maternal and fetal cardiovascular response to exercise during pregnancy
TRANSCRIPT

Maternal and Fetal Cardiovascular Response to Exercise During Pregnancy Jean-Claude Veille
With the two-dimensional Doppler echocardiogram and M-mode echocardiogram, one can study maternal and fetal cardiovascular physiology during rest and exercise. Using such noninvasive tech- niques, studies indicate that left ventricular function is mainta ined even during vigorous bicycle exercise in healthy pregnant subjects during the second half o f pregnancy. In early pregnancy, the left ventricle adapts to strenuous bicycle exercise by increasing its contractile reserve, enhancing ventricular emptying, whereas in late pregnancy, the left ventricle increases its pre load reserve without significantly increasing its contractile reserve. Thus, women are "cardiovascularly" disadvantaged early in pregnancy. Using Doppler signals, early (E-passive) flow and late peak (A-active) flow reflect left ventricular diastolic filling propert ies . Using such techniques, we found that diastolic filling pat terns are significantly influenced by pregnancy and that each tr imester influences these diastolic filling pat terns during upright bicycle exercise. Doppler studies o f uteroplacental circulation during or af ter exercise have yielded conflicting results. Some have descr ibed an increase in " the vascular resistance" of this pelvic bed during strenuous exercise, whereas others have not. I t seems safe to conclude that more studies are needed to elucidate this p roblem. Exercise does not seem to influence the resistivity index of the umbilical artery in either singleton or twins, and may even cause it to decrease. Ventricular diastolic filling proper t ies o f the fetal hear t do not seem to be influenced by maternal bicycle exercise. Further studies are needed to de termine if less active pregnant subjects, women with chronic hypertensive disorders, women with sickle cell anemia, or women with insulin- dependent diabetes adapt to exercise as well as their "no rma l" counterparts . Copyright �9 1996 by W.B. Saunders Company
W ith the recent deve lopment of noninvasive techniques, such as Doppler , two-dimen-
sional echocardiograms and M-mode echocardi- ograms, the study of cardiovascular adaptat ion to pregnancy has been possible. Doppler flow imaging, with ei ther two-dimensional echocardi- ography or pulsed Doppler are the current state- of-the-art ul t rasound equ ipmen t and have been used to study maternal and fetaI response to ex- ercise. I
M-Mode E e h o c a r d i o g r a p h y
Signal Acquisition
Two-dimensional echocardiography allows the visualization of the materna l or fetal heart. The
From the Department of Obstetrics and Gynecology, Bowman Gray School of Medicine, Winston-Salem, NC. Address reprint requests to Jean-Claude Veille, MD, Department of Obstetrics and Gynecology, Bowman Gray School of Medicine, Medi- cal Center Blvd, Winston-Salem, NC 27157-1066. Copyright �9 1996 by WB. Saunders Company O146-0005/96/2004-0009505. 00/0
parasternal long-axis is used to visualize the r ight and left ventricles, the mitral valve, the tricuspid valve, and the two outflow tracts. The first step in pe r fo rming an adequate M-mode echocardio- gram in ei ther the mothe r or the fetus is to proper ly identify these cardiac structures. The M-mode cursor is then d ropped parallel to the ventricular cavity- (Fig 1) to pe r fo rm a sweep of the ventricles f rom the apex to the base of the ventricles. 2
Using the parasternal long axis view, the M- mode cursor is placed at the level of the atrioven- tricular Valves to obtain ventricular wall and sep- tal motion.
In terpre ta t ion o f the M-Mode Signal
The ventricles contract during systole and relax during diastole. During systole, the poster ior ventricular wall of the left ventricle and the ante- rior wall of the right ventricle are moving closer to the interventricular septum, the ventricular cavities are getting smaller, and the leaflets of the atrioventricular closing. During diastole, the ventricular cavities are relaxing, getting larger,
250 Seminars in Perinatology, Vol 20, No 4 (August), 1996: pp 250-262

Maternal and Fetal Cardiovascular Response 251
RV ~ RA
LV AO
LA
Figure 1. M-mode echocardiography.
and the atrioventricular valve leaflets are open- ing. By recording the ventriCular dimensions during diastole (end-diastolic dimension [EDD]) and during systole (end-systolic d imension [ESD] ) at the level of the atrioventricular valves, ventricular fractional shortening can be calcu- lated and cardiac function estimated. Using EDD and ESD, end-diastolic and end-systolic volumes can be estimated. 2 The difference between these two volumes reflects the ejected volume or the stroke volume (Fig 2).
M-Mode Echocardiography During Bicycle Exercise in Normal Pregnancy
In a recent publ ished study, 16 healthy subjects underwent M-mode echocardiography at rest and dur ing progressive increase in workload bi- cycle exercise. Every 3 minutes, work load inten- sity was increased by 150 kg-m/min . Left ventric- ular funct ion was assessed 2 minutes into each of the stages. Results are described in Figs 3 a n d 4 .
