march 5th, 2007 mcb 135k discussion lecture 14- 16, 18
Post on 21-Dec-2015
222 views
TRANSCRIPT

March 5th, 2007
MCB 135k Discussion Lecture 14- 16, 18
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Neurons that can proliferate into adulthood include:
• Neuroblasts in the subventricular zone (SVZ) and subgranular layer which migrate towards the olfactory bulb and hippocampus respectively
• Dormant Neuroprogentior cells • Neuroglia
The rate of degeneration far exceeds the ability of these cells to compensate for neuronal loss
Research seeking to activate/increase proliferation of these cells to regenerate lost brain tissue (neural stem cells) in neurodegenerative diseases
Major Function of the Nervous SystemMajor Function of the Nervous System
The major function of the CNS is to The major function of the CNS is to communicate & to connect:communicate & to connect:
•with other CNS cellswith other CNS cells
•with peripheral tissues (outside CNS)with peripheral tissues (outside CNS)
•with the external environment (including physical and social with the external environment (including physical and social environments)environments)
This communication regulates:This communication regulates:•MobilityMobility•Sensory informationSensory information•Cognition Cognition •Affect and moodAffect and mood•Functions of whole-body systemsFunctions of whole-body systems

Neurons:
Axons- transmit signal, only one per cell
Dendrites- receive signal, numerous projections per cell
Glial Cells:
Astrocyte- structural/nutritional support for neurons
Oligodendrocyte- sheath axons, allow for faster action potential transmittance- protective roles
Microglia- neuronal immune cells
• In normal aging, moderate neuronal loss occurs in the:
Locus Ceruleus: nucleus in the brain stem (inferior to the cerebellum in the caudal midbrain/rostral pons) apparently responsible for the physiological reactions involved in stress and panic. This nucleus is the major location of neurons that release norepinephrine throughout the brain. Implicated in wide ranging disorders: depression, panic, anxiety disorders, Posttraumatic stress disorder
Substantia Nigra: A dark band of gray matter deep within the brain where cells manufacture the neurotransmitter dopamine for movement control. Degeneration of cells in this region may lead to a neurologic movement disorder such as Parkinson's disease
Nucleus basalis of meynert:Lateral part of the tuber cinereum that provides most of the acetylcholine to the cerebral cortex. Decrease in production seen in Alzheimer’s disease and Lewy Body dimentia.
Hippocampus: The part of the brain that assists in storing memory by sorting and sending new bits of information to be stored in appropriate sections of your brain and recalling them when necessary

Major functional deficits/ pathologies involve:
Motility (e.g. Parkinson’s Disease)
Senses and communication
Cognition (e.g. dementias)
Affect and mood (e.g. depression)
Blood circulation (stroke, multi-infarct dementia)

Pathological and Cellular Pathological and Cellular Changes with Normal AgingChanges with Normal Aging
Pathological and Cellular Pathological and Cellular Changes with Normal AgingChanges with Normal Aging
• Increased intracellular deposits of lipofuscinIncreased intracellular deposits of lipofuscin• Intracellular formation of PHFsIntracellular formation of PHFs• Accumulation of amyloid deposits in the neuritic Accumulation of amyloid deposits in the neuritic
plaques and surrounding the cerebral blood vesselsplaques and surrounding the cerebral blood vessels• Accumulation of Lewy bodiesAccumulation of Lewy bodies• Cell death (apoptosis, necrosis)Cell death (apoptosis, necrosis)
• Increased intracellular deposits of lipofuscinIncreased intracellular deposits of lipofuscin• Intracellular formation of PHFsIntracellular formation of PHFs• Accumulation of amyloid deposits in the neuritic Accumulation of amyloid deposits in the neuritic
plaques and surrounding the cerebral blood vesselsplaques and surrounding the cerebral blood vessels• Accumulation of Lewy bodiesAccumulation of Lewy bodies• Cell death (apoptosis, necrosis)Cell death (apoptosis, necrosis)

