march 2018 nursing commission regular meeting€¦ · c. substance use disorder...
TRANSCRIPT

Nursing Care Quality Assurance Commission (NCQAC) Retreat Agenda
Thursday, July 12 2018 8:30 AM- 5:00 PM
Red Lion Inn- Hanford House 802 Washington Way Richland, WA 99352
DIRECTIONS
Commission Members: Tracy Rude, LPN, Chair Mary Baroni, PhD, RN, Vice-Chair Lois Hoell, MS, MBA, RN, Secretary/Treasurer Gerianne Babbo, EdD, RN Adam Canary, LPN Jeannie Eylar, MSN, RN Edie Higby, Public Member Helen Myrick, Public Member Sharon Ness, RN Donna L. Poole MSN, ARNP, PMHCNS-BC Tiffany Randich, LPN Renee Ruiz, Public Member Laurie Soine PhD, ARNP
Yvonne Strader, RN Vacant, RN
Assistant Attorney General: Gail S. Yu, Assistant Attorney General
Staff: Paula R. Meyer, MSN, RN, FRE, Executive Director Kathy Anderson, Financial Manager Chris Archuleta, Management Analyst Amber Bielaski, Policy and Performance Analyst Debbie Carlson, MSN, RN, CPM Associate Director,
Nursing Practice & Licensing Teresa Corrado, LPN, CPM Licensing Manager John Furman, PhD, MSN, CIC, COHN-S, Director, Washington Health Professional Services (WHPS) Karl Hoehn, Legal Manager Grant Hulteen, Chief Investigator Rozanne McCarty, BS, MS, Health Services Consultant Mindy Schaffner, PhD, MSN-CNS, RN, Associate
Director, Nursing Education & Research Catherine Woodard, Associate Director, Discipline
NCQAC Business Meeting July 12-13, 2018
1

If you have questions regarding the agenda, please call the Nursing Care Quality Assurance Commission (NCQAC) office at 360-236-4713. Agenda items may be presented in a different order. If you wish to attend the meeting for a single item, contact our office at the number listed above and request a specific time scheduled for that item. If you have limited English language expertise call 360-236-4713 before July 3, 2018.
This meeting is accessible to persons with disabilities. Special aids and services can be made available upon advance request. Advance request for special aids and services must be made no later than July 3, 2018. If you need assistance with special needs and services, please leave a message with your request at 1-800-525-0127 or, if calling from outside Washington State, call 360-236-4052. TDD may also be accessed by calling the TDD relay service at 711. If you need assistance due to a speech disability, Speech-to-Speech provides human voicers for people with difficulty being understood. The Washington State Speech to Speech toll free access number is 1-877-833-6341.
If attending remotely, please mute your connection in order to minimize background noise during the meeting.
Smoking and vaping are prohibited at this meeting.
I. 8:30 AM - 9:00 AM Call to Order -Tracy Rude, Chair
A. Introduction of NCQAC and pro tem members B. Order of Agenda
II. 9:00 AM – 10:30 AM Disciplinary workload analysis – Chris Archuleta, Catherine
Woodard, Karl Hoehn, Grant Hulteen, Kathy Anderson – DISCUSSION/ACTION Each year, the NCQAC holds a retreat to allow time to review their work. At today’s retreat, the NCQAC receives information on an analysis of the disciplinary workload, trends, and recommendations for performance improvement. Resource considerations will be presented. At the end of the day, the NCQAC may consider recommendations for improvements. The recommendations may be forwarded to sub-committees or task forces. These groups may present items to the NCQAC in the future for discussion and actions.
10:30 – AM – 11:00 AM BREAK III. 11:00 AM – 12 NOON Disciplinary workload analysis, continued –
DISCUSSION/ACTION
12:00 PM – 1:00 PM Lunch IV. 1:00 PM – 2:00 PM Disciplinary workload analysis, continued–
DISCUSSION/ACTION 2:00 PM – 2:30 PM BREAK
NCQAC Business Meeting July 12-13, 2018
2

V. 2:30 PM – 3:00 PM Disciplinary workload analysis, continued– DISCUSSION/ACTION
VI. 3:00 – 4:00 Computer training for new members All current NCQAC and pro tem members who have had computer training are excused.
NCQAC Business Meeting July 12-13, 2018
3

NCQAC Business Meeting July 12-13, 2018
4

NCQAC Business Meeting July 12-13, 2018
5

NCQAC Business Meeting July 12-13, 2018
6

NCQAC Business Meeting July 12-13, 2018
7

NCQAC Business Meeting July 12-13, 2018
8

NCQAC Business Meeting July 12-13, 2018
9

NCQAC Business Meeting July 12-13, 2018
10

NCQAC Business Meeting July 12-13, 2018
11

NCQAC Business Meeting July 12-13, 2018
12

NCQAC Business Meeting July 12-13, 2018
13

NCQAC Business Meeting July 12-13, 2018
14

NCQAC Business Meeting July 12-13, 2018
15

NCQAC Business Meeting July 12-13, 2018
16

NCQAC Business Meeting July 12-13, 2018
17

Nursing Care Quality Assurance Commission (NCQAC)
Meeting Agenda Friday, July 13, 2018 8:30 AM- 5:00 PM
Red Lion Inn- Hanford House 802 Washington Way Richland, WA 99352
DIRECTIONS To attend via webinar, please register for the meeting at:
https://attendee.gotowebinar.com/register/1962534088672720131
Commission Members: Tracy Rude, LPN, Chair Mary Baroni, PhD, RN, Vice-Chair Lois Hoell, MS, MBA, RN, Secretary/Treasurer Gerianne Babbo, EdD, RN Adam Canary, LPN Jeannie Eylar, MSN, RN Edie Higby, Public Member Helen Myrick, Public Member Sharon Ness, RN Donna L. Poole MSN, ARNP, PMHCNS-BC Tiffany Randich, LPN Renee Ruiz, Public Member Laurie Soine PhD, ARNP Yvonne Strader, RN Vacant, RN Assistant Attorney General: Gail S. Yu, Assistant Attorney General
Staff: Paula R. Meyer, MSN, RN, FRE, Executive Director
Kathy Anderson, Financial Manager Chris Archuleta, Management Analyst Amber Bielaski, Policy and Performance Analyst Debbie Carlson, MSN, RN, CPM Associate Director, Nursing
Practice & Licensing Teresa Corrado, LPN, CPM Licensing Manager John Furman, PhD, MSN, CIC, COHN-S, Director, Washington Health Professional Services (WHPS) Karl Hoehn, Legal Manager Grant Hulteen, Chief Investigator Rozanne McCarty, BS, MS, Health Services Consultant Mindy Schaffner, PhD, MSN-CNS, RN, Associate Director,
Nursing Education & Research Tim Talkington, Staff Attorney Catherine Woodard, Associate Director, Discipline
NCQAC Business Meeting July 12-13, 2018
18

If you have questions regarding the agenda, please call the Nursing Care Quality Assurance Commission (NCQAC) office at 360-236-4713. Agenda items may be presented in a different order. If you wish to attend the meeting for a single item, contact our office at the number listed above and request a specific time scheduled for that item. If you have limited English language expertise call 360-236-4713 before July 3, 2018.
This meeting is accessible to persons with disabilities. Special aids and services can be made available upon advance request. Advance request for special aids and services must be made no later than July 3, 2018. If you need assistance with special needs and services, please leave a message with your request at 1-800-525-0127 or, if calling from outside Washington State, call 360-236-4052. TDD may also be accessed by calling the TDD relay service at 711. If you need assistance due to a speech disability, Speech-to-Speech provides human voicers for people with difficulty being understood. The Washington State Speech to Speech toll free access number is 1-877-833-6341.
This meeting will be digitally recorded to assist in the production of accurate minutes. All recordings are public record. The minutes of this meeting will be posted on our website after they have been approved at the September 14, 2018 NCQAC meeting. For a copy of the actual recording, please contact the Public Disclosure Records Center (PDRC) at [email protected].
If attending remotely, please mute your connection in order to minimize background noise during the meeting.
Smoking and vaping are prohibited at this meeting.
I. 8:30 AM Opening – Tracy Rude, Chair – DISCUSSION/ACTION
Brad Haggard, Presentation of the flags
II. 8:45 AM New officers take their positions A. Tracy Rude, chair B. Mary Baroni, vice chair C. Lois Hoell, secretary/treasurer
III. 8:50 AM Call to Order
A. Introductions – any new members appointed by Governor Inslee introduced B. Order of the Agenda C. Correspondence D. Announcements
IV. 8:50 AM Consent Agenda – DISCUSSION/ACTION
Items listed under the consent agenda are considered to be routine agency matters and approved by a single motion of the NCQAC without separate discussion. If separate
NCQAC Business Meeting July 12-13, 2018
19

discussion is desired, that item will be removed from the consent agenda and placed on the regular business agenda.
A. Approval of Minutes
1. NCQAC Business Meeting, May 11, 2018 2. Advanced Practice Subcommittee
a. March 21, 2018 b. April 18, 2018
3. Discipline Subcommittee a. April 24, 2018
4. Licensing Subcommittee a. April 28, 2018 b. May 18, 2018
B. Out-of-State Travel Reports 1. National Organization of Alternative Programs, March 26-30, New
Orleans, LA: Yvonne Strader 2. National Council of State Boards of Nursing (NCSBN) IT/Operations
Conference, May 15-16, Albuquerque, NM: Chris Archuleta 3. NCSBN Discipline Case Management Summit, June 6-8, Denver, CO:
Tracy Rude, Grant Hulteen C. Letter from Kathy Thomas, president, National Council of State Boards of
Nursing, May 2018
V. 8:55 AM – 9:00 AM NCQAC Panel Decisions – DISCUSSION
The NCQAC delegates the authority as provided by law for certain decision to a panel of at least three members. A member of the NCQAC must chair panels. Pro tem members of NCQAC may serve as panel members. The following reports are provided for information.
A. Nursing Program Approval Panel (NPAP) B. Nursing Assistant Program Approval Panel (NAPAP)
VI. 9:00 AM – 9:45 AM Chair Report – Tracy Rude – DISCUSSION/ACTION
A. Subcommittee chair and member appointments B. Legislative Panel members: the panel members are usually appointed at the November
meeting. Due to the need to review anticipated legislative changes to the HIV/AIDS chapter, the legislative panel requests early appointments.
C. National Council of State Boards of Nursing (NCSBN) annual meeting, August 15-17, Minneapolis MN
1. Attending meeting: Tracy Rude, Lois Hoell, Mary Baroni, Paula Meyer, Karl Hoehn, Suellyn Masek (award reception), Kathy Moisio
2. Delegates: Tracy Rude, Paula Meyer 3. NCSBN Board of Director recommendations: NCQAC discusses the
recommendations and may give the delegates direction on voting 4. Slate of candidates
D. Operating Agreement annual review: The NCQAC delegated to the officers the work on the Operating Agreement. The officers will report back to NCQAC on the annual review.
NCQAC Business Meeting July 12-13, 2018
20

E. 2018-2019 Educational schedule: The NCQAC decided to have working lunches and an educational presentation during this time at every meeting. The plan for the upcoming year is presented.
VII. 9:45 AM – 10:30 AM Executive Director Report – Paula Meyer – DISCUSSION/ACTION
A. Budget Report – Kathy Anderson B. Performance Measures Report
1. NCQAC 2. Education 3. Legal 4. WHPS
C. Rules Report – Amber Bielaski D. Electronic signatures – Procedures H15 & A54
Each year, the NCQAC members approve the use of their electronic signatures and the process to protect their signatures.
E. 2017 - 2018 Board Pay Summary Each July meeting, a summary of categories of board pay is presented.
F. 2018 - 2019 proposed meeting dates and locations The NCQAC schedules their upcoming meeting dates and locations through June 2019. The dates and locations are then filed with the Washington State Code Reviser Office.
G. License Fee Surcharge and Nursing Resource Center: contract with Washington Center for Nursing – Paula Meyer- DISCUSSION/ACTION In 2005, the legislature placed a $5.00 surcharge on all LPN and RN initial and renewal licenses. The proceeds from the surcharge are used to provide grants to a central nursing resource center. Ms. Meyer provides an update on recent contract negotiations and use of grant funds for this next biennium.
10:30 AM – 10:45 AM Break VIII. 10:45 AM – 11:30 AM Subcommittee Report – DISCUSSION/ACTION
A. Advanced Practice – Laurie Soine, Chair
1. Acupuncture education for ARNPS: plan to work with representatives from the East Asian Medicine Advisory Committee and WA East Asian Medicine Association
B. Consistent Standards of Practice C. Discipline – Adam Canary, Chair D. Licensing – Jeannie Eylar, Chair E. Research – Mary Baroni, Chair
1. Research Sub-committee position description 11:30 AM – 1:00 PM Lunch
IX. 12:00 PM – 1:00 PM Education Session – Disciplinary Process, the Big Picture – Tim
Talkington
NCQAC Business Meeting July 12-13, 2018
21

The July 12 retreat concentrated on data analysis, trends, and performance improvement recommendations for the disciplinary process. Today’s presentation reviews the current disciplinary process from complaint intake through compliance and reinstatement. The presentation includes the regulations directing the process.
X. 1:00 PM – 1:15 PM Open Microphone
Open microphone is for public presentation of issues to the NCQAC. If the public has issues regarding disciplinary cases, please call 360-236-4713.
XI. 1:15 PM – 2:00 PM Prescription Monitoring Program – Chris Baumgartner - DISCUSSION/ACTION At the May 11 NCQAC meeting, the NCQAC adopted a motion to write a letter to Governor Inslee encouraging Washington State to be a member of a national prescription monitoring data base. Mr. Baumgartner will update the NCQAC on efforts for Washington to be included in interstate data sharing. Mr. Baumgartner will also provide an update on the Prescription Monitoring Program.
XII. 2:00 PM – 2:30 PM – ESHB 1427 Opioid Prescribing Rules – Paula Meyer –
DISCUSSION/ACTION ESHB 1427, now law, directs the NCQAC, Medical Commission, Dental Commission, State Board of Osteopathic Medicine and Surgery and the Board of Podiatry to adopt rules on prescribing opioids. The NCQAC drafted and presented rules at the May meeting. Constituent comments identified concerns with some of the draft language and will be presented to the NCQAC. The anticipated hearing date for the rules is August 10. The NCQAC may consider modifying language and the date of the hearing.
2:30 PM – 2:45 PM BREAK
XIII. 2:45 PM – 3:45 PM Education Report–Mindy Schaffner DISCUSSION/ACTION A. Higher Education Complaint Portal
The NCQAC receives an update on the Washington Student Achievement Council’s work regarding a joint complaint portal for state agencies that approve educational programs, including the nursing commission.
B. Action Now! and New Brief The Action Now! Coalition created a Brief paper that describes the issues facing nursing education and identifies solutions to address these issues. NCQAC receives an update on the work of the Coalition and the plans for the Solution Summit on October 18th at the Doubletree Hotel in Tukwila.
C. Update on the LTC Committee work The 2018 legislature passed a budget proviso requiring an assessment and evaluation of nursing workforce issues in Long Term Care Settings. The NCQAC receives an update on the meetings scheduled and topics to be included in the meetings.
D. NCSBN Safe Student Report Study The NCQAC receives a report on the newly created incident reporting system created by NCSBN. Nursing programs are encouraged to report student incidents using this national
NCQAC Business Meeting July 12-13, 2018
22

data base. Researchers utilize the data to analyze student incidents throughout the United States. Since September 21, 2016, the NCQAC collects reports of incidents that involve harm, unreasonable risk of harm, or allegations of diversion.
E. Annual Nursing Education Report -- Mary Sue Gorski Each year, the NCQAC produces the education report. The education report gathers and analyzes information submitted by nursing education programs. The NCQAC considers adoption of the annual report.
XIV. 3:45 PM Meeting Evaluation XV. 4:00 PM Closing
NCQAC Business Meeting July 12-13, 2018
23

Nursing Care Quality Assurance Commission (NCQAC)
Friday, May 11, 2018 8:30 AM – 5:00 PM
Department of Health Point Plaza East, Room 152/153
310 Israel Road SE Tumwater, WA 98501
This meeting was held by webinar. To view the webinar recording, please click here:
https://attendee.gotowebinar.com/register/1311492362329431555 Commission Members: Tracy Rude, LPN, Chair Donna L. Poole MSN, ARNP, PMHCNS-BC, Vice-Chair Lois Hoell, MS, MBA, RN, Secretary/Treasurer Gerianne Babbo, EdD, RN Mary Baroni, PhD, RN Adam Canary, LPN Jeannie Eylar, MSN, RN Edie Higby, Public Member Suellyn M. Masek, MSN, RN, CNOR Helen Myrick, Public Member Sharon Ness, RN Tiffany Randich, LPN Renee Ruiz, Public Member Laurie Soine PhD, ARNP Yvonne Strader, RN Assistant Attorney General: Gail S. Yu, Assistant Attorney General
Staff: Paula R. Meyer, MSN, RN, FRE, Executive Director (Excused)
Kathy Anderson, Financial Manager Chris Archuleta, Management Analyst Amber Bielaski, Policy and Performance Analyst Debbie Carlson, MSN, RN, CPM, Associate Director, Nursing
Practice & Licensing Teresa Corrado, LPN, CPM, Licensing Manager Kristen Durborough, Practice Assistant John Furman, PhD, MSN, CIC, COHN-S, Director, Washington Health Professional Services (WHPS) Mary Sue Gorski, PhD, RN, Research and Policy Analyst Karl Hoehn, Legal Manager (Excused) Grant Hulteen, Chief Investigator Rozanne McCarty, BS, MS, Health Services Consultant Kathy Moisio, PhD, RN, Nursing Education Consultant Mindy Schaffner, PhD, MSN-CNS, RN, Associate Director of
Nursing Education Catherine Woodard, Associate Director, Discipline
NCQAC Business Meeting July 12-13, 2018
24

This meeting was digitally recorded. All recordings are public record. The minutes of this meeting will be posted on our website after they have been approved at the July 13, 2018 NCQAC meeting. For a copy of the actual recording, please contact the Public Disclosure Records Center (PDRC) at [email protected].
I. Opening – Tracy Rude, Chair – DISCUSSION/ACTION
II. Call to Order: was called to order at 8:30 AM
Ms. Rude thanked everyone for coming to the meeting and acknowledged nurses week. Ms. Rude thanked all nurses for the work they do.
A. Introductions – Tracy Rude B. Order of the Agenda - Accepted C. Correspondence – Nothing to report at this time. D. Announcements – Tracy Rude
1. NCSBN Award Winners: Suellyn Masek and Lois Hoell 2. Staff Award: Karl Hoehn 3. New Staff: Catherine Woodard introduced new staff
a. Jocelyn King – Investigator b. Tara Serrano – Investigator c. Bryan Medina – Legal Assistant
III. Consent Agenda – DISCUSSION/ACTION
Consent Agenda items are considered routine and are approved with one single motion
A. Approval of Minutes 1. NCQAC Business Meeting: March 9, 2018 2. NCQAC Special Business Meeting: April 11, 2018 3. Advanced Practice Sub-committee
a. December 20, 2017 b. February 21, 2018
4. Consistent Standards of Practice Sub-committee a. February 7, 2018 b. April 11, 2018
5. Discipline Sub-committee a. January 23, 2018 b. February 27, 2018
6. Licensing Sub-Committee: January 26, 2018 B. Out-of-State Travel Reports
1. National Council of State Boards of Nursing (NCSBN) Midyear Meeting, March 5-7, Chicago: Tracy Rude, Lois Hoell, Mary Baroni, Paula Meyer
2. National Organization of Alternative Programs, March 26-30, New Orleans, LA: John Furman, Lori Linenberger, Yvonne Strader
3. APRN Roundtable, April 10, Rosemont IL: Donna Poole, Laurie Soine, Mary Sue Gorski
C. Substance Use Disorder Conference-Debriefing Report 1. Substance Use Disorder Debrief
D. Letter from NCSBN President Kathy Thomas
NCQAC Business Meeting July 12-13, 2018
25

IV. NCQAC Panel Decisions – DISCUSSION
The NCQAC delegates the authority as provided by law for certain decision to a panel of at least three members. A member of the NCQAC must chair panels. Pro tem members of NCQAC may serve as panel members. The following reports are provided for information.
A. Nursing Program Approval Panel (NPAP) – February 1 & 8, 2018; March 1 &
8, 2018 and April 5, 2018 B. Nursing Assistant Program Approval Panel (NAPAP) – February 12, 2018;
March 12, 2018 and April 9, 2018 No discussion occurred.
MOTION: Moved by Ms. Ness with a second Dr. Baroni to accept the consent agenda. Motion carried.
V. Chair Report – Tracy Rude – DISCUSSION/ACTION
A. Recognition of NCQAC and Pro Tem members completing their terms of
service 1. Suellyn Masek 2. Erica Benson-Hallock 3. Lin Murphy 4. Daniel Simonson
The following Pro Tem members will not be returning next year: 1. Teri Trillo 2. Debbie Conner
B. Out of State Travel Plan 1. June 6, 2018 – NCSBN Case management summit. The following attending:
a. Ms. Hoell b. Ms. Rude c. Mr. Hulteen d. Ms. Woodard
C. NCSBN Annual Meeting, August 15 – 17, Minneapolis: Chair and Executive Director as Delegates The following will be in attendance:
1. Ms. Meyer 2. Ms. Rude 3. Dr. Baroni 4. Ms. Hoell 5. Mr. Hoehn
D. NCQAC Annual Award Nomination(s): Kathy Moisio – Discussed in Announcements (Karl Hoehn)
E. NCQAC Annual Evaluation: Tiffany Randich, Edie Higby The annual evaluation included positive feedback, honest evaluation of concerns and constructive feedback. NPAP satisfaction increased from 84% last year to 96% this year. 93% of NCQAC members completed the survey and 18.75% of Pro Tems completed the survey. NCQAC’s goal is 100% participation on survey next year. The NCQAC thought the format of the survey was spectacular which made it very easy to complete.
NCQAC Business Meeting July 12-13, 2018
26

VI. Executive Director Report – Paula Meyer – DISCUSSION/ACTION Catherine Woodard provides the executive director report.
A. Budget Report: Kathy Anderson Latest budget report through March demonstrates little change. Fees increased and revenue increased. NCQAC is 5% underspent (last year 10-12% underspend). We have a few staff members on extended personnel leave and upcoming retirements. Overall budget is healthy. Discussed Health Systems Quality Assurance fund. NCQAC portion remains healthy, but overall, the HSQA fund is low. Ms. Hoell presented current RN and ARNP numbers in Washington State. Number of RN licensees increased 3% from last year, and ARNP’s increased 8% from last year. Inactive licenses increased as well. Concerns remain with a decrease in the number of people taking the NCLEX nationally. NCQAC members raised a question of age distribution data and projected enrollment in nursing schools. Dr. Moisio reported that we are projected to complete that analysis in August. Dr. Schaffner informed NCQAC that projected nursing school enrollment will be discussed at July meeting with the annual nursing education report. She went on to say that the enrollment of nursing schools is concerning and relates to lack of faculty.
B. Performance Measures Report
1. NCQAC 2. Education 3. Legal 4. WHPS
Ms. Woodard informed the NCQAC that information is different from last meetings. At the last couple meetings chart dates were updated, but the data was not. The numbers are now correct. An increase in the number of complaints play a role in the decreased performance levels. At the July retreat, there will be more detailed discussion around performance.
Ms. Rude added that performance measures also reflect on the NCQAC members. There is a responsibility we have to stay on task with our cases, and meet timelines. Ms. Hoell asked if a lot of the issue was getting reports from pain clinics. Mr. Hulteen stated there are two investigations finish. Ms. Hoell added that in nursing, acuity levels are used, and maybe there may be a way to apply this to the discipline cases. Ms. Woodard stated that system isn’t used in investigations, but Mr. Hoehn does break the more complex cases out. Each case is assigned a priority level. Ms. Anderson related this back to a decision package, giving tangible reasons why we may need to increase staff.
C. Suellyn Masek: serving as a NCQAC member and chair through the pilot project
(1103), presenting the 1518 report making permanent the enhanced authority, and negotiating an Operating Agreement – declined report in interest of time
D. 2019 Hearing Dates Have been posted, please sign up. E. NCQAC Business Meeting Noon Educational Presentation Topics Ms. Carlson – Options were presented to the NCQAC. Requested input from NCQAC
NCQAC Business Meeting July 12-13, 2018
27

1. Dr. Baroni – a. Multiple factors limiting our workforce, specifically in nursing educators. b. LPN issue in our state and nationally. Is it acceptable that LPNs are
decreasing? 2. Ms. Poole – What does the big picture of discipline look like?
F. Rules update – Amber Zawislak
1. Second emergency CR-101 filed for the implementation of rules addressing graduates of non-traditional nursing education programs. Workshops are being held.
2. Rules implementing ESHB 1427, Opioid Prescribing – Concluded task force and stakeholder work resulted in draft rules.
VII. Opioid Prescribing – Donna Poole - DISCUSSION/ACTION
A. ESHB 1427 draft rules
On April 11, the NCQAC held a special meeting to review the draft language implementing ESHB 1427 Opioid Prescribing. Ms. Poole presents the draft rules for any further comments. NCQAC anticipates a hearing on this set of rules at the September 14 meeting.
Ms. Poole– NCQAC held a special meeting on April 11th to review the draft rules and completed CR 101. Ms. Zawislak informed the NCQAC that once draft language is approved, NCQAC will file a CR 102. She also spoke about a letter received from Governor Jay Inslee requesting NCQAC move forward with an accelerated process. This would require a hearing by August requiring another special meeting. NCQAC discussed dates and locations for an August special meeting. NCQAC members requested the meeting be held closer to SeaTac to decrease travel costs for NCQAC members not local to Olympia. Possibility of having the hearing at the July NCQAC meeting was raised. A July hearing is unlikely due to the review process taking a couple months. The NCQAC will plan for an August special meeting.
Comments: Pg. 105: Louis Kaplan comments about exclusions (WAC 246-840-463). Pg. 106: Differentiating chronic from acute pain. Ms. Poole cautioned to avoid making changes that will make the rules different from other boards and commissions included in the task force. Dr. Baroni and Ms. Hoell agreed with the change.
MOTION: Moved by Dr. Baroni, with a second by Dr. Soine to adopt verbiage “that causes continuous or intermittent pain more than 12 weeks in duration lasting months or years.” Motion Carried. Pg. 107: Related to definition of hospice – not necessary for rules that exempts hospice anyway
No change. Pg. 107: Definition #10 of hospitals - should include eastern and western state hospitals. MOTION: Moved by Dr. Soine with a second by Ms. Masek to include statute for Eastern and Western State Hospitals. Motion carried.
NCQAC Business Meeting July 12-13, 2018
28

Pg. 108: Inpatient Definition: What about other treatment facilities, Residential treatment facilities, impatient rehab facilities, ambulatory surgical facility, and dental, and inpatient?
No reason to change the definition of inpatient. Change language in definition of Inpatient to: “A patient who has been hospitalized for more than 24 hours?”
Leave as is and research more in depth. Pg. 108: Operative procedures performed in day surgery and dental sites. These are dealt with under perioperative section. No change. Last comment on Pg. 108: Definition of “accepted conversion tables.” Change to “generally accepted tables or calculators” MOTION: Moved by Dr. Soine with a second by Ms. Ness to change to “generally accepted tables or calculators.” Motion carried. Pg. 110: use Washington State Prescription Monitoring Program
Dr. Baroni questioned if we are limited to WA Prescription Monitoring Program and when prescribers must query. Pg. 112: First issuance of opioid in this instance means from “that provider.” We should further clarify “by an individual prescriber.” This issue was discussed in April and NCQAC decided against a change. By keeping the wording the same may result in different interpretations.
MOTION: Moved by Dr. Baroni with a second by Dr. Soine to continue discussion of verbiage. Motion carried. MOTION: Dr. Baroni moved to withdraw her motion. Motion withdrawn. Pg. 114: Continuing Education requirement being four hours, differs from other Boards and commissions in the task force: “Continuing Education must be four hours in length.” MOTION: Moved by Dr. Soine with a second by Ms. Masek to end the sentence with period after the word length. Motion carried. Pg. 114: Comment regarding when the continuing education must be done. This is the first full cycle or the first cycle after January 2019. No change. Pg. 114: ICD card being updated No Change Pg. 114: Can this count for pharmacology. No Change Pg. 115: Comment- consider using “recommending or prescribing.”
NCQAC Business Meeting July 12-13, 2018
29

MOTION: Moved by Dr. Soine with a second by Dr. Baroni. Accept verbiage “recommending or prescribing.” Motion carried. Pg. 116: drugs of concern – There are drugs of concern listed. No Change Pg. 117: Includes “at a minimum.” Could clarify more, but not needed.
No change.
Pg. 117: subsection 6 – “typically” should be put in before “not indicated.” MOTION: Moved by Dr. Soine with a second by Dr. Baroni to add “typically” before “not indicated.” Motion carried. Pg. 119: subsection 4 “normal course of recovery” should be changed to “expected course of recovery.” MOTION: Moved by Dr. Soine with a second by Dr. Baroni to change “normal course of recovery” to “expected course of recovery.” Motion carried. Pg. 134: Comment about interpretation of this rule, but we don’t have authority to change chronic pain rules. No change. Pg. 135: subsection 2: suggestion to add “in addition to current WAC 246-840-493, add relevant WACS regarding other prescribing professions governed by ESHB 1427. MOTION: Moved by Dr. Soine with a second by Ms. Randich to add “in addition to current WAC 246-840-493, add relevant WACS regarding other prescribing professions governed by ESHB 1427. Motion carried. Pg. 138: Should it be two or four years for ARNPs. NCQAC can decide if it’s every two years, or change to four years.
No change. Pg. 138: subsection 3 delete “treatment center”, substitute “clinic.” Subsection 4 delete “setting”, substitute “clinic” MOTION: Moved by Dr. Soine, with a second from Dr. Baroni for subsection 3: change “treatment center” to “clinic,” and subsection 4: change “setting” to “clinic.” Motion Carried. Pg. 139: CRNAs as pain management specialists. Request to have their national certification added to the approved list so they can do a 120 MEQ consultation. No change. Pg. 140: Subsection 2: “ARNP shall consider tapering, changing, discontinuing treatment, getting a referral when patient requests a referral…”
No change. Pg. 144: New WAC 246-840-4960 about prescribing sleeping medications with opioids, z drugs. Comments that “z drugs” needs clarification.
NCQAC Business Meeting July 12-13, 2018
30

MOTION: Moved by Dr. Soine with a second by Ms. Strader to replace “sleeping medications” with “non-benzodiazepine hypnotics.” Motion withdrawn MOTION: Moved by Dr. Soine with a second by Ms. Strader to replace “sleeping medications” with “non-benzodiazepine hypnotics (z drugs).” Motion carried. Pg. 146: WAC 246-840-4990: Prescription Monitoring Program (PMP) registration, query and document. Subsection 2: Comment: “authorized designee” seems vague. “PMP WAC 246-470-050” Designee has to be a licensed healthcare practitioner since providers are the only people with access. MOTION: Moved by Dr. Soine moves with a second by Dr. Baroni to change to “authorized designee as defined in WAC 246-840-050.” Motion Carried. Pg. 146: subsection 3: At a minimum an ARNP shall ensure PMP query is done prior to prescribing an opioid, or drug listed on WAC 246-840-4960. NCQAC can only make requirements about opioids in this current rule. MOTION: Moved by Dr. Soine, with a second by Ms. Randich to delete “or of a medication listed in WAC 246-840-4960” In subsection 3. Motion carried. MOTION: Moved by Dr. Baroni with a second by Ms. Randich that NCQAC approves the opioid rule language as agreed to and amended today and as required as engrossed substitute house bill 1427 be filed with the code reviser as a CR-102. Motion carried.
B. Adding Gabapentin as a Prescription Monitoring Program (PMP) reportable drug Due to growing concerns of abuse of Gabapentin, the Pharmacy Quality Assurance Commission requests Gabapentin be added to the list of drugs reportable on the PMP. The NCQAC considers supporting the addition or concerns related to adding this drug to the list of reportable medications.
MOTION: Moved by Ms. Poole with a second by Dr. Baroni to send a letter to the Pharmacy Commission supporting the addition of Gabapentin to PMP as a recordable PMP drug per WAC 246-470-020. Three opposed, motion carried. Ms. Masek – Questions why are we not on the national PMP list? National prescribing data bases exist and it appears Washington State is not participating.
VIII. Sub-committee Report – DISCUSSION/ACTION
A. Advanced Practice – Laurie Soine, Chair
1. Dental anesthesia – Removed. Nothing to report. 2. Advanced Registered Nurse Practitioner degree requirements for CRNA.
Ms. Soine shared a statement from an April 18 discussion on licensing requirements for ARNPs through endorsement per WAC 246-840-342. The discussion focused on CRNA graduate degrees and whether or not their
NCQAC Business Meeting July 12-13, 2018
31

graduate degree must be from a school of nursing. Dr. Soine pointed out a lack of specificity in the rules that CRNAs need to obtain a graduate degree from a School of Nursing. The Advance Practice Subcommittee requested this document act as clarification that the rules be interpreted as written. Mrs. Yu noted the document stands for itself and clearly articulated the argument made by the applicant. Dr. Soine stated the intention that if CRNAs meet all four of the requirements, the applicant should not be hindered from obtaining credential:
a. An active RN and ARNP license from another jurisdiction without
restrictions or sanctions; b. A graduate degree from an advanced nursing education program that
is accredited by a national nursing accreditation body recognized by the U.S. Department of Education;
c. Certification from a national certifying body approved by the Commission; and,
d. Has been performing advanced clinical practice as a licensed ARNP for at least 250 hours within the previous two years.
The full statement is included with the minutes of the meeting.
Mr. Simonson asked if applicants need to provide additional documentation from educational programs. Mrs. Yu clarified that the NCQAC panel is permitted to ask for further documentation of education.
B. Consistent Standards of Practice – Suellyn Masek, Chair
1. Advisory Opinion Review – There are many old Advisory Opinions and some documents are ten to twenty years old. These documents are in need of revision or being rescinded by NCQAC. The subcommittee is currently working on advisory opinions and FAQs to address many of the topics. While the sub-committee recommends rescinding nine documents, the documents were not in packet. The documents with recommendations will be brought to July NCQAC meeting.
C. Discipline – Adam Canary, Chair
1. Supervision language in legal orders – a. The sub-committee is working on consistent language for orders
corresponding with legal definitions of direct, indirect, supervised supervision.
b. Previous language “has assessed patient’ to be replaced with “supervisor needs to know any restrictions on license.”
2. Procedure A27 Sanction Standards for Continuing Competency a. WAC 246-840-230 Continuing Competency Audits: If nurses did not
fully comply with the continuing competency requirements, the nurse must complete 177 hours of active practice and 15 hours of continuing education within one year. This is referred to as a 177/15 requirement. While many nurses intend to on finish the requirement, many do not complete the necessary hours.
MOTION: Moved by Mr. Canary with a second by the Discipline subcommittee to add the underlined language on pg. 155 to Procedure A27 Sanctioning Standards. Motion Carried.
NCQAC Business Meeting July 12-13, 2018
32

D. Licensing – Jeannie Eylar, Chair
1. Continuing Competency a. Absence of strong evidence that continuing competency regulations
improves competency and the resultant workload were presented to the NCQAC. Teresa Corrado, licensing manager, projected 5 FTE employees to be able to be compliant with audits required in rules.
MOTION: Moved by Ms. Eylar with a second by Ms. Strader to recommend opening the current continuing competency rules Motion Carried. MOTION: Moved by Mrs. Eylar with a second by licensing subcommittee to suspend the audit process until new rules are established. Motion Carried. Ms. Corrado informed NCQAC that Licensing will revise the renewal notice and change the attestation to correspond with this action. The reactivation application will be revised as well. A newsletter article will be submitted explaining this action. A letter will be sent to people due for a 177-15 to inform they will not be audited. Audits currently in process will be finished.
IX. Education Session: Civility, Conflict, and Communication– Margaret Holm, RN,
JD Ms. Holm is a nurse consultant with the Nursing Commission Unit. Ms. Holm works with employers and nurses and provides extensive education on the Nurse Practice Act, Nursing Scope of Practice and consults on nursing regulatory issues. One of Ms. Holm’s most frequently requested presentations is on Civility in the Workplace.
X. 1:00 PM – 1:15 PM Open Microphone Open microphone is for public presentation of issues to the NCQAC. If the public has issues regarding disciplinary cases, please call 360-236-4713. Curt Eschels- President of Washington East Asian Medical Association. Mr. Eschels presented a letter questioning required training for nurses to provide acupuncture. Mr. Eschels expressed concerns that NCQAC needs more transparency in regards to policy making and supports Representative Eileen Cody’s request for rule making. Rule-making offers a wide open process to involve the public and a path to consensus. Melissa Johnson – Lobbyist Washington Association of Nurse Anesthetist. Ms. Johnson stated the “why” was missed in this morning’s conversation related to CRNA applications and documentation of masters degrees from a nursing program. Ms. Johnson expressed she is heartened that NCQAC reiterated the degree doesn’t have to be housed in a school of nursing. Hopes that endorsing CRNA’s that meet the four requirements in the WAC do not have to jump through further hoops for licensure. Jian Wang – Acupuncturist, on the board of Washington East Asian Medicine Association and licensed as an acupuncturist for 20 years. The Washington East Asian Medicine Association would be pleased to share knowledge with NCQAC. Washington East Asian Medicine Association have suggestions and will cooperate with NCQAC’s work.
XI. Legislative Panel – Donna Poole – DISCUSSION/ACTION The Legislative Panel reviews and analyzes bills during the legislative sessions. In addition, the Legislative Panel recommends actions for legislation for the NCQAC. Ms. Poole presents the recommendations for the 2019 session.
NCQAC Business Meeting July 12-13, 2018
33

Recommend continued work on background checks with Senator Rivers. Recommend continued with WSNA, DOH, and DSHS to work on Nursing Assistants Recommend to work on a decision package going forward. Submission would need to be in late September. Recommend to remove HIV requirement since people receive this with their education. MOTION: Moved by Ms. Poole with a second by legislative panel to adopt the four recommendations for 2019 legislative session.
1. Continued work on background checks with Senator Rivers. 2. Continued work with WSNA, DOH, and DSHS on Nursing Assistants. 3. Decision package requesting increased spending authority. Submission needs to
be in late September. 4. Remove HIV education requirements for licensure. Motion Carried.
Ms. Masek raised the question as to why our PMP isn’t linked with the majority of the states for data sharing.
XII. Petition to open rules on Acupuncture: Representative Eileen Cody On April 3, 2018, the NCQAC received a letter from Representative Eileen Cody related to ARNPs and acupuncture. The letter was considered as a petition to open rules. The NCQAC previously adopted an advisory opinion recognizing medical acupuncture as within the scope of practice for ARNPs with adequate education to perform safely. A question of which argument is being made? Is this a question of Eastern vs Western medicine? Is acupuncture being looked at as a procedure or a philosophical approach? Ms. Poole thought potentially opening the rules to create a process to give individuals the ability to make their own decisions about what they can do based on their knowledge, and competency. This could reduce the amount of Advisory Opinions NCQAC currently produces. NCQAC needs a process to determine scope of practice issues that grows as healthcare grows and evolves. Discussion of overlap between procedures similar to the overlap between ARNs and MD practice. Further discussion regarding why ARNPs are being told they shouldn’t be able to practice this procedure, while MDs are able to do this procedure after taking a 300 hour class.
MOTION: Moved by Dr. Soine with a second by Ms. Poole to open the rules for Scope of Practice. Consider inserting a decision tree. While that process is underway the Advisory Opinion will be intact.
AMENDED MOTION: Moved by Dr. Soine with a second by Ms. Poole to open rules for Scope of Practice. Meanwhile continue with the Advisory Opinion to provide guidance. Three oppose, motion carried.
NCQAC Business Meeting July 12-13, 2018
34

