maternal adaptations to pregnancy merlind m. montinola – morales, md
TRANSCRIPT
MATERNAL ADAPTATIONS TO PREGNANCY Merlind M. Montinola – Morales, MD

• Reproductive Tract Changes
• Skin and Breasts
• Metabolic changes
• Hematological changes
• Cardiovascular system
• Respiratory Tract
• Urinary System
• Gastrointestinal tract
• Endocrine System
• Musculoskeletal System
• Central Nervous System

REPRODUCTIVE TRACT CHANGES

UTERUS
• Can weigh as much as 1100 g by term (non-pregnant weight = 70g)
• Total volume of contents 5 L – 20 L
• Uterine hypertrophy stimulated by action of estrogen and progesterone in early pregnancy; in late pregnancy – pressure of the expanding products of conception
• Uterine enlargement more marked at the fundus

Uterine Size During Pregnancy
UTERUS
• Braxton – Hicks contractions - irregular painless uterine contractions;
5 – 25 mm hg in intensity
• Blood flow increases progressively 500 – 750 mL/ min
• Maternal placental blood flow progressively increases due to vasodilation.
• Decrease in vascular resistance due to progesterone, estrogen and relaxin
• Also vascular refractoriness to effects of angiotensin II and norepinephrine

CERVIX
• Chadwick’s sign
• Goodell’s sign
• Hegar’s sign
• Cervical ripening - remodeling which decreases collagen
and proteoglycan concentrations and increases water
content
• Cervical glands undergo marked proliferation
– cervical eversion

CERVIX
• Cervical mucus – beading; result of progesterone
• Amniotic fluid leakage – ferning
• Arias Stella Reaction – endocervical gland
hyperplasia and hypersecretory
appearance
OVARIES
• Corpus luteum of pregnancy – functions maximally during the first 6-7 weeks of pregnancy; secretes progesterone
• Decidual reaction on and beneath the surface of ovaries
• Ovarian vascular pedicle increases from 0.9 – 2.6 cm at term
• Theca lutein cysts – from markedly elevated serum BhCG
FALLOPIAN TUBES
• Undergoes little muscle hypertrophy
• Epithelium of tubal mucosa flattens
• Fallopian tube torsion in presence of paratubal or paraovarian cysts

VAGINA AND PERINEUM
• Increased vascularity and hyperemia
• Chadwick sign
• Increase mucosal thickness, loosening of the connective tissue, and smooth muscle hypertrophy
• Acidic pH 3.5 – 6 from increased production of lactic acid from glycogen by the action of Lactobacillus
• 10-20 fold increase in vulvovaginal candidiasis

SKIN AND BREASTS
• Breast enlargement
• Nipples are larger, more deeply pigmented and more erectile
• Areola become broader and deeply pigmented
• Striae gravidarum

SKIN AND BREASTS
• Linea nigra
• Chloasma or melasma gravidarum
• Diastasis recti
• Vascular spiders
• Palmar erythema

METABOLIC CHANGES

ADDITIONAL ENERGY DEMANDS
• Approximately 77,000 kcal• 1st trimester - 85 kcal/day• 2nd trimester - 285 kcal/day• 3rd trimester - 475 kcal/day
WEIGHT GAIN
• Average weight gain during pregnancy is approximately 12.5 kg or 27.5 lbs
• Most of the normal increase in weight during pregnancy is attributable to the uterus and its contents, the breasts, and increases in blood volume and extracellular fluid
• Smaller fraction results from metabolic alterations that increase accumulation of cellular water, fat and protein

METABOLIC CHANGES
• Water metabolism• Increased water retention mediated in part by fall in plasma osmolality 10
mOsm/kg• Minimum account of extra water accrued is 6.5 L (3.5 L – fetus, placenta and
amniotic fluid; 3 L – maternal blood volume, uterus and breast)• Edema of ankles and legs
• Protein metabolism• Fetus and placenta contain approx. 500 g of protein; remaining 500 g added
to uterus, breasts and blood• Amino acid concentration higher in fetal than in maternal compartment
regulated by the placenta