Key terms:
Lipofuscin: Lipofuscin are brown pigment granules representing lipid-containing residues of lysosomal digestion and considered one of the aging or "wear and tear" pigments; found in the liver, kidney, heart muscle, adrenals, nerve cells, and ganglion cells.
PHF: Paired helical filaments (PHF) are abnormal, approximately 20-25-nm wide periodically twisted filaments,
which accumulate in Alzheimer's disease (AD) brain and other neurodegenerative disorders, including corticobasal degeneration (CBD). PHF are primarily composed of highly phosphorylated tau protein,
proteins that interact with and stabilize microtubules, promote tubulin assembly (MAP).
Amyloid:insoluble fibrous protein aggregations sharing specific structural traits (cross-beta quaternary structure) commonly found in Alzheimer’s disease. Main constituent of amyloid plaques are Abeta (Amyloid beta)proteins, formed after cleavage of amyloid prescursor protein (APP). Autosomal-dominant mutations can cause early onset AD.
Lewy Body: abnormal aggregates of protein that develop inside nerve cells. A Lewy body is composed of the protein alpha-synuclein associated with other proteins such as ubiquitin, neurofilament protein, and alpha B crystallin. Linked to Parkinson’s disease.
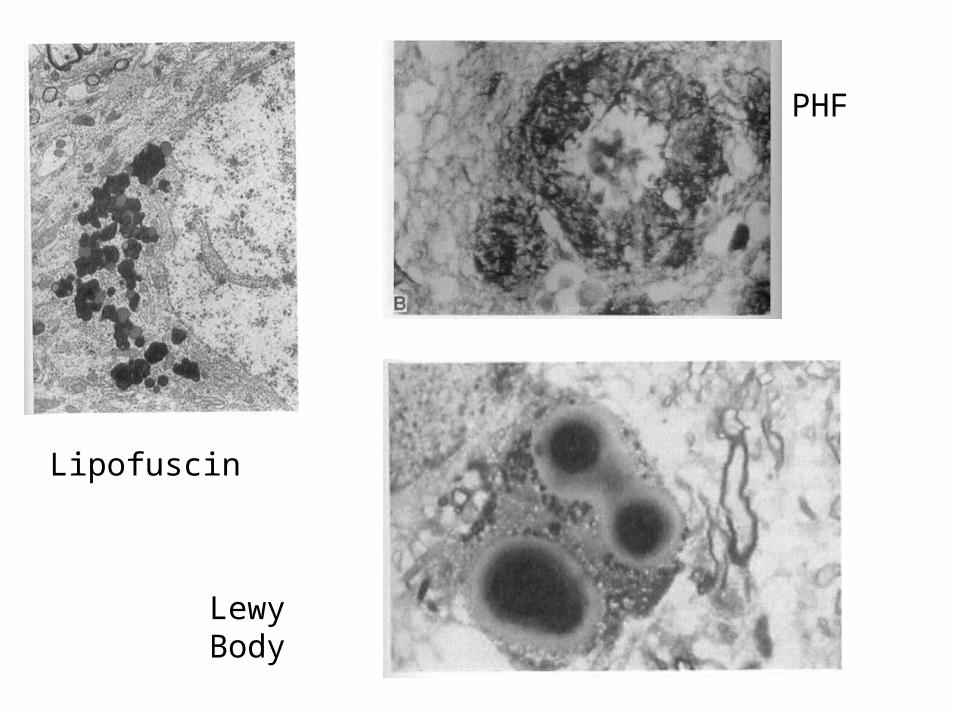
Lipofuscin
PHF
Lewy Body

Short video on Parkinson’s Disease and GDNF therapy:http://www.youtube.com/watch?v=gnDHMveS9_M
Parkinson’s Disease:
Parkinson's disease (also known as Parkinson disease or PD) is a degenerative disorder of the central nervous system that often impairs the sufferer's motor skills and speech
Symptoms:
•Tremor
•Rigidity
•Bradykinesia/akinesia: respectively, slowness or absence of movement
•Postural Instability
•Gait abnormalities
•Fatigue
•Soft speech/Drooling

