managing diabetes in peritoneal dialysis western pd days april 9, 2015 presented by : sharon kelly...
TRANSCRIPT
Managing Diabetes in Peritoneal Dialysis
Western PD Days
April 9, 2015
Presented by :
Sharon Kelly RN BN CDE
Pat Holmes RN BN BSc MSc CDE
Diabetes Nurse Clinicians
Southern Alberta Renal program
DISCLOSURES

Renal Replacement Therapies:Chronic Critical Care for Years to
Decades.
Critical care medicine provides technologically advanced support for failing organ systems , thereby preventing what previously was the
inevitable demise of the organism.
In doing so, man enters an unnatural state supported by medications and machines.
Hollander et al; Nutrition in clinical Practice, 21:587 – 604, Dec./2006.
TEAMWORK- the power of a multidisciplinary approach
Patient and family
Nephrologist
Nurse Clinician
Diabetes Educator
Pharmacist
Registered Dietitian
Social Work

OUTLINE
Clinical Practice Guidelines and Recommendations
Diabetes characteristics in advanced CKD.Glucose patterns.Targets
Significance of Hgb A1C and home glucose testingThe role of Lifestyle assessment
How glycemia may affect the peritoneal membrane
Tailoring Diabetes Drugs to BG patterns and PD.
Cardiovascular risk in Diabetes and in CKD

Clinical Practice Guidelines
Canadian CPG 2013KDIGO, 2012KDOQI 2014ADA: Standards of Medical Care in Diabetes: 2015Kidney Disease: A Report from an ADA Consensus Conference/Oct. 2014CPG and Recommendations on PD Adequacy 2011.

Canadian Clinical Practice Guidelines 2013
Focus on prevention, screening, therapies, complications, DM1, DIP. Targets 4-7 mmol fasting ; 5-8 mmol PC HgbA1C < 7%Little to no information on management in ESRDIndividualized A1C targets for people with:• longer duration of diabetes• established CV risk factors• severe hypoglycemia episodes• higher ac and pc meal target glucose ranges
Diabetes Drug use

KDIGO, 2012
Importance of glycemic control to improve outcomes in patients with diabetes and ckd due to higher risk.
Integration with other chronic disease management including diabetes, hypertension and heart failure.
Diabetes Drug Use in CKD

KDOQI, 2012
Extensive discussion re : diabetes drug use in Stage 4- 5 CKD
Interpretation of Hg A1C, similar to Canadian CPG
Hypoglycemia risk:Prolonged action of some diabetes drugsImpaired gluconeogenesis
Optimize safety

ADA: Standards of Medical Care in Diabetes: 2015
Emphasize management of albuminuria and hypertensionGlycemic control as CVD risk management
Referral to Nephrology when GFR is < 30 ml/min. Discussion on factors that affect the A1C value ; individualize goals Similar ac/pc meal glucose goals (AC 4.4-7.2 mmol ;Pc < 10.0 mm0l)Use of real-time CGMUse of Insulin Analogs – prev. of Hypoglycemia

Kidney Disease: A Report from an ADA Consensus Conference/Oct. 2014
• Glycemic control and regression of albuminuria – Hgb A1C < 8%.
• Increased incidence of CVD events associated with CKD and Diabetes.
• Factors that affect the A1c value• Hypoglycemia: longer duration of diabetes
drug effects, malnutrition, deficiency of gluconeogenic precursors
• Hypoglycemia as a reason for higher mortality

CPG’s and Recommendations on Peritoneal Dialysis Adequacy – 2011
• Volume status as important parameter of “adequate PD”
• Relationship of volume status to CVD risk factors and risk reduction.
• Address Glycemic control and exposure to hypertonic glucose solutions and contribution to UF
• Increased atherogenic profile of PD patients• “Few data exist to guide the management of diabetes
in this population” (p 15). • Adherence to CPG where possible; avoid
hypoglycemia• Address some diabetic drugs
Diabetes and CKD
Uremia alters the entire metabolism including that of carbohydrates, proteins and fats. It also causes electrolyte disturbances and upsets mineral and hormonal homeostasis. Directly or indirectly, glucose metabolism is disturbed by all these things’.
Kumar, K.V. S. et al: Glycemic Control in Patients of Chronic Kidney Disease. \www.ijddc.com/article.asp?issn=0973-3939;year=2007; volume27; issue=4
International Journal of Diabetes in Developing Countries.

