management of obstructed airway
TRANSCRIPT
8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 1/54
MANAGEMENT OF
OBSTRUCTED AIRWAY

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 2/54
IMPORTANT STRUCTURE
OF THE AIRWAY

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 3/54
ANATOMY OF THE AIRWAY
UPPERAIRWAY
LOWER
AIRWAY

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 4/54
SENSORY INNERVATIONS
OF THE AIRWAY
Upper airway:
1. Trigeminal nerve(V)
2. Facial nerve (VII)
3. Glossopharyngeal
nerve (IX).
8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 5/54
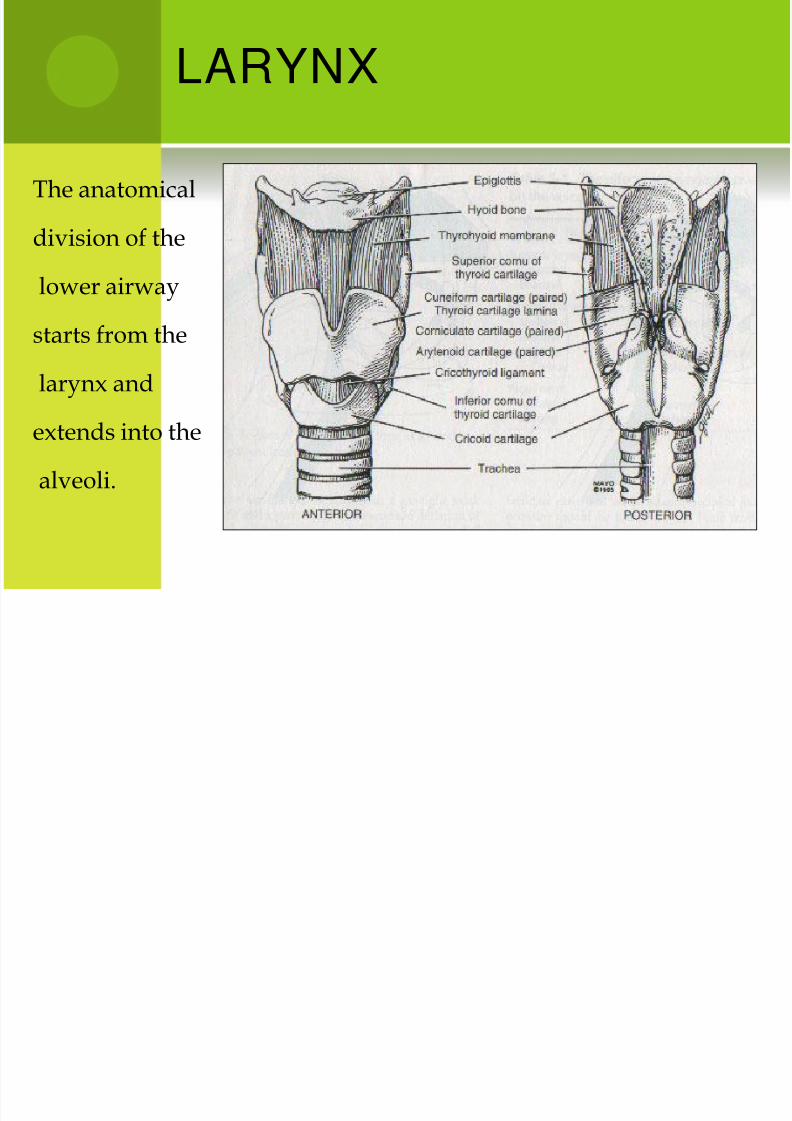
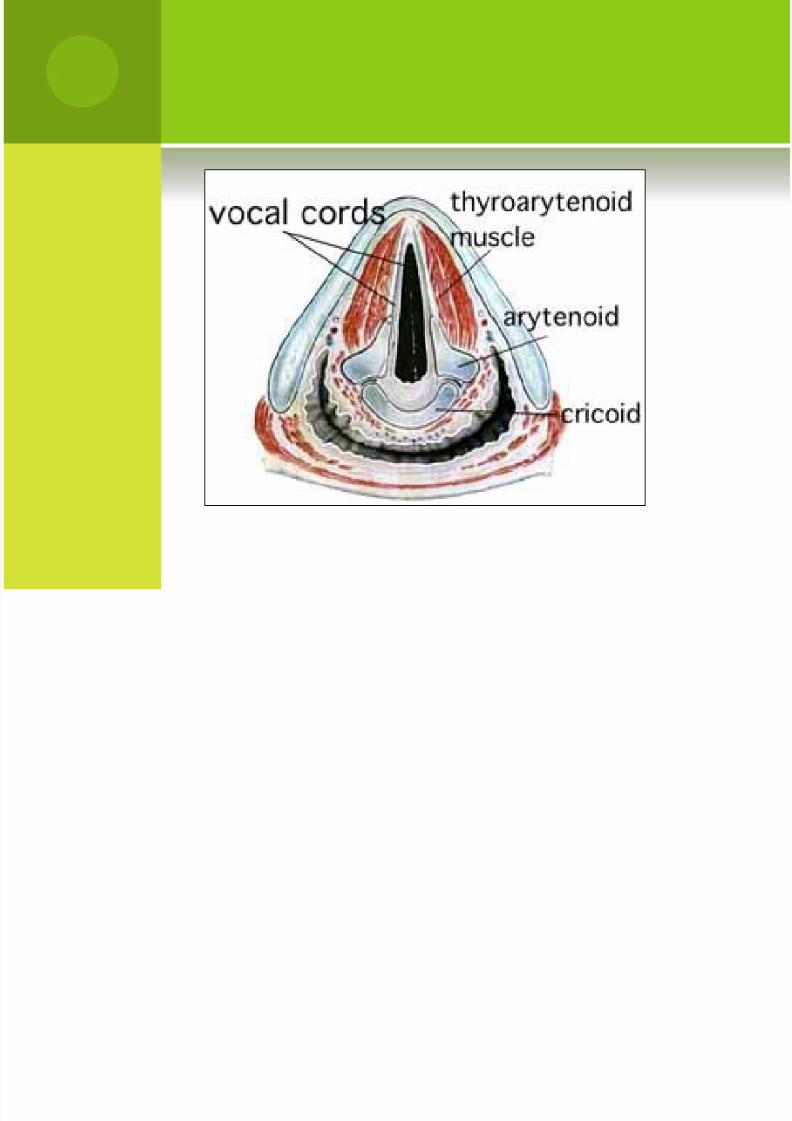
LARYNX
The anatomical
division of the
lower airway
starts from the
larynx and
extends into the
alveoli.

