management of not yet classified aub..cesarean scar defect,uterine arteriov fistula,myometrial...
TRANSCRIPT
Management of Not yet Classified group of Abnormal uterine bleeding
(AUB-N)
Prof . Refaat I El-Sheemy Professor of Obstetrics and GynecologyFaculty of medicine – Al-Azhar University (Damietta)

• To describe the new nomenclatures
• Why Changes …. What Changed.? • Is it could be applied.?• Is Still we need more researches forUnexplained causes ………
• Is there any new treatment apart from hysterectomy??
.

• Mostly .PUBLISHED IN AM J and those under publication.
• In Auther website.
Researches at our department in
DOMYAT .
• Mostly .PUBLISHED IN AM J and those under publication.
• In Auther s website.• www.
Prof_shimy8m.com
Researches at our department in
DOMYAT .

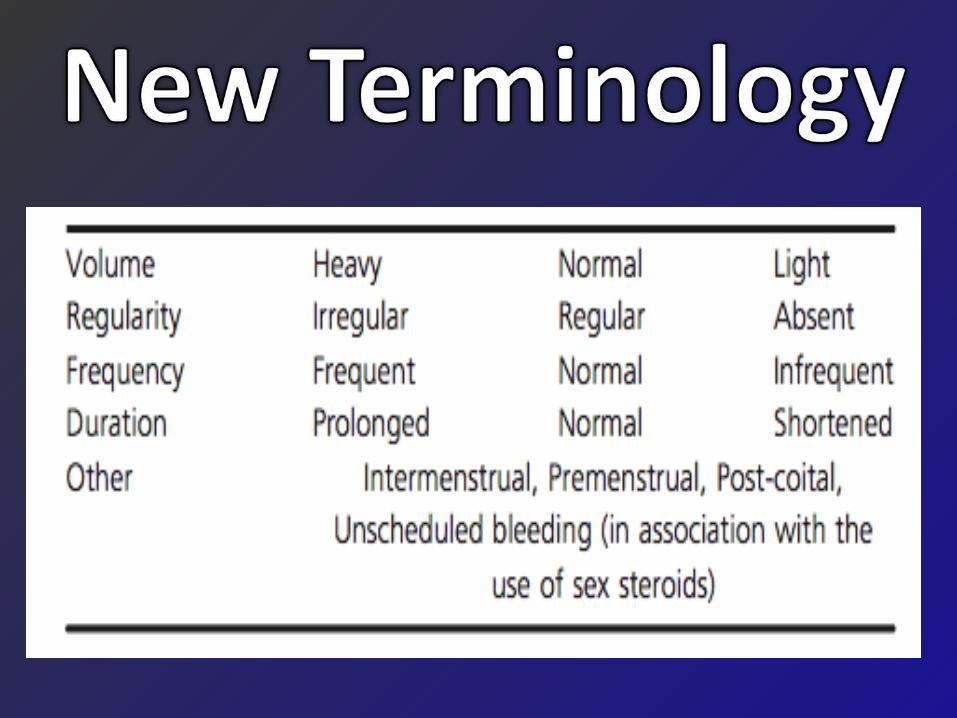
HistoryLong time use of non-standardized, ambiguous terminology.
English language terminologies with Greek or Latin roots are poorly defined and create ambiguity in meaning and usage. .
In 2005, interest group of 35 experts did historical review, and recommendations made for uniform terminology published.
They recommended discarding the confusing terminology, and replace with simple descriptive terms that could be understood by patients and translated into most languages

DISCARDED TERMINOLOGY CONT.
Dysfunctional uterine bleeding Functional uterine bleeding Metropathica hemorrhagica .
Amenorrhea – retained term

Accepted Abbreviations Describing Menstrual Symptoms
AUB…….. Abnormal uterine bleeding
HMB……. Heavy menstrual bleeding
HPMB.. Heavy and prolonged menstrual bleeding
IMB… Intermenstrual bleeding
PMB… Postmenopausal bleeding
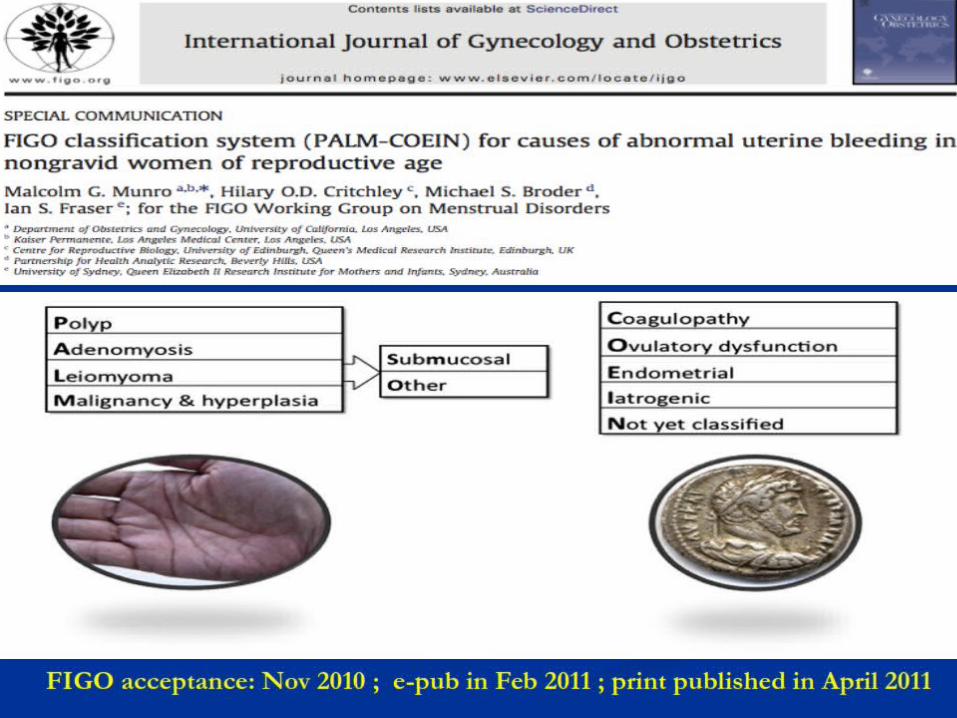
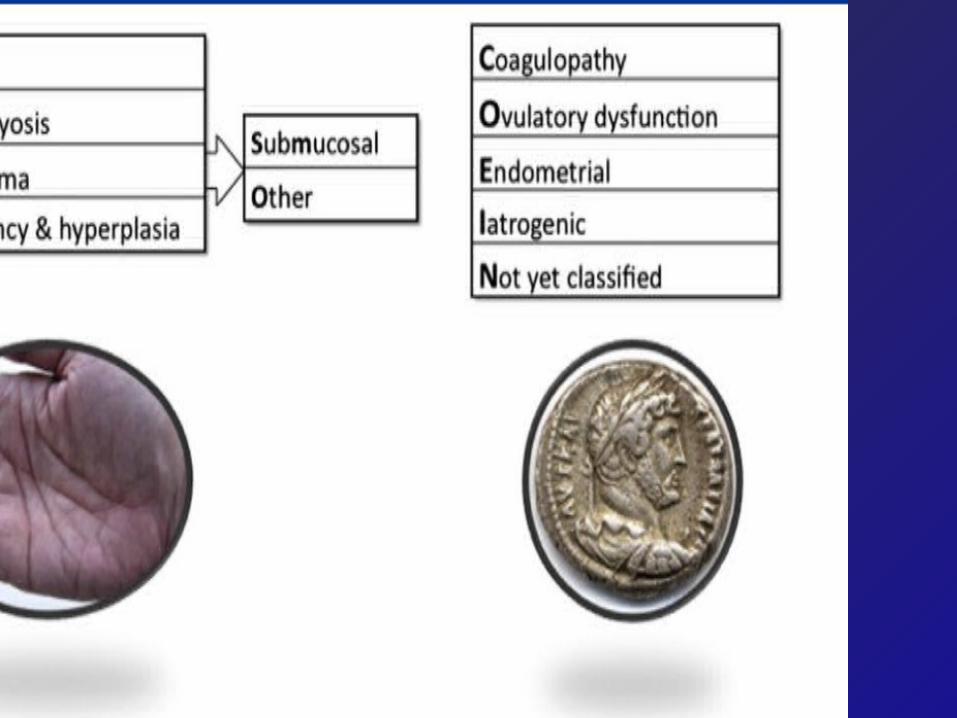