XIII. Nurse Strike Team and the Emergency Preparedness System in WA State – Andrew Rose – DISCUSSION/ACTION Mr. Rose presents the concept of a Nurse Strike Team that has been used in Emergency Response in several states. Mr. Rose also describes the emergency responder system used in WA state and new legislation. Mr. Rose was unable to attend today’s meeting and this item will be rescheduled to a future meeting.
XIV. Education Report – DISCUSSION/ACTION
A. Update on Action Now! – Drs. Mary Baroni, Mary Sue Gorski, Geri Babbo, Kathy Moisio, and Mindy Schaffner A need exists for communication with Washington’s citizens to understand the problem of underpaid nurse faculty and the impact on patient care. A new nursing graduate’s initial salary is often more a faculty member with ten years’ experience and has a masters’ degree in nursing. Nursing faculty salaries in community colleges are very low in comparison to staff nurses. It’s very difficult for people to afford to work as faculty. Ms. Masek points out her opinion that this is a women’s issue. Requests sending the governor a letter about inadequate pay in nursing faculty. MOTION: Moved by Ms. Masek with a second Ms. Randich to send a letter to the governor about inadequate compensation for nurse faculty and inform him of lack of membership in national Prescription Monitoring data base issue. Motion Carried. Dr. Schaffner recommends building a decision package to get funding to build in capacity for nursing education, to develop a preceptorship academy, increasing simulation throughout the state, and potential use of a simulation program to evaluate nurses that are in the discipline program.
B. Poster Presentations – Refer to Business Packet Posters from Action Now! Presentations were provided for the NCQAC. Descriptive Analysis OF RN-to-BSN Program Designs and Faculty Perspectives- Mary Baroni, PhD, Suzanne Sikma, PhD, RN, and Renee Hoeksel, PhD, RN, ANEF A Decade of Academic Progression in Washington State: Poster Symposium Overview-Mary Baroni, PhD, RN and Renee Hoeksel, PhD, RN, ANEF Does Regulatory Oversight of RN-to-BSN Programs Assure Quality Academic Progression?-Mary Sue Gorski, PhD, RN, Mary Baroni, PhD, RN, and Mindy Schaffner, PhD, RN
XV. Gap Analysis of Surveys Providing Information to Understand Washington State Supply of Nurse Practitioners – Tracy Stearns-Church, AGNP-PC Student, University of Washington – DISCUSSION/ACTION Tracy Stearns-Church, AGNP-PC, a student from the University of Washington, presented her Capstone Project, “A Gap Analysis of Surveys Providing Information to Understand the Washington State Supply of Nurse Practitioners”. She provided policy areas to consider that might help change the workforce trend including population recruitment, incentives, and industry support. She discussed an issue concerning Nursys demographic data not connecting with the DOH licensing system.
NCQAC Business Meeting July 12-13, 2018
35

XVI. Election of New Officers – DISCUSSION/ACTION Each year at the May meeting, the NCQAC elects officers for chair, vice chair and secretary/treasurer. New officers take their positions at the July 13, 2018 NCQAC meeting. Jeannie Eylar, chair of nominations, read the slate of candidates: Tracy Rude for Chair, Mary Baroni and Helen Myrick for Vice-Chair, and Lois Hoell for Secretary/Treasurer. Donna Poole conducted the meeting through the election process. Gail Yu reviewed the Election Process Procedure prior to voting. Total of 14 votes cast Chair: Tracy Rude (14), Total of 14 votes cast for Secretary/Treasurer: Lois Hoell (14), Total of 14 votes cast for Vice-Chair: Mary Baroni (8), Helen Myrick (6).
XVII. Meeting Evaluation
Thank you for the nursing recognition activities, (cake) special thank you to Adena Nolet for the beautiful cookies. Congratulations to Suellyn Masek, food was great (other than broccoli), some microphone issues, Several kudos about Margaret Holm’s presentation, packed agenda. Thank you to Gail for the 1427 work. Suellyn gave a thank you for the well-wishes. Laurie Soine gave a special thank you to Gail Yu and Karl Hoehn for their guidance about the challenging issues the NCQAC is currently addressing. Renee Ruiz gave a special thank you to Erica Benson-Hallock for mentoring and support.
XVIII. 4:13 PM Adjourned
NCQAC Business Meeting July 12-13, 2018
36

Nursing Care Quality Assurance Commission (NCQAC) Advanced Practice Sub-committee Agenda
March 21, 2018 7:00 pm to 8:00 pm
GoToMeeting Please join my meeting from your computer, tablet or smartphone.
https://global.gotomeeting.com/join/449994717
You can also dial in using your phone. United States: +1 (872) 240-3412
Access Code: 449-994-717 Committee Members:
Laurie Soine, PhD, ARNP, Chair
Donna Poole, MSN, ARNP, PMHCNS-BC Daniel Simonson, ARNP-CRNA, MHPA, Pro Tem Heather Bradford, CNM, ARNP, FACNM, Pro Tem Heather Schoonover, MN, ARNP, PHCNS-BC, Pro Tem Christine Burnell, DNP, ARNP-FNP, Pro Tem Daniel Petersen, MSN, ARNP-FNP, RN-BC, Pro Tem Staff: Mary Sue Gorski, PhD, RN, Nurse Consultant Advisor
Kristen Durborough, Practice Administrative Assistant
If you have questions regarding the agenda, please call Kristen Durborough 360-236-4724. Items may be taken out of order. If you wish to attend the meeting for a single item, contact our office at the number listed above and request a specific time scheduled for that item. This meeting is accessible to persons with disabilities. Special aids and services can be made available upon advance request. Advance request for special aids and services must be made no later than March 15, 2018. If you need assistance with special needs and services, please leave a message with that request at 1-800-525-0127 or, if calling from outside Washington State, call (360) 236-4052. If you have limited English language expertise, call Mary Sue Gorski at (360) 915-3334 before March 15, 2018. TDD may also be accessed by calling the TDD relay service at 1-800-833-6388. If you need assistance due to a speech disability, Speech to Speech provides human voicers for people with difficulty being understood. The Washington State Speech to Speech toll free access number is 1-877-833-6341. This meeting will be digitally recorded to assist in the production of accurate minutes. All recordings are public record. The minutes of this meeting will be posted on our website after they have been approved at the May 11, 2018 NCQAC meeting. For a copy of the actual recording, please contact the Public Disclosure Records Center (PDRC) at [email protected]. Questions from the public will be held and answered at the end of the meeting. Use the question panel to submit questions.
NCQAC Business Meeting July 12-13, 2018
37
I. Call to Order • Introduction - Laurie • Public Disclosure Statement - Laurie • Roll Call - Laurie
II. Standing Agenda Items
• Announcements/Hot Topic/NCQAC Business Meeting Updates - None • National Council State Boards of Nursing Advanced Practice Registered Nurse
(APRN) Network Updates – None, next call April 12, 2018 • APSC Meeting Minutes (Draft for review) – February 21, 2018 – Consensus • Opioid Prescribing – Updates – Donna Poole –
o Gave update on the last gathering of the multidisciplinary year long Rule Writing workgroup work. Draft rules are undergoing final revisions and will be available by March 28th.
III. Old Business • Regulatory Background Review of Advanced Practice Hour Requirements
Update – Update given by Mary Sue.
IV. New Business • Practice hours and continuing competency – Update given by Mary Sue. This
project is still being worked on.
V. Ending Items • Open Microphone (as time permits)
o Louise – Commented on Opioid rules. She requested that as the NCQAC reviews and discusses the rules that they be very specific in clarifying when a pain management specialist is required. To help people understand that an ARNP may still care for patients requiring opioids and not be a pain management specialist to minimize the unintended consequences of practices not willing to treat patients requiring care. Once rules have been finalized she suggested creating a comprehensive F&Q sheet to help explain the changes.
o Melissa – Commented on information WANA will be putting together information on the proposed changes included in the new rules to be distribute to CRNA’s regarding education around pain management.
• Review of Actions • Date of Next Meeting – April 18, 2018 • Adjournment – 8:00 PM or earlier if business is finished
NCQAC Business Meeting July 12-13, 2018
38

Nursing Care Quality Assurance Commission (NCQAC) Advanced Practice Sub-committee Minutes
April 18, 2018 7:00 pm to 8:00 pm
GoToMeeting Please join my meeting from your computer, tablet or smartphone.
https://global.gotomeeting.com/join/449994717
You can also dial in using your phone. United States: +1 (872) 240-3412
Access Code: 449-994-717 Committee Members Present:
Laurie Soine, PhD, ARNP, Chair
Christine Burnell, DNP, ARNP-FNP, Pro Tem Daniel Simonson, ARNP-CRNA, MHPA, Pro Tem Daniel Petersen, MSN, ARNP-FNP, RN-BC, Pro Tem Absent Donna Poole, MSN, ARNP, PMHCNS-BC
Heather Bradford, CNM, ARNP, FACNM, Pro Tem Heather Schoonover, MN, ARNP, PHCNS-BC, Pro Tem Kathleen Errico, PhD, ARNP, Pro Tem Dayna Morgan, MN, ARNP, Pro Tem
Staff: Mary Sue Gorski, PhD, RN, Nurse Consultant Advisor Debbie Carlson, MSN, RN, Associate Director of Nursing Practice Kristen Durborough, Practice Administrative Assistant Karl Hoehn, JD, Attorney Manager
If you have questions regarding the agenda, please call Kristen Durborough 360-236-4724. Items may be taken out of order. If you wish to attend the meeting for a single item, contact our office at the number listed above and request a specific time scheduled for that item. This meeting is accessible to persons with disabilities. Special aids and services can be made available upon advance request. Advance request for special aids and services must be made no later than April 11, 2018. If you need assistance with special needs and services, please leave a message with that request at 1-800-525-0127 or, if calling from outside Washington State, call (360) 236-4052. If you have limited English language expertise, call Mary Sue Gorski at (360) 915-3334 before April 11, 2018. TDD may also be accessed by calling the TDD relay service at 1-800-833-6388. If you need assistance due to a speech disability, Speech to Speech provides human voicers for people with difficulty being understood. The Washington State Speech to Speech toll free access number is 1-877-833-6341.
NCQAC Business Meeting July 12-13, 2018
39

This meeting will be digitally recorded to assist in the production of accurate minutes. All recordings are public record. The minutes of this meeting will be posted on our website after they have been approved at the July 13, 2018 NCQAC meeting. For a copy of the actual recording, please contact the Public Disclosure Records Center (PDRC) at [email protected]. Questions from the public will be held and answered at the end of the meeting. Use the question panel to submit questions.
NCQAC Business Meeting July 12-13, 2018
40

I. Call to Order • Introduction – Laurie • Public Disclosure Statement - Laurie • Roll Call - Laurie
II. Standing Agenda Items
• Announcements/Hot Topic/NCQAC Business Meeting Updates • National Council State Boards of Nursing Advanced Practice Registered
Nurse (APRN) Network Updates April 5, 2018 – Kristen gave brief update on topics discussed on this month’s call.
• APSC Meeting Minutes (Draft for review) – March 21, 2018 – consensus to send to commission
III. Old Business • Regulatory Background Review of Advanced Practice Hour Requirements
Update – Mary Sue gave update for project. Informed the committee that Kathleen Errico has been brought on as a Pro-tem to assist with this project.
IV. New Business • Revised Medical Marijuana Authorization Guidelines – No new updates. • CRNA Educational Requirements-
Karl reviewed the process of ARNPs seeking licensure via endorsement WAC 246-840-342. He reminded the group about the 2016 updates listing the requirements for ARNP licensure by endorsement:
1) An active RN and ARNP license from another jurisdiction without restrictions or sanctions;
2) A graduate degree from an advanced nursing education program that is accredited by a national nursing accreditation body recognized by the U.S. Dept. of Education;
3) Certification from a national certifying body approved by the Commission; and
4) Has been performing advanced clinical practice as a licensed ARNP for at least 250 hours within the previous two years.
Karl explained that if the licensing department has questions about an applicant’s educational qualifications, the application is referred to the Commission’s education director, who reviews the information the applicant is required to submit, such as transcripts, and may request additional information about the program, such as program objectives and course descriptions. WAC 246-840-342(2)(e) and (f). A Nursing Program Approval Panel (NPAP) may approve the educational preparation, request further
NCQAC Business Meeting July 12-13, 2018
41

information from the applicant regarding the four primary qualifications for ARNP licensure, or determine that the applicant’s educational preparation does not meet the requirements of the rule. As questions have arisen regarding the meaning of the requirement that an applicant for licensure by endorsement as a Certified Registered Nurse Anesthetist (CRNA) must have “a graduate degree from an advanced nursing education program as identified in WAC 246-840-340(1)(b).” WAC 246-840-342(1)(b), and whether the program must be part of a school of nursing. An “advanced nursing education program,” as identified in WAC 246-840-340(1)(b), must be “accredited by a national nursing accreditation body recognized by the United States Department of Education.” A “nursing education program” is defined in WAC 246-840-010(28) as “a division or department within a state supported educational institution or other institution of higher learning, charged with the responsibility of preparing nursing students and nurses to qualify for initial licensing or higher levels of nursing practice.” Questions have arisen as to whether a Certified Registered Nurse Anesthetist (CRNA) with a graduate degree from a nurse anesthesia educational program accredited by the Council on Accreditation of Nurse Anesthesia Educational Programs (COA) that is not housed within a school of nursing meets the qualification for licensure by endorsement. Historically, many CRNA programs were housed within medical centers, often affiliated with a university. However Karl explained because they provide higher education and grant degrees, these program qualify as being within “institutions of higher learning.” Karl then explained that per our rule, as it currently stands, a CRNA with a graduate degree from an advanced nursing education program that is charged with preparing nurses for higher levels of nursing practice and is accredited by a recognized national nursing accreditation body does meet the qualifications in WAC 246-840-342 . The rule does not specify that the program conferring the graduate degree must be administered by a school of nursing. This clarification was met by great enthusiasm from members of the subcommittee as well as the many CRNA guests and CRNA faculty who joined the call. When Chair Laurie asked Karl for next action, Karl suggest that we could make a motion to reinforce the rules as they currently stand. There was unanimous agreement by all on the call to “agree” to reinforce the rules.
V. Ending Items • Open Microphone (as time permits) –
Melissa Johnson – Thanked the subcommittee as this is an outcome they were hoping for. Jeff – President of WANA, this created a lot of anxiety amongst CRNA community. Encouraged to reach out for a CRNA perspective if needed.
• Review of Actions
NCQAC Business Meeting July 12-13, 2018
42

Will take a motion to the Commission to reaffirm the point that the advance nursing education program is a program that nurses come into to get training for advance level of practice. Does not have to be a School of Nursing but rather what the rules say.
• Date of Next Meeting – May 16, 2018 • Adjournment – 8:00 p.m.
NCQAC Business Meeting July 12-13, 2018
43

Nursing Care Quality Assurance Commission (NCQAC) Discipline Sub-committee Minutes April 24, 2018 3:30 pm to 5:30 pm
Committee Members: Adam Canary, LPN, Chair Edie Higby, Public Member Lois Hoell, MS, MBA, RN
Sharon Ness, RN Tiffany Randich, LPN
Tracy Rude, LPN ad hoc Staff: Catherine Woodard, Associate Director of Discipline (excused) Mary Dale, Discipline Manager
Karl Hoehn, Legal Manager John Furman, Director, WHPS (excused) Grant Hulteen, Chief Investigator Rozanne McCarty, HSC
I. 3:30 pm Opening – Adam • Call to order – digital recording announcement • Roll call
II. March 27, 2018 Minutes – Adam
Consensus was to add the March minutes to the NCQAC agenda for approval.
III. Performance Measures – Lois Lois reviewed Quarter 2 performance measures. Intake is at 100 %; Investigations within timelines is 57%; Case Disposition is at 89%; overdue investigations are over target by 10%; overdue case disposition is less than 2% over target. Grant and Karl explained that case intake has increased 70% in the last two years, and cases are getting backlogged in investigations. The workload coming to legal is increasing the number of cases assigned to the attorneys. Two investigators were just hired; we were waiting for the fee increase before filling the positions. This will make an impact on the performance measures.
IV. Discipline Report – Grant Grant and Karl presented the statistics for discipline. The attorneys have a target of closing 10 cases per month per attorney. Grant presented an additional spreadsheet of comparative information and will send copies to the subcommittee.
NCQAC Business Meeting July 12-13, 2018
44

V. Opening Cases Based on Blood Alcohol Content (BAC) - John John was not available for this meeting, and forwarded an email from Barry Lubin, and one from Dr. David Beck. The subcommittee had asked if there was a certain blood alcohol content that would indicate a substance use disorder. Both agreed that a correlation cannot be made between the two. Dr. Beck also said, because of the variation in the alcohol user, in the person doing the testing, and in a given individual’s ability to perform the tests, it would be difficult to find an objective measure. Mary will forward Dr. Beck’s email, with attachments, to the subcommittee. This topic will be on the May agenda.
VI. Recreational and Medical Marijuana – Karl Information from the American Cannabis Nursing Association, Canada, and other states was provided. Karl has researched Canada marijuana laws, and they are developing standards according to amounts and types of cannabis. However, marijuana cannot be prescribed here. The concern we hear from nurses is regarding their licenses being at risk if they administer. This topic is for information only, and will be taken off the work plan.
VII. Work Plan – Adam Adam reviewed the status of items on the work plan. The Newsletter article was submitted. The next discipline report will be in July. The workgroup looking at the WHPS procedures has held their first meeting. Recreational and Medical Marijuana discussion is complete. Opening cases based on blood alcohol content will be on the May agenda. Mary will take her name off the work plan and replace with Catherine’s.
VIII. Meeting Evaluation – All Everyone agreed the meeting went well. Sharon is looking forward to the articles on BAC; Lois likes the additional discipline report; Tiffany is interested in medical marijuana information.
IX. Closing 4:47 p.m.
NCQAC Business Meeting July 12-13, 2018
45

Nursing Care Quality Assurance Commission (NCQAC) Licensing Sub-committee Minutes
April 27, 2018 9:30 am to 11:30 am Register for the GOTOMeeting below
https://global.gotomeeting.com/join/116459909 You can also dial in using your phone.
United States: +1 (669) 224-3412 Access Code: 116-459-909 Audio Pin: 59#
Committee Members Present:
Jeannie Eylar, MSN, RN, Chair Margaret Kelly, LPN
Suzy Cook, MN, RN, CHSE, CNE Lois Hoell, MS, MBA, RN Members Absent
Yvonne Strader, RN, BSN, BSPA, MHA Tracy Rude, LPN Geri Babbo, EdD, MN, RN
Staff Present:
Teresa Corrado, LPN, CPM, Licensing Manager
Karl Hoehn, JD, Legal Manager Kristen Durborough, Nurse Practice Assistant
Tom Bolender, Licensing Lead
If you have questions regarding the agenda, please call Kristen Durborough 360-236-4724. Items may be taken out of order. If you wish to attend the meeting for a single item, contact our office at the number listed above and request a specific time scheduled for that item. This meeting is accessible to persons with disabilities. Special aids and services can be made available upon advance request. Advance request for special aids and services must be made no later than April 18, 2018. If you need assistance with special needs and services, please leave a message with that request at 1-800-525-0127 or, if calling from outside Washington State, call (360) 236-4052. If you have limited English language expertise, call Kristen Durborough at 360-236-4724 before April 18, 2018. TDD may also be accessed by calling the TDD relay service at 1-800-833-6388. If you need assistance due to a speech disability, Speech to Speech provides human voicers for people with difficulty being understood. The Washington State Speech to Speech toll free access number is 1-877-833-6341. This meeting will be digitally recorded to assist in the production of accurate minutes. All recordings are public record. The minutes of this meeting will be posted on our website after they have been approved at the July 13, 2018 NCQAC meeting. For a copy of the actual recording, please contact the Public Disclosure Records Center (PDRC) at [email protected].
NCQAC Business Meeting July 12-13, 2018
46

If you are attending the meeting as a webinar, please mute your microphone in order to minimize background noise during the meeting. Smoking is prohibited at this meeting.
I. Call to Order • Introduction - Jeannie • Public Disclosure Statement - Jeannie • Roll Call - Jeannie
II.
Standing Agenda Items • Announcements/Hot Topic/NCQAC Business Meeting Updates:
Tracy - Mentioned Mary Dale’s retirement as of April 27th. Lois - Discussed special meeting regarding opioid rules. Object was to hear from the community and receive input as well as educate them on the potential rules. Meeting was said to have been successful.
• Licensing Meeting Minutes (Draft for review) – February 23, 2018 – consensus to go to July commission meeting.
• Work Plan Review- Teresa– Gave update on work plan.
III. Old Business
• Renewing from Expired to Retired – Karl – Explained the internal procedure that was included in the packet as well as his reasoning for recommending it go to the full commission. Margaret – participated with her suggestions for the document.
• Continuing Competency Recommendation – Teresa – explained recommendations brought forth in regards to continuing competency and audits. Will bring this issue forth to the business meeting in May.
IV. New Business • Continuing Competency- Preceptor Hours-
Teresa – This topic arose from an email originally sent to Mindy Schaffner. It was discussed and handled prior to meeting. Teresa did not think it was necessary to continue conversation around this topic.
• Rules Review – WAC 246-840-050 - Teresa Corrado
V. Ending Items • Open Microphone (as time permits) • Review of Actions
o Recommendation of the procedure of renewing from expired to retired to the full commission in July
NCQAC Business Meeting July 12-13, 2018
47

o Recommending to the full commission in May to open the continuing competency rules and suspend auditing
• Date of Next Meeting – May 18, 2018 • Adjournment- 10:52 A.M.
NCQAC Business Meeting July 12-13, 2018
48

Nursing Care Quality Assurance Commission (NCQAC) Licensing Sub-committee Minutes May 18, 2018 9:30 am to 11:30 am
Register for the GOTOMeeting below
Please join my meeting from your computer, tablet or smartphone. https://global.gotomeeting.com/join/116459909
You can also dial in using your phone. United States: +1 (669) 224-3412
Access Code: 116-459-909 Audio Pin: 59#
Committee Members: Jeannie Eylar, MSN, RN, Chair
Margaret Kelly, LPN Geri Babbo, EdD, MN, RN Suzy Cook, MN, RN, CHSE, CNE Lois Hoell, MS, MBA, RN Yvonne Strader, RN, BSN, BSPA, MHA
Staff: Teresa Corrado, LPN, CPM, Licensing Manager Kristen Durborough, Nurse Practice Assistant
If you have questions regarding the agenda, please call Kristen Durborough 360-236-4724. Items may be taken out of order. If you wish to attend the meeting for a single item, contact our office at the number listed above and request a specific time scheduled for that item. This meeting is accessible to persons with disabilities. Special aids and services can be made available upon advance request. Advance request for special aids and services must be made no later than May 11, 2018. If you need assistance with special needs and services, please leave a message with that request at 1-800-525-0127 or, if calling from outside Washington State, call (360) 236-4052. If you have limited English language expertise, call Kristen Durborough at 360-236-4724 before May 11, 2018. TDD may also be accessed by calling the TDD relay service at 1-800-833-6388. If you need assistance due to a speech disability, Speech to Speech provides human voicers for people with difficulty being understood. The Washington State Speech to Speech toll free access number is 1-877-833-6341. This meeting will be digitally recorded to assist in the production of accurate minutes. All recordings are public record. The minutes of this meeting will be posted on our website after they have been approved at the July 13, 2018 NCQAC meeting. For a copy of the actual recording, please contact the Public Disclosure Records Center (PDRC) at [email protected]. If you are attending the meeting as a webinar, please mute your microphone in order to minimize background noise during the meeting.
NCQAC Business Meeting July 12-13, 2018
49

Smoking is prohibited at this meeting.
I. Call to Order 9:33 – Jeannie Eylar, MSN, RN, Subcommittee Chair • Introduction • Public Disclosure Statement • Roll Call
II.
Standing Agenda Items • Announcements/Hot Topic/NCQAC Business Meeting Updates
o Commission moved to open continuing competency rules, and suspend audits in the meantime.
o Teresa – licensing unit is drafting documents and changes needing to be made to current documents. Hoping to get distributed to public next week. Teresa created a project plan to roll out message to public.
o Ms. Hoell offered to read the documents for clarity. Ms. Strader, and Ms. Eylar would also like to review them.
• Licensing Meeting Minutes (Draft for review) – April 27, 2018 – Consensus to take to July business meeting.
• Work Plan Review- Teresa Corrado
III. Old Business • Renewing from Expired to Retired – Karl Hoehn, Teresa Corrado
o After the commission decision on May 11th there is no reason to continue editing this internal policy.
• Continuing Competency Rule Changes – Teresa Corrado o Discussion around bringing rules to subcommittee to work on
potential verbiage. Decided against it due to not being able to draft language prior to stakeholder work.
IV. New Business
• None
V. Ending Items • Open Microphone (as time permits) • Review of Action
o Once Karl legally reviews documents Teresa will send documents to Ms. Eylar, Ms. Hoell. And Ms. Strader for review.
o Teresa will continue to give updates at upcoming licensing meetings.
• Date of Next Meeting – June 22, 2018 • Adjournment- 9:52 AM
NCQAC Business Meeting July 12-13, 2018
50

National Organization of Alternative Programs Annual Conference
March 26 -March 30, 2018 New Orleans, LA Yvonne Strader
Purpose: The National Organization of Alternative Programs (NOAP) annual conference brings health and other professional disciplines together to share and learn about best practices in the alternatives to discipline in licensure while promoting safe practice and retention of those individuals with addiction or impairment through rehabilitation, and monitoring. There are many complexities in treating and monitoring individuals through their recovery and rehabilitation. NOAP assists to bring professionals working in this field and those on the national state boards of nursing to learn from each others’ practices and experiences. Education is presented about best practices, laboratory science, access to care, barriers to treatment and monitoring, and decreasing and eliminating the stigma associated with addiction and mental illness. Outcomes:
• The sharing of best practices and components of successful monitoring across states as well as challenges encountered in their respective programs.
• Navigating the National Practitioner Data Bank and NCSBN resources that included locating NCSBN Substance Use Disorder resources and the Opioid toolkit.
• Tennessee experiences in Mental Health and on-line support groups and successes in working with collaborative partnerships.
• Opioid free anesthesia discussed how to use blocks in lieu of opioids as well as education regarding opioid induced analgesia.
• Face to face mental health support groups to support nurses with co-occurring disorders. There was much discussion on the stigma of mental health disorders.
• Collegiate Recovery Alliance discussion was about the college student populations and the peer pressures surrounding those with SUD issues and the lack of resources available to many schools.
• Pain management in the monitoring program. • Alternative to Discipline program types. • Medical Review Officer and toxicology discussion and methods of testing. • CRNA reentry discussed the unique challenges of this profession and return to
work guidelines with their environment. Recommendation: The NAOP conference is held annually and is the fundamental meeting for state Alternative to Discipline programs for nurses and other health professionals. As we continue to work with nurses who have SUD and other co-occurring disorders, we need to stay current with national standards of practice and innovative ideas sought from other agencies. My recommendation is have annual attendance and involvement in NOAP conferences by commission members and WHPS personnel.
NCQAC Business Meeting July 12-13, 2018
51

NCSBN 2018 IT/Operations Conference
May 15 – 16, 2018 Albuquerque, NM Chris Archuleta
PURPOSE:
• Discuss strategies to: o Safeguard against a network attack and provide tips to develop an effective Security
Awareness program. o Improve quality in processes. o Prepare for an FBI Audit. o Prevent and detect Fraud.
• Provide an opportunity to ask questions and learn from each other. • Promote face-to-face collaboration, idea exchange and interactions. • Deliver tools to assist operations and technology employees in their day-to-day activities.
OUTCOME:
• Developing a Secure Network – Federico Campbell, MBA, CFE, EnCE, Director of Cyber Risk & Information Security Services, Navigant Mr. Campbell presented on the current cyber threat environment, developing risk-based cyber security program, and provide some practical tips for effective cyber security. According to Mr. Campbell, outside actors perpetrate 75% of data breaches and 81% of breaches are the result of stolen or weak passwords. A common theme of the discussion was on ways to assist and educate the people element of cyber security.
• How to Build a Security Awareness Program – Winn Schwartau, Founder, The Security Awareness Company Mr. Schwartau provided a high energy and engaging discussion on building a security awareness program. This complimented the earlier presentation. To successfully create and implement a security awareness program, the message needs to be clear, the training needs to be relevant, and approaching the program through a marketing lens is beneficial. The challenge is keeping the message present and fresh in daily routines will ensure a successful implementation and buy in.
• FBI Audit Preparation – Tom Purdy, CISSP, CIO, North Carolina BoN; Adrian Guerrero, Area II Director, NCSBN, Director of Operations, Kansas State BoN; Mark Majek, Director of Operations, Texas BoN FBI criminal background check audits are required at a minimum every three years. The panel discussed their recent experiences with preparing for and going through the audit process. They also provided tips and recommendations to ensure compliance. The NCQAC being an umbrella agency and the fact we use DOH resources for background checks ensures we do not directly receive the audit; DOH would receive the audit.
• Managing Quality – John Orlando, Independent Management Consultant Mr. Orlando presented on how to manage quality by using a four-quadrant framework. The focus is on the experience of the employee and the customer, how those experiences are related, how they differ, and drive the success of the change. The quality of each experience will dictate the success.
NCQAC Business Meeting July 12-13, 2018
52

• Fraud Detection – Lori Scheidt, MBA-HCM, Director-at-Large, NCSBN Board of Directors, Executive Director, Missouri State BoN; Veronica Robertson, Program Supervisor, Texas BoN Ms. Scheidt and Ms. Robertson provided an update on their presentation at the 2016 IT/Ops Conference on fraud issues during the licensing process. During their investigation of numerous cases of fraudulent applications submitted to their respective boards, they uncovered multiple trends and compiled a list of red flags to look out for in detecting fraud. Fraud is an issue for all state boards of nursing.
• NCSBN Showcase – updates were provided on the following NCSBN resources and applications:
o Nursys o Nursing Regulations o Interactive Services o eNLC o ORBS
RECOMMENDATION: Continued attendance at this conference is highly recommended. Staying current with training on the prevention of data breaches is critical to protecting NCQAC data and processes. The NCQAC and staff would benefit from additional training on security awareness and creating a best practices program. The networking aspect of this conference was very beneficial. Discussing IT best practices with other state boards of nursing and reviewing their accomplishments and remaining challenges is encouraging.
NCQAC Business Meeting July 12-13, 2018
53

NCSBN 2018 Discipline Case Management Conference
June 6-8, 2018 Denver, CO Tracy Rude
PURPOSE: Preparation in advanced interviewing, locate current marijuana legislation, consequences of a varied regulation regarding criminal convictions, nuances of investigations involving compact states, BON liense reinstatement process, consider definition of good moral character in a regulatory context, NPDB processes for subject statement and dispute resolution, issues influencing toxicology results. OUTCOME: The first agenda item of this meeting provided an important review of the history of cannabis in the US and was presented by Maureen Cahill, Rene Cronquist, Kent Gowen, and Kathleen Russel from NCSBN. In 1850 it was sold OTC for a variety of ailments and conditions. Gradually, it became more tightly controlled. In recent history many states have allowed use in certain medical circumstances and others allow medical use along with recreational use. Federal regulations remain steadfast regarding the use and authorization by prescribers. Public opinion is beginning to shift in favor of legalization with millennials leading generationally. In 2016 NCSBN began looking at regulatory implications of the use of cannabis. Research confirms there is very little applicable information for nurses. Of states with medical marijuana programs Illinois has the most approved conditions. Of note, APRN’s in WA have within their scope of practice to certify a qualifying condition for authorization of cannabis. In disciplining nurses, it is important to be aware of state regulations and Right-Touch Regulation is advised. Therapeutic effects along with adverse effects were presented as well as the effects of overdose, abuse, dependence and withdrawal. Research has been ongoing for at least 50 years and still there is no reliable way to measure impairment. NCSBN recommends cannabis-specific education content in ARNP programs. The struggle is where to fit it in the curriculum. I also attended “Catch Me (If You Can): The Impaired Provider.” Claudia Garcia, RN and Rodrigo Garcia, CRNA related their story of Rodrigo’s addiction. They are married and were working at the same hospital when Rodrigo was injured and subsequently suffered addiction to opioids. This couple present a wonderful retelling of their story through the addiction and treatment process and their continuing work in a treatment center now. We were fortunate to have this couple present at our SUD conference last October and it was a pleasure to see them again. Brett Thompson-May, JD provided a look into discipline for nurses with multi-state privilege. It is necessary for states to communicate with each other to ensure eNLC stipulations are observed and discipline is appropriately administered. Two speakers, Morgan Ransdall, JD and Tomm Crabb, JD, addressed CFR 42 and CFR 42 Part 2. Federal regulations were clearly outlined for requesting records from treatment programs
NCQAC Business Meeting July 12-13, 2018
54

receiving federal funding. Discussion included what happens once those records are received and the handling according to federal law. It is not impossible to get these records if the Good Cause Exemption is met. Work has been done to remove unnecessary language in the records requests and consent and has provided more clarity in the use and dissemination of these records. Amy Fitzhugh, JD related a NC BON voluntary surrender case that started in 2005 and was in litigation for ten years. It brought to the forefront the need for as much detail and information on documents regarding what the BON expects from the respondent. There are certain facts the nurse must acknowledge. Louis D. Kelly, JD presented information on transparency and technology. He talked about the challenges in maintaining public trust and managing public correspondence on emerging platforms. He related several instances of careless communication and how to ensure information is handled in the most professional and transparent way possible. There were many opportunities to collaborate with attendees from other jurisdictions regarding the issues presented at this meeting. What I discovered is Washington remains at the forefront in our practices and are willing to adopt the most current evidence based practices available. RECOMMENDATION: I would recommend continued participation and attendance at this meeting.
NCQAC Business Meeting July 12-13, 2018
55

NCSBN 2018 Discipline Case Management Conference
June 6-8, 2018
Denver, Colorado
Grant Hulteen
PURPOSE: Provide principles and examples for:
• Reid Telephone interviewing techniques • Current legislation for legal marijuana uses • Various regulations regarding criminal convictions • Case investigations involving compact states • BON licensure reinstatement process • Definition of good moral character in regulatory context • NPDB processes for subject statement and dispute resolution • Toxicology results analysis.
OUTCOME: I attended the Medical Marijuana and Nursing Practice lecture Maureen Cahill, Rene Cronquist, Kent Gowen, and Kathleen Russell. They explained the history cannabis and it uses, about how NCSBN had a committee conduct research, develop guidelines for nurses and education. NCSBN has been looking at regulations and implications of legal cannabis. In 2017 NCSBN charged a committee with developing guidelines for nurses and education guidelines for BON’s. Their report is currently in draft format.
The Catch Me (If You Can) presentation by Rodrigo and Claudia Garcia was an excellent lecture. I would recommend this training to the all the discipline section staff, including WHPS. They talked about the 5 factors of chance, addiction and the brain, how everyone from the employer, BON, legal, AAG, treatment facility, credentialing, and compliance have to work together and hold the diverter/addict accountable and monitored for five years and anything less significantly lowers the success rate.. The Substance Use Treatment Records lectures were interesting about legal procedures for subpoenaing 42 C.F.R protected records and updates to 42 C.F.R. BON’s may obtain the treatment records if they can show good cause to safe practice. The Reid lecture always has excellent information. This lecture was a repeat of the lecture at the BBONIT with a focus on telephone interviews, pros and cons.
NCQAC Business Meeting July 12-13, 2018
56

The Transferring Information to the Investigatory Report training was excellent despite some technically difficulties with the electronics. Also, a good training the investigators should receive. The only portion of the conference that was not up to the usual par was the Dialogue Huddles. I attended the Investigators huddle. About half of the conference attendees were present and spread out across the large room. It started out very slow and never really got into deep discussions. RECOMMENDATION: Over all I would and do recommend we continue to send staff to this conference.
NCQAC Business Meeting July 12-13, 2018
57

post-board meeting update
Letter from the PresidentLetter from the President
June 8, 2018
“Learn from the past, live in the present, plan for the future.”
Audrey Farrell
Dear Colleagues,
At the 2018 Midyear Meeting, our CEO David Benton’s address, “Past, Present and Future,” challenged us to think differently as we move from reactive and proactive to a predictive regulatory perspective model, and from a jurisdictional to a global perspective. The future clearly offers us challenges, but I believe we have the talent and the will to lead regulation as we have since our founding mothers took the bold step to form NCSBN in 1978.
The Board of Directors (BOD) met on May 7–9, 2018, in Chicago. The following is a summary of the discussions and actions of the BOD at this meeting.
ENVIRONMENTAL SCANThe BOD members, CEO and staff reported the following trends:
1. Medicinal and recreational marijuana laws continue to be introduced and enacted in states. Thirty states and the District of Columbia currently have laws broadly legalizing marijuana in some form. Eight states and the District of Columbia have adopted laws legalizing marijuana for recreational use. By the end of the summer, recreational marijuana will be legal across Canada’s provinces and territories. National legislation legalizes the sale, cultivation and use of marijuana. Age restrictions, who can sell marijuana, where you can sell or consume, etc. is left to the provinces.
2. The eNLC has been adopted in 30 states. The most recent state to pass the compact was Kansas, to be implemented in July 2019. The Commission adopted an initial set of rules to implement the compact in 2017 and will consider adoption of further rules at the Aug. 14, 2018, face-to-face meeting in Minneapolis. These rules are available for comment on party state websites and on the NCSBN webpage.
3. The use of criminal history for employment and licensure continues to be a subject of discussion by policymakers at the jurisdictional level. “Ban the Box” initiatives seek to require employers to remove from their hiring applications the check box that asks if applicants have a criminal record. State policymakers are increasingly discussing decriminalization of certain crimes for licensure purposes, including those involving drugs and alcohol.
4. Some nurses licensed by more than one board (e.g., paramedic/nurse and professional midwife/nurse midwife), and reported for violations of the law, have sought jurisdiction by the non-nursing board.
5. Changes to disciplinary appeal processes that increase the burden on nurse licensure boards are surfacing in some states. They include requirements for de novo trials in district courts. This is essentially a retrial of the case before a state judge.
6. Some health care companies are starting to shift nursing clinical services and decision making on medical care overseas, primarily to India and the Philippines. Some of the jobs being sent abroad include so-called “pre-service nursing,” in which nurses at insurance firms, for example, help assess patient needs and determine treatment methods. This conflicts with many U.S. nurse licensing laws as the location of the nurse is in a foreign country and patients are in the U.S.
1NCQAC Business Meeting July 12-13, 2018
58

7. Opioid prescribing legislation continues to be introduced in states requiring prescription drug monitoring program registration for advanced practice registered nurse (APRN) prescribers; opioid education requirements for prescribers; and limits on amount of opioids prescribed.
8. Total Triage Nurse is a company providing triage “Uber nurses” who are online nurses. It is our understanding this company only uses nurses from compact states.
GOVERNMENTAL/POLICY AFFAIRSGovernment Affairs Director, Elliot Vice reported that five new commissioners were appointed to the Federal Trade Commission (FTC). We are uncertain of the future priorities of the FTC. The Department of Justice (DOJ) is conducting round tables on occupational licensure and may be issuing guidance related to the North Carolina Dental Board decision. The Veteran’s Administration (VA) continues to rollout full practice authority in their facilities. Publication of telehealth rules by the VA will be forthcoming. NCSBN is working with the VA on a pilot project of select facilities using eNotify. A bill has been introduced in Congress that provides telehealth treatment for opioid use disorders. The Tri-Regulator organizations are working together on this legislation to assure that patient safety concerns are considered.
FINANCE COMMITTEETreasurer Gloria Damgaard presented the financial statements for the second quarter of fiscal year 2018 (FY18). The BOD accepted the financial statements for the period ending March 31, 2018. Treasurer Damgaard reported the organization continues to be fiscally sound and there continues to be a positive return on investments.
COMMITTEE REPORTSThe BOD received reports from all committees. These reports will be included in the Delegate Assembly (DA) Business Book.
2019 COMMITTEESThe BOD selected the Awards Committee, CORE Committee, Finance Committee, IRE Committee, NCLEX® Examination Committee, and NCLEX® Item Review Subcommittee to continue this year and selected one new committee, the Model Act and Rules Committee. Only five committees are seeking new members. A call has gone out to members seeking applications for these committees. Committee appointments will be confirmed by the BOD at the July 2018 meeting. Members appointed to committees will be notified prior to the 2018 DA.
The BOD has also discussed using work groups for issues that arise during the year. These groups are anticipated to provide opportunity for engagement experiences of shorter duration than a year but with greater impact. They may be appropriate for electronic participation, be more timely, be more convenient and require shorter time commitments by our members.
EXAM USER MEMBER TERMS AND CONDITIONS MEMBERSHIP AGREEMENTThe BOD considered feedback from members received at the Midyear meeting and approved a final agreement to be presented to the DA in August.
APPLICATIONS FOR MEMBERSHIPOne application for associate membership was received and determined to meet the requirements for this level of membership. Kazakhstan was recommended for associate membership to the DA. Three applications were received for exam user member (EUM). The BOD determined that the applications met requirements for this level of membership and recommended them for EUM status to the DA.
2018 DELEGATE ASSEMBLY BUSINESS AGENDA AND RECOMMENDATIONSThe BOD approved the 2018 DA business agenda and summary of recommendations to the DA. Primary recommendations include approval of the NCLEX-RN® Test Plan, approval of the Terms and Conditions of NCSBN Exam User Membership, applications for exam user membership, and application for associate membership. The BOD also received the 2018 Slate of Candidates prepared by the Leadership Succession Committee.
CORE PORTALThe Commitment to Ongoing Regulatory Excellence (CORE) Committee was charged by the BOD with creating a portal to facilitate collection of data and customized reporting of CORE data. The portal has been developed and piloted by the Committee. The BOD viewed a demonstration of the new portal. Next steps will include development of an instruction guide and video for users, followed by a rollout to members.
2NCQAC Business Meeting July 12-13, 2018
59

