marcussen - splinting & casting pearls-thursday7-2-2...marcussen - splinting & casting...
TRANSCRIPT

9/22/14
1
Britt Marcussen, MD Sports Medicine University of Iowa
! None
! 1. Discuss indications for splinting ! 2. Discuss advantages/disadvantages of splints ! 3. Go through splinting materials ! 4. Discuss casting indications and different materials
! 5. Cover a smattering of ortho pearls ! 6. Discuss common fractures and assocated splints/casts
! 7. Discuss basics of making each type of splint
! Provides non-‐circumferential support ! Accommodates swelling ! Useful for acute injuries ! Held in place by elastic bandage
9/22/14
2
! Stabilize acute injury (sprain, fx, reduction) ! Immobilization…initial ! Pain control ! Prevent further injury ! Tenosynovitis ! Arthritis ! Gout ! Post surgery
! Accommodates swelling ! May take off and re-‐apply if needed ! Faster to apply ! Easier to apply ! Prefabricated splints available
! Allows more motion at site of injury than cast ! Patients can take them off…non compliance ! May not provide definitive care
9/22/14
3
! Circumferential support ! Better immobilization at fracture site ! Provides definitive care ! Most patients can’t take them off
! Cost…fiber glass is more $$ ! Moldability…plaster has more ! Accommodation of swelling…plaster has more
! Heat production ! Curing time 24 hrs for plaster ! Use in reduction…plaster usually preferred ! Contact with water…plaster loses structure ! Waterproof padding available
