material selection for direct posterior restoratives · pdf filematerial selection for direct...
TRANSCRIPT

Publication date: Sept. 2011Expiration date: Aug. 2014
AbstractThe posterior restorative material of choice depends on the individual clinical situation and patient. Amalgam has a long history of use and clinical success. Esthetic restorations are increas-ingly in demand, and include glass ionomers, compomers and composite resins. Fluoride release is a desirable attribute in a restorative material, as are wear resistance, low polymerization shrinkage and low polymerization stress. Recently, technolo-gies have been incorporated into composite resins that lower polymerization shrinkage and stress.
Learning Objectives:The overall goal of this article is to provide dental professionals with information on the options available for posterior esthetic restorations. Upon completion of this course, the participant will be able to do the following:1. List and describe the considerations involved
in the selection of posterior restorative materials
2. List and describe the history and safety profile of amalgam, its advantages and disadvantages
3. List and describe how polymerization stress occurs and its relevance to restoration failure
4. List and describe the technologies that can now be incorporated into posterior composite restoratives to combat polymerization shrinkage and/or polymerization stress
Author ProfilesJohn O. Burgess, DDS, MS— Dr. Burgess is the Assistant Dean for Clinical Research and the Director of The Biomaterials Graduate Program at the University of Alabama in Birmingham. He graduated from Emory University School of Dentistry and completed graduate training at the University of Texas Health Science Center in Houston. Dr. Burgess is a diplomat of the Federal Services Board in General Den-tistry and the American Board of General Dentistry. He is a member of the Academy of Operative Dentistry, The American and International Associations for Dental Research, the Alabama Dental Association and the ADA. Dr. Burgess is the author of over 300 journal articles, textbook chapters and abstracts and has presented more than 800 continuing education programs nationally and internationally.
Deniz Cakir, DDS, MS— Dr. Deniz Cakir is an instructor the University of Alabama at Birmingham, School of Dentistry teaching graduates and dental students. She graduated from Ankara University School of Dentistry in 2002, and completed graduate training at the University of Alabama in Birmingham, School of Dentistry in 2005. Dr. Cakir is a member of the American Dental Association and the International Association for Dental Research.
Author DisclosureThe author(s) of this course has/have no commercial ties with the sponsors or the providers of the unrestricted educational grant for this course.
This course has been made possible through an unrestricted educational grant.
Supplement to PennWell Publications This course was written for dentists, dental hygienists and assistants, from novice to skilled. Educational Methods: This course is a self-instructional journal and web activity. Provider Disclosure: Pennwell does not have a leadership position or a commercial interest in any products or services discussed or shared in this educational activity nor with the commercial supporter. No manufacturer or third party has had any input into the development of course content.Requirements for Successful Completion: To obtain 2 CE credits for this educational activity you must pay the required fee, review the material, complete the course evaluation and obtain a score of at least 70%.
CE Planner Disclosure: Michelle Fox, CE Coordinator does not have a leadership or commercial interest with DENTSPLY Caulk, the commercial supporter, or with products or services discussed in this educational activity.
Educational Disclaimer: Completing a single continuing education course does not provide enough information to result in the participant being an expert in the field related to the course topic. It is a combination of many educational courses and clinical experience that allows the participant to develop skills and expertise.
Registration: The cost of this CE course is $49.00 for 2 CE credits. Cancellation/Refund Policy: Any participant who is not 100% satisfied with this course can request a full refund by contacting PennWell in writing.
Go Green, Go Online to take your coursePennWell designates this activity for 2 Continuing Educational Credits
Material Selection for Direct Posterior RestorativesA Peer-Reviewed Publication Written by John O. Burgess, DDS, MS and Deniz Cakir, DDS, MS
Earn
2 CE creditsThis course was
written for dentists, dental hygienists,
and assistants.

www.ineedce.com 2
Educational ObjectivesThe overall goal of this article is to provide dental profession-als with information on the options available for posterior esthetic restorations. Upon completion of this course, the participant will be able to do the following:1. List and describe the considerations involved in the
selection of posterior restorative materials2. List and describe the history and safety profile of
amalgam, its advantages and disadvantages3. List and describe how polymerization stress occurs and
its relevance to restoration failure4. List and describe the technologies that can now be incor-
porated into posterior composite restoratives to combat polymerization shrinkage and/or polymerization stress
AbstractThe posterior restorative material of choice depends on the individual clinical situation and patient. Amalgam has a long history of use and clinical success. Esthetic restorations are increasingly in demand, and include glass ionomers, com-pomers and composite resins. Fluoride release is a desirable attribute in a restorative material, as are wear resistance, low polymerization shrinkage and low polymerization stress. Recently, technologies have been incorporated into compos-ite resins that lower polymerization shrinkage and stress.
IntroductionMaterial selection for restoring posterior teeth depends upon the patient’s age, caries risk, esthetic requirements, ability to isolate the tooth and functional demands placed on the restoration. Although amalgam has been an effective restorative material for Class I and II cavity preparations, patient expectations are varied and range from high func-tional requirements to high esthetic demands. Each mate-rial used to restore posterior teeth has specific advantages and disadvantages and these should be carefully weighed before selecting a restorative material. Compomers, glass ionomers and composite resins bond to tooth structure and may reinforce weakened tooth structure. They have proven longevity in minimally invasive preparations, are excellent thermal insulators, esthetic, and produce varying levels of fluoride release, which may inhibit recurrent caries. How-ever, esthetic restorative materials have disadvantages. Composite resin, while the most durable of the esthetic direct restorative materials, has clinical limitations that restrict its use as a posterior restorative material, especially in areas where isolation is poor and wear is high. Resin res-torations require greater attention to detail during adhesive placement, increased placement time and are technically more difficult than a similar-sized amalgam restoration. Postoperatively, sensitivity to cold is a frequent complaint with Class II restorations, due primarily to polymerization shrinkage or poor adhesive placement – both of which cre-ate leakage at the resin/tooth interface.