RESOURCE FUND POLICYThe BOD reviewed fund usage and found overall use by boards of nursing (BONs) increased from 141 requests in FY14 to 188 requests in FY17, while total expenditures increased from $229,851 in FY14 to $265,859 in FY17. The BOD moved and approved amendments to the resource fund policy that stress the need for those receiving funds to attend all meeting sessions; that the application for funding should include an attestation that alternative sources of funding have been considered; and that there should be an increase in the net funds available for this budget item.
DATA SHARING POLICIESDuring review of policies in FY17, the BOD identified that separate storage, access and use policies existed for various data sources used by NCSBN. The BOD established a workgroup of staff, BOD and legal counsel to conduct a thorough review of data policies and recommend updates to the policies.
At the May meeting, the BOD reviewed the report of the workgroup, including recommendations for data sharing policies. To minimize risk and bring clarity to how data can be accessed for NCSBN staff purposes, member use and third party access, the BOD adopted new policies and a data classification framework.
NURSYS SERVICES UPDATESThere are 57 member boards that have signed Nursys® participation agreements and share licensure data with other BONs. All these states have consented to public license look-up. Of the 57 licensure submitting members, four BONs have chosen not to participate in Nurse Licensure Verification for Endorsement (Alabama, California RN, California VN, and Pennsylvania). Michigan participation is currently on hold while the Michigan Licensing and Regulatory Agency and NCSBN continue discussion on updating their licensure data in Nursys. Hawaii has authority to participate and is reviewing the participation agreement to move forward with Nursys participation. Temporary license information is currently provided by 17 states while APRN licensing information is provided by 20 states. There are 22 states that are participating in the Nurse Workforce Repository. The e-Notify service currently has more than 5,600 active institutions and more than 815,500 nurses enrolled.
NURSE AIDE ASSESSMENT PROGRAMThe BOD considered a process for review of issues related to the NNAAP® examination, the role of nurse aides (NAs) going forward, and the regulation of NAs and determined that an extensive literature review would be performed and input from a broad stakeholder group would be initiated to inform if future changes to education, examination and regulations should occur.
LEADERSHIP PROGRAM REDESIGNAs reported following the February BOD meeting, the BOD considered the report and recommendations from Dr. Stephanie Ferguson, consultant. In particular, members identified the need to redesign the Institute of Regulatory Excellence (IRE). To this end, the BOD approved a new Regulatory Excellence Institute (REI) which will provide opportunities for regulators from diverse jurisdictions to learn, interact and collaborate. REI will be a credit-based certification program for regulators. It will be free of charge and will consist of a variety of educational options including conferences, e-learning, journal clubs, etc. Each participant will customize their overall program based upon their current needs and future goals. Staff will offer guidance. The BOD approved the initial REI program with a focus on a comprehensive package of education to support the advancement of nurse regulatory excellence.
APRN COMPACT UPDATESince adoption of the APRN Compact, three states have passed the compact into law --- Idaho, Wyoming and North Dakota. Meanwhile, Transition to Practice legislation has passed in more than a dozen states with requirements ranging from 1,000 to 10,000 hours. It is unclear how these provisions would operate under the APRN Compact. Other supervisory provisions for certain specific practice modalities also raise questions regarding how they would be treated under the APRN Compact. The BOD approved a meeting of executive officers or designees to convene this summer to consider these issues.
APRN ACUTE AND PRIMARY CARE UPDATESince the launch of the Consensus Model (CM) in 2008, some newly licensed nurse practitioners (NPs) have continued to accept employment that is not congruent with their advanced education and certification. Specifically, there are primary care NPs accepting acute care employment. The CM specifies that certified nurse practitioners are prepared to practice as primary care NPs, acute care NPs or both. Each role has separate national consensus-based competencies and separate certification processes. Scope of practice of the primary care or acute care NP is not setting specific, but is based on patient care needs. The BOD will continue to monitor regulatory implications of this issue and will consider further directions at the July BOD meeting.
3NCQAC Business Meeting July 12-13, 2018
60

40th ANNIVERSARY 2018 marks the 40th Anniversary of NCSBN. The year is being celebrated in several special ways with input from the 40th Anniversary Committee, the BOD, our CEO and NCSBN staff. These activities include:
1. Donation of $140,000 to the Foundation of the National Student Nurses’ Association, to provide scholarships to qualified undergraduate nursing students;
2. A seminal Global Regulatory Atlas, the first comprehensive resource of nursing regulation around the world, set to debut in August;
3. Publication, in cooperation with the National Forum of State Nursing Workforce Centers, of the 2017 National Nursing Workforce Survey;
4. A new NCSBN logo to be unveiled on NCSBN’s official “birthday” June 5; 5. A new NCSBN website to be launched in July; and 6. A booklet for new nurses titled “NCSBN Welcomes You to the Nursing Profession” has already been distributed as a
gift to more than 60,000 newly licensed nurses with the goal of making sure all new nurses will receive it this year.
The Annual Meeting will include a celebration of our past as we honor our founding mothers at a special luncheon. Other events will highlight a vision for the future. Members told us last year that our global focus should continue and grow. To that end, the BOD has provided scholarships for 10 international nurse regulators to join us at this meeting. The agenda will also include special presentations by two prominent international regulatory leaders.
Red is the traditional color of 40th Anniversary celebrations. Please wear RED if you are planning to attend the Awards Ceremony and Dinner during our annual meeting!
STRATEGIC OUTCOMES REPORTProgress on targets for the Fiscal Years 17–19 Strategic Plan are reviewed by the BOD at each meeting. Examples of updates reviewed at this meeting include:
• CORE Portal is complete;• The first student in the graduate experience track of the Regulatory Scholars Program completed the program and was
interviewed for the fall 2017 issue of Leader To Leader. She will use her new regulatory knowledge in her leadership role in long-term care;
• An applicant for the paid internship program was selected and will be in Chicago for eight weeks this summer assigned to a specific project;
• One Regulatory Scholar grant was funded this year; and• The Citizens Advocacy Center is reviewing the Regulation 2030 recommendations from a public perspective.
The BOD will next meet July 12–13, 2018.
We look forward to seeing you at the Annual Meeting and celebrating this momentous occasion!
Warm regards,
Katherine A. [email protected]
111 E. Wacker Drive, Ste. 2900, Chicago, IL 60601
Main 312.525.3600 | Fax 312.279.1032 | www.ncsbn.org
4NCQAC Business Meeting July 12-13, 2018
61

Washington State
Nursing Care Quality Assurance Commission NPAP REPORT
Date: 04-16-2018 to 06-30-2018
Actions Number Added
2018 Total YTD
2017 Totals
Instate Approved Programs Out of State Approved Programs
Letter of Determination: A 5 LPN Programs 26 ADN Programs 14 BSN Programs 16 RNB Programs 103 Post BSN Programs 8 Refresher Programs
18 RNB Programs 346 Other Programs 2 LPN-BSN
Intent to Withdraw Approval Conditional Approval 2 3 4 Deny Approval 2 7 4 Letter of Decision: Approval – Programs 18 40 45 Approval – Sub Change 2 5 26
Plan of Correction (POC) Required 2 4 6 Acceptance of Submitted Documents or POC
2 5 30
Additional Documents or Actions Required 20 41 53
Deferred Action 8 23 38 Removal of Conditional Approval 2 Voluntary Closure 2 Monitoring Report: Accept 8 19 16 Not Accept Student Waivers: 8 Accept 2 Not Accept Instructor Applications: Accept 1 1 Not Accept 4 Deferred 10 Complaints: Open 2 3 5 Closed 2 2 Complaint Investigation Reviewed: Action Required 3 No Action Required 1 Licensing Exemption (Waiver) Request: Exemption Request Approved 2 Exemption Request Denied 6 Refer to CMT 1
Work plan for 2018 was reviewed and updated.by both panels. Action Now, NPAP Operation Procedure Review, ARNP CRNA Licensing Edu Review, LPN and CRNA Discussion.
NCQAC Business Meeting July 12-13, 2018
62

Washington State
Nursing Care Quality Assurance Commission NAPAP REPORT
Date: 04-17-2018 to 06-30-2018
Actions Number
Total YTD
2017 Totals
Approved Programs
Letter of Determination: A 24 Healthcare Assistants 10 Medical Assistants 5 Medication Assistant Endorsement 150 Traditional Programs
Intent to Withdraw Approval 1 2 3 Conditional Approval 1 2 Deny Approval 2 5 4 Letter of Decision: Approval - Programs 4 12 16 Approval – Substantive Change 3 1 Plan of Correction (POC) Required 1 Approval / Denial of Instructor 1 Acceptance of Submitted Documents or POC
2
2
Additional Documents or Actions Required
6
15
30 Deferred Action 4 15 12 Removal of Conditional Approval 3 Program Closure 1 2 Site Visit 1 2 23 Program Director/Instructor Application:
Approval 1 1 Denial 5 Referral to CMT: 2 3 2 Complaints: Open 5 7 Closed 3 3 4 Complaint Investigation Reviewed: Action Required 1 1 No Action Required
Work plan for 2018 was reviewed and updated
NCQAC Business Meeting July 12-13, 2018
63

Washington State Nursing Care Quality Assurance Commission
Position Description Legislative Panel Purpose: To review and take positions on legislative bills on behalf of the Nursing Commission. Membership: The panel is restricted to three members plus the Chair. The chair of the legislative panel is the Vice-Chair of the Nursing Commission and assumes one of the following four positions: ARNP Member Registered Nurse Member Licensed Practical Nurse Member Public Member Duties and Responsibilities: 1. Commission vice chair serves as the chair of the legislative panel. 2. The Legislative Panel meets weekly during the legislative session. Commission staff send
the agendas to the GovDelivery at least 48 hours in advance of the meeting. Meeting agendas include:
a. Opening b. NCQAC Bill report
i. Review each bill ii. Determine position and action on each bill
iii. Weekly report on actions c. Conclusion
3. The Legislative Panel presents legislative issues to the Nursing Commission throughout
Legislative session. 4. Each member accesses the leg.wa.gov website prior to the meeting to review bills in
preparation for the meeting. 5. The Legislative Panel presents recommendations for legislative changes at every May
commission meeting. Staff: Executive Director An Associate Director Legal Manager Performance and Policy Consultant Approved: 7/06, 7/08 Revised: 6/08, 03/11, 3/15, 11/17
NCQAC Business Meeting July 12-13, 2018
64

Summary of Recommendations to the 2018 Delegate Assembly
Board of Directors Recommendations:
1. Approve the Terms and Conditions of NCSBN Exam User Membership. Rationale: The NCSBN Bylaws, article III, section 2 states, “To qualify for approval, and to maintain
membership as a Member Board or Exam User Member, a jurisdictional board of nursing that regulates registered nurses and/or practical/vocational nurses must… execute a current Terms and Conditions of NCSBN Membership, as amended from time to time by Delegate Assembly…”.
Fiscal Impact: None
2. Approve the College of Registered Nurses of British Columbia as an Exam User Member of NCSBN.
Rationale: The NCSBN Bylaws, article III, section 1c states, “An Exam User Member is a jurisdictional board of nursing that has an organizational mandate exclusively related to the regulation of the profession and protection of the public and uses the pre-licensure exam developed by NCSBN…” The Bylaws require approval of the membership by the full membership of the Delegate Assembly. The current applications for Exam User Membership meet the qualifications as stated in the NCSBN Bylaws.
Fiscal Impact: Upon acceptance, each new Exam User Member will pay a $750 annual fee.
3. Approve the College of Registered Nurses of Manitoba as an Exam User Member of NCSBN.
Rationale: The NCSBN Bylaws, article III, section 1c states, “An Exam User Member is a jurisdictional board of nursing that has an organizational mandate exclusively related to the regulation of the profession and protection of the public and uses the pre-licensure exam developed by NCSBN…” The Bylaws require approval of the membership by the full membership of the Delegate Assembly. The current applications for Exam User Membership meet the qualifications as stated in the NCSBN Bylaws.
Fiscal Impact:
Upon acceptance, each new Exam User Member will pay a $750 annual fee.
4. Approve the College of Nurses of Ontario as an Exam User Member of NCSBN.
Rationale:
NCQAC Business Meeting July 12-13, 2018
65

The NCSBN Bylaws, article III, section 1c states, “An Exam User Member is a jurisdictional board of nursing that has an organizational mandate exclusively related to the regulation of the profession and protection of the public and uses the pre-licensure exam developed by NCSBN…” The Bylaws require approval of the membership by the full membership of the Delegate Assembly. The current applications for Exam User Membership meet the qualifications as stated in the NCSBN Bylaws.
Fiscal Impact: Upon acceptance, each new Exam User Member will pay a $750 annual fee.
5. Approve the National Center for Independent Examination (NCIE) - Kazakhstan as an Associate
Member of NCSBN. Rationale: The NCSBN Bylaws, article III, section 1d states, “An Associate Member is a nursing regulatory body or empowered regulatory authority that is in whole or in part empowered by government to license and regulate nursing practice in the jurisdiction.” The Bylaws require approval of the membership by the full membership of the Delegate Assembly. The current applications for Associate Membership meet the qualifications as stated in the NCSBN Bylaws. Fiscal Impact: Upon acceptance, each new associate member will pay a $1,500 annual fee.
NCLEX® Examination Committee Recommendation: 6. Adopt the proposed 2019 NCLEX-RN® Test Plan.
Rationale:
The NCLEX® Examination Committee reviewed and accepted the report of findings from the 2017 RN Practice Analysis: Linking the NCLEX-RN® Examination to Practice (NCSBN, 2017) as the basis for recommending revisions to the 2016 NCLEX-RN® Test Plan to the Delegate Assembly. Empirical evidence from the practice analysis, feedback from the Members Boards of Nursing and the professional judgment of the NCLEX® Examination Committee provide support for the recommendation to the Delegate Assembly to adopt the proposed 2019 NCLEX-RN® Test Plan.
Fiscal Impact: Incorporated into the FY2018 budget.
Leadership Succession Committee (LSC) Recommendations:
7. Present the 2018 Slate of Candidates.
Rationale:
The Leadership Succession Committee has prepared the 2018 Slate of Candidates with due regard for the qualifications required by the positions open for election, fairness to all candidates, and attention to the goals and purpose of NCSBN. Full biographical information and application responses for each candidate are posted in the Business Book under the Report of the Leadership
NCQAC Business Meeting July 12-13, 2018
66

Succession Committee. Candidates will present himself or herself at the Candidate’s Forum on Wednesday, August 15, 2018.
Fiscal Impact:
Incorporated into the FY2018 budget. References:
A. Proposed Changes to the 2019 NCLEX-RN® Test Plan B. 2018 Slate of Candidates
NCQAC Business Meeting July 12-13, 2018
67

2018 Slate of Candidates The following is the slate of candidates developed and adopted by the Leadership Succession Committee. Each candidate profile is taken directly from the candidate’s nomination form. The Candidate Forum will provide the opportunity for candidates to address the 2018 Delegate Assembly. Board of Directors President-elect Jim Cleghorn GA Area III Paula Meyer WA Area I Director-at-Large (4 positions) Peggy Benson AL Area III Cathy Borris-Hale DC Area IV Tammy Claussen Vaughn AR Area III Ann Coughlin PA Area IV Elizabeth Lund TN Area III Mark Majek TX Area III Lori Scheidt MO Area II Sharyl Toscano AK Area I Ellen Watson VT Area IV Leadership Succession Committee Area I Member Susan Engle CA Area I Area II Member Lori Glenn MI Area II Melissa Hanson ND Area II JoAnn Klaassen KS Area II Area III Member Sandra Culpepper MS Area III Sara Griffith NC Area III Area IV Member Vacant DETAILED INFORMATION, as taken directly from application forms and organized as follows: 1. Name, Jurisdiction, Area 2. Present board of nursing position, board of nursing name 4. Application Questions:
• Board of Directors: 1) Describe all relevant professional, regulatory, and community experience. 2) What is your perspective regarding the following issues affecting nursing regulation?
a. Borderless healthcare delivery b. Regulation of nursing education c. The role of regulation in evolving scopes of practice
3) Please describe a strategy or activity to increase participation in the leadership of the
NCQAC Business Meeting July 12-13, 2018
68

organization.
• Leadership Succession Committee: 1) Describe all relevant professional, regulatory, and community experience. 2) Please describe a strategy or activity to increase participation in the leadership of the
organization. 3) Why do you want to serve in the role you are applying for?
NCQAC Business Meeting July 12-13, 2018
69

Board of Directors President-elect Jim Cleghorn, MA Executive Director, Georgia State Board of Nursing
1. Describe all relevant professional, regulatory, and community experience.
Serving as the executive director of the Georgia Board of Nursing since August 2010, I have instituted several innovative program changes to streamline regulatory processes and have taken advantage of the opportunities afforded to me through involvement with NCSBN. The executive coaching program in 2012-2013 provided a “jump start” in a broader look at regulation. As a member of the Commitment to Ongoing Regulatory Excellence (CORE) Committee from 2012 through 2014 the importance of documenting and defining the immediate outcomes of the regulatory work became clear in helping identify promising practices for public safety. In September 2014 I was appointed to the Board of Directors as Area III Director and have worked ardently to learn the essential elements of representing the membership and the organization. In 2015 I was appointed as board member liaison to the NCLEX Committee. Over the last three years I have gained a deeper understanding of the developmental process and administration of the NCLEX. Prior to my work with the Georgia Board of Nursing I served as business analyst with the Georgia Secretary of State’s Office. In that role, I worked with the agency’s Professional Licensing Boards Division to review licensure and discipline processes, identify inconsistencies and inefficiencies and recommend improvements to maximize constituent services, agency productivity and protection of the public.
My service with NCSBN has provided me with many rewarding opportunities to learn from the examples set by leaders in nursing regulation. The invaluable education and experience has
NCQAC Business Meeting July 12-13, 2018
70

enabled me to increase my personal knowledge of board operations, regulation and management principles and has challenged me to become a well-rounded leader.
Our family is very involved with our local church where my wife and I participate in various ministries and lead a Sunday School class for young couples.
2. What is your perspective regarding the following issues affecting nursing regulation?
a. Borderless healthcare delivery
The healthcare delivery system is rapidly changing and the number of patients seeking care is rising. Telemedicine has enabled providers to work to meet the new demands by expanding their practice across jurisdictional lines into other states and even into other countries. I am enthusiastic about the future of the enhanced Nurse Licensure Compact and look forward to working with boards of nursing and NCSBN to identify issues and barriers and develop solutions to ensure that our constituents continue to have access to safe and competent care through every possible delivery model.
b. Regulation of nursing education
New models of nursing education are being developed to meet the demands of an increasingly complex healthcare system. Advances in technology are changing the classroom and increasing access for interested students. Boards of nursing must work to advance regulatory structures for programs using evidence based research to maintain high quality program outcomes. This effort will require collaboration and partnerships with education programs and practice settings.
c. The role of regulation in evolving scopes of practice
As our healthcare system continues to grow and evolve, the scope of practice for nurses will have to expand to meet the increasing needs. As practice changes, we will see tasks shifted and ultimately, tasks reserved for a person who has been in nursing for many years will be performed by entry level nurses. As the nursing profession advocates for increased scope of practice, nursing regulation must be a partner in the process and work to enable nurses to practice to the full extent of their knowledge and training to ensure safe and competent care is available to all consumers.
3. Please describe a strategy or activity to increase participation in the leadership of the organization.
The National Council of State Boards of Nursing (NCSBN) provides many opportunities for individuals to explore leadership roles, develop leadership traits and be mentored by individuals
NCQAC Business Meeting July 12-13, 2018
71

with proven track records of successful leadership. I believe early engagement is absolutely essential to increase participation in the leadership of the organization. A new member who becomes aware of the importance and benefit of participation in NCSBN activities early on will learn about the opportunities available to them and be encouraged to develop and utilize their leadership skills.
Additionally, I believe that a targeted approach to identifying potential leaders may be appropriate. Each member has a unique set of talents and abilities. NCSBN may benefit from maintaining an inventory of specific education and leadership strengths for members. This inventory could be utilized to match strengths and expertise with membership needs when seeking candidates for committee appointments and other leadership activities.
Finally, the potential impact of personal encouragement cannot be understated. Encouraging members to take advantage of the numerous leadership development opportunities that are presented by the organization is essential. Truly, each member has a responsibility to work toward the future success of the organization. There are opportunities for service and leadership development at every level. It is incumbent upon the organization’s leadership to seek out potential leaders. As a membership organization, we all must be ready to identify potential leaders and help them start the leadership journey today!
NCQAC Business Meeting July 12-13, 2018
72

President-elect Paula Meyer, MSN, RN, FRE Executive Director, Washington State Board of Nursing
1. Describe all relevant professional, regulatory, and community experience.
I have 20 years experience as the executive director of the WA State Nursing Commission. I included some of the highlights below. Advanced Practice: In 1998, Advanced Registered Nurse Practitioners (ARNP) in WA had independent practice with prescriptive authority for Schedule V and legend drugs. Legislation passed allowing ARNPs prescriptive authority for Schedule II through IV drugs under a collaborative agreement. The legislation directed the Medical Commission, Board of Osteopathic Medicine and Nursing Commission to collaboratively write the rules. I lead the session and the draft rules were adopted without questions or comments. One year later, ARNPs presented research to the legislature demonstrating no increase in disciplinary cases and increased patient satisfaction. The legislature overwhelming passed removal of the collaborative agreement giving ARNPs full, independent prescriptive authority and practice. The Nursing Commission recently recognized Clinical Nurse Specialists as ARNPs. Washington is now fully compliant with the Consensus Model by including Nurse Practitioners, Certified Nurse Anesthetists, Certified Nurse Midwives and Clinical Nurse Specialists. The educational requirements listed in the Consensus Model mirror the requirements for advanced practice in Washington State. The Nursing Commission is currently developing rules for Opioid Prescribing with members of the Medical Commission, Board of Osteopathic Medicine, Dental Commission and Board of Podiatrists. Model rules have been drafted for each individual board to consider adopting in September, 2018.
Registered Nurses and Licensing Practical Nurses. In 2008, rules were adopted for continuing competency. The rules required active practice and continuing education for an active license.
NCQAC Business Meeting July 12-13, 2018
73

Washington now has a much clearer number of the nurses working in nursing. On January 1, 2018, the rules for collection of demographic data became required for active licensure. Each nurse must complete a two part survey: one question collecting ethnic data specific to Washington state; the second survey uses the E-notify registration and profile to collect data. At the end of 2018, Washington will have a full data set to use for its supply data. Increased Authority for the Nursing Commission: Using CORE data and state performance measures, the Nursing Commission was granted additional budget and personnel authority. Working in an umbrella agency, this significant increase in authority lead to increased independence. The project and report was the basis for my Fellowship in Regulatory Excellence.
2. What is your perspective regarding the following issues affecting nursing regulation?
a. Borderless healthcare delivery
Large, multistate health care organizations now require multistate practice. Large medical centers have provided multistate care to people in large regions for decades. School nurses accompany students on field trips across the United States and even to countries beyond our national borders. States along our national borders cooperate to provide medical care in the face of natural disasters. This glimpse of multistate practice confirms the necessity for nursing licenses to be portable. This portability demands a system allowing the nurse to provide care to patients regardless of location. The regulatory system needs to assure patient safety in the case of a poor outcome. The Enhanced Nurse Licensure Compact meets these requirements.
b. Regulation of nursing education
Nursing Education must meet the demands of our ever changing health care delivery system. Nurse Educators, nurse regulators and healthcare industry representatives must work together to identify knowledge and competencies necessary to prepare new nurses to provide fundamental nursing care. Educators, regulators and industry representatives need to work together to identify resources needed to address the shortage of faculty and cooperative solutions. Educators, regulators and industry representatives must work together on projecting healthcare demands of the near future to assure nurses continue their education to respond to patients’ needs. Multistate health care organizations provide care across the continuum. Initial and continuing nursing education needs to be inclusive of care settings beyond acute care.
c. The role of regulation in evolving scopes of practice
Nursing care continues to evolve and meet the ever changing demands of patient care. As regulators, we need to assure safe patient care. Regulators need to allow nursing practice to expand and not place barriers that may limit safe nursing practice. The Scope of Practice decision
NCQAC Business Meeting July 12-13, 2018
74

tree, used by many state boards of nursing, places the responsibility for professional nursing practice with the individual nurse to determine possession of necessary knowledge and competencies to safely perform nursing functions. The nurse determines if there are prohibitions in law or professional standards. The nurse determines if they are competent and safe to perform the intervention. The nurse must also possess the confidence necessary to say no if they do not possess the knowledge and competency to perform the interventions.
3. Please describe a strategy or activity to increase participation in the leadership of the organization.
Early engagement of new members nurtures new leaders. Twenty potential leaders are now new executive officers! Each year, there are new board presidents, each holding competencies necessary to provide leadership in our organization. Members express concern about the time needed to be a leader in our organization. While there is a considerable amount of time needed to invest in being leaders, the multiple rewards outweigh the investment of the time. Members possess competencies in leading meetings, recruiting and assessing stakeholder input, and conducting research to provide evidence to support regulatory decisions. Engagement includes encouraging new members to serve on committees, participate in knowledge networks, and come to meetings. Executive officers (EO) are the key to early engagement by encouraging and recruiting new leaders. EOs recognize talent and abilities in each other, in their staff and board members. NCSBN announces opportunities for service on committees each year. EOs need to identify peers, staff and board members possessing the competencies necessary to serve. EOs need to encourage people to serve and provide the resources to allow service: time, finances, and access to learning. Finances are available through NCSBN resource funds. NCSBN also financially supports the expenses for people to attend committee meetings. If time is the issue, EOs may need to communicate with board members and employers and influence them to invest in their board members and employees. The EO can also find resources to fill in for staff so they can participate in events. This allows new staff to step up and provides career progression. EOs need to be comfortable recruiting new leaders. Recruiting takes time to build a relationship, assess skills and abilities, and begin to match the emerging leader with opportunities. Recruiting requires the EO to work through anxieties expressed by the emerging leader. The new leader may just need the encouragement to serve or access to information.
NCQAC Business Meeting July 12-13, 2018
75

Director-at-Large Peggy Benson, RN, MSHA, MSN BC-NE Executive Officer, Alabama State Board of Nursing
1. Describe all relevant professional, regulatory, and community experience.
Peggy brings 39 years of experience in nursing and healthcare leadership to her role with ABN. She is a board-certified nurse executive who has worked in various executive roles in nursing and human resources. Peggy’s previous roles include Chief Nursing Officer (CNO), System Director of Critical Care and Medical Surgical Nursing over a five-hospital system, Director of Nursing for Specialty Services, and Assistant Administrator of Human Resources, Deputy Director, and Executive Officer of the Alabama Board of Nursing. She has served as a Board Member and President of the Alabama Board of Nursing, member of the Governor’s Task Force on Healthcare Improvement, Chair of the Governor’s Infrastructure Committee, board member and Past President of the Alabama Organization of Nurse Executives, past board member and Secretary for the Central District Alabama Organization of Nurse Executives, and current member of the Standards Committee-NCSBN. Extensive experience in nursing regulation at all levels.
2. What is your perspective regarding the following issues affecting nursing regulation?
a. Borderless healthcare delivery
I believe and support borderless health care and easing the burden of practice across state lines. With seamless care comes the responsibility to ensure a safe process that protects all citizens. The NLC is off to a good start and I look forward to the final development of bylaws, policies, and procedures that will define the exact structure of the compact. I have worked with many of Alabama’s healthcare leaders on telehealth issues and regulatory processes to expedite delivery of care in Alabama.
NCQAC Business Meeting July 12-13, 2018
76

b. Regulation of nursing education
I believe strongly that nursing education programs must be held to the highest possible standards and boards of nursing are in the best position to ensure those standards. A paramount issue we see in Alabama is accreditation requirements for proprietary and distance programs, which has become a national problem and priority for nursing regulation. Boards cannot ensure the rigor of programs without clear regulatory authority and standards.
c. The role of regulation in evolving scopes of practice
The ABN began addressing this issue 16 years ago with the establishment of a standardized procedure process which allows for the scope of practice to be expanded as nursing practice evolves beyond basic education. However, advanced practice nurses continue to experience difficulties in practicing to their full scope, especially in those practice settings where APRN scope intersects with the practice of other professionals. Regulatory boards working together can be a driver of change and change initiatives to ensure full practice authority. In Alabama, the pharmacy, medical, and nursing boards conduct routine tri-regulator meetings to address potential conflicts proactively.
3. Please describe a strategy or activity to increase participation in the leadership of the organization.
To create synergy and engagement, I believe the current NCSBN leadership should develop processes for member boards that include: An Executive Officer consultant group to aid struggling boards. Executive Officer engagement groups to identify issues of common concern and build a team mentality across jurisdictional lines. Revamped policy paradigm that invites participation from all member boards throughout the NCSBN planning process. This will open lines of communication, create opportunities for active participation, and develop the inclusive culture and synergy necessary to foster involvement by otherwise disengaged or inactive members.
NCQAC Business Meeting July 12-13, 2018
77

Director-at-Large Tammy Claussen Vaughn, MSN, RN, CNE Program Coordinator – Education, Arkansas State Board of Nursing
1. Describe all relevant professional, regulatory, and community experience.
I have worked at the Arkansas State Board of Nursing for more than seven years as the Program Coordinator for Nursing Education. With more than 60 nursing schools, I have site visited and provided regulatory guidance to each of them. I also have regulatory responsibility for Medication Aid Certified (MA-C) programs and International graduate licensure. Since joining the Board I have been actively involved in promoting the mission of the National Council of State Boards of Nursing (NCSBN). I served five years on the NCLEX Examination Committee (NEC) and I am currently serving my third year on the NCLEX Item Review Subcommittee (NIRSC). I have also attended and participated in many NCSBN Annual and Midyear meetings, Leadership and Policy conferences and Education Consultant round tables and conference calls. Prior to beginning my work at the Arkansas State Board of Nursing, I worked in a variety of nursing education and clinical roles. From the first day of nursing school I knew education was my passion and was determined to make it my future. Following graduation from a Baccalaureate of Science in Nursing program, I worked in the maternal-newborn clinical area before beginning my role as a nurse educator in a hospital based diploma registered nurse program. I spent many years in nursing education, teaching foundations, maternal-newborn and leadership and management. I earned a Master of Science degree in Nursing Administration and Education and also earned credentials from NLN as a Certified Nurse Educator (CNE). Throughout my nursing career, I actively participated in professional nursing associations on the state and national level, serving in many elected and appointed roles.
NCQAC Business Meeting July 12-13, 2018
78

Each of these areas of professional responsibility has enhanced my knowledge of regulation and increased my passion for assuring that nurses provide safe and effective care and the public remains protected.
2. What is your perspective regarding the following issues affecting nursing regulation?
a. Borderless healthcare delivery
Technology has played a huge role in the evolution of health care and how it is delivered. Nurses must be able to provide care through many electronic means and provide it in a safe and effective manner. NCSBN has been a leader in the discussion on telehealth and providing solutions to borderless health care delivery. Through support of the enhanced nurse licensure compact, nurses can provide care and have more mobility, while Boards continue to meet their mission of protecting the public. As technology and health care continues to become more mobile on a national and even global level, we must be quick at identifying solutions to ensure that the public is receiving safe care across all borders.
b. Regulation of nursing education
Regulation of nursing education is becoming difficult as more online and alternative programs are being implemented. Boards of nursing must work together to develop consistent strategies to evaluate programs and program outcomes, to provide the highest quality and standards for nursing education at all levels. NCSBN is in the early stages of trying to address this concern through collecting data from each Board on how program approval is completed. As the research is completed, it will be important for Boards to collaborate with NCSBN in developing standards and approval processes that are consistent and provide quality nursing education for all students.
c. The role of regulation in evolving scopes of practice
Regulation exists to ensure that the nurse functions to their full scope of practice and education, while standards are maintained to protect the public. As nursing practice continues to evolve and expand at all levels of nursing, Boards need to remain at the forefront of assuring that educational preparation is appropriate, so the public remains confident that nurses in their state are competent to perform safe and effective care.
3. Please describe a strategy or activity to increase participation in the leadership of the organization.
Strong leadership is needed in an ever-changing and fast-paced health care environment. In order
NCQAC Business Meeting July 12-13, 2018
79

to sustain an organization and maintain its viability, an organization is dependent on volunteer leaders. Although some people believe that leadership is a trait gained only at birth, I am convinced that a person can develop leadership abilities if they are truly passionate about a cause. NCSBN has so many causes to be excited about at the present time; promotion of the new generation NCLEX; the new eNLC research being done with the Education Outcomes and Metrics committee; regulations being developed by the Marijuana Regulatory Guidelines Committee; and, so much more. The NCSBN Leadership Succession does a wonderful job of getting the word out to the membership about leadership opportunities and also provides guidance towards valuable tools and resources to learn more about the organization. I think this needs to continue with added strategies to attract new leaders in the organization. Just as a marathon runner has to love running to prepare and train for a race, leaders must have the passion to want to be involved as a leader and gain more knowledge about the organization. We can attract these potential leaders, who are excited about the causes NCSBN is promoting, through identifying them early and developing a mentor type relationship. We need to engage them in discussion and empower them with the knowledge they need to grow as a leader in the organization. I’ve always been taught that the success of an effective leader in any organization is to cultivate leadership in others.
NCQAC Business Meeting July 12-13, 2018
80

Director-at-Large Cathy Borris-Hale, RN, BSN, MHA Discipline, District of Columbia Board of Nursing
1. Describe all relevant professional, regulatory, and community experience.
My nursing career spans 35 years; my greatest success has been bringing significant, positive changes to nursing practice to improve healthcare delivery in a variety of roles and settings. In 2008, I joined the executive team at SHW-Hadley Hospital as the Chief Nursing Officer and methodically rose in the ranks to become the second African American Woman appointed CEO of a District of Columbia Hospital. My work, in conjunction with the nursing directors and nurse educators, empowered nursing practice and instituted nurse directed protocols. As a consequence, the hospital experienced a 78% decrease in hospital acquired infections and zero acquired pressure ulcer rate. In 2012, I was appointed Chair, District of Columbia Board of Nursing and subsequently the Regulation and Discipline Sub-Committee. Currently as the Nurse Specialist for discipline for the D. C Board of Nursing, my work includes fostering a “just culture” and creating a forum where governmental agencies, schools and healthcare providers work together to address the needs our community. During the 2017 delegate assembly, I served as Chair of the Resolutions Committee. I am an active member of NCSBN’s Medical Marijuana Regulatory Guidelines Committee which is commissioned to develop guidelines for nurses, make recommendations for education, and establish guidelines for Boards of Nursing as well as explore trends related to marijuana use and its relationship to nursing regulation.
2. What is your perspective regarding the following issues affecting nursing regulation?
a. Borderless healthcare delivery
Technological advances in the areas of communication and medicine provide a previously unimaginable path to improving health care across the nation and globally. Researchers and providers now have an opportunity to share knowledge that will enhance health care safety and delivery previously only dreamt about. The formation of such partnerships will potentially reduce
NCQAC Business Meeting July 12-13, 2018
81

replicating, identify best practices, and bring high-level, evidence based care to patients in under served areas of our nation and world. Nursing regulators need to be forward thinking and create regulations which allow for expanding roles but ensure safe care for the public.
b. Regulation of nursing education
Since the role of the nurse is crucial to the health of our communities and the care of the ill, it is imperative that nursing education has a minimum standard of academic rigor from all institutions. How can we truly protect the public and the profession if Boards don’t hold schools of nursing accountable for providing the highest quality nursing education and instituting guidelines for nursing practice and nursing assistant personnel practice regulations. Our community is entitled to safe and compassionate care and high standards of practice.
c. The role of regulation in evolving scopes of practice
Nurse’s role in healthcare has been a topic of discussion for policy-makers, health-care reform activist for as long as modern nursing has existed. With the changing landscape and push for healthcare reform, nursing is in a position to make huge strides in improving access, decreasing cost and improving outcomes. Regulators play a key role in protecting the public as well as advancing the scope of nursing by making meaningful regulatory amendments, removing ambiguous language and supporting the use of the “Scope of Nursing Practice Decision-Making Framework” tool to determine if a specific task falls within the state’s licensing laws.
3. Please describe a strategy or activity to increase participation in the leadership of the organization.
Identifying opportunities for state board members and/or staff to engage with the organization, may be useful in recruiting emerging nurse leaders who could be instrumental in implementing meaningful change and their successes shared with the membership.
Organizational change meets with success when leaders recognize efforts must include cultural changes and as complete participation as possible from all holders. In order to achieve meaningful and lasting cultural change, a robust plan that includes specific goals, establishes methods to meet them, and strategies to create interest and participation. One such way would be to create leadership training workshops for your non-traditional nurse leaders
NCQAC Business Meeting July 12-13, 2018
82

to gain insight into the skills they possess and how they can use these to lead in their personal and professional life.
NCQAC Business Meeting July 12-13, 2018
83

Director-at-Large Ann Michelle Coughlin, RN, MSN, MBA Vice Chair, Pennsylvania Board of Nursing
1. Describe all relevant professional, regulatory, and community experience.
I have over 24 years’ experience in the healthcare industry; including a clinical nurse in an acute care hospital, case management supervisor in the insurance industry, triage nurse for a disease management company, clinical nursing supervisor for a large university hospital and a nurse regulator. My previous position as a Regulatory Affairs and Compliance Auditor for a large Mail Order Pharmacy, Specialty Pharmacy and Infusion Company demanded a focus on regulations. My Supervisory position in Regulatory Affairs has enhanced my knowledge and experience with regulations for the past 8 years. My role as an Internal Auditor required review of regulations for individual states as well as review of federal regulations. My current role as Manager for the department of Patient and Family Experience at an academic medical center has broadened my knowledge in patient safety, satisfaction, quality of care and risk management.
I was honored to be appointed to the Pennsylvania State Board of Nursing in 2010 and to be named Vice-Chair 2012 and Chair for 2013 & 2014 term. In addition, I served on the following committees: IT, Finance, Probable Cause and Application Review. For three years I served on the Leadership Succession Committee (LSC) for NCSBN. I also have served on the NCLEX Item Sub-Review Committee. I am dedicated to continuing my commitment and passion for regulation in order to enhance and support the development of regulation and the role of nursing in the healthcare environment. I look to support NCSBN and will lend my diverse experience and knowledge to support the mission and vision. It would be an honor to continue to serve with the talented group of professionals to identify and nurture leadership in nursing that is pivotal to the advancement of nursing regulation and safety of the public.
2. What is your perspective regarding the following issues affecting nursing regulation?
NCQAC Business Meeting July 12-13, 2018
84

a. Borderless healthcare delivery
Border Technology and innovation is driving treatment options in the healthcare market. Virtual tools to monitor and maintain health are popular items utilized across the world. Also tele health and tele rounding are utilized in many venues and impact borderless delivery. We will continue to see tremendous growth with technology and borderless delivery. We need to work together to maintain high standards and regulations. Borderless healthcare will assist with the collaboration the ability to share resources, information and knowledge. Borderless healthcare will need to be monitored and closely regulated in order to maintain patient safety. In the current healthcare market I think borderless healthcare delivery is vital, important and will continue to expand across the globe. Policymakers, stakeholders and practitioners need to work together to implement creative solutions when crossing borders. The need for expanding healthcare access continues to grow so we need to think on a national and global level to stay progressive in the efforts to address borderless healthcare delivery.
b. Regulation of nursing education
I think we need to regulate nursing education. We need to maintain quality, evidence based practice, high standards of education and ongoing nursing research. Nurses need to hold one another accountable for safe patient care and to high standards of practice. Nurses need the ability to practice to their full scope of authority. Boards of Nursing, nursing schools, nursing programs, regulators and accreditors all need to work together to maintain the highest standards of nursing education. We need to be collaborative, creative and innovative to protect the safety of the public and maintain the highest standard with nursing education.
c. The role of regulation in evolving scopes of practice
I have had exposure to the issues related to education and nursing regulation with the Pennsylvania Board and NCSBN. NCSBN is very involved and leading the required collaborative efforts that are necessary between regulators and accreditors. The RN Model rules are an excellent example of representation of this endeavor. The current work involving distance education should be embraced by regulators to meet the IOM initiative for nurses to advance their education. We need to continue to work together to develop the best practice standards and to assist all states with implementation of them. A key part is education and communication; we all need to be respectful to concerns of the individual states as well as support initiatives, goals and national standards to promote evolving scopes of practice.
3. Please describe a strategy or activity to increase participation in the leadership of the organization.
NCQAC Business Meeting July 12-13, 2018
85

