mathy vanbuel, atit, belgium - using 3d for training of surgeons
TRANSCRIPT

Using 3D for training of surgeonsMathy Vanbuel

Training Consultancy
Production Management
ATiT

Production
History in the Mirror, 2016
• Documentary on classroom practice
• Ministry of education, Flanders
Gynetics Product Wizard, 2015
• Aimed at IVF centres
• Integrated platform with video, animation
Medical Training Events
• Integra Ankle Arthrosis Training Event, Leuven
• Interactive HD Video links from multiple hospitals

Production ESGE2014: day 1 and 2
• 7 x 90 min live surgeries via videoconferencing (SD – 2 Mbps videoconference H.323) from 7 different surgical hospitals in Belgium
• 1 Operation theatre per hospital

Gent
Godinne
GentGent
Bonheiden
Liege
LeuvenBrussels



Production ESGE2014: day 3 and 4
• 2 x 240 mins live surgeries via satellite in HD-3D from 3 different surgical hospitals in Belgium
• Day 3: 1 Operation theatre in hospital A (Leuven)1 Operation theatre in hospital B (Leuven)
• Day 4: 4 Operation theatres in hospital C (Brussels)

Operation theatre
• 3D endoscopic image sources operated by surgeon:
• Storz (DVI-I 1080/60p line by line)
• Olympus (HD-SDI 1080/50i side by side)
• 3D field cameras Panasonic AG-3DA1 (HD-SDI 1080/50i side by side), operated by camera operator
• 3D Video mixers (cascaded)
• 3D monitors (surgeon + switcher)
• Headsets microphone surgeon
• Loudspeakers
• Audio mixer (n-1)
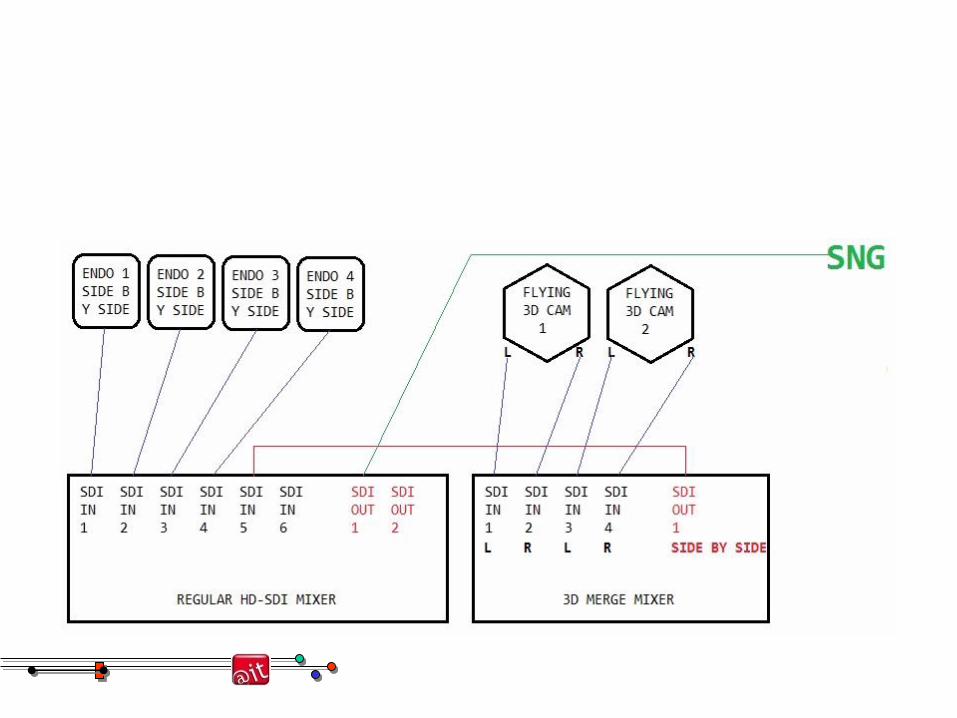

Video
OT6-9 4 x Camera Olympus Endoscopie: output 3D side by side Mixer SNG Square
2 x External camera 3D
Audio
Audio PGM (4 x OK) Microphone headset surgeon (OK 6-9) Audio mixer SNG Square
Hand mcrophone on stand (OK 6-9)
Audio return (From Brussels Square) Skype Headset surgeon (OK 6-9)
Alto speaker (OK 6-9)
Alternative audio return (option as “Intercom”) (From Brussels Square) GSM Headset surgeon (OK 6-9)
Alto speaker (OK 6-9)