! Heat production inversely proportional to setting time (fiberglass = more heat)
! More layers of plaster = more heat ! Increased pressure applied = more heat ! Hotter water = faster setting time ! Colder water = slower setting time ! No water = slowest setting time, best when starting out
! Mind the surface the arm is resting on…
! Harder to apply ! Does not accommodate swelling as well as splint
! Increased risk for complications ! Lasts about 6 weeks, starts to crumble ! Falls apart in water contact ! Messy

9/22/14
4
! Swelling accommodation <plaster and <<splint
! Not as good as plaster following fx reduction
! Roll on material…don’t pull tight ! Let the material go where is wants to go… ! Make cuts to adjust ! When wet, apply paper cut outs or cast material shapes for fun designs.
! Assess the injury ! Determine need for immobilization ! Neurovascular exam prior to AND after splint application Function Arterial pulse Capillary refill Temperature Sensation
! Stockinette ! Padding ! Fiberglass or plaster ! Tape ! Container of water ! Elastic bandage (Ace wrap) ! Sheets…to keep the patient dry ! Bandage scissors ! Strong scissors to cut fiberglass
9/22/14
5
! Pick appropriate size, no too tight, not too loose
! Error on the side of leaving too long on both ends
! Make slits in areas of folding
! Typically 2 or 3 layers thick ! More padding over areas of pressure ! Overlap ~50% each time ! Apply padding 2-‐3 cm beyond intended edges of splint
! Tear out folds ! Tear technique… ! Too much padding = less support ! Cast index
! Measure twice…cut once… ! Reseal the edge! ! Wet the strip…pad dry ! Mold to desired body location ! Trim sharp edges
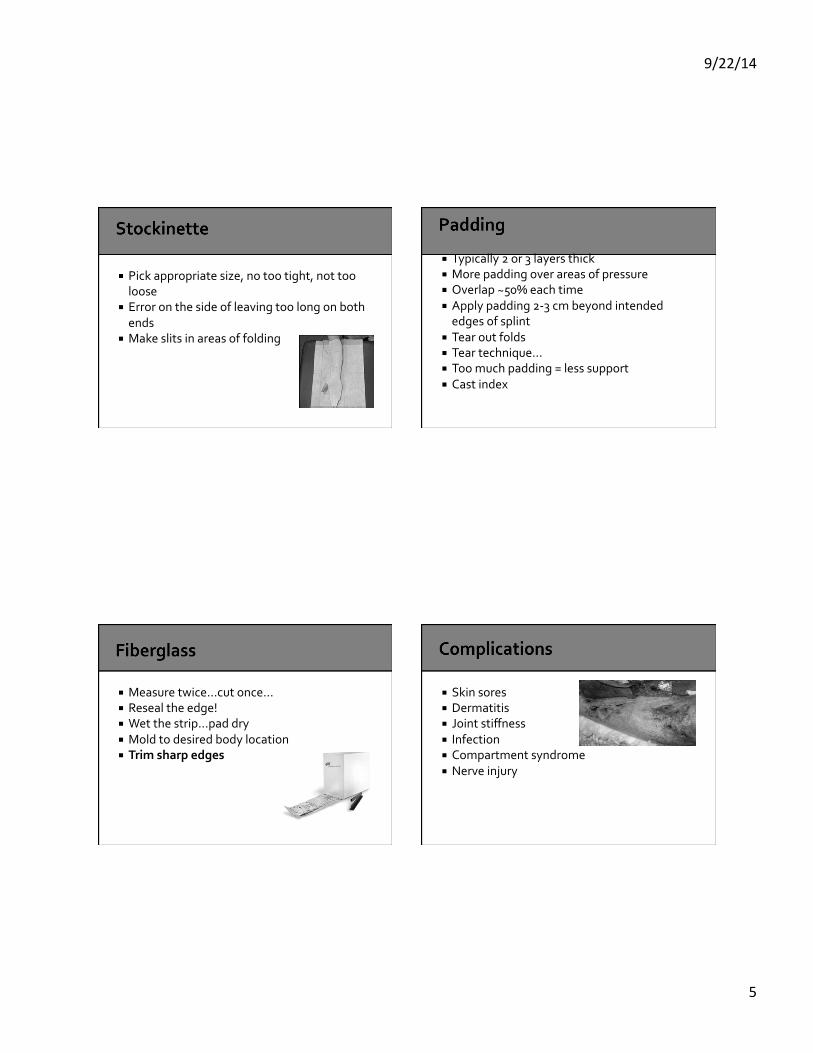
! Skin sores ! Dermatitis ! Joint stiffness ! Infection ! Compartment syndrome ! Nerve injury
9/22/14
6
! Long arm: 1. Displaced distal radius fx 2. Scaphoid fx 3. Combined radius & ulnar fracture 4. Proximal forearm fractures 5. Elbow fractures ! Short arm: 1. Thumb fx 2. Non displaced distal radius fx 3. Transition out of long arm cast ! Anytime want to minimize rotation of forearm or immobilize the elbow
! “Never bad to start with long arm”
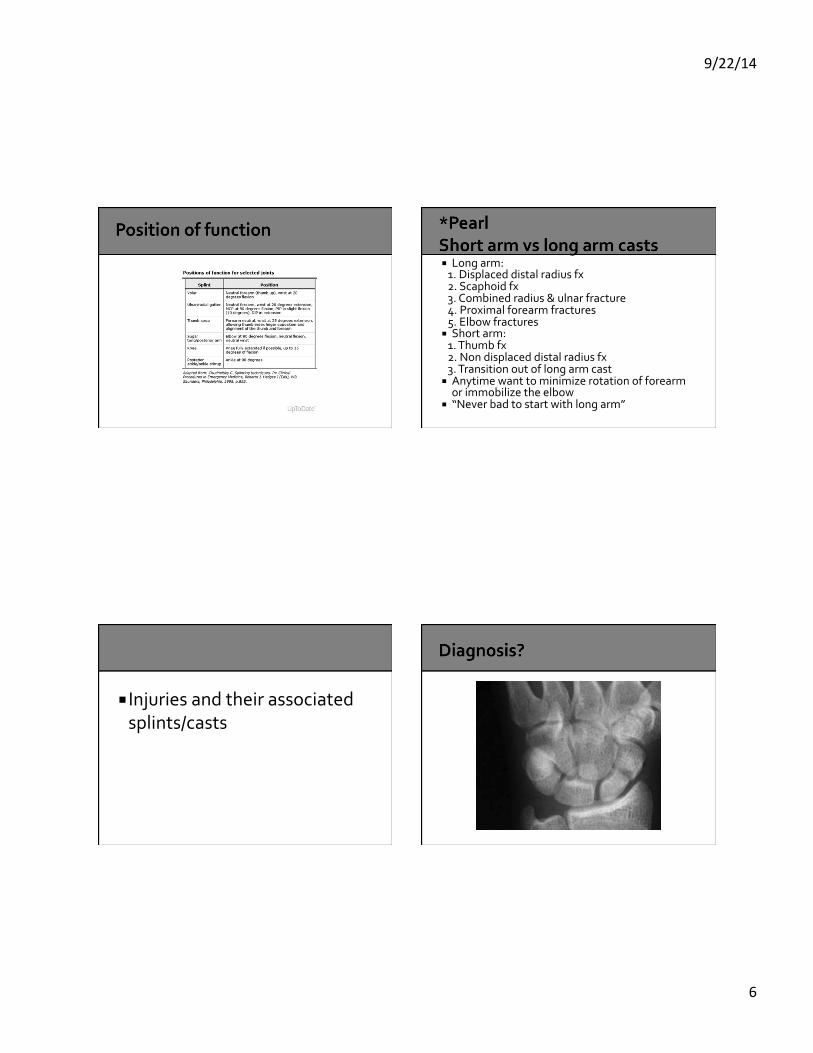
! Injuries and their associated splints/casts
9/22/14
7
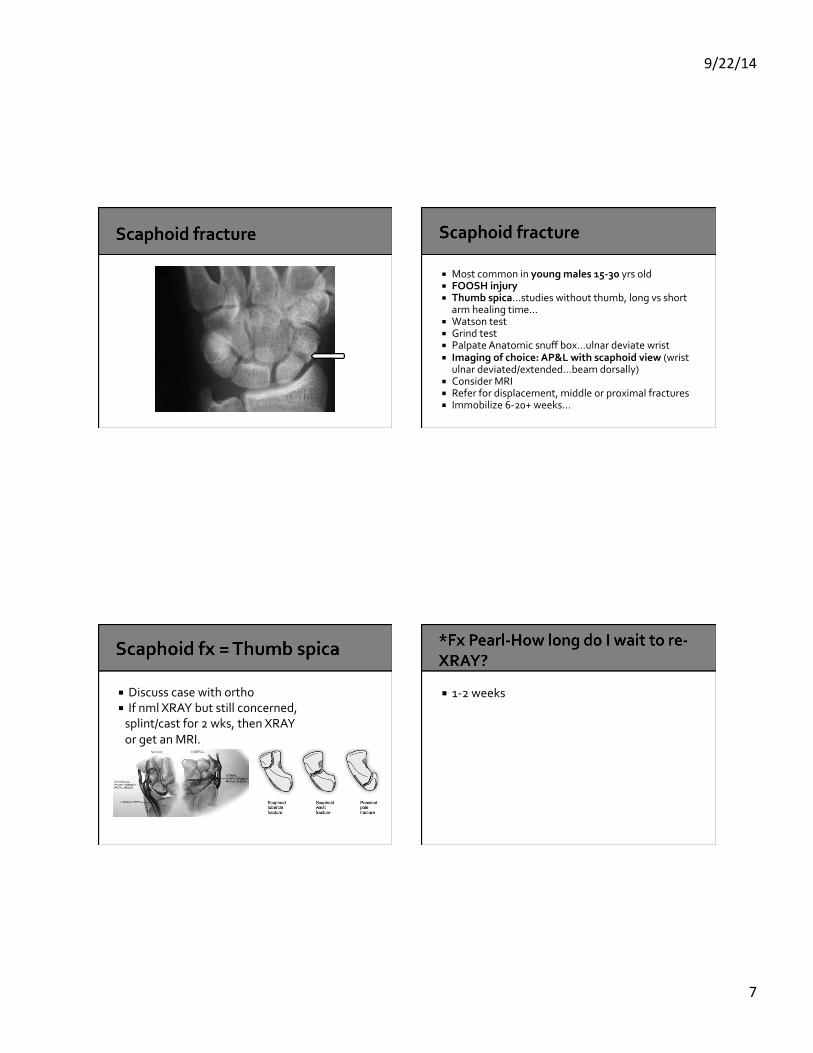
! Most common in young males 15-‐30 yrs old ! FOOSH injury ! Thumb spica…studies without thumb, long vs short
arm healing time… ! Watson test ! Grind test ! Palpate Anatomic snuff box…ulnar deviate wrist ! Imaging of choice: AP&L with scaphoid view (wrist
ulnar deviated/extended…beam dorsally) ! Consider MRI ! Refer for displacement, middle or proximal fractures ! Immobilize 6-‐20+ weeks…
! Discuss case with ortho ! If nml XRAY but still concerned, splint/cast for 2 wks, then XRAY or get an MRI.