DIABETES IN STAGES 4 / 5
Chronic Kidney Disease associated with :
INCREASED INSULIN RESISTANCE –
Factors include uremia, anemia, elevated PTH, deficient Vit D, metabolic acidosis, increased plasma FFA, atherogenic lipid profiles, increased pro-inflammatory cytokines
DECREASED INSULIN DEGRADATION – PARTICULARLY AT GFR< 20%

Should we apply clinical practice guidelines, based on studies on people with adequate kidney function, to Stage 5 CKD and Peritoneal Dialysis?
Question?

What is missing?

We are missing:
The role of the kidney in glucose metabolism:
A practical treatment model.
Target blood glucose ranges in PD.
Lab/meter comparisons
Research

CV risk in PD populations + Diabetes - Why is glycemic control important?
• Hypoglycemia• Hyperglycemia• Glucose variability• Inflammatory response to both hyperglycemia and
PD solutions.

Hypoglycemia : The Treatment Limiting Factor

Recovery from hypoglycemia is impaired.Key factors: renal atrophy, growth hormone and IGF aberrations, blunted glucagon and epinephrine response, prolonged action of insulin
Severe hypoglycemia can lead to falls, cardiac ischemia and arrhythmias, seizures, brain damage.

+CKD, +Diabetes-CKD, +Diabetes
+CKD, -Diabetes-CKD, -Diabetes
0
1
2
3
4
5
6
7
8
9
Glucose < 3.9 and >3.3 mmol/L
Glucose < 3.3 and >2.8 mmol/L
Glucose < 2.8 mmol/L
3.28
1.661.53
1
7.21
3.56
1.58
1
8.43
4.09
1.62
1
Risk for hypoglycemia in veterans classified by presence or absence of chronic kidney disease
(CKD) and diabetes.
Moen M F et al. CJASN 2009;4:1121-1127
Inci
dent
Rat
e Ra
tios
All p-values <0.0001, (95% CI)

Prolonged action of insulin is not the only factor.
Without a model of renal glycemic function, we are:
Looking for lows in all
the wrong places !

MOST OF OUR LIVES ARE SPENT IN THE POSTPRANDIAL STATE
Breakfast Lunch Dinner 0.00 am 4.00 am
Postprandial state
Postabsorptive state
Fasting state
Monnier L. et al. European Journal of Clinical Investigation 2000; 30 Suppl 2:3–11.

The Kidneys:Contribute to blood glucose 24/7 !
A safety catch to provide constant glucose balancing.
Eliminate excess glucoseGluconeogenesis: fasting, post absorptive and post prandial Recovery from hypoglycemia
The Diabetes Insulin Model: No Kidney Disease
Based on excessive gluconeogenesisThe liver gets most of the credit for hyperglycemiaKidneys thought to contribute about 20 % of glucose in fasting state.Cano: Up to 54 % after hypoglycemia
Bedtime long acting insulin used to prevent fasting hyperglycemia. No consideration of renal disease.