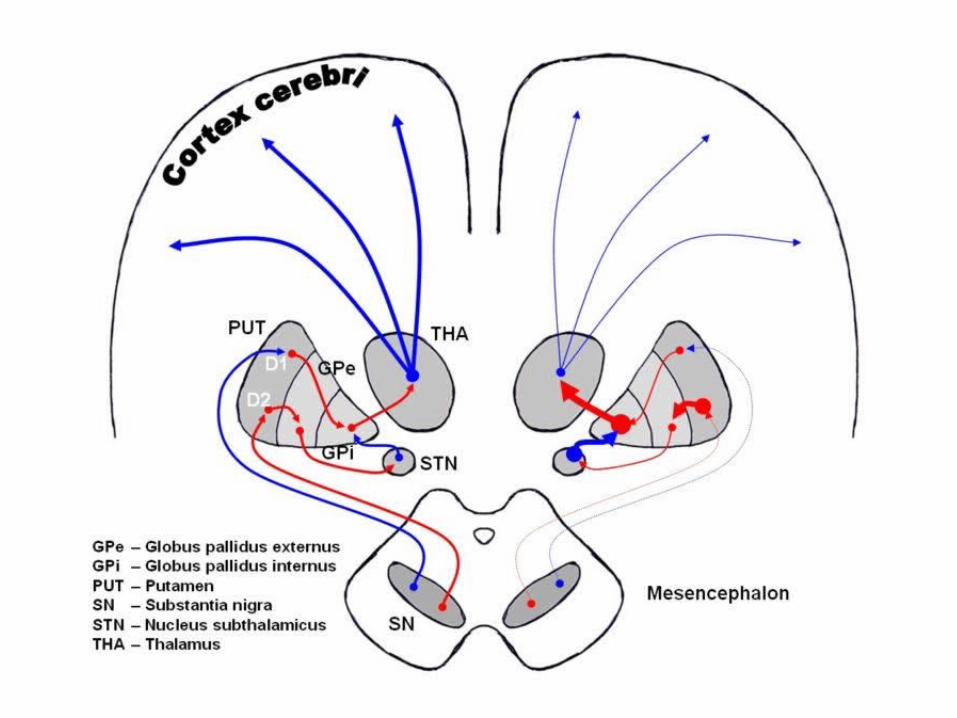
•Results from the loss of pigmented dopamine-secreting (dopaminergic) cells
•Neurons project to the striatum and their loss leads to alterations in the activity of the neural circuits within the basal ganglia that regulate movement, in essence an inhibition of the direct pathway and excitation of the indirect pathway.
•The direct pathway facilitates movement and the indirect pathway inhibits movement, thus the loss of these cells leads to a hypokinetic movement disorder.
•The lack of dopamine results in increased inhibition of the ventral lateral nucleus of the thalamus, which sends excitatory projections to the motor cortex, thus leading to hypokinesia.
•The mechanism by which the brain cells in Parkinson's are lost may consist of an abnormal accumulation of the protein alpha-synuclein bound to ubiquitin in the damaged cells. The alpha-synuclein-ubiquitin complex cannot be directed to the proteosome. This protein accumulation forms proteinaceous cytoplasmic inclusions called Lewy bodies.

Alzheimer's disease (AD), also known simply as Alzheimer's, is a neurodegenerative disease characterized by progressive cognitive deterioration together with declining activities of daily living and neuropsychiatric symptoms or behavioral changes. It is the most common type of dementia. The ultimate cause of the disease is unknown
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

Three major competing hypotheses exist:
"cholinergic hypothesis" and suggests that AD begins as a deficiency in the production of the neurotransmitter acetylcholine
tau protein abnormalities initiate the disease cascade, supported by the long-standing observation that deposition of amyloid plaques do not correlate well with neuron loss
beta amyloid deposits are the causative factor in the disease - cytotoxicity of mature aggregated amyloid fibrils, which are believed to be the toxic form of the protein responsible for disrupting the cell's calcium ion homeostasis and thus inducing apoptosis


OLD
YOUNG
0
200
400
600
800
Rea
ctio
n T
ime
(mse
c)2 Letters 6 Letters
FAST ---------------------> SLOW
Neural recruitment
Information processing speed
LESS ---------------------> MORE