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 6/54
SENSORY INNERVATIONS
OF THE LARYNX
Superior Laryngeal Nerve (Vagus nerve)
Internal -glottis and supraglottis,
which includes the pharynx,underside of the epiglottis and thelarynx above the cords. Remember:SIS-superior internal sensory.
External -It supplies motor functionto the crycothyroid muscle whichtenses the vocal cords and couldcause laryngopasm.
Recurrent Laryngeal Nerve –
It provides sensation to thesubglottic (ie. vocal cords,esophagus)

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 7/54
LOCATION OF LARYNGEAL
NERVES

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 8/54

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 9/54
TRI-SPHINCTER MECHANISM
Aryepiglottic fold: : closesduring swallowing, divertingliquid and food away guardingagainst the entrance of ingestedforeign bodies and vomitus
during retching and gagging
False Vocal Cord (ventricularfold): function as exit valvesto prevent the egress of airfrom the trachea
(expectorative function). True Vocal Cords: Primary
role is protection of theairway (most significant ofthe tiers against aspiration).

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 10/54
GLOTTIC CLOSURE REFLEX
Produced by rapid contraction of thethyroarytenoid muscle in response to superiorlaryngeal nerve stimulation.
Sensory stimuli other than those classically elicitedby direct SLN stimulation are also capable ofeliciting this reflex.
Examples of these include stimulation of all majorcranial afferent nerves and other special sensoryand spinal somatic nerves.
8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 11/54

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 12/54
LARYNGOSPASM
Physiologic exaggeration of the glottic closure reflex- but itis more forceful and prolonged closure of the larynx.Maintained well beyond the cessation of mucosal irritation.
The most common causes are inhaled irritants,manipulation of the upper aerodigestive tract, foreignbodies, mucus, or blood in the glottic chink.
Most likely to occur when the patient is in the ORundergoing endotracheal intubation
Produced obstructive apnea and death by asphyxia
Laryngospasm is inhibited by: increased arterial pCO2,decreased arterial pO2, positive intrathoracic pressure, andthe inspiratory phase of respiration.

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 13/54
COUGH REFLEX
May be voluntary, but more often in response tostimulation of receptors in the larynx or lowerrespiratory tract.
It consists of three phases:
inspiratory- larynx opens wide to permit rapidand deep inspiration;
compressive- tight closure of the glottis andstrong activation of expiratory muscles;
expulsive- larynx opens widely and a suddenoutflow of air in the range of 6-10 liters/sec.

