martin schillinger - meet congressmeetcongress.com/pdf/meet2008/friday june...
TRANSCRIPT

SFA long term results
Martin Schillinger

Long Term Results
20 years… not available
10 years… Palmaz stentsWallstent stents
• after 4 years no significant advantage compared to PTA• TASC A lesions• no nitinol stents
Nitinol Stents
Wallstents
24211815129630
100
80
60
40
20
0Mo
Log Rank p=0.008
7
25
8
28
9
33
13
38
17
53
21
69
32
91
45
113
52
123
Cumulative
Patency
69% - Nitinolstents
34% - Wallstents
Radiology 2004
Balloon expa
nding stent
s and Wallsten
ts did not im
prove
outcomes at 1
, 2, 3, 4 year
s…
… do we really
care about l
ong term data
of these ste
nts?
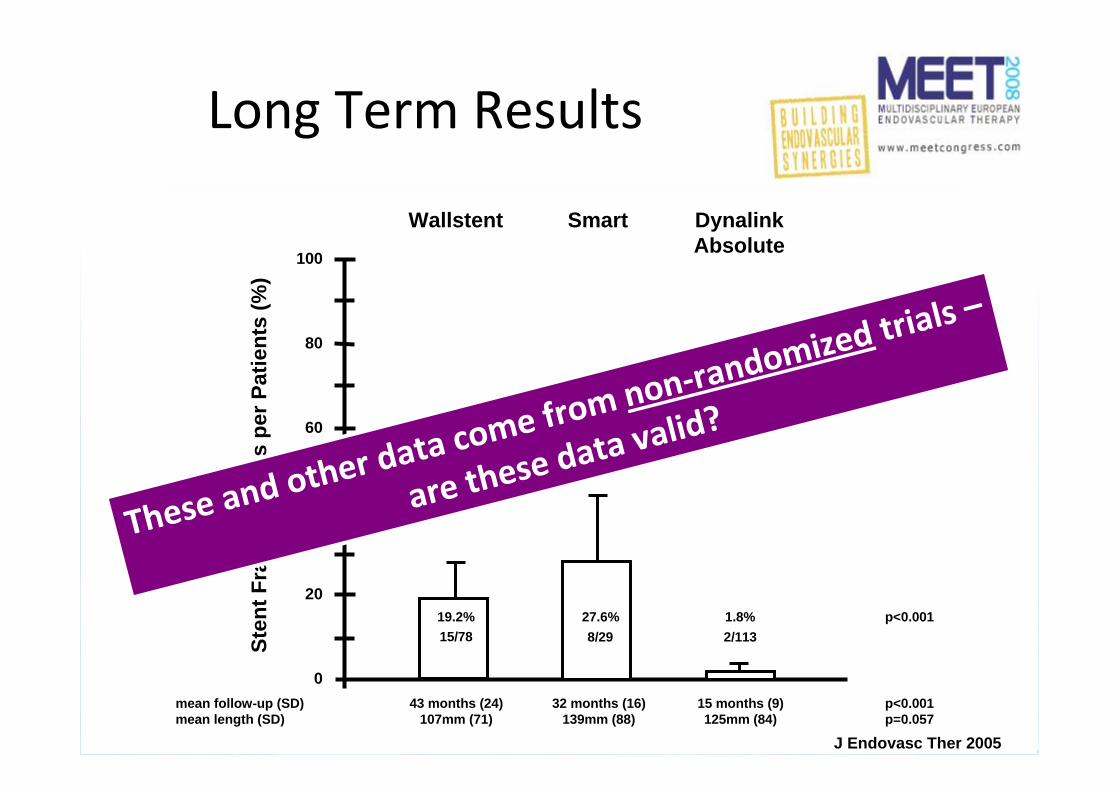
Long Term Results
20 years… not available
10 years… Palmaz stentsWallstent stents
3 to 5 years… Nitinol stents – non RCTs
J Endovasc Ther 2005J Endovasc Ther 2005
0
20
40
60
80
100St
ent F
ract
ure
Rat
es p
er P
atie
nts
(%)
15/78 8/29 2/11319.2% 27.6% 1.8%
43 months (24)107mm (71)
32 months (16)139mm (88)
15 months (9)125mm (84)
mean follow-up (SD)mean length (SD)
Wallstent Smart DynalinkAbsolute
p<0.001p=0.057
p<0.001
J Endovasc Ther 2005
These and o
ther data co
me from non‐r
andomized tr
ials –
are these da
ta valid?

