management of pain
TRANSCRIPT

7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 1/40
Management of Pain
Dr U I Hapuarachchi
Department of Surgery01/07/2009

7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 2/40
Learning objectives At the end of this lecture, you should be
able to demonstrate the;
Classification of pain
Advantages of relief of pain
WFSA & WHO Pain ladder Treatment options available
Side effects of the options mentioned
Management of common side effects

7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 3/40
Content Definition of Pain
Types of pain Advantages of relief of pain
Assessment of Pain
Pharmacological interventions Regional techniques
Therapeutic adjuncts

7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 4/40
Definition
An unpleasant sensory & emotional
experience resulting from a stimuluscausing, or likely to cause, tissuedamage (nociception), or expressed interms of that damage

7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 5/40
Advantages of pain relief Humanitarian reasons
Reduced cardiovascular complications Reduced respiratory complications
Reduced gastro-intestinal effects
Less salt/water retention Less impairment of sleep/mental function
Early hospital discharge
Economical

7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 6/40
Classification Pathophysiology
Nociceptive or Neuropathic
Onset
Acute or Chronic
Etiology Postoperative or Cancer
Affected area
Headache or Low back pain

7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 7/40
ClassificationNociceptive pain-
Originates in the presence of normal painpathways
Noxious stimuli stimulate peripheral receptors& messages relayed via the dorsal horn to
higher brain centres to warn of impending orongoing tissue damage
7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 8/40
ClassificationNeuropathic pain-
Occurs when there abnormal activation of pain pathways as result of damage ordysfunction within the nervous system itself
Sometimes pain persists despite healing of
the damaged tissues
Pain persisting >3 months – Chronic Pain

7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 9/40
Classification Acute pain-
Caused by noxious stimulation due to injury, adisease process or the abnormal function of muscle or viscera
Usually nociceptive
Typically associated with a neuroendocrinestress

7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 10/40
ClassificationChronic pain-
Pain that persists beyond the usual course of
an acute disease or after a reasonable time forhealing to occur ( 01 to 06 months )
Nociceptive, neuropathic or mixed
Psychological mechanisms or environmentalfactors play major role
Often have attenuated or absentneuroendocrine stress response
Have prominent sleep & mood disturbances

7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 11/40
Assessment of Pain Visual Analogue Scale
0_______________________________10No pain 10 cm line Worst pain
experienced
Numerical Scale
0__ 1__ 2__3__ 4__5__ 6__7__8__9__10No pain 10 cm line Worst pain
experienced

7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 12/40
Assessment of Pain Descriptive Scale
No pain - mild - moderate - severe - excruciating
McGill Pain Questionnaire
Check list of words describing symptoms
Psychological questionnaires for analysis of personality & pain

7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 13/40
Assessment of Pain
Wong-Baker FACES Pain Rating Scale
Is used in children

7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 14/40
Management of Post operative
Pain
Multimodal Approach
According to the WFSA ladder
Systemic analgesics
Regional techniques

7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 15/40
WFSA Pain Ladder
7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 16/40
Systemic analgesics
Opioids – Morphine, pethidine, fentanyl,
remifentanyl,
NSAIDs – Diclofenac sodium, ibuprofen,
ketorolac
Others – Paracetamol, Tramadol

7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 17/40
Opioids
Strong analgesic for moderate to severepain
Can be given as im, iv, sc, oral, Patientcontrolled analgesia (PCA), transdermal,spinal/epidural
PCA – bolus dose, lockout interval
+/- background infusion

7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 18/40
PCA Pump
7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 19/40
Opioids
Dose
Morphine –
0.1 mg/kg Pethidine – 1 mg/kg
Fentanyl – 1-3 µg/kg
Remifentanyl – 0.025-0.1 µg/kg/min
7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 20/40
Opioids
Respiratory depression
Hypotension
Tachy / bradycardia
Sedation
Euphoria / dysphoria
Nausea / vomiting Uriticaria
Urine retention
7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 21/40
Opioids
Respiratory depression
If RR < 10 /min – Awaken the patient
If RR < 8 /min – O2 via face mask
Naloxone 40 µg iv boluses
Urticaria
Chlopheniramine 5-10 mg
Naloxone 40 µg iv

7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 22/40
Opioids
Nausea & vomiting
Promethazine -12.5-25 mg im / iv
Metoclopramide – 5-10 mg slow iv / im
Ondansetrone – 4-8 mg iv
Urine retention
General measures
catheterization

7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 23/40
NSAIDs
Can be given as oral, suppositories, iv
Potent analgesic for mild to moderate
pain
Can cause renal toxicity
Precipitate bronchial asthma Peptic ulceration
Fluid retention
7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 24/40
NSAIDs
Dose
Diclofenac sodium – 1 mg/kg tds (maximum -3 mg/kg/day) - > 1 yr
Ibuprofen – 5-10 mg/kg tds

7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 25/40
Other drugs
Paracetamol
Analgesic for mild to moderate pain
Liver damage in overdose
Can be given as oral, suppositories, iv
Dose – 20 mg/kg & then 15 mg/kg 4 hrly
Maximum dose – 90 mg/kg
7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 26/40
Other drugs
Tramadol
Has opioid & non-opioid mechanism of action
Has less respiratory depression, constipation,euphoria than other opioids
Causes nausea, dizziness, dry mouth
Increased S/E in conjunction with otheropioids
Can be given as oral, slow iv / im
50-100 mg 4 hrly

7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 27/40
Regional techniques
Epidural – Continuous infusion / boluses
PCEA, Caudal
Nerve plexus blocks – Supraclavicular,
axillary, lumber plexus
Individual nerve blocks – median, ulnar,
sciatic, femoral
Intra-pleural analgesia
Infiltration