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 14/54
CIRCULATORY REFLEXES
Stimulation of the larynx can produce changes in heart rateand blood pressure.
Direct result of laryngeal stimulation on blood pressure is
hypertension, but if laryngeal stimulation producessignificant bradycardia by vagal stimulation, hypotension canindirectly occur.
This effect is most evident during induction of anesthesia and
can occur in natural circumstances such as obstructive sleepapnea.
Afferent (Superior Laryngeal Nerve) is responsible for thisreflex, transection of this nerve abolishes cardiovascular
responses to laryngeal stimulation and elective SLNstimulation affects BP and HR.
8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 15/54
OBSTRUCTION IN AIRWAY

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 16/54
MANEUVER FOR UNBLOCKING
URT
Heimleich maneuver
Suction
Finger sweep technique
8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 17/54
HEIMLEICH MANEUVER -
ADULT From behind, wrap arms around the victim's waist.
Make a fist and place the thumb side of fist against the victim's upperabdomen, below the ribcage and above the navel.
Grasp fist with your other hand and press into their upper abdomen with aquick upward thrust. Do not squeeze the ribcage; confine the force of the thrustto hands.
Repeat until object is expelled.
If unable to reach around victim, place the victim on back.
Facing the victim, kneel astride the victim's hips.
With one hand on top of the other, place the heel of bottom hand on the upperabdomen below the rib cage and above the navel. Use body weight to pressinto the victim's upper abdomen with a quick upward thrust.
Repeat until object is expelled.
If the Victim has not recovered, proceed with CPR.
Don't slap the victim's back.

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 18/54

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 19/54
HEIMLEICH MANEUVER -
CHILD
Lay the child down, face up, on a firm surface andkneel or stand at the victim's feet, or hold infant onlap facing away.
Place the middle and index fingers of both handsbelow rib cage and above navel.
Press into the victim's upper abdomen with a quickupward thrust; do not squeeze the rib cage.
Repeat until object is expelled.
If victim not recovered, proceed with CPR.
Don't slap the victim's back.

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 20/54

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 21/54
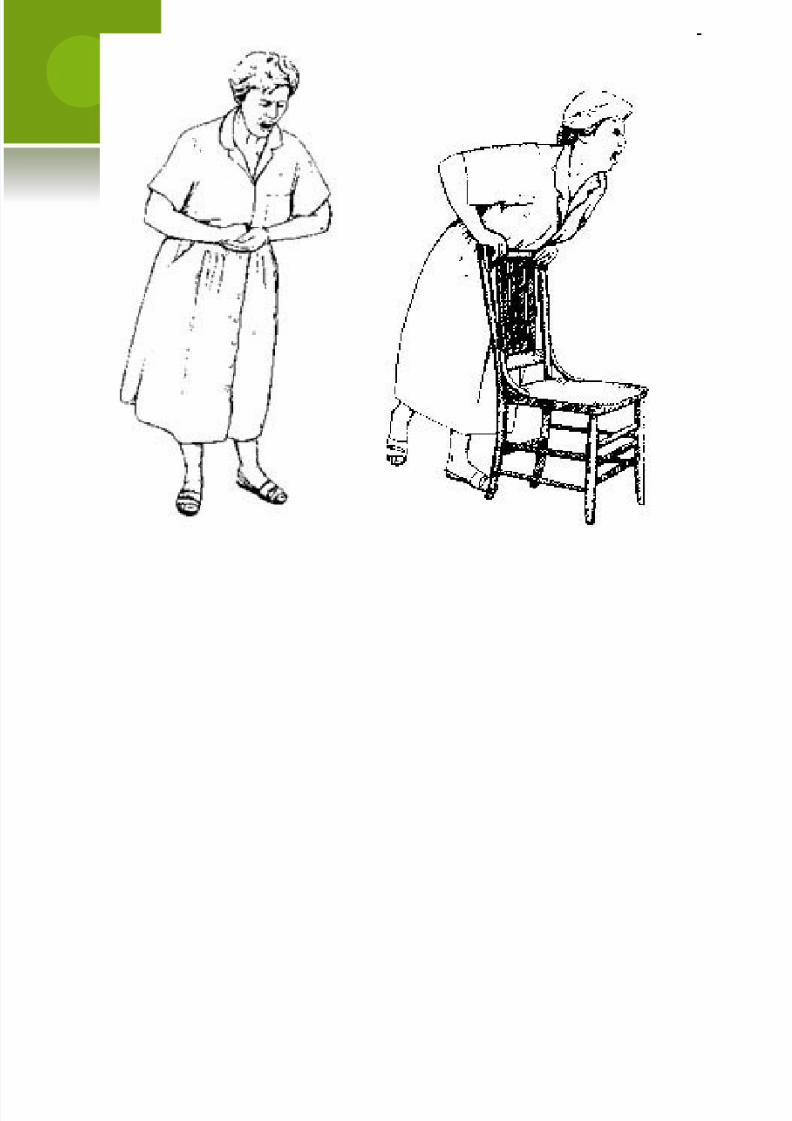
HEIMLEICH MANEUVER -
SELF
Make a fist and place the thumb side offist against your abdomen, below theribcage and above the navel.
Grasp fist with other hand and pressinto upper abdomen with a quickupward thrust.
Repeat until object is expelled.
Alternatively, lean over a fixedhorizontal object (table edge, chair,railing) and press upper abdomenagainst the edge to produce a quickupward thrust. Repeat until object isexpelled.
8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 22/54

