manubriosternal arthritis: the role of thoracic...
TRANSCRIPT
Annals of the Rheumatic Diseases, 1986; 45, 345-348
Case report
Manubriosternal joint dislocation in rheumatoidarthritis: the role of thoracic kyphosisM C KELLY, N D HOPKINSON, AND G C ZAPHIROPOULOS
From the Department ofRheumatology, Coventry and Warwickshire Hospital, Coventry
SUMMARY A case report of manubriosternal joint (MSJ) dislocation in a rheumatoid patientwith thoracic kyphosis is presented together with a review of the relevant literature. Variations inthe anatomical nature of the MSJ between normal individuals are described. In 43% of thepopulation its characteristics are noted to be such that it may be involved in rheumatoid arthritis(RA). A joint thus involved can be dislocated by forces generated by longstanding thoracickyphosis and transmitted to the manubrium via the first rib. Xeroradiographs of the MSJ regionin our patient showed dislocation of the joint in the upright position and its subsequent reductionon lying the patient flat. We suggest that this demonstrated reduction is secondary to thelessening of the thoracic kyphosis that occurs in the supine position. It is concluded that in RAMSJ dislocation is a function of thoracic kyphosis.
Radiological surveys of the manubriosternal joint(MSJ) of patients with rheumatoid arthritis (RA)have shown its frequent involvement in the diseaseprocess. '-3However, the number of case reports of actual
dislocation of the joint is very small. One furthersuch case is presented here, and the literature isreviewed. In addition, the development andanatomy of the joint in so far as it is relevant to itsinvolvement in RA is outlined and the factorsinvolved in its dislocation are discussed.
Case history
A 54 year old lady with seropositive RA of 14 yearsduration had noted an increasing prominence overher sternum for three years. It was otherwiseasymptomatic. There was no history of trauma. Shehad occasional episodes of vasculitis and had beenon steroids for many years.
Clinically there was evidence of widespread
Accepted for publication 21 August 1985.Correspondence to Dr G C Zaphiropoulos. Department ofRheumatology. Coventry and Warwickshire Hospital. CoventryCVI 4FH.
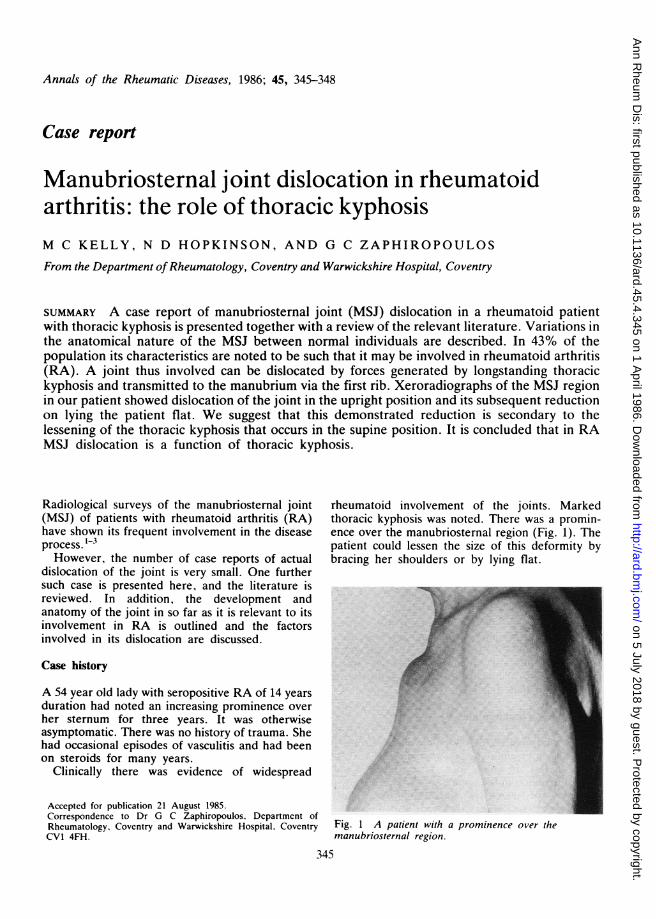
rheumatoid involvement of the joints. Markedthoracic kyphosis was noted. There was a promin-ence over the manubriosternal region (Fig. 1). Thepatient could lessen the size of this deformity bybracing her shoulders or by lying flat.
Fig. 1 A patient with a prominence over themanubriosternal region.