Long Term Results
20 years… not available
10 years… Palmaz stentsWallstent stents
3 to 5 years… Nitinol stents – non RCTs
1 to 2 years… Nitinol stents – RCTs
???
Valid „long
term“ data from RCTs
are available
only
up to 2 year
s

Evidence fromrandomised trials
Lesion length
4.5cm 6.5cm 8.4cm 12.0cm
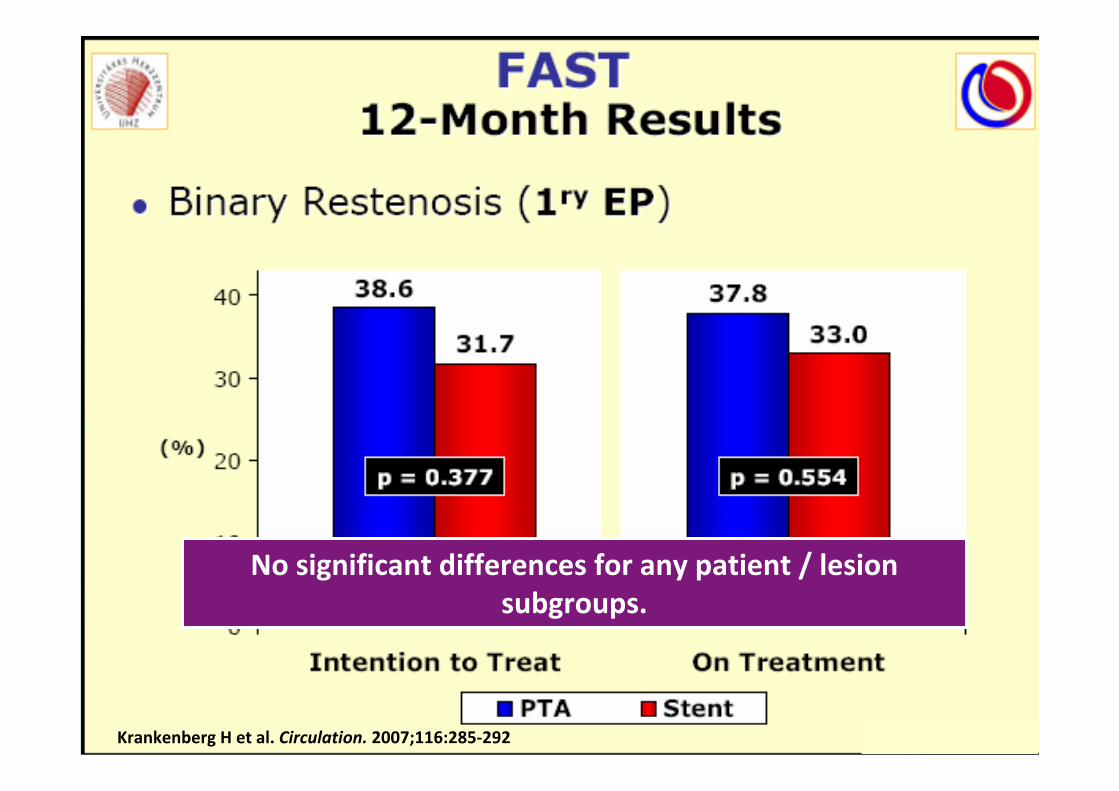
FAST
RESILIEN
T
ASTRO
N
ABS
OLU
TE
>15.0cm
…

FAST TrialBaseline Characteristics
• n=244• PTA (n=121) vs. primary stenting (n=123)
• Rutherford stages 2 to 5• de‐novo lesions• mean lesion length 4.5 cm (range 1 to 10cm)
• 1/4 chronic total occlusions• Luminexx nitinol stent (Bard)
Krankenberg H et al. Circulation. 2007;116:285‐292
Lesion length
4.5cm
Krankenberg H et al. Circulation. 2007;116:285‐292
No significant differences for any patient / lesion subgroups.