METABOLIC CHANGES
• Carbohydrate metabolism• Mild fasting hypoglycemia, postprandial hyperglycemia and hyperinsulinemia• Pregnancy induced state of peripheral insulin resistance • Mechanism of insulin resistance not completely understood (progesterone
and estrogen, placental lactogen)
• Fat metabolism• Increased concentration of lipids, lipoproteins, apolipoproteins in plasma • Caused by increased insulin resistance and estrogen stimulation• Concentration of lipid decreases after delivery and with lactation• Increased leptin levels (play a role in fat and energy expenditure regulation);
abnormally high levels associated with preeclampsia and GDM
METABOLIC CHANGES
• Electrolyte and Mineral metabolism• Serum K and Na are slightly decreased because of expanded plasma volume
(although with increased total accumulation); but levels remain very near the normal range of non-pregnant
• Decreased non-ionized calcium (due to lowered alb); but serum ionized Ca is unchanged
• Significant demand on maternal calcium homeostasis by developing fetus• Mg levels slightly decline• Increased requirement for iron• Iodine requirement increase due to:
• Increased production of maternal T4 in early gestation• Fetal thyroid hormone production during 2nd half of pregnancy• Increased iodide glomerular filtration rate

HEMATOLOGICAL CHANGES
• Increase in blood volume by 40-45% after 32 – 34 weeks
• Pregnancy induced hypervolemia:1. Meets metabolic demands of enlarged uterus2. Provides abundant nutrients and elements to support rapidly growing
placenta and fetus3. Safeguards the mother against adverse effects of parturition-associated
blood loss

HEMATOLOGICAL CHANGES
• Blood volume expansion results from increase in both plasma and erythrocytes
HEMATOLOGICAL CHANGES
• Hemoglobin concentration and hematocrit decreases slightly during pregnancy because of great plasma augmentation
• Average hemoglobin 12.5 g/dL;
• ≤ 11 g/dL – abnormal and usually due to iron deficiency
IRON METABOLISM
• Iron used in latter half of pregnancy. Iron requirement larger after midpregnancy at approx. 6 – 7 mg/day
• Iron supplementation needed since iron stores not enough for required amount

IMMUNOLOGICAL FUNCTIONS
• Pregnancy is both proinflammatory and anti-inflammatory
• 3 distinct immunological phases:• Early pregnancy – proinflammatory; implantation and placentation involves
invasion of the endometrial tissue• Midpregnancy – anti-inflammatory – period of rapid fetal growth and
development • Parturition – inflammatory; influx of immune cells into the myometrium
• Anti-inflammatory component – suppression of TH1 and Tc1 cells which decreases secretion of IL-2, IFN and TNF
• Upregulation of TH2 cells to increase secretion of IL-4, IL-6, and IL-13
• Peak levels of IgA and IgG in cervical mucus
IMMUNOLOGICAL FUNCTIONS
• Leukocytes• Depressed leukocyte function• Leukocyte count higher than non-pregnant (average 14,000 – 16,000/uL)• Cause for marked increase is unknown
• Inflammatory markers such as ALP cannot be used reliably during pregnancy because of slight elevation during pregnancy

COAGULATION AND FIBRINOLYSIS
• Both coagulation and fibrinolysis are augmented but remain balanced to maintain hemostasis
• Increased concentration of all clotting factors except factors XI and XIII
• Levels of anticoagulants activated protein C and S decline
• Platelets – average platelet count is decreased slightly during pregnancy to 213,000/uL• Decreased platelet conc due to hemodilution• Increased platelet consumption• Production of thromboxane A2, progressively increase
• Hypersplenism – spleen enlarges by up to 50%