The PALM-COEIN Classification System for Causes of AUB
PALM – visually objective structural criteria COEI – unrelated to structural anomalies
N – entities not yet classified
Coagulopathy (AUB-C) Polyps (AUB-P) ,Ovulatory disorders (AUB-O) Adenomyosis (AUB-A) ,Endometrial (AUB-E) Leiomyoma (AUB-L) ,Iatrogenic (AUB-I) Malignancy (AUB-M) ,Not yet Classified
Components of the PALM-COEIN Classification System
Polyps (AUB-P)
Polyps are categorized as either present or absent. Diagnosed by TVUS, saline infusion sonography or hysteroscopy.
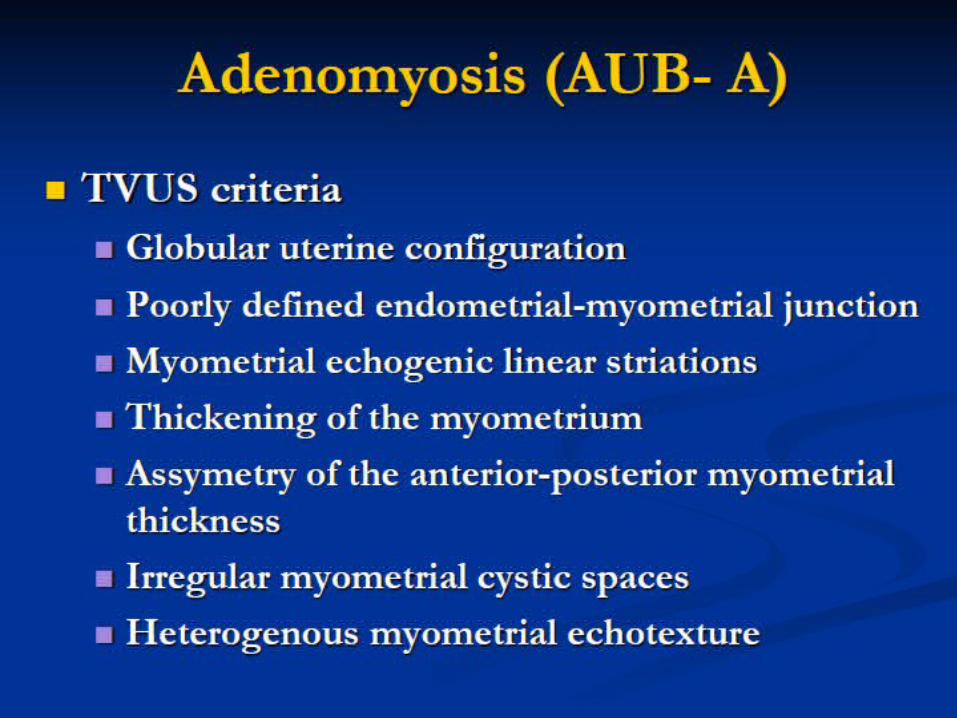
Adenomyosis (AUB-A)
Diagnosed by ultrasound or MRI.

Leiomyomas (AUB-L)
Higher association of AUB with submucosal lesions, compared to intramural and subserosal leiomyomas.
Malignancy (AUB-M)
Includes both premalignant and malignant lesions.