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 23/54
8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 24/54
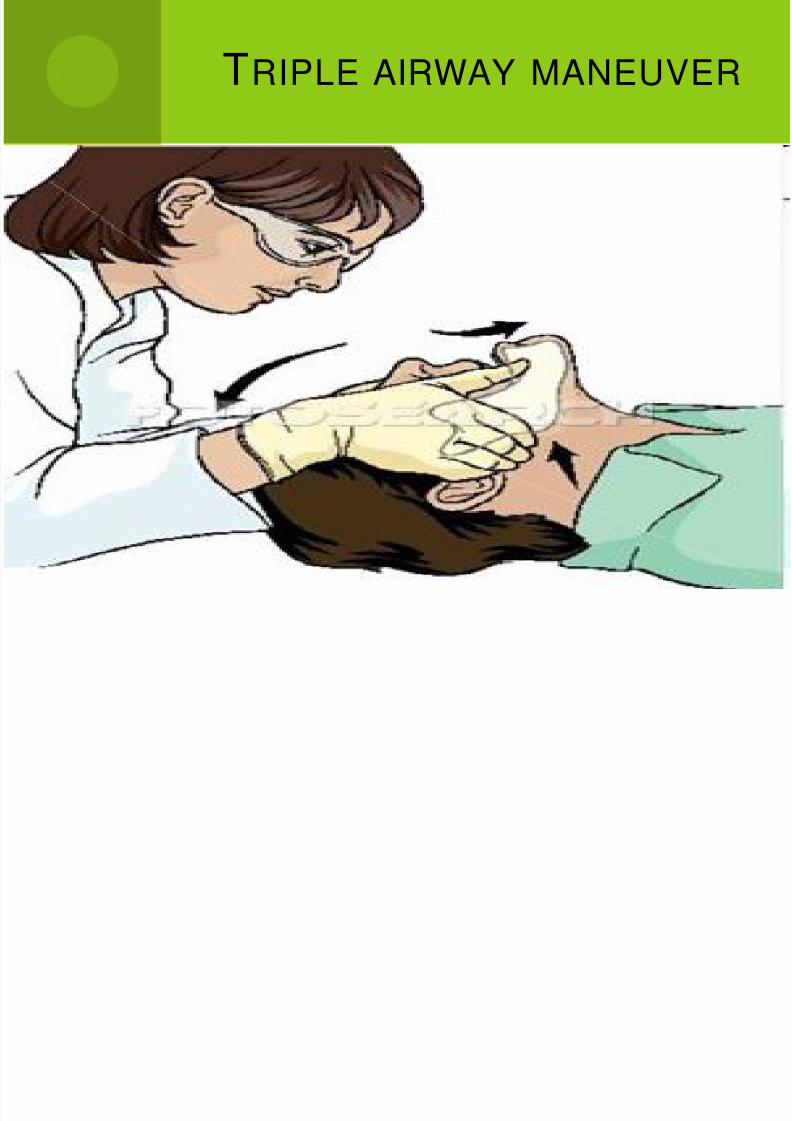
TRIPLE AIRWAY MANEUVER
8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 25/54
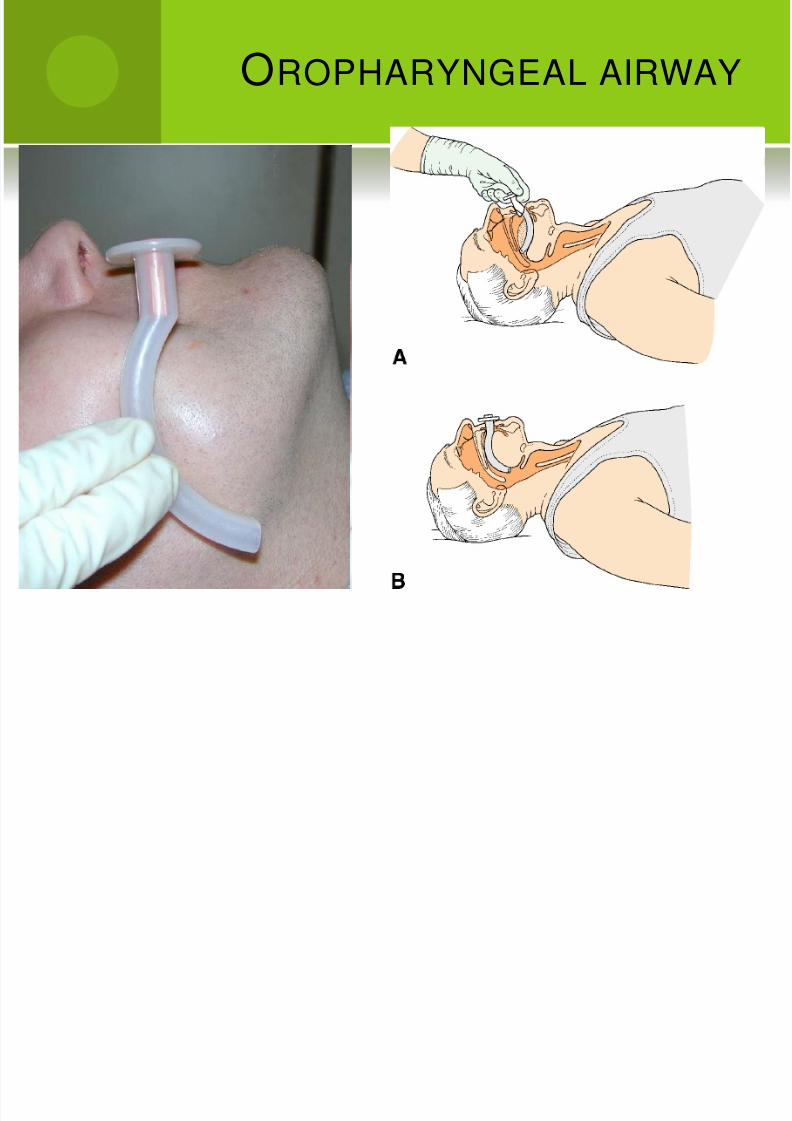
OROPHARYNGEAL AIRWAY