Posterior Amalgam RestorationsAmalgam has a long-term clinical history of success for sever-al reasons: the margins corrode and seal, it has good moisture tolerance and excellent wear resistance. Although amalgam does not bond to tooth structure and has other limitations, such as galvanism, high thermal conductivity, and poor es-thetics, it may be placed in areas when some contamination, especially blood and saliva, are likely and still provide good clinical results. Amalgam can be used to successfully restore decimated teeth (Figures 1, 2).
Figure 1. Placement of amalgam restorations
Figure 2. Polished amalgam restorations
Amalgam restorations may be bonded to tooth structure with adhesives using the bonded amalgam technique. One of the most clinically successful systems is the 4-META-based Amalgambond Plus (Parkell). In amal-gam bonding, the bonding agent bonds to dentin by cre-ating a hybrid layer. The attachment of the bonding resin to amalgam, however, is largely mechanical rather than chemical. Unset amalgam is condensed into the bonding resin before it polymerizes, incorporating fingers of resin into the amalgam at the interface.1 Several clinical studies of bonded amalgam restorations have demonstrated their success.2,3,4 Belcher and Stewart compared the clinical success of amalgams that were pin-retained, retained with Amalgambond Plus with no filler powder or re-tained with Amalgambond Plus with filler. At two years, all restorations were intact with minimal sensitivity, good marginal adaptation and no recurrent caries. Summitt et al. recorded a six-year recall of Amalgambond-retained cuspal coverage Tytin restorations with no failures in the bonded amalgam group.
3 www.ineedce.com
Amalgam has been strongly criticized, especially when used as a restorative material in children, since it contains mercury. Two recent well-conducted randomized controlled clinical studies sponsored by the NIH have provided addi-tional evidence for the safety of amalgam in children. More than 500 children were studied in two clinical trials. In the first clinical trial the children were followed for seven years,5 and in the second for five years.6 In each study, children with carious lesions were randomized to one of two groups to receive either amalgam or composite resin restorations. After conducting numerous tests (IQ, blood, urine, social interaction tests, etc.), no significant differences in the health of the children were reported. Nonetheless, amalgam use has declined as greater numbers of clinicians and patients have se-lected esthetic, adhesive, mercury-free restorative materials.
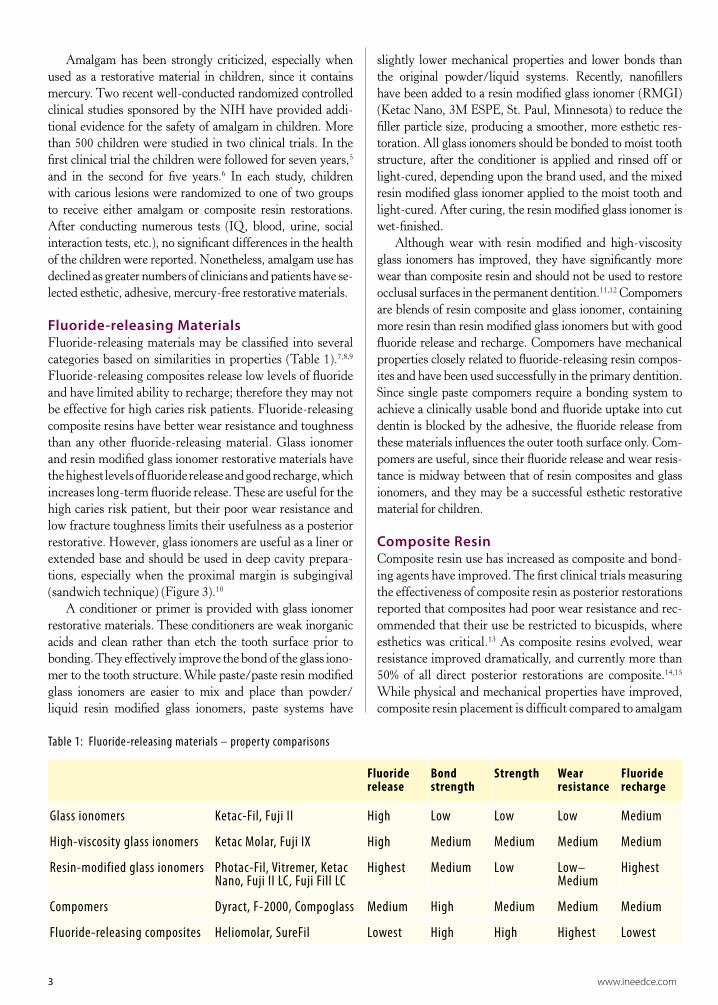
Fluoride-releasing Materials Fluoride-releasing materials may be classified into several categories based on similarities in properties (Table 1).7,8,9 Fluoride-releasing composites release low levels of fluoride and have limited ability to recharge; therefore they may not be effective for high caries risk patients. Fluoride-releasing composite resins have better wear resistance and toughness than any other fluoride-releasing material. Glass ionomer and resin modified glass ionomer restorative materials have the highest levels of fluoride release and good recharge, which increases long-term fluoride release. These are useful for the high caries risk patient, but their poor wear resistance and low fracture toughness limits their usefulness as a posterior restorative. However, glass ionomers are useful as a liner or extended base and should be used in deep cavity prepara-tions, especially when the proximal margin is subgingival (sandwich technique) (Figure 3).10
A conditioner or primer is provided with glass ionomer restorative materials. These conditioners are weak inorganic acids and clean rather than etch the tooth surface prior to bonding. They effectively improve the bond of the glass iono-mer to the tooth structure. While paste/paste resin modified glass ionomers are easier to mix and place than powder/liquid resin modified glass ionomers, paste systems have
slightly lower mechanical properties and lower bonds than the original powder/liquid systems. Recently, nanofillers have been added to a resin modified glass ionomer (RMGI) (Ketac Nano, 3M ESPE, St. Paul, Minnesota) to reduce the filler particle size, producing a smoother, more esthetic res-toration. All glass ionomers should be bonded to moist tooth structure, after the conditioner is applied and rinsed off or light-cured, depending upon the brand used, and the mixed resin modified glass ionomer applied to the moist tooth and light-cured. After curing, the resin modified glass ionomer is wet-finished.