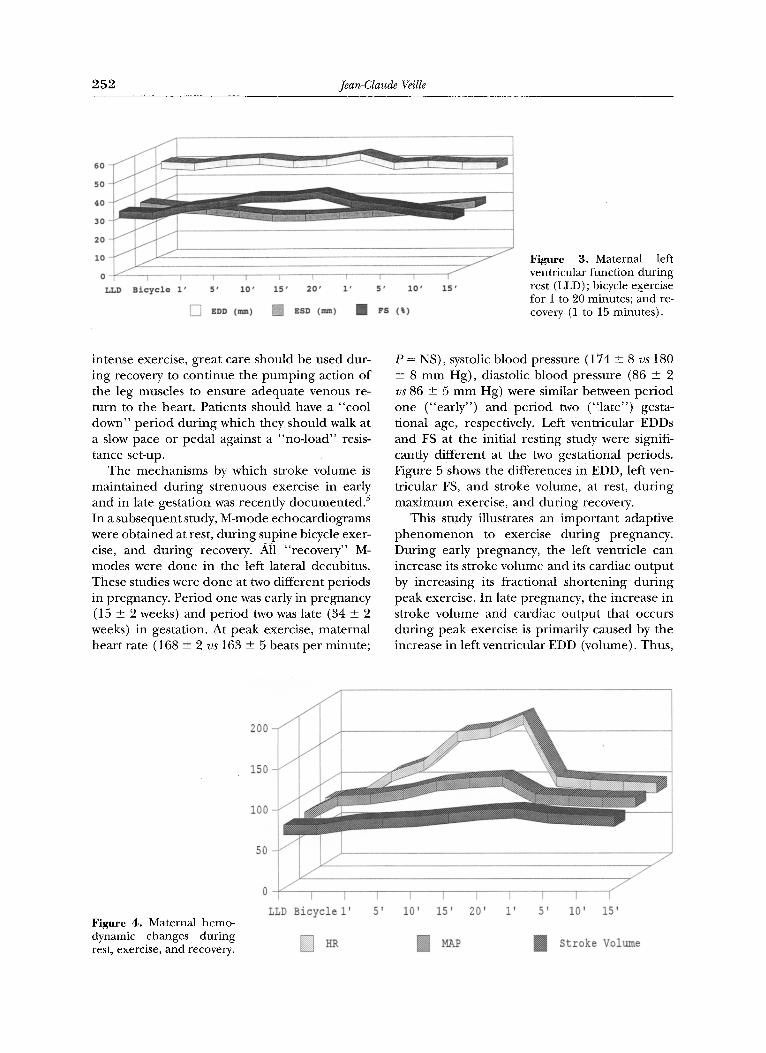
Figure 3 illustrates the maternal left ventricu-
lar function while resting in the left lateral de- cubitus (LLD), at rest on the bicycle (B), during 1, 5, 10 and 20 minutes of the exercise per iod and during the 1, 5, 10 and 15 minutes into recovery. 3 During m a x i m u m exercise (20 min- utes) left ventricular EDD increased, fractional shortening (FS) significantly increased, and left ventricular ESD significantly decreased. 3 Such M-mode studies indicate that left ventricular function is mainta ined dur ing vigorous bicycle exercise in healthy p regnan t subjects in the sec- ond half of the pregnancy.
Despite impor tan t hemodynamic changes that are found to occur dur ing pregnancy, stroke volume and ventricular contractility can still in- crease during exercise, indicating that the left ventricle was able to respond adequately to he- modynamic stresses. Thus, dur ing high levels of exercise, the increased ventricular contractility along with the decrease in end-systolic volume contr ibute to the observed increase in stroke vol- ume, Upr ight exercises are associated with sys- temic, venous pool ing and decreased ventricular filling pressures, and could potentially reduce end-diastolic volume, stroke volume, and cardiac output. 4 In this study, recovery was not associated with a decrease in stroke volume mainly because all of the "recovery" studies were pe r fo rmed in the left lateral decubitus. Thus, it is recom- mended, and would seem advisable, that after
T RV FreeWall
.T. Inter ventricular septum
I LV FreeWall
Figure 2. Using EDD and ESD, end-diastolic and end- systolic volumes can be estimated. The difference be- tween these two volumes reflects the ejected volume or the stroke volume. LV, left ventricular; RV, right ventricular.
2S2 Jean-Claude Veille
6 0
5 0 - / /
4 0 - /
30 J
2 0 - f
1 0 - " /
0 f
V .LD
I I k t I I T ~ � 8 4 I I
Bicycle 1' 5' 10' 15" 20' 1' 5' 10'
[ ] ED. ( ~ ) [ ] EnD ( ~ ) [ ] FS (~)
1 5 '
Figure 3. Maternal left ventricnlar function during rest (LLD) ; bicycle exercise for 1 to 20 minutes; and re- covery (1 to 15 minutes).
intense exercise, great care should be used dur- ing recovery to continue the pumping action of the leg muscles to ensure adequate venous re- turn to the heart. Patients should have a "cool down" per iod dur ing which they should walk at a slow pace or pedal against a "no- load" resis- tance set-up.