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 26/54
OPA
Measure for correct size by measuring from the center ofthe mouth to the angle of the jaw, or from the corner of themouth to the earlobe.
Mouth is opened using the “crossed” finger technique.
OPA is inserted in the patient’s mouth upside down so thetip of the OPA is facing the roof of the patient’s mouth.
As the airway is inserted it is rotated 180 degrees until theflange comes to rest on the patient’s lips and/or teeth.
The OPA may be inserted with the pharyngeal curvatureif a tongue blade is used to depress the tongue.
If patient begins to retch/gag, remove the OPA.

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 27/54
NASOPHARYNGEAL
AIRWAY
8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 28/54
NPA
Select the proper size airway by measuring from the tipof the patient’s earlobe to the tip of the patient’s nose.The diameter of the airway should be the largest thatwill fit by selecting the size that approximates thediameter of the patient’s little finger.
Lubricate the airway with a water-soluble lubricant.
With the patient’s head in a neutral position, gently pullback the tip of the patient’s nose.
Insert the airway; bevel toward the nasal septum, intothe right nostril following the natural curvature of thenasal passage.
The flange should rest against the nasal opening.
8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 29/54
BAG VALVE MASK

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 30/54
BMV While positioned at the top of the patient’s head, open the airway using the head -tilt/chin-lift maneuver or the jaw-thrust maneuver.
Insert the appropriate sized airway adjunct.
Choose the appropriate size mask for the patient.
Mask should be transparent with an air cushion that rests against the patient’s face.
Hold mask position and place mask over patient’s face assuring the top of the mask is over the bridge of the nose and the bottom is in thegroove between the lower lip and the chin.
Using the “OK” hand position, with both hands, manually open the airway and maintain the mask seal. Connect the bag-valve unit to themask.
Ventilate the patient by squeezing the entire bag over 1-2 seconds and then release the bag. Each ventilation must be a minimum of 800cc.Assure appropriate chest rise during ventilations.
Continue to ventilate the patient for 30 seconds prior to attaching the oxygen. Next, assemble the oxygen tank and regulator.
Attach oxygen tubing to the regulator and to the BVM’s reservoir.
Turn on the oxygen and adjust the regulator to 15 liters per minute.
Allow the reservoir to fill with oxygen prior to the first ventilation.
Reposition patient and begin artificial ventilations.
As completed earlier, open the airway, place mask over the patient’s face, continue with proper mask/face seal, and begin venitlations.
If two rescuers present, one will maintain a mask seal using both hands while maintaining an open airway while the other will ventilatethe patient by collapsing the bag on the BVM fully with both hands.