Krankenberg H et al. Circulation. 2007;116:285‐292

ConclusionsFAST
• In patients with a mean lesion length around 4 cm, primary stenting using the Luminexx Nitinol Stent did not improve morphological or clinical outcome at 12 months follow‐up.
• Subgroup analysis did not show a significant benefit of the Luminexx Stent for any lesion or patient subgroup.
Krankenberg H et al. Circulation. 2007;116:285‐292

Katzen B et al. TCT. 2007
• n=206• PTA (n=72) vs. primary stenting (n=134)
• Rutherford stages 1 to 3• mean lesion length 6.5 cm (range <15cm)
• 1/5 chronic total occlusions• Life Stent (Edwards)
RESILIENT TrialBaseline characteristics
Lesion length
6.5cm

Katzen B et al. TCT. 2007
RESILIENT TrialBaseline characteristics

Katzen B et al. TCT. 2007
RESILIENT TrialBaseline characteristics
BUT: 40.2% patients in the PTA group underwent bail‐out
stenting and were included as PTA‐failures at day 0!

ConclusionsRESILIENT
• In patients with a mean lesion length around 6 cm, primary stenting using the Lifestent improved morphological and clinical outcome compared to PTA alone.
• BUT: It remains unclear, whether primary stenting was superior compared to provisional stenting (PTA plus bail‐out stenting) in these patients.
Katzen B et al. TCT. 2007

ASTRON TrialBaseline characteristics
• n=73• PTA plus optional stenting (n=39) vs. primary stenting (n=34)
• Rutherford stages 2 to 5• de‐novo and restenotic lesions• mean treated length 8.4 cm (range 3 to 25cm)
• 1/3 chronic total occlusions• Devices: Astron Stent (Biotronik)
Schillinger M et al.
Lesion length
8.4cm
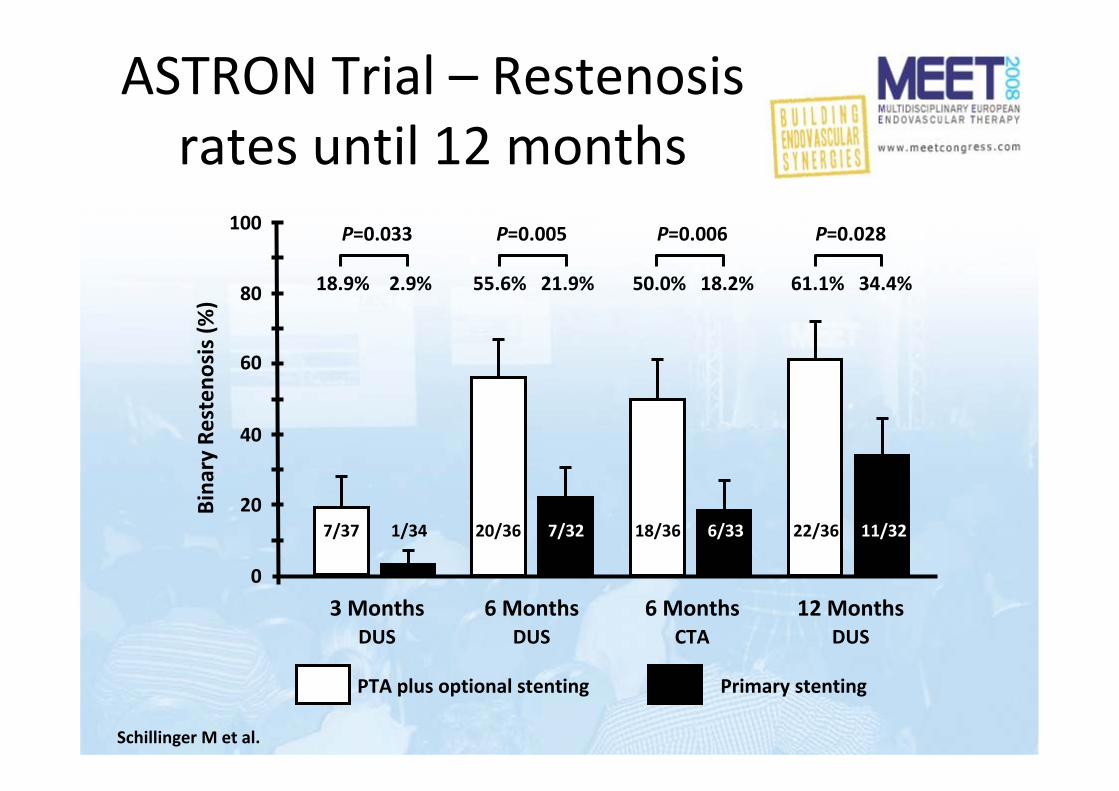
ASTRON Trial – Restenosisrates until 12 months
Schillinger M et al.
0
20
40
60
80
100
7/37 1/34 20/36 7/32 18/36 6/33 22/36 11/32
18.9% 2.9% 55.6% 21.9% 50.0% 18.2% 61.1% 34.4%
P=0.033 P=0.005 P=0.006 P=0.028Bina
ry Resteno
sis (%
)
3 Months 6 Months 6 Months 12 MonthsDUS DUS CTA DUS
PTA plus optional stenting Primary stenting