CARDIOVASCULAR SYSTEM

CARDIOVASCULAR SYSTEM
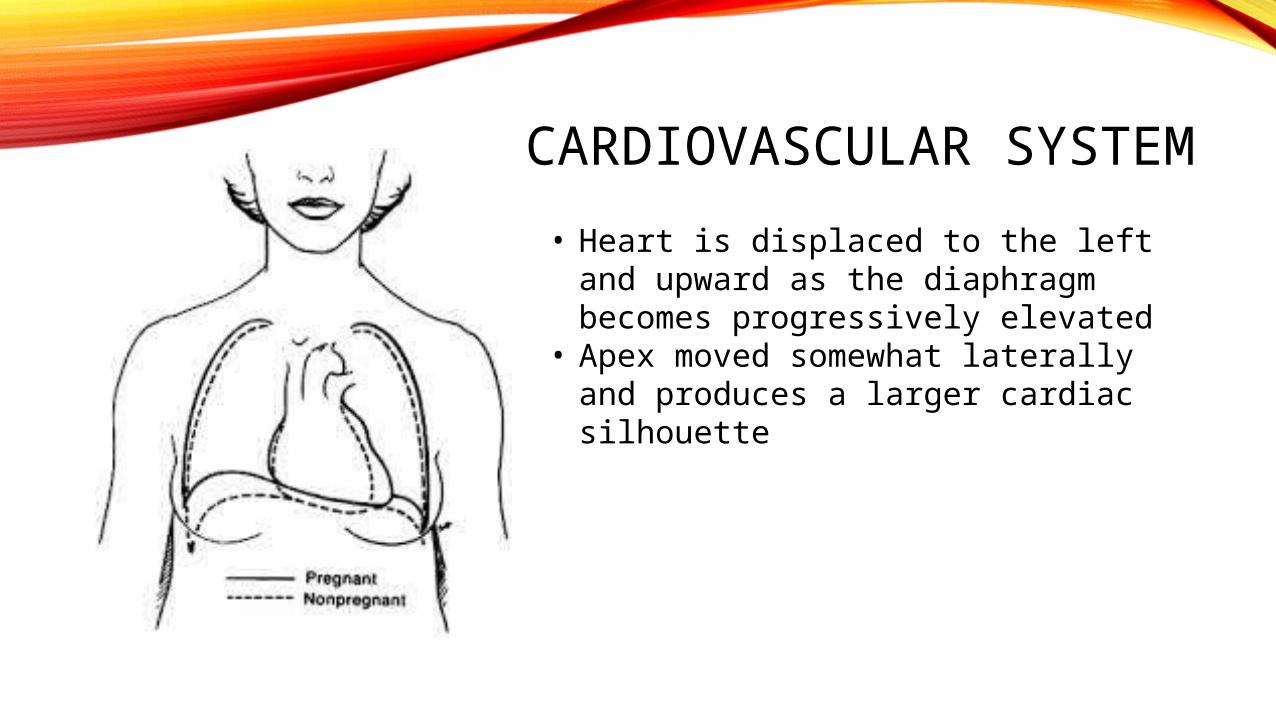
• Heart is displaced to the left and upward as the diaphragm becomes progressively elevated
• Apex moved somewhat laterally and produces a larger cardiac silhouette
CARDIOVASCULAR SYSTEM
• Cardiac sounds are modified:• Exagerrated splitting of the first heart sound• No definite changes in the aortic and pulmonary elements of the second
sound• Loud, easily heard third sound• Soft systolic mumur
• Enlarging end-systolic and end-diastolic dimensions; no change in septal thickness or in ejection fraction
• Not proven if there is hypertrophy of cardiac myocytes as a result of pregnancy

CIRCULATION AND BLOOD PRESSURE
• Changes in posture affect arterial BP (brachial artery pressure when sitting is lower than in lateral recumbent supine)
• Arterial pressure decreases to a nadir at 24 – 26 weeks then rises thereafter
• Supine hypotension – occurs in 10% of women – supine compression of the uterus causes significant arterial hypotension
• Refractoriness to angiotensin II may be related to progesterone
• ANP and BNP – secreted by cardiac myocytes regulate blood volume by provoking natriuresis, diuresis and vascular smooth muscle relaxation; maintained in non-pregnant range
• Prostaglandin – increased; control of vascular tone, BP and sodium balance
• Endothelin – vasoconstrictor produced in endothelial and vascular smooth muscle cells; identified in amnion, amniotic fluid, decidua and placenta; vascular sensitivity to endothelin 1 not altered in normal pregnancy
• Nitric oxide – potent vasodilator released by endothelial cells; one of the most important mediators of placental vascular tone and development; abnormal synthesis linked to preeclampsia development