Coagulopathies (AUB-C)
13% of women with HMB have a disorder of hemostasis that may be overlooked during the differential diagnosis.
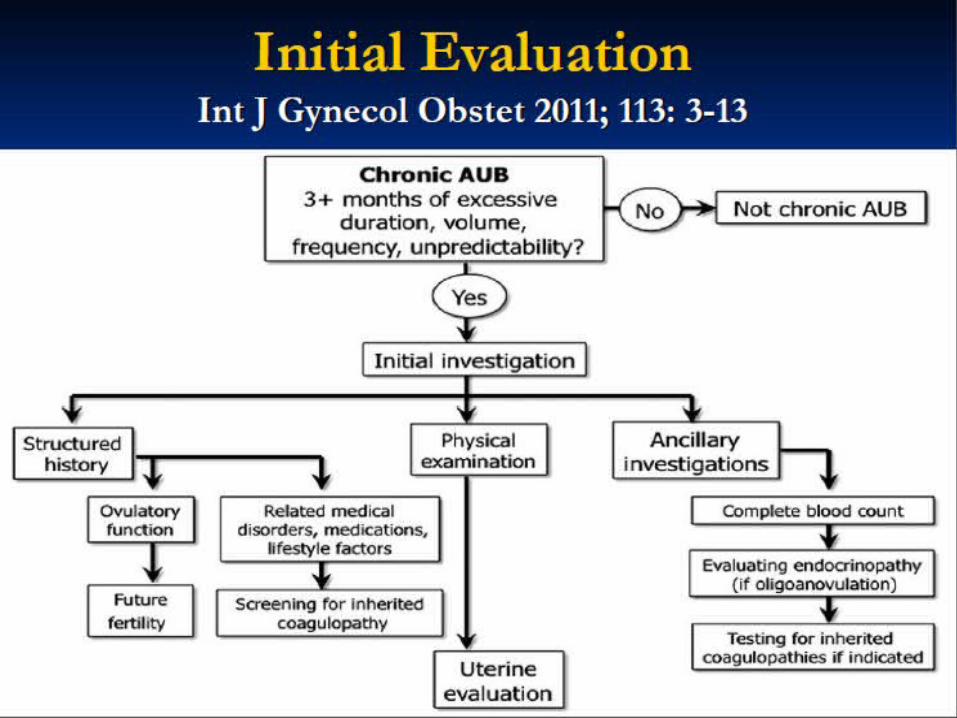
Ovulatory Dysfunction (AUB-O)
Usually associated with endocrinopathies, such as polycyctic ovary syndrome or hypothyroidism. Evaluate for ovulatory dysfunction.
Endometrial Causes (AUB-E)
Most patients in this category will have regular cycles, normal ovulation and no definable cause of AUB.

Iatrogenic (AUB-I)
Causes include IUD, exogenous gonadal steroids and other systemic agents that affect blood coagulation or ovulation.
Bleeding from anticoagulation therapy is listed under AUB-C rather than AUB-I.
Not Yet Classified (AUB-N)
Reserved for entities that are poorly defined and/or not well examined, such as :
Arteriovenous malformation
Myometrial hypertrophy.
Chronic endometritis.,,,,,,,and new that will be discovered ,

NOT YET CLASSIFIED (AUB-N)
With more evidence, entities that discovered will be placed into a new or existing class
Accordingly our ongoing studies supported that CS scar defect should be included among a new category of FIGO 2012.
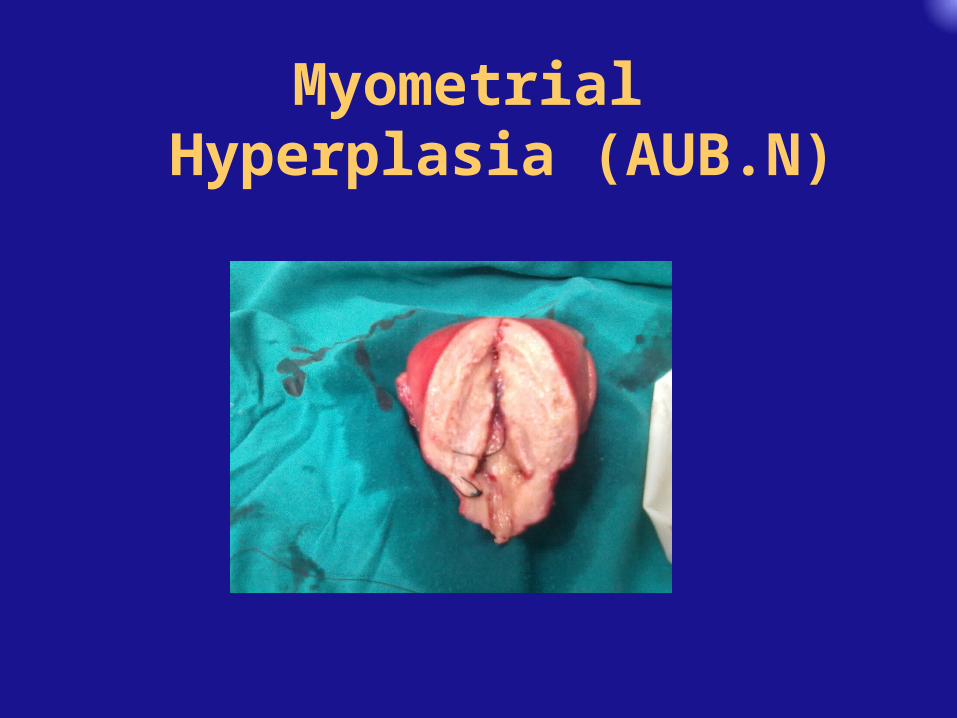
Myometrial Hyperplasia (AUB.N)