! 1-‐2 weeks
9/22/14
8
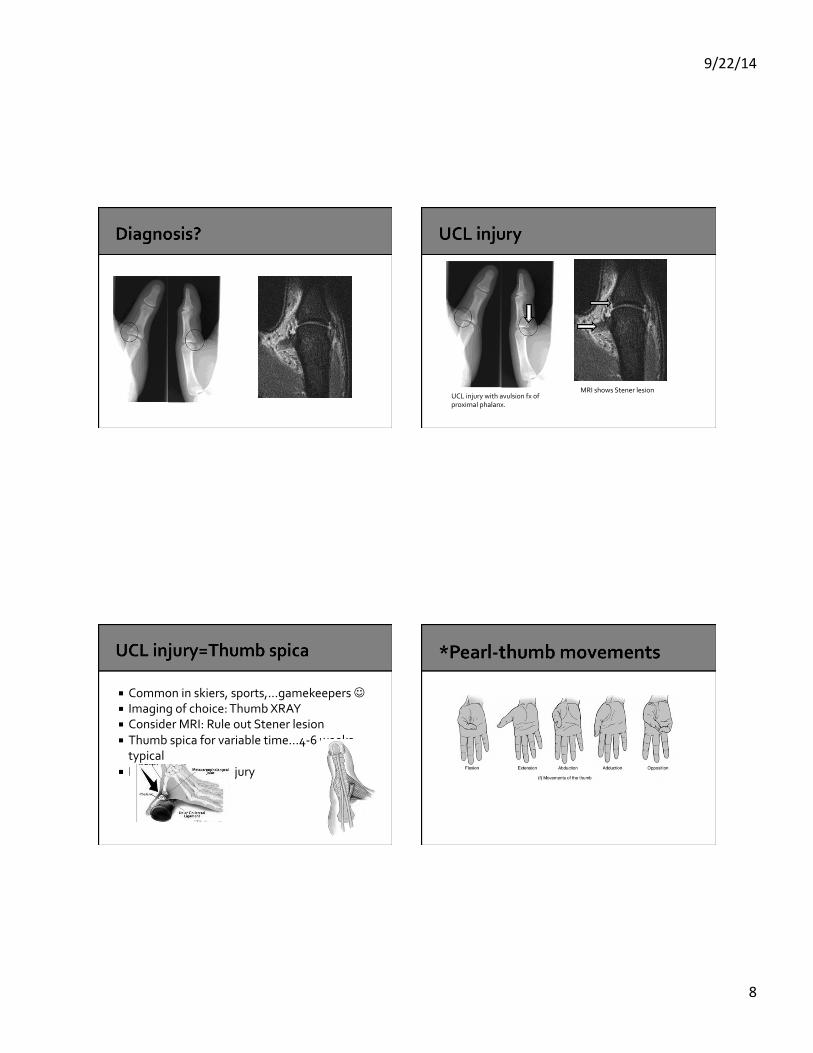
MRI shows Stener lesion UCL injury with avulsion fx of proximal phalanx.
! Common in skiers, sports,…gamekeepers ☺ ! Imaging of choice: Thumb XRAY ! Consider MRI: Rule out Stener lesion ! Thumb spica for variable time…4-‐6 weeks typical
! Refer for grade III injury
9/22/14
9
! MeatLOAF ! Meat= Median nerve ! L= Lumbricals 1&2 ! O= Opponens pollicus ! A=Abductor pollicus ! F=Flexor pollicus
! Extension=Radial nerve ! Adduction=Ulnar nerve
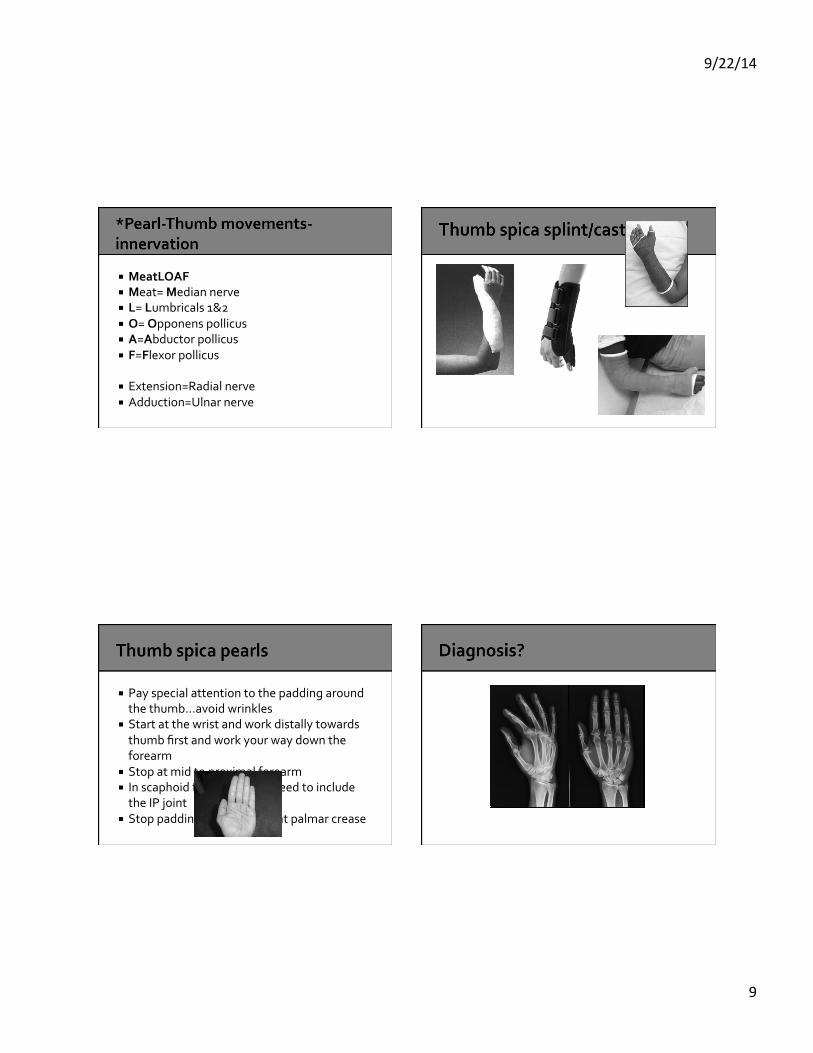
! Pay special attention to the padding around the thumb…avoid wrinkles
! Start at the wrist and work distally towards thumb first and work your way down the forearm
! Stop at mid to proximal forearm ! In scaphoid fx cast doesn’t need to include the IP joint
! Stop padding/cast material at palmar crease

9/22/14
10
! Boxer fx or street fighter fracture ! Note angulation ! Neck fracture: 30-‐40 degrees tolerated ! Shaft fracture: <20 degrees tolerated ! ~6 weeks immobilization
! Put padding between fingers…avoid maceration
! Use a wide enough splint ! Cover the DIP joint ! Position of function
! 2nd or 3rd metacarpal fracture/injury

9/22/14
11
! Augmentin first line ! Doxy, Bactrim, Pen VK, Cefuroxime, Cipro, Moxi, Levo ! Agents lacking activity against Eikenella corrodens
should be avoided; these include: 1. First-‐generation Cephalosporins (such as cephalexin) 2. Penicillinase-‐resistant penicillins (such as Dicloxacillin) 3. Macrolides (such as erythromycin) 4. Clindamycin 5. Aminoglycosides ! Local resistance patterns
! Aka Torus fracture ! Kids, boys>girls ! FOOSH injury ! Imaging of choice: at least 2 views of forearm AP&L
! Splint: volar, Sugar tong, pre-‐fabricated splint, etc
! Short arm cast 3-‐6 weeks ! Removable splint may provide definitive tx
9/22/14
12
! Stabilizes wrist and elbow ! Minimizes pronation/supination ! Minimizes flex/extend wrist ! Limits elbow motion ! Start/stop just shy of MCP joints ! Flush with elbow ! Reverse sugar tong !