The mechanisms by which stroke volume is mainta ined dur ing strenuous exercise in early and in late gestation was recently documented . 5 In a subsequent study, M-mode echocardiograms were obta ined at rest, dur ing supine bicycle exer- cise, and dur ing recovery. AI1 "recovery" M- modes were done in the left lateral decubitus. These studies were done at two different periods in pregnancy. Period one was early in pregnancy (15 _+ 2 weeks) and per iod two was late (34 _+ 2 weeks) in gestation. At peak exercise, maternal heart rate (168 _+ 2 vs 163 _+ 5 beats per minute;
P = NS), systolic blood pressure (174 + 8 vs 180 _+ 8 m m Hg) , diastolic blood pressure (86 _+ 2 vs 86 _+ 5 m m Hg) were similar between per iod one ("ear ly") and per iod two (" la te") gesta- tional age, respectively. Left ventricular EDDs and FS at the initial resting study were signifi- cantly different at the two gestational periods. Figure 5 shows the differences in EDD, left ven- tricular FS, and stroke volume, at rest, dur ing m a x i m u m exercise, and during recovery.
This study illustrates an impor tan t adaptive p h e n o m e n o n to exercise dur ing pregnancy. During early pregnancy, the left ventricle can increase its stroke volume and its cardiac ou tpu t by increasing its fractional shortening dur ing peak exercise. In late pregnancy, the increase in stroke volume and cardiac output that occurs during peak exercise is primarily caused by the increase in left ventricular EDD (volume). Thus,
Figure 4. Maternal hemo- dynamic changes during rest, exercise, and recovery.
200
150
I00
50 J
f
0
LLD Bicycle I' 5' I0' 15' 20' i' 5' I0' 15'
[] HR N MAP ~ Stroke Volume

Maternal and Fetal Cardiovascular Response 253
I00 -
80
60
40
20
0 I I I Rest Max Rec
Figure 5. Hemodynamic . ~ SV 1 (ml) results during early and late I FS 2 (%) gestation.
SV2 (ml) J FS 1 (%)
dur ing in early pregnancy, the left ventricle adapts to strenuous bicycle exercise by increas- ing the contractile reserve, enhancing ventricu- lar emptying. In late pregnancy, the left ventricle is " l a rge r" and uses an increase in pre load re- serve without significantly increasing its contrac- tility reserve. 5
M-Mode Echocardiography During Hand- Grip Exercise in Abnormal Pregnancy
Pregnancy-induced hypertension is associated with significant left ventricular changes in re- sponse to the increase in afterload. To investi- gate the adverse cardiovascular effects of hyper-
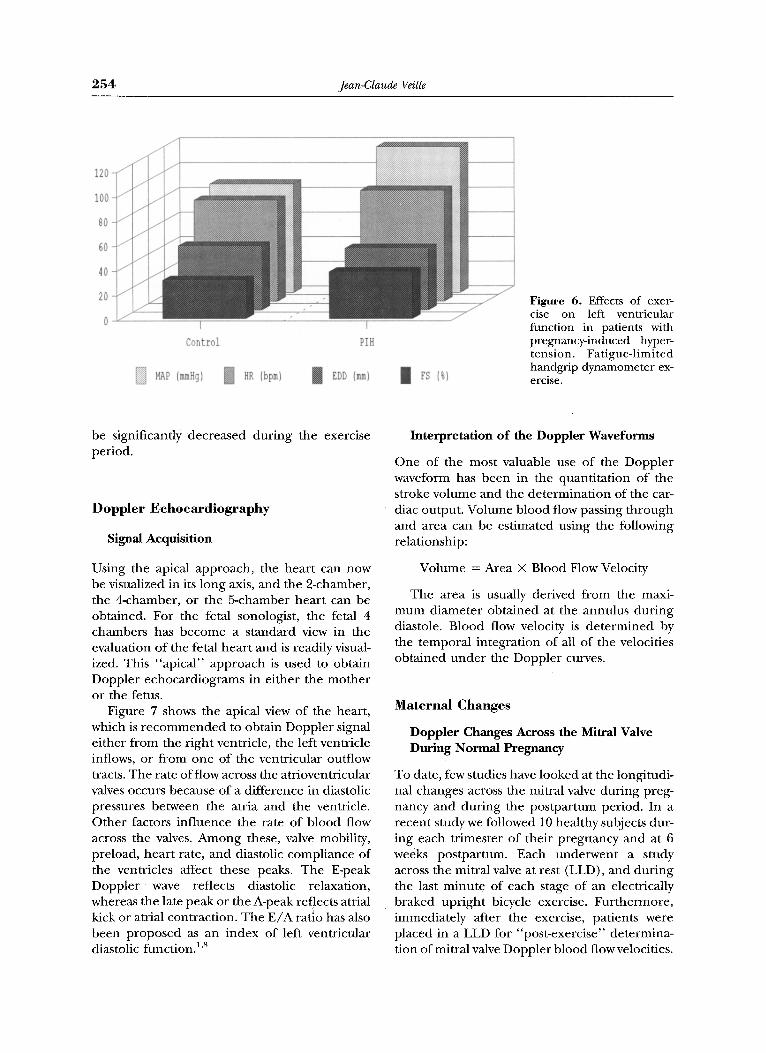
�9 tension on left ventricular function, a g roup of p regnan t patients with pregnancy-induced hy- per tension were studied in the left lateral decubi- ms, using M-mode echocardiograms. 6 Patients were asked to maximally squeeze a hand-grip dynamometer . The squeeze was then held at 50% of m a x i m u m until the patients exper ienced fatigue. Echocardiographic determinat ions of the left ventricular function was de te rmined dur- ing the last 30 seconds of the exercise. The main purpose of this study was to test the hypothesis was that sudden increase in afterload could jeop- ardize left ventricular function in these patients with pregnancy-induced hypertension. The re- sults are illustrated in Fig 6.