LOCALIZED MYOMETRIAL H
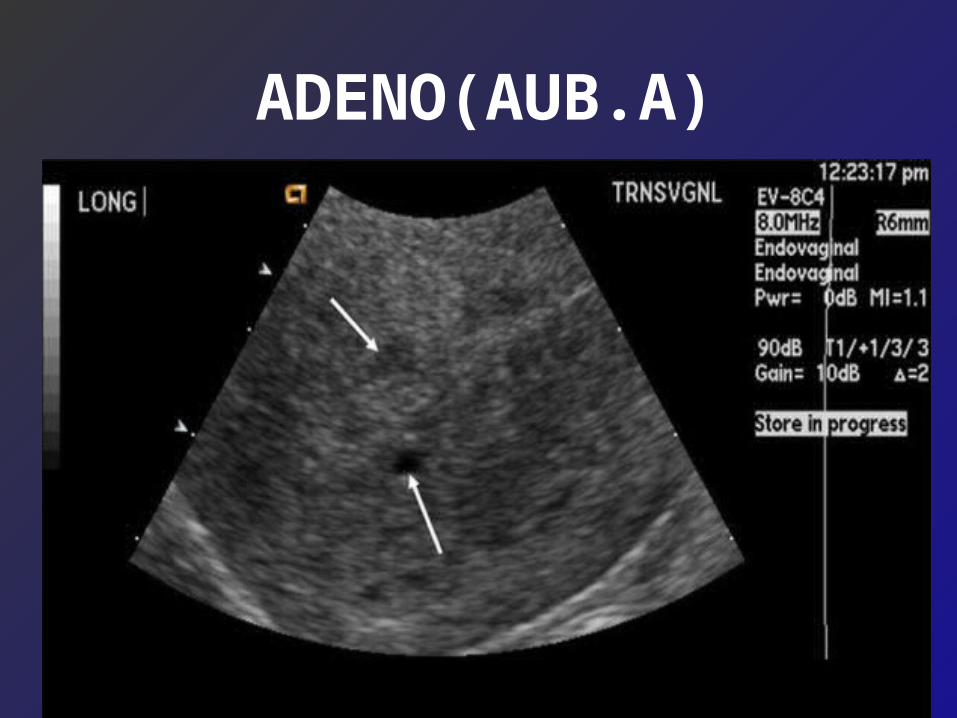
ADENO(AUB.A)

ADENO(AUB.A)


Myometrial hyperplasia (MMH) is a structural variation with irregular zones of hypercellularity and increased nucleus/cell ratio that appears in adolescence, can progress during the childbearing years, and can sometimes cause grossly detectable bulges on pathologic examination. MMH can be inframucosal, intramural (microscopic), or subserosal.myometrial hyperplasia which may be localized or diffuse
AUB.N AV FISTULA
Cong or AcquiredAny uterine manipulation can cause it.
Acquired AVMs are small arteriovenous fistulas between intramural arterial branches and the myometrial venous plexus. They appear as a vascular tangle
5%

The classical presentation of uterine AVMs is often
one of severe uterine bleeding with no obvious cause.
The onset and cessation of bleeding are abrupt, comparable to the opening and closing of a faucet

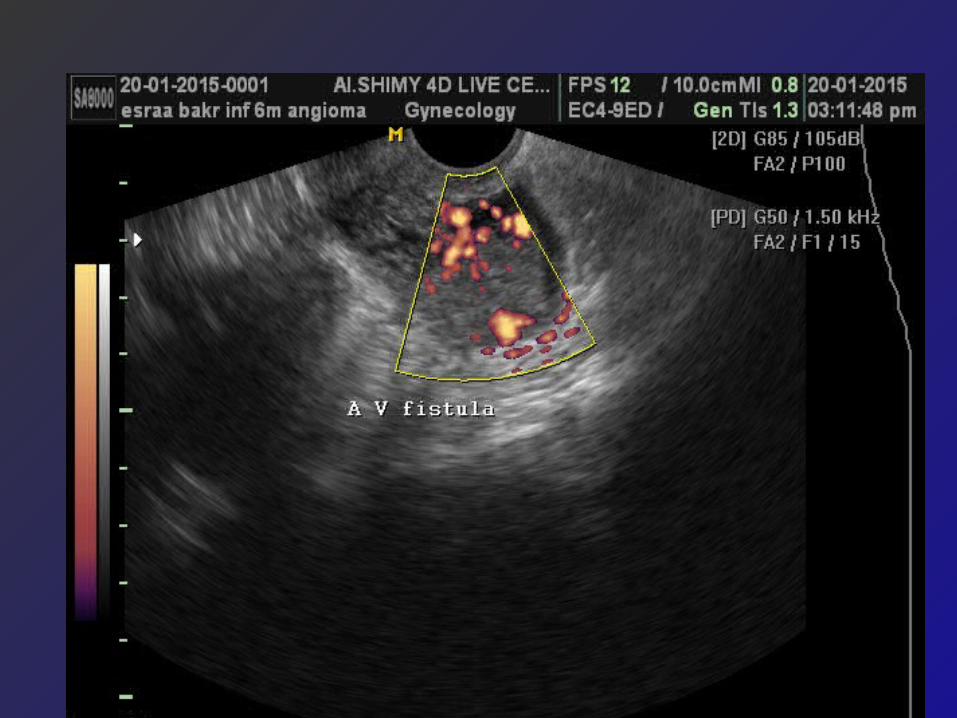

AUB N – UAV FISTULA

ULTRASONOGRAPHY OF UTERUS IN TRANSVERSE AXIS WITH COLOR DOPPLER FLOW SHOWING PULSATILE VENOUS FLOW INSIDE THE ENDOMETRIAL CAVITY.

05/15/13
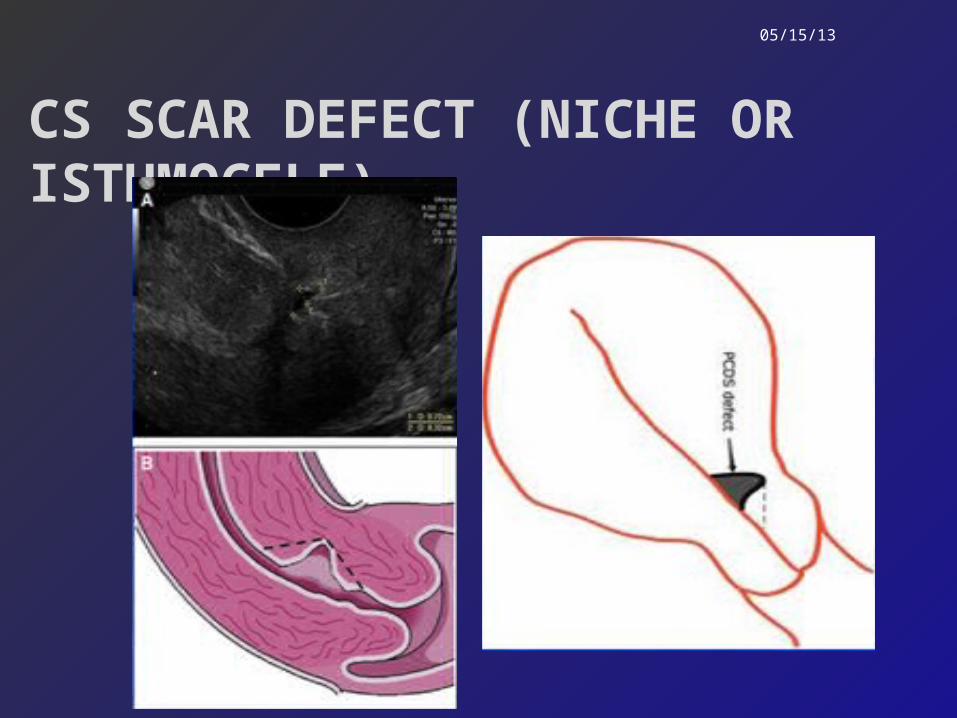
CS SCAR DEFECT (NICHE OR ISTHMOCELE)