Although wear with resin modified and high-viscosity glass ionomers has improved, they have significantly more wear than composite resin and should not be used to restore occlusal surfaces in the permanent dentition.11,12 Compomers are blends of resin composite and glass ionomer, containing more resin than resin modified glass ionomers but with good fluoride release and recharge. Compomers have mechanical properties closely related to fluoride-releasing resin compos-ites and have been used successfully in the primary dentition. Since single paste compomers require a bonding system to achieve a clinically usable bond and fluoride uptake into cut dentin is blocked by the adhesive, the fluoride release from these materials influences the outer tooth surface only. Com-pomers are useful, since their fluoride release and wear resis-tance is midway between that of resin composites and glass ionomers, and they may be a successful esthetic restorative material for children.
Composite ResinComposite resin use has increased as composite and bond-ing agents have improved. The first clinical trials measuring the effectiveness of composite resin as posterior restorations reported that composites had poor wear resistance and rec-ommended that their use be restricted to bicuspids, where esthetics was critical.13 As composite resins evolved, wear resistance improved dramatically, and currently more than 50% of all direct posterior restorations are composite.14,15 While physical and mechanical properties have improved, composite resin placement is difficult compared to amalgam
Table 1: Fluoride-releasing materials – property comparisons
Fluoride release
Bond strength
Strength Wear resistance
Fluoride recharge
Glass ionomers Ketac-Fil, Fuji II High Low Low Low Medium
High-viscosity glass ionomers Ketac Molar, Fuji IX High Medium Medium Medium Medium
Resin-modified glass ionomers Photac-Fil, Vitremer, Ketac Nano, Fuji II LC, Fuji Fill LC
Highest Medium Low Low–Medium
Highest
Compomers Dyract, F-2000, Compoglass Medium High Medium Medium Medium
Fluoride-releasing composites Heliomolar, SureFil Lowest High High Highest Lowest

www.ineedce.com 4
placement.16 Ideal proximal contacts are difficult to obtain with composite resins because composite condensation does not deform the matrix band against the adjacent tooth.17,18 To remove some of the difficulties associated with develop-ing a contact area, sectional matrices have been developed.
Composite resin shrinkage during polymerization
contributes to marginal breakdown and postoperative thermal sensitivity.19,20,21 Visible light-cured composite resin is placed in 2 mm increments into a cavity preparation, contoured to the desired shape and light-cured. This time-consuming incremental placement procedure is necessary, as light attenuates as it passes through composite resin. Photoinitiators in the composite resin, typically camphoro-quinone, are activated by visible light in the presence of an amine accelerator/catalyst.22 The photoactivated diketone/amine complex initiates polymerization of the dimeth-acrylate resin monomers. Composite resins may contain a combination of photoinitiators, each requiring its own specific wavelength for maximum reactivity. While many composite resins contain camphoroquinone, it imparts a yellow color to composites and alternate photoinitiators are used to reduce yellowing. These alternate photoinitiators absorb light in the 390–410 nm range, which is lower than the wavelength emitted by most LED curing lights. Curing composite resin containing these alternative photoinitia-tors requires the use of curing lights with a wider spectral distribution (such as quartz-tungsten-halogen or plasma arc curing lights that will polymerize all photoinitiators). Poorly cured composite resin has poor mechanical properties and low wear resistance; therefore, most composite resins should be cured in 2 mm increments with a curing light that emits the proper wavelength of light.
Soft-start curing lights and other curing modes have been advocated as a means for decreasing polymerization stress in composite resin restorations. In the last 15 years, various light-curing units have been developed to decrease contraction stress by slowing the rate of composite resin polymerization. These units cure at an initial low intensity and/or a short pulse cure.23,24 It is thought that this slower set permits movement of the polymer chains, thereby al-lowing stress relief and enabling improved marginal integ-rity.25 The objective with curing lights with variable output (soft-start polymerization curing units) is to reduce or delay polymerization stress without reducing the conversion rates of the polymer. These methods of “soft curing” include step-curing, ramp-curing and pulse-delayed curing. In vitro studies have shown mixed results. In our laboratory, we could find no significant difference in leakage when using these techniques.26,27 The pulse delay or the pulse cure tech-nique places increments of composite resin and cures each increment using 20- to 30-second cure times.28 The final enamel replacement increment is cured with a brief burst of energy for two to three seconds. After a three-to-five-minute delay to allow the composite time to flow and shrink,
Figure 3. Sandwich technique
Enamel
SureFil SDR flow adaptable up to 4 mm in one increment
Wear resistantcomposite
Enamel
Wear resistantcomposite
Dentin-enameljunction
Dentin-enameljunction
Compositeresin
Resin modified glass ionomer
Sandwich technique
SureFil SDR flow adaptableup to 4 mm in one increment
SureFil SDR is applied in a larger increment compared with the traditional GI technique, leaving a single 2 mm increment for the final composite layer
Enamel
Dentin-enamel junction
Dentin
Enamel Compositeresin
Sandwich technique
Resin modifiedglass ionomer

5 www.ineedce.com
the restoration is finished and polished. After finishing, the restoration is cured at high intensity to complete polymer-ization of the composite. While this technique has in vitro support, its clinical support is weak, with several studies reporting no significant difference in marginal integrity or marginal discoloration when composite resins are polymer-ized with or without a soft-start polymerization or with a chemical-cured composite resin.29,30,31,32,33,34 The literature shows that attempts to reduce polymerization stress with a curing light remain unproven.
Flowable Composites Flowable composite resins are often used today to reduce po-lymerization stress. Flowable composites are conventional or microfilled composite resins with a reduced filler load, which lowers their viscosity, resulting in better adaptation to the cavity walls.35 Low filler content has caused some concern, since highly filled composites have greater wear resistance for contact-supporting posterior restorations and less polym-erization shrinkage than flowable composites.36 However, flowable composite resins are now available with filler loads ranging from 34% to 68%, which provides a wide range of properties. In small noncontact restorations where longev-ity may be dictated by abrasion, flowable microfilled resins may be adequate. One clinical study related the wear of three flowable composite resins and evaluated the performance of flowables in three different-sized occlusal preparations.37 In small occlusal cavity preparations (defined as those with an isthmus width that did not exceed one-fourth of the inter-cuspal distance), one-year clinical performance was good. In larger preparations, wear was high and it was determined that flowable composites were contraindicated for load-bearing posterior restorations in permanent teeth with wide isthmus widths.