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 31/54
LARYNGEAL MASK AIRWAY
• Completely deflate the cuff
8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 32/54
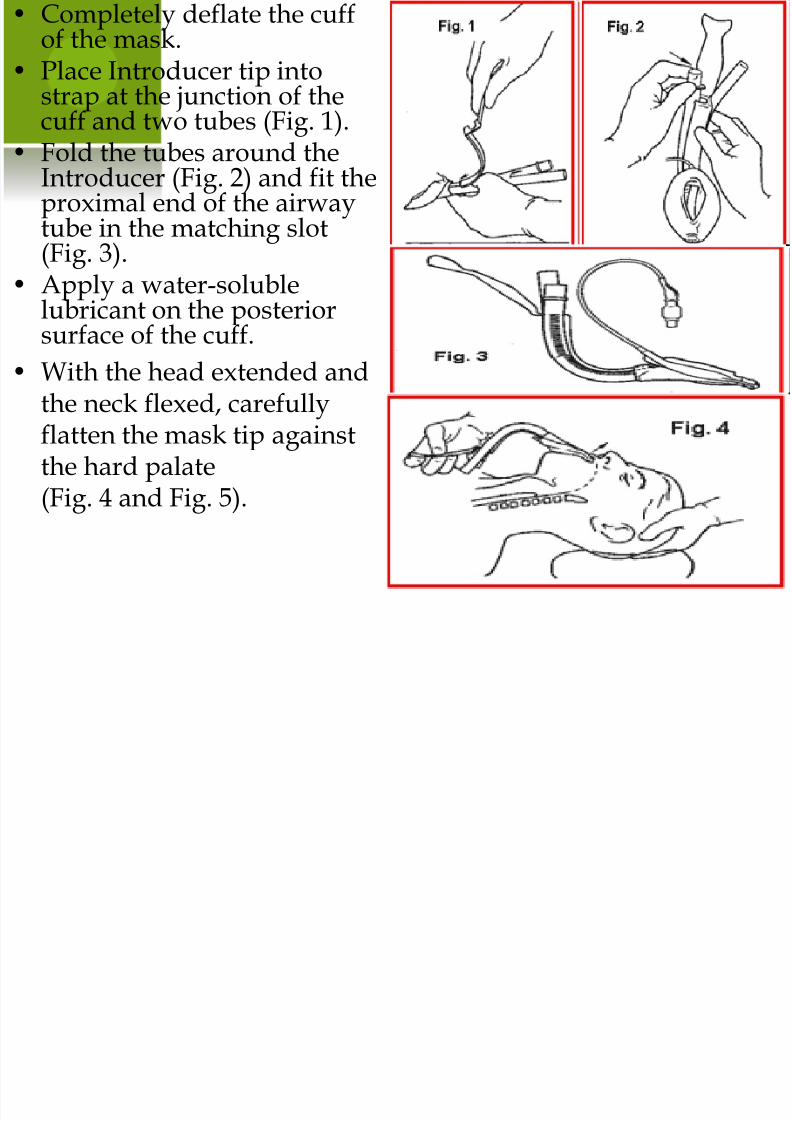
Completely deflate the cuffof the mask.
• Place Introducer tip intostrap at the junction of thecuff and two tubes (Fig. 1).
• Fold the tubes around theIntroducer (Fig. 2) and fit theproximal end of the airwaytube in the matching slot(Fig. 3).
• Apply a water-solublelubricant on the posteriorsurface of the cuff.
• With the head extended and
the neck flexed, carefullyflatten the mask tip againstthe hard palate(Fig. 4 and Fig. 5).
Keep the Introducer blade close

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 33/54
Keep the Introducer blade closeto the chin and rotate the LMAProSeal™ inward in one smoothcircular movement following thecurve of the Introducer (Fig. 6).
Advance into the hypopharynxuntil a definite resistance is felt(Fig. 7).
Before removing the Introducer,hold the LMA ProSeal™ tubewith the non-dominant hand tostabilize the tube. At this point,the LMA ProSeal™ should becorrectly placed with its tipfirmly pressed against the upper
esophageal sphincter (Fig. 8).Remove the Introducer. Inflatethe cuff with just enough air toobtain a seal (an intracuffpressure of ~ 60 cm H2O). Neveroverinflate the cuff.