ConclusionsASTRON
• In patients with a mean treated length around 8 cm, primary stenting using the Astron Nitinol Stent improved morphological and clinical outcome compared to PTA with optional stenting.
Schillinger M et al.
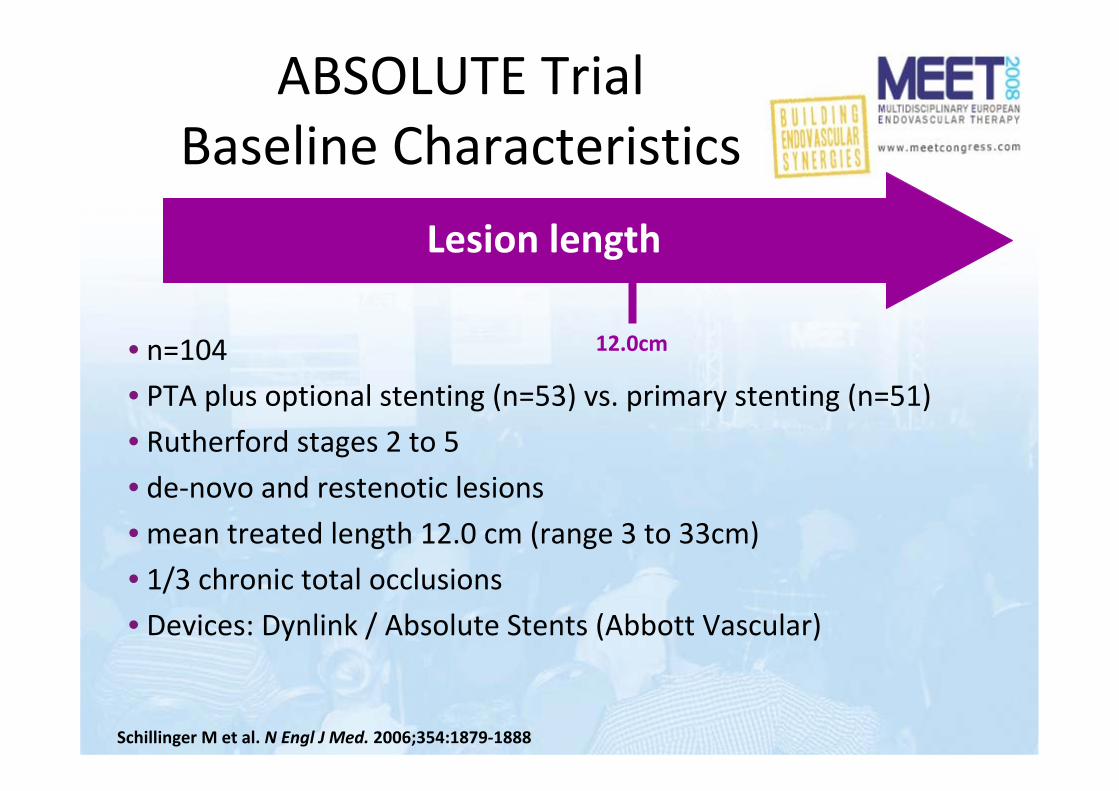
ABSOLUTE TrialBaseline Characteristics
Schillinger M et al. N Engl J Med. 2006;354:1879‐1888
• n=104• PTA plus optional stenting (n=53) vs. primary stenting (n=51)
• Rutherford stages 2 to 5• de‐novo and restenotic lesions• mean treated length 12.0 cm (range 3 to 33cm)
• 1/3 chronic total occlusions• Devices: Dynlink / Absolute Stents (Abbott Vascular)
Lesion length
12.0cm