The members of the NCSBN are de facto people interested in nursing and the promotion of the highest standards of our profession. Therefore, it seems evident that they possess the qualities necessary for a leader. They are committed to the profession, they are interested in shaping the direction and values of our organization and they are bright, caring and dedicated individuals. Many of us certainly qualifies for a leadership post. So why are so few of us running? I think each of us may have our own reasons and perhaps going forward we would like to conduct a survey, as we have done in the past, to assess those reasons, but in the meantime, we may want to implement a few novel strategies to improve participation in our electoral process. I suggest we engage each state board to identify members who may be interested in pursuing a leadership position at the national level. We should then work with the state board to nurture and prepare new leaders, providing education, mentorship and support to promote their involvement in elections and leadership roles. Creating a leadership institute comparable to our research institute to engage ‘fellows’ who would be interested in developing leadership skills by participating in an ongoing mentorship program would also be an initiative to encourage participation in leadership roles. Finally, I think that we need to empower LSC to assist members interested in running in preparing and organizing their campaigns. Standardizing the process would also create a more equal playing field for candidates. Members could then delineate the information they want to make a decision and determine the process for disseminating that information. Our goals should be to create as non-political a process as possible for our elections. I thank you for your attention and look forward to working together.
NCQAC Business Meeting July 12-13, 2018
86

Director-at-Large Elizabeth Lund , MSN, RN Executive Director, Tennessee State Board of Nursing
1. Describe all relevant professional, regulatory, and community experience.
My regulatory experience began thirty-three years ago when I was appointed executive director of the Tennessee Board of Nursing after nine years in academic nursing. I took the first opportunity to volunteer for an NCSBN Committee, appointed to the Bylaws Committee where I served six years, four as chair. During that tenure, the committee accomplished the first comprehensive revision of the bylaws that positioned NCSBN to more nimbly respond to changing environments, allowing greater participation by members through special committees. Later I chaired the Regulation Subcommittee that examined the existing model of nursing regulation. After considering such models as a federal/national model and “fast” endorsement, the committee proposed a new mutual recognition model, beginning the journey that led to the interstate nurse licensure compact. Later, I chaired the Anniversary Planning Committee which started the tradition of an evening gala event that has served as a cherished model for subsequent anniversary celebrations. I have served on all the subsequent anniversary committees. Other committee service includes the Finance Committee, Awards Panel and co-lead of the executive officer group. More recently, I chaired the Executive Officer Succession Resource committee which produced a flexible online toolkit that has been used successfully by a number of boards to assist with leadership transition. I have volunteered as a mentor for many executive officers. I served as treasurer of the executive committee of the Nurse Licensure Compact Administrators and a member of the e-NLC Workgroup. In 2015, I was honored to be awarded the Meritorious Service Award. Currently, I serve on the NCSBN Board of Directors as a Director-at-Large and serve as liaison to the Standards Development Committee.
2. What is your perspective regarding the following issues affecting nursing regulation?
NCQAC Business Meeting July 12-13, 2018
87

a. Borderless healthcare delivery
Partnerships with national and international colleagues heighten our appreciation that we share the common goal to deliver healthcare more safely and efficiently irrespective of borders. We recognize the value in congruent standards that flow from and are consistent with our overarching statutes and rules. Importantly we share knowledge, experience and resources and gain synergy from our efforts. As nursing regulators we face challenges to occupational licensure itself. It is imperative that we cross both physical and professional borders to make an evidenced case for professional licensing that can meet our common purpose to protect the public.
b. Regulation of nursing education
With a continuing rise in schools struggling to achieve their mission and boards challenged to regulate from an evidence informed base, it is vital to foster research efforts comparable in quality and usefulness to the landmark NCSBN Simulation Study. I support NCSBN’s current nursing education study to identify evidence-based red flags and regulatory quality indicators. The results will provide much needed data to support school approval processes and reduce reliance on NCLEX pass rates as a sole measurement of education quality.
c. The role of regulation in evolving scopes of practice
Nursing regulation has an ethical duty to support the provision of care by those qualified at every point along the caregiver continuum when grounded by sound evidence. Studies demonstrate that APRNs provide care equivalent to that of physicians. RNs and LPN/LVNs must be more effectively utilized to practice to the full scope of their education, harnessing the capabilities of these licensees to participate more fully in improving health outcomes. We must critically examine traditional models and build safe models for our burgeoning population of patients, many of whom would prefer to receive care at home or electronically.
3. Please describe a strategy or activity to increase participation in the leadership of the organization.
First, I believe that leadership in NCSBN does not equate with elected office; however, the goal to serve in an elected capacity is facilitated by taking full advantage of the leadership development opportunities available. One opportunity is committee membership. It is encouraging that members wish to participate in committees and my observation is there are ever more qualified members. Members report that it is frustrating to desire to serve and not be selected for limited slots on committees. These committees provide leadership opportunities that serve as a foundation for elected office. I suggest developing an open ended leadership inventory of members to form a database of willing members and their expertise. The inventory database has
NCQAC Business Meeting July 12-13, 2018
88

potential to level the playing field between new members seeking opportunity and those experienced leaders whose expertise is well known. Members would be encouraged to register in the database and these interested volunteers could form an identified group for leadership promotion activities. The inventory database would serve as a resource to match qualified applicants when leadership opportunities arise. Being elected to and serving on the Board of Directors is an honor. Experience in a broad array of NCSBN activities, committees as well as attendance and participation in meetings and conferences, provides invaluable leadership preparation and opportunity.
NCQAC Business Meeting July 12-13, 2018
89

Director-at-Large Mark Majek, MA, PHR, SHRM-CP Director, Operations, Texas State Board of Nursing
1. Describe all relevant professional, regulatory, and community experience.
Special Services Division Group, 1994; Delegate Assembly Page, 1995-2000; Licensure Verification Task Force, 1995-1997; Licensure Verification Task Force, Chair, 1996-1997; Information System Users Group, 1998-1999; Phase II User Group Nursys, 1999-2000; Nursys Advisory Panel, 2000-2001; NCSBN Board of Directors, Area III Director, 2001-2005; Member Board Leadership Development Advisory Panel, 2006-2007; Finance Committee, 2008-2011; Leadership Succession Committee, 2012-2015; and, Bylaws Committee, Chair, 2015-2017. Professional Organizations: Society for Human Resource Management Texas State Human Resources Association Texas Small Agency Task Force, Chair Community Involvement: Marbridge Foundation, Volunteer Knights of Columbus Council 10209, Austin, Texas
2. What is your perspective regarding the following issues affecting nursing regulation?
NCQAC Business Meeting July 12-13, 2018
90

a. Borderless healthcare delivery
As barriers to borderless healthcare delivery dissipate, the question of quality must be addressed as to market access, regulation, standards, and information security. This is one area where regulation is lagging due to the rapid advances in telehealth and technology. As regulators, we are addressing some of the issues with the eNLC and NURSYS. The driver for borderless healthcare delivery will be how nurses are prepared to cross borders with their knowledge and experience and how we hold nurses accountable and protect all citizens. This could be addressed by the NCLEX or other national nursing examinations, which drive nursing education.
b. Regulation of nursing education
There is tension regarding the oversight of nursing education between boards of nursing and policy makers. It is a tug-o-war of quality versus quantity and the pendulum swings between the two depending on costs and NCLEX pass rates. Finding a balance will be important as the complexity of nursing practice increases and is reflected in the NCLEX. There is a “caveat emptor” system in place for most healthcare disciplines, when it comes pass rates. Nursing Regulators must continue to provide evidence of the importance of quality factors which impact NCLEX pass rates and are vital to public protection.
c. The role of regulation in evolving scopes of practice
The role of boards of nursing is to seek out partnerships with healthcare associations, schools of nursing, public organizations and policy makers to forge common ground based on research and healthcare outcomes. We should focus on all levels of nursing and the NCSBN should be leading in research on how the appropriate expansion of scopes of practice would benefit citizens and drive down the cost of healthcare. As contentious as this may be, boards of nursing are key partners in the success of defining and pushing the envelope on this issue and need to be at the table as these discussions take place.
3. Please describe a strategy or activity to increase participation in the leadership of the organization.
Develop a formal mentorship program that creates a pool of seasoned NCSBN members such as current and former directors, committee chairs, and executive officers who can mentor prospective leaders on a one-to-one basis for up to one year. This program should also include the resources to allow prospective leaders to attend one delegate assembly and one board of directors meeting to be exposed to the dynamics and environment of the NCSBN. You must understand the NCSBN culture to be a successful leader in the organization and this strategy could form a cornerstone in building a stronger succession plan.
NCQAC Business Meeting July 12-13, 2018
91

Director-at-Large Lori Scheidt, MBA-HCM Executive Director, Missouri State Board of Nursing
1. Describe all relevant professional, regulatory, and community experience.
Lori Scheidt is the Executive Director of the Missouri State Board of Nursing, a position she has held since 2001. Prior to that, she served as the Board’s Licensure Director and has performed almost every position within the board office during vacancies. Ms. Scheidt earned an Associate in Arts from Columbia College in 1997, a Bachelor of Science in Computer Information Management from William Woods University in 2000 and a MBA in Healthcare Management from Western Governors University in 2012. Ms. Scheidt is finishing her first two-year term on the NCSBN Board as a Director at Large. Prior NCSBN service: Vice Chair, Nurse Licensure Compact Administrators 2012-2016 Fraud Detection Committee - Chair – 2015 Enhanced NLC Legislative Strategy Team 2015 Member Board Agreement Review Committee – Chair - 2013 Discipline Effective Practices Subcommittee – 2014-2015 Nurse Licensure Models Committee - 2011-2012 Awards Panel - 2004-2006 CORE Committee- 2005 Nursys Advisory Panel - 2003-2004 Test Service Technical Subcommittee - 2001-2002 Examination Committee - 1997-2000 NCLEX Evaluation Task Force - 1996 Committee for Special Projects (CAT) – 1995 IT/Operations Conference - Speaker – 2014, 2013, 2012, 2007 NCSBN Mid- Year Meeting – Speaker – 2016, 2015, 2013, 2011
NCQAC Business Meeting July 12-13, 2018
92

NCSBN Annual Meeting – Speaker – 2015, 2013 NLCA Meeting –Speaker – 2016 AWARDS: NCSBN Outstanding Contribution Award – 2001
Missouri Board of Nursing awarded the NCSBN Regulatory Achievement Award – 2012 Missouri Governor’s Award for Quality and Productivity for significant improvements in nursing investigations – 2004
2. What is your perspective regarding the following issues affecting nursing regulation?
a. Borderless healthcare delivery (100 words or less)
NCSBN has built a solid foundation to move ahead of the regulation curve in this area by committing significant resources to enact the enhanced nurse licensure compact in all states. Their presence in Washington, DC and strong alliances with key stakeholders will serve the organization and its’ members well. NCSBN’s strategic initiative to champion regulatory solutions to address borderless health care delivery requires us to be well-informed about technology, how that interacts with our regulatory model, and how we may need to adapt our regulatory framework without sacrificing our public protection mission.
b. Regulation of nursing education (100 words or less)
NCSBN has invested in committee work and research that addresses the regulation of nursing education programs. The NCSBN National Stimulation Study provided critical information for an expert panel to make evidence-based recommendations for simulation in prelicensure nursing programs. Without a doubt, nurses need and demand flexible educational systems that promote seamless academic progression. Member boards struggle with faculty shortages, evaluating the effectiveness of online education, and lack of appropriate clinical facilities. NCSBN must continue to embark on relevant research to provide the evidence member boards need to make sound regulations. Changes in the health care system and practice environments require changes in education. We have to adapt to this evolving and complex health care system with a careful balance of flexibility and regulations that allow the profession to evolve while protecting the public.
c. The role of regulation in evolving scopes of practice (100 words or less)
The patchwork of varying scope of practice and borderless healthcare make it difficult for patients, practitioners, employers and payers to navigate. To further complicate matters, boards of nursing are creatures of statute and can only enforce state laws, as they exist. NCSBN has worked with key
NCQAC Business Meeting July 12-13, 2018
93

organizations to develop the APRN consensus model. The consensus model work rightly focuses on citing research on the safe, cost-effective, high-quality care delivered by APRNs and how the model will benefit public safety. NCSBN needs to continue seek solutions that are rooted in evidence and keep the spotlight on patient safety.
3. Please describe a strategy or activity to increase participation in the leadership of the organization.
I remember when I was new to the board of nursing and the NCSBN and can understand how overwhelming it may be to balance your duties to your own board with your desire to participate on a national level. I think the NCSBN Orientation Roadmap is a good start, followed by joining the knowledge networks tailored to your subject matter expertise or job role. By joining the knowledge networks, you will be informed of conference calls so you can participate in the various networking opportunities and collaborate with your peers. I have learned so much by just talking to my peers and finding out how they do things, what has worked, what hasn’t and hearing different perspectives. It also allows you to develop relationships. Attending NCSBN-offered meetings is another way to develop relationships and learn from others. There is also a wealth of online courses available on the learning extension site, but it may be hard to figure out where to start. Having a guide of courses tailored by role or expertise could be helpful. The next logical step is to volunteer to serve on committees or provide input to committee work (even if you aren’t a committee member). The famous quote, “None of us is as good as all of us.” is so very true. The NCSBN has a leadership assessment tool and self-inventory of competencies that can be helpful to identify your strengths and opportunities. I believe it is helpful to participate before you lead. To be a leader, you need to realize you can make a difference, you can grow, and you need your colleagues. It takes all of us to make this organization and our work successful.
NCQAC Business Meeting July 12-13, 2018
94

Director-at-Large Sharyl Toscano, PhD, MS, BS, RN-CPN RN Member, Alaska State Board of Nursing
1. Describe all relevant professional, regulatory, and community experience.
I have been a RN for 24 years. I have worked in Massachusetts, Hawaii, Vermont and now Alaska. I was appointed to the Alaska BON on 3/1/2015; I have served as Vice Chair and Chair of that Board. I am serving my second term on the NCSBN CORE Committee. My RN experience currently focuses on inpatient pediatrics, low level PICU, and level II NICU. Alaska Native Medical Center exist as an urban hub providing specialty services and trauma care to rural areas throughout Alaska. I serve the Alaska Native Customer Owners. I am committed to strength based; family focused and culturally centered care. I have been a nursing faculty member for 18 years and currently hold the rank of Professor. I have taught in undergraduate and graduate programs. My program of research focuses on Women’s Roles, Relationships, and Health. Special projects within my faculty role have focused on undergraduate program evaluation. I currently serve locally on the Narcotic Drug Treatment Center Board and the Winterberry Charter School Board. Although I have trained and practiced as a FNP, I found my heart was at the bedside and my commitment is to the RN role. There are many talented members on the board of directors most often from board staff or APRN roles. I am committed to keeping a national focus on the RN role, believe in BS entry to practice and feel the board of NCSBN should include balanced representation.
2. What is your perspective regarding the following issues affecting nursing regulation?
a. Borderless healthcare delivery
I believe nurses should hold a license and/or compact license privilege in the state where the patient is located. In the state of Alaska, patients have unique needs. Patients have suffered where a one size fits all approach has been applied from a state having no knowledge of our population and/or our needs. I do not feel this is unique to Alaska. Alaska has also benefited from the advantages of telehealth specialty services. In a service industry where quality is a
NCQAC Business Meeting July 12-13, 2018
95

hidden factor; regulation is in place to ensure quality and safety.
b. Regulation of nursing education
I feel nursing education has departed from core values. There are so many and to obtain both entry and advanced practice. Quantity rather than quality has been the focus. We need to broaden our focus beyond pass rates. We need to move to BS entry to practice and facilitate bridge program but those bridge programs should not exist as a permanent path to entry. The bridge should be just that, a bridge until the BS entry is realized.
c. The role of regulation in evolving scopes of practice
The APRN role has inadvertently created a ceiling for the RN where the RN role might have naturally expanded. There are clearly things that are APRN roles but not all expanded scopes require APRN certifications. The two are not mutually exclusive. On the other hand nurses are requesting expanded scope in areas that are not nursing. Allowing those expansions gives the consumer a false sense of security where being a nurse is not an added quality factor. Regulators need to keep up with professional practice organizations such that the limits of practice are safety related and not territorial.
3. Please describe a strategy or activity to increase participation in the leadership of the organization.
I do not know what has been done up to this point so I would suggest beginning with an appreciative inquiry approach and have no preconceived notion regarding the outcome of that inquiry.
NCQAC Business Meeting July 12-13, 2018
96

Director-at-Large Ellen Watson, MS, APRN, FNP-BC Chair, Vermont State Board of Nursing
1. Describe all relevant professional, regulatory, and community experience.
Regulatory Experience I was appointed to the Vermont Board of Nursing in 2011 and reappointed in 2017 Chair of the Alternative to Public Discipline Committee since 2013 Vice Chair of the Vermont Board from September 2014 until September 2017 I am now Board Chair, elected September 2017 Serving on the Vermont BON Education Committee I served on the NCSBN APRN Committee that looked into grandfathering of APRNs I served on the Leadership Academy Committee I served as Area IV Director from 8/2015 to 8/2017. In that role, I attended many conferences and other events focused on Regulation. For example, I attended two Tri-Regulator Symposium meetings, Regulation 2030, many NCSBN events and traveled with CEO David Benton to visit our Associate Member in Manitoba last May. I was liaison for the APRN Education Committee that was charged with looking Member Board regulation of APRN programs. (NOTE: I loved this work and would have happily run for a second term, but my real job had a dramatic, but temporary increase in responsibility that made it impossible to adequately fulfill the duties of an NCSBN Board member. Those extra duties are ending and I will be able to do this once again. I feel that one term allowed me to learn all that I need to so that I can be of even greater service.) I love this work. I am in the second year of the IRE Fellowship Program Other Relevant Experience I am a Family Nurse Practitioner. I see patients in a Primary Care Clinic for half of my work week and teach at the University of Vermont during the other half. I serve on the Graduate Education Committee and participated in the preparation for accreditation visits for our new DNP Program, as well as re-accreditation of our undergraduate program, ADN to BSN Program and Clinical Nurse Leader Program. I serve on the Green Mountain Care Board Primary Care Advisory Committee Have been a member and chaired many other organizations over the years, in jobs, membership organizations and in the general community Opportunity is missed by most people
NCQAC Business Meeting July 12-13, 2018
97

because it is dressed in overalls and looks like work. Thomas Edison
2. What is your perspective regarding the following issues affecting nursing regulation?
a. Borderless healthcare delivery (100 words or less)
The goal of borderless healthcare delivery has become more and more important, as developments in technology and changes in the workforce mandate the need for greater flexibility and dynamic problem solving to meet the needs of an aging population with complex chronic illnesses that demand new models of care delivery. Team-based care is required to meet the needs of so many and to achieve the best outcomes. And team members can be in the office, or the city or the state next door.
b. Regulation of nursing education (100 words or less)
Nurse regulators have a unique perspective and a singular primary purpose. We work to protect the public and ensure that nurses, from their initial education and licensure, to their continuing education and renewals are safe and professional. Nursing education programs are evaluated and re-evaluated periodically, in the hope of ensuring high standards in nursing education. This accreditation work may well lead to enhanced public protection, but without the eyes of the regulator also looking into programs, the foundation of any nurse could be deficient. This is a key component of nursing regulation, in my opinion.
c. The role of regulation in evolving scopes of practice (100 words or less)
It is essential that regulators stay current with the evolution of all aspects of practice. The IOM Report on the Future of Nursing, the IHI Chronic Care Model and Initiatives along with other robust and forward thinking organizations have promoted the idea that everyone in healthcare needs to rise to the challenge of working at the top level that their licensure allows. This will provide for improved access to care as well as some degree of cost containment by using teams of caregivers with differing skill sets to provide comprehensive healthcare. Regulators need to be able to reframe Statute and Rules to allow this to happen and to appreciate the questions and issues that are sure to arise. We need fresh perspective and new eyes to assure that scopes of practice and regulations truly offer the opportunity for right touch regulation that protects the public and allows for growth.
3. Please describe a strategy or activity to increase participation in the leadership of the organization.
Leadership and learning are indispensable to each other said John F. Kennedy, in Dallas, on the
NCQAC Business Meeting July 12-13, 2018
98

day he died. We need to provide more opportunities for the membership to learn about leadership and to practice being a leader. I believe that people will never gravitate toward leadership positions unless they feel qualified and competent to take on the task. Many people are gifted with natural leadership abilities, but they often need to learn how to harness them and use them in various situations. Sometimes, they just need to be made aware of the talents they have. I served on Leadership Academy Committee. And while I don’t feel committed to the plan or curriculum that was put forth from that group, I like the idea of a leadership academy for the NCSBN membership. This sort of program would need to be self-paced, on-line, not duplicative of existing leadership training and promoted to both Board Executive Officers and staff and to Board members. I think an important task of any activity to increase participation in NCSBN leadership is to make it more accessible. The idea of taking on a leadership position in this organization can be challenging and even frightening. Perhaps mentors could be offered. A leadership online journal might be a way to make stories of NCSBN leadership journies available and the process less daunting. I would love to work on this type of a project.
NCQAC Business Meeting July 12-13, 2018
99

Leadership Succession Committee Area I Member Susan Engle, DNP, MSN, BSN, PHN Nursing Education Consultant, California R-N
1. Describe all relevant professional, regulatory, and community experience.
I hold a Doctor of Nursing Practice Healthcare Systems Leadership degree with Distinction from Chamberlain University, College of Nursing (2016), Masters of Science in Nursing and a Bachelors of Science Degree from California State University, Dominguez Hills. I am a Nursing Education Consultant for the California Board of Registered Nursing. I was Associate Dean, Director of pre-licensure RN program and professor at Napa Valley College. Prior to academia, I held leadership positions that included clinical nursing director, manager, supervisor and charge nurse. I am a member of Sigma Theta Tau, California American Nurses Association, Association of Clinical Nurse Leaders. I was a member of the Nursing Education work group that developed the proposed regulations for nurse practitioners.
2. Please describe a strategy or activity to increase participation in the leadership of the organization.
Many strategies are cited in the literature that could be used to increase participation in the leadership of the organization. Some strategies include application of leadership styles to influence potential leaders, communicating positively about the leadership position, and role modeling. Role modeling is one strategy that I have employed in my role as a nursing education consultant, Associate Dean, director of a pre-licensure nursing program, professor, and Clinical Nursing Director.
NCQAC Business Meeting July 12-13, 2018
100

When role modeling, leaders need to exhibit leadership skills, knowledge, abilities, and attitudes. These leadership skills or competencies include effective communication methods, conflict management, integrity including trust, and flexibility. These skills are essential for an effective leader to influence future leaders. My role modeling as a leader has influenced many of my colleagues to assume leadership positions. Recently, I attended a White Coat Ceremony for a colleague of mine who is completing their Master’s degree with an emphasis as a Clinical Nurse Leader. The student in the graduate degree program was a student that I taught in the pre-licensure nursing program. As a nursing education consultant, role modeling is used with every encounter such as speaking with constituents, program directors, or board members. As a member of the Leadership Succession Committee, role modeling will be important to retain and recruit leaders.
3. Why do you want to serve in the role you are applying for?
I want to serve in the role on the Leadership Succession Committee (LSC). The LSC committee members are charged to assist the National Council State Boards of Nursing (NCSBN) to ensure that the mission of the council is met. In addition, to ensure that there are leaders to carry on the NCSBN mission. The NCSBN mission is to provide education, service, and research through collaborative leadership to promote evidence-based regulatory excellence for patient safety and public protection (Adopted by Delegate Assembly 2010). As a member of the LSC, I will be able to demonstrate effective communication, leadership, critical thinking and public policy. The skills, attitudes, and abilities that I possess have been gained through my academic degree progression, my leadership positions held in both clinical practice and academia and as a Nursing Education Consultant for the California Board of Registered Nursing. I possess many of the leadership competencies addressed in the Self-Inventory: Leadership Competencies. I aspire to learn more about the NCSBN and how I can assist in protecting the public in relationship to the mission statement. I am willing to take on new opportunities that will influence my professional trajectory as a Registered Nurse. Thank you for considering me to be elected to serve as an Area I member of the Leadership Succession Committee for a one-year term FY19. I look forward to serving on the Leadership Succession Committee.
NCQAC Business Meeting July 12-13, 2018
101

Area II Member Lori Glenn, DNP, CNM, RN Leadership Succession Committee, Michigan Board of Nursing
1. Describe all relevant professional, regulatory, and community experience.
Lori Glenn has been a member of the Michigan Board of Nursing since 2017. She is an associate clinical professor of nursing at the University of Detroit Mercy, where she has served as chair of the Second Degree Option BSN program since 2013. In that role she has educated prelicensure students and developed programs that enhance NCLEX success. Dr. Glenn has been active at the both the college and university levels, as member and chair of several bodies that contribute to decision making about leadership roles at the University. These include the university faculty assembly, promotion and tenure committee, and faculty/dean search committees. Dr. Glenn has also played an active role in regional organizations committed to improving the nursing care of mothers and neonates. She has been consulted to provide expertise on legislation surrounding the licensure of non-nurse midwives in the State of Michigan. Dr. Glenn also practices part time as a Certified Nurse Midwife in Flint, Michigan, where she has contributed to establishing a robust midwifery practice and enhancing the hospital quality and safety.
2. Please describe a strategy or activity to increase participation in the leadership of the organization.
The participation in the leadership of this organization would be enhanced if leaders continue to reach out and illustrate the importance of contributing to the future of NCSBN. As a new member, I was so impressed with the history and accomplishments of the organization over the past 40 years, I was inspired to apply for this position. Perhaps sharing the 40 year presentation that was shown at the Mid-Year meeting with members across the country, and enhance this with personal stories from those leaders who have made an impact would inspire others. I recommend continuation the email campaign to attract new leaders. Tony Graham’s video and presentation at
NCQAC Business Meeting July 12-13, 2018
102

the Mid-Year meeting were also great strategies. Coming from a board that is populated with busy people, reaching out to members using alternative attendance through online meetings would give others greater flexibility to participate.
3. Why do you want to serve in the role you are applying for?
Over the past 40 years, the NCSBN has grown into a powerful organization that contributes significantly to the profession of nursing. I have been dedicated to educating pre-licensure nurses for 10 years, including leading a successful effort to enhance NCLEX preparation. I would welcome the opportunity to have a greater impact though selecting leaders who will contribute to unifying and enhancing the regulation and licensing of nurses. As new nurses come into the profession, we are required to be nimble in our response to their learning needs and novice abilities in practice. Bridging the gap between nurse education and regulation is vital to developing nurses who are first and foremost safe, providing quality care and yet staying committed to nursing in a challenging health care environment. Advanced practice nursing is facing issues with resistance from medicine who continues attempts to marginalize and restrict practice without evidence that care inferior. Regulation of APRNs is more important than ever, to ensure quality, address disciplinary issues, and demonstrate their abilities and worth. As regulation evolves, and we face chaotic times in health care, it is vital to have leaders that can protect our current status and guide us toward advancing the nursing profession. Not only do leaders need to be well versed in the laws, rules, and policies relevant to the profession, they must be able to speak to the issues articulately, effectively, and with passion. As I continue to develop my knowledge and understanding of the many aspects of the Michigan Board of Nursing and NCSBN, I feel my 31 years in nursing, 25 in nurse midwifery, and 10 in nursing education I will provide a vital perspective on the many challenges facing the nursing profession that will inform the leadership needs of the organization.
NCQAC Business Meeting July 12-13, 2018
103

Area II Member Melissa Hanson, MSN, RN Associate Director for Compliance, North Dakota State Board of Nursing
1. Describe all relevant professional, regulatory, and community experience.
I have been an RN since 1993 (almost 25 years). I have hospital nursing experience in the areas of Neonatal Intensive Care, Dialysis, Diabetes Education, and Case Management. I received a Master’s Degree in Nursing Management in 2006. With this degree I taught nursing at a BSN nursing program for 9 years. During these years of teaching, I also worked, during school breaks, at a Walk-In Clinic, and as a contracted Health Coach. This varied experience has provided me with knowledge of hospital nursing, clinic nursing, health care reimbursement, case management and discharge planning, as well as experience in academia. I have 8 years of experience in nursing regulation. I first became involved with the North Dakota Board of Nursing in 2010 when I was accepted as a member of the Nursing Practice Committee. I served on this committee from 2010 to July 2014. In July 2014, I was appointed by the Governor of North Dakota to serve as an RN Board Member which included service as chair of the Nursing Education Committee. I served in this role until July 2015 when I was hired as Board staff. I have been the Associate Director for Compliance since July 2015 (2 years). This has provided me with various opportunities to see nursing regulation in action in the areas of nursing practice, nursing education, and now compliance/discipline. My community experience includes service on several statewide committees. These include: 3 years (2011-2014) as a member of the North Dakota Partners in Nursing Gerontology Consortium (including Co-chair of the Education Committee for 3 years); 1 year of service (July 2016- Nov. 2017) on the North Dakota Center for Nursing 2017 Annual Conference Planning Committee; and 2 years and continuing participation (2015- present) in the North Dakota Reducing Pharmaceutical Narcotics Task Force.
NCQAC Business Meeting July 12-13, 2018
104

2. Please describe a strategy or activity to increase participation in the leadership of the organization.
First, I would like to applaud the newest strategy that the Leadership Succession Committee has already been working on- to take a closer look at those who are currently engaged, those who are actively participating in NCSBN meetings, conferences, programs, and committees and then encouraging those that have been actively involved to consider applying for a leadership role. This is a great start!
An additional strategy that would increase the pool of participants would be to increase opportunities for NCSBN members to participate. In addition to attendance at Mid-Year and Annual meeting, to provide a greater number of opportunities for people to share their talents and abilities on committees, project groups, taskforces, or research groups. The more people we can get to participate in these opportunities, the more we will see people’s talents shine. In addition, this participation can increase leadership self-confidence, communication skills, and networking opportunities. It will also be important to incorporate, either formally or informally, mentorship into this strategy. For many people, getting involved in a committee, project group, taskforce, or research group can be intimidating. Especially on a national level, like with NCSBN. Often you may be working or participating with members who have amazing credentials and loads of experience. But every member has gifts, talents, knowledge, and experience to bring to the table. Having some sort of mentorship within these opportunities can make the experience less intimidating, and again allow all members to feel comfortable providing their own valuable insight.
3. Why do you want to serve in the role you are applying for?
I have had the opportunity to serve on LSC for almost 2 years now. It has been a great experience. I have been able to work with many amazingly talented people from all around the nation. This role has provided me with opportunities to develop and increase my own leadership skills. It had provided me with countless opportunities to observe how successful leaders behave, how they engage others, and how they successfully communicate. What better way to learn! It has also increased my awareness of the importance of leadership succession planning- to ensure the future success of your organization. The future of any organization relies on its ability to build and grow leaders. When we improve the leadership skills and abilities of NCSBN members, this also improves their leadership in their own home state. It is a win-win! The collaboration and teamwork opportunities that NCSBN offers to its members are invaluable. North Dakota has found our collaboration with NCSBN and the resources provided to be highly valuable to our regulatory work in our state. Leadership Succession Committee encourages teamwork, the sharing
NCQAC Business Meeting July 12-13, 2018
105

of ideas, and problem solving. I hope to continue to serve NCSBN in the role of Leadership Succession Committee Area II Member, to contribute my knowledge and skills and to continue to develop my leadership abilities.
NCQAC Business Meeting July 12-13, 2018
106

Area II Member JoAnn Klaassen President, Kansas State Board of Nursing
1. Describe all relevant professional, regulatory, and community experience.
I have served on the Kansas Board of Nursing for the past six years and as Board President for the past two years. I’ve been on the Disciplinary Committee for the Board for all six years and served on the Practice Committee for four years.
I have been a nurse for many years and attorney for more than a decade. I have been a Clinical Associate Professor at the School of Nursing and Health Studies at the University of Missouri-Kansas City for the past eleven years. Prior to that I was a nurse educator in several other settings. I practiced primarily as a psychiatric-mental health nurse in both acute and community settings but have experience in medical-surgical nursing and public health. My legal experience includes work as a disciplinary defense attorney and with a plaintiff’s firm doing medical malpractice, personal injury, products liability, and nursing home abuse cases. I have conducted research and published in the areas of educational innovation and rural nursing. In addition, I have conducted and participated in a number of medical mission trips to various countries around the world.
2. Please describe a strategy or activity to increase participation in the leadership of the organization.
One strategy to more effectively increase participation in organization leadership would be to promote relationships between specific LSC members and designated Boards of Nursing. For example, if each LSC member were to have opportunity to present or visit with designated Boards to identify board members and/or staff with an interest and potential for NCSBN
NCQAC Business Meeting July 12-13, 2018
107

leadership service, participation could be increased. This type of networking would not only increase identification of potential leaders but would enhance relationships between the LSC and the various Boards of Nursing to allow for leadership development opportunities.
3. Why do you want to serve in the role you are applying for?
Strong leadership is essential for viable organizations. Additionally, thriving organizations identify potential leaders and provide development to grow effective leaders. While most NCSBN members are aware of the LSC and its role in identifying future leaders, very few members have a relationship with the LSC in a way that enhances knowledge, interest and networking within the organization to facilitate leadership. I would like to be a part of a committee process that expands the ability of the LSC to promote strong, skilled leaders for NCSBN.
NCQAC Business Meeting July 12-13, 2018
108

Area III Member Sandra Culpepper LPN Board Member, Mississippi State Board of Nursing
1. Describe all relevant professional, regulatory, and community experience.
Professional, Regulatory, and Community Experience
Member of the Mississippi Board of nursing Licensed Practical Nurse- Educated at Pearl River Community College
Member of the Mississippi Licensed Practical Nurses Association- Secretary of Board Employed at Pearl River County Hospital and Nursing Home as an Educator for Certified Nurse Aides
Professional Experiences working in LTC units, Acute Care, ED, Post-Operative Care, Nurse Aide Educator for Pearl River Community College, and A Psych/Disabled Persons Community Homes. Currently serve on the Administrative Code Committee, the Practice Committee, and Compliance Committee at the Mississippi Board of Nursing.
Former member of the Office of Nursing Workforce Committee that has now been completed and is flourishing under the MBON.
NCQAC Business Meeting July 12-13, 2018
109
The first LPN to chair a committee for the MBON in regards to the feasibility of transferring authority of LPN. Educational Programs to the MBON with great success and to begin on July 1, 2018.
Actively involves in and assist with hosting an Annual Paint the Town Pink Event raising funds for breast cancer patients/survivors for the last 6 years. I serve my community by volunteering as a Baseball Commissioner to the local youth sports league.
I continue to participate in mission trips to the Dominican Republic providing healthcare services to the residents of Barahona and to Haitian Refugees located in the mountains. I volunteer as a High School Band/Color guard parent to assist with fund raising, traveling assignments, keeper of teenage girls lipsticks, and as well as keeping the students in check with their behavior.
2. Please describe a strategy or activity to increase participation in the leadership of the organization.
Strategy for Increasing Participation in Leadership Roles. I believe that to bring people together and provide a positive experience will help facilitate more participation within NCSBN. I would first begin by using a light, fun team building exercise that allows for questions in a relaxed environment because tend to be more open minded when they feel free to express thoughts and concerns in more of a light manner. By doing this it allows our partners at NCSBN to address any concerns, fears of obligation, and general apprehension some members may have related to time constraints, or the role they would be asked to fulfill. I truly believe in empowering a group to be informed with the ability to critically think in a healthcare environment that is constantly evolving and changing. We have to be able to have those that are able to critically think to address issues in as many areas as possible to keep up with this ever changing healthcare environment to provide regulation that goes above and beyond. I firmly believe by following this strategy, NCSBN will find the best and brightest in Nursing as well as meeting the goals of NCSBN.
3. Why do you want to serve in the role you are applying for?
I feel that it is of utmost importance to continue to provide the best possible care to our clients/patients on every level from medications, treatments, assessments, care plans, but most importantly from the human aspect! I am an advocate for those I am charged to care for and with that you have to have regulation that is crucial in the ability for us to be able to provide all of those things. I thoroughly love the regulation aspect of nursing and how it affects healthcare across the world. We are all aware of how important regulation is to not only our profession and how it
NCQAC Business Meeting July 12-13, 2018
110

guides our decision making processes but how it will also affect our client/patient outcomes. For me, I would be extremely excited and honored to be able to be a part of a team that will help me to also succeed and become an even stronger leader in regulation with in our nursing practice!
Area III Member Sara Griffith, MSN, RN Regulation Consultant, North Carolina State Board of Nursing
1. Describe all relevant professional, regulatory, and community experience.
I began my professional nursing career about 18 years ago at an 800-bed hospital as a cardiac surgery staff nurse and transitioned into nursing administration for approximately three years. As staff nurse, I was active in shared governance and journey to Magnet status. I completed my Masters Degree in Nursing Education in 2008. I am a current student in the Nursing PhD Program at East Carolina University with a regulatory research focus on substance use disorder in nursing. In 2007, I was elected to NCBON as board member and served the public for 7 ½ years. During my tenure on the Board, I served on a variety of committees which enhanced my knowledge of regulatory functions. I was elected as the Board’s Vice-Chair serving for two consecutive years. As Vice-Chair, my role included Chair of Board Governance which oversees the Board’s processes for conducting business in congruence with Mission, Vision, and Values. As board member, I was appointed to serve on the NIRSC for two terms and then was selected to serve on CORE. I am currently in my second term on the CORE Committee. In 2014, I transitioned from serving the public as a board member to board staff. My current responsibilities as a Regulation Consultant are conducting investigations, interpretation of NC Nursing Practice Act and collaborating with other agencies to meet the mandate of public protection. I focus, primarily, on investigating nurses in advanced practice roles. I am active on multiple board staff committees such as Board Orientation Education and Succession Planning, research, quality, and staff engagement and
NCQAC Business Meeting July 12-13, 2018
111

appreciation. My service to the community extends outside of nursing with my involvement in Girl Scouts as a leader and treasurer, management of club soccer teams, and volunteering to prepare and provide meals with Brown Bag Ministries.
2. Please describe a strategy or activity to increase participation in the leadership of the organization.
Engagement, identification, and mentoring are keys to successfully presenting a slate of candidates for NCSBN’s future leadership positions on the Board of Directors and Leadership Succession Committee (LSC). NCSBN currently has 11 standing committees with a wide range of expertise and leadership experience on each committee. The engagement of committee members in open discussions about their future goals is imperative to implementing continual succession planning and sustainability of the organization.
A strategy for increasing participation in leadership position could be accomplished by requesting time on committee agendas to discuss positions opening within the next year, qualifications for the positions, responding to questions, and encouraging individuals to apply. Additionally, first time attendees at NCSBN conferences should be identified prior to the meeting, contacted through email, and information provided about leadership opportunities within the organization. The targeting of first-time attendees would engage members to consider leadership opportunities, retain their passion for nursing regulation, and provide experiential diversity to the slate of candidates. Exit-interviews with board members and LSC members completing terms to discuss accomplishments, benefits, and advise for future leaders could be added to the current Leadership Engagement calls.
3. Why do you want to serve in the role you are applying for?
Through continual engagement in NCSBN conferences, offered NCSBN conference calls, and service on NCSBN committees, I have seen the growth of the organization in meeting the mission and strategic initiatives. Being an active participant in pursing the mission, growing with the organization, and engaging in the strategic plan of NCSBN, would meet personal and professional goals while enhancing my jurisdictional responsibilities and commitments. I thrive on the challenge of helping people recognize their leadership attributes and abilities through encouraging, motivating, and eliciting interest. I am a firm believer in mentoring and coaching roles (formal and informal). I have had mentors that believed in my ability and planted seeds to assist me in identification and pursuit of goals. Sometimes that seed can be planted related to one’s leadership expertise, qualities, and strengths that makes the difference in pursuing a formal leadership role. Rosalynn Carter stated “A leader takes people where they want to go. A great leader takes people where they don’t necessarily want to go, but ought to be.” The sustainability
NCQAC Business Meeting July 12-13, 2018
112

of NCSBN leadership is vital in ensuring the mission of NCSBN is met while supporting the mission of every member board within the organization. Through my experiences with NCSBN committee work, I have developed a strong understanding of the mission and strategic plan of NCSBN. I am committed to the work of NCSBN and of the NCBON. Serving on the Leadership Succession Committee will continue to develop me as a leader while actively engaging the membership to consider being placed on the ballot for either the BOD or LSC.
NCQAC Business Meeting July 12-13, 2018
113