Flowable composite resin was originally used as a resin liner to improve the adaptation of condensable composites to the prepared tooth, especially in a cavity preparation with sharp line angles and uneven pulpal floors. Later it was specu-lated that even though flowables had higher polymerization shrinkage than highly filled composite resins, flowable com-posite resins with their lower elastic modulus would deform and create less stress at the tooth composite interface. Flow-able composites would then act as a stress-absorbing layer between the hybrid layer created by the bonding agent and the highly filled resin composite. Cadenaro et al. reported significant differences in the contraction stress development of different flowable composite resins.38 In this study, Filtek Supreme XT Flowable had the highest stress values and the lowest values were recorded with Tetric Flow (which was the only flowable composite with lower stress values than the conventional composite Filtek Z250). The authors concluded that most flowable composites had shrinkage stress compa-rable to conventional resin restorative materials, supporting the hypothesis that “flowable materials do not automatically
lead to stress reduction” and that the risk of debonding at the adhesive interface due to polymerization contraction is similar for some flowables and highly filled composite resins. In another study supporting this premise, Stavridakis et al. measured the linear polymerization displacement and po-lymerization forces induced by polymerization shrinkage of 22 flowable resin-based restorative materials.39 Polymeriza-tion forces (3.23 to 7.48 kilograms) were recorded showing that flowable resins produced considerable shrinkage stress. Flowable composites vary substantially in contraction force generated as well as wear and other properties. The in vitro and in vivo data demonstrate that using flowable composites to reduce polymerization shrinkage stress is controversial and may be dependent upon the specific flowable material used. This debate is further complicated by the clinical studies demonstrating no difference in marginal integrity between flowable lined composite resin restorations and composite restorations where no flowable was used.40 The consensus seems to be that the major benefit in using a flowable com-posite is cavity adaptation.
Composite Resin Shrinkage and StressAnother method to reduce polymerization shrinkage of com-posite resin uses new chemistry. Polymerization shrinkage of composite resins ranges from 3.7% to 0.9%.41,42 While in-creasing filler content of composite reduces shrinkage, it also increases composite stiffness, which also increases the forces of contraction.43 Recently, new resin monomers have been developed with different chemistries to reduce polymeriza-tion shrinkage stress. The first low-shrinkage commercially available composite resin was Filtek LS (3M ESPE, St. Paul, Minnesota), based on a silorane ring-opening chemistry. In our laboratory, shrinkage measurements for this composite ranged from 0.7% to 0.9% vol. Another newly developed composite, N’Durance (Septodont, New Castle, Delaware), uses dimer chemistry and has shrinkage measurements of 1.2% vol. Thiolene polymers also offer potential for reducing polymerization stress. Carioscia and Lu reported that thiol-ene/thiol-epoxy hybrid networks produced significantly reduced shrinkage stress of 0.2 MPa, which is 90% lower than the stress developed in a control dimethacrylate resin.44,45 This chemistry is not available commercially.
While clinical verification for these low-shrinkage composite resins is still being gathered, it seems likely that these commercially available low shrinkage composites have significant advantages when compared to conventional com-posite resins.
The shape of the preparation or the C-factor (the ratio of the bonded surfaces of the restoration to the unbonded surfaces) affects the stress created at the margins.46,47 In this classification system, a Class I or Class V preparation would create the greatest stress at the marginal interfaces. During polymerization of the composite resin, stress buildup can be reduced by flow of the resin. Incremental placement of

www.ineedce.com 6
composite resin can partially compensate for shrinkage by flow of the composite material; however, this is time con-suming and voids can be created during placement of incre-mental layers.48 Composite with higher shrinkage produces postoperative sensitivity by creating marginal defects into which percolation can occur,49,50 and it is indicated for use as a bulk-fill base to be overlaid with a methacrylate-based composite resin.
Low-stress CompositeA low-stress “adaptable” material has been developed that can be polymerized in one 4 mm increment rather than in the typical 1–2 mm (Figure 3). This material (Stress Decreasing Resin (SDR™) Technology) was engineered to create a new resin system that would allow internal reduction of the stress resulting from polymerization shrinkage. To control stress development within a radically polymerizable material, it was necessary to regulate the overall modulus development while maintaining its polymerization rate and conversion. With SDR™ Technology, a polymerization modulator was chemically embedded in the polymerizable resin backbone (Figure 4). Based on scientific evidence gathered to date, the polymerization modulator synergistically interacts with the camphorquinone photoinitiator to slow modulus develop-ment, allowing stress reduction without a reduction in the polymerization rate or conversion. The SDR™ Technology resin provides significantly lower curing stress than other conventional resin systems, while maintaining a high degree of conversion of the material. This ensures the development of the required physical and mechanical properties for the
use of the material as a posterior bulk fill flowable base. Es-sentially, the entire radical photopolymerization process is mediated by the polymerization modulator specially built into the resin; this allows more linear/branching chain propagation without much cross-linking and hence slower modulus development. This modulating effect allows ex-tended polymerization without a sudden increase in cross-link density. Thus, the extended “curing phase” maximizes the overall degree of conversion and minimizes the resulting polymerization stress.
This adaptable material is placed in the box and bulk light-cured up to the enamel margin. Its rheology makes it highly adaptable to the preparation form to avoid the incor-poration of voids (Figure 5).
Figure 5. Photomicrograph of bulk-cured stress-reducing resin
Note: excellent adaptation and virtual absence of voids
High translucency allows significant light transmission to bulk polymerize the material. This adaptable composite should not be placed onto the enamel occlusal margin of the cavity preparation due to its low wear resistance. Although not a low-shrinkage material (polymerization shrinkage is 3.6% vol.), it is a low-stress-producing mate-rial. It is important to understand that shrinkage stress, not shrinkage, is the cause of many stress related restorative complications. Note in Figure 6 that the shrinkage of the adaptable material is not dissimilar to other commonly used flowable composites, while shrinkage stress is consid-erably lower (Figure 7). Because the adaptable material is a flowable composite and not indicated for larger occlusal surfaces, a highly filled material should be placed in the final occlusal increment. The material self-levels, ensuring that the occlusal surface of the material is even for place-ment of the final increment of highly filled material. This two-increment technique reduces placement time and is effective and efficient for Class I and II restorations. In an ongoing clinical trial with the material, we have placed more than 100 restorations with excellent success. The case example below shows the use of SureFil SDR for posterior restorations.