7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 28/40
Regional techniques

7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 29/40
Regional techniques
Less stress response
Less bleeding
Better organ perfusion
Better gut motility
Less DVT
Motor block
CVS instability – Hypotension
Urine retention with spinal/epidural opioids
7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 30/40
Regional techniques
Epidural / PCEA – 0.125 –0.1% Bupivacaine
+ /- opioidOther blocks – 0.25-0.5% Bupivacaine
PCEA – better pain relief less overdose

7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 31/40
Regional techniques
Hypotension
Rapid iv fluid infusion Vasoconstrictors – ephedrine 5-10 mg iv
Inform the Pain relief team
7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 32/40
Management of NeuropathicPain
Pharmacological interventions
Antidepressants – Block presynaptic reuptake of serotonin,
norephinephrine or both
Anticonvulsants-Block voltage gated sodium channels & can
suppress spontaneous neural discharges

7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 33/40
Management of NeuropathicPain
Pharmacological interventions
NeurolepticsBlock dopaminergic receptors in mesolimbic sites
Corticosteroids
Has anti-inflammatory & analgesic actions
α2 Adrenergic agonists
Activate descending inhibitory pathways in thedorsal horn

7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 34/40
Management of NeuropathicPain
Therapeutic adjuncts
Psychological interventionsCognitive therapy, Behavioral therapy, Biofeedback,
Relaxation techniques & Hypnosis
Physical therapyHeat & cold therapy, Exercise

7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 35/40
Cognitive therapy
7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 36/40
Management of NeuropathicPain
Therapeutic adjuncts
AcupuctureIn chronic pain – chronic musculosketal
disorders & headache
Electrical stimulation
TENS, Spinal cord stimulation, Intracerebral
stimulation

7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 37/40
TENS
7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 38/40
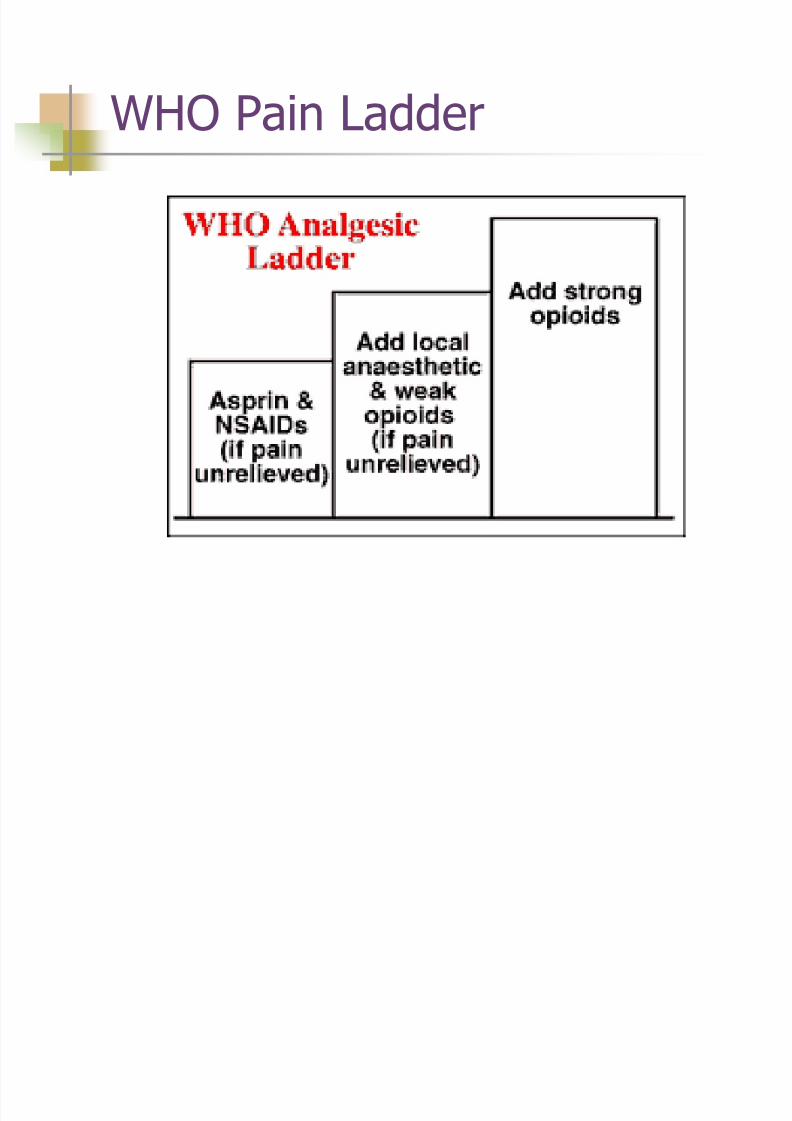
WHO Pain Ladder

7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 39/40
References
Management of Acute pain
National Guidelines-Anaesthesiology, Ministry of Healthcare & nutrition, Sri Lanka. Pg70-91
Atkinson RS, Rushman GB, Davies NJH. Acute painLee’s Synopsis of Anaesthesia 11 th Edition Chapter 26
Kirk RM, Ribbans WJ. Management of Post-operative pain
Clinical Surgery in General-RCS Course Manual 4 th Edition
Pg 357-369 http://www.frca.co.uk
Resources>Clinical Anaesthesia>Acute pain
Morgan GE, Mikhail MS, Murray MJ. Pain Management
Clinical Anaesthesiology 4 th
Edition Pg 359-411

7/27/2019 Management of Pain
http://slidepdf.com/reader/full/management-of-pain 40/40
Thank you