NCQAC Business Meeting July 12-13, 2018
114

NCQAC Business Meeting July 12-13, 2018
115

NCQAC Business Meeting July 12-13, 2018
116

NCQAC Business Meeting July 12-13, 2018
117

NCQAC Business Meeting July 12-13, 2018
118

NCQAC Business Meeting July 12-13, 2018
119

NCQAC Business Meeting July 12-13, 2018
120

NCQAC Business Meeting July 12-13, 2018
121

NCQAC Business Meeting July 12-13, 2018
122

NCQAC Business Meeting July 12-13, 2018
123

NCQAC Business Meeting July 12-13, 2018
124

NCQAC Business Meeting July 12-13, 2018
125

NCQAC Business Meeting July 12-13, 2018
126

NCQAC Business Meeting July 12-13, 2018
127

NCQAC Business Meeting July 12-13, 2018
128

NCQAC Business Meeting July 12-13, 2018
129

Proposed Date Topic Presenter(s) Coordinator Completed7/13/2018 Discipline‐The Big Picture Catherine Woodard
9/14/2018 Jurisprudence Model UnveilingMargaret Holm, JD, RN Shana Johnny, MN, RN Debbie Carlson
11/9/2018
Global Perspecive of International Nursing‐Swaziland‐Creating a Nursing Program Louise Kaplan, PhD, MN, ARNP‐FNP Debbie Carlson
1/11/2019 Action Now!
Mindy Schaffner, PhD, MSN, CNS, RN Mary Baroni, PhD, RN Gerianne Babbo, EdD, MN, RN Mary Sue Gorski, PhD, RN Kathy Moisio, PhD, RN Mindy Schaffner
3/8/2019 Human Trafficking Michelle Kulkanek, MSN, RNC‐OB, C‐EFM Debbie Carlson5/10/2019 Opioids Gary Franklin, MD, MPH (Tentative) Debbie Carlson
OTHER SUGGESTED TOPICSState and National LPN IssuesCannabis and the Nurse's Role
Nursing Care Quality Assurance Commission Educational Activity Schedule 7‐01‐18 to 6‐30‐19
NCQAC Business Meeting July 12-13, 2018
130

NURSING BUDGET STATUS REPORT – APRIL 2018
BUDGET/ALLOTMENTS:
This report covers the ten month period of July 1, 2017 through April 30, 2018, with 14 months remaining in the biennium. The Nursing Commission budget is underspent by 5% in appropriation authority.
Within our direct budget, we are overspent in Board Salaries. We have hired several extra pro tems to address some of our needs. In the area of staffing, we are in the process of filling the last couple of vacancies, and have hired a couple of temporary employees to help assist in the meantime. Once we are fully staffed, we should fully expend all of our allotment authority for the biennium.
The Service Unit section shows some over expenditures in a few areas. We are overspent in the FBI Background Check unit. The Investigative and Legal Services units continue to be substantially overspent. Our allotment is this area is based on our last two years of expenditures. Due to an unexpected increase in a few sexual misconduct cases, it appears that we may be under budgeted in that area. The over-expenditure in Suicide Assessment is just a timing issue and they do not anticipate expending more than the total amount budgeted overall. There may be an adjusted to our allotment in the Service Unit Section for fiscal year 2019 based on the additional spending authority that HSQA was granted in the supplemental budget this year.
As discussed at the May Commission meeting under the 2019 proposed Legislation, we are anticipating submitting a decision package to increase NCQAC spending authority due an increase in workload. The decision package will be submitted with the DOH 19-21 budget request in September to the Governor’s Office to be considered for inclusion in his budget.
REVENUES:
The recommended revenue balance or “reserve” should be approximately 12.5% of our budget, or approximately $2.8 million. Our current estimated revenue balance is showing $3.9 million. We are entering our busy application season that significantly increases our revenues for several months. We are not yet seeing the declining number of Registered Nurses that was anticipated nationwide at this point in time. Once we are fully staffed, we should fully spend our appropriation authority this biennium, which will impact the reserve. If a decision package is approved for the increased workload for the next biennium, we will have sufficient revenues to cover the increase without additional fee increases.
NCQAC Business Meeting July 12-13, 2018
131

NURSING BUDGET STATUS REPORTAs of April 30, 2018 (10 months)
EXPENDITURES TYPES BIENNIAL BUDGET/ALLOTMENT EXPENDITURES VARIANCE % SPENTBUDGET TO‐DATE TO‐DATE TO‐DATE TO‐DATE
DIRECT EXPENDITURES:FTEs 57.53 57.53 54.00 3.53 93.86%Staff Salaries & Benefits $10,907,298 $4,500,644 $4,399,329 $101,315 97.75%Commission Salaries $450,000 $187,500 $200,691 ($13,191) 107.04%Goods & Services $843,039 $389,140 $268,722 $120,418 69.06%Rent $650,040 $270,850 $244,460 $26,390 90.26%Attorney General (AG) $1,300,080 $487,530 $446,428 $41,102 91.57%Travel $450,000 $187,500 $161,219 $26,281 85.98%Equipment $99,600 $41,500 $25,787 $15,713 62.14%IT Support & Software Licenses $383,188 $117,934 $97,715 $20,219 82.86%TOTAL DIRECT $15,083,245 $6,182,598 $5,844,351 $338,247 94.53%
SERVICE UNITS:FBI Background Checks $607,949 $250,374 $282,093 ($31,719) 112.67%Office of Professional Standards $390,940 $160,928 $113,568 $47,360 70.57%Adjudication Clerk $196,858 $81,020 $76,038 $4,982 93.85%HP Investigations $51,971 $21,426 $52,314 ($30,888) 244.16%Legal Services $32,476 $13,372 $23,680 ($10,308) 177.09%Call Center $211,746 $86,250 $67,241 $19,009 77.96%Public Disclosure $257,182 $105,900 $103,973 $1,927 98.18%Revenue Reconciliation $160,066 $65,173 $62,935 $2,238 96.57%Online Healthcare Provider Lic $167,809 $139,840 $98,178 $41,662 70.21%Suicide Assessment Study $57,576 $34,585 $43,814 ($9,229) 126.68%TOTAL SERVICE UNITS $2,134,573 $958,868 $923,834 $35,034 96.35%
INDIRECT CHARGES:Agency Indirects (15.4%) $2,624,348 $1,082,036 $1,027,997 $54,039 95.01%HSQA Division Indirects (11.5%) $1,957,052 $806,894 $744,936 $61,958 92.32%TOTAL INDIRECTS (26.9%) $4,581,400 $1,888,930 $1,772,933 $115,997 93.86%
GRAND TOTAL $21,799,218 $9,030,396 $8,541,118 $489,278 94.58%
NURSING REVENUE To‐DateBEGINNING REVENUE BALANCE $2,751,90517‐19 REVENUE TO‐DATE $9,717,67717‐19 EXPENDITURES TO‐DATE $8,541,118ENDING REVENUE BALANCE $3,928,464
NCQAC Business Meeting July 12-13, 2018
132

Nursing Care Quality Assurance Commission
Performance Measures
NCQAC Business Meeting July 12-13, 2018
133

NPAP Panel
02468
101214161820
Days LetterDrafted
Edited (Average) Signed Mailed Total Days(Average)
NPAP April 5 & 19, 2018
NPAP Panel B 4/5/2018 NPAP Panel A 4/19/2018
05
1015202530354045
Days LetterDrafted
Edited (Average) Signed Mailed Total Days(Average)
NPAP May 3 & 10, 2018
NPAP Panel B 5/3/2018 NPAP Panel A 5/10/2018
0123456789
Days LetterDrafted
Edited (Average) Signed Mailed Total Days(Average)
NPAP June 7 & 14, 2018
NPAP Panel B 6/7/2018 NPAP Panel A 6/10/2018
NCQAC Business Meeting July 12-13, 2018
134

Legal Performance Measures
0
10
20
30
40
50
60
70
Jun. 2017 Jul. 2017 Aug. 2017 Sept. 2017 Oct. 2017 Nov. 2017 Dec. 2017 Jan. 2018 Feb. 2018 Mar. 2018 Apr. 2018 May. 2018
Legal Case Closures
Number of Cases Forwarded to AAG Finalized with Legal Review onlyFinalized by Default or Final Order After Hearing Finalized by STID, AO or APUC (Settlements)Other (releases, reinstatements)
0
20
40
60
80
Jun. 2017 Jul. 2017 Aug. 2017 Sept. 2017 Oct. 2017 Nov. 2017 Dec. 2017 Jan. 2018 Feb. 2018 Mar. 2018 Apr. 2018 May. 2018
Legal Caseloads
Average Caseload per Attorney Total Cases Assigned to LegalTotal Finalized Cases Target Finalized Cases per AttorneyAverage of Finalized Cases per Attorney (Target 10 per month)
0%
20%
40%
60%
80%
100%
Jun. 2017 Jul. 2017 Aug. 2017 Sept. 2017 Oct. 2017 Nov. 2017 Dec. 2017 Jan. 2018 Feb. 2018 Mar. 2018 Apr. 2018 May. 2018
Legal Performance
Percentage of Legal Reviews Sent to RCM in 30 Days or less
Document drafting time: Percentage of Drafts to AAG or SOA Served in 30 Days or less
Target (77%)
NCQAC Business Meeting July 12-13, 2018
135

WHPS Performance Measures
0
1
2
3
4
5
6
7
8
9
Jun. 2017 Jul. 2017 Aug. 2017 Sept. 2017 Oct. 2017 Nov. 2017 Dec. 2017 Jan. 2018 Feb. 2018 Mar. 2018 Apr. 2018 May. 2018
WHPS Measures
Average Days Positive Drug Test Turn-Around TimeAverage Days from Significant Contract Non-Compliance to Discipline Notification
0
50
100
150
200
250
300
350
Jun. 2017 Jul. 2017 Aug. 2017 Sept. 2017 Oct. 2017 Nov. 2017 Dec. 2017 Jan. 2018 Feb. 2018 Mar. 2018 Apr. 2018 May. 2018
WHPS Participants
NCQAC Business Meeting July 12-13, 2018
136

Nursing Care Quality Assurance Commission
Current Rules in Progress, July 2018
Rules CR 101 Adopted CR 102 Adopted CR 103 Adopted CR 105 Adopted Hearing Date
Repeal of RCW 18.79.380
• CR 101 Interim Practice Permits, WAC 246-840-010, 246-840-090
• CR 101 ARNP Interim Practice Permits, WAC
• 246-840-340 • 246-840-342 • 246-840-344 • 246-840-360 • 246-840-365 • 246-840-367
• Second CR 103 Emergency filed April 4, 2018
• New section: WAC 246-840-048. Then follow with broader CR 101
Interim Practice Permits (Nontraditional and ARNP)
• CR-101 filed on February 23, 2018 WSR# 18-06-009
• Workshops Scheduled: April 25, 2018 May 8, 2018 May 16, 2018
WAC 246-840-533 Preceptor Experience Requirements
• CR-101 filed March 23, 2018 WSR# 18-08-018
• Workshops: April 24, 2018 May 8, 2018 May 16, 2018 June 18, 2018
NCQAC Business Meeting July 12-13, 2018
137

Rules CR 101 Adopted CR 102 Adopted CR 103 Adopted CR 105 Adopted Hearing Date
House Bill 1427 - Opioids
• 7 joint rulemaking workshops held with 5 boards/commissions.
• April 11, 2018 Special NCQAC Business Meeting to review draft language
• Role of RNs and LPNs in assessing patients using opioids and pain relief (Education)
• CR101 filed August 22, 2017 WSR #17-17-142
• Draft rule language approved May 11, 2018
• CR-102 packet in division/agency review
• Anticipated CR-102 filing date of July 5, 2018
• Hearing scheduled for August 10, 2018
*Rules must be in effect by January 1, 2019
August 10, 2018 SeaTac Cowne Plaza
Scope of Practice
• CR-101 Packet in development
• Anticipated filing date of late July/Early August
• Begin stakeholder work in August
Continuing Competency
• CR-101 in development
• Anticipated filing date of August
Temporary Practice Permits 264-840-095
• CR-101 to decrease length of time from 6 months to a 1 month time period, allowable 30 day extension
NCQAC Business Meeting July 12-13, 2018
138

NCQAC Business Meeting July 12-13, 2018
139

NCQAC Business Meeting July 12-13, 2018
140

NCQAC Business Meeting July 12-13, 2018
141

NCQAC Business Meeting July 12-13, 2018
142
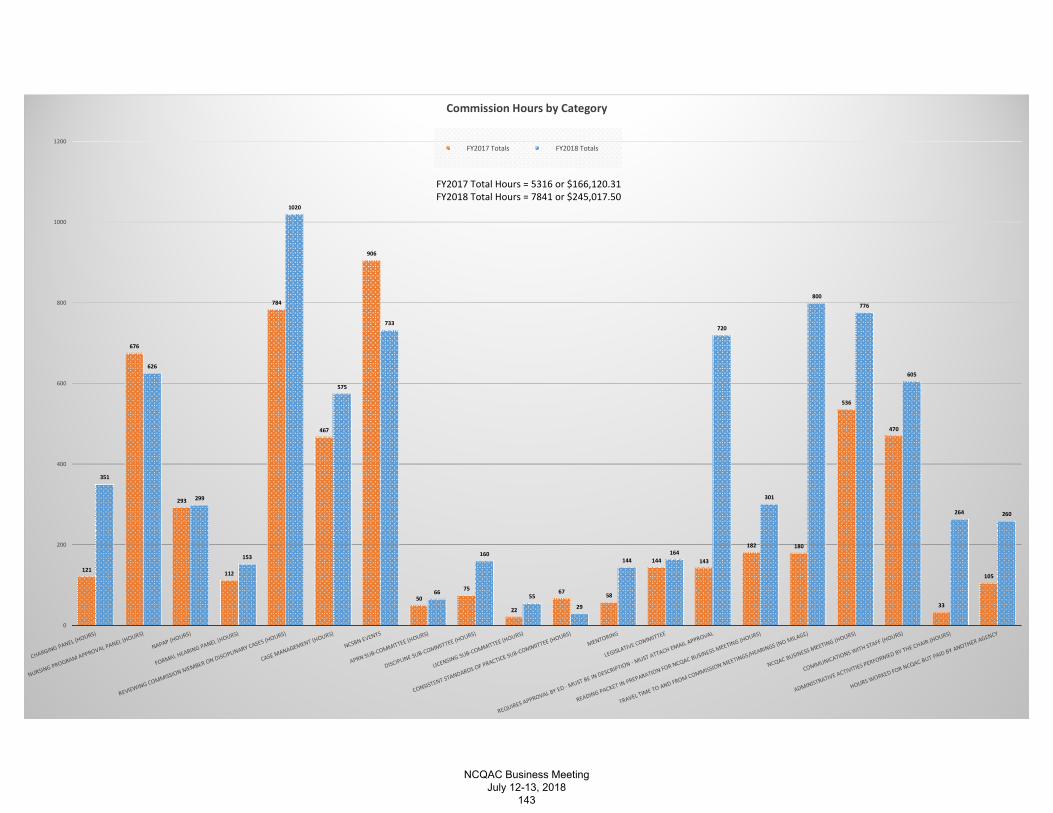
121
676
293
112
784
467
906
50
75
22
67 58
144 143
182 180
536
470
33
105
351
626
299
153
1020
575
733
66
160
55
29
144164
720
301
800776
605
264 260
0
200
400
600
800
1000
1200
Commission Hours by Category
FY2017 Totals FY2018 Totals
FY2017 Total Hours = 5316 or $166,120.31FY2018 Total Hours = 7841 or $245,017.50
NCQAC Business Meeting July 12-13, 2018
143

MEETING LOCATION COMMITTEE NOTES FROM CONFERENCE CALL ON 2/6/2015
Members: Jeannie Eylar (spokesperson), Gene Pingle, Margaret Kelly, Charlotte Foster, Kathy Anderson
Meeting began with the discussion about fiscal impacts of the length and location of meetings around the State. Meetings east of the mountains are substantially more expensive than those located in the Tumwater/Kent area, as most members and staff live in the northwest portion of the State. Although it is a little more expensive to have meetings in Kent due to staff needing to travel, the convenience for most of the Commission members outweighed the cost of transporting staff to the Kent facility.
There was also discussion around the number of meetings per year, and whether it was possible to reduce it down from six to four. There was a unanimous concern that having four meetings per year would hinder commission business needs.
The committee tried to look at both the fiscal impacts as well as the benefits of forming good working relationships and teamwork. The two day meetings (or dinner meetings prior to the Commission meeting) helped provide the means and time for new Commission members to meet others and get comfortable in their role as a part of the Commission and for all the members to bond as a unit.
Based on the above discussions, the committee is recommending the following:
• Continue with six meetings per year • Have one two-day meeting each year in July, alternating between Tumwater (2015) and
Spokane (2016) and have some training opportunities incorporated into one of the days • Have five one-day meetings in Kent each year (with the exception of the year we have a
two-day meeting in Spokane, then have one one-day meeting in Tumwater) • Move the May 2015 meeting from Spokane to Kent since a contract has not been signed • Continue to pursue more teleconferencing capabilities for the public, as well as staff
stationed in other areas • Continue to work on “getting the word out” for public participation in the meetings
NCQAC Business Meeting July 12-13, 2018
144

2017-2018 NCQAC Meetings & Workshops Locations & Venues
Planning Guide
Date Time Location Audio Food Lodging Noon Education Topic & Speaker/Contact
Workshop Topic (if scheduled) &
Speaker/Contact
July 12, 2018 8:30 AM
Red Lion Inn Pasco/Richland
802 George Washington
Way Richland, WA
99352
Spiritborne
Red Lion Inn
Pasco/Richland
Red Lion Inn
Pasco/Richland
Discipline Process and Analysis
July 13, 2018 8:30 AM
Red Lion Inn 802 George Washington
Way Richland, WA
99352
Spiritborne
Red Lion Inn
Pasco/Richland
Red Lion Inn
Pasco/Richland
Disciplinary Process, the Big Picture – Tim
Talkington Coordinator : Debbie
Carlson
September 14, 2018 8:30 AM
DOH – PPE 152/153
310 Israel Rd SE
Tumwater, WA 98501
DOH Budd Bay Cafe
Hilton Garden
Inn TBD
November 9, 2018 8:30 AM CenterPoint?
Kent, WA Spiritborne Alki Bakery?
Hampton Inn? TBD
January 11, 2019 8:30 AM TBD TBD
March 8, 2019 8:30 AM TBD TBD
NCQAC Business Meeting July 12-13, 2018
145

Date Time Location Audio Food Lodging Noon Education Topic & Speaker/Contact
Workshop Topic (if scheduled) &
Speaker/Contact
May 10, 2019 8:30 AM TBD TBD
July 12, 2019 8:30 AM TBD TBD
September 13, 2019 8:30 AM TBD TBD
November 8, 2019 8:30 AM TBD TBD
NCQAC Business Meeting July 12-13, 2018
146

RCW 18.79.202
License fee surcharge—Use of proceeds—Nursing resource center account—Report to the legislature—Review—Rules.
(1) In addition to the licensing fee for registered nurses and licensed practical nurses licensed under this chapter, the department shall impose an additional surcharge of five dollars per year on all initial licenses and renewal licenses for registered nurses and licensed practical nurses issued under this chapter. Advanced registered nurse practitioners are only required to pay the surcharge on their registered nurse licenses.
(2) The department, in consultation with the commission and the workforce training and education coordinating board, shall use the proceeds from the surcharge imposed under subsection (1) of this section to provide grants to a central nursing resource center. The grants may be awarded only to a not-for-profit central nursing resource center that is comprised of and led by nurses. The central nursing resource center will demonstrate coordination with relevant nursing constituents including professional nursing organizations, groups representing nursing educators, staff nurses, nurse managers or executives, and labor organizations representing nurses. The central nursing resource center shall have as its mission to contribute to the health and wellness of Washington state residents by ensuring that there is an adequate nursing workforce to meet the current and future health care needs of the citizens of the state of Washington. The grants may be used to fund the following activities of the central nursing resource center:
(a) Maintain information on the current and projected supply and demand of nurses through the collection and analysis of data regarding the nursing workforce, including but not limited to education level, race and ethnicity, employment settings, nursing positions, reasons for leaving the nursing profession, and those leaving Washington state to practice elsewhere. This data collection and analysis must complement other state activities to produce data on the nursing workforce and the central nursing resource center shall work collaboratively with other entities in the data collection to ensure coordination and avoid duplication of efforts;
(b) Monitor and validate trends in the applicant pool for programs in nursing. The central nursing resource center must work with nursing leaders to identify approaches to address issues arising related to the trends identified, and collect information on other states' approaches to addressing these issues;
(c) Facilitate partnerships between the nursing community and other health care providers, licensing authority, business and industry, consumers, legislators, and educators to achieve policy consensus, promote diversity within the profession, and enhance nursing career mobility and nursing leadership development;
(d) Evaluate the effectiveness of nursing education and articulation among programs to increase access to nursing education and enhance career mobility, especially for populations that are underrepresented in the nursing profession;
NCQAC Business Meeting July 12-13, 2018
147

(e) Provide consultation, technical assistance, data, and information related to Washington state and national nursing resources;
(f) Promote strategies to enhance patient safety and quality patient care including encouraging a safe and healthy workplace environment for nurses; and
(g) Educate the public including students in K-12 about opportunities and careers in nursing.
(3) The nursing resource center account is created in the custody of the state treasurer. All receipts from the surcharge in subsection (1) of this section must be deposited in the account. Expenditures from the account may be used only for grants to an organization to conduct the specific activities listed in subsection (2) of this section and to compensate the department for the reasonable costs associated with the collection and distribution of the surcharge and the administration of the grant provided for in subsection (2) of this section. No money from this account may be used by the recipient towards administrative costs of the central nursing resource center not associated with the specific activities listed in subsection (2) of this section. No money from this account may be used by the recipient toward lobbying. Only the secretary or the secretary's designee may authorize expenditures from the account. The account is subject to allotment procedures under chapter 43.88 RCW, but an appropriation is not required for expenditures. Grants will be awarded on an annual basis and funds will be distributed quarterly. The first distribution after awarding the first grant shall be made no later than six months after July 24, 2005. The central nursing resource center shall report to the department on meeting the grant objectives annually.
(4) The central nursing resource center shall submit a report of all progress, collaboration with other organizations and government entities, and activities conducted by the center to the relevant committees of the legislature by November 30, 2011. The department shall conduct a review of the program to collect funds to support the activities of a nursing resource center and make recommendations on the effectiveness of the program and whether it should continue. The review shall be paid for with funds from the nursing resource center account. The review must be completed by June 30, 2012.
(5) The department may adopt rules as necessary to implement chapter 268, Laws of 2005.
[ 2005 c 268 § 4.]
NCQAC Business Meeting July 12-13, 2018
148

Washington State Nursing Care Quality Assurance Commission
Position Description Research Sub-committee
Purpose: Improve access and utilization of available data to inform policy decisions, evidence- based regulatory practice, and research.
Membership: (Chair appointed by the NCQAC Chair) 1. There will be a minimum of 3 Members of the Nursing Care Quality Assurance
Commission (NCQAC), one of whom shall be the chair of the Subcommittee. 2. Pro tem members will be selected to represent geographic areas and specialties and
provide expertise for selected projects being addressed.
Duties and Responsibilities of the Sub-committee 1. With assistance from staff, prepares the agenda of the sub-committee meetings. 2. In consultation with sub-committee members, establishes the dates and times for the sub-
committee meetings, at least two weeks prior to the NCQAC business meetings. 3. Prepare and present reports to the NCQAC at business meetings with possible action
items. 4. Advise the NCQAC on the processes to identify and prioritize research activities and act
on results of the research if appropriate 5. Advise the NCQAC on how to continue to improve access and utilization of available
data to inform policy decisions, evidence based regulatory practice and research.
Goals: Committee goals include the following: 1. Assure all research complies with protection of human subjects IRB approvals. Use the
DOH IRB unless there is a student involved, then use their university. 2. May recommend and complete grant applications
Staff: Advanced Practice Nursing Consultant
NCQAC Business Meeting July 12-13, 2018
149

Introduction to the Discipline Process
Nursing Care Quality Assurance Commission[NCQAC]
Washington State Department of Health[DOH]
NCQAC Business Meeting July 12-13, 2018
150

Nursing Care Quality Assurance Commission
Chapter 18.79 RCW (Revised Code of Washington) [Statutes]
Nursing Commission Core Functions – Protecting the public through the regulation of nursing:
Education
Licensing
Discipline
Chapter 246-840 WAC (Washington Administrative Code) [Rules]
NCQAC Business Meeting July 12-13, 2018
151

Chapter 18.79 RCW
NCQAC Business Meeting July 12-13, 2018
152

RCW 18.79.010
NCQAC Business Meeting July 12-13, 2018
153

Nursing Care Quality Assurance Commission
Chapter 18.79 RCW (Revised Code of Washington) [Statutes]
Nursing Commission Core Functions – Protecting the public through the regulation of nursing:
Education
Licensing
Discipline
Chapter 246-840 WAC (Washington Administrative Code) [Rules]
Levels of licensure and practice
Nursing Technician
Licensed Practical Nurse [LPN]
Registered Nurse [RN]
Advanced Registered Nurse Practitioner [ARNP]
NCQAC Business Meeting July 12-13, 2018
154

Discipline Overview
Safeguarding the public's health and safety is the paramount responsibility of every DOH disciplining authority.
Statutory Authority and Nursing Practice Regulations
Chapter 18.130 RCW – Uniform Disciplinary Act
• RCW 18.130.180 – Unprofessional conduct
Chapter 246-840 WAC – Practical and Registered Nursing
• WAC 246-840-710 – Violations of standards of nursing conduct or practice
Discipline system provides due process to applicants and licensees
Discipline system seeks to ensure competence, patient safety, and professional ethics
NCQAC Business Meeting July 12-13, 2018
155

Discipline Process
Complaint intake and assessment (anonymized):
Open for investigation
Close
If you are notified of a complaint against you:
Don’t panic
Maintain focus
Act professionally
Right to legal counsel
Investigation – duty to cooperate
Case disposition (anonymized):
• Close
• Early remediation (ER) for minor first-time practice issues
• Authorize disciplinary action
NCQAC Business Meeting July 12-13, 2018
156

Disciplinary Actions
If discipline authorized:
• Informal
• Statement of Allegations/Stipulation to Informal Disposition
• Formal
• Statement of Charges/Agreed Order/Hearing
• Summary action/emergency suspension – “immediate threat to the public health and safety”
• RCW 18.130.050(8); RCW 18.130.135
• Sanctions/compliance
Public access
Reporting to national databanks
Public records act – Chapter 42.56 RCW
NCQAC Business Meeting July 12-13, 2018
157

Sanction Considerations
Disciplining authority must first consider what sanctions are necessary to protect the public—only then may it consider requirements designed to rehabilitate the license holder.
Chapter 246-16 WAC – Standards of professional conduct
Nursing Commission sanction standards and policies
Patient harm/risk of harm
State of mind
• Intentional/willful
• Reckless disregard
• Negligence/inadvertence
Dishonesty, fraud, misrepresentation, cover-up
History of prior discipline
Aggravating/mitigating factors [WAC 246-16-890]NCQAC Business Meeting
July 12-13, 2018 158

Common Violations Leading to Discipline
Medication administration discrepancies and controlled substance diversion; misuse of alcohol or drugs - substance use disorder
Sanctions: Safe medication administration and documentation course, Washington Health Professional Services (WHPS) monitoring program
Practice errors associated with negligence or scope of practice
Sanctions: CE coursework, practice restrictions including supervision and employment settings
Practice errors associated with staffing and systems issues
Sanctions: Incorporate just culture principles, remediation to address deficiencies
Unprofessional conduct associated with dishonesty, corruption, or moral turpitude; risk of severe patient harm
Sanctions: Suspension, revocation, practice restrictions, ethics CE, restitution, fine
NCQAC Business Meeting July 12-13, 2018
159

Mandatory Reporting
Duty to self-report
• WAC 246-16-230
• Criminal convictions
• Findings of unprofessional conduct
• Incapacity
• Disqualification from federal Medicare/Medicaid programs
Duty to report other license holders
• WAC 246-16-235
Duty of employer/facility to report
• WAC 246-16-245
• WAC 246-16-270
NCQAC Business Meeting July 12-13, 2018
160

WAC 246-16-230
NCQAC Business Meeting July 12-13, 2018
161

WAC 246-16-235
NCQAC Business Meeting July 12-13, 2018
162

WAC 246-16-245
NCQAC Business Meeting July 12-13, 2018
163

WAC 246-16-270
NCQAC Business Meeting July 12-13, 2018
164

Capacity to Practice with Reasonable Skill and Safety:
Mental or Physical Conditions
RCW 18.130.170
Consent to mental, physical, psychological examination and waiver of provider/patient privilege
Disciplining authority pays for examination during investigation phase
Waiver of objection to admissibility or use of examination reports or testimony
NCQAC Business Meeting July 12-13, 2018
165

Nursing Practice Strategies to Avoid Complaints and Discipline
Read and understand nursing standards, functions, scope of practice, and conduct
WAC 246-840-700, -705, -710
Scope of Practice Decision Tree
Stay current
Document completely, consistently, and accurately
Communicate clearly
Seek assistance when necessary
Before accepting a nursing assignment, consider personal competence in addition to staffing, patient needs, etc.
Do NOT falsify, misrepresent, misreport, steal, lie, or cover-up
NCQAC Business Meeting July 12-13, 2018
166

WAC 246-840-700
NCQAC Business Meeting July 12-13, 2018
167

WAC 246-840-700 (cont’d)
NCQAC Business Meeting July 12-13, 2018
168

Nursing Scope of Practice Decision Tree
NCQAC Business Meeting July 12-13, 2018
169

Nursing Practice Strategies to Avoid Complaints and Discipline
Read and understand nursing standards, functions, scope of practice, and conduct
WAC 246-840-700, -705, -710
Scope of Practice Decision Tree
Stay current
Document completely, consistently, and accurately
Communicate clearly
Seek assistance when necessary
Before accepting a nursing assignment, consider personal competence in addition to staffing, patient needs, etc.
Do NOT falsify, misrepresent, misreport, steal, lie, or cover-up
NCQAC Business Meeting July 12-13, 2018
170

Nursing Care Quality Assurance Commission
Nursing is regarded as the most trusted profession in America
Nursing touches every life
Thank you for your commitment to the nursing profession!
To take a short quiz, click to advance
Questions? Please contact [email protected]
NCQAC Business Meeting July 12-13, 2018
171

Quiz: Test Your Knowledge
NCQAC Business Meeting July 12-13, 2018
172

Quiz
1. The Nursing Commission is a state agency created by an act of the:
A. United States Department of Health and Human Services
B. Washington State Legislature
C. Washington State Governor
D. National Council for the State Boards of Nursing
Answer: B
NCQAC Business Meeting July 12-13, 2018
173

Quiz
2. The Washington State Nursing Commission regulates nursing:
A. Licensing, scheduling, overtime payscale
B. Education, licensing prep courses, discrimination issues
C. Discipline, medicare reimbursements, employment decisions
D. Licensing, education, discipline
Answer: D
NCQAC Business Meeting July 12-13, 2018
174

Quiz
3. The legal structure for health care provider discipline in Washington state is the:
A. Uniform Disciplinary Act
B. HIPAA
C. Civil Rights Act
D. Uniform Controlled Substances Act
Answer: A
NCQAC Business Meeting July 12-13, 2018
175

Quiz
4. A health care provider in Washington state must self-report:
A. Their own criminal convictions
B. Findings of unprofessional conduct made in another forum
C. Incapacity to practice with reasonable skill or safety because of a mental or physical condition
D. A, B, and C
Answer: D
NCQAC Business Meeting July 12-13, 2018
176

Quiz
5. Sanctions are conditions that must be complied with, and:
A. Always have a nexus with the nature of the violation
B. Are based in rule and in policy
C. May be increased if the nurse tried to cover-up their actions
D. A, B, and C
Answer: D
NCQAC Business Meeting July 12-13, 2018
177

Quiz
6. During an investigation, the Respondent:
A. Has a duty to provide a statement in writing addressing the allegations
B. Should make sure all of the witnesses have the same story
C. May want to introduce false evidence into the process to create confusion
D. Should go into hiding
Answer: A
NCQAC Business Meeting July 12-13, 2018
178

Quiz
7. The Commission reports disciplinary actions to national databanks:
A. Sometimes, depending on how egregious the violation was
B. All of the time because it is required by law
C. Depends on whether it is Washington’s year to report
D. Only suspensions and revocations are reported to the national databanks
Answer: B
NCQAC Business Meeting July 12-13, 2018
179

Quiz
8. The discipline process is designed to protect the public by ensuring:
A. Professional attire, personal hygiene, social media savvy
B. Respectful communication, diversity and inclusion, clean facilities
C. Competence, safety, professional ethics
D. B and C
Answer: C
NCQAC Business Meeting July 12-13, 2018
180

Quiz
9. If a practice error occurs:
A. Document accurately and report it as soon as possible
B. Document what you meant to do
C. Forge another nurse’s name in the report
D. Abandon your assignment and go home
Answer: A
NCQAC Business Meeting July 12-13, 2018
181

Quiz
10. Controlled substance discrepancies in medication administration:
A. Have a high correlation with drug diversion
B. Occur when a nurse withdraws a controlled substance but then fails to document administration and/or waste
C. Are a low priority for facilities and the Commission
D. A and B
Answer: D
NCQAC Business Meeting July 12-13, 2018
182

Introduction to the Discipline Process
Nursing Care Quality Assurance Commission[NCQAC]
Washington State Department of Health[DOH]
Questions? Please contact [email protected] Business Meeting
July 12-13, 2018 183

Chapter 246-840 WAC
PRACTICAL AND REGISTERED NURSING
WAC
ADVANCED PRACTICE—OPIOID PRESCRIBING
246-840-460
Opioid Prescribing—Intent and Scope.
246-840-463
Exclusions.
246-840-465
246-840-4651
246-840-4653
246-840-4655
246-840-4657
246-840-4659
246-840-4661
246-840-4663
246-840-4665
246-840-4667
Definitions.
Patient notification, secure storage, and disposal.
Use of alternative modalities for pain treatment.
Continuing education requirements for opioid prescribing.
Diagnosis identified on prescriptions.
Patient evaluation and patient record- Acute pain.
Treatment plan- Acute non-operative pain.
Treatment plan- Acute perioperative pain.
Patient evaluation and patient record- Subacute pain.
Treatment plan- Subacute pain.
246-840-467
Patient evaluation and patient record- Chronic pain.
246-840-470
Treatment plan- Chronic pain.
246-840-475
Written agreement for treatment- Chronic pain.
246-840-477
Periodic review- Chronic pain.
NCQAC Business Meeting July 12-13, 2018
184

246-840-485
Consultation—Recommendations and requirements.
246-840-487
Consultation—Exemptions for exigent and special circumstances.
246-840-490
Consultation—Exemptions for the advanced registered nurse practitioner.
246-840-493
246-840-4935
246-840-4940
246-840-4950
246-840-4955
246-840-4960
246-840-4970
246-840-4980
246-840-4990
Pain management specialist.
Tapering requirements- Chronic pain.
Patients with chronic pain, including those on high doses, establishing a relationship
with a new practitioner.
Special populations – Patients twenty-five years of age or under, pregnant patients, and
aging populations.
Episodic care of chronic opioid patients.
Co-prescribing with certain medications.
Co-prescribing of opioids for patients receiving medication assisted treatment.
Co-prescribing of naloxone.
Prescription monitoring program – Required registration, queries, and documentation.
NCQAC Business Meeting July 12-13, 2018
185

ADVANCED PRACTICE—PAIN MANAGEMENT
AMENDED SECTION
WAC 246-840-460 Pain management—Intent. WAC 246-840-460 through
WAC 246-840-4990 govern the use of opioids in the treatment of pain in
the acute, perioperative, subacute, and chronic phases. Treatment mo-
dalities including opioid use can serve to improve the quality of life
for those patients who suffer from pain, as well as reduce the morbid-
ity and costs associated with under-treatment or inappropriate treat-
ment of pain. For the purpose of these rules, the inappropriate treat-
ment of pain includes non-treatment, under-treatment, overtreatment,
and the continued use of ineffective treatments. In addition to these
rules, the nursing commission recommends practitioners adhere to ap-
plicable state Agency Medical Directors’ Group (AMDG) and federal Cen-
ters for Disease Control and Prevention (CDC) guidelines for the
treatment of pain in all phases.
[Statutory Authority: RCW 18.79.400. WSR 11-10-064, § 246-840-460,
filed 5/2/11, effective 7/1/11.]
AMENDED SECTION
WAC 246-840-463 Exclusions. WAC 246-840-460 through 246-840-4990
do not apply to:
NCQAC Business Meeting July 12-13, 2018
186

(1) The treatment of patients with cancer-related pain;
(2) The provision of palliative, hospice, or other end-of-life
care;
(3) The treatment of inpatient hospital patients; or
(4) Procedural pre-medications.
[Statutory Authority: RCW 18.79.400. WSR 11-10-064, § 246-840-463,
filed 5/2/11, effective 7/1/11.]
AMENDED SECTION
WAC 246-840-465 Definitions. The following definitions apply in
WAC 246-840-460 through 246-840-4990, unless the context clearly re-
quires otherwise.
(1) “Aberrant behavior” means behavior that indicates misuse,
diversion, or substance use disorder. This includes, but is not lim-
ited to, multiple early refills or renewals, or obtaining prescrip-
tions for the same or similar drugs from more than one practitioner or
other health care provider.
(2) "Acute pain" means the normal, predicted physiological re-
sponse to a noxious chemical, thermal, or mechanical stimulus, and
NCQAC Business Meeting July 12-13, 2018
187

typically is associated with invasive procedures, trauma, and disease.
Acute pain is considered to be six weeks or less in duration.
(3) “Biological specimen test” or “biological specimen testing”
means testing of bodily fluids or other biological samples including,
but not limited to, urine or hair for the presence of various drugs
and metabolites.
(4) "Chronic pain" means a state in which pain persists beyond
the usual course of an acute disease or healing of an injury, or that
may or may not be associated with an acute or chronic pathologic pro-
cess, that causes continuous or intermittent pain more than twelve
weeks in duration, lasting months or years. Chronic pain includes pain
resulting from cancer or treatment in a patient who is two years post
completion of curative anti-cancer treatment with no current evidence
of disease.
(5) "Comorbidities" means a preexisting or coexisting physical or
psychiatric disease or condition.
(6) "Episodic care" means medical care provided by an advanced
registered nurse practitioner other than the designated primary care
practitioner in the acute care setting, for example, urgent care or
emergency department.
NCQAC Business Meeting July 12-13, 2018
188