345
on 5 July 2018 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.45.4.345 on 1 A
pril 1986. Dow
nloaded from
346 Kelly, Hopkinson, Zaphiropoulos
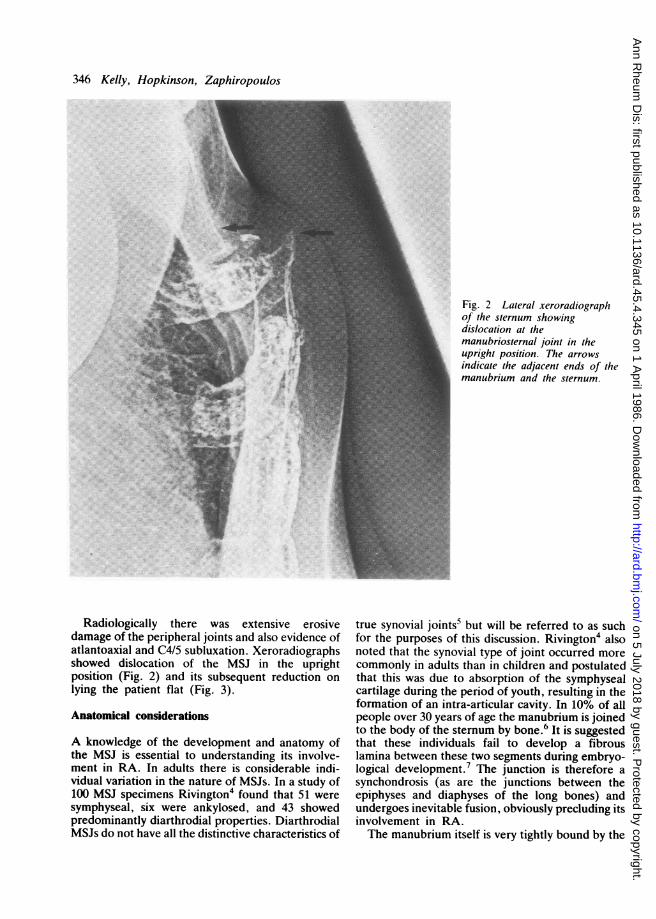
Fig. 2 Lateral xeroradiographof the sternum showingdislocation at themanubriosternal joint in theupright position. The arrowsindicate the adjacent ends of themanubrium and the sternum.
Radiologically there was extensive erosivedamage of the peripheral joints and also evidence ofatlantoaxial and C4/5 subluxation. Xeroradiographsshowed dislocation of the MSJ in the uprightposition (Fig. 2) and its subsequent reduction onlying the patient flat (Fig. 3).
Anatomical considerations
A knowledge of the development and anatomy ofthe MSJ is essential to understanding its involve-ment in RA. In adults there is considerable indi-vidual variation in the nature of MSJs. In a study of100 MSJ specimens Rivington4 found that 51 weresymphyseal, six were ankylosed, and 43 showedpredominantly diarthrodial properties. DiarthrodialMSJs do not have all the distinctive characteristics of
true synovial joints5 but will be referred to as suchfor the purposes of this discussion. Rivington4 alsonoted that the synovial type of joint occurred morecommonly in adults than in children and postulatedthat this was due to absorption of the symphysealcartilage during the period of youth, resulting in theformation of an intra-articular cavity. In 10% of allpeople over 30 years of age the manubrium is joinedto the body of the sternum by bone.6 It is suggestedthat these individuals fail to develop a fibrouslamina between these two segments during embryo-logical development.7 The junction is therefore asynchondrosis (as are the junctions between theepiphyses and diaphyses of the long bones) andundergoes inevitable fusion, obviously precluding itsinvolvement in RA.The manubrium itself is very tightly bound by the
on 5 July 2018 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.45.4.345 on 1 A
pril 1986. Dow
nloaded from
Manubriosternal joint dislocation in RA 347
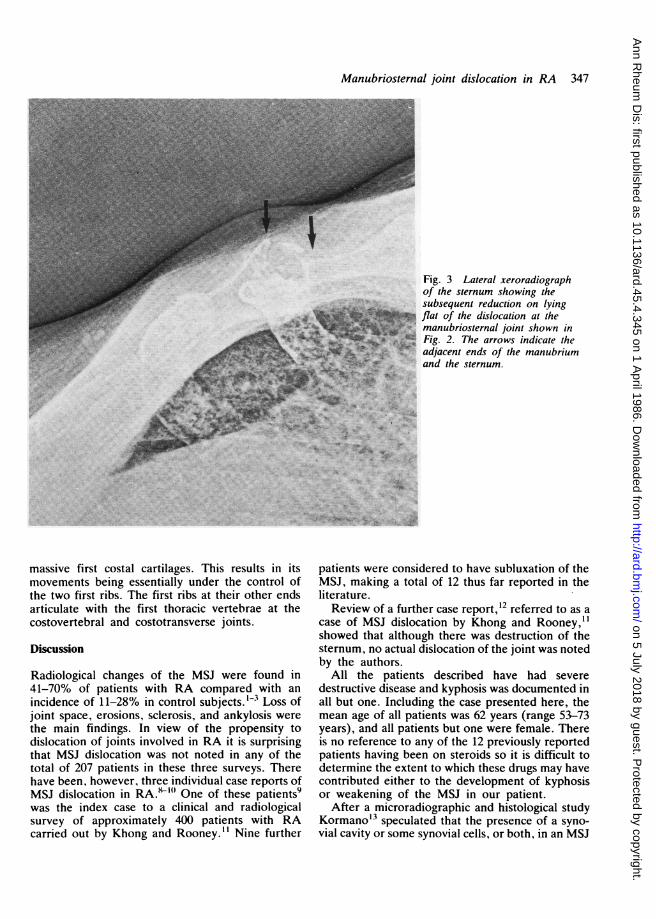
Fig. 3 Lateral xeroradiographof the sternum showing thesubsequent reduction on lyingflat of the dislocation at themanubriosternal joint shown inFig. 2. The arrows indicate theadjacent ends of the manubriumand the sternum.
massive first costal cartilages. This results in itsmovements being essentially under the control ofthe two first ribs. The first ribs at their other endsarticulate with the first thoracic vertebrae at thecostovertebral and costotransverse joints.
Discussion