When Do We Need Insulin ?
•
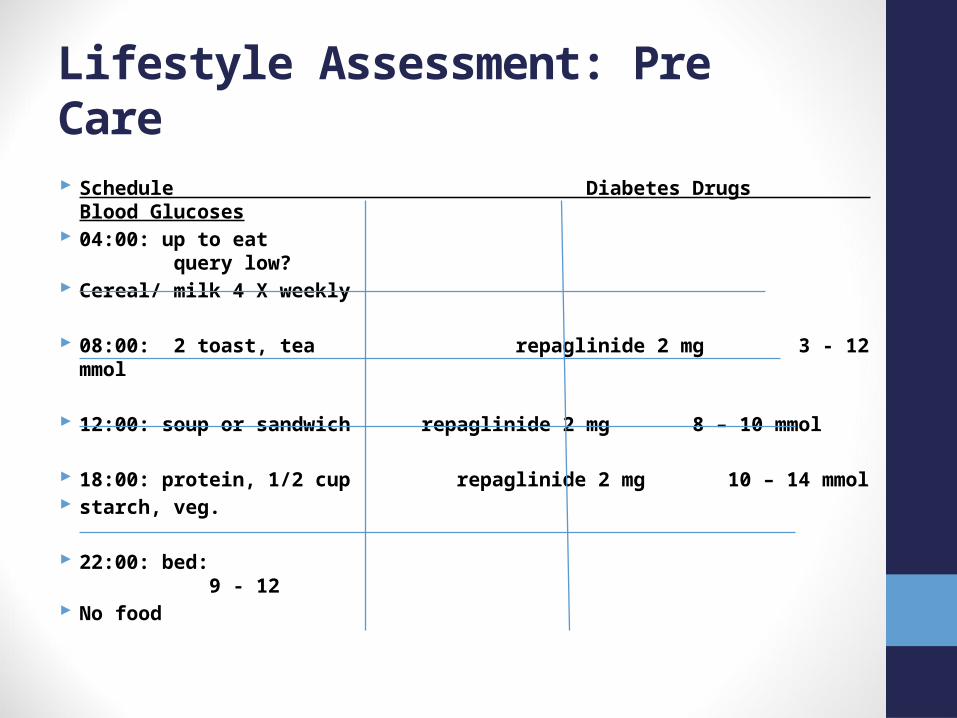
Lifestyle Assessment: Pre Care
Schedule Diabetes Drugs Blood Glucoses 04:00: up to eat query low? Cereal/ milk 4 X weekly
08:00: 2 toast, tea repaglinide 2 mg 3 - 12 mmol
12:00: soup or sandwich repaglinide 2 mg 8 – 10 mmol
18:00: protein, 1/2 cup repaglinide 2 mg 10 – 14 mmol starch, veg.
22:00: bed: 9 - 12 No food

From observation, people have difficulty going without carbohydrate for more than 4 – 6 hours.

For both Pre Care and PD clients:
Determine
when people are fasting from
carbohydrates.