Memory Load2 6 2 6
500
750
1000
1250
1500
Young Old
Reaction Time (msec)

YOUNG ELDERLYUNDER
RECRUITMENTOVER
RECRUITMENT
YOUNG
OLD
NON-SELECTIVE RECRUITMENT

FASTEST SLOWEST
YOUNG
OLD

ApoptosisProgrammed Cell Death - executed in such a way as to
safely dispose of cell corpses and fragments.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
•Evolutionarily conserved
•Occurs in all multicellular animals studies (plants too!)
•Stages and genes conserved from nematodes (worms)and flies to mice and humans
•Important in embryogenesis
•Selection/ Eliminates non-functional cells
•Immunity-eliminates dangerous cells
•Organ size - eliminates excess cells
•Tissue remodeling - mammary gland/ prostate
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.QuickTime™ and a
TIFF (Uncompressed) decompressorare needed to see this picture.
Lack of proper apoptosis during development can lead to fused toes / fingers
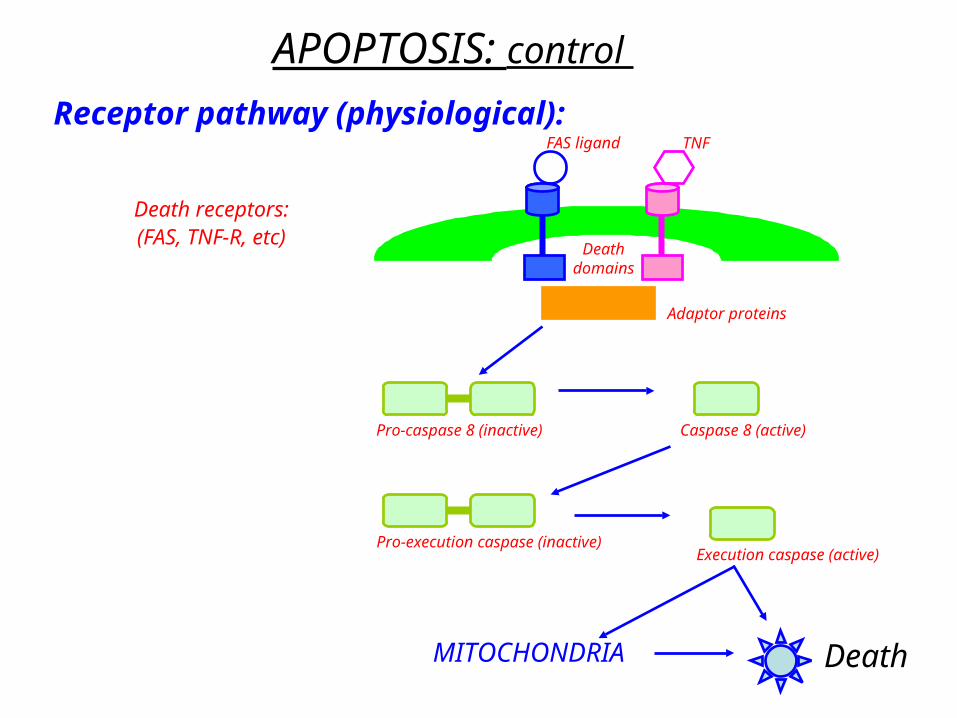
APOPTOSIS: control
Receptor pathway (physiological):
Death receptors:(FAS, TNF-R, etc)
FAS ligand TNF
Deathdomains
Adaptor proteins
Pro-caspase 8 (inactive) Caspase 8 (active)
Pro-execution caspase (inactive)Execution caspase (active)
DeathMITOCHONDRIA
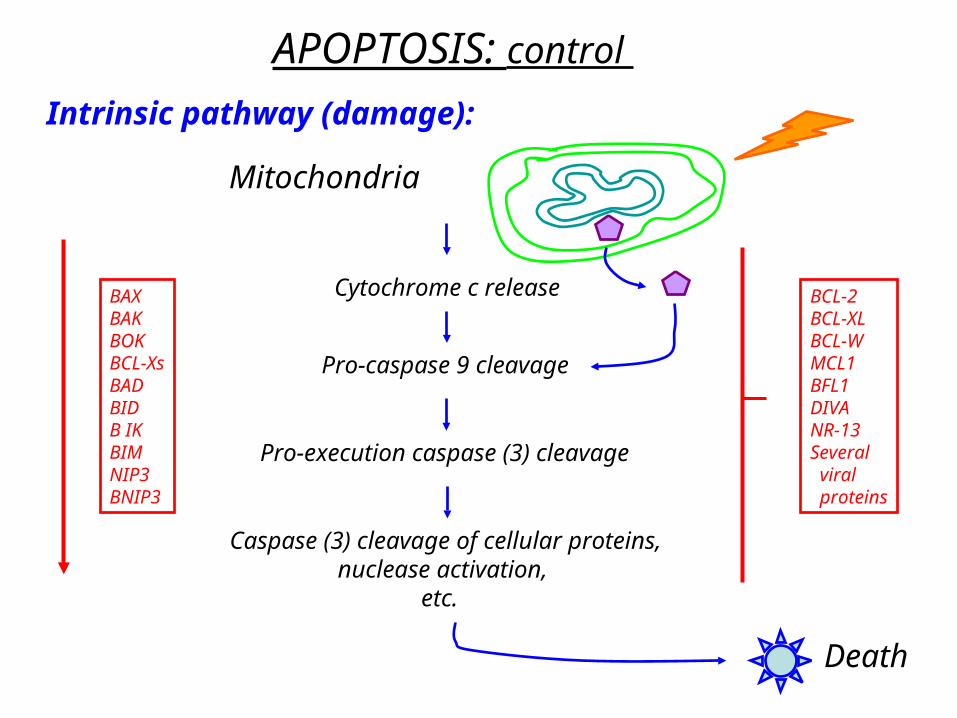
APOPTOSIS: control
Intrinsic pathway (damage):
Mitochondria
Cytochrome c release
Pro-caspase 9 cleavage
Pro-execution caspase (3) cleavage
Caspase (3) cleavage of cellular proteins,nuclease activation,
etc.
Death
BAXBAKBOKBCL-XsBADBIDB IKBIMNIP3BNIP3
BCL-2BCL-XLBCL-WMCL1BFL1DIVANR-13Several viral proteins