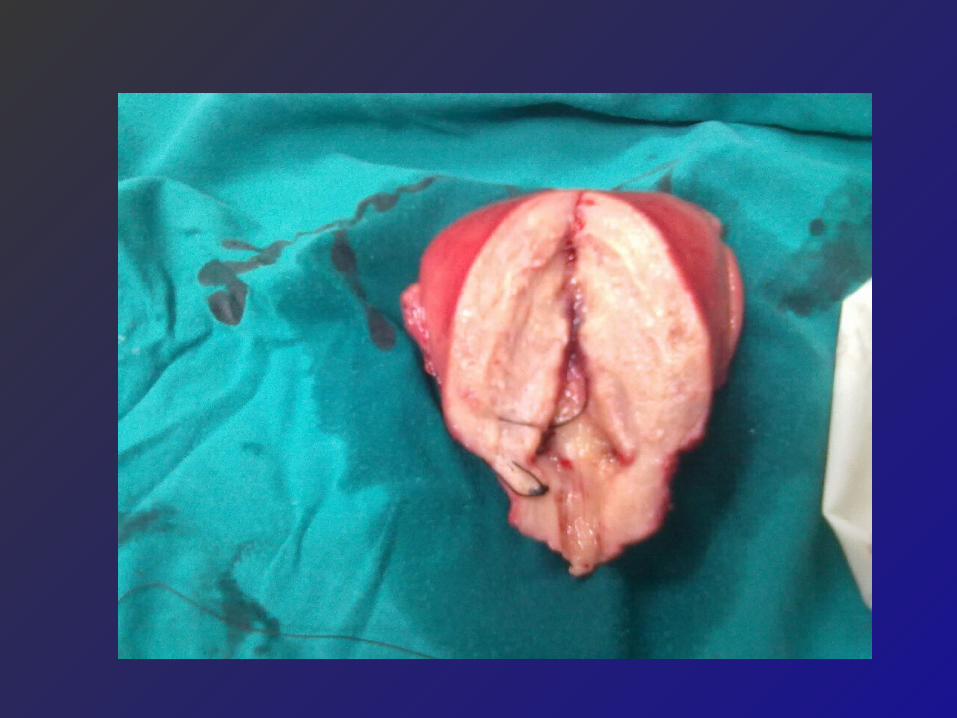
HYSTERECTOMY SPECIMENS ISTHMOCELE


05/15/13
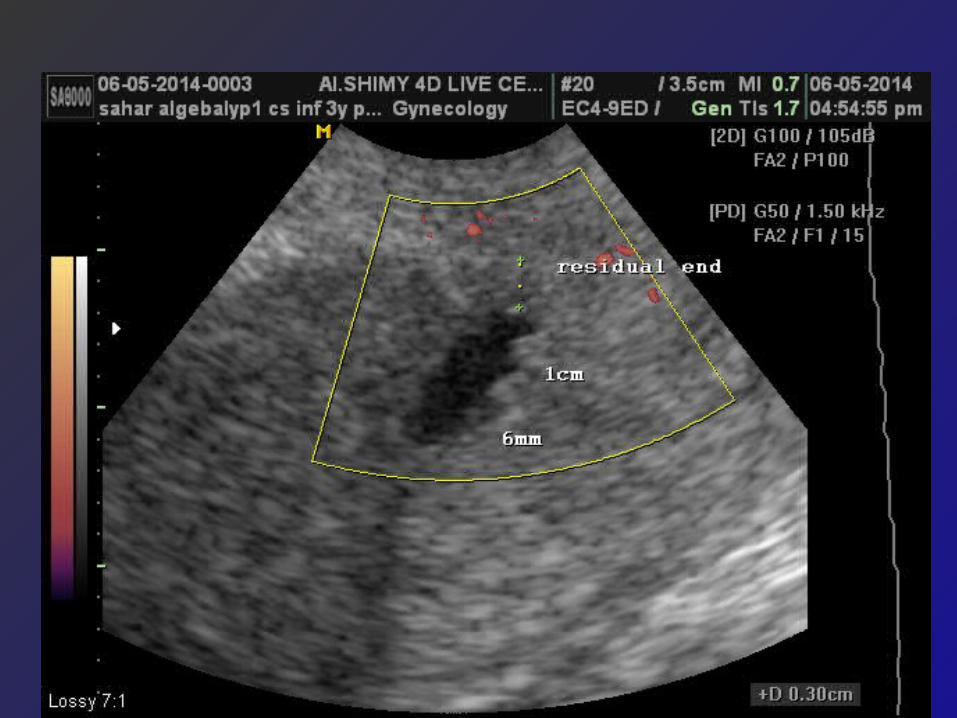
MEASUREMENT OF THE NICHE
{Intact myom
Remaining myom >
Niche
C…..=remaining myometrium…D=Intact myometrium
endometrium
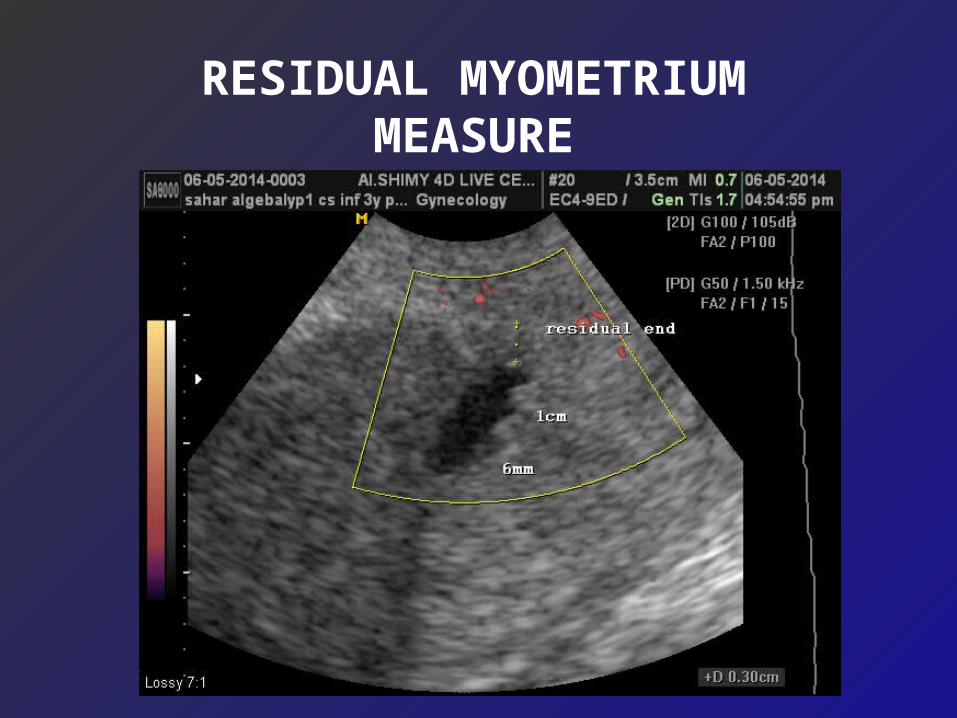
RESIDUAL MYOMETRIUM MEASURE