0
20
40
60
80
100
Angiograp
hic resten
osis
at 6 m
onths (%
)
P=0.032
PTA +/‐ Stent Stent(primary)
Intention to treat
23/53 12/51
43.4% 23.5%
P=0.010
PTA only Stent(primary or secondary)
Per protocol(as treated)
18/36 17/68
50.0% 25.0%
ABSOLUTE Trial ‐ 6 month angiographic restenosis
Schillinger M et al. N Engl J Med. 2006;354:1879‐1888

ABSOLUTE Trial – Restenosisrates until 2 years
Schillinger M et al. N Engl J Med. 2006;354:1879-1888 Circulation. 2007;115:2745-2749

0 3 6 9 12 15 18 21 24Follow‐up time (months)
20
40
60
80
100
Cumulative freedo
m
from
resteno
sis (%
)
Log rank P=0.02
4652
39 (7)40 (12)
33 (13)28 (24)
33 (13)28 (24)
29 (17)19 (33)
27 (19)19 (33)
27 (19)17 (35)
27 (19)17 (35)
25 (21)16 (36)
StentPTA
45.7%
69.2%
1st year2nd year
ABSOLUTE Trial ‐ Pattern of Restenosis until 24 months
• Sustained benefit of nitinol stents @ 2‐year follow‐up• No ‘catch‐up’ phenomenon• Restenosis later than 12 months was rare
Schillinger M et al. N Engl J Med. 2006;354:1879‐1888 Circulation. 2007;115:2745‐2749
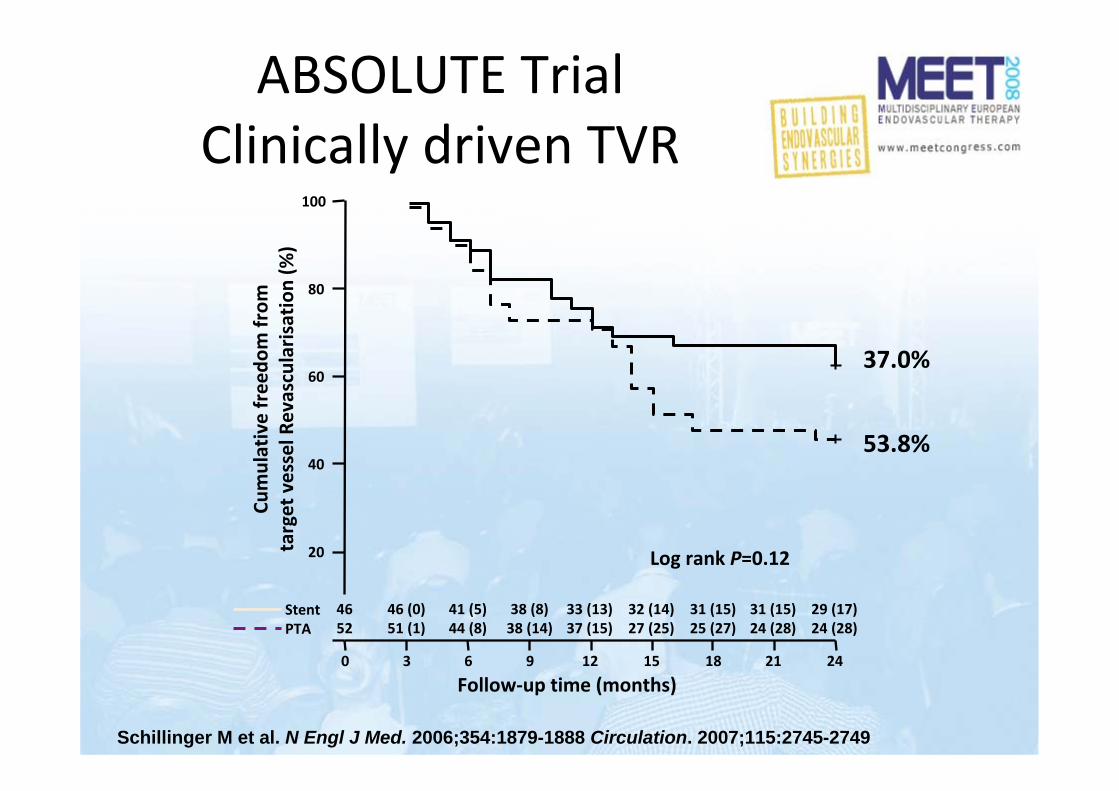
37.0%
53.8%
0 3 6 9 12 15 18 21 24
Follow‐up time (months)
20
40
60
80
100
Cumulative freedo
m from
target vessel R
evascularisation
(%)
Log rank P=0.12
4652
46 (0)51 (1)
41 (5)44 (8)
38 (8)38 (14)
33 (13)37 (15)
32 (14)27 (25)
31 (15)25 (27)
31 (15)24 (28)
29 (17)24 (28)
ABSOLUTE TrialClinically driven TVR
StentPTA
Schillinger M et al. N Engl J Med. 2006;354:1879-1888 Circulation. 2007;115:2745-2749