Glucose Patterns in Peritoneal Dialysis:
Look for both hyperglycemia and hypoglycemia.
Unique use of diabetes drugs
Unique dietary strategiesUnique intake of carbohydrate from peritoneal dialysis solutions.
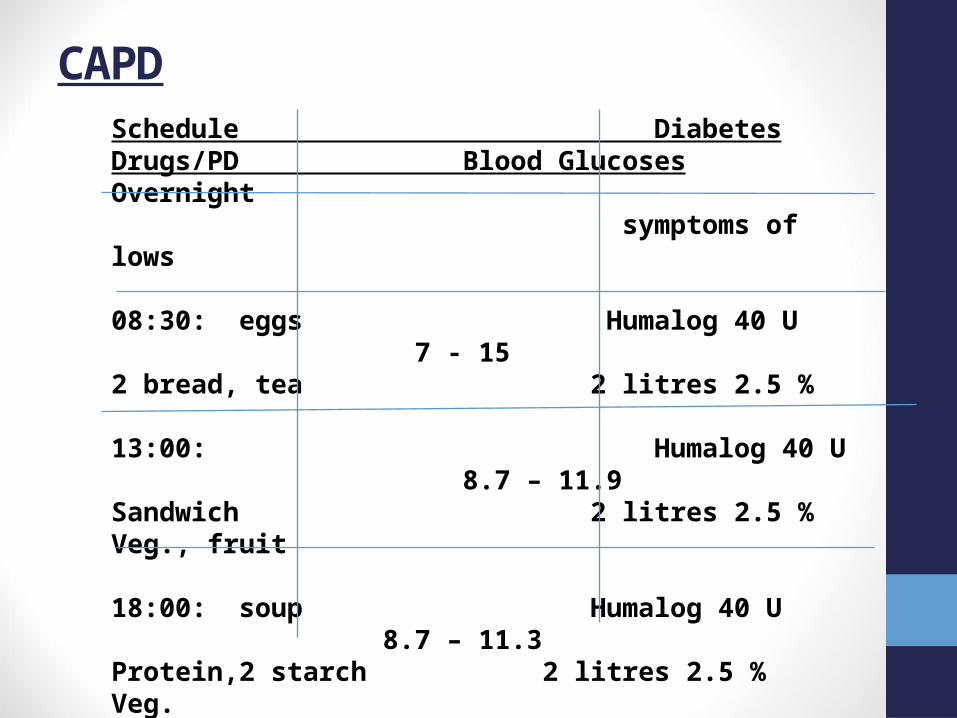
Schedule Diabetes Drugs/PD Blood GlucosesOvernight symptoms of lows
08:30: eggs Humalog 40 U 7 - 152 bread, tea 2 litres 2.5 % 13:00: Humalog 40 U 8.7 – 11.9Sandwich 2 litres 2.5 %Veg., fruit 18:00: soup Humalog 40 U 8.7 – 11.3 Protein,2 starch 2 litres 2.5 %Veg.
22:00: Lantus 60 U 11 – 15 no food 2 litres extraneal
CAPD
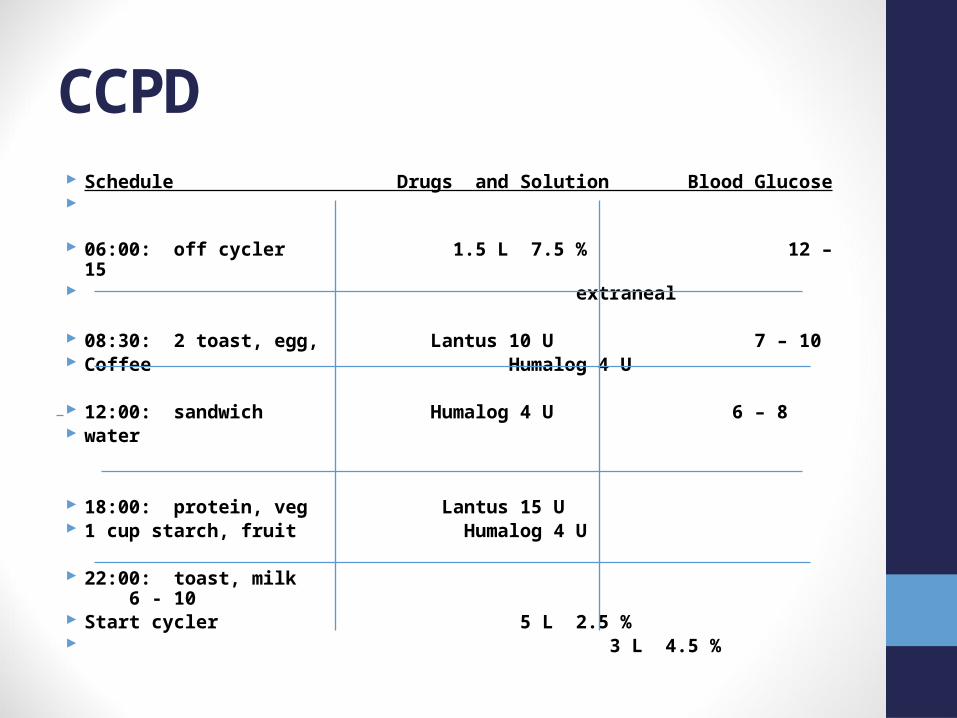
CCPD Schedule Drugs and Solution Blood Glucose 06:00: off cycler 1.5 L 7.5 % 12 – 15 extraneal
08:30: 2 toast, egg, Lantus 10 U 7 – 10 Coffee Humalog 4 U
12:00: sandwich Humalog 4 U 6 – 8 water
18:00: protein, veg Lantus 15 U 1 cup starch, fruit Humalog 4 U
22:00: toast, milk 6 - 10 Start cycler 5 L 2.5 % 3 L 4.5 %
Goals of Diabetes Care Specific to Peritoneal Dialysis
Prevent hyper- and hypo - glycemia
Stabilize blood glucose patterns
Adapt to diet and gastro intestinal disorders
Adapt diabetes therapies to dialysis prescription
Promote ULTRAFILTRATION and volume control
Prevent infections
Prevent further complications of diabetes
ENHANCE PATIENT WELL-BEING