05/15/13
BIODEVIN1961
<Isthmocele

05/15/13
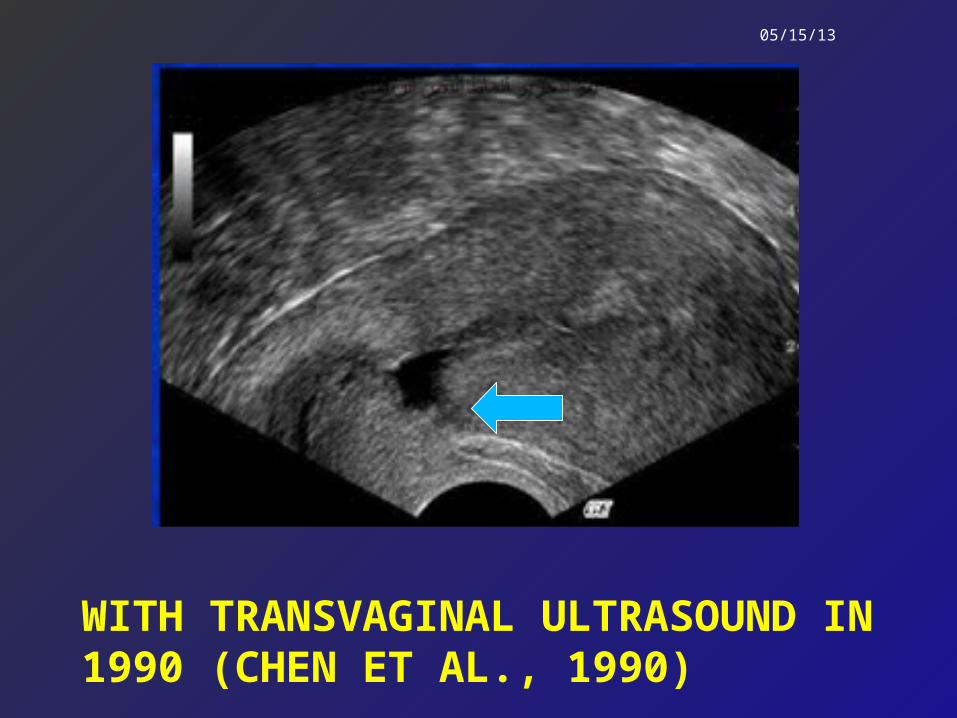
Transabdominal sonography in 1982 (Burge et al., 1982)
niche
05/15/13
WITH TRANSVAGINAL ULTRASOUND IN 1990 (CHEN ET AL., 1990)

05/15/13
3D
1 2
2 2C S Scar defects one is high,other is
low
Endocervical canal
3D one woman in this study two CS scars ARE seen
05/15/13
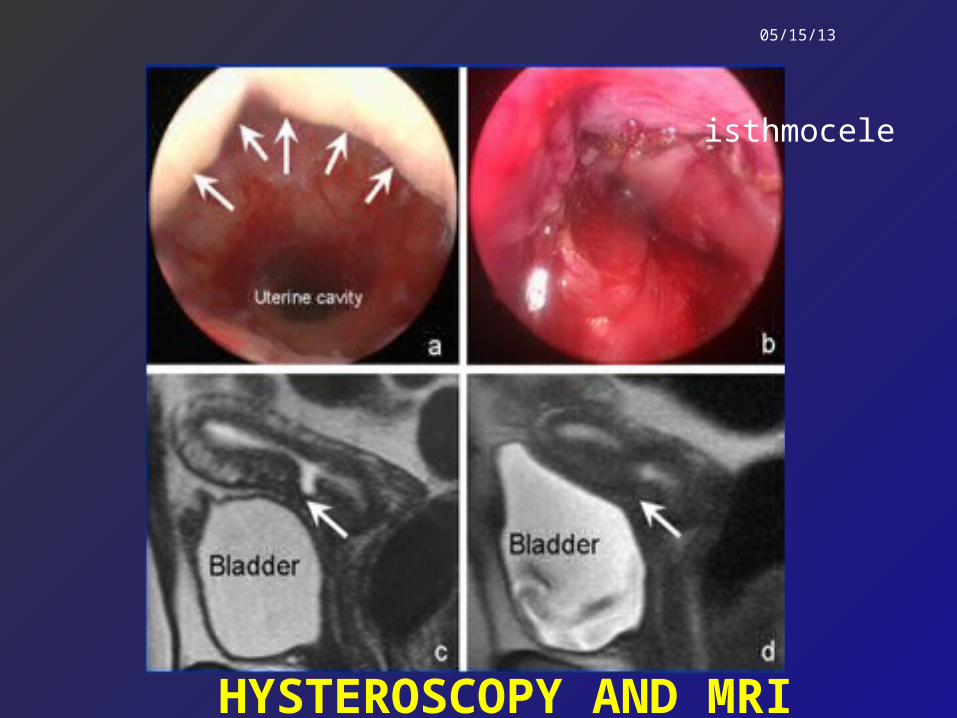
HYSTEROSCOPY AND MRI
isthmocele