The results of this study indicated that despite a " ch ron ic " elevation in afterload, sudden in- crease in b lood pressure did not compromise
left ventricular function. The ability of the left ventricle to maintain adequate contractility and function shows an adaptive p h e n o m e n o n that is mostly, a result of a geometrical remodel ing of the left ventricutar cavity. In the same study, we found that the radius (r) of the ventricle to ven- tricular wall thickness (h), or the r / h ratio, significantly decreased in patients with preg- nancy-induced hypertension. This ventricular remodel ing in turn decreases wall stress and improves ventricular per formance . This relation- ship is best illustrated by the two formulas below.
Ventricular Per formance o~ 1/Wall Stress;
Wall Stress oz Intraventr icular Pressure
• Geometry ( r /2h)
Thus, if the ventricular radius to wall ratio ( r /h ) decreases in response to an increase in afterload, wall stress may ei ther be preserved or even decreased. Such ventricular geometry de- creases wall stress, which in turn improves ven- tricular per formance . Such was the case in the study done in a group of te rm patients with preg- nancy-induced hypertension.
In a more recent study, Van H o o k et al stud- ied 10 healthy p regnan t volunteers between 25 and 36 weeks of gestation using isometric leg exercise. 7 They found that total per ipheral resis- tance increased and hear t rate increased with this type of exercise. Using Doppler studies, they found no change in cardiac output dur ing or after such exercise. Stroke volume was found to
254 Jean-Claude Veille
/ 120 - /
/ 100 - /
80 /
60 / /
40 / /
20 / /
/ 1 I
Control PIH
MAP (mmHg) N HR (bpm) ! EDD (ram) I FS (%)
Figure 6. Effects of exer- cise on left ventricular function in patients with pregnancy-induced hyper- tension. Fatigue-limited handgrip dynamometer ex- ercise.
be significantly decreased during the exercise period.
Doppler Echocardiography
Signal Acquisition
Using the apical approach, the hear t can now be visualized in its long axis, and the 2-chamber, the 4-chamber, or the 5-chamber hear t can be obtained. For the fetal sonologist, the fetal 4 chambers has become a standard view in the evaluation of the fetal hear t and is readily visual- ized. This "apica l" approach is used to obtain Doppler echocardiograms in ei ther the mothe r or the fetus.
Figure 7 shows the apical view of the heart, which is r e c o m m e n d e d to obtain Doppler signal ei ther f rom the r ight ventricle, the left ventricle inflows, or f rom one of the ventricular outflow tracts. The rate of flow across the atrioventricular valves occurs because of a difference in diastolic pressures between the atria and the ventricle. Other factors influence the rate of b lood flow across the valves. Among these, valve mobility, preload, hear t rate, and diastolic compliance of the ventricles affect these peaks. The E-peak Doppler wave reflects diastolic relaxation, whereas the late peak or the A-peak reflects atrial
J kick or atrial contraction. The E / A ratio has also been proposed as an index of left ventricular diastolic func t ionJ '8
Interpretation of the Doppler Waveforms
One of the most valuable use of the Doppler waveform has been in the quanfitation of the stroke volume and the determinat ion of the car- diac output. Volume blood flow passing through and area can be estimated using the following relationship:
Volume = Area X Blood Flow Velocity
The area is usually derived f rom the maxi- m u m diameter obta ined at the annulus dur ing diastole. Blood flow velocity is de te rmined by the t empora l integration of all of the velocities obta ined unde r the Doppler curves.
Maternal Changes
Doppler Changes Across the Mitral Valve During Normal Pregnancy
To date, few studies have looked at the longitudi- nal changes across the mitral valve during preg- nancy and dur ing the pos tpar tum period. In a recent study we followed 10 healthy subjec~ dur- ing each tr imester of their pregnancy and at 6 weeks postpar tum. Each underwent a study across the mitral valve at rest (LLD), and dur ing the last minute of each stage of an electrically braked upr ight bicycle exercise. Fur thermore , immediately after the exercise, patients were placed in a LLD for "post-exercise" determina- tion of mitral valve Doppler blood flow velocities.

Maternal and Fetal Cardiovascular Response 255
.er Transducer
;evel if []let ;@le
Velocity
I Figure 7. The apical view Apical 4-Chambers of the heart.
A=Atrial
E=Early
d i I 1 1 t I I I I I I I ) } r . . . . . . . . . . . . . '
! l ! ! ! ! ! ! ! l l l l
Figure 8 illustrates some of those preliminary results.
These results suggest that significant differ- ences exist in the diastolic function between the "p regnan t " hear t and the "pos tpar tum" heart. Fur thermore, each trimester seems to influence diastolic function at each level of upright bicycle exercise. Thus, transmitral pressure gradient and consequently mitral flow velocity were af- fected by the pregnant state. By significantly af- fecting the early peak (E), one can assume that relaxation and compliance of the left ventricle is influenced by the pregnant state.