ABSOLUTE TrialWalking capacity
Schillinger M et al. N Engl J Med. 2006;354:1879‐1888 Circulation. 2007;115:2745‐2749

ABSOLUTE TrialHaemodynamic outcome
Schillinger M et al. N Engl J Med. 2006;354:1879‐1888 Circulation. 2007;115:2745‐2749
• Primary stenting with the ABSOLUTE nitinol stent improved primary patency rates and clinical outcomes until 24 months, when compared with balloon angioplasty with optional stenting in lesions with a mean treated length of 12 cm.
ABSOLUTE TrialConclusion

12 mo restenosis vs. lesion length:Data from randomised trials
Length of the lesion (cm)
Bina
ry resteno
sis @ 12 mon
ths (%
)
PTA
Stent
FAST
FAST
RESILIENT
ASTRON
ABSOLUTE
ABSOLUTE
ASTRON
RESILIENT

Length of the lesion (cm)
Bina
ry resteno
sis @ 12 mon
ths (%
)
PTA plus provisional stent
Stent
FAST
FAST
RESILIENT
ASTRON
ASTRONABSOLUTE
ABSOLUTE
RESILIENT
12 mo restenosis vs. lesion length:Data from randomised trials

… with long/complex lesionsFAST – RESILIENT – ASTRON – ABSOLUTE
… with restenosis after prior PTAeven Wallstents were better than repeat PTA
… when an optimal primary result is crucial (CLI)because ulcer healing rather than long‐term patency counts
Primary stenting in patients…
CLI, critical limb ischaemia

Biamino et al TCT 2004
Long Term Problems:Which stents should we use?

Factors that determine fracture rates:– Length of the lesion– Type of stent– Fracture rates beyond 12 months?
Fracture rates in the context: Data from randomised trials
SIROCCO I SIROCCO II ABSOLUTE FAST RESILIENT
6 months 19% 9% 1.5% – 2.2%
12 months 31% 11% 1.5% 12% 2.9%
Length 85 mm 82 mm 124 mm 45mm 65mm

How to treat instent restenosis?
Unresolved long term problems of SFA stenting
How to handle stent fractures?

Do current data support the use of primary nitinol stenting?
– Currently liberal ‘stenting on indication’
Which stents should we use?– Stents with approved low restenosis and low
fracture rates from randomised trials
Why should we stent the SFA?– Symptomatic SFA disease is usually long and
complex: the best results in this indication are obtained with stents
Treating the SFA in 2008:in the Absence of Long‐Term Data

The future of interventional therapy for superficial femoral artery disease

The Future…is not:
POBA obviously is not the ideal treatment for longsegment SFA disease.
baseline Post PTA 3 months 6 months

The Future…
Technically feasible, but even non‐randomizedstudies are not convincing…
…there are very good reasons why RCTare not initiated for these devices.
Freez it?
CryoplastyCut it?
Cutting balloonAtherectomy
Burn it?
Laser

The Future…is not:
0
20
40
60
80
100
Conventionalballoon
Cutting Balloon
32% 62%
6 Mon
ths an
giograph
icresten
osis (%
)p=0.048
Amighi et al. Radiology 2008
SFA de‐novo lesions
0%
20%
40%
60%
80%
100%
Bina
ry Resteno
sis Ra
te (>
50%)
17/68
PTA PCB
p=0.421 month
6/22 2/17
PTA PCB
16/22 11/17
PTA PCB
9/22 8/17
p=0.753 months
p=0.736 months
27% 12% 41% 47% 73% 65%
Dick P et al. Radiology 2008
SFA instent restenosis

The Future…
A purely mechanic
al concept (sten
t) hardly will
be sufficient to r
esolve the prob
lem of SFA disease!