Radiological changes of the MSJ were found in41-70% of patients with RA compared with anincidence of 11-28% in control subjects. 1-3 Loss ofjoint space, erosions, sclerosis, and ankylosis werethe main findings. In view of the propensity todislocation of joints involved in RA it is surprisingthat MSJ dislocation was not noted in any of thetotal of 207 patients in these three surveys. Therehave been, however, three individual case reports ofMSJ dislocation in RA.i'" One of these patients9was the index case to a clinical and radiologicalsurvey of approximately 400 patients with RAcarried out by Khong and Rooney." Nine further
patients were considered to have subluxation of theMSJ, making a total of 12 thus far reported in theliterature.Review of a further case report, 12 referred to as a
case of MSJ dislocation by Khong and Rooney,i"showed that although there was destruction of thesternum, no actual dislocation of the joint was notedby the authors.
All the patients described have had severedestructive disease and kyphosis was documented inall but one. Including the case presented here, themean age of all patients was 62 years (range 53-73years), and all patients but one were female. Thereis no reference to any of the 12 previously reportedpatients having been on steroids so it is difficult todetermine the extent to which these drugs may havecontributed either to the development of kyphosisor weakening of the MSJ in our patient.
After a microradiographic and histological studyKormanoi3 speculated that the presence of a syno-vial cavity or some synovial cells, or both, in an MSJ
. 4.1.
?:.i, --- I
...'t
*1lt-- -P7.
Im.- 41'
on 5 July 2018 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.45.4.345 on 1 A
pril 1986. Dow
nloaded from
348 Kelly, Hopkinson, Zaphiropoulos
could lead to its being involved in RA. Reference tothe anatomical considerations above indicates such asituation in some 43% of the population. Thisinvolvement will lead to bony ank4losis of the jointin as many as 12% of patients. However, suchweakening of the joint as occurs in the substantialmajority of patients will render it susceptible todislocation in the event of it being subjected toappropriate forces.
Dislocation of the MSJ as a consequence offlexion-compression injuries of the thoracic spinehas been well described in traumatology."4 15Fowler16 in his comprehensive review suggests thatacute flexion of the thoracic spine transmits pre-dominantly via the first ribs a downward andbackward force to the manubrium, leading to itsseparation from the body of the sternum. The lowerborder of the manubrium then occupies a positionbelow and behind the upper border of the body.We suggest that chronic flexion of the thoracic
spine transmits via the first rib similar if less acuteforces to the manubrium, which can ultimately leadto dislocation of a joint weakened by RA. In anumber of Fowler's cases as in ours reduction of thedislocation was achieved by lying the patients flat.