X O
O O
O
O
O O
O
R
R1
R
X X
XY Y
+SDR
Conventional:
Curing
Polymerization modulator
Figure 4. Curing of stress-decreasing resin

7 www.ineedce.com
Figure 6. Percent shrinkage of bulk-fill base material compared with other flowable composites
SureFil SDR flow
Esthet-X flow
TPH3 flow
Brand A
Brand B
Brand C
Brand D
Brand E
Brand F
0
1
2
3
4
5
3.6
4.5 4.54.3 4.4
3.8 3.93.5
4.9
Figure 7. Shrinkage stress of bulk-fill base material compared with other flowable composites
SureFil SDR flow
Esthet-X flow
TPH3 flow
Brand A
Brand B
Brand C
Brand D
Brand E
Brand F0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
5.0
1.4
3.2 3.12.9
4.1
3.2
4.2
33.2
Case StudyIn this case, a carious lesion was detected distally by radio-graph in tooth number 13. A rubber dam was placed over the tooth, followed by cavity preparation and placement of a sectional matrix and band.
Figure 8. Tooth #13 pre-operatively
Figure 9. Preparation and placement of sectional matrix and band
Etchant was first applied, the tooth rinsed and dried, and Prime and Bond NT® was then applied to the dried prepa-ration. SureFil SDR flow adaptable was then placed in the preparation using the disposable unit dose.
Figure 10. Application of etchant
Figure 11. Application of bonding agent
Figure 12. Placement of bulk layer flow adaptable composite
Figure 13. Preparation filled to enamel margin with adaptable flowable composite

www.ineedce.com 8
Following placement of the bulk layer, this was light cured. Subsequently, EsthetX HD was placed occlusally and light cured to provide the final layer of composite, and the restora-tion finished .
Figure 14. Placement of final composite layer occlusally
Figure 15. Light-curing of final composite layer
Figure 16. Tooth #13 DO after finishing
SummaryWhile amalgam has a long history of safe use, patients and clinicians increasingly select esthetic tooth-colored pos-terior restorative materials. Each material has advantages and limitations. New developments in esthetic composite resins have resulted in low polymerization shrinkage and most recently a low-stress-producing esthetic restorative
material. Each restorative material has advantages and should be used with the understanding that the material(s) selected depend upon the needs of the individual patient and clinical situation.
References1 Summitt, JB, Burgess JO, Berry TG, Robbins JW, Osborne JW,
Haveman CW. The performance of bonded vs. pin-retained complex amalgam restorations: a five-year clinical evaluation. J Am Dent Assoc. 2001;132(7):923–31.
2 Ibid.3 Browning WD, Johnson WW, Gregory PN. Clinical performance
of bonded amalgam restorations at 42 months. J Am Dent Assoc. 2000;131(5):607–11.
4 Belcher MA, Stewart GP. Two-year clinical evaluation of an amalgam adhesive. J Am Dent Assoc. 1997;128(3):309–14.
5 DeRouen TA, Martin MD, Leroux BG, Townes BD, Woods JS, Leitão J, Castro-Caldas A, Luis H, Bernardo M, Rosenbaum G, Martins IP. Neurobehavioral effects of dental amalgam in children: a randomized clinical trial. J Am Med Assoc. 2006;295(15):1784–92.
6 Bellinger DC, Trachtenberg F, Daniel D, Zhang A, Tavares MA, McKinlay S. A dose-effect analysis of children’s exposure to dental amalgam and neuropsychological function: the New England Children’s Amalgam Trial. J Am Dent Assoc. 2007;138(9):1210–6.
7 Burgess J, Norling B, Summitt JB. Advances in glass ionomer material. Esthet Dent Update. 1993;4:54–8.
8 Burgess J, Norling B, Summitt JB. Resin ionomer restorative materials: the new generation. J Esthet Dent. 1994;6(5):207–15.
9 Burgess JO, Norling BK, Rawls HR, Ong JL. Directly placed esthetic restorative materials—the continuum. Compend Contin Educ Dent. 1996;17(8):731–2, 734 passim; quiz 748.
10 Burgess JO, Summitt JB, Robbins JW et al. Clinical evaluation of base, sandwich and bonded Class 2 resin composite restorations [abstract 304]. J Dent Res. 1999;78:531.
11 Yip HK, Smales RJ, Ngo HC, Tay FR, Chu FC. Selection of restorative materials for the atraumatic restorative treatment (Art) approach: a review. Spec Care Dentist. 2001;21(6):216–21.
12 Burgess JO, Norling BK, Rawls HR, Ong JL. Directly placed esthetic restorative materials—the continuum. Compend Contin Educ Dent. 1996;17(8):731–2, 734 passim; quiz 748.
13 Phillips RW, Avery DR, Mehra R, Swartz ML, McCune RJ. One-year observations on a composite resin for Class II restorations. J Prosthet Dent. 1971;26(1):68–77.
14 Barkmeier W et al. In vitro wear assessment of high density composite resins. J Dent Res. (Abstract 2737), 1999; 78:448.
15 Winkler M, Xu X, Burgess JO. In vitro contact wear of 8 posterior resin composites. J Dent Res. (Abstract 1082), 2000;79:279.
16 Lutz F, Krejci I. Amalgam substitutes: a critical analysis. J Esthet Dent. 2000;12(3):146–59.
17 Bagby M et al. Interproximal contacts of packable composites. J Dent Res. (Abstract 2440), 2000;79:448.
18 Peumans M, Van Meerbeek B, Asscherickx K, Simon S, Abe Y, Lambrechts P, Vanherle G. Do condensable composites help to achieve better proximal contacts? Dent Mater. 2001;17(6):533–41.