RESPIRATORY TRACT
• Diaphragm rises about 4 cm during pregnancy
• Subcostal angle widens as transverse diameter of the thoracic cage lengthens
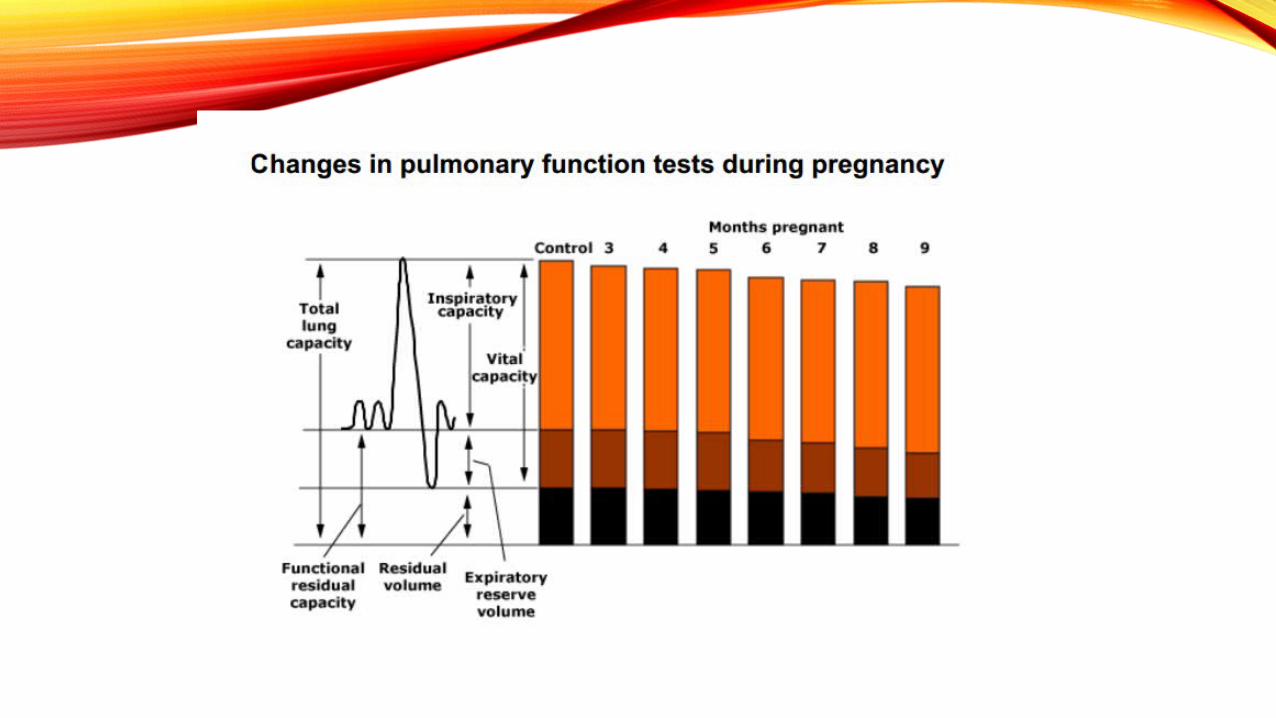


PULMONARY FUNCTIONS
• Lung compliance – unaffected
• Airway conductance – increased
• Total pulmonary resistance – reduced
• Maximum breathing capacity and forced or timed vital capacity are not altered appreciable