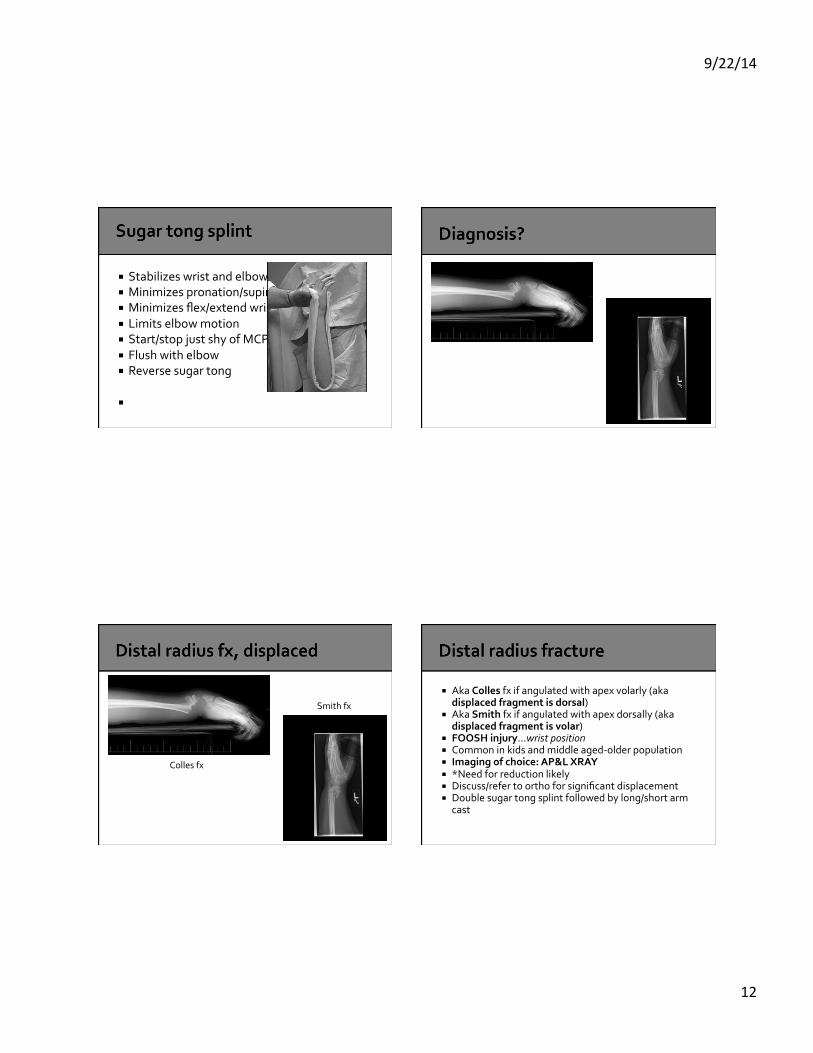
Colles fx
Smith fx
! Aka Colles fx if angulated with apex volarly (aka displaced fragment is dorsal)
! Aka Smith fx if angulated with apex dorsally (aka displaced fragment is volar)
! FOOSH injury…wrist position ! Common in kids and middle aged-‐older population ! Imaging of choice: AP&L XRAY ! *Need for reduction likely ! Discuss/refer to ortho for significant displacement ! Double sugar tong splint followed by long/short arm
cast
9/22/14
13
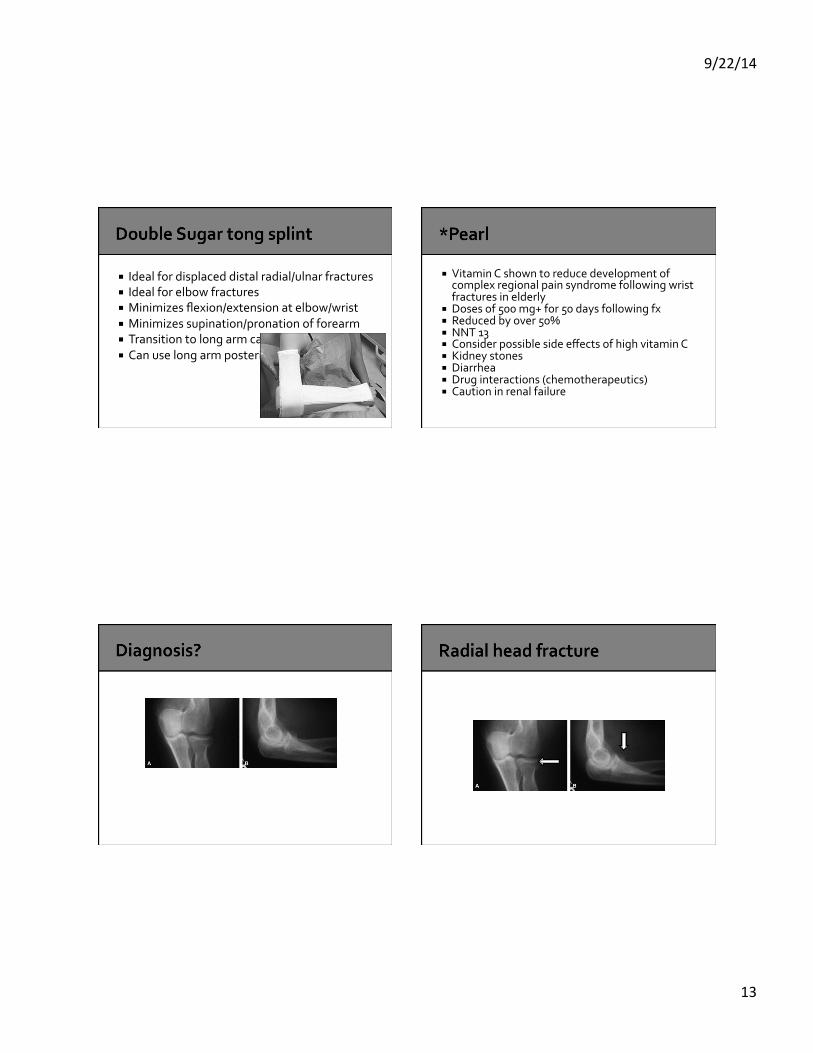
! Ideal for displaced distal radial/ulnar fractures ! Ideal for elbow fractures ! Minimizes flexion/extension at elbow/wrist ! Minimizes supination/pronation of forearm ! Transition to long arm cast ! Can use long arm posterior splint