(7) “High dose” means ninety milligram morphine equivalent dose
(MED), or more, per day.
(8) “High-risk” means a category of patient at increased risk of
morbidity or mortality, such as from comorbidities, polypharmacy, his-
tory of substance use disorder or abuse, aberrant behavior, high dose
opioid prescription, or the use of any central nervous system depres-
sant.
(9) "Hospice" means a model of care that focuses on relieving
symptoms and supporting patients with a life expectancy of six months
or less.
(10) “Hospital” means any institution, place, building, or agency
licensed by the department under chapters 70.41 or 71.12 RCW or desig-
nated as a state hospital under chapter 72.23 RCW, to provide accommo-
dations, facilities, and services over a continuous period of twenty-
four hours or more, for observation, diagnosis, or care of two or more
individuals not related to the operator who are suffering from ill-
ness, injury, deformity, or abnormality, or from any other condition
for which obstetrical, medical, or surgical services would be appro-
priate for care or diagnosis.
(11) “Inpatient” means a person who has been admitted to a hospi-
tal for more than twenty-four hours.
NCQAC Business Meeting July 12-13, 2018
189

(12) ”Medication assisted treatment (MAT)” means the use of phar-
macologic therapy, often in combination with counseling and behavioral
therapies, for the treatment of substance use disorders.
(13) "Morphine equivalent dose (MED)" means a conversion of vari-
ous opioids to a morphine equivalent dose by the use of accepted con-
version tables or calculators.
(14) "Multidisciplinary pain clinic" means a facility that pro-
vides comprehensive pain management and includes care provided by mul-
tiple available disciplines, practitioners, or treatment modalities.
(15) “Multimodal management of pain” means the application of
non-opioid analgesic mechanisms, such as, but not limited to, anti-
depressants, anticonvulsants, anti-inflammatory medications, aceta-
minophen, interventional procedures, or any nonpharmacological pain
treatments.
(16) “Non-operative pain” means pain which does not occur as a
result of surgery.
(17) “Opioid analgesic” or “opioid” means a drug that is either
an opiate derived from the opium poppy, or opiate-like semi-synthetic
or synthetic drugs. Examples include morphine, codeine, hydrocodone,
oxycodone, fentanyl, meperidine, and methadone.
NCQAC Business Meeting July 12-13, 2018
190

(18) "Palliative care" means care that maintains or improves the
quality of life of patients and their families facing serious, ad-
vanced, or life-threatening illness. With palliative care, particular
attention is given to the prevention, assessment, and treatment of
pain and other symptoms, and to the provision of psychological, spir-
itual, and emotional support.
(19) “Pain” means an unpleasant sensory or emotional experience
associated with actual or potential tissue damage, or described in
terms of such damage.
(20) “Pain management clinic” means a publicly or privately owned
facility for which a majority of patients are receiving chronic pain
treatment.
(21) “Perioperative pain” means acute pain that occurs as the re-
sult of surgery.
(22) “Prescription monitoring program” or “PMP” means the Wash-
ington state prescription monitoring program authorized under chapter
70.225 RCW.
(23) “Practitioner” means an advanced registered nurse practi-
tioner licensed under chapter 18.79 RCW, a dentist licensed under
chapter 18.32 RCW, a physician licensed under chapter 18.71 or 18.57
NCQAC Business Meeting July 12-13, 2018
191

RCW, a physician assistant licensed under chapter 18.71A or 18.57A
RCW, or a podiatric physician licensed under chapter 18.22 RCW.
(24) “Risk assessment tools” means validated tools or question-
naires appropriate for identifying a patient’s level of risk for sub-
stance use or misuse.
(25) "Subacute pain" means a continuation of pain, of six to
twelve weeks in duration.
(26) "Substance use disorder” means a primary, chronic, neurobio-
logical disease with genetic, psychosocial, and environmental factors
influencing its development and manifestations. Substance use disorder
is not the same as physical dependence or tolerance that are normal
physiological consequences of extended opioid therapy for pain. It is
characterized by behaviors that include, but are not limited to, im-
paired control over drug use, craving, compulsive use, or continued
use despite harm.
[Statutory Authority: RCW 18.79.400. WSR 11-10-064, § 246-840-465,
filed 5/2/11, effective 7/1/11.]
NEW SECTION
WAC 246-840-4651 Patient notification, secure storage, and disposal.
(1) The practitioner shall provide information to the patient educat-
ing them of:
NCQAC Business Meeting July 12-13, 2018
192

(a) Risks associated with the use of opioids as appropriate to the
medical condition, the type of patient, and the phase of treatment;
(b) The safe and secure storage of opioid prescriptions; and
(c) The proper disposal of unused opioid medications including,
but not limited, to the availability of recognized drug take-back pro-
grams.
(2) The practitioner shall document such notification in the patient
record.
(3) Patient notification must occur, at a minimum, at the following
points of treatment:
(a) The first issuance of a prescription for an opioid; and
(b) The transition between phases of treatment, as follows:
(i) Acute non-operative pain or acute perioperative pain to subacute
pain; and
(ii)Subacute pain to chronic pain.
NEW SECTION
WAC 246-840-4653 Use of alternative modalities for pain treatment.
The practitioner shall consider multimodal pharmacologic and non-
pharmacologic therapy for pain rather than defaulting to the use of
opioid therapy alone whenever reasonable as evidence-based, clinically
appropriate alternatives exist. A practitioner may combine opioids
NCQAC Business Meeting July 12-13, 2018
193

with other medications and treatments including, but not limited to,
acetaminophen, acupuncture, chiropractic, cognitive behavior therapy,
nonsteroidal anti-inflammatory drugs (NSAIDS), osteopathic manipula-
tive treatment, physical therapy, massage, or sleep hygiene.
NEW SECTION
WAC 246-840-4655 Continuing education requirements for opioid pre-
scribing.
(1) In order to prescribe an opioid in Washington state, an ad-
vanced registered nurse practitioner licensed to prescribe opioids
shall complete a one-time continuing education requirement regarding
best practices in the prescribing of opioids. Additionally, a chronic
pain management specialist must meet the continuing education require-
ments in WAC 246-840-493. The continuing education must be at least
four hours in length.
(2) The advanced registered nurse practitioner shall complete
the one-time continuing education requirement described in subsection
(1) of this section by the end of the advanced registered nurse prac-
titioner’s first full continuing education reporting period after Jan-
uary 1, 2019, or during the first full continuing education reporting
period after initial licensure, whichever is later. The four hour
course may count toward any NCQAC required continuing education.
NCQAC Business Meeting July 12-13, 2018
194

NEW SECTION
WAC 246-840-4657 Diagnosis identified on prescriptions.
The advanced registered nurse practitioner shall include the diagnosis
or the International Classification of Diseases (ICD) code on all opi-
oid prescriptions.
New Section
WAC 246-840-4659 Patient evaluation and patient record- Acute.
Prior to prescribing an opioid for acute non-operative pain or acute
perioperative pain, the advanced registered nurse practitioner shall:
(1) Conduct and document an appropriate history and physical ex-
amination including screening for risk factors for overdose and severe
postoperative pain;
(2) Evaluate the nature and intensity of the pain or anticipated
pain following surgery; and
(3) Inquire about any other medications the patient is prescribed or
is taking including type, dosage, and quantity prescribed.
NEW SECTION
WAC 246-840-4661 Treatment plan- Acute non-operative pain.
The advanced registered nurse practitioner shall comply with the re-
quirements in this section when prescribing opioid analgesics for
NCQAC Business Meeting July 12-13, 2018
195

acute non-operative pain and shall document completion of these re-
quirements in the patient record.
(1) The advanced registered nurse practitioner shall consider
recommending or prescribing non-opioid analgesics as the first line of
pain control in patients under the provisions of WAC 246-840-4653, un-
less not clinically appropriate.
(2) The advanced registered nurse practitioner, or practition-
er’s authorized designee as defined in WAC 246-470-050, shall conduct
queries of the prescription monitoring program (PMP) in accordance
with the provisions of WAC 246-840-4990 to identify any schedule II-V
medications or drugs of concern received by the patient, and document
their review and any concerns.
(3) If the advanced registered nurse practitioner prescribes
opioids for effective pain control, such prescription must not be in
greater quantity than needed for the expected duration of pain severe
enough to require opioids. A three day supply or less will often be
sufficient; more than a seven day supply will rarely be needed. The
advanced registered nurse practitioner shall not prescribe beyond a
seven day supply without clinical documentation in the patient record
to justify the need for such a quantity.
NCQAC Business Meeting July 12-13, 2018
196

(4) The advanced registered nurse practitioner shall reevaluate
the patient who does not follow the expected course of recovery. If
significant and documented improvement in function or pain control has
not occurred, the advanced registered nurse practitioner shall recon-
sider the continued use of opioids, or whether tapering or discontinu-
ing opioids is clinically indicated.
(5) Follow-up visits for pain control must include objectives or
metrics to be used to determine treatment success if opioids are to be
continued. This includes, at a minimum:
(a) Change in pain level;
(b) Change in physical function;
(c) Change in psychosocial function; and
(d) Additional planned diagnostic evaluations to investigate causes
of continued acute non-operative pain or other treatments.
(6) Long-acting or extended release opioids are not typically
indicated for acute non-operative pain. Should an advanced registered
nurse practitioner need to prescribe a long-acting opioid for acute
pain, that reason must be documented in the patient record.
(7) Medication assisted treatment (MAT) medications shall not be
discontinued when treating acute pain, except as consistent with the
provisions of WAC 246-840-4970.
NCQAC Business Meeting July 12-13, 2018
197

(8) If the advanced registered nurse practitioner elects to
treat a patient with opioids beyond the six-week time period of acute
non-operative pain, the advanced registered nurse practitioner shall
document in the patient record that the patient is transitioning from
acute pain to subacute pain. Rules governing the treatment of subacute
pain, WAC 246-840-4665 and WAC 246-840-4667, shall apply.
NEW SECTION
WAC 246-840-4663 Treatment plan- Acute perioperative pain.
The advanced registered nurse practitioner shall comply with the re-
quirements in this section when prescribing opioid analgesics for
perioperative pain and shall document completion of these requirements
in the patient’s record.
(1) The advanced registered nurse practitioner shall consider
prescribing non-opioid analgesics as the first line of pain control in
patients under the provisions of WAC 246-840-4653, unless not clini-
cally appropriate.
(2) The advanced registered nurse practitioner, or practition-
er’s authorized designee as defined in WAC 246-470-050, shall conduct
queries of the prescription monitoring program (PMP) in accordance
with the provisions of WAC 246-840-4990 to identify any schedule II-V
NCQAC Business Meeting July 12-13, 2018
198

medications or drugs of concern received by the patient, and document
in the patient record their review and any concerns.
(3) If the advanced registered nurse practitioner prescribes
opioids for effective pain control, such prescription shall be in no
greater quantity than needed for the expected duration of pain severe
enough to require opioids. A three-day supply or less will often be
sufficient; more than a fourteen-day supply will rarely be needed for
perioperative pain. The advanced registered nurse practitioner shall
not prescribe beyond a fourteen-day supply from the time of discharge
without clinical documentation in the patient record to justify the
need for such a quantity. For more specific best practices, the ad-
vanced registered nurse practitioner may refer to clinical practice
guidelines including, but not limited to, those produced by the Agency
Medical Directors’ Group (AMDG), the Centers for Disease Control and
Prevention (CDC), or The Bree Collaborative.
(4) The advanced registered nurse practitioner shall reevaluate
a patient who does not follow the expected course of recovery. If sig-
nificant and documented improvement in function or pain control has
not occurred, the advanced registered nurse practitioner shall recon-
sider the continued use of opioids, or whether tapering or discontinu-
ing opioids is clinically indicated.
NCQAC Business Meeting July 12-13, 2018
199

(5) Follow-up visits for pain control should include objectives
or metrics to be used to determine treatment success if opioids are to
be continued. This includes, at a minimum:
(a) Change in pain level;
(b) Change in physical function;
(c) Change in psychosocial function; and
(d) Additional planned diagnostic evaluations or other treatments.
(6) If the advanced registered nurse practitioner elects to pre-
scribe a combination of opioids with a medication listed in WAC 246-
840-4960 or to a patient known to be receiving a medication listed in
WAC 246-840-4960 from another practitioner, such prescribing must be
in accordance with WAC 246-840-4960.
(7) If the advanced registered nurse practitioner elects to
treat a patient with opioids beyond the six-week time period of acute
perioperative pain, the advanced registered nurse practitioner shall
document in the patient record that the patient is transitioning from
acute pain to subacute pain. Rules governing the treatment of subacute
pain, WAC 246-840-4665 and WAC 246-840-4667, shall apply unless there
is documented improvement in function or pain control, and there is a
documented plan and timing for discontinuation of all opioid medica-
tions.
NCQAC Business Meeting July 12-13, 2018
200

NEW SECTION
WAC 246-840-4665 Patient evaluation and patient record- subacute pain.
The advanced registered nurse practitioner shall comply with the re-
quirements in this section when prescribing opioid analgesics for sub-
acute pain and shall document completion of these requirements in the
patient record.
(1) Prior to prescribing an opioid for subacute pain, the ad-
vanced registered nurse practitioner shall:
(a) Conduct an appropriate history and physical examination or review
and update the patient’s existing history and examination taken during
the acute non-operative or acute perioperative phase;
(b) Evaluate the nature and intensity of the pain;
(c) Inquire about other medications the patient is prescribed or tak-
ing including type, dosage, and quantity prescribed;
(d) Conduct, or cause the practitioner’s authorized designee as de-
fined in WAC 246-470-050 to conduct, a query of the prescription moni-
toring program (PMP) in accordance with the provisions of WAC 246-840-
4990, to identify any schedule II-V medications or drugs of concern
received by the patient, and document their review and any concerns;
(e) Screen and document the patient’s potential for high-risk behav-
ior and adverse events related to opioid therapy. If the advanced reg-
NCQAC Business Meeting July 12-13, 2018
201

istered nurse practitioner determines the patient is high-risk, con-
sider lower dose therapy, shorter intervals between prescriptions,
more frequent visits, increased biological specimen testing, and pre-
scribing rescue naloxone.
(f) Obtain a biological specimen test if the patient’s function is
deteriorating or if pain is escalating; and
(g) Screen or refer the patient for further consultation for psycho-
social factors that may be impairing recovery including, but not lim-
ited to, depression or anxiety.
(2) The advanced registered nurse practitioner treating a pa-
tient for subacute pain with opioids shall ensure that, at a minimum,
the following are documented in the patient record:
(a) The presence of one or more recognized diagnoses or indications
for the use of opioid pain medication;
(b) The observed significant and documented improvement in function
or pain control forming the basis to continue prescribing opioid anal-
gesics beyond the acute pain episode;
(c) The result of any queries of the PMP;
(d) All medications the patient is known to be prescribed or taking;
NCQAC Business Meeting July 12-13, 2018
202

(e) An appropriate pain treatment plan, including the consideration
of, or attempts to use, non-pharmacological modalities and non-opioid
therapy;
(f) Results of any aberrant biological specimen testing results and
the risk-benefit analysis if opioids are to be continued;
(g) Results of screening or referral for further consultation for
psychosocial factors that may be impairing recovery including, but not
limited to, depression or anxiety;
(h) Results of screening for the patient’s level of risk for aberrant
behavior and adverse events related to opioid therapy;
(i) The risk-benefit analysis of any combination of prescribed opioid
and benzodiazepines or sedative-hypnotics, if applicable; and
(j) All other required components of the patient record, as estab-
lished in statute or rule.
(3) Follow-up visits for pain control must include objectives or
metrics to be used to determine treatment success if opioids are to be
continued. This includes, at a minimum:
(a) Change in pain level;
(b) Change in physical function;
(c) Change in psychosocial function; and
(d) Additional planned diagnostic evaluations or other treatments.
NCQAC Business Meeting July 12-13, 2018
203
NEW SECTION
WAC 246-840-4667 Treatment plan- Subacute pain.
(1) The advanced registered nurse practitioner shall recognize
the progression of a patient from the acute non-operative or acute
perioperative phase to the subacute phase and take into consideration
the risks and benefits of continued opioid prescribing for the pa-
tient.
(2) If tapering has not begun prior to the six to twelve week
subacute phase, the advanced registered nurse practitioner shall
reevaluate the patient who does not follow the expected course of re-
covery. If significant and documented improvement in function or pain
control has not occurred, the advanced registered nurse practitioner
shall reconsider the continued use of opioids, or whether tapering or
discontinuing opioids is clinically indicated. The advanced registered
nurse practitioner shall make reasonable attempts to discontinue the
use of opioids prescribed for the acute pain event by no later than
the twelve-week conclusion of the subacute phase.
(3) If the advanced registered nurse practitioner prescribes
opioids for effective pain control, such prescription shall be in no
greater quantity than needed for the expected duration of pain severe
enough to require opioids. The advanced registered nurse practitioner
NCQAC Business Meeting July 12-13, 2018
204

shall not prescribe beyond a fourteen-day supply of opioids without
clinical documentation to justify the need for such a quantity during
the subacute phase.
(4) If the advanced registered nurse practitioner elects to pre-
scribe a combination of opioids with a medication listed in WAC 246-
840-4960 or prescribes opioids to a patient known to be receiving a
medication listed in WAC 246-840-4960 from another practitioner, such
prescribing must be in accordance with WAC 246-840-4960.
(5) If the advanced registered nurse practitioner elects to treat
a patient with opioids beyond the six to twelve week subacute phase,
the advanced registered nurse practitioner shall document in the pa-
tient record that the patient is transitioning from subacute pain to
chronic pain. Rules governing the treatment of chronic pain, WAC 246-
840-467 through WAC 246-840-4940, shall apply.
AMENDED SECTION
WAC 246-840-467 Patient evaluation and patient record. The ad-
vanced registered nurse practitioner shall evaluate and document the
patient's health history and physical examination in the patient’s
health record prior to treating for chronic pain.
(1) The patient's health history shall include:
(a) The nature and intensity of the pain;
NCQAC Business Meeting July 12-13, 2018
205

(b) The effect of pain on physical and psychosocial function;
(c) Current and past treatments for pain, including medications
and their efficacy;
(d) Review of any significant comorbidities;
(e) Any current or historical substance use disorder;
(f) Current medications and, as related to treatment of the pain,
the efficacy of medications tried; and
(g) Medication allergies.
(2) The patient evaluation prior to opioid prescribing must in-
clude:
(a) Appropriate physical examination;
(b) Consideration of the risks and benefits of chronic pain
treatment for the patient;
(c) Medications the patient is taking including indication(s),
type, dosage, quantity prescribed, and as related to treatment of the
pain, efficacy of medications tried;
(d) Review of the prescription monitoring program (PMP) to iden-
tify any schedule II-V medications or drugs of concern received by the
patient in accordance with the provisions of WAC 246-840-4990;
(e) Any available diagnostic, therapeutic, and laboratory re-
sults;
NCQAC Business Meeting July 12-13, 2018
206

(f) Use of a risk assessment tool and assignment of the patient
to a high, moderate, or low risk category. The advanced registered
nurse practitioner should use caution and shall monitor a patient more
frequently when prescribing opioid analgesics to a patient identified
as high risk;
(g) Any available consultations, particularly as related to the
patient’s pain;
(h) Pain related diagnosis, including documentation of the pres-
ence of one or more recognized indications for the use of pain medica-
tion;
(i) Treatment plan and objectives including:
(i) Documentation of any medication prescribed;
(ii) Biologic specimen testing ordered; and
(iii) Any labs or imaging ordered;
(j) Written agreements, as described in 246-840-475 for treatment
between the patient and the advanced registered nurse practitioner;
(k) Patient counseling concerning risks, benefits, and alterna-
tives to chronic opioid therapy.
(3) The health record must be maintained in an accessible manner,
readily available for review, and contain documentation of require-
ments in subsections (1) and (2) of this section, and all other re-
NCQAC Business Meeting July 12-13, 2018
207

quired components of the patient record, as set out in statute or
rule.
[Statutory Authority: RCW 18.79.400. WSR 11-10-064, § 246-840-467,
filed 5/2/11, effective 7/1/11.]
AMENDED SECTION
WAC 246-840-470 Treatment plan. (1) When the patient enters the
chronic pain phase, the advanced registered nurse shall reevaluate the
patient by treating the situation as a new disease.
(2) The chronic pain treatment plan must state the objectives
that will be used to determine treatment success and must include, at
a minimum:
(a) Any change in pain relief;
(b) Any change in physical and psychosocial function; and
(c) Additional diagnostic evaluations or other planned treat-
ments.
(3) After treatment begins, the advanced registered nurse practi-
tioner shall adjust drug therapy to the individual health needs of the
patient.
(4) The advanced registered nurse practitioners shall complete
patient notification in accordance with the provisions of WAC 246-840-
4651.
NCQAC Business Meeting July 12-13, 2018
208

[Statutory Authority: RCW 18.79.400. WSR 11-10-064, § 246-840-470,
filed 5/2/11, effective 7/1/11.]
AMENDED SECTION
WAC 246-840-475 Written agreement for treatment. The advanced
registered nurse practitioner shall use a written agreement for treat-
ment with the patient who requires long-term opioid therapy for chron-
ic pain that outlines the patient’s responsibilities. This written
agreement for treatment must include:
(1) The patient's agreement to provide biological samples for bi-
ological specimen testing when requested by the advanced registered
nurse practitioner;
(2) The patient's agreement to take medications at the dose and
frequency prescribed, with a specific protocol for lost prescriptions
and early refills or renewals;
(3) Reasons for which opioid therapy may be discontinued;
(4) The requirement that all chronic opioid prescriptions are
provided by a single prescriber, a single clinic, or a multidiscipli-
nary pain clinic;
(5) The requirement that all chronic opioid prescriptions are to
be dispensed by a single pharmacy or pharmacy system whenever possi-
ble;
NCQAC Business Meeting July 12-13, 2018
209

(6) The patient's agreement to not abuse substances that can put
the patient at risk for adverse outcomes;
(7) A written authorization for:
(a) The advanced registered nurse practitioner to release the
agreement for treatment to:
(i) Local emergency departments;
(ii) Urgent care facilities;
(iii) Other practitioners caring for the patient who might pre-
scribe pain medications; and
(iv) Pharmacies; and
(b) Other practitioners to report violations of the agreement to
the advanced registered nurse practitioner treating the patient’s
chronic pain and to the prescription monitoring program (PMP);
(8) Acknowledgment that it is the patient's responsibility to
safeguard all medications and keep them in a secure location; and
(9) Acknowledgment that, if the patient violates the terms of the
agreement, the violation and the advanced registered nurse practition-
er's response to the violation will be documented, as well as the ra-
tionale for changes in the treatment plan.
[Statutory Authority: RCW 18.79.400. WSR 11-10-064, § 246-840-475,
filed 5/2/11, effective 7/1/11.]
NCQAC Business Meeting July 12-13, 2018
210

AMENDED SECTION
WAC 246-840-477 Periodic review. (1) The advanced registered
nurse practitioner shall periodically review the course of treatment
for chronic pain. The frequency of visits, biological testing, and
prescription monitoring program (PMP) queries are determined based on
the patient's risk category:
(a) For a high-risk patient, at least quarterly;
(b) For a moderate-risk patient, at least semiannually;
(c) For a low-risk patient, at least annually;
(d) Immediately upon indication of concerning aberrant behavior;
and
(e) More frequently at the advanced registered nurse practition-
ers discretion.
(2) During the periodic review, the advanced registered nurse
practitioner shall determine:
(a) Patient's compliance with any medication treatment plan;
(b) If pain, function, or quality of life have improved, dimin-
ished, or are maintained using objective evidence; and
(c) If continuation or modification of medications for pain man-
agement treatment is necessary based on the advanced registered nurse
practitioner's evaluation of progress towards treatment objectives.
NCQAC Business Meeting July 12-13, 2018
211

(3) Periodic or patient evaluations must also include:
(a) History and physical examination related to the pain;
(b) Use of validated tools to document either maintenance of
function and pain control or improvement in function and pain level;
and
(c) Review of the PMP to identify any schedule II-V medications
or drugs of concern received by the patient at a frequency determined
by the patient’s risk category, and otherwise in accordance with the
provisions of WAC 246-840-4990 and subsection (1) of this section.
(4) The advanced registered nurse practitioner shall assess the
appropriateness of continued use of the current treatment plan if the
patient's progress or compliance with current treatment plan is unsat-
isfactory. The advanced registered nurse practitioner shall consider
tapering, changing, or discontinuing treatment in accordance with the
provisions of WAC 246-840-4935.
[Statutory Authority: RCW 18.79.400. WSR 11-10-064, § 246-840-477,
filed 5/2/11, effective 7/1/11.]
AMENDED SECTION
WAC 246-840-485 Consultation—Recommendations and requirements.
(1) The advanced registered nurse practitioner shall consider and doc-
ument referring the patient for additional evaluation and treatment as
NCQAC Business Meeting July 12-13, 2018
212

needed to achieve treatment objectives. Special attention should be
given to those chronic pain patients who are under eighteen years of
age or who are potential high-risk patients. The management of pain in
patients with a history of substance use or with comorbid psychiatric
disorders may require extra care, monitoring, documentation, and con-
sultation with, or referral to, an expert in the management of such
patients.
(2) The mandatory consultation threshold is one hundred twenty
milligrams morphine equivalent dose (MED). If an advanced registered
nurse practitioner prescribes a dosage amount that meets or exceeds
the mandatory consultation threshold of one hundred twenty milligrams
MED per day, a consultation with a pain management specialist as de-
scribed in WAC 246-840-493, WAC 246-853-750, WAC 246-854-330, WAC 246-
817-965, WAC 246-918-880, WAC 246-919-940, or WAC 246-922-750 is re-
quired, unless the consultation is exempted under WAC 246-840-487 or
246-840-490. The mandatory consultation shall consist of at least one
of the following:
(a) An office visit with the patient and the pain management spe-
cialist;
(b) A consultation between the pain management specialist and the
advanced registered nurse practitioner;
NCQAC Business Meeting July 12-13, 2018
213

(c) An audio-visual evaluation conducted by the pain management
specialist remotely, where the patient is present with either the ad-
vanced registered nurse practitioner or with a licensed health care
practitioner designated by the advanced registered nurse practitioner
or the pain management specialist; or
(d) Other chronic pain evaluation services as approved by the
commission.
(3) The advanced registered nurse practitioner shall document
each consultation with the pain management specialist. Any written
record of a consultation by the pain management specialist shall be
maintained as a patient record by the specialist. If the pain manage-
ment specialist provides a written record of the consultation to the
advanced registered nurse practitioner, the advanced registered nurse
practitioner shall maintain it as part of the patient record.
(4) The advanced registered nurse practitioner shall use great
caution when prescribing opioids to children and adolescents with
chronic pain; appropriate referral to a specialist is encouraged.
[Statutory Authority: RCW 18.79.400. WSR 11-10-064, § 246-840-485,
filed 5/2/11, effective 7/1/11.]
AMENDED SECTION
NCQAC Business Meeting July 12-13, 2018
214

WAC 246-840-487 Consultation—Exemptions for exigent and special
circumstances. An advanced registered nurse practitioner is not re-
quired to consult with a pain management specialist as defined in WAC
246-840-493 when the advanced registered nurse practitioner has docu-
mented adherence to all standards of practice as defined in WAC 246-
840-460 through 246-840-493, and when any one or more of the following
conditions apply:
(1) The patient is following a tapering schedule;
(2) The patient requires treatment for acute pain, which may or
may not include hospitalization, requiring a temporary escalation in
opioid dosage with expected return to their baseline dosage level or
below;
(3) The advanced registered nurse practitioner documents reasona-
ble attempts to obtain a consultation with a pain management special-
ist and the circumstances justifying prescribing above one hundred
twenty milligrams morphine equivalency dosage (MED) per day without
first obtaining a consultation; or
(4) The advanced registered nurse practitioner documents the pa-
tient's pain and function is stable, and the patient is on a non-
escalating dosage of opioids.
NCQAC Business Meeting July 12-13, 2018
215

[Statutory Authority: RCW 18.79.400. WSR 11-10-064, § 246-840-487,
filed 5/2/11, effective 7/1/11.]
AMENDED SECTION
WAC 246-840-490 Consultation—Exemptions for the advanced regis-
tered nurse practitioner. The advanced registered nurse practitioner
is exempt from the consultation requirement in WAC 246-840-485 if one
or more of the following qualifications are met:
(1) The advanced registered nurse practitioner is a pain manage-
ment specialist under WAC 246-840-493;
(2) The advanced registered nurse practitioner has successfully
completed, within the last two years, a minimum of twelve continuing
education hours on chronic pain management approved by the profes-
sion's continuing education accrediting organization. At least two of
these hours must be dedicated to substance use disorder;
(3) The advanced registered nurse practitioner is a pain manage-
ment practitioner working in a multidisciplinary chronic pain clinic
or a multidisciplinary academic research facility; or
(4) The advanced registered nurse practitioner has a minimum
three years of clinical experience in a chronic pain management clin-
ic, and at least thirty percent of the advanced registered nurse prac-
NCQAC Business Meeting July 12-13, 2018
216

titioners’ current practice is the direct provision of pain management
care.
[Statutory Authority: RCW 18.79.400. WSR 11-10-064, § 246-840-490,
filed 5/2/11, effective 7/1/11.]
AMENDED SECTION
WAC 246-840-493 Pain management specialist. A pain management
specialist, functioning as a consultant for the prescribing of chronic
opioid therapy, shall meet the following qualifications:
(1) Credentialed in pain management by a Washington state nursing
care quality assurance commission-approved certifying or credentialing
entity; or
(2) Meet all of the following:
(a) A minimum of three years of clinical experience in a chronic
pain management care setting;
(b) Successful completion of a minimum of at least eighteen con-
tinuing education hours in pain management during the past two years;
and
(c) At least thirty percent of the advanced registered nurse
practitioner’s current practice is the direct provision of pain man-
agement care or is in a multidisciplinary pain clinic.
NCQAC Business Meeting July 12-13, 2018
217

[Statutory Authority: RCW 18.79.400. WSR 11-10-064, § 246-840-493,
filed 5/2/11, effective 7/1/11.]
NEW SECTION
WAC 246-840-4935 Tapering requirements. The advanced registered nurse
practitioner shall assess and document the appropriateness of contin-
ued use of the current treatment plan if the patient's response to, or
compliance with, the current treatment plan is unsatisfactory. The ad-
vanced registered nurse practitioner shall consider tapering, chang-
ing, discontinuing treatment, or referral for a substance use disorder
evaluation when:
(1) The patient requests;
(2) The patient experiences a deterioration in function or pain;
(3) The patient is non-compliant with the written agreement;
(4) Other treatment modalities are indicated;
(5) There is evidence of misuse, abuse, substance use disorder, or
diversion;
(6) The patient experiences a severe adverse event or overdose;
(7) There is unauthorized escalation of doses; or
(8) There is continued dose escalation with no improvement in pain,
function, or quality of life.
NCQAC Business Meeting July 12-13, 2018
218

NEW SECTION
WAC 246-840-4940 Patients with chronic pain, including those on high
doses, establishing a relationship with a new practitioner.
(1) When a patient receiving chronic opioid pain medication(s)
changes to a new advanced registered nurse practitioner, the advanced
registered nurse practitioner shall query the prescription monitoring
program (PMP). It is normally appropriate for the new advanced regis-
tered nurse practitioner to initially maintain the patient’s current
opioid doses. Over time, the advanced registered nurse practitioner
may evaluate if any tapering or other adjustments in the treatment
plan can or should be done.
(2) An advanced registered nurse practitioner’s treatment of a
new high dose chronic pain patient is exempt from the mandatory con-
sultation requirements of WAC 246-840-485 and the tapering require-
ments of WAC 246-840-4935 if:
(a) The patient was previously being treated with a dosage of opioids
in excess of one hundred twenty milligram MED for chronic pain under
an established written agreement for treatment of the same chronic
condition or conditions;
(b) The patient’s dose is stable and non-escalating;
NCQAC Business Meeting July 12-13, 2018
219

(c) The patient has a demonstrated history in their record of compli-
ance with treatment plans and written agreements as documented by med-
ical records and PMP queries; and
(d) The patient has documented functional stability, pain control, or
improvements in function or pain control, at the dose in excess to one
hundred twenty milligram MED.
(3) With respect to the treatment of a new patient under subsec-
tion (1) or (2) of this section, this exemption applies for the first
three months of newly established care, after which the requirements
of WAC 246-840-485 and WAC 246-840-4935 shall apply.
NEW SECTION
WAC 246-840-4950 Special populations– Patients twenty-five years of
age or under, pregnant patients, and aging populations.
(1) Patients twenty-five years of age or under. In the treatment
of pain for patients twenty-five years of age or under, the advanced
registered nurse practitioner shall treat pain in a manner equal to
that of an adult but must account for the weight of the patient and
adjust the dosage prescribed accordingly.
(2) Pregnant patients. Use of medication assisted treatment
(MAT) opioids, such as methadone or buprenorphine, by a pregnant pa-
tient shall not be discontinued without oversight by the MAT prescrib-
NCQAC Business Meeting July 12-13, 2018
220

ing practitioner. The advanced registered nurse practitioner shall
weigh carefully the risks and benefits of opioid detoxification during
pregnancy.
(3) Aging populations. As people age, their tolerance and metab-
olizing of opioids may change. The advanced registered nurse practi-
tioner shall consider the distinctive needs of patients who are sixty-
five years of age or older and who have been on chronic opioid therapy
or who are initiating opioid treatment.
NEW SECTION
WAC 246-840-483 Episodic care of chronic opioid patients.
(1) When providing episodic care for a patient who the advanced
registered nurse practitioner knows is being treated with opioids for
chronic pain, such as for emergency or urgent care, the advanced reg-
istered nurse practitioner shall review the prescription monitoring
program (PMP) to identify any schedule II-V or drugs of concern re-
ceived by the patient and document in the patient record their review
and any concerns.
(2) An advanced registered nurse practitioner providing episodic
care to a patient who the advanced registered nurse practitioner knows
NCQAC Business Meeting July 12-13, 2018
221

is being treated with opioids for chronic pain should provide addi-
tional opioids to be equal to the severity of the acute pain. If opi-
oids are provided, the advanced registered nurse practitioner shall
limit the use of opioids to the minimum amount necessary to control
the acute non-operative pain, acute perioperative pain, or similar
acute exacerbation of pain until the patient can receive care from the
practitioner who is managing the patient’s chronic pain treatment.
(3) The episodic care advanced registered nurse practitioner shall
report known violations of the patient’s written agreement to the pa-
tient's treatment practitioner who provided the agreement for treat-
ment.
(4) The episodic care advanced registered nurse practitioner shall
coordinate care with the patient's chronic pain treatment practitioner
if that person is known to the episodic care advanced registered nurse
practitioner, when practicable.
NEW SECTION
WAC 246-840-4960 Co-prescribing with certain medications.
(1) The advanced registered nurse practitioner shall not know-
ingly prescribe opioids in combination with the following schedule II-
IV medications without documentation in the patient record of clinical
judgment and discussion of risks with the patient:
NCQAC Business Meeting July 12-13, 2018
222

(a) Benzodiazepines;
(b) Barbiturates;
(c) Sedatives;
(d) Carisoprodol; or
(e) Non-benzodiazepine hypnotics also known as Z drugs.
(2) If a patient receiving an opioid prescription is known to be con-
currently prescribed one or more of the medications listed in subsec-
tion (1) of this section, the advanced registered nurse practitioner
prescribing opioids shall consult with the other prescriber(s) to es-
tablish a patient care plan for the use of the medications concurrent-
ly or consider whether one of the medications should be tapered.
NEW SECTION
WAC 246-840-4970 Co-prescribing of opioids for patients receiving med-
ication assisted treatment (MAT).
(1) Where practicable, the advanced registered nurse practition-
er providing acute non-operative pain or acute perioperative pain
treatment to a patient known to be receiving medication assisted
treatment (MAT) shall prescribe opioids for pain relief either in con-
sultation with the MAT prescribing practitioner or a pain specialist.
(2) The advanced registered nurse practitioner shall not discon-
tinue MAT medications when treating acute non-operative pain or acute
NCQAC Business Meeting July 12-13, 2018
223

perioperative pain without documentation of the reason for doing so,
nor shall use of these medications be used to deny necessary operative
intervention.
NEW SECTION
WAC 246-840-4980 Co-prescribing of naloxone.
(1) The advanced registered nurse practitioner shall confirm or
provide a current prescription for naloxone when 50 MED or above, or
when prescribed to a high-risk patient.
(2) The advanced registered nurse practitioner should counsel
and provide an option for a current prescription for naloxone to pa-
tients being prescribed opioids as clinically indicated.
NEW SECTION
WAC 246-840-4990 Prescription monitoring program– Required registra-
tion, queries, and documentation.
(1) The advanced registered nurse practitioner shall register to
access the prescription monitoring program (PMP) or demonstrate proof
of having registered to access the PMP if they prescribe opioids in
Washington state.
NCQAC Business Meeting July 12-13, 2018
224

(2) The advanced registered nurse practitioner is permitted to
delegate performance of a required PMP query to an authorized design-
ee, as defined in WAC 246-470-050.
(3) At a minimum, the advanced registered nurse practitioner
shall ensure a PMP query is performed prior to the prescription of an
opioid at the following times:
(a) First opioid prescription for acute pain unless clinical ex-
ception is documented; such exceptions should be rare, occurring in
less than 10% of the first prescriptions;
(b) First refill for acute pain if not checked with initial pre-
scription due to documented clinical exception;
(c) Time of transition from acute to subacute pain;
(d) Time of transition from subacute to chronic pain; and
(e) Time of pre-operative assessment for any elective surgery or
prior to discharge for non-elective surgery.
(4) For chronic pain management, the advanced registered nurse
practitioner shall ensure a PMP query is performed at a minimum fre-
quency determined by the patient’s risk assessment, as follows:
(a) For a high-risk patient, a PMP query shall be completed at
least quarterly.
NCQAC Business Meeting July 12-13, 2018
225

(b) For a moderate-risk patient, a PMP query shall be completed
at least semiannually.
(c) For a low-risk patient, a PMP query shall be completed at
least annually.
(5) The advanced registered nurse practitioner shall ensure a
PMP query is performed for any chronic pain patient immediately upon
identification of aberrant behavior.
(6) The advanced registered nurse practitioner shall ensure a
PMP query is performed when providing episodic care to a patient who
the advanced registered nurse practitioner knows to be receiving opi-
oids for chronic pain, in accordance with WAC 246-840-4955
(7) For the purposes of this section, the requirement to consult
the PMP does not apply when the PMP or the electronic medical record
(EMR) cannot be accessed by the advanced registered nurse practitioner
due to a temporary technological or electrical failure. The query
shall be completed as soon as technically feasible.
(8) Pertinent concerns discovered in the PMP shall be documented
in the patient record.
REPEALER
NCQAC Business Meeting July 12-13, 2018
226

The following sections of the Washington Administrative Code are
repealed:
WAC 246-840-473 Informed consent.
WAC 246-840-480 Long-acting opioids, including methadone.
WAC 246-840-483 Episodic care.
NCQAC Business Meeting July 12-13, 2018
227

