "Arthroscopy of the elbow." The
elbow and its disorders. Morrey BF ed. 1993 W.B. Saunders Company. Philadelphia: 120-130.
36. O'DRISCOLL SW, MORREY BF. "Arthroscopy of the elbow." Master
techniques in orthopedic surgery: The elbow. Morrey BF ed. 1994 Raven Press. New York: 21-34.
37. OGILVIE-HARRIS DJ, GORDON R, MacKAY M. Arthroscopic
treatment for posterior impingement in degenerative arthritis of the elbow. Arthroscopy. 11: 437-43, 1995.
38. OGILVIE-HARRIS DJ, SCHEMITSCH E. Arthroscopy of the elbow
for removal of loose bodies. Arthroscopy. 9: 5-8, 1993.
39. PAPILION J, NEFF R, SHALL L. Compression neuropathy of the
radial nerve as a complication of elbow arthroscopy: A case report and review of the literature. Arthroscopy. 4: 284-286, 1988.
40. PHILLIPS BB, STRASBURGER S. Arthroscopic treatment of arthrosibrosis of the elbow joint. Arthroscopy. 14: 38-44, 1998.
41. POEHLING G, WHIPPLE T, SISCO L, GOLDMAN B. Elbow
arthroscopy: A new technique. Arthroscopy. 5: 222-224, 1989.
42. REDDEN JF, STANLEY D. Arthroscopic fenestration of the olecranon
fossa in the treatment of osteoarthritis of the elbow. Arthroscopy. 9: 14-16, 1993.
43. RUCH DS, POEHLING GG. Arthroscopic treatment of Panner's disease. Clin Sports Med. 10: 629-36., 1991.
44. RUCH DS, POEHLING GG. Anterior interosseus nerve injury
following elbow arthroscopy. Arthroscopy. 13: 756-8., 1997.
45. SAVOIE FH, 3rd, FIELD LD. "Complications of elbow arthroscopy."
Arthroscopy of the elbow. Savoie FH, 3rd, Field LD ed. 1996 Churchill Livingston Inc. New York: 178.
46. SCHNEIDER T, HOFFSTETTER I, FINK B, JEROSCH J. Long-term
results of elbow arthroscopy in 67 patients. Acta Orthop Belg. 60: 378-
383, 1994.
47. SHEPPARD J, MARION J, HURST D. Arthroscopic elbow surgery:
five year experience and observations in 48 cases. Am J Arthroscopy. 1: 13-19, 1991.
48. SMALL NC. Complications in arthroscopic surgery performed by experienced arthroscopists. Arthroscopy. 4: 215-221, 1988.
49. THOMAS M, FAST A, SHAPIRO D. Radial nerve damage as a

complication of elbow arthroscopy. Clin Orthop. 215: 130-131, 1987.
50. TIMMERMAN LA, ANDREWS JR. Arthroscopic treatment of
posttraumatic elbow pain and stiffness. Am J Sports Med. 22: 230-235, 1994.
51. WARD WG, ANDERSON TE. Elbow arthroscopy in a mostly athletic
population. J Hand Surg. 18A: 220-224, 1993.
52. WOODS G. Elbow arthroscopy. Clinics Sport Med. 6: 557-564, 1987.
Maîtrise Orthopédique n°115 - June 2002