! Vitamin C shown to reduce development of complex regional pain syndrome following wrist fractures in elderly
! Doses of 500 mg+ for 50 days following fx ! Reduced by over 50% ! NNT 13 ! Consider possible side effects of high vitamin C ! Kidney stones ! Diarrhea ! Drug interactions (chemotherapeutics) ! Caution in renal failure
9/22/14
14
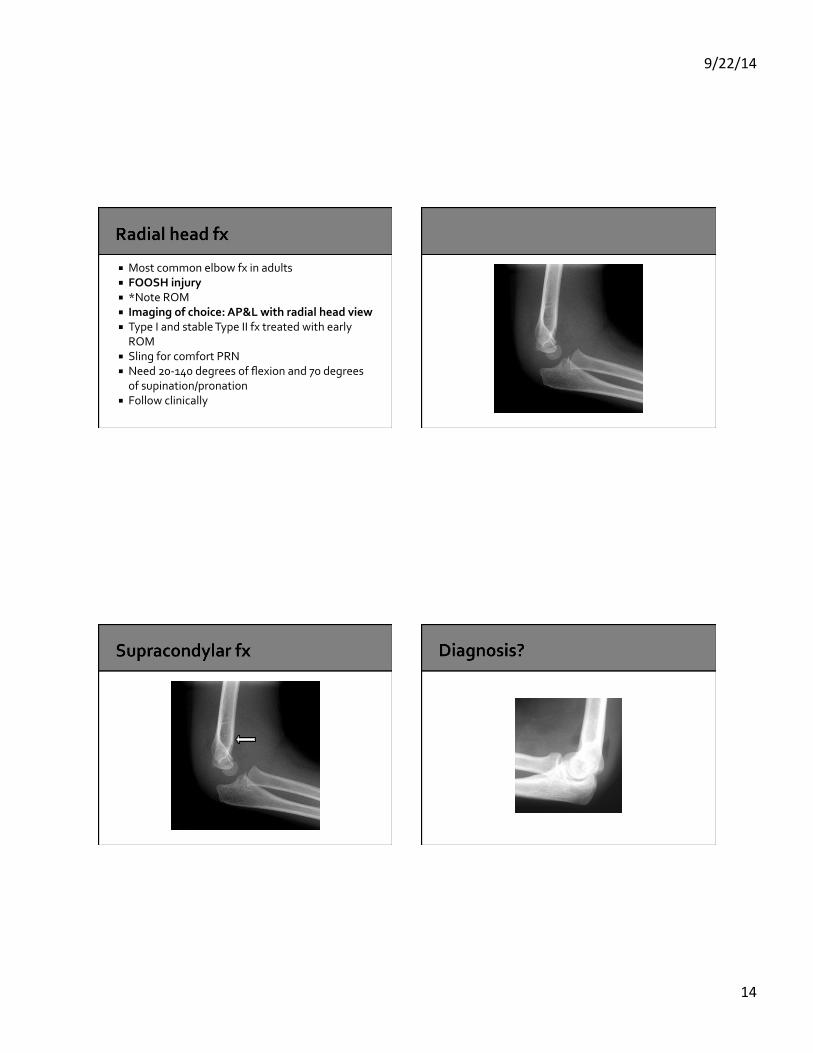
! Most common elbow fx in adults ! FOOSH injury ! *Note ROM ! Imaging of choice: AP&L with radial head view ! Type I and stable Type II fx treated with early ROM
! Sling for comfort PRN ! Need 20-‐140 degrees of flexion and 70 degrees of supination/pronation
! Follow clinically

9/22/14
15
! Most common fracture in kids ! Imaging of choice: AP & L elbow films ! Consider humerus and forearm ! Splint: Double sugar tong or long arm posterior
! Cast: Long arm ! Immobilize 4-‐6 weeks ! Refer for displaced fractures