PD Solutions and Glycemic control
With the use of dextrose solutions, high MW glucose polymers such as icodextrin and non-glucose based solutions such as Nutraneal – the CHALLENGE is to control glycemia in an environment of intermittently high and prolonged glucose exposure.
1744- red wine used as osmotic agent in peritoneal lavage!

Post prandial period after meals and with PD solutions:
How do we interpret non fasting blood glucoses ?

Canadian Clinical Practice Guidelines 2013
FPG or preprandial PG target of 4.0–7.0 mmol/L and a 2-hour pc target of 5.0–10.0 mmol/L ADA: 4 .4 – 7.2 pc < 10 mmol
[Grade B, Level 2 (2) for type 1; Grade B, Level 2 (1,11) for type 2 diabetes].
Canadian Clinical Practice Guidelines 2013
LACK of evidence-based research where effect of postprandial glucose values on outcome is the major objective of the study.
Most of the large outcome trials conducted so far have been mostly based on preprandial glucose and A1C targets.
? Contribution of Post prandial hyperglycemia to complications as an independent variable.

PD patients have:
2 hours immediate post prandial period 4 hours total post prandial.
Overlap with 16 hours daily of CAPD.Add 8 hours for CCPD.
14 – 16 hour daily immediate post prandial post prandial period.16 – 20 hour total post prandial period. May retain some glucose solutions after draining.

How do we determine target glucose goals? For safety, aim for higher than 4 – 7 mmol ac meals and higher than 5 – 10 pc meals.Eg: 6 – 9 ac meals and 7 – 12 pc meals? Encourage research re: blood glucose patterns and target goals in PD. Encourage focused SMBG

How do we determine the accuracy of home glucose testing?
Lab/Meter comparisons. Companies recommend fasting comparisons. PD patients live in post prandial state.

Lab/Meter Comparisons
Fasting lab/meter comparisons: Venous and capillary blood samples carry about the same amount of glucose at 4.5 or more hours after eating.
Up to 15 % difference is acceptable.

Post prandial period:
A glucose meter may read up to 30 % higher than the lab in the immediate post prandial period.
Cembrowski, George et al: Assessing the Accuracy of Your Blood Glucose Meter. Lifescan, 2000.

How do we interpret glucose readings in peritoneal dialysis?
Assume there is 15 – 20 % less glucose in veins than in capillary blood samples.
Base assumptions on frequent lab/meter comparisons done in a non fasting state.

How Do we interpret Hg A1C values?
Glycated hemoglobin (A1C) is an estimate of mean glucose levels over the previous 3 to 4 months for most individuals.
Blood glucose (BG) in the previous 30 days contributes 50% of the result.The prior 90 to 120 days contributes 10% (2,3).
In renal disease, red blood cell physiology is an strong contributor to the A1C value.


Assess Red Blood Cell Physiology and Glycemia: Diabetes CPG 2013
• Raise A1C• Hyperglycemia• Acidosis• Hypothyroidism• Iron deficiency anemia• B 12 deficiency• Splenectomy• Hemoglobinopathies• Hypoxia• Race other than
Caucasian (.3 - .5 %)• Alcoholism
• Lower A1C• Hypoglycemia• Increased RBC pH• Shortened lifespan of the
red blood cell• Erythropoeitin agents• Hemoglobinopathies• Blood loss with HD and
with frequent blood sampling
• Blood transfusions
TOOL: Hg A1C Profile on Electronic Chart
Hg A1C Hg Fasting glucose Random glucose lab /meter
Iron studiesTriglycerides TSHVitamin D B 12 WBC PTH

Glycated Albumin (fructosamine)A measure of glycosolation of plasma albumin.Based on an expected 20 day half life of albumin. Accurate in HD.
PD: loss of 5 – 15 gm protein daily via dialysate, including albumin. Add albumin losses via residual kidney function.
Half life of albumin is variable and less than 20 days.