During the same study, using the Doppler sig- nal, which was obtained at the level of the valve leaflets so as to record maximum transvalvular
velocities, the A-peak across the mitral valve was also analyzed. Results are illustrated in Fig 9. Figure 9 shows that pregnancy significantly af- fected atrial contraction during strenuous bicy- cle exercise, especially during the first trimester, when the increase in stroke volume and cardiac output has not yet been established:
Maternal Changes in Cardiac Output in Response to Changes in Position
If changing position is viewed as a form of mild exercise, Sorensen et al recently repor ted on the changes in the maternal cardiac output using continuous Doppler techniques. 9 The patient population was comprised of normotensive and hypertensive subjects, with and without elevation
140
120
I00
80
60
40
20
0
Baseline 25 kpm 50 kpm 75 kpm i00 kpm 125 kpm
1 st Trim [] 2 nd Trim [] 3 rd Trim [] PP
- - - - 4
7 Figure 8. Mean values of the E-peak Doppler veloci- ties .at each stage of bicycle exercise. Peak early Dopp- ler velocity at the level of the mitral valve.

2 5 6 Jean-Claude Veille
140
120
I00
80
60
40
20
0 I I I I Baseline 25 kpm 50 kpm 75 kpm
1 st Trim ~ 2 nd Trim
I [ I00 kpm 125 kpm
3 rd Trim [] PP
Figure 9. Mean A-peak Doppler velocity across the mitral valve during preg- nancy and postpartum. In- creasing stages of upright bicycle exercise.
in the total peripheral resistance. A summary of the per t inent results is illustrated in Fig 10.
Although these investigators found no sig- nificant differences in changes with position among the groups, they found significant differ- ences in the maternal cardiac output when mea- surements were compared with the preceding position in hypertensive patients with elevated peripheral resistance.
In a group of normal pregnant subjects, we recently per formed an "orthostat ic" study look- ing at the effect of a head-down (30 ~ and head- up (upright) of the isovolumetric ventricular re- laxation (ventricular Doppler diastolic filling) of the left ventricle. The only significant difference was found during the "head-down position." This difference was mostly a result of the high values found during the postpartum period and the early pregnancy period. The results are illus- trated in Fig 11.
Although minor changes were found in the left ventricular isovolumetric relaxation with changes in maternal position, we concluded that acute changes in maternal position did not sig- nificantly affect this hemodynamic parameter.
D o p p l e r Changes in Maternal Peripheral Vasculature During Normal Pregnancy
Uteroplacental Circulation. Doppler studies of uteroplacental circulation during or after exer- cise have yielded conflicting results (Table 1). Some Doppler studies suggest increases in "resis- tance" with strenuous maternal exercise, whereas others have suggested that despite an increase in blood flow to the exercising lower limbs, uteroplacental blood flow does not seem to be significantly changed. Baumann et al looked at the pulsed Doppler response of the uteroplacental vessels in 13 women during the 36th to the 41st week of gestation after bicy-
Figure 10. Maternal car- diac output (L/rain). Effect of changes in position.
I0
8
6
4
2
0 i
T,LD
] HBP - High TPR
J r
Sitting Standing
[] HBP- N TPR [] Normotensive

Maternal and Fetal Cardiovascular Response 2 5 7
12D
100
80
so
40
20
0
1st Trim Figure ] ] . Isovolumetfic relaxation. Effect of posi- tion. [ ] LLD
I I I 2nd Trim 3rd Trim PP
[ ] Head-up [ ] Head-Down
cling, a~ Nei ther the resistance index no r the pul- sitility index of the uteroplacental vessels changed with maternal exercise.
In a more recent publication, 21 p regnan t volunteers were studied before and after aerobic dancing. The gestational age ranged between 34 and 40 weeks of gestation. Pulsed Doppler stud- ies of the maternal uterine arteries were sampled at regular intervals, u Nei ther the peak systolic velocity nor the pulsitility index of the uter ine artery changed significantly with this type of ex- ercise. These investigators concluded that aero- bic dancing did not significantly change the uter- ine b lood flow. n
In three studies using Doppler ul trasound, the systolic to diastolic ratio of the uterine artery was found to increase significantly with materna l exercise, ha3 Two other studies could not repro- duce such an increase in the systolic to diastolic ratio of the uterine artery. 1~
Morrow followed the systolic to diastolic ratio of the uterine artery before exercise, dur ing ex- ercise, and dur ing the recovery period, and found that bicycle exercise significantly in-
creased this ra t io) ~ Figure 12 shows the S /D ra- tio of the uterine artery before exercise, dur ing exercise and immediately after exercise. 12
All of these studies have failed to documen t the location of the placenta in relation to the site of the uterine artery sampling. It is possible that these discrepant results could be explained by the "fact that the placenta was of the side of the uterine artery or away f rom it. Such variation in placenta location could affect uterine artery resistivity indices. More studies are needed to elucidate this problem. Thus, the final answer on the effects of exercise on the uterine vascula- ture and on uter ine b lood flow is still controver- sial.