Critical Need in Nursing Education Nursing Workforce and the Health of Our Citizens At Risk
With LACK OF NURSING FACULTY identified as a main obstacle, RN programs turn away an estimated 34% of qualified
student applicants (NLN, 2016)*. In Washington state, that equals 814 students in one year (NCQAC, 2017). With 70% of
Washington nursing programs reporting faculty vacancies (WCN, 2017), capable students are being denied the education
needed to enter nursing at a time when the demand for nursing care is great and increasing. The projected growth rate
for RN employment nationally is 15% through 2026 (vs. 7.4% for all occupations) (BLS, 2016), and Washington projections
through 2024 are estimated to be even higher at 19.6% (Projections Central, 2016). Washington’s nursing faculty shortage
limits educational and economic advancement opportunities for diverse students and has direct, negative impact on the
number of nurses available to provide healthcare in our state—all of which puts the health of our citizens at risk.
Nursing faculty must hold a graduate degree, preferably at the doctoral level, and they serve in an advanced nursing
practice role. Yet, recruitment and retention efforts are stymied by significantly discrepant salaries compared to nurses in
other areas of practice, even where much less education is required: One Washington skilled nursing facility reported that
the average hourly pay is $40.99 for a staff RN (typically from a 2-year RN program)—for a FT annual salary of $85,259;
meanwhile, the master’s-prepared faculty teaching in that 2-year RN program earns between $53,300 and $67,700
(NCQAC, 2018). Not surprisingly, 73% of Washington nursing faculty report being dissatisfied or very dissatisfied with their
income (WCN, 2017; NCQAC, 2018). Nursing programs often reveal faculty workloads above a 1.0 FTE—a result of both low
faculty numbers and insufficient base salaries (NCQAC, 2018). A particular workload burden—and enrollment limitation—is
securing clinical practice experiences for nursing students: 63% of Washington nursing programs report inadequate
availability of clinical practice sites (NCQAC, 2018). Low salaries and high workloads create a losing battle for recruitment
and retention: Last year, 13.5% of Washington nursing faculty were in their first year of employment while another 8.9% of
faculty resigned (NCQAC, 2018). Compounding matters, limited enrollments restrict the development of new, demographically
diverse faculty even as 13.9% of the state’s current nursing faculty expect to retire in the next five years (NCQAC, 2018).
1—Provide a salary increase to nurses teaching in higher public education institutions that is similar to the salary
increase received by nurses employed in state institutions and governmental agencies in July 2017.
2—Encourage public-private partnership in the use of the Washington State Opportunity Scholarship program to prepare,
recruit, and retain a diverse, well-qualified pool of nursing faculty and expand enrollment capacity of nursing programs.
3—Remove policy barriers that prevent nursing programs from directly accessing and allocating available funds to support
faculty pay and program costs.
4—Implement leadership and finance courses tailored to the needs of nurse administrators.
5—Implement a preceptor training program to prepare and support nurses in clinical/practice settings in the teaching of
nursing students and to increase the capacity to develop/educate more nurses.
6—Increase use of simulation from 11% toward the 50% allowed in rule to expand available clinical/practice opportunities
and enrollment capacity; maximize cross-program collaboration and education-industry partnering in this effort.
Nurse leaders in Washington have been working with stakeholders through the Action Now! initiative to develop solutions
to assure appropriate, quality nursing care for our citizens. Launched by the Council on Nursing Education in Washington
State, the Nursing Care Quality Assurance Commission, and the Washington Center for Nursing—Action Now! has four
“Solutions Workgroups” focused on the nursing faculty shortage and other challenges threatening ongoing development
of a robust, qualified, and diverse nursing workforce necessary to assure quality care for all Washington citizens. ‘
Contact information for this document and more information about Action Now! may be found on the back of this page.
Rev. 6/12/18 *Note: References for data provided may be found on the back of this page. NCQAC Business Meeting July 12-13, 2018
228

Action Now!
Nursing Education: Securing the Future of a Healthier Washington
Several complex issues facing nursing are impeding Washington State’s ability to produce the nursing workforce needed by our growing and changing communities: a nursing faculty shortage; nursing education funding that fails to keep pace; and a lack of quality clinical practice experiences for all students. Coupled with these challenges is a national call to advance nursing education so that nurses have access to and are enabled to succeed at the baccalaureate and graduate levels. A group of Washington State nursing leaders have come together to form a new statewide initiative called Action Now! to tackle these challenges and transform the state’s nursing education system. Action Now! is spearheaded by the Council on Nursing Education in Washington State, the statewide organization of deans and directors of Washington nursing programs; the Washington State Nursing Care Quality Assurance Commission, the state’s nursing regulatory board; and the Washington Center for Nursing, the statewide central nursing resource center. Action Now! is working with key stakeholders to develop priorities, strategies and initiatives to:
Create a stronger and more diverse faculty and nursing leadership pool Establish sustainable financing for nursing programs Ensure quality clinical practice experience for all nursing students Provide opportunities for nurses to advance their education
For more information or to get involved, please contact Action Now! executive team members:
Mindy Schaffner, PhD, MSN, CNS, RN
Nursing Care Quality Assurance Commission
(360) 236-4745
Sarah Bear, Ed.D. MSN, RN, CNE
Council on Nursing Education in Washington
(360) 650-3332
Sofia Aragon, JD, BSN, RN
Washington Center for Nursing
(206) 787-1200 x107
References
—Bureau of Labor Statistics, U.S. Department of Labor, News Release (October 24, 2017). Employment Projections, 2016-26. Retrieved on 5/24/18 from: https://www.bls.gov/news.release/pdf/ecopro.pdf
—Bureau of Labor Statistics, U.S. Department of Labor (last modified April 13, 2018). Occupational Outlook Handbook. Retrieved 5/24/18 from: https://www.bls.gov/ooh/healthcare/registered-nurses.htm
—National League for Nursing (2016). Biennial Survey of Schools of Nursing, 2016. Retrieved 5/24/18 from: http://www.nln.org/docs/default-source/newsroom/nursing-education-statistics/percentage-of-qualified-applications-turned-away-by-program-type-2016-(pdf).pdf?sfvrsn=0
—Nursing Care Quality Assurance Commission (2017). Nursing Education Programs 2015-16 Annual School Report: Statistical Summary and Trends Analysis. Retrieved 5/25/18 from: https://www.doh.wa.gov/Portals/1/Documents/6000/669269.pdf
—Nursing Care Quality Assurance Commission (2018). Internal information and preliminary statistics that will be reported in Nursing Education Programs 2016-17 Annual School Report: Statistical Summary and Trends Analysis.
—B. Strader, Chief Executive Officer/Chief Financial Officer, Panorama City/Panorama, Inc., personal communication, 5/23/18.
—Projections Central, State Occupational Projections (2014-2024). Long Term Projections, Registered Nurses ,Washington State. Retrieved 5/25/18 from: http://www.projectionscentral.com/Projections/LongTerm
—Washington Center for Nursing (2017). Survey of Nursing Educators in Washington State. Retrieved 6/1/18 from: http://www.wcnursing.org/uploads/file/Reports/WCN%20Nursing%20Faculty%20Survey%20Report%202017%201-18-18_final.pdf
NCQAC Business Meeting July 12-13, 2018
229

The Publication That Brings Nursing Regulation & Education Together Spring 2018
IN THIS ISSUE …
New Nurse Booklet
Hot Topics in Nursing Education
Nursing Education Outcomes and Metrics Committee
Next Generation NCLEX®
APRN Compact
eNLC Resources
… and more
continued on page 2
INTERVIEW:
Researchers Discuss Groundbreaking StudyIn 2013, NCSBN awarded a Center for Regulatory Excellence (CRE) grant to two researchers, Jane Barnsteiner, PhD, RN, FAAN and Joanne Disch, PhD, RN, FAAN (see bios on page 2). They developed an innovative reporting and tracking tool, called Safe Student Reports (SSR), for nursing student errors and near misses. Nothing like this exists in the health professions, nor outside the U.S. NCSBN is now making it available to schools of nursing free of charge through participation in a research study. NCSBN spoke with Barnsteiner and Disch about the SSR.
What is your experience with nursing programs policies and procedures dealing with student errors?
DR. JANE BARNSTEINER: In a national faculty workshop that we did with support from the Robert Wood Johnson Foundation, Joanne and I were teaching the Institute of Medicine (IOM) and the Quality and Safety of Nursing (QSEN) competencies. While teaching, we learned from faculty questions that schools of nursing had limited policies in place for managing near misses or errors by students or faculty, particularly in the clinical setting, but also in simulation.
Additionally, we found that when students do make a mistake, faculty often-times work with them based on their own personal beliefs rather than with school systems/structures in place. Moreover, their approaches were often punitive. Joanne and I identified the need to learn more, and with a grant from NCSBN, we did a national study on schools of nursing, finding that only 16 percent (of those that responded) had policies/processes in place to address handling errors/near misses. That study was published in the October 2017 American Journal of Nursing (AJN). Based on the research findings, we designed a data repository with a standardized tool, and developed and piloted a form that is integrated into the tool.
Q: As an educator, how can I get involved with NCSBN?
A: One of the best opportunities NCSBN offers to educators is to serve on an Item Review or Item Writing panel. The volun-teers who participate on these panels are an integral part of the NCLEX item development process, thus making an impact nationally on the licensing of new graduates. They will learn,
continued on page 5
Jane Barnsteiner, PhD, RN, FAAN
Joanne Disch, PhD, RN, FAAN
NCQAC Business Meeting July 12-13, 2018
230

Researchers Discuss SSR continued from page 1
SPRING 2018 www.ncsbn.org 2
continued on page 3
Why did you develop the SSR tool?
DR. JOANNE DISCH: The first reason was to standardize what they reported and also the process they use to report. We needed a standardized reporting mechanism because nursing programs did not always define errors the same way. Therefore, we wanted to shape the thinking in order to have a baseline of what counts as an error and a near miss. We also introduced recommendations on who should complete the tool because oftentimes this was not standardized either. For schools just getting started, this really gives them a focus. Our experiences in designing the online data repository and the reporting tool were published in the Journal of Nursing Regulation in 2014.
A second reason is, by having a very open, receptive tool, we hope that it would help destigmatize errors. Sometimes people in our work would call these “violations of practice,” which are very broad words, so we came up with the language of “incident occur-rence.” This was not to help normalize errors, but to not condemn before we even know the nature of the error.
The third reason is we can identify trends and areas for improvement. For example, if an error is happening in one school of nursing, and you see it is also happening in another school, maybe it is a bigger system issue and not just one program being aberrant. This really helps us identify trends. Because of that, we have a database where we can do ongoing research and look into the sources of errors and those types of things.
Were faculty interested in using the SSR tool when you developed it?
DISCH: The vast majority of faculty were supportive. We have heard that many faculty are excited and have been waiting for a tool like this, one that is well used and subscribed to. Some faculty were nervous, thinking there would be repercussions if they reported errors; some even stated that none of their students have ever made an error. The vast majority, however, saw that it would be incredibly helpful to look at why these things are happening and what they can learn from them.
BARNSTEINER: For many faculty, this is a light bulb moment. Sometimes their approach is so steeped in tradition that they have not thought of another way of looking at it, and it changes their thinking 180 degrees. Along with our study results published in the October edition of the AJN, we also published an article in November on steps faculty could put in place to move to a just culture. It has
Dr. Barnsteiner is Professor Emerita at the University of Pennsylvania, School of Nursing, and Editor for Translational Research and Quality Improvement for the American Journal of Nursing. She has served as a Magnet Hospital appraiser since 2006. She is internation-ally recognized as a leader in quality, safety, and evidence-based practice.
Barnsteiner has been honored for her work with the Eastern Nursing Research Society Distinguished Researcher Award and the Sigma Theta Tau International Dorothy Garrigus Adams Award for Excellence in Fostering Professional Standards. In 2009 she was awarded the Lindback Award for Distinguished Teaching from the University of Pennsylvania and in 2014 she received the Alumni Award for Distinguished Leadership from the School of Nursing. She is a member of The Joint Commission Patient Safety Advisory Group and a member of the American Academy of Nursing.
Jane Barnsteiner, PhD, RN, FAAN
Dr. Disch is Professor ad Honorem at the University of Minnesota School of Nursing. Starting her career as a staff nurse in cardiovascular intensive care, Disch served as chief nurse executive at two major medical centers, as interim dean at the University of Minnesota School of Nursing, and as president of the American Association of Critical-Care Nurses and the American Academy of Nursing.
Disch has received a number of awards for her work, including two from Sigma Theta Tau International — one for excellence in fostering professional standards and one for excellence in leadership. Other awards include the Polly Bednash Lectureship Award from the American Association of Colleges of Nursing; the President’s Award from the American Academy of Nursing; and the Distinguished Alumna Award from the University of Wisconsin.
Joanne Disch, PhD, RN, FAAN
NCQAC Business Meeting July 12-13, 2018
231

SPRING 2018 www.ncsbn.org 3
“… it would validate the good work schools are doing, or suggest other strategies they might try as far as tracking, trending, preventing and mitigating the impact of errors.”
– Joanne Disch, PhD, RN, FAAN
“With the SSR tool in place, a school will have the ability to look at their report and compare themselves against the national data.”
– Jane Barnsteiner, PhD, RN, FAAN
Researchers Discuss SSR continued from page 2
had a tremendous response, and is one of the AJN’s most downloaded articles of 2017. That has made us concretely very hopeful that people really want to do the right thing; they just have not had a mechanism in place previously on how to put systems and structures in place. There is no doubt that there will be a certain percentage of faculty who will lag in getting involved, but clearly, people are enthusiastic about this new approach for schools of nursing.
How should the SSR tool be used?
BARNSTEINER: It can be used in a number of ways very effectively to promote safe and high-quality care in the learning of students as well as faculty. First of all, within a school of nursing, it provides a standardized approach for faculty and students to use in reporting occurrences. A school can look across their entire program to see what kind of occurrences are taking place, and whether or not these occurrences should inform their teaching. That internal piece can be extremely informative for a school of nursing.
Secondly, having a national data repository allows the aggregation of knowledge. There is nothing that exists today in schools of nursing or any other professional health schools that will allow the aggregation of data to be able to look at similarities or differences across programs/schools of nursing. With the SSR tool in place, a school will have the ability to look at their report and compare themselves against the national data. Schools can then decide changes that may need to be made in a curriculum, or in the way students are taught across the board.
What is meant by a “just culture” and how could use of the SSR tool promote that?
BARNSTEINER: A “just culture” is one where a provider, student or faculty member can report an error or near miss without fear of retribution. It is an approach that does not start with, “Who did this?” Instead, we talk about five questions that need to be answered when a just culture is in place: “What happened? Has this happened before? Can it happen again? What caused it? Who needs to be told?”
The tool can be used to analyze the vulnerabilities in a system and what needs to be corrected to have a safe environment or safe care. We know through many studies in safety science that roughly 90 to 95 percent of errors and near misses that take place are the result of system errors. Things are not designed to be mistake-proof, so that is where the emphasis needs to start: to look at what the vulnerabilities are in the system. Then, 5 percent or so at a time, you have egregious behavior on the part of the individual. For a student who never comes to clinical prepared, or blatantly disregards safe practices, individual action needs to take place. People are held accountable for their actions, but we also look at the system and see what changes need to take place. Sometimes, in the just culture, you have to take individual action. Sometimes students need to repeat a course, and sometimes nursing is just not cut out for them. The use of the tool helps to promote that analysis.
What would be the advantages of schools becoming part of the SSR tool community?
DISCH: Our real hope for this tool is to create a common database and common terminol-ogy, to develop a research base, and as we exchange information and look at trends, to
continued on page 4
NCQAC Business Meeting July 12-13, 2018
232

SPRING 2018 www.ncsbn.org 4
Researchers Discuss SSR continued from page 3
not just record it into a data dump, but to provide reports. With this common database and the ability to look at sources of frequent errors/near misses and share this information, it would validate the good work schools are doing, or suggest other strategies they might try as far as tracking, trending, preventing and mitigating the impact of errors.
We also think it creates a movement with forward-thinking schools who demonstrate a concern for quality and safety and who want to use data to improve how they teach students. We hope it becomes a prideful thing to become a part of this community, to show your school is on the cutting edge of doing whatever it can to improve not only the student learning experience, but also to develop safe practitioners going into the clinical setting. We hope it will be a very vibrant community of learning, improving quality and safety, and preparing students for realistic clinical practice.
About the ProgramThe Center for Regulatory Excellence (CRE) grant program provides funding for scientific research projects that advance the science of nursing policy and regulation and build regulatory expertise worldwide.
Award InformationInvestigators may apply for grants up to $300,000. All Projects must be completed in 12–24 months following the project start date.
Research PrioritiesResearch priorities include, but are not limited to:
Substance use disorders in nursing National and international regulatory issues Remediation Innovations in nursing education Delegation Impact of legalized marijuana Economic analyses, e.g., Nurse Licensure
Compact, APRN practice, etc.
Upcoming proposal submission deadline: Oct. 5, 2018NCSBN Grant Program
APPLY TODAY
Visit the SSR webpage for further information on how to join this groundbreaking research study. For the purposes of this study, NCSBN has obtained a Certificate of Confidentiality from the National Institutes of Health (NIH), which means the data collected during this study cannot be disclosed to anyone who is not connected with the research. Only your program will have the ability to see its data, and only national aggregate data will be reported by NCSBN. All deans and directors from prelicensure nursing programs should have received letters inviting them to participate. For any comments or questions, contact [email protected].
NCQAC Business Meeting July 12-13, 2018
233

NCSBN is commemorating our 40th anniversary with many celebrations and surprises! One such surprise is a gift to all new graduates: we have published a first-ever booklet welcoming newly licensed nurses to the profession, from a regulatory perspective. “NCSBN Welcomes You to the Nursing Profession” helps new graduates learn about their responsibilities with maintaining and renewing their licenses and of the importance of reading their Nurse Practice Acts (NPA). Some typical violations of the NPA are presented, and cases are integrated throughout the booklet, highlighting principles violated (when appropriate) and nursing takeaway.
Important issues in nursing are discussed, such as substance use disorder and the opiate crisis, social media violations in health care, maintaining professional boundaries and ethical dilemmas new graduates might face. Whenever possible, we have included links to valuable online resources like our brochures and videos. New graduates often are put in the position of needing to speak up for patient safety, but they are sometimes hesitant because of being so new to nursing. TeamSTEPPS strategies are provided to help them take action when they are concerned about safety issues.
At the end of this booklet is a risk control self-assessment checklist, used with permission from the Nurses Service Organization and their insurance carrier partner, which is designed to enhance patient safety and to minimize liability exposure.
Our 40th Anniversary Gift to New Graduates:
A Booklet Welcoming Them to Practice!
SPRING 2018 www.ncsbn.org 5
This is a must-have resource for all new graduates and it is available now! Visit our website to download or order free printed copies.
continued from page 1TESTIMONIAL:
“It has strengthened my understanding of test-taking processes and helped me to learn how to write effective test questions. “
– Janna Hackett, MSN, RN, clinical instructor at Clovis Community College in New Mexico
firsthand, how the NCLEX is developed. While of course the educators must maintain confidentiality of the items, the training they receive to develop or review the items is invaluable. Further, they will network with educators from across the country and Canada, developing an appreciation for different perspectives in nursing education.
If you are interested in volunteering to be an item writer or reviewer, simply complete an online application.
NCQAC Business Meeting July 12-13, 2018
234

SPRING 2018 www.ncsbn.org 6
T he 2018 Institute of Regulatory Excellence (IRE) Conference in San Francisco, Jan. 24–25, 2018, focused on “Using Data to Navigate the Future of Nursing.”
In one of the sessions, an interactive panel discussed the leading issues in nursing education today and their impact on nursing education and nursing regulation. The future of nursing relies on the state of nursing education, and nursing education programs constantly face challenges educating nurses who will be prepared for the evolving and changing health care environment. Panel members from boards of nursing (BONs) were, in essence, describing their use of data in decision making for advancing nursing education.
A list of “hot topics” was compiled for the IRE participants through a review of BON publications, current nursing journals, topics included in recent professional meetings, discussions in the Education Outcomes and Metrics Committee, a report from NCSBN’s 2016 Issues and Trends Committee, a BON survey, and conversations with program directors. All of these hot topics pose serious challenges for nursing programs as they try to meet the needs of society by providing safe, competent graduates who can practice in the complex health care system. Items on the list were clustered and culled down to the leading hot topics listed at the left.
The panel’s moderator was Janice Hooper, PhD, RN, FRE, CNE, FAAN, ANEF, nursing consultant for education at the Texas Board of Nursing.
The panel members were selected from across several states, based upon their areas of expertise. They included:
Sue Petula, PhD, RN, NEA-BC, FRE, nursing education advisor, Pennsylvania Department of State, Bureau of Professional & Occupational Affairs
Tammy Buchholz, MSN, RN, CNE, associate director for education, North Dakota Board of Nursing
Anne Marie Shin, MN, RN, MSc (QIPS), manager, Education Program, College of Nurses of Ontario
Mary A. Baroni, PhD, RN, professor, Nursing and Health Studies, University of Washington, Bothell; board member of the Washington State Nursing Care Quality Assurance Commission; and chair of the IRE Committee
Each panel member discussed the impact of one of the hot topics and invited questions from the audience. The audience was encouraged to continue with the hot topic discus-sion during the reception that followed the panel presentation.
HOT TOPIC #1 – CLINICAL SCARCITY
Petula described the Pennsylvania State Board of Nursing’s deployment in 2007 of a web-based information technology system designed to create efficiencies in information exchange between the BON and all prelicensure nursing programs across
Hot Topics in Nursing Education: An Interactive Panel at the 2018 IRE Conference
HOT TOPICS IN NURSING EDUCATION
TOP FOUR:
Clinical Scarcity
Faculty Shortage
Gap between Education and Practice
Curriculum Models
OTHER TOPICS:
New Generation of Students
Teaching Strategies
Accreditation
Interprofessional Education
Tracks (RN to BSN, other)
Preceptors
Standardized Examinations
Simulation
Clinical Evaluation
Global Clinical Experiences
At-risk Students
Next Generation NCLEX
Technology
Faculty Development
continued on page 7
NCQAC Business Meeting July 12-13, 2018
235

SPRING 2018 www.ncsbn.org 7
The results of this study supported the establishment of a structured developmental program for graduate nursing students in the role of nurse faculty.
Hot Topics continued from page 6
continued on page 8
the Pennsylvania commonwealth. This database supports the ability of prelicensure nursing education programs to timely identify clinical settings and to achieve prompt BON approval of the sites. These efforts arise from the fervent desire to provide essential, and quality, clinical learning experiences where nursing students could provide nursing care for actual patients.
In preparing future nurses to enter complex work environments, the system contains close to 4,000 clinical agencies where students are engaged in supervised clinical experiences, including ones in acute care, wellness clinics, school districts, neighborhood centers, inter-professional health care settings and housing projects. In addition, the use of simulation developed in accordance with established national standards augments clinical experiences.
HOT TOPIC #2 – FACULTY SHORTAGE
Tammy Buchholz discussed an innovative approach implemented by the North Dakota Board of Nursing (ND BON) through a Faculty Developmental Program (FDP) that began in 2004-2005, and was enforced by legislation in 2011. The FDP permits the use of graduate students as baccalaureate-level nursing instructors in the clinical area. In order to gather evidence of the effectiveness of this model, the Nurse Faculty Intern (NFI), a pilot study was conducted by the ND BON from 2006–2009, and was funded by NCSBN’s Center for Regulatory Excellence Grant Program. The results of this study supported the establishment of a structured developmental program for graduate nursing students in the role of nurse faculty. The new and amended North Dakota Administrative Code that
included the FDP and related requirements was approved by the North Dakota attorney general and adopted by the BON on April 1, 2011, as an innovative approach to the faculty shortage in North Dakota. The program has been especially helpful to rural nursing programs to meet their faculty needs.
Audience responses indicated similar programs have been implemented in Louisiana, New Hampshire and Texas. These initiatives have relieved faculty shortages to some degree and provided a mechanism for programs to “grow their own” nursing faculty, without negative impact on program outcomes.
HOT TOPIC #3 – GAP BETWEEN EDUCATION AND PRACTICE
Anne Marie Shin offered a perspective from our Canadian neighbors. The challenges of new nurses transitioning to the
level of nursing practice expected by employers is correlated with the “gap” between education and readiness for practice. The regulator is perhaps best poised to develop strategies to build and strengthen the bridge across the gap. The College of Nurses of Ontario is involved in a process of developing a standardized program approval method for all entry-level nursing programs in Ontario that would apply the same objective academic standards to all nursing programs. A scorecard based on three standards and 10 indicators will provide the framework for program approval, with safety being the overarching concept.
NCQAC Business Meeting July 12-13, 2018
236

SPRING 2018 www.ncsbn.org 8
Hot Topics continued from page 7
The regulator is perhaps best poised to develop strategies to build and strengthen the bridge across the gap.
Two strategies that were used in the development process that facilitated the bridge were (1) using data from practice to inform program approval processes, and (2) meaningful stakeholder engagement with the academic sector. Data were collected over five years and analyzed to determine the top five nursing standards that were breeched and were used to form the foundational standards for curriculum mapping. Initial engagement with practice representatives and academia, and later with students, nurses, practice leaders, and more academic leaders, resulted in gaining various perspec-tives and establishing effective professional relationships.
The goal of these strategies is to use the data to inform downstream processes (man datory curriculum indicators) to affect upstream consequences and to see a decrease in breeches of the nursing standards by the new graduate nurses.
HOT TOPIC #4 – CURRICULUM MODELS
Baroni described an emerging initiative in Washington state referred to as ACTION NOW. This initiative is sponsored by the Washington Nursing Care Quality Assurance Commis-sion, the Washington Center for Nursing, and the Council for Nursing Education in Washington state. A nursing education solution summit is scheduled for Oct. 18, 2018, that will build on the previous four years of Robert Wood Johnson Foundation grant funds to address academic progression in Washington state. Four active statewide workgroups areas for the initiative include:
Opportunities to advance nurses’ education;
Opportunities to assure a diverse nursing education faculty and administrator pool;
New models for quality practice experiences; and
Venues for assuring sustainable financial support systems for nursing education.
The workgroups are composed of representatives from practice, education and regulation committed to the “maximum impact concept” as a guiding mechanism for selection of possible solutions that can be a “triple win” for students and faculty, practice partners and communities. The end goal is to identify one or two evidence-based curriculum models
continued on page 9
NCQAC Business Meeting July 12-13, 2018
237

SPRING 2018 www.ncsbn.org 9
… committed to the “maximum impact concept” as a guiding mechanism for selection of possible solutions that can be a “triple win” for students and faculty, practice partners and communities.
Hot Topics continued from page 8
for a formal, statewide demonstration project that will engage students and faculty in practice that will impact population health. Currently, five models are under consideration:
Structured Preceptor Preparation;
Simulation Care Delivery Model;
Lifestyle Change Program;
Hospital Elder Life Program; and
Accountable Care Organization.
Final Thoughts
While final solutions to the challenges the “hot topics” posed to nurse regulators were not provided, the dialogue was stimulating and provoked ideas that BONs could consider using in their states. Attendees were encouraged by the fact that BONs are reaching out to stakeholders and designing strategies to assist programs to maintain quality in nursing education.
2018 NCSBN
Scientific SymposiumOct. 24 , 2018 | Chicago
SAVE THE DATE
NCQAC Business Meeting July 12-13, 2018
238

SPRING 2018 www.ncsbn.org 10
T he eNLC has been implemented in 29 states as of April 2018, and it will be implemented in Kansas as of July 1, 2019. This is excellent news for the
nursing community!
Building on the existing Nurse Licensure Compact (NLC), the eNLC increases access to health care by allowing nurses to provide care in-person or via telehealth (and other state-of-the-art technologies) in other compact states. It also enhances patient safety by allowing other eNLC states to take action quickly on unsafe or incompetent nurses.
Licensure costs are reduced because nurses hold one multistate license in the state of residence and are able to practice in all eNLC states. This can benefit employers who bear the expense of multiple licenses for nurse employees. Likewise, the eNLC removes multiple and duplicate regulatory requirements, thus further cutting down on costs for nurses.
Additionally, recent disasters such as hurricanes in the south and southeast helped to raise awareness of interstate compacts for health care professionals. These compacts would allow providers to cross borders into states impacted by disasters and begin providing care immediately.
For educators, the eNLC allows faculty to teach distance education courses/content to students in other eNLC states without holding a separate license in those states. It is important for faculty to remember that providing education is practice, and practice takes place in the state
where the recipient of nursing service is located. This includes distance education as well as telephone or telehealth contact with patients located in other states.
Below are some resources nursing faculty or students may access. We suggest that you meet with faculty and students to discuss the eNLC and its implications.
Public Resources:
eNLC Fast Facts – Check out our new infographic for a quick overview of the eNLC.
Nursys Authorization to Practice Map – NCSBN’s new interactive Nursys Authorization to Practice Map is a free resource that can help you quickly determine if a nurse has a multistate license and in which states the nurse may practice.
Uniform Licensure Requirements – Review the multistate license requirements
Take Action – The eNLC advocacy site is a one-stop resource providing an overview of the compact, a quick reference of each state’s status, and a tool for sending a letter of support to legislators.
Follow the eNLC on Facebook and Twitter.
Enhanced Nurse Licensure Compact (eNLC) Update
MORE THAN 2 MILLION NURSES L IVE IN eNLC STATES AND HAVE THE OPPORTUNITY TO PRACTICE IN OTHER eNLC STATES
eNLC STATES ALLOWNURSES TO EASILYPRACTICE ACROSS
BORDERS IN OTHEReNLC STATES
eNLC FAST FACTS
LPN
RN
MULTISTATELICENSE
LPN
RN
SINGLE-STATELICENSE
RN AND LPN/VN APPLICANTS THAT MEET UNIFORM LICENSURE REQUIREMENTS ARE ELIGIBLE FOR A MULTISTATE LICENSE IN eNLC STATES
RN AND LPN/VN APPLICANTS THAT DO NOT MEET UNIFORM LICENSURE REQUIREMENTS MAY BE ELIGIBLE FOR A SINGLE-STATE LICENSE
NURSES IN eNLC STATESWITH MULTISTATE LICENSES ARE ABLE TO PRACTICE VIA
TELENURSING IN ALL eNLC STATES
NURSE EDUCATORS IN eNLC STATES WITHMULTISTATE LICENSES ARE ABLE TO TEACH VIA
DISTANCE EDUCATION IN ALL eNLC STATES
THE eNLC ALLOWS NURSES TO QUICKLY AND EASILY RESPOND TO PROVIDE NURSING SERVICES DURING DISASTERS IN OTHER eNLC STATES
NCQAC Business Meeting July 12-13, 2018
239

SPRING 2018 www.ncsbn.org 11
Educators can raise awareness of the APRN Compact by educating their students on the elements of the compact, in addition to the various ways a multistate license could open up practice opportunities.
continued on page 12
E ducators and their students should know about the APRN Compact which is being discussed in a number of states. The APRN Compact offers a solution to road-
blocks in modern health care delivery. This compact is an interstate agreement allowing an advanced practice registered nurse (APRN) to have one multistate license with the privilege to practice as an APRN in other states party to the compact. Introduced into state legislatures in 2016, the APRN Compact increases access to care electronically, telephonically, and in-person while maintaining public protection at the state level. Advancements in technology have expanded access to health care and telehealth is transforming care delivery, but without the APRN Compact, multiple licenses are required for APRNs who work with patients across state lines. By adopting the APRN Compact, however, qualifying APRNs will not require additional licenses to practice in other compact states, via telehealth or in person.
As of early 2018, the APRN Compact has been enacted in three states (Idaho, North Dakota and Wyoming). To join the APRN Compact, states must enact the model language legislatively. Once 10 states have enacted the legislation, the APRN Compact
will come into effect. Several states have pending APRN Compact legislation, and more are expected to introduce the language in the coming
legislative sessions.
Increased mobility for APRNs will assist primary care provision in health professional shortage areas and increase access to
services for rural and underserved populations. APRNs living across a border from these areas will be able to provide care for these populations, and those providers using telehealth can reach these areas from afar.
Another advantage of the APRN Compact is when APRNs who hold a multistate privilege to practice use the Prescription Drug Monitoring Program (PDMP) in participating states. If their border states are also APRN
Compact members, APRN prescribers may be able to, or required to, check the PDMP in their neighbor states.
Without it, the patient may acquire meds across a state border without their ability to check for that.
The APRN Compact encompasses many elements of the APRN Consensus Model. The seven elements of the APRN Consensus
Model are title, role recognition (all four), maintenance of national certifica-tion, dual licensure as an RN and APRN, graduate or post-graduate education, and
independent practice and prescribing. As graduate-level prepared practitioners, all roles’ education and certification begin with a common core with identical assessment, physiology, and pharmacology requirements in the four roles. In addition to the common core, the APRNs are then educated and certified in their role and population. As states continue to adopt elements of the APRN consensus model, they are increasingly interested in joining the APRN Compact.
The APRN Compact: A Modern Nurse Licensure Solution for the 21st Century
NCQAC Business Meeting July 12-13, 2018
240

SPRING 2018 www.ncsbn.org 12
If your state has introduced a bill to enact the APRN Compact, you can help get the legislation passed!
The APRN Compact continued from page 11
States are trying to broaden their coalitions for supporting the APRN Compact—looking beyond nursing organizations to groups representing disaster preparedness, military families, consumers and patients, business partners and educators to help efforts.
Educators can raise awareness of the APRN Compact by educating their students on the elements of the APRN Compact, in addition to the various ways a multistate license could open up practice opportunities (for example, in areas of telehealth, telephonic nursing and online education). Remember, practice occurs where the patient or student is, and
having a discussion on how APRN nursing education crosses state lines can be helpful. This is particularly important for faculty who supervise clinical experi-
ences for APRN students located outside of the state where the nursing program is located. When preceptors reside in Compact states, they can supervise students in other compact states without needing another license.
If your state has introduced a bill to enact the APRN Compact, you can help get the legislation passed! Access the APRN Compact advocacy
site for more information on the APRN Compact, view an up-to-date map on which states have and are pursuing the compact, and contact
your lawmakers to ask them to support the APRN Compact. Additionally, you can visit the NCSBN APRN Compact page for more information and resources.
Coming August 2018
NCSBN Global Regulatory Atlas
NCSBN is creating the first comprehensive resource of nursing regulation around the world. Providing invaluable information to nurses, educators and researchers, this free publication will detail the regulatory bodies of each country, registration or licensure requirements, levels of nursing and mandatory education, as well as many other aspects of regulatory data.
Find out what information the Regulatory Atlas will offer,
when it will be available and more.
Watch the video now!
NCQAC Business Meeting July 12-13, 2018
241

SPRING 2018 www.ncsbn.org 13
T he NCSBN Board of Directors (BOD) established the Nursing Education Outcomes and Metrics Committee in September 2016, and the first meeting was held in
January 2017. The BOD charged this committee with establishing a set of outcomes and associated metrics to recommend processes to assess nursing education programs:
Review current literature on program approval metrics and their relevance to public safety.
Recommend factors in addition to first-time NCLEX pass rates that can be used to determine criteria for a legally defensible Board of Nursing’s (BON) approval/removal process.
From January to May 2017, the committee spent a considerable amount of time collecting available data and evidence that would assist us in meeting our charge. Some of the actions we took included:
Reviewing the literature;
Interviewing the national nursing accreditors;
Analyzing the differences between first-time NCLEX pass rates when programs are accredited by national nursing accreditors, versus when they are not;
Conferencing with experts about the U.S. Department of Education requirements;
Conferencing with experts in systematic evaluation of nursing education programs;
Meeting with a legal expert about legally defensible recommendations;
Meeting with the chief officer of Exams and chief operating officer at NCSBN to learn about the role of NCLEX pass rates for measuring nursing program outcomes; and
Conferencing with Canadian nurse regulators for their perspectives.
Armed with that background information, we are now moving forward with conducting research to provide us with more evidence supporting program approval. One study we are conducting uses the Delphi technique, and the participation of expert nurse educators will be crucial to this study. The Delphi technique uses multi-staged surveys (three in our study) to gain consensus on important issues. We will be surveying regulators who approve nursing programs, educators who teach prelicensure RN and LPN students, and
employers of new graduates to identify consensus among these three groups with characteristics of programs that graduate safe and competent students, red flags when programs don’t meet that standard and outcomes that are feasible for BONs to collect. We need your help with this important study. If you receive an email inviting you to participate, please take the time to read about the study and consider participating.
When the Delphi study is completed, we will integrate the results with the literature and other studies we are conducting to provide our BONs with recommendations on improving the approval process. Stay tuned for the results.
Nursing Education Outcomes and Metrics Committee Updateby Nancy Spector, PhD, RN, FAAN, director, Regulatory Innovations, NCSBN, and Janice Hooper, PhD, RN, FRE, CNE, board staff, Texas Board of Nursing
NCQAC Business Meeting July 12-13, 2018
242

SPRING 2018 www.ncsbn.org 14
NCSBN CELEBRATES 40 YEARS
1. AUSTRALIA 2. CANADA 3. ENGLAND 4. HONG KONG 5. INDIA 6. JAPAN 7. MEXICO 8. PHILIPPINES 9. PUERTO RICO 10. TAIWAN
U.S. BOARDS OF NURSING REGULATE MORE THAN 4.8 MILLION LICENSED NURSES .
NCSBN CALLED TO ORDER ITS FIRST MEETING ON JUNE 5, 1978.
IN 2018, NCSBN HAS 59 MEMBERSAND 30 ASSOCIATE MEMBERS
ACROSS THE GLOBE.
MORE THAN 138,300 NURSE LICENSURECANDIDATES HAVE TAKEN THE NCLEX ® IN
10 INTERNATIONAL TEST CENTERS.
FROM APRIL 1, 1994 THROUGHDEC. 31, 2017, MORE THAN
5.4 MILLION CANDIDATES FORNURSES LICENSE HAVE TAKEN
NCLEX ® EXAMINATIONS VIA CAT.
NCQAC Business Meeting July 12-13, 2018
243

SPRING 2018 www.ncsbn.org 15
Paramount in NCSBN’s approach to potential evolutionary transformation to its exam was the foundational tenet that any changes must be evidence-based.
continued on page 16
NCSBN’s Next Generation NCLEX® Endeavors to Go Beyond the Leading Edge
A s the producer of one of the preeminent exams in the world, NCSBN is taking an analytical look at its NCLEX® exams to determine how to take what is already the
standard bearer of testing further beyond the leading edge.
The way students learn and the environment in which they are educated is rapidly chang-ing. Can nurses at the entry level, appropriately put together the facts they learn, assess the client under their care, and make crucial clinical judgments about the care they need to deliver? And, from a licensure exam perspective, is decision making and critical thinking measurable? That is what NCSBN is trying to find out.
To determine whether the test is actually assessing what needs to be measured, NCSBN commissioned a literature review of 200 peer-reviewed articles detailing what is occurring in nursing practice, education and testing. What emerged was that nursing education had already made critical thinking, clinical decision making, and clinical judgment a standard part of nursing curricula.
Recognizing that the NCLEX measures practice, not education, NCSBN decided that it needed to do an observational practice analysis. The country was divided into quadrants and observers were deployed to watch novice nurses do their job. Everything that happened was recorded. Focus groups of both novice and experienced nurses were also conducted. What was observed was divided into either task, skills or attributes. This generated 1,000 plus pages of data, which were analyzed to determine the strength of association between entry-level nurse tasks and nurse skills. Many of the attributes and tasks required problem solving, critical thinking and clinical judgment. This is the evidence of how important those three proficiencies are.
The next step in the process was an assessment of the current NCLEX item bank to ascertain whether its item types adequately measure clinical judgment, critical thinking and problem solving skills on a consistent basis. The analysis found that there were three areas where the current items could measure clinical judgment, about a half that could moderately measure it but there were still large gaps.
NCQAC Business Meeting July 12-13, 2018
244

SPRING 2018 www.ncsbn.org 16
Next Generation NCLEX continued from page 15
Paramount in NCSBN’s approach to potential evolutionary transformation to its exam was the foundational tenet that any changes must be evidence-based. The construct must be built first and then the items that can be used to measure it can be described. NCSBN first defined clinical judgment as “the observed outcome of critical thinking and decision making. It is an iterative process that uses nursing knowledge to observe and assess presenting situations, identify a prioritized client concern, and generate the best possible evidence-based solutions in order to deliver safe client care.”
NCSBN then embarked upon research, another literature review and pilot studies to develop a comprehensive clinical judgment assessment model (Dickison, Luo, Kim & Woo, 2016). The Clinical Judgment Model (CJM) represents a fundamental shift from the current dichotomous measurement models in which something is either right or wrong. When context is removed and items are extremely sterile, a very precise and stable measure-ment can be obtained. The CJM (see Figure 1 at left) is complex but can be broken down into four levels: the nurse (1) forms hypothe-ses, (2) prioritizes them, (3) gener-ates solutions and then (4) takes actions. The next layer is one that has not been introduced in any psychometric models before now — the context. Philip Dickison, PhD, RN, NCSBN chief officer, Examina-tions, explains, “The question is
whether you can put context around items in a way that you actually make it more real. In addition to the exam being psychometrically sound and legally defensible, one more condition must be introduced as we move forward into the future — fidelity. Does it look like what we do as nurses?”
NCSBN believes that measuring clinical judgment is not only new to how it tests its candidates but also new to the field of measurement. It is a game changer that stretches beyond nursing into all instances where public safety is involved.
Recognizing that it was necessary to ascertain whether clinical judgment is more than just possessing nursing knowledge, NCSBN conducted a pilot study in 2016 (Muntean et al. 2016 AERA presentation). The study found that the average ability of a nurse to demonstrate the different steps in the clinical judgment process (cue recognition, hypothesis generation, hypothesis evaluation, taking actions and evaluating outcomes) is progressive. Thus, a nurse’s ability to
recognize cues, develop hypotheses and take appropriate actions does not guarantee the ability to evaluate the outcomes of the action taken. In short, having content knowledge does not always translate to having clinical judgment skills.
Armed with this knowledge, NCSBN chose to move forward with what is now called the Next Generation NCLEX® (NGN) project. Bringing together experts from technology,
ClinicalDecisions
Client Needs
Clinical Judgement
Refine Hypotheses
RecognizeCues
AnalyzeCues
PrioritizeHypotheses
GenerateSolutions
Satisfied
Form Hypotheses
Not Satisfied
Layer 0
Layer 1
Layer 2
Layer 3
Layer 4
Evaluation
Take Actions
Evaluate Outcomes
Environment
Medical Records
Time Pressure
Patient Observation Knowledge
Specialty ExperienceTime
Pressure
Resources Knowledge
Candidate Characteristics
Consequences & Risks
Skills
Task Complexity
Cultural Consideration
Knowledge
Experience
Skills
Experience
Patient Observation
continued on page 17
NCQAC Business Meeting July 12-13, 2018
245