Optimization of Blood Glucose Values
Consider all factors affecting blood glucoses. Blend SMBG tests, lab tests, diabetes drugs, PD solutions, food, activity and PD changes.
* Consider abrupt onset of glucose diffusion at start of PD and abrupt stop when PD glucose solution is drained.
Teamwork: Client, family, nephrologist, dietitian, renal nurses, endocrinologists, diabetes nurses, social workers, pharmacists, family physician.
Peritoneal Membrane
Hypothesis: Chronic exposure to glucose containing solutions promotes peritoneal membrane damage over time (De Vriese).
“Glucose likely has a detrimental effect on the peritoneal membrane both from systemic hyperglycemia and from local effects of the dialysate. [Chugh, et.al 2014]
Diabetes:Uremic people with diabetes have a greater degree of damage to the peritoneal membrane BEFORE STARTING PD.
Can we minimize damage and prolong the PD lifespan of the peritoneal membrane with appropriate blood glucose control?

MEDIATORS OF ENDOTHELIAL INFLAMMATION WITH
HYPERGLYCEMIA
MEDIATORS OF PERITONEAL MEMBRANE INFLAMMATION

Ultrafiltration ‘Analysis of the data between small solute transport rate and fluid transport parameters could contribute to an understanding of why peritoneal ultrafiltration capacity is often reduced in high transporters, as well as answer the general question of whether fluid and solute pathways are linked’.
Sobiecka, D. et al: Peritoneal Fluid Transport in CAPD Patients with Different Transport Rates of Small Solutes. Peritoneal Dialysis International; Vol 24, pp 240 – 251.
NEED FOR MORE RESEARCH INTO THE ROLE OF BETTER GLYCEMIC CONTROL ON THE LONGEVITY OF THE PERITONEAL MEMBRANE.
Glucose and Ultrafiltration- migration across the peritoneal membrane

Canadian Clinical Practice Guidelines 2013
Little evidence-based guidelines for glycemic management in ESRD. In Peritoneal dialysis lack of well-designed, long-term outcome studies on value of post-prandial control .
What we do not know???

Research Questions?
What blood glucose range is associated with:: safety : optimal ultrafiltration? : minimal use of hypertonic PD solutions? : minimized damage to the peritoneal membrane ?

Proposed Method:• Use Continuous Glucose Monitoring. • Lab/meter/CGM/glucose meter comparisons.
• Track use of various PD solutions• Compare glycemic control and ultrafiltration.
• Over time, see if PD associated lifespan of peritoneal membrane is extended in those with (to be determined ) optimal blood glucose control.
• Involve nephrology, PD nurses, diabetes nurses, dietitians, pharmacists

Diabetes Drugs

0 25 50 75 100
Metformin
Glyburide
Gliclazide/Glimepiride
Repaglinide
TZD
Sitagliptin
Acarbose
30
15
30 50
30
Insulin
Linagliptin
Exenatide
50
30
50
Severe (15-29)
Moderate (30-59) Mild (60-89)Terminal (<15)
Liraglutide
60
25
50
Yale JF. December 2011
SafeCaution / Reduced doseNot recommended
Saxagliptin
15 50
Antihyperglycemic Agents and Renal Failure
Glomerular Filtration Rate (ml/min)
Official indication Slide
30

Drugs that are used frequently are Repaglinide (gluconorm) and Insulins.