Ultrasound scans showing the most common niche shapes: the semicircular niche (a), triangular niche (b), droplet-
shaped niche (c)and inclusion cysts (d).
a b
c d
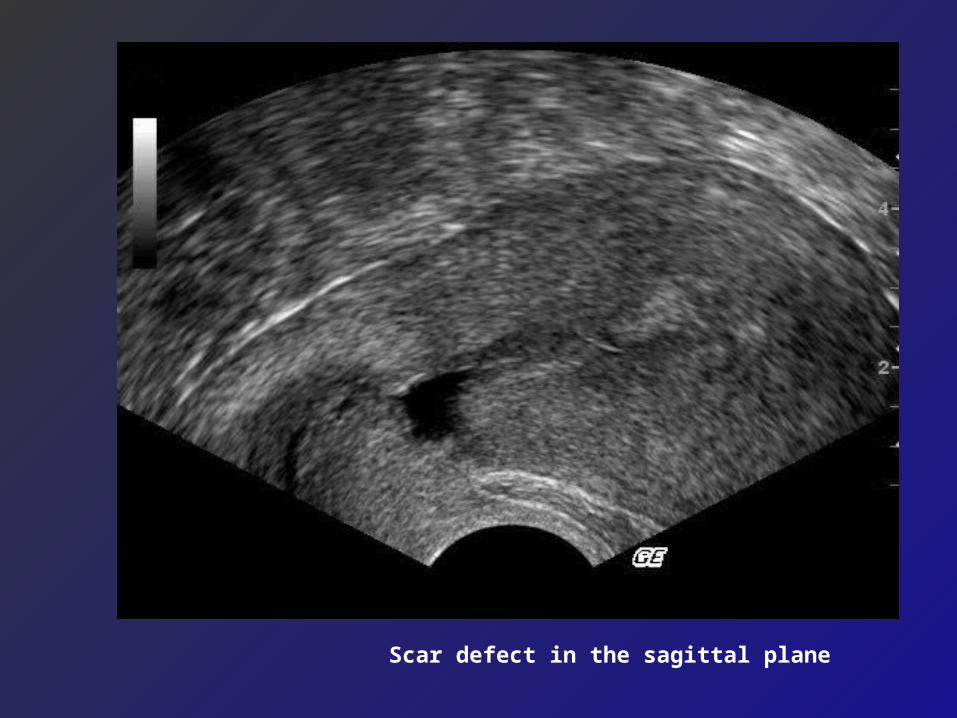
Scar defect in the sagittal plane
WHAT ADDED BY FIGO2012
In management

(ADOPTED FROM: SCHORGE ET AL., 2010.)
Previously………..Unexplained

FIRST STUDY:
HISTOPATHOLOGY OF SYMPTOMATIC SCAR DEFECT
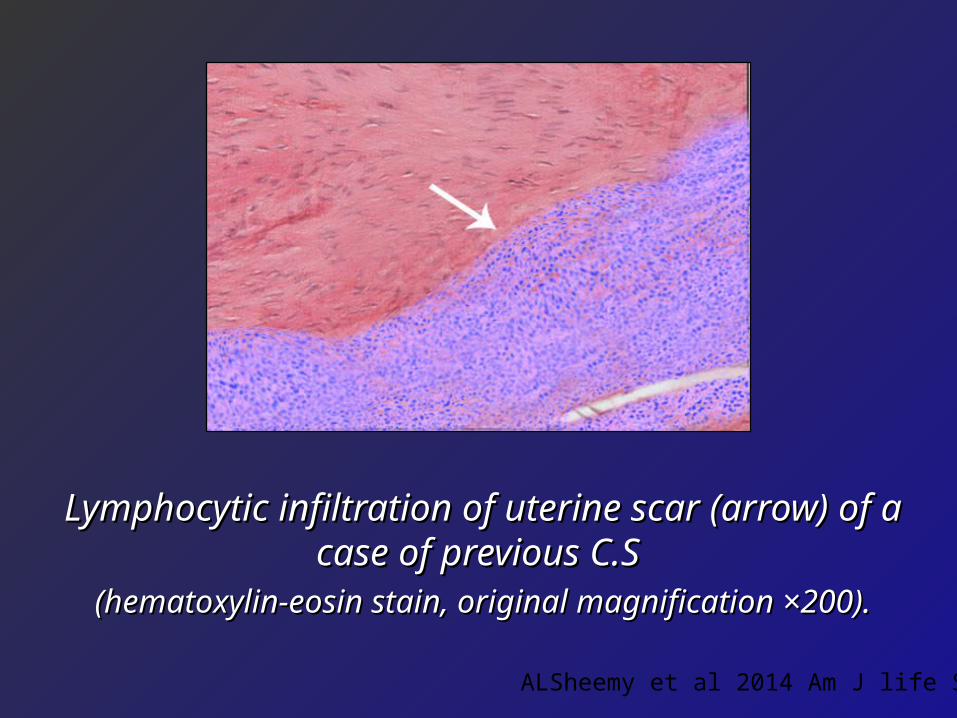
Lymphocytic infiltration of uterine scar Lymphocytic infiltration of uterine scar (arrow) of a case of previous C.S (arrow) of a case of previous C.S
(hematoxylin-eosin stain, original magnification (hematoxylin-eosin stain, original magnification ×200).×200).
ALSheemy et al 2014 Am J life Sc

Focal adenomyosis of uterine scar of a Focal adenomyosis of uterine scar of a case of previous C.S case of previous C.S
(hematoxylin-eosin stain, original magnification (hematoxylin-eosin stain, original magnification ×200).×200).
ALSheemy et al 2014 Am J life Sc