19 Lai JH, Johnson AE. Measuring polymerization shrinkage of photoactivated restorative materials by a water-filled dilatometer. Dent Mater. 1993;9(2):139–43.
20 Davidson CL, de Gee AJ, Feilzer A. The competition between the composite-dentin bond strength and the polymerization contraction stress. J Dent Res. 1984;63(12):1396–9.
21 Suliman AH, Boyer DB, Lakes RS. Polymerization shrinkage of composite resins: comparison with tooth deformation. J Prosthet Dent. 1994;71(1):7–12.
22 Albers HF. Resin polymerization. ADEPT Report. 2000; 6(3).23 Kanca J 3rd, Suh BI. Pulse activation: reducing resin-based

9 www.ineedce.com
composite contraction stresses at the enamel cavosurface margins. Am J Dent. 1999;12(3):107–12.
24 Goracci G, Mori G, Casa de’Martinis L. Curing light intensity and marginal leakage of resin composite restorations. Quintessence Int. 1996;27:355–62.
25 Ibid.26 Walker RS, Burgess JO. Microleakage of class V composite
restorations with different visible-light-curing methods. J Dent Res. (Abstract 397), 1999;78:155.
27 Walker RS, Burgess JO. Microleakage of class V composite restorations with different curing methods. J Dent Res. 2000;79:45.
28 Kanca J 3rd, Suh BI. Pulse activation: reducing resin-based composite contraction stresses at the enamel cavosurface margins. Am J Dent. 1999;12(3):107–12.
29 Lopes GC, Baratieri LN, Monteiro S, Vieira LC. Effect of posterior placement technique on the resin-dentin interface formed in vivo. Quintessence Int. 2004;35(2):156–61.
30 van Dijken JW, Hörstedt P, Waern R. Directed polymerization shrinkage versus a horizontal incremental filling technique: interfacial adaptation in vivo in Class II cavities. Am J Dent. 1998;11(4):165–72.
31 Oberländer H, Friedl KH, Schmalz G, Hiller KA, Kopp A. Clinical performance of polyacid-modified resin restorations using “softstart-polymerization.” Clin Oral Investig. 1999;3(2):55–61.
32 Brackett WW, Covey DA, St Germain HA Jr. One-year clinical performance of a self-etching adhesive in class V resin composites cured by two methods. Oper Dent. 2002;27(3):218–22.
33 Bernardo, Martin, Johnson. J Dent Res. (Abstract 442), 2002.34 Chan DC, Browning WD, Frazier KB, Brackett MG. Clinical
evaluation of the soft-start (pulse-delay) polymerization technique in Class I and II composite restorations. Oper Dent. 2008;33(3):265–71.
35 Clelland NL, Pagnotto MP, Kerby RE, Seghi RR. Relative wear of flowable and highly filled composite. J Prosthet Dent. 2005;93(2):153–7.
36 Ibid.37 Gallo JR, Burgess JO, Ripps AH, Walker RS, Bell MJ, Turpin-
Mair JS, Mercante DE, Davidson JM. Clinical Evaluation of Two Flowable Composites. Quintessence Int. 2006;37(3):225–31.
38 Cadenaro M, Marchesi G, Antoniolli F, Davidson C, De Stefano Dorigo E, Breschi L. Flowability of composites is no guarantee for contraction stress reduction. Dent Mater. 2009;25(5):649–54. Epub 2009 Jan 10.
39 Stavridakis MM, Dietschi D, Krejci I. Polymerization shrinkage of flowable resin-based restorative materials. Oper Dent. 2005;30(1):118–28.
40 Efes BG, Dörter C, Gömeç Y, Koray F. Two-year clinical evaluation of ormocer and nanofill composite with and without a flowable liner. J Adhes Dent. 2006;8(2):119–26.
41 Rees JS, Jacobsen PH. The polymerization shrinkage of composite resins. Dent Mater. 1989;5(1):41–4.
42 Puckett AD, Smith R. Method to measure the polymerization shrinkage of light-cured composites. J Prosthet Dent. 1992;68(1):56–8.
43 Ferracane JL, Greener EH. The effect of resin formulation on the degree of conversion and mechanical properties of dental restorative resins. J Biomed Mater Res. 1986;20(1):121–31.
44 Carioscia JA, Lu H, Stansbury JW, Bowman CN. Thiol-ene oligomers as dental restorative materials. Dent Mater. 2005;21(12):1137–43.
45 Carioscia JA, Stansbury JW, Bowman CN. Evaluation and control of thiol-ene/thiol-epoxy hybrid networks. Polymer (Guildf). 2007;48(6):1526–32.
46 Feilzer AJ, De Gee AJ, Davidson CL. Quantitative determination of stress reduction by flow in composite restorations. Dent Mater. 1990;6(3):167–71.
47 Feilzer AJ, De Gee AJ, Davidson CL. Setting stress in composite resin in relation to configuration of the restoration. J Dent Res.
1987;66(11):1636–9. 48 Ibid.49 Eick JD, Welch FH. Polymerization shrinkage of posterior
composite resins and its possible influence on postoperative sensitivity. Quintessence Int. 1986;17(2):103–11.
50 Borgmeijer PJ, Kreulen CM, van Amerongen WE, Akerboom HB, Gruythuysen RJ. The prevalence of postoperative sensitivity in teeth restored with Class II composite resin restorations. ASDC J Dent Child. 1991;58(5):378–83.
Author ProfileJohn O. Burgess, DDS, MSDr. Burgess is the Assistant Dean for Clinical Research and the Director of The Biomaterials Graduate Program at the Uni-versity of Alabama in Birmingham. He graduated from Emory University School of Dentistry and completed graduate training at the University of Texas Health Science Center in Houston. He served as military consultant to the Surgeon General in General Dentistry and was Chairman of Dental Research and Dental Materials at Wilford Hall Medical Center. Dr. Burgess is a diplomat of the Federal Services Board in General Dentistry and the American Board of General Dentistry. He is a Fellow of the Academy of Dental Materials and the American College of Dentists, and an elected member of The American Academy of Esthetic Dentistry and The American Restorative Academy. He is a member of the Academy of Operative Dentistry, The American and International Associations for Dental Research, the Alabama Dental Association and the ADA. Dr. Burgess is the author of over 300 journal articles, textbook chapters and abstracts and has presented more than 800 continuing education programs nation-ally and internationally. Dr. Burgess is an active investigator on clinical trials evaluating posterior composites, adhesives, fluoride releasing materials, impression materials and class 5 restorations. He maintains a part-time practice in general dentistry.