APOPTOSIS: control
Physiological Intrinsicreceptor pathway damage pathway
MITOCHONDRIAL SIGNALS
Caspase cleavage cascade
Orderly cleavage of proteins and DNA
CROSSLINKING OF CELL CORPSES; ENGULFMENT(no inflammation)

APOPTOSIS: Role in Disease
TOO MUCH: Tissue atrophy
TOO LITTLE: Hyperplasia
NeurodegenerationThin skin
etc
CancerAthersclerosis
etc

APOPTOSIS: Role in DiseaseAGING
Aging --> both too much and too little apoptosis(evidence for both)
Too much (accumulated oxidative damage?)---> tissue degeneration
Too little (defective sensors, signals?---> dysfunctional cells accumulatehyperplasia (precancerous lesions)
Discussion questions:
What are the function of glial cells in the nervous system?
What are the similarities and differences between Parkinson’s disease and Alzheimer’s diseases?
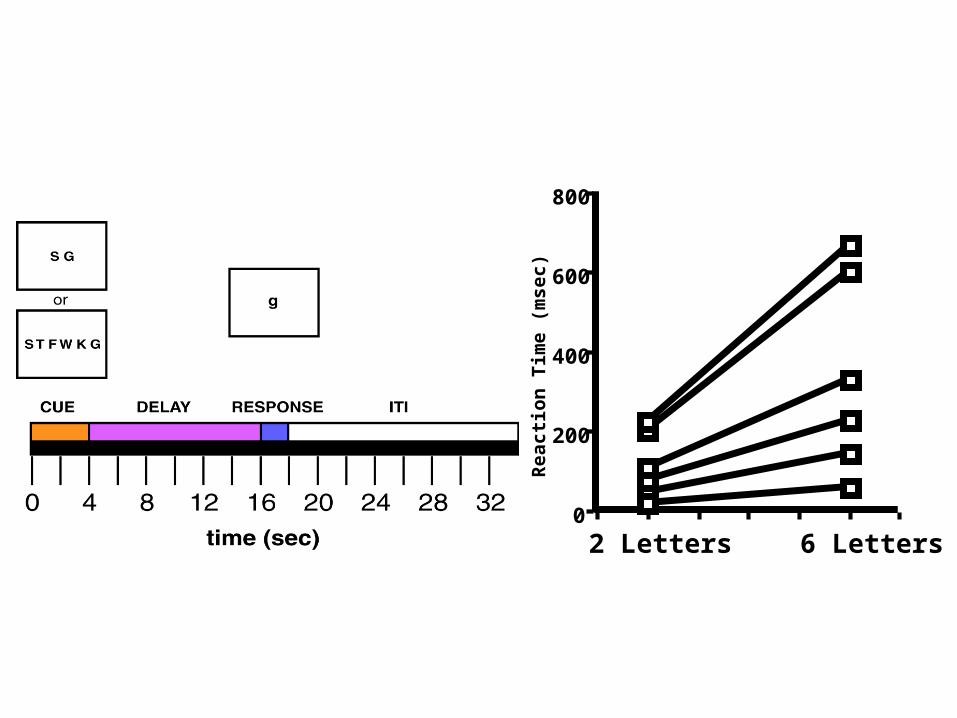
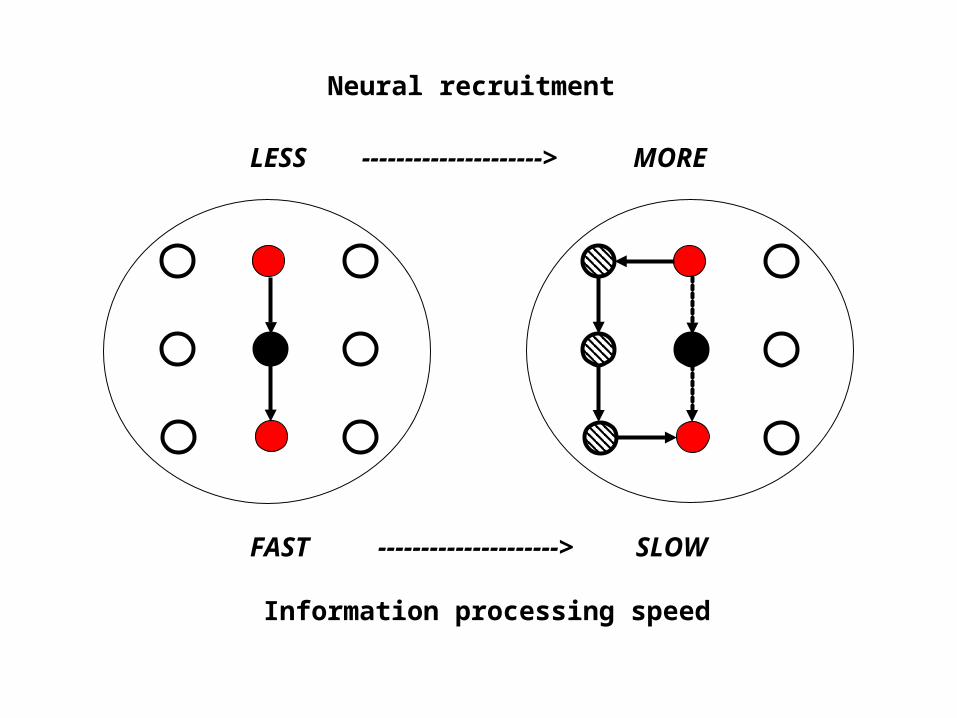
What does fMRI data reveal about memory tasks in old versus young individuals?
What roles does apoptosis have in disease? How can apoptosis be characterized as an example of antagonistic pleiotropy?