Changes in Other Maternal Vascular Beds: Femoral Artery and Carotid. Baumann et al looked at the pulsed Doppler response of the maternal ca- rotid, the femoral artery and vein in 13 women dur ing the 36th to the 41st week of gestation, after bicycling. 1~ Maximum systolic velocity in the carotid and femoral arteries increased after the exercise. Although the mean velocity of the carotid artery did not significantly change with
Table 1. Summary of Some of the Published Studies on the Effects of Exercise on the Uterine Artery
Authors GA Type of Exercise Area of Interest Results After Exercise
Morrow, 12 1989 36-41 Bicycle Uterine arteries Baumann, 1~ 36-40 Bicycle Uterine arteries
1989 Hackett, ~3 1992 30-37 Bicycle Uteroplacental
Errkkola, TM 1992 35-38 Bicycle Uterine arteries Asakura, u 1994 34-40 Aerobic dancing Uterine arteries
Significant increase in S/D ratio Pulsitility index did not
significantly change Pulsitility index did increase
with exercise Significant increase in S/D ratio Pulsifility index did not
significantly change

258 Jean-Claude Veille
2-i
1.8 - j
1.6 - j
1.4
i
l
Baseline Ex5 Ext0 Exl5 Rt R2 R3 R4
Uterine Art S/D
R5 Figure 12. S/D ratio of the main uterine artery before, during and after exercise. B, baseline; Ex, exercise; R, recovery.
exercise, the mean velocity in both the femoral artery and the femoral vein significantly in- creased with exercise. This observation led the investigators to conclude that femoral blood flow is increased during exercise and that peripheral vascular resistance is decreased with exercise.
In a more recent publication, 21 pregnant volunteers were studied before and after aerobic dancing. The gestational age ranged between 34 and 40 weeks of gestation.ll Pulsed Doppler stud- ies of the maternal femoral and carotid arteries were sampled at regular intervals. The peak sys- tolic velocity of the femoral artery increased by 130% over baseline, the volume blood flow to this vessel increased by 337%, and the pulsitility index decreased by 80%. 11 Neither the peak sys- tolic velocity nor the pulsitility index of the ca- rotid artery changed significantly with this type of exercise. Fetal heart rate increased from a baseline of 142 _+ 2.5 bpm to 161 + 4 bpm after exercise. These investigators concluded that aer- obic dancing increased blood flow to the extrem- ities without significantly changing cerebral blood flow.
Fetal Changes
Doppler Changes in Umbilical Artery After Bicycle Exercise in Normal Pregnancy
Although the fetal hear t responses to maternal exercise have been previously publishedJby many investigators, 15"26 only a few have looked at the Doppler response of ei ther the umbilical artery or the fetal ventricles immediately after strenu-
ous maternal exercise. Table 2 summarizes the published Doppler studies specifically looking at the fetal hemodynamic response to maternal ex- ercise.
Thus, the majority of studies either show no changes in the umbilical artery resistivity indices or no ted a decrease in the umbilical artery as to the ratio reflecting a decrease in the "vascular resistance" within that circulation during or after exercise.
In a study looking at the effects of changing maternal position, Sorensen et al looked at the umbilical artery systolic to diastolic ratio (S/D) in a group of normotensive subjects and in a group of hypertensive subjects with and without elevation of total peripheral resistance. 9 The summary of the results are shown in Fig 13.
There were no significant differences at rest between the three groups. With exercise, the hy- pertensive group with high total peripheral resis- tance had a significant increase in the systolic to diastolic ratio when standing. Such findings support t h e previously repor ted data f rom Raumaro and Forss. 3~
More recently, we have conducted longitudi- nal studies on normal pregnant patients with sin- gletons and twins. For the singleton pregnancies, we used pulsed Doppler ultrasound to evaluate not only the umbilical artery resistivity indices, but also looked at blood flow velocities across the atrioventricular valves of the fetal heart before bicycle exercise and immediately after exercise. Results on the umbilical pulsitility index are illus- trated in Fig 14.

Maternal and Fetal Cardiovascular Response 2 5 9
Table 2. Summary of Published Doppler Studies Examining Fetal Hemodynamic Response to Maternal Exercise
GA Authors Year (whs) Type of Exercise Area of Interest Results after Exercise
Pipers 27 1984 Bicycle Fetal descending No significant change aorta
1989 28 -+ 6 Bicycle Umbilical artery No significant change in S/D ratio 1989 36-41 Bicycle Umbilical arteries No significant change in S/D ratio 1989 36-40 Bicycle Umbilical artery Significant decrease in the umbilical
artery, PI 1990 14-37 Knee bends No significant change in the PI 1992 35-38 Bicycle No significant change in the S/D
ratio 1992 3rd Tri Changes in position No significant changes in S/D ratio 1994 34-40 Aerobic dancing Significant decrease in the umbilical
artery, PI
Veille 2s Morrow 12 Baumann 1~
Ruissen 29 Umbilical artery Errkkola 14 Umbilical artery
Sorensen u' Umbilical artery Asakura 11 Umbilical artery
Abbreviation: PI, pulsitility index.
The above results indicate that the pulsitility index of the umbilical artery was not significantly changed by maternal bicycle exercise at any of the time periods studied. There was a significant decrease in the value of the pulsitility index with advancing gestational age. 31
Fetal Cardiac Evaluation After Maternal Exerc i se
The diastolic ventricular filling was assessed in 15 healthy subjects three times during the preg- nancy. The Doppler sampler was placed at the level of the right and the left atrioventricular valves, respectively, before and immediately after exercise. The early (E) peak velocity and the
late (A) peak velocities were assessed for both v6ntricles. The E / A ratios were analyzed for each geStational period. The results are tabulated in Fig 15.