Promising Concepts –for the near future
Drug coated balloons
Biodegradable Stents
Drug eluting Stents
Drug eluting balloons –THUNDER Trial
Tepe et al. N Engl J Med. 2008;358:689‐699
• n=154 randomized to three groups:
‐ Paclitaxel coated balloon (n=48)
‐ Standard balloon (n=54)
‐ Paclitaxel disolved in contrast medium (n=52)
• Endpoints:
‐ Late lumen loss by angiography at 6 months
‐ TLR until 24 months

Drug eluting balloons –THUNDER Trial
Tepe et al. N Engl J Med. 2008;358:689‐699
• claudication or critical limb ischemia (mean ABI 0.5)
• mean age 68 years
• 49% diabetics
• 27% chronic total occlusions
• 36% restenotic lesions
• mean leasion length 7.4cm

Drug eluting balloons –THUNDER Trial
Tepe et al. N Engl J Med. 2008;358:689‐699
0
0.5
1
1.5
2
2.5
3
3.5
4
StandardBalloon
PaclitaxelBalloon
Contrast Mediaplus Paclitaxel
Angiograp
hic late lumen
loss @
6mo p<0.001
P=0.11

Drug eluting balloons –THUNDER Trial
Tepe et al. N Engl J Med. 2008;358:689‐699
0102030405060708090
100
StandardBalloon
PaclitaxelBalloon
Contrast Mediaplus Paclitaxel
Bina
ry Resteno
sis @ 6 m
o (%
)
44%55%
17%

Drug eluting balloons –THUNDER Trial
Tepe et al. N Engl J Med. 2008;358:689‐699
0102030405060708090
100
StandardBalloon
PaclitaxelBalloon
Contrast Mediaplus Paclitaxel
Target lesion
revascularisation
(%)
37% 52%
4% 15%
29% 40%
6 months
24 months

Restenosis vs. lesion length:Data from randomised trials
Length of the lesion (cm)
Bina
ry resteno
sis @ 12 mon
ths (%
)
PTA
Stent
FAST
FAST
RESILIENT
ASTRON
ABSOLUTE
ABSOLUTE
ASTRON
RESILIENT
THUNDER (6 Months)

Drug eluting balloons –THUNDER Trial
Tepe et al. N Engl J Med. 2008;358:689‐699

Drug eluting balloons
Drug eluting balloon technology may improve restenosis
rates in short‐ to medium‐length SFA lesions.
However, the problems of residual stenosis and
elastic recoil remain unresolved.

Drug‐eluting Stents
30 days after coronary stenting (pigs)
Bare metal stent DES (Sirolimus)

Duda et al. Circulation 2002
Baseline Post Stent 6 Months
Drug‐eluting Stents

Restenosis at 2 years:DES 22.9%BMS 21.1%
Duda et. al JEVT 2006
0
10
20
30
40
6 Months 9 Months 18 Months 24 Months
SIROCCO I + II –Follow‐up until 2 Years

Drug‐eluting Stents –critical issues
• choice of drug: ‐limus family vs. paclitaxel
• duration of drug‐delivery
• polymeric vs. non‐polymeric stent platform
• dosage of delivered drug
• carrier platform (stent fractures!)

Drug‐eluting Stents –ongoing trials
Zilver‐PTX
• paclitaxel
• fast delivery
• non‐polymeric stent platform
• nitinol
STRIDES
• everolimus
• slow release kinetics
• polymeric stent platform
• nitinol
After the drug i
s released, DES
remains a purely m
echanical
concept, will thi
s be sufficient t
o resolve the
problem of SFA d
isease in the lon
g‐term?

Biodegradable Stents –critical issues
• choice of material: Mg‐alloy vs. polymeric materials
• problematic mechanical properties:‐ limited radial strength‐ limited flexibility‐ investigational products are all balloon expanding
• duration until stent desintegration / complete degradation
• vessel wall reaction to degradation process
• with vs. without drug coating
• coronary and BTK data are disappointing

The Future of SFA Treatment
1. next generation bare Nitinol stents– minimized fracture rates– optimized radial strength– short term restenosis < 1 year will remain the problem
2. Drug eluting Nitinol stents– based on latest generation nitinol BMS– postpone restenosis to > 1 year
3. Biodegradable (drug eluting) stents– resolve mechanical problems?– resolve restenosis?
4. Pro‐healing technologies??