In RA an increased incidence of thoracic kyphosishas been described.'7 18 Kyphosis also increaseswith age, and the rate of increase is higher infemales than in males.'9 21) This appears moreobvious after the age of 40 years.21
Accordingly, MSJ dislocation would be expectedto occur predominantly in older women if thoracickyphosis, as we suggest, is indeed the determiningfactor. That virtually all of the small number ofpatients described in the literature are older femaleswith kyphosis seems to lend support to this view.However, the main evidence for the important roleof thoracic kyphosis is provided by the demon-strated reduction of the MSJ dislocation in ourpatient on lying her flat.
Furthermore, minor degrees of joint subluxationmay similarly be reduced during radiological ex-amination. Lateral radiographs of the chest in orderto include the MSJ would involve patients beingpositioned with their shoulders braced, thus lessen-ing thoracic kyphosis. This may in part account forthe low number of reported cases of dislocation ofthe joint in RA.
In summary, the anatomical development of theMSJ lends itself to potential involvement in RA in43% of the population. When the joint is weakenedby RA longstanding thoracic kyphosis transmitsforces to the manubrium via the first rib that canultimately lead to its dislocation.
The authors wish to thank Mrs Joyce Hill for her assistance inpreparing this manuscript.
References
1 Savill D L. The manubriosternal joint in ankylosing spondylitis.J Bone Joint Surg 1951; 33B: 56-64.
2 Dilsen N, McEwen C, Poppel M, Gersh W J, Di Tata D,Carmel P. A comparative roentgenologic study of rheumatoidarthritis and rheumatoid (ankylosing) spondylitis. ArthritisRheum 1962; 5: 341-68.
3 Laitinen H, Saksanen S, Suoranta H. Involvement of themanubriosternal articulation in rheumatoid arthritis. ActaRheumatol Scand 1970; 16: 40-6.
4 Rivington W. Remarks on dislocations of the first and secondpieces of the sternum. Med-Chir Trans 1874; 57: 101-17.
5 Warwick R, Williams P L, eds. Gray's anatomy. London:Longman, 1973; 390.
6 Warwick R, Williams P L, eds. Gray's anatomy. London:Longman, 1973; 420.
7 Ashley G T. The morphological and pathological significance ofsynostosis at the manubriosternal joint. Thorax 1954; 9: 159-66.
8 Rapoport R J, Carrera G F, Kozin F. Manubriosternal jointsubluxation in rheumatoid arthritis. J Rheumatol 1979; 6: 174-7.
9 Holt M E, Rooney P J. Manubriosternal joint subluxation inrheumatoid arthritis. J Rheumatol 1980; 7: 260-2.
10 Wiseman M J. Dislocation of the manubriosternal joint inrheumatoid arthritis. Ann Rheum Dis 1981; 40: 307-8.
11 Khong T K, Rooney P J. Manubriosternal joint subluxation inrheumatoid arthritis. J. Rheumatol 1982; 9: 712-5.
12 Perrin R L, Poller W R, Perkins D G. Sternal destruction inrheumatoid arthritis. Skeletal Radiol 1977; 2: 95-7.
13 Kormano M. A microradiographic and histological study of themanubriosternal joint in rheumatoid arthritis. Acta RheumatolScand 1970; 16: 47-59.
14 Sevitt S. Fatal road accidents. Injuries, complications andcauses of death in 250) subjects. Br J Surg 1968; 55: 481-505.
15 Park W M, McCall I W, McSweeney T, Jones B F. Cervico-dorsal injury presenting as sternal fracture. Clin Radiol 1980;31: 49-53.
16 Fowicr A W. Flexion-compression injury of the sternum. JBone Joint Surg 1957; 39B: 487-97.
17 Sharp J. Differcntial diagnosis of ankylosing spondylitis. BrMed J 1957; i: 975-8.
18 Bradford D S. Kyphosis. Clin Orthop 1977; 128: 2-4.19 Cowan N R. The frontal cardiac silhoucttc in older peopic. Br
Heart J 1965; 27: 231-5.20 Fon G T, Pitt M J, Thics A C. Thoracic kyphosis: rangc in
normal subjects. AJR 1980; 134: 979-83.
on 5 July 2018 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.45.4.345 on 1 A
pril 1986. Dow
nloaded from