Deniz Cakir, DDS, MS Dr. Deniz Cakir is an instructor the University of Alabama at Birmingham, School of Dentistry teaching graduates and dental students. She graduated from Ankara University School of Den-tistry in 2002, and completed graduate training at the University of Alabama in Birmingham, School of Dentistry in 2005. Dr. Cakir is a member of the American Dental Association and the International Association for Dental Research. She is an active researcher in the area of dental materials and has authored nu-merous articles and abstracts on dental materials.
DisclaimerThe author(s) of this course has/have no commercial ties with the sponsors or the providers of the unrestricted educational grant for this course.
Reader FeedbackWe encourage your comments on this or any PennWell course. For your convenience, an online feedback form is available at www.ineedce.com.

Online CompletionUse this page to review the questions and answers. Return to www.ineedce.com and sign in. If you have not previously purchased the program select it from the “Online Courses” listing and complete the online purchase. Once purchased the exam will be added to your Archives page where a Take Exam link will be provided. Click on the “Take Exam” link, complete all the program questions and submit your answers. An immediate grade report will be provided and upon receiving a passing grade your “Verification Form” will be provided immediately for viewing and/or printing. Verification Forms can be viewed and/or printed anytime in the future by returning to the site, sign in and return to your Archives Page.
www.ineedce.com 10
Questions
Questions
1. Material selection for restoring posterior teeth depends upon _______________.a. the patient’s age and caries riskb. esthetic and functional requirementsc. the ability to isolate the toothd. all of the above
2. _______________ bond to tooth structure and may reinforce weakened tooth structure.a. Compomersb. Glass ionomersc. Composite resinsd. all of the above
3. Amalgam restorations may be bonded to tooth structure with adhesives using the _______________.a. self-adhesive techniqueb. chelating amalgam techniquec. bonded amalgam techniqued. none of the above
4. Recent studies on amalgam by the _______________ have provided addi-tional evidence for the safety of amalgam in children.a. ADAb. NIHc. FDAd. all of the above
5. Fluoride-releasing composites _______________.a. release low levels of fluorideb. have better wear resistance and toughness than
other fluoride-releasing restorative materialsc. may not be effective for high-caries-risk patientsd. all of the above
6. Glass ionomer and resin-modified glass ionomer restorative materials _______________.a. have the highest levels of fluoride releaseb. have good recharge of fluoride which increases
long-term fluoride releasec. are useful for high-caries-risk patientsd. all of the above
7. The conditioners used with glass ionomer cements _______________ the tooth surface prior to bonding and effectively improve the bond of the glass ionomer to the tooth.a. cleanb. etchc. dessicated. all of the above
8. Nanofillers added to resin-modified glass ionomer cement _______________. a. improve its estheticsb. improve its handlingc. result in a smoother restorationd. all of the above
9. Compomers are blends of _______________.a. acrylic and glass ionomerb. acrylic and resin compositec. glass ionomer and resin composited. none of the above
10. Compomers _______________.a. contain more resin than resin-modified glass
ionomersb. offer good fluoride release and rechargec. have been used successfully in the primary denti-
tiond. all of the above
11. Currently more than _______________of all direct posterior restorations are composite.a. 20%b. 30%c. 40%d. 50%
12. The use of _______________ matrices removes some of the difficulties associated with composite resin placement.a. circularb. sectionalc. segregatedd. all of the above
13. Composite resin polymerization shrink-age contributes to _______________.a. marginal breakdownb. high release of fluoridec. postoperative thermal sensitivityd. a and c
14. The placement of visible light-cured composite resin in 2 mm increments is _______________.a. time-savingb. time-consumingc. efficientd. b and c
15. Photoinitiators in composite resin are activated by _______________in the pres-ence of an amine accelerator/catalyst.a. invisible lightb. visible lightc. infrared lightd. none of the above
16. Poorly cured composite resin _______________.a. has low wear resistanceb. has poor mechanical propertiesc. can result from the use of curing lights that do
not have the correct spectral distribution for the composite being used
d. all of the above17. Light-curing units have been developed
to decrease contraction stress by _______________ the rate of composite resin polymerization.a. acceleratingb. slowingc. maximizingd. none of the above
18. Some studies have reported no signifi-cant difference in _______________when composite resins are polymerized with or without a soft-start polymerization.a. marginal integrityb. marginal discolorationc. speed of polymerizationd. a and b
19. Flowable composites _______________.a. are conventional or microfilled composite resinsb. have lower viscosity than other compositesc. result in better adaptation to cavity wallsd. all of the above
20. Flowable composites with higher percentage filler loads reduce the concern for _______________compared to lower percentage filler loads.a. greater wear resistanceb. greater esthetic appealc. polymerization shrinkaged. a and c