9/22/14
16
9/22/14
17
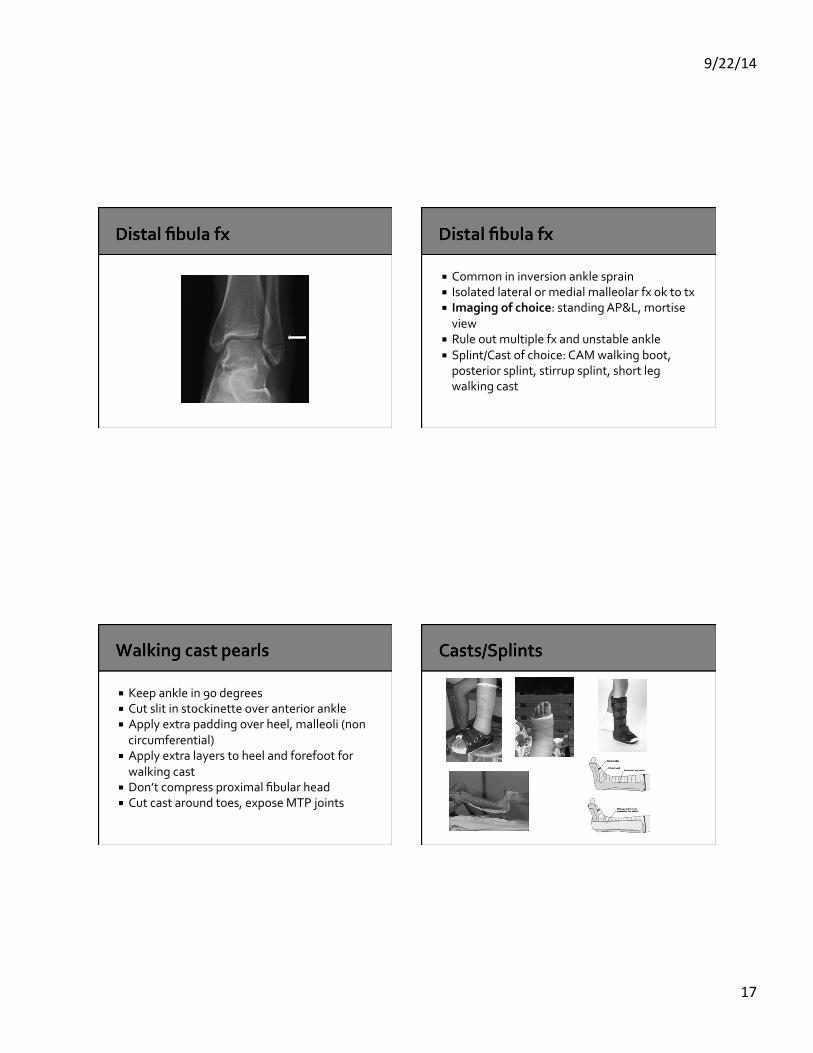
! Common in inversion ankle sprain ! Isolated lateral or medial malleolar fx ok to tx ! Imaging of choice: standing AP&L, mortise view
! Rule out multiple fx and unstable ankle ! Splint/Cast of choice: CAM walking boot, posterior splint, stirrup splint, short leg walking cast
! Keep ankle in 90 degrees ! Cut slit in stockinette over anterior ankle ! Apply extra padding over heel, malleoli (non circumferential)
! Apply extra layers to heel and forefoot for walking cast
! Don’t compress proximal fibular head ! Cut cast around toes, expose MTP joints

9/22/14
18
! Steady hand with index finger or thumb on cast
! Use multiple short cuts ! Don’t leave in same place too long (seconds) ! Push down until feel “give”