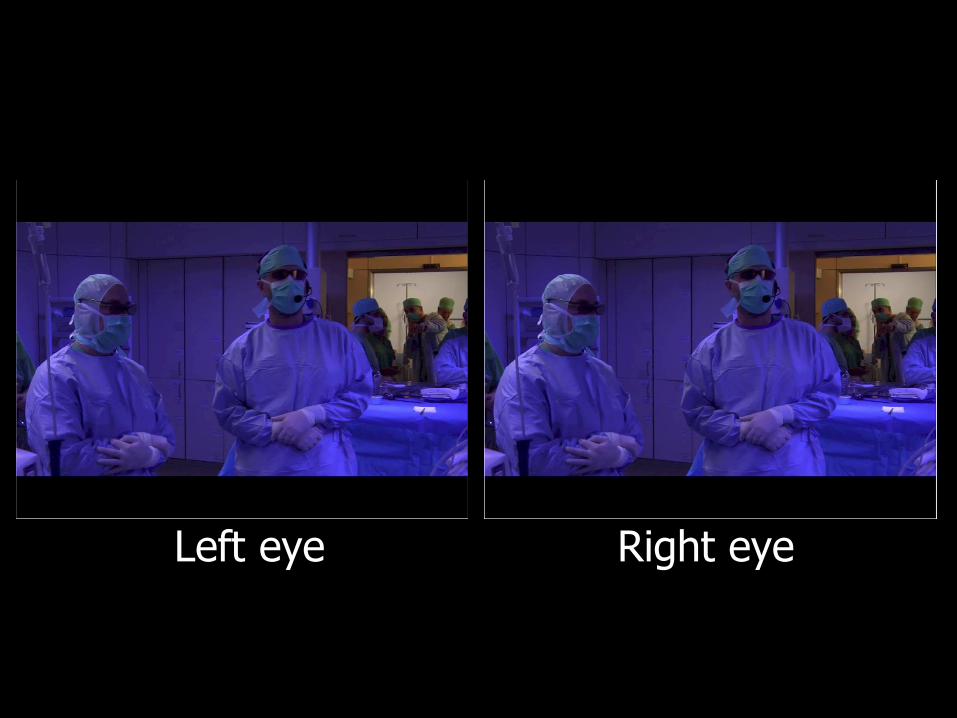
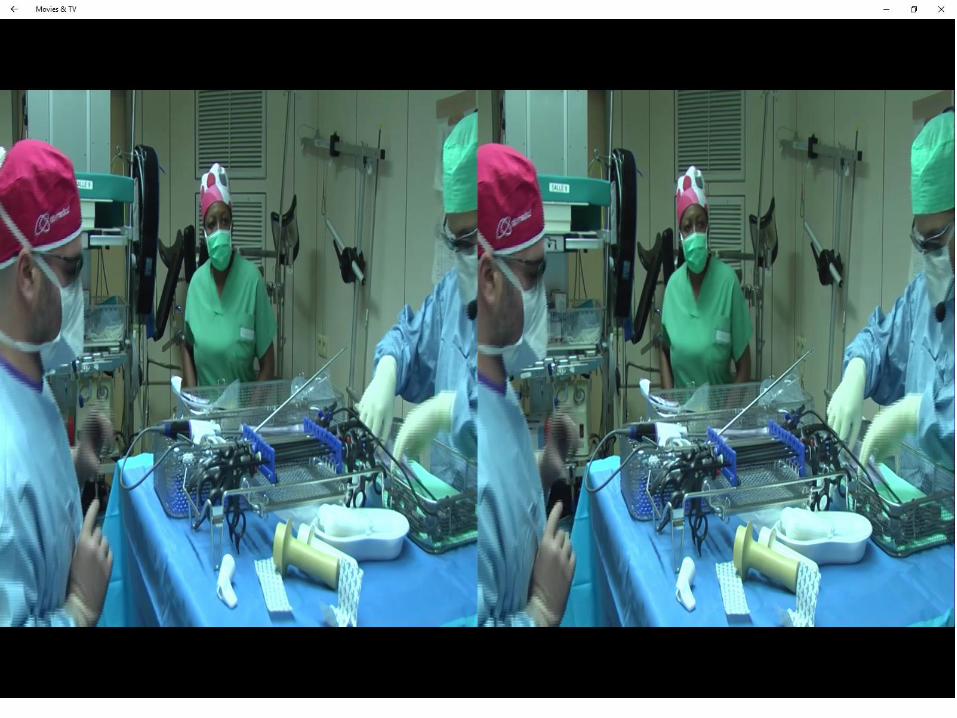
Left eye Right eye

1080 px x 1920 px

1080 px x 1920 px


Transmission
• Mpeg4, 16 Mbps
• DVB-S2 Satellite one way A+V (even over short distance, due to the terrain)
• Audio return via IP phone with GSM back up



Reception and display
• Requirements:
• High definition
• No active viewing glasses (not manageable in a non permanent situation)
• One day: pola glasses (because of availability of branded glasses)
• Second day: Infitec technology (selective interference filters)
• 3 projectors (Left + Right + spare)
• High intensity projection needed (filters take light away)


Viewing
• Active glasses
• Expensive, noisy, faulty, heavy, uncomfortable
• Excellent discretion
• Pola glasses
• Cheap to produce (but quality matters: axis adjustment, quality of filter)
• Takes light away
• Requires special (expensive) screen
• Interference glasses
• Moderately expense (70 Euros piece)
• Recyclable (cleaning needed)
• Any white screen will do





Reactions
• Both technologies (polar and infitec) were received equally (but were we comparing like with like?)
• Satisfaction is almost 80 %
• Complains about:
• Disturbing light diffraction (doors opening and closing, room lights dimmed…)
• Nauseatic reaction to camera handling (endoscopy, tunneling effect)
• Surgeons: (small informal survey)
• 50% considers a major advantage,
• 30% does not see any advantage
• 20% gets nauseatic or is stereo blind

Conclusions
• High additional cost (about 50%)
• At all levels: installation, QA
• Lack of dominant standards causes technical challenges
• Capturing, recording and transmission, display, distribution
• The use of glasses is a big disadvantage
• Use in the OT is increasingly becoming a standard (but expensive) practice especially with operation robots (Da Vinci)