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 34/54
ENDOTRACHEAL
INTUBATION PROCEDURE

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 35/54
ASSESSING THE
PATIENT
Physical examination
I. Vital signs and oxygen saturation
II. Examine the mouth and oral cavity (the best combination for east airwaymanagement is a large oral cavity with a small mobile tongue)
III. Evaluate the extent and symmetry of mouth opening (three finger breadths isoptimal)
IV. Check for loose, missing or cracked teeth
V. Note any prominent buck teeth or particularly large incisors that may interferewith laryngoscopy (dental and oral injuries are common complications oflaryngoscopy)
VI. Note the size of the tongue (large tongues may interfere with use of thelaryngoscope)
VII. Note the arch of the palate (high arched palates have been known to hampervisualization of the larynx)
8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 36/54
Examine the pharynx. The appearance of theposterior PHARYNX may predict ease of laryngoscopy andvisualization of the LARYNX. Malampatti has classifiedpatients in classes I-IV based on visualization of structuresduring pre-operative evaluation.
If the whole of the tonsillar pillars are visualized, the airway israted Class I and intubation is likely to be uncomplicated.
If the uvula, but not the tonsillar pillars can be visualized, theairway is rated as Class II.
Class III is characterized by visualization of part of the uvula andsoft palate.
8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 37/54
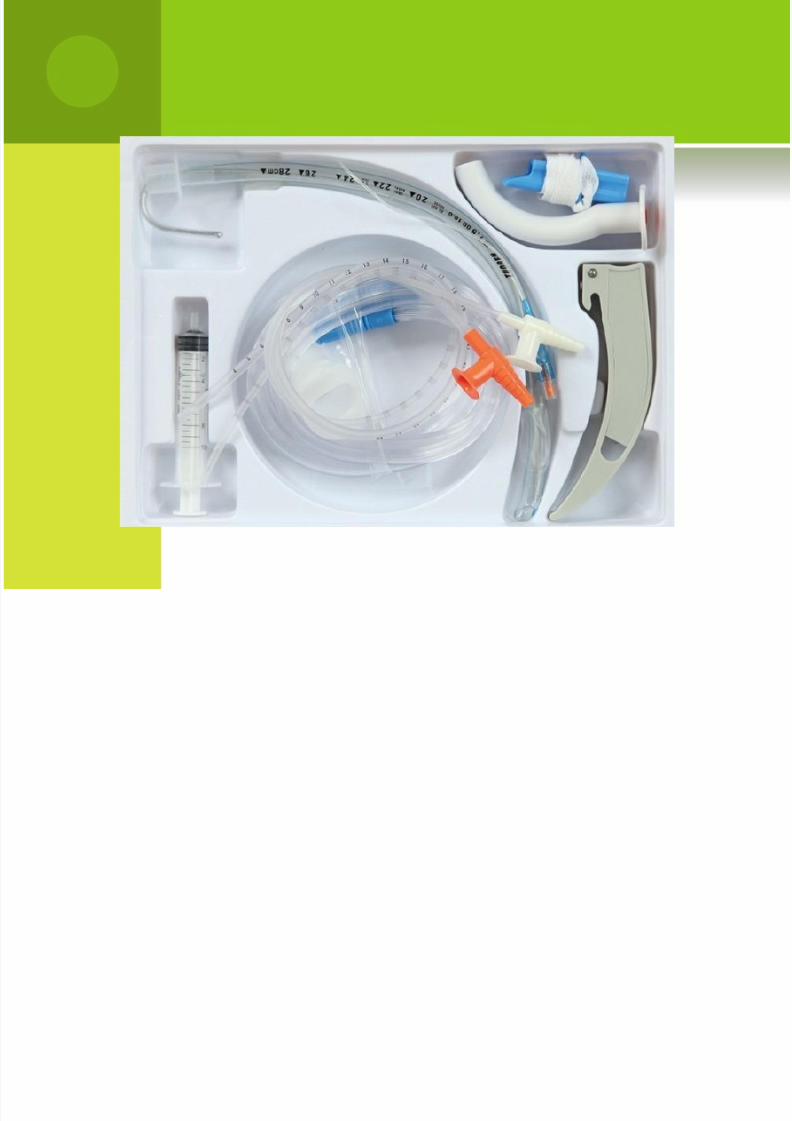
REQUIRED EQUIPMENTS
Endotracheal tube
I. 7.5 mm is the “Universally Accepted” size for an unknown victim
II. Men are usually larger, therefore an 8.0 mm tube may be appropriate
III. Females are usually smaller, therefore a 7.0 mm tube may be appropriate
10 cc Syringe – used to fill the cuff at the end of the endotracheal tube
Stylet – a wire inserted into the endotracheal tube in order to stiffen itduring passage
Water soluble lubrication – KY Jelly or Surgilube
Stethoscope – to check for proper placement of the endotracheal tube

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 38/54
Magill forceps – May be used to help guide an endotracheal tubefrom the pharynx into the larynx
Laryngoscope handle
Laryngoscope blade
Oropharyngeal airway (bite block) – to prevent the patient frombiting down on the endotracheal tube
Tape – to secure the endotracheal tube in place
Gloves
Ambu-bag – to facilitate positive pressure ventilations
Suction Device – to clear the airway of debris (blood, mucous,saliva)
8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 39/54