URINARY SYSTEM


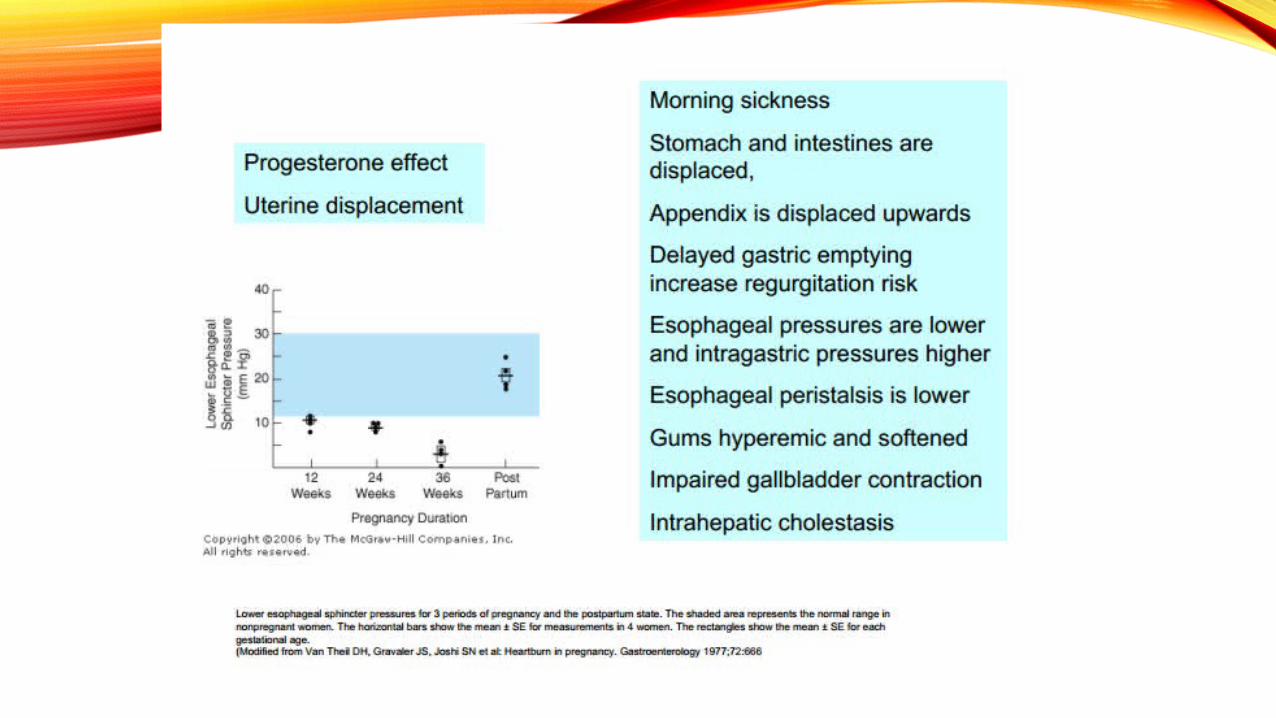
GASTROINTESTINAL TRACT

ENDOCRINE SYSTME
• Pituitary gland enlarges by 135% - caused by estrogen-stimulated hypertrophy and hyperplasia of lactotrophs
• Increased maternal serum prolactin levels
• Gonadotrophs decline in number
• Corticotrophs and thyrotrophs are constant
• Somatotrophs are depressed due to negative feedback by placental production of growth hormone
• Maternal pituitary gland is not essential for pregnancy maintenance; supplemental hormones may be given in patient who had hypophysectomy
ENDOCRINE SYSTME
• Thyroid gland moderate enlargement due to glandular hyperplasia and increased vascularity
• Early in first trimester, increase in TBG – increase total T4 and T3 concentrations but do not affect serum T4 and T3 levels
• HCG with intrinsic thyrotropic activity

• Liver function tests• Alkaline phosphatase – doubles• AST, ALT, GGT and bilirubin – slightly lower compared with non-pregnant
values• Serum albumin – decreases but total body albumin are increased

MUSCULOSKELETAL SYSTEM
• Progressive lordosis
• Sacroiliac sacrococcygeal, and pubic joints have increased mobility (not correlated with hormones)
CENTRAL NERVOUS SYSTEM
• Problems with attention, concentration and memory throughout pregnancy and early puerperium
• Decline not attributable to depression, anxiety, sleep deprivation or other physical changes
• Transient and quickly resolve following delivery
• Mean blood flow in middle and posterior cerebral arteries decreased progressively; mechanism unknown
EYES
• Intraocular pressure decreases partly due to increased vitreous outflow
• Decreased corneal sensitivity
• Krukenberg spindles – brownish red opacities on posterior surface of cornea – increased
• Visual function unaffected

• Sleep• Difficulty going to sleep 12 weeks to first 2 monhs postpartum• Greatest disruption of sleep encountered postpartum and may contribute to
postpartum blues or depression

THANK YOU