Although there was a significant increase in tile E /A ratio of both the right and the left blood flow velocities across both of these valves with advancing pregnancy, maternal bicycle exercise did not significantly affect blood flow velocities across these valves, and did not affect diastolic ventricular filling patterns of the fetal ventricles. Heart rate was not significantly changed after maternal exercise. These preliminary data sug- gest that fetal ventricular filling is not signifi- cantly affected by strenuous maternal bicycle ex- ercise, zz
Figure 13. Changes in um- bilical S/D ratio in re- sponse to changes in mater- nal position.
J
J
J
f L LLD
HBP -High TPR
L Sitting Standing
N HBP-NTPR I Normotensive
I
I
/

260 Jean-Claude Veille
i .4- 1
00: 0 . 6
0 . 4
0
r r i
1 st 2 nd 3 rd
,0st Ex m PreEx
Figure 14. Pulsitility index of the umbilical artery: Maternal bicycle exercise done at each trimester.
To date, most of the effects of maternal exer- cise have been studied on singleton pregnancies. Minimal data exist on the effect of exercise on twin or higher orders of pregnancies. In a recent study, twin pregnancies were exercised on an electrically braked stationary bicycle. The dia- stolic ventricular filling was determined twice during pregnancy using pulsed Doppler before and immediately after strenuous exercise. Pre- liminary results are illustrated in Fig 16.
These preliminary results indicate that mater- nal bicycle exercise does not significantly affect either of the fetal right or the left ventricular diastolic function in either of the twins.
C o n c l u s i o n
This brief review concentrated on studies pub- lished that have documented maternal and fetal response using noninvasive pulsed Doppler ul-
trasound. Although many other studies that have documented the fetal heart response to mater- nal exercise have not been reported here, they all serve to understand the physiological adapta- tion to important hemodynamic changes associ- ated with exercise, m-32 The overall conclusion is that maternal exercise seems to be well tolerated by the maternal cardiovascular system, and that maternal ventricular performance seems to be preserved even in "abnormal" pregnancies. The uterine circulation may be decreased dur ing strenuous exercise as assessed indirectly by the systolic to diastolic ratio of the uterine circula- tion, but more studies are needed to clarify some of the conflicting results published over the last decade. The fetus seems to tolerate maternal ex- ercise well, al though some reports have de- scribed a transitional decrease in fetal heart rate during and after strenuous maternal exercise. This transient decrease in fetal heart rate may occur because of an increased pooling in the maternal venous system when the pumping ac- tion of the leg muscles have stopped, as a result of decrease in maternal blood pressure, or de- crease in uterine blood flow. On the other hand, prolonged adverse fetal effects secondary to these transient exercise-induced fetal heart rate changes have not been documented in hu- mans. 33 Thus, additional studies using artifact- free, noninvasive techniques are needed to further examine maternal placental/fetal re- sponses to maternal exercise.. Further studies are needed in twin pregnancies: in pregnancies com- plicated by chronic hypertension or diabetes: or in patients with stable hemoglobinopathies such
0,6-
0.7-
0.6- o 0.5-
tv 0.4 -
.< 0.a- tu O.2 -
0.t 0
|
l I I 1st 2nd 3rd
E/A RV Post N E/A RV Pro E/A LV Post I E/A LV Pre
Figure 15. E/A ratio: Left and right fetal ventricle be- fore and after maternal bi- cycle: Diastolic ventricular filling.

Maternal and Fetal Cardiovascular Response 2 6 1
F igure 16. Diastolic ven- t r icular filling velocities be- fore a n d af ter exercise: Fe- tal r igh t a n d left ventricles.
o.8 0.7-' 0.6
0 , 4
0 . 3 -
0 , 2
0
Study 1 Study 2
[ ] ~VPr~E/~ ~ RVP~t~/A [ ] LVP~*~/~ [ ] LVPOSt~/A
as sickle cell anemia under careful supervision. Fur thermore , most of the present studies have been published in highly motivated women who have a keen interest in exercise physiology, who are interested in "keep ing in shape" dur ing pregnancy, and who are well conditioned. Re- searchers in this field should consider studying women who are less avid exercisers and who are more sedentary, because the current publ ished data regarding the maternal and fetal adaptive mechanisms may differ in this large subgroup of patients.