SPRING 2018 www.ncsbn.org 17
Leader to Leader is published biannually by National Council of State Boards of Nursing (NCSBN) 111 E. Wacker Drive, Suite 2900 · Chicago, IL 60601-4277 www.ncsbn.org
Phone: 312.525.3600
Editor: Nancy Spector, PhD, RN, FAAN, Director, Regulatory Innovations, NCSBN [email protected]
NCSBN provides education, service and research through collaborative leadership to promote evidence-based regulatory excellence for patient safety and public protection.
Copyright © 2018 NCSBN. All rights reserved.
content and measurement to imagine item prototypes that could measure clinical judgment, NCSBN worked on creating items that could be inserted as a Special Research Section in real candidate examinations. These new item prototypes being tested have the possibility to measure the second, third and fourth layers of the CJM. Examples of the prototypes include: enhanced hot spots, enhanced multiple response and extended
drag and drop.
The first set of these NGN prototypes were included as a voluntary component on the NCLEX exam beginning in July 2017. The Special Research Section is offered to select candidates taking the NCLEX-RN and takes approximately 30 minutes to complete. This section is administered following the regular exam and does not count as part of the NCLEX score. Candidates are making valuable contributions by their participation. Data obtained will be used to ascertain which items accurately measure clinical judgment and nursing competence.
NCSBN plans to provide continual updates about this long-term research endeavor. One such mechanism is the new Next Generation NCLEX® News that will be published quarterly. Information about the Next Generation NCLEX can be found on the NCSBN website. As time goes on, various other communi-cations vehicles will be implemented.
REFERENCES
Dickison, P., Luo, X., Kim, D., Woo, A. (2016). Assessing Higher-Order Cognitive Constructs by Using an Information Processing Framework, Vol. 17(1). Retrieved from
www.jattjournal.com/index.php/atp/article/view/89187.Muntean, W., Lindsay, M., Betts, J., Kim, D., Woo, A., Dickison, P. (2016, April). Separating Assessment of Subject Matter Knowledge from Assessment of Higher-Order Cognitive Constructs. Paper presented at American Educational Research Association Annual Meeting, Washington, D.C.
Next GenerationNCLEX NEWS
®
SPRING 2018
The Next Generation NCLEX® News is a quarterly publication that provides the latest information about the research being done to assess potential changes to the NCLEX. In this issue, you will find information related to the usability studies conducted as part of the Next Generation NCLEX (NGN) research.
The Next Generation NCLEX® Usability StudiesUsability studies are conducted to understand the extent to which a product can be used by a specific group to achieve defined goals with effectiveness, efficiency and satisfaction within a defined context of use. Usability is a quality attribute for improving ease-of-use during the design process and is defined by the following quality components.
Continued on next page
The Next Generation NCLEX® Usability Studies
Next Generation NCLEX continued from page 16
NCQAC Business Meeting July 12-13, 2018
246

An Innovative Reporting and Tracking Tool for Nursing Student Errors
20173013#17094580.0
NCQAC Business Meeting July 12-13, 2018
247

Benefits of SSR include:• Reports about the numbers and types of errors and
near misses that occur in your program - only your program will see these reports;
• The ability to analyze data related to student errors and near misses;
• Quarterly reports from NCSBN about the aggregate numbers and types of errors and near misses so that you can compare them with your program reports; and
• The opportunity to collaborate with a network of colleagues who are interested in patient safety and just culture in schools of nursing.
Nursing is the first health care discipline to provide educators with a database that collects and analyzes their students’ errors and near misses and compares them to other participating nursing schools.
Prelicensure nursing schools interested in participating in the SSR study can contact the principal investigator, Nancy Spector, PhD, RN, FAAN, at [email protected].
w
A National Web-based Network for Anonymous Reporting of Student Errors and Near MissesPrelicensure nursing schools are invited to participate in this research study at the National Council of State Boards of Nursing (NCSBN).
In 2013 NCSBN awarded a Center for Regulatory Excellence (CRE) grant to two researchers, Joanne Disch, PhD, RN, FAAN, and Jane Barnsteiner, PhD, RN, FAAN. They developed an innovative reporting and tracking tool for nursing student errors and near misses. Nothing like this exists in the health professions, nor outside the U.S. NCSBN is now making it available to schools of nursing free of charge through participation in a research study.
Benefits of SSR include:• Reports about the numbers and types of errors and
near misses that occur in your program - only your program will see these reports;
• The ability to analyze data related to student errors and near misses;
• Quarterly reports from NCSBN about the aggregate numbers and types of errors and near misses so that you can compare them with your program reports; and
• The opportunity to collaborate with a network of colleagues who are interested in patient safety and just culture in schools of nursing.
Nursing is the first health care discipline to provide educators with a database that collects and analyzes their students’ errors and near misses and compares them to other participating nursing schools.
Prelicensure nursing schools interested in participating in the SSR study can contact the principal investigator, Nancy Spector, PhD, RN, FAAN, at [email protected].
NCQAC Business Meeting July 12-13, 2018
248

123
Mai
n St
reet
Ad
dre
ss G
oes
Her
e
111
E. W
acke
r D
rive
, Ste
. 290
0C
hica
go,
IL 6
0601
ww
w.n
csb
n.o
rgss
r@nc
sbn.
org
NCQAC Business Meeting July 12-13, 2018
249

NURSING EDUCATION PROGRAMS
2016-2017 ANNUAL SCHOOL REPORT
STATISTICAL SUMMARY AND TRENDS ANALYSIS
DOH 669-269 (Revised May 2018)
Public Health – Always Working for a Safer and Healthier Washington
DRAFTSTATE OF WASHINGTON
DEPARTMENT OF HEALTHNursing Care Quality Assurance Commission
P.O. Box 47864Olympia, WA 98504-7864
NCQAC Business Meeting July 12-13, 2018
250

INTRODUCTION .........................................................................................................................................................4
BACKGROUND 4
NURSES LICENSED IN WASHINGTON ...........................................................................................................................4
NUMBER LICENSED 4 TABLE 1. LICENSED NURSES 5 2017 NCLEX TEST TAKERS 5 FIGURE 1: TOTAL NUMBER OF NCLEX FIRST-TIME TEST TAKERS 5
STATE PROGRAMS .....................................................................................................................................................6
UNDERGRADUATE PROGRAMS 6 FIGURE 2: TOTAL UNDERGRADUATE PROGRAM GRADUATES BY TYPE OF PROGRAM 6 TABLE 2. STATE UNDERGRADUATE GRADUATIONS 7 FIGURE 3: COMPARING AD RN AND TOTAL BSN GRADUATE TRENDS 7 TABLE 3. STATE UNDERGRADUATE PROGRAM COMPLETION RATES BY PROGRAM 8 DIRECT TRANSFER AGREEMENT (DTA) 2016-2017 8 RN TO BSN 2016-2017 8 FIGURE 4: NUMBER OF ENROLLED AND GRADUATED RNB STUDENTS BY YEAR 9 TABLE 4: CLINICAL HOURS BY PROGRAM AND TYPE. 9 GRADUATE PROGRAMS 10 FIGURE 5: MASTER’S AND DOCTORAL TOTAL NUMBER OF GRADUATES BY PROGRAM 10 TABLE 5. STATE GRADUATES BY PROGRAM AND SPECIALTY AREA 11 FACULTY AND STUDENT ETHNICITY 11 FIGURE 6: FACULTY AND STUDENT RACE/ETHNICITY COMPARED WITH CENSUS 11 NURSING FACULTY 12 FACULTY TURNOVER 12 TABLE 6: COMBINED FULL TIME AND PART TIME FACULTY TURNOVER 2016-2017 12 FACULTY EDUCATION 12 FIGURE 7: FACULTY LEVEL OF EDUCATION 2016 - 2017 13 FACULTY SALARY 13 TABLE 7: AVERAGE FACULTY SALARY RANGES 13
OUT-OF-STATE PROGRAMS ...................................................................................................................................... 14
TABLE 8: APPROVED OUT OF STATE PROGRAMS AND STUDENT CLINICAL PLACEMENTS 14 OUT-OF-STATE STUDENT STATISTICS 14 TABLE 9: NUMBER OF STUDENTS WITH CLINICAL SITE PLACEMENT FROM OUT OF STATE PROGRAMS 14 TABLE 10: NUMBER AND TYPES OF OUT OF STATE PROGRAMS WITH CLINICAL SITE PLACEMENTS 14
ANALYSIS/RECOMMENDATIONS .............................................................................................................................. 15
ACADEMIC PROGRESSION 15 NURSING WORKFORCE DATA 16 FACULTY 16 CONCLUSIONS 17
REFERENCES: ........................................................................................................................................................... 18
Acronyms
DRAFT
NCQAC Business Meeting July 12-13, 2018
251

AD-RN .......... Associate Degree in Nursing – Registered Nurse
AD-MS .......... Associate Degree in Nursing to Masters of Nursing
ARNP ............ Advanced Registered Nurse Practitioner
BSN ............... Bachelor of Science in Nursing – Registered Nurse
PN............... ... Licensed Practical Nurse
PN-RN ........... Licensed Practical Nurse to Associate Degree in Nursing Programs
GE.................. Graduate Entry Programs – Registered Nurse
MSN............. . Master of Science Nursing
NCLEX®...... . National Council Licensure Examination
NCQAC........ . Nursing Care Quality Assurance Commission
RN ................. Registered Nurse
RNB ............... Registered Nurse Bachelor (Bachelor’s degree programs for licensed RNs)
PMC .............. Post Master’s Certificate Nurse
DNP ............... Doctorate of Nursing Practice
MN ................ Masters of Nursing
MS ................. Master of Science
DRAFT
NCQAC Business Meeting July 12-13, 2018
252

Nursing Programs Annual Report
2016-2017 ACADEMIC YEAR
Introduction
Background
The Nursing Care Quality Assurance Commission (NCQAC) requires all nursing education programs to
provide information annually [WAC 246-840-520(3)]. This report summarizes 2016-2017 academic year survey
data from approved Washington State nursing programs and out-of-state distance learning programs,
highlighting selected data trends since 2002.
Forty-one approved nursing schools in Washington State completed the annual survey, including 12 universities
and 29 community and technical colleges (CTC). Seventy schools approved for clinical placements completed
the out-of-state survey, during the 2016-2017 academic year and 1,417 student clinical placements in
Washington State.
Determining accurate program completion rates is important but can be difficult because of the variety of
program types and student preference in the pace of their studies. This survey was revised in 2015-2016 to
refine and improve the measure for expected time of completion designed to honor individual variation yet
provide a measure for comparison across programs.
Schools were asked to describe how they calculate the completion rates using the following criteria. First,
schools indicated designated entry point for the program, choosing either the first nursing course, the first
course at the school, or other. Next, they were asked the allotted time for completion in semesters or quarters.
Finally, schools were asked to estimate the number of graduates who completed in 100 and 150 percent of the
allotted program time. An impressive 93 to 100 percent of all graduates across all in-state programs completed
within 150 percent of their allotted program time. More specifics on program completion rates are provided
below.
This report presents both in-state and out-of-state program survey results together. The number of nurses
licensed in the state and first-time NCLEX test takers are provided below for background and comparison. The
report will provide the student and faculty in-state program survey results of undergraduate and graduate
programs. Next, the more limited but valuable out-of-state program results are provided. When appropriate,
Washington state responses will be compared to national benchmarks and selected research findings. Finally,
there is a summary and analysis of the annual survey findings, with a list of recommended actions based on
these results and trend analysis.
Nurses Licensed in Washington
Number Licensed
The total number of licensed nurses is 116,835, including 11,541 PNs, 97,399 RNs, and 8,026 ARNPs. The
numbers include nurses from nursing programs in the State of Washington, other states and territories, and other
countries. These numbers represent a snapshot of nursing workforce supply data, which were downloaded April
2018 from the National Council for State Boards of Nursing (NCSBN, 2018). This is an estimate of the workforce
supply data. More accurate and complete workforce supply data will be available in 2019 after full
implementation of the requirement for nurses to complete a workforce survey when they are relicensed.
DRAFT
NCQAC Business Meeting July 12-13, 2018
253

Table 1. Licensed Nurses
License Type Active
PN 11,541
RN 97,399
ARNP 8,026
Total 116,835
NCSBN, retrieved April 2018 from https://reports.nursys.org/Dashboard.aspx?KEY=70E127DC-81BD-4E64-
A6E8-B7915032C37F
2017 NCLEX Test Takers
The total number of RN students taking the NCLEX test in 2017 for the first time was 2,611, which is an
increase from 2016 (2,393). There were 1,693 graduates from ADN programs and 992 from BSN or GE
programs taking the NCLEX in 2017. Those taking the NCLEX for the first time went from nearly equal
numbers from AD programs (487) and BSN (484) program in 2001 to almost twice as many from AD programs
as those from BSN programs. The total BSN and GE test takers since 2010 increased from 794 to 992.
Figure 1: Total Number of NCLEX First-Time Test Takers
0
500
1000
1500
2000
2500
3000
PN AD-RN BSN/GE RN Total
NCLEX First Time Test Takers
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
DRAFT
NCQAC Business Meeting July 12-13, 2018
254

The total ADN test takers since 2010 (1,692 to 1,696) has remained the same. The number of PN first-time test
takers was 495, similar to 498 in 2016; however, there is a continuing steady decline since 2011, when there
were 1,006 PNs taking the exam.
State Programs
Forty-one approved nursing schools in Washington State completed the annual survey. There are seven licensed
practical nurse (PN) programs, and 27 associate degree RN (AD-RN) programs. Five universities and three
community colleges offer RN to BSN (RNB) programs. Nine universities offer bachelor of science in nursing
(BSN) programs. There are three ADN to MSN (AD-MS) programs, two programs offering master’s degree
graduate entry to the RN (GE), and four master’s degree advanced registered nurse practitioner (ARNP) and six
other master’s programs. Finally, there are three post-master’s certificate (PMC) programs, five doctoral of
nursing practice (DNP) and two Ph.D. programs. The graduate programs are outlined below. Twenty-two of 29
community or technical colleges have national nursing accreditation and 11 of the 12 universities have national
nursing accreditation (one new program was in process at the time of the survey).
Undergraduate Programs
Since 2006, the number of pre-licensure graduates continued to increase as outlined below. In 2016-2017,
practical nursing programs (PN) had 264 graduates, a decrease from 293 graduates the previous year. Since
2001, the number of AD-RN graduates has nearly doubled. In 2016-2017, AD-RN programs graduated 1,741
students, which is an increase from 1,633 graduates the previous year.
The number of BSN program graduates has more than tripled since 2001. In 2016-2017, BSN programs
graduated 937 students, an increase from 881 the previous year. The total number of graduates from
undergraduate and graduate programs preparing students for the registered nurse (RN) licensure (AD-RN, BSN,
and GE) in Washington State has continued to increase over the past nine years from 2,360 in 2005-2006 to
2,678 graduates in 2016-2017. Those completing GE degrees are included in these graduation numbers because
they are pre-licensure programs; however, the GE student and faculty demographics are included with the
graduate program results.
Figure 2: Total Undergraduate Program Graduates by Type of Program
0
200
400
600
800
1000
1200
1400
1600
1800
2000
LPN
AD-RN
BSN/GE
RNB
DRAFT
NCQAC Business Meeting July 12-13, 2018
255

Table 2. Undergraduate Graduations
PN AD BSN/GE RNB
2013-2014 330 1,672 1,075 466
2014-2015 352 1,712 1,283 536
2015-2016 293 1633 967 718
2016-2017 264 1741 937 987
The table below provides undergraduate and GE program graduations for comparison to the past two years’
totals. There is a slight decrease in graduates from all program types except the RNB. The Institute of Medicine
Report (IOM) [2010], titled The Future of Nursing, identifies that nurses should achieve higher levels of
education and training through an improved education system that promotes seamless academic progression.
Washington State has been a leader in successful strategies for academic progression from AD to BSN. The
following table gives a different picture of these successful strategies when combining RN to BSN graduates
with BSN and GE graduate to compare with AD graduates.
Figure 3: Comparing AD RN and total BSN graduate trends
As described above, schools were asked to provide an allotted time for completion in semesters or quarters, and
to estimate the number of graduates who completed in 100 and 150 percent of the chosen allotted program time.
The completion rates for the undergraduate programs are provided below. The RNB programs have the lowest
completion rates (70 percent) in 100 percent of the allotted time, which is consistent with part-time programs.
AD programs have the highest completion rates with 93 and 100 percent completion rates, however, because the
allotted time for completion is chosen by the program, it is difficult to compare programs.
0
500
1000
1500
2000
2500
AD-RN
BSN-GE-RNB
DRAFT
NCQAC Business Meeting July 12-13, 2018
256

Table 3. State Undergraduate Program Completion Rates by Program
Program Type Percent of students graduating in 100 percent of the allotted time
PN 84 percent
AD 93 percent
RNB 70 percent
BSN 83 percent
The variation in completion rates may be related to the structure of the program, student demographics, choice
of allotted completion time, or other factors. PN and AD programs chose the first nursing course as their entry
point. PN programs chose an average of five quarters (60 credits) allotted completion time with a range of four
to seven (44 to 78 credits) and AD programs require an average of six quarters (84 credits) with a range of four
to 12 quarters (37 to 135 credits). There was a wide variation in the choices of allotted completion times for
RNB, and BSN programs because of the different structure and makeup of the programs.
Direct Transfer Agreement (DTA) 2016-2017
The support over four years of funding from the Robert Wood Johnson Foundation (RWJF) helped accelerate
the progress toward a higher educated workforce by supporting the adoption of the Direct Transfer Agreement
(DTA) streamlining academic progression between ADN and BSN programs. Several questions were added to
the annual survey to track progress and to evaluate success.
Thirteen community colleges had implemented the Associate in Nursing DTA at the time of the survey,
reporting a total of 1,117 students currently enrolled in this pathway. Three hundred graduates were awarded
this new degree.
Eleven of the 13 colleges that had not yet implemented the DTA were either in the process of implementation
(five) or interested in implementation, but not yet started (six). One school will not implement the DTA because
it has implemented its own RN to BSN program. A second school will not implement because it has an existing
agreement with a university that meets students’ needs.
The number of students graduating from a DTA program progressing directly to the BSN is an essential terminal
evaluation point. Six RNB programs in the state reported 327 students enrolled who graduated from DTA
programs and 40 RNB graduates representing a small percentage of the 987 total graduates from in-state RNB
programs.
However, with 1,117 students enrolled and 11 more colleges planning to implement the DTA, this streamlined
pathway from AD to BSN is poised to have a major effect on increasing the overall education level of nurses in
the state.
RN to BSN 2016-2017
The number of RN to BSN graduates in Washington schools rose sharply in 2010-2011 academic year and
continued to rise through 2016-2017 with 987 graduates and 2,461 students enrolled in RNB programs, a
significant increase from the previous year reported.
DRAFT
NCQAC Business Meeting July 12-13, 2018
257

Figure 4: Number of Enrolled and Graduated RNB Students by Year
The average number of clinical hours in PN programs is 369 with a range of 283-444. The average clinical
hours in AD-RN programs is 595 with a range of 493-870. Finally, the average clinical hours in the BSN
programs are 835 with a range of 780-960. The breakdown of the average clinical hours by program type is
seen below.
Overall direct care experiences make up an average of 87 percent of the total clinical experience hours in PN,
88 percent in ADN and 87 percent in BSN programs. Clinical observation and simulation percentages are
outlined in the table below.
Table 4: Clinical Hours by Program and Type.
Clinical Hours PN AD BSN
Average 369 595 835
Range 283-444 493-870 780-960
Percent Direct Care 87 88 87
Percent Observation 4 6 6
Percent Simulation 9 6 7
RNB Graduates RNB Enrolled
2006-2007 231 506
2007-2007 290 838
2008-2009 264 994
2009-2010 278 775
2010-2011 429 817
2011-2012 420 514
2012-2013 383 550
2013-2014 466 930
2014-2015 536 1038
2015-2016 718 2352
2016-2017 987 2461
0
500
1000
1500
2000
2500
3000
DRAFT
NCQAC Business Meeting July 12-13, 2018
258

Nursing faculty members plan, evaluate, and supervise clinical experiences for nursing students. Clinical
experiences provide direct patient care activities and increase student learning. Clinical learning is critical to
providing quality nursing education and can be a barrier to increasing enrollment. Thirty colleges and
universities reported inadequate clinical sites for their students as recently as 2012-2013. This number
decreased to 17 schools in 2015-2016 reporting difficulty and has increased again this year to 26 schools
reporting clinical site availability is not adequate. The most common difficulty is in obstetrics and pediatric
clinical sites for undergraduate programs and ARNP sites. Nursing programs could increase clinical practice
experience by use of simulation. WAC 246-840-534 allows LPN, RN, or RN to BSN programs to use
simulation up to fifty percent of a clinical, practice course. Nursing programs report use of simulation at a very
low percentage of total clinical hours.
Graduate Programs
Two categories of MSN graduates from master’s degree programs in nursing, but not ARNP (222) and RN to
MS graduates (179) are combined in Figure 6. There were 151 master’s prepared advanced registered nurse
practitioner graduates in 2016-2017 combined with the 17 post master’s certificate in nursing (PMCN)
graduates for display below.
Programs reported 140 DNP and 21 Ph.D. graduates for a total of 161 graduates with a nursing doctorate in
2016-2017. The total number of graduates from master’s and doctoral programs from 2005-2006 through 2016-
2017 is outlined below.
Although there were 87 graduates from GE programs during 2016-2017, the graduates were reported above
with undergraduate pre-licensure programs, so they will not be included in these graduation numbers.
Figure 5: Master’s and Doctoral Total Number of Graduates by Program
2005-2006
2006-2007
2007-2008
2008-2009
2009-2010
2010-2011
2011-2012
2012-2013
2013-2014
2014-2015
2015-2016
2016-2017
MSN/ADMN 139 101 136 125 95 160 143 136 257 241 421 401
MSN/ARNP/PMCN 177 151 171 214 204 228 178 175 187 192 145 168
PhD/DNP 10 13 18 16 33 37 78 55 72 104 141 161
0
50
100
150
200
250
300
350
400
450
DRAFT
NCQAC Business Meeting July 12-13, 2018
259

Nursing programs chose a time for completion of their programs, reporting students who graduated in 100
percent of that time and those who graduated in 150 percent of that time. Overall 95 percent students from
master’s programs preparing them for ARNP roles completed in the allotted time and 78 percent of MSN
students completed in the allotted time. PMCN programs reported a 53 percent completion and DNP programs
reported an 81 percent completion rate. The variations in completion rates may be related to the structure of the
programs or to students’ choice for slower progression plans because of personal or economic concerns.
The graduates prepared in different specialty areas meet needs across the state in primary care, education,
research, and other areas of practice. The graduates by program and specialty area are outlined below.
Graduates were reported from seven types of programs and 10 different specialty areas. There were 185
graduates from MSN programs with a specialty in education (72), administration (90), or other (23). Graduates
from programs preparing for the ARNP included 151 from MSN and 96 from DNP programs. The most
common specialty area for graduates of ARNP programs was the FNP (170).
Table 5. Graduates by Program and Specialty Area
CNS FNP ANP MHNP PNP GNP MW ANES ED Ad OTH TOT
ARNP 2 120 5 19 0 5 0 0 0 0 0 151
MSN 72 90 23 185
Pre ARNP
DNP 0 45 0 18 14 0 11 0 0 0 21 109
Post ARNP
DNP 5 2 1 12 20
TOTALS 2 170 5 39 14 5 11 0 72 90 56
Faculty and Student Ethnicity
Eighty-three percent of combined fulltime and part time faculty members are White/Caucasian, 5 percent Asian,
4 percent black/African American, and 3 percent for both Hispanic/Latino, and Native Hawaiian/other Pacific
Islander. Mixed race and American Indian/Alaskan Native are with1 percent each. Nursing programs reported
1,259 faculty members employed during 2015-2016 academic year. There were 611 full-time faculty members
and 648 part-time faculty members. The 110 with missing ethnicity data were not included in the percentage
calculations below.
Figure 6: Faculty and Student Race/Ethnicity Compared with Census
0%20%40%60%80%
100%
WashingtonState Census
2016
Students UG Graduate Faculty
Mixed Race
Hispanic/ Latino
Native Hawaiian / Other PacificIslander
Black/ African American
DRAFT
NCQAC Business Meeting July 12-13, 2018
260

Nursing Faculty
Increasing the overall education level of practicing nurses requires increased numbers of nursing faculty
members. Washington State regulations require a minimum of a master’s degree in nursing, or a bachelor’s
degree in nursing and a master’s degree in a related field, to teach registered nursing. Practical nursing faculty
members must have a minimum of a bachelor’s degree in nursing. Washington State nursing programs are
experiencing increasing difficulty in hiring nursing faculty members. In addition, the American Association of
Colleges of Nursing (AACN 2013-2014) reported on Salaries of Instructional and Administrative Nursing
Faculty in Baccalaureate and Graduate Programs in Nursing and predicted a wave of faculty retirements across
the U.S. over the next decade.
Strategies to attract and retain nursing faculty members continue to be explored by nursing programs. Workload
adjustment, sharing faculty, support for ongoing academic endeavors, and professional development are the
major strategies reported to address the problem. Beyond the need for increasing nursing faculty pay, nursing
programs identified faculty workload adjustment around the rigors of clinical instruction, committee work, and
mentoring of new faculty members as areas critical to program continuation or expansion.
Faculty Turnover
Community college nursing programs reported 13 percent of their nursing faculty members are anticipating
retiring in the next five years. University programs reported 15 percent. Additional factors adding to the
difficulties are resignations and orientation of new faculty members. There were 11 percent of the total PT and
FT faculty at community colleges who resigned the previous year and 6 percent at university programs.
Fourteen percent of faculty members at community colleges were in their first year of employment during 2016-
2017 compared to 13 percent in the university programs. Given the difficulty nursing programs are having
finding nursing faculty members, tracking this information as we develop strategies to address the nursing
faculty shortage will be essential.
Table 6: Combined Full time and part time Faculty Turnover 2016-2017
Percent expected to
retire in 5 years
Percent who resigned Percent in first year of
employment
Community and
Technical College
13 percent (86/645) 11 percent (73/645) 14 percent (93/645)
University 15 percent (86/589) 6 percent (38/589) 13 percent (74/589)
Faculty Education
Forty-two percent of nursing faculty members at universities are prepared at the master level and 50 percent at
the doctoral level, which is a slight increase in overall education level of faculty since the previous year.
Community and technical colleges have 69 percent of their faculty prepared at the MSN and 6 percent at the
DRAFT
NCQAC Business Meeting July 12-13, 2018
261

doctorate level showing little change from the previous year. The difference in faculty preparation between
community colleges and universities in 2016 - 2017 is illustrated below.
Figure 7: Faculty Level of Education 2016 - 2017
Faculty Salary
Salary is reported as a barrier to successful recruitment and retention of nursing faculty members. Respondents
answered the following questions, which were revised from the previous year’s survey. What are the contract
lengths and associated salary ranges for your full-time nursing faculty? Please do not include time for non-
teaching activities such as administration. The largest number of programs (38) reported nine-month contracts
with the lowest nine-month salary reported as $40,000 and the highest $200,313. The average salary ranges for
nine- and 12-month contracts at community colleges and universities are reported below. Community and
technical college faculty members’ average nine-month salary range was $53,469 to $67,525, and the university
average faculty nine-month salary range was $60,232 to $101,538.
Table 7: Average Faculty Salary Ranges
Contract Length Organization Low High
Nine-Month Community College $53,469 $67,525
Nine-Month University $60,232 $101,538
12-Month Community College $52,074 $73,352
12-Month University $80,307 $109,934
0
20
40
60
80
100
120
Univ CTC
Univ and CTC Faculty Preparation by percent of total faculty
Doc
MSN
MS
BS/BSN
DRAFT
NCQAC Business Meeting July 12-13, 2018
262

Out-of-State Programs
The out-of-state nursing program approval process for student clinical placement in Washington State began
2012. Initial data were gathered by calendar year in 2013 and 2014. The out-of-state survey was revised to
reflect the academic year beginning 2014-2015 so it could be reported with the data from in-state programs to
offer a more complete picture of nursing education program capacity in the state. Because the approval process
relates to clinical placements only, the data gathered are different from that gathered from the in-state programs.
The 70 nursing schools that completed the survey were approved at the time of the survey, for clinical
placements in Washington State.
Table 8: Approved Out of State Programs and Student Clinical Placements
College/University (70 total) Total Programs Total Clinical Students
Undergraduate 63 849
Graduate 169 568
Totals 232 1,417
Out-of-State Student Statistics
Approved out-of-state programs provided 1,417 clinical site placements for students across 232 programs in the
2016-2017 academic year, an increase from a total of 904 students in 2014-2015. The increase in ADN clinical
placements represent more accurate reporting of students in schools bordering Washington State in Oregon and
Idaho. The significant increase in the number of RN to BSN students is notable and represents schools from all
over the country, mirroring the increases in enrollments and graduations the in-state programs are experiencing.
Table 9: Number of Students with Clinical Site Placement from Out of State Programs
PN AD/RN BSN AD-BS AD-MS GE MNA MN ARNP PMNP. DNP PhD Total
2014-2015 25 89 323 105 15 0 180 110 18 31 0 904
2015-2016 25 159 349 142 8 2 162 125 12 33 0 1,017
2016-2017 48 198 354 249 19 0 313 137 31 66 2 1417
Thirty-two of the programs with clinical students in Washington State prepare graduates for PN or RN
licensure. There are four licensed practical nurse (PN) programs and six (AD-RN) programs. Twelve schools
have students in bachelor of science in nursing (BSN) programs. Three of the approved schools offer a graduate
entry (GE) option. The remaining programs with clinical students prepare graduates to advance their education
post-licensure. There are 28 AD to BS programs, six AD to MS, 35 ARNP and 39 other master’s programs.
Finally, there are 30 post master’s certificate programs (PMCN), 42 doctoral of nursing practice (DNP) and
eight Ph.D. programs. The total number of programs by type is outlined below.
Table 10: Number and Types of Out of State Programs with Clinical Site Placements
PN AD/RN RN-BS BSN AD-MS GE MN ARNP MN PMCN DNP PhD Oth Total
2014-2015 2 5 19 9 7 5 24 24 20 25 5 148
2015-2016 3 5 21 12 5 1 27 29 23 28 4 2 160
2016-2017 4 6 28 22 14 3 35 39 30 42 8 1 232
DRAFT
NCQAC Business Meeting July 12-13, 2018
263

Analysis/Recommendations
Washington State nurse educators made the commitment in 2011 for a higher educated and more diverse
nursing workforce, when the Council for Nurse Education in Washington State (CNEWS) and the Washington
Center for Nursing (WCN) collaborated to develop a Master Plan for Nursing Education (WCN, 2014). This
report highlights trends in the direction to meet the goals.
Academic Progression
Access to academic progression for nurses at all levels from PN to Ph.D. is important. The progress toward a
higher educated workforce continue to accelerate as the Direct Transfer Agreement (DTA) streamlining
academic progression between ADN and BSN programs is fully implemented. Nurse educators in Washington
have responded with increased enrollments and education capacity. The availability and adoption of the DTA
will facilitate a smooth pathway for community colleges and universities to collaborate on programs providing
students rapid and seamless progression to the BSN.
The recent addition of two RNB programs, and expansion of current RNB programs, has resulted in significant
increases in enrollment and graduations. Two community colleges offer RNB programs and more community
colleges are considering this option. Thanks to these significant efforts of nurse educators, the capacity needs
for RNB programs are being met at this time. Figure 3 above illustrates the number of BSN graduates has
outpaced the number of AD grads for the first time when combining RNB graduates to prelicensure BSN and
GE students. Figure 9 below provides a projection model indicating a prediction of the ratio of AD to BSN
graduates in 2025 if the rate of change since 2010 continues.
Figure 8. Projected graduates from AD and BSN programs maintaining current trends
0
500
1000
1500
2000
2500
3000
2010 2011 2012 2013 2014 2015 2016 2017 2018 2019 2020 2021
AD-RN
BSN TotalDRAFT
NCQAC Business Meeting July 12-13, 2018
264

One potential concern is a continued slight decline in pre-licensure BSN/GE graduates. Although a change in
reporting to improve the accuracy of the annual survey accounts for some of this decrease, it is important to
continue robust BSN enrollments and graduations to meet workforce needs.
Enrollment and graduations in graduate programs have shown impressive increases responding to the shortage
of nurse faculty, primary care providers, and researchers. Our state mirrors national trends with more ARNP
students moving to DNP programs from MSN programs. Enrollment and graduations in GE programs have
increased and provide additional options for student academic progression. Approval of out-of-state programs
for clinical placements helps ensure quality and additional capacity in high-need areas.
Although we are making impressive gains, we cannot meet our goal of RNs prepared at BSN or higher if
we continue to graduate and license more ADN nurses than BSN nurses.
More community college nursing program students must move directly to the BSN.
Students entering at the community college should have an opportunity to choose a program where they
exit and take NCLEX at the BSN.
University nursing programs in the state should increase growth in BSN and GE programs.
There must also continue to be an increase in graduate programs with an emphasis on preparing nurse
educators to serve as faculty members as program capacity increases. Continued increases in ARNP and
DNP programs for practice particularly in primary care will also be essential.
RNB program capacity is currently meeting need but must be maintained to serve community college
students moving more rapidly to the BSN.
Nursing Workforce Data
Increases in nursing school enrollment and graduates have moved to alleviate shortages. However, uneven
distribution is a longstanding feature of health care in the United States. A recent national study of nursing
workforce projected regional RN workforce growth from 2015 through 2030 in the U.S. (Auerbach 2017)
predicting zero expected growth in RN FTE per capita in the Pacific region (Washington, Oregon and
California). Until more accurate data is available, it is important to respond to the available data.
Starting in January 2018 a rule was passed by the Nursing Commission to require all licensee to complete
demographic data at the time of application or license renewal. Consequently, starting in 2019 accurate and
complete nursing supply data will be available to more precisely plan for the effect of regional and national
trends. Out-of-state programs approved for clinical placements have responded to current and future unmet state
needs, particularly in the areas of RNB, and graduate programs. We should continue to support quality out-of-
state programs through the NCQAC approval process.
Faculty
Meeting state nursing workforce needs, and educational advancement requires a sufficient, robust, and diverse
faculty pool. The Action Now! Initiative — launched by the Council for Nursing Education in Washington
State (CNEWS), the Nursing Care Quality Assurance Commission (NCQAC), and the Washington Center for
Nursing (WCN) — is working with practice partners and other stakeholders toward solutions to many nursing
education challenges. This group has identified ensuring a sufficient, robust, and diverse faculty pool as a
No. 1 priority. Analysis of the NCQAC Nursing Annual Report reinforces the urgency of the faculty need.
The overall educational preparation of faculty needs to be increased to meet state (WAC 246-840-523) and
national (CCNE 2017) standards for a master’s degree in CTC and a doctorate in universities. The table above
shows how many faculty must complete graduate studies potentially accruing additional debt and further
DRAFT
NCQAC Business Meeting July 12-13, 2018
265

straining income inequities. In addition to the imperative to increase nursing faculty education level, there are
impending retirements and vacancies. Right now, seventy percent (70 percent) of nursing programs report
faculty vacancies (WCN, 2017). Fifteen percent of university faculty and 13 percent of Community and
Technical College (CTC) faculty anticipate retirement in the next five years.
Providing a nursing faculty workforce that reflects the diversity of their students and the population of
Washington State is essential. A diverse nursing workforce can help improve patient and population health
outcomes, particularly with regard to reducing disparities in health (Williams SD 2014). The undergraduate
student diversity closely resembles Washington residents, and graduate students are showing some positive
changes. However, the nursing faculty diversity is furthest from the state population and there have been no
changes over the past four years (NCQAC 2017).
We must act now to increase the number of full time nurse educators by providing comparable salaries
with nursing practice, so we can recruit and retain nursing faculty.
Conclusions
Now is the time to take bold steps to accelerate our progress in providing the right educational mix of nurses for
safe and quality care in Washington State. The complex multiple education pathways in nursing can be a
challenge, but they also provide multiple opportunities to increase the overall education level of nurses. Across
settings, nurses are being called upon to coordinate care and to collaborate with a variety of health
professionals, including physicians, social workers, physical and occupational therapists, and pharmacists, most
of whom hold master’s or doctoral degrees. (IOM 2011) The Future of Nursing: Leading Change, Advancing
Health. RNB, masters, and doctoral enrollments and graduations have continued to increase, significantly
adding to a higher educated workforce, but we must continue to accelerate our progress to meet the growing
health care needs of the residents of Washington State.
DRAFT
NCQAC Business Meeting July 12-13, 2018
266

References:
Aiken LH, Sloane DM, Bruyneel MS, et al., for the RN4CAST consortium. 2014. Nurse staffing and education
and hospital mortality in nine European countries: a retrospective observational study. Lancet, 383(9931): 1824-
1830.
Aiken LH, Cimiotti JP, Sloane DM, et al. 2011. Effects of nurse staffing and nurse education on patient deaths
in hospitals with different nurse work environments. Medical Care, 49(12): 1047-1053.
Aiken LH, Clarke SP, Cheung RB, et al. 2003. Education levels of hospital nurses and surgical patient
mortality. Journal of the American Medical Association, 290(12): 1617-1623.
Auerbach, D., Buerhaus, P., & Staiger, D
(2015). Do Associate Degree Nurses Fare Differently in the Nurse Labor Market Compared to Baccalaureate
Prepared RNs? Nurse Economics, 33(1), 8-13.
Auerbach, DI, Staiger, DO (2017) How fast will the registered nurse workforce grow through 2030? Projections
in nine regions of the country, Nursing Outlook.
Charting Nursing’s Future “The Case for Academic Progression” issue
(http://www.rwjf.org/content/dam/farm/reports/issue_briefs/2013/rwjf407597).
Institute of Medicine. (2010). The future of nursing: Leading change, advancing health.
Retrieved from http://www.nap.edu/catalog/12956.html
Kutney-Lee A, Sloane DM, & Aiken LH. 2013. An increase in the number of nurses with baccalaureate degrees
is linked to lower rates of post surgery mortality. Health Affairs, 32(3): 579-586.
National Council of State Boards of Nursing (NCSBN), retrieved April 11, 2017 from
https://reports.nursys.org/Dashboard.aspx?KEY=70E127DC-81BD-4E64-A6E8-B7915032C37F.
Needleman J & Hassmiller S. 2009. The role of nurses in improving hospital quality and efficiency: real-world
results. Health Affairs 2,8(4): w625-w633.
US Census (2015). Retrieved from http://www.census.gov/quickfacts/chart/RHI125214/53.
US Census Bureau (2015) Washington State statistics retrieved April 11, 2017 from
https://www.census.gov/quickfacts/table/PST045216/53.
Washington Center for Nursing (2014). Retrieved from https://www.wcnursing.org/nursing-education/master-
plan-for-nursing-education/.
Yakusheva, O., Lindrooth, R., Weiss, M. 2014. Economic Evaluation of the 80 percent Baccalaureate Nurse
Workforce Recommendation A Patient-level Analysis. Medical Care, 52 (10).
DRAFT
NCQAC Business Meeting July 12-13, 2018
267