21. Polymerization shrinkage of composite resins ranges from _______________.
a. 1.7% to 0.3%b. 2.7% to 0.6%c. 3.7% to 0.9%d. none of the above
22. Flowable composite resin was originally used as _______________ to improve the adaptation of condensable composites to the prepared tooth.a. an indirect pulp capb. a direct pulp capc. a resin linerd. an outer layer
23. Cadanero et al. found that most flowable composites _______________.a. had shrinkage stress much higher than conven-
tional resin restorative materialsb. had shrinkage stress much lower than conventional
resin restorative materialsc. had shrinkage stress comparable to conventional
resin restorative materialsd. none of the above
24. _______________ et al. found that flowable resins produced considerable shrinkage stress.a. Stavriotosb. Stavridakisc. Stephanopolosd. Stakis
25. With respect to flowable composites and the results from clinical studies conducted by various investigators on these, _______________.a. their use to reduce polymerization shrinkage stress
is controversialb. shrinkage stress may be product dependentc. the consensus appears to be that their major benefit
is cavity adaptationd. all of the above
26. Increasing the filler content of composite _______________.a. increases composite stiffnessb. increases the forces of contractionc. reduces shrinkaged. all of the above
27. The use of new chemistries for com-posites has resulted in _______________ polymerization shrinkage stress.a. increasedb. maintenance of c. decreasedd. none of the above
28. The use of ____________ in composite resins results in lower polymerization shrinkage.a. dimer chemistryb. silorane ring-opening chemistryc. zinc oxide eugenold. a or b
29. The use of a new polymerization modu-lator embedded in the polymerizable resin has resulted in _______________.a. reduced curing stress b. an extended curing phase, maintaining a high
conversion rate c. no reduction in the polymerization rated. all of the above
30. _______________ of material containing polymerization modulator enables the curing of 4 mm increments versus 2 mm increments for conventional composite resins, saving time.a. Low translucencyb. Low opacityc. High translucencyd. Low transmissability
ANSWER SHEET
Material Selection for Direct Posterior Restoratives
Name: Title: Specialty:
Address: E-mail:
City: State: ZIP: Country:
Telephone: Home ( ) Office ( ) Lic. Renewal Date:
Requirements for successful completion of the course and to obtain dental continuing education credits: 1) Read the entire course. 2) Complete all information above. 3) Complete answer sheets in either pen or pencil. 4) Mark only one answer for each question. 5) A score of 70% on this test will earn you 2 CE credits. 6) Complete the Course Evaluation below. 7) Make check payable to PennWell Corp. For Questions Call 216.398.7822
Educational Objectives1. List and describe the considerations involved in the selection of posterior restorative materials
2. List and describe the history and safety profile of amalgam, its advantages and disadvantages
3. List and describe how polymerization stress occurs and its relevance to restoration failure
4. List and describe the technologies that can now be incorporated into posterior composite restoratives to combat polymerization shrinkage and/or polymerization stress
Course Evaluation1. Were the individual course objectives met? Objective #1: Yes No Objective #3: Yes No
Objective #2: Yes No Objective #4: Yes No
Please evaluate this course by responding to the following statements, using a scale of Excellent = 5 to Poor = 0.
2. To what extent were the course objectives accomplished overall? 5 4 3 2 1 0
3. Please rate your personal mastery of the course objectives. 5 4 3 2 1 0
4. How would you rate the objectives and educational methods? 5 4 3 2 1 0
5. How do you rate the author’s grasp of the topic? 5 4 3 2 1 0
6. Please rate the instructor’s effectiveness. 5 4 3 2 1 0
7. Was the overall administration of the course effective? 5 4 3 2 1 0
8. Please rate the usefulness and clinical applicability of this course. 5 4 3 2 1 0
9. Please rate the usefulness of the supplemental webliography. 5 4 3 2 1 0
10. Do you feel that the references were adequate? Yes No
11. Would you participate in a similar program on a different topic? Yes No
12. If any of the continuing education questions were unclear or ambiguous, please list them. ___________________________________________________________________
13. Was there any subject matter you found confusing? Please describe. ___________________________________________________________________ ___________________________________________________________________
14. How long did it take you to complete this course? ___________________________________________________________________ ___________________________________________________________________
15. What additional continuing dental education topics would you like to see? ___________________________________________________________________ ___________________________________________________________________
PLEASE PHOTOCOPY ANSWER SHEET FOR ADDITIONAL PARTICIPANTS.
AGD Code 253
For iMMEDiATE results, go to www.ineedce.com to take tests online.
Answer sheets can be faxed with credit card payment to (440) 845-3447, (216) 398-7922, or (216) 255-6619.
Payment of $49.00 is enclosed. (Checks and credit cards are accepted.)
If paying by credit card, please complete the following: MC Visa AmEx Discover
Acct. Number: ______________________________
Exp. Date: _____________________
Charges on your statement will show up as PennWell
If not taking online, mail completed answer sheet to
Academy of Dental Therapeutics and Stomatology,A Division of PennWell Corp.
P.O. Box 116, Chesterland, OH 44026 or fax to: (440) 845-3447
COURSE EVALUATION and PARTICIPANT FEEDBACKWe encourage participant feedback pertaining to all courses. Please be sure to complete the survey included with the course. Please e-mail all questions to: [email protected].
INSTRUCTIONSAll questions should have only one answer. Grading of this examination is done manually. Participants will receive confirmation of passing by receipt of a verification form. Verification of Participation forms will be mailed within two weeks after taking an examination.
PROVIDER INFORMATIONPennWell is an ADA CERP Recognized Provider. ADA CEROP is a service of the American Dental association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP does not approve or endorse individual courses or instructors, not does it imply acceptance of credit hours by boards of dentistry.
Concerns or complaints about a CE Provider may be directed to the provider or to ADA CERP ar www.ada.org/cotocerp/
COURSE CREDITS/COSTAll participants scoring at least 70% on the examination will receive a verification form verifying 2 CE credits. The formal continuing education program of this sponsor is accepted by the AGD for Fellowship/Mastership credit. Please contact PennWell for current term of acceptance. Participants are urged to contact their state dental boards for continuing education requirements. PennWell is a California Provider. The California Provider number is 4527. The cost for courses ranges from $29.00 to $110.00.
RECORD KEEPINGPennWell maintains records of your successful completion of any exam for a minimum of six years. Please contact our offices for a copy of your continuing education credits report. This report, which will list all credits earned to date, will be generated and mailed to you within five business days of receipt.
Completing a single continuing education course does not provide enough information to give the participant the feeling that s/he is an expert in the field related to the course topic. It is a combination of many educational courses and clinical experience that allows the participant to develop skills and expertise.
CANCELLATION/REFUND POLICYAny participant who is not 100% satisfied with this course can request a full refund by contacting PennWell in writing.
© 2011 by the Academy of Dental Therapeutics and Stomatology, a division of PennWell
CEDMAT911DE
Customer Service 216.398.7822 www.ineedce.com