References
1. Silverman NH, Schmidt KG: The current role Doppler echocardi0graphy in the diagnosis of heart disease in children. Cardiol Clin 7:265-297, 1989
2. Ha te L, kalgelesen B: Doppler Ultrasound in Cardiol- ogy: Physical Principles and Clinical Applications, 2nd ed. Philadelphia, PA, Lea & Febiger, 1985
3. Veille JC, Hellerstein HK, Bacevice AE: Maternal left ventricular performance during bicycle exercise. Am J Cardiol 69:1506-1508, 1992
4. Higginbotham MB, Morris KG, Williams RS, et al: Regu- lation of stroke volume during submaximal and maximal upright exercise in normal man. Circ Res 58:281-291, 1986
5. VeilleJC, Hellerstein HK, Cherry B, Bacevice AE: Effects of advancing pregnancy on left ventricular function dur- ing bicycle exercise. Am J Cardiol 73:609-610, 1994
6. Veille JC, Hosenpud JD, Morton MJ: Cardiac size and function in pregnancy-induced hypertension. Am J Ob- stet Gynecol 150:443-449, 1984
7. Van HookJW, Gill P, Easterling TR, et al: Hemodynamic effects of isometric exercise during late normal preg- nancy. AmJ Obstet Gynecol 169:870-873, 1993
8. Spirito P, Maron BJ, Bonow RO: Noninvasive assessment of left ventricular diastolic function: Comparative analy- sis of Doppler echocardiographic and radionuclide angi- ographic techniques. J Am Coll Cardiol 7:518-526, 1986
9. Sorensen T, Hendricks SK, Easterling TR, et ah Effect of orthostatic stress during pregnancy. Obstet Gynecol 72:550-552, 1992
10. Baumann H, Huch A, Huch R: Doppler sonographic
evaluation of exercise-induced blood flow velocity and waveform changes in fetal, uteroplacental and large ma- ternal vessels in pregnant women. J Perinat Med 17:279- 287, 1989
11. Asakura H, Nakai A, Yamaguchi M, et al: Ultrasono- graphic Mood flow velocimetry in maternal and umbili- cal arteries during maternal exercise. Acta Obst Gynae- colJpn 46:308-314, 1994
12, Morrow RJ, Ritchie JWK, Bull SB: Fetal and maternal hemodynamics response to exercise in pregnancy as- Sessed by Doppler ultrasound. Am J Obstet Gynecol 160:138-140, 1989
13. Hackett GA, Cohen-Overbeek T, Campbell S: The effect of exercise on uteroplacental Doppler waveforms in nor- mal and complicated pregnancies. Obstet Gynecol 79:919-923, 1992
14. Erkkola RU, Pirhonen JP, Kivijarvi AK: Flow velocity waveforms in uterine and umbilical arteries during sub- maximal bicycle exercise in normal pregnancy. Obstet Gynecol 79:611-615, 1992
15. Artal R, Romen Y, Paul RH, Wiswell R: Fetal heart rate responses to maternal exercise. Am J Obstet Gynecol 155:729-733, 1986
16. Carpenter MW, Sady SP, Hoegsberg B, et al: Fetal heart rate response to maternal exertion. JAMA 259i3006- 3009, 1989
17. Collings CA, Curet LB, Mullin JP: Maternal and fetal response to a maternal aerobic exercise program. Am j Obstet G~ecol 145:702-707, 1983
18. Dale EK, Mullinax KM, Bryan: Exercise during preg- nancy: Effect on the fetus. Can J Appl Sport Sci 7:98- 103, 1982
19. Jovanovic L, Kessler A, Peterson CM: Human maternal and fetal response to graded exercise. J Appl Physiol 58:1719-1722, 1985
20. Veille JC, Hohimer AR, Burry K, Speroff L: The effect of exercise on uterine activity in the last eight weeks of pregnancy-. Am J Obstet Gynecol 151:727-730, 1985
21. McMurray RG, Mottola MF, Wolfe LA, et al: Recent ad- vances in understanding maternal and fetal responses to exercise. Med Sci Sports Exerc 25:2305-1321, 1993
22. Clapp JF, Little IO), Capeless EL: Fetal hear ratet re- sponse to sustained recreational exercise. Am J Obstet Gynecol 168:198-206, 1993
23. Webb KA, Wolfe LA, McGrath MJ: Effects of acute and chronic maternal exercise on fetal heart rate. J Appl Physiol 77:2207-2213, 1994
24. Katz VL, McMurray RG, Berry MJ, et al: Renal response

2 6 2 Jean-Claude Veille
to immersion and exercise in pregnancy. Am J Perinatal 7:118-121, 1990
25. Clapp JF: A clinical approach to exercise during preg- nancy. Clin Sports Med 13:443-458, 1994
26. Clapp JF: Exercise and fetal health. J Dev Physiol 15:9- 14, 1991
27. Pipers L, WladimiroffJW, McGhieJ: Effects of short-term maternal exercise on maternal and fetal cardiovascular dynamics. BrJ Obstet Gynaecol 91:1081-1086, 1984
28. Veille JC, Bacevice AE, Wilson B, et al: Umbilical artery waveform during bicycle exercise in normal pregnancy. Obstet Gynecol 73:957-996, 1989
29. Ruissen C, Jager W, v. Drongelen M, Hoogland H: The influence of maternal exercise on the pulsitility index of the umbilical artery blood velocity waveform. Eur J Obstet Gynecol Reprod Biol 37:1-6, 1990
30. Rauramo I, Forss M: Effect of exercise on maternal he- modynamics and placental blood flow in heahhy women. Acta Obstet Gynecol Stand 67:21-25, 1988
31. VeilleJC, Kitzman DR, Tatum K, et al: Effects of advancing pregnancy on the umbilical artery pulsitility index after strenuous non-weight bearing exercise: Abstract presented at the 16th Annual Meeting of the Society of Perinatal Obstetricians, Kamuela, Hawaii, February 4-10, 1996
32. VeilleJC, Kitzman DR, Tatum K, et al: Effect of advanc- ing gestation on E/A ratio of the fetal left and the right ventricle after maternal strenuous bicycle exercise. Ab- stract presented at the 16th Annual Meeting of the Soci- ety of Perinatal Obstetricians, Kamuela, Hawaii, Febru- ary 4-10, 1996
33. ACOG: Exercise during pregnancy and the postpartum period. Tech Bull 189, February 1994