When do we need insulin with PD? Need to consider :
Timing of diabetes drugs, start and finish
Abrupt start and stop to glucose diffusion.Diabetes drugs working when diffusion starts. Prevent excessive ongoing action of diabetes drugs after PD glucose diffusion stops.Consider impaired gluconeogenesis.
Hypoglycemia:
Adjust dose of diabetes drugs that are working when hypoglycemia occurs.
In PD, often we reduce the dose of long acting insulin.
Add carbohydrates

Hyperglycemia:
Basal or long acting insulin dose titrated to prevent hypoglycemia in periods of little glucose intake.
Add adding short or rapid acting diabetes oral drugs or insulins for hyperglycemic periods.
Minimize carbohydrate intake where possible.
Strategies: Add bedtime carbohydrate/protein food.
Aim for blood glucoses of 10 – 12 at bedtime or;Aim for blood glucose levels that lead to safe morning blood glucoses.
Adjust diabetes drugs doses that are effective when hypoglycemia and gluconeogenesis are relevant factors.
Strategies Based on Lifestyle Analysis and Safety
Move basal insulin to breakfast (CAPD)Move basal insulin to supper (CCPD)BID basal insulin ?Add R “X” U at cycler start? Add low dose H/NR for heater bag? Leave candy/juice at bedside (for sleeping in)Rapid or short acting diabetes drugs with
meals or pc meals (GI concerns)
INSULIN THERAPYSubcutaneous vs Intraperitoneal
Principles are the same as for non-dialysis patients.
Initial starting dose –reduce by as much as 50%
Depends on uremia , nutritional status, comorbidities
Titrate per SMBG
• requires much larger doses
• Adjustments more complex d/t schedules, timing of meals, etc.
• Risks - bacterial contamination, binding of insulin to plastic tubing, peritoneal fibroblast proliferation, adverse lipid profile

People with diabetes and kidney disease already have increased risks for microvascular and cardiovascular disease.

Microvascular and cardiovascular disease is complex.
Glycemia is a major factor.
Individuals can address glycemia.
There are other major factors.

PATHOGENESIS OF DIABETIC COMPLICATIONS
Hyperglycemia
Glycation Susceptibility
Dicarbonyl stress AGE’s GenesMitochondrial Superoxides
Oxidative stress metals ( free radicals)
Polysorbitol pathway
Hexosamine pathway Protective
Protein Kinase C Genes
Nitric Oxide Synthase
Growth Factors- VEGF, IGF, TGF
Retinopathy, Nephropathy, Neuropathy, CVD

Optimal management of vascular disease and optimal glycemic control?
Need to consider:1. Life support : dialysis
2. Prevention of acute diabetes problems: hypo and hyper glycemia
3. Minimization of diabetes microvascular complications
4. Preparation for transplant.

IMPENDIA AND EDEN combined trials
( Li, et. Al, JASN 2013)
Suggested that
glucose-sparing PD dialysis solutions
improve some metabolic parameters
of diabetes linked to CV disease.
But- may adversely affect volume control.

HUMAN BEHAVIOURAL VARIABLES
PERHAPS MORE IMPORTANT THAN ANYTHING!!
CONSIDER:
What is person able / willing to do?
What are their own goals for therapy?
Effect on QOL
Cost
Capacity
Cultural beliefs

TEAMWORK- the power of a multidisciplinary approach
Patient and family
Nephrologist
Nurse Clinician
Diabetes Educator
Pharmacist
Registered Dietitian
Social Work

Canadian Clinical Practice Guidelines 2013
Individualize !

“Many factors contribute to glycemic control:
net effect is that insulin requirements are not easily predicted and careful
individualized therapy is essential”
Berns, J et al: Management of Hyperglycemia with End Stage Renal Disease. Up to date. http//www.uptodate.com/home/store/do. Last updated May 25, 2010.
THE FINAL WORD…………
Canadian Clinical Practice Guidelines 2013
Individualize !



Appendix

Hormonal Recovery from Hypoglycemia
Long Duration of Type 1 and 2 DM :
• Loss of or impaired glucagon response in 1 -2 years• Diminished epinephrine response in 10 years• Require very low blood glucose to stimulate
epinephrine• Diminished epinephrine response with age and beta blockers
All individuals with Stage 4- 5 CKD: • altered insulin and counter regulatory hormones.