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 40/54

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 41/54
Open the mouth by separating the lips and pulling on theupper jaw with the index finger.
Hold the laryngoscope in the left hand. Insert thelaryngoscope into the mouth with the blade directed to theright tonsil. Once the right tonsil is reached, sweep theblade to the midline keeping the tongue on the left.
8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 42/54
This brings the epiglottis into view. DO NOT LOSE SIGHTOF IT.
Advance the laryngoscope blade till it reaches the anglebetween the base of the tongue and the epiglottis.
Lift the laryngoscope upwards and away from the nose -towards the chest. This manoeuvre should bring the vocal
cords into view, but it may be necessary for an assistant topress on the trachea to improve the direct view of the larynx.

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 43/54

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 44/54
Take the endotracheal tube in the right hand. Keep theconcavity of the tube facing the right side of the mouth. Thiscauses least interruption to the view of the vocal cords. Watchthe tube entering the larynx and insert it through the cordsonly till the cuff is just below the cords.
Inflate the cuff to provide a minimal leak when the bag issqueezed.
Listen for air entry at both apices and both axillae to ensurecorrect placement, using a stethoscope and look at the chestfor expansion with each breath.

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 45/54
CRICOTYROTOMY
INDICATIONS

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 46/54
INDICATIONS
Failure of oral or nasalintubation or adequateoxygenation and ventilationwith airway adjuncts (laryngealmask airway, etc.).
Massive oral, nasal, orpharyngeal hemorrhage
Masseter muscle spasm
Clenched teeth
Structural deformities of theoropharynx, whether congenitalor acquired
Stenosis of the upper airway(pharynx or larynx)
Laryngospasm
Mass effect (cancer, tumor,polyp, web, or other mass)
Airway obstruction (partial orcomplete)
Oropharyngeal edema
Foreign body obstruction
Obstruction of the airway due todisplacement of normalstructures

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 47/54

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 48/54
TECHNIQUE
Prepare all necessary equipment and test the tracheostomy tube byinflating the tube with air from 10-cc syringe.
Position the patient . He or she should be supine, with a rolled bathtowel under the shoulders, and with the neck in hyperextension.
Sterilize the skin from the sternal notch to chin and laterally to thebase of the neck.
Identify the cricothyroid membrane.
Anesthetize the skin over the membrane using the 10-cc syringe with25-gauge needle with the 1% lidocaine.
Make a transverse incision of the skin over the cricothyroidmembrane.
Identify the membrane and then continue the incision through itapproximately 1 cm on each side of the midline.

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 49/54
TECHNIQUE
With the mosquito or kelly clamp in the left hand, insert the clampinto the incision and spread it . This is sufficient to provide an airwayfor a patient with supraglotic airway obstruction.
With the right hand insert the tracheostomy tube or the orotrachealtube through the incision into the trachea, directing it caudally.
Connect the bag-valve unit to the tube and ventilate the patient thepatient with 100% oxygen.
Observe respiratory movements of the chest and breath sounds.
Inflate the tube balloon
Fixate
Suction
Obtain a chest x-ray to check the position of the tube.
POST PROCEDURE

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 50/54
POST-PROCEDURE
CARE
Obtain a post-procedure chestradiograph.
COMPLICATIONS

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 51/54
COMPLICATIONS
Laryngotracheal injury
Tension pneumothorax
Clogging of the tracheostomy tube with blood or secretions

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 52/54
REFERENCES
Danzl DF, Vissers RJ. Tracheal intubation and mechanicalventilation. In: Tintinalli JE, Kelen GD, Stapczynski JS, MaOJ, Cline DM, eds. Emergency Medicine: A ComprehensiveStudy Guide. 6th ed. New York, NY: McGraw-Hill; 2004:
chap 19.
Barash, PG; Cullen, BF; Stoelting, RK, eds (2009). Clinical Anesthesia (6th ed.). Philadelphia: Lippincott Williams &Wilkins. Retrieved 2010-10-16.
Bhishagratna, KL, ed (1907). Sushruta Samhita, Volume1:Sutrasthanam. Calcutta: Kaviraj Kunja Lal Bhishagratna.Retrieved 2010-10-16.
Benumof, JL, ed (2007). Benumof's Airway Management:Principles and Practice (2nd ed.). Philadelphia: Mosby-Elsevier. Retrieved 2010-10-16

8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 53/54
8/3/2019 Management of Obstructed Airway
http://slidepdf.com/reader/full/management-of-obstructed-airway 54/54
THANKS!!