FACTORS CONTRIBUTING TO PERITONEAL TISSUE REMODELING IN
PERITONEAL DIALYSIS
Schilte, et al., 2009

Contributing factors to Hypoglycemia:
Diabetes drugsExerciseAlcoholImpaired digestionMeal time carbohydrate intakeImpaired gluconeogenesis
Abrupt cessation of glucose intake via PDCycler malfunction
Counter regulatory changes
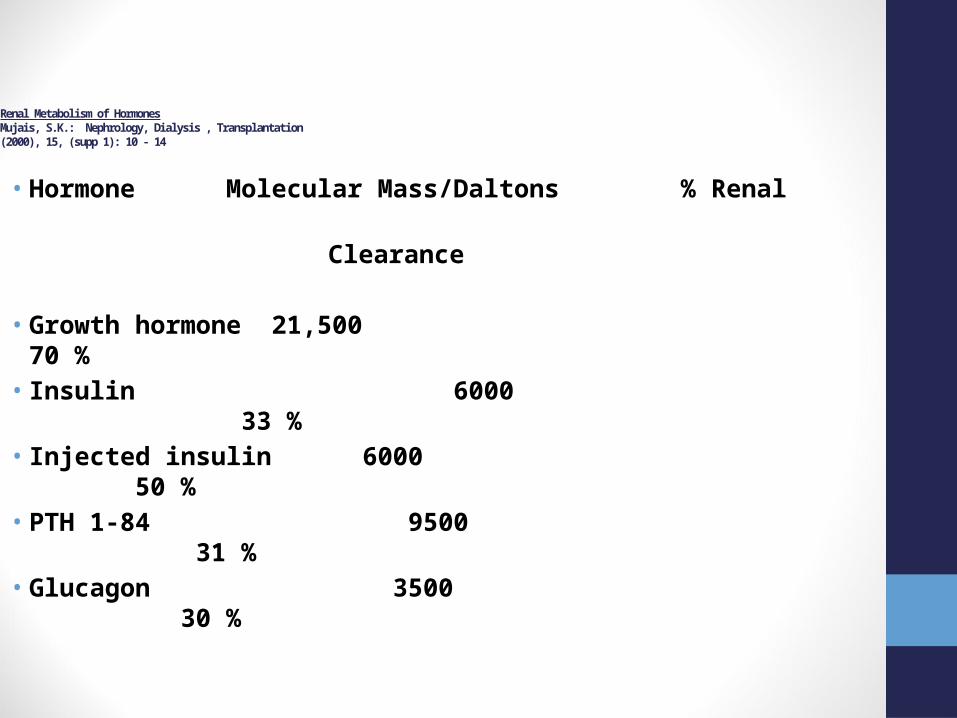
Renal Metabolism of HormonesMujais, S.K.: Nephrology, Dialysis , Transplantation (2000), 15, (supp 1): 10 - 14
• Hormone Molecular Mass/Daltons % Renal
Clearance
• Growth hormone 21,500 70 %• Insulin 6000 33 %• Injected insulin 6000 50 % • PTH 1-84 9500 31 %• Glucagon 3500 30 %

Prednisone
• Prednisone patterns are superimposed on pre-existing glucose patterns.
• Two Phases:• Period of hyperglycemia is dose
dependant.• Lengthened with higher doses and
decreased with lower doses.• Hypoglycemia most likely at 18 – 26
hours post administration.

Steroid Induced Diabetes Iwamoto, T. et al: Steroid Induced Diabetes Mellitus and Related Risk Factors, 2004
Sampling Point Normal blood glucose
Impaired blood glucose
Diabetes level blood glucose
Before breakfast
24 1 0
2 hours pc breakfast
17 4 4
2 hours pc lunch
2 10 13
2 hours pc dinner
7 7 10
Final diagnosis of SDM
2 10 13
Acknowledgements and Thank you’s

HEMOGLOBIN A1C
Review
• Target Associated with best outcomes in CKD predialysis patients not established.
• Likewise for dialysis patients
• Problems with the use of HgbA1c in advanced CKD
• Alternative measure?
Glycated Albumin