LocalizedAdenomyosis
Beside the niche
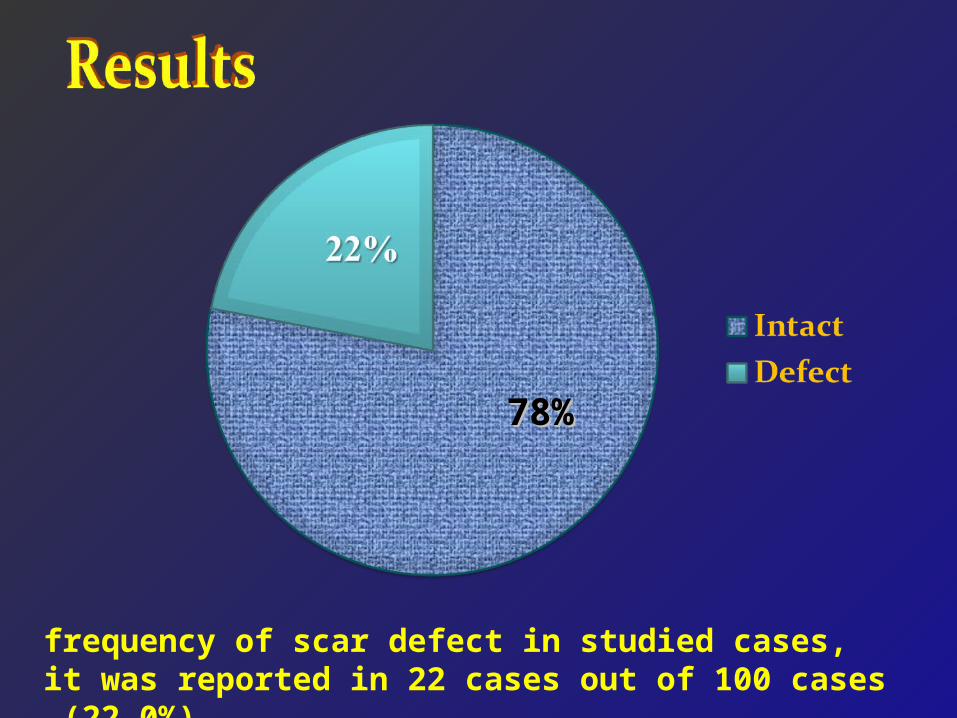
frequency of scar defect in studied cases, it was reported in 22 cases out of 100 cases (22.0%).
78%78%
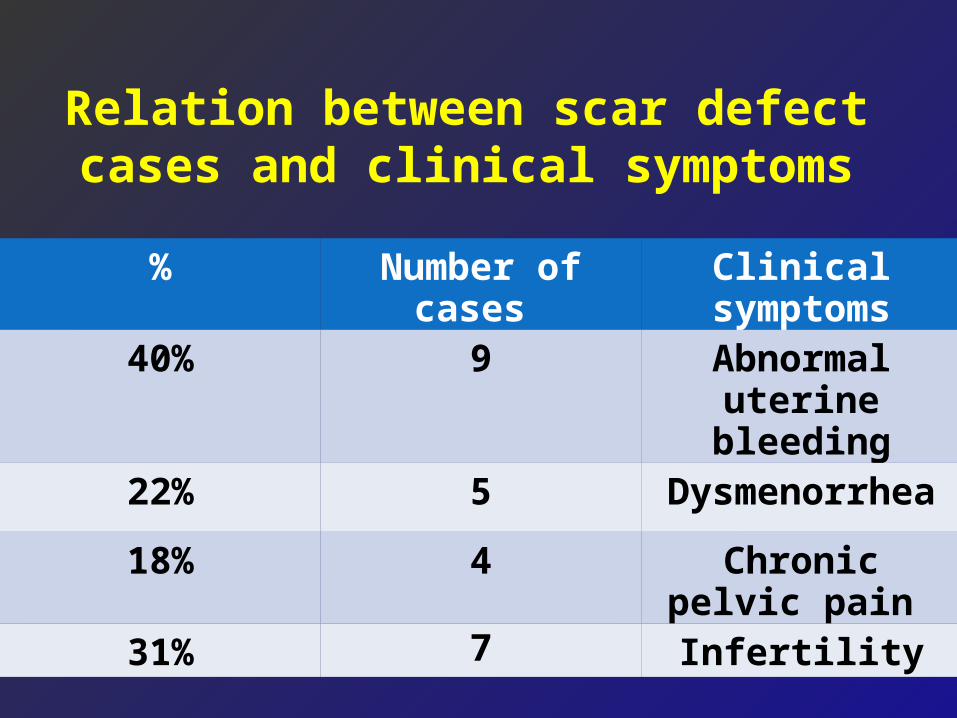
Relation between scar defect cases and clinical symptoms
Clinical symptomsNumber of cases %
Abnormal uterine bleeding
940%
Dysmenorrhea522%
Chronic pelvic pain 418%
Infertility731%
Screening for all women with CS scar is mandatory to correlate the scar pattern with the clinical presentation as abnormal uterine bleeding pelvic pain dysmenorrhea
infertility and dyspareunia .
Recommendation of the first study
The Second study

05/15/13
The aim of the study was to evaluate a new operation of vaginal uterine artery ligation in treatment of abnormal bleeding related to the scar and this was presented in 17th Ain shams conference 2013
Aim
AlSheemy et al 2015



2014
Idea of Vaginal ligation of the uterine artery is to ligate the artery in continuity close to the cervix, the cervical tissues are included in the suture so the edges of the CS scar defect is included in the sutures laterally. Ligation Of the uterine artery has its own benefit of controlling menorrhagia
Idea of Vaginal ligation of the uterine artery
Alsheemy & Samia E 2014 MD thesis

<
Site of vaginal ligation of U A,at 2 levels.
MATERIALSusing Voluson 730 Pro.( USA)
or Medison 8000SA live
(Korea), ultrasound machine,
equipped with a 7–9-MHz
transvaginal probe.
Previously………..Unexplained

n
No lesion Uterine fibroid less than 3cmUterine fibroid more than3 cm Uterine fibroid with adenomyosisDiffuse adenomyosis C scar defectArterio venous fistula
C S S D
No Lesion
M (Large)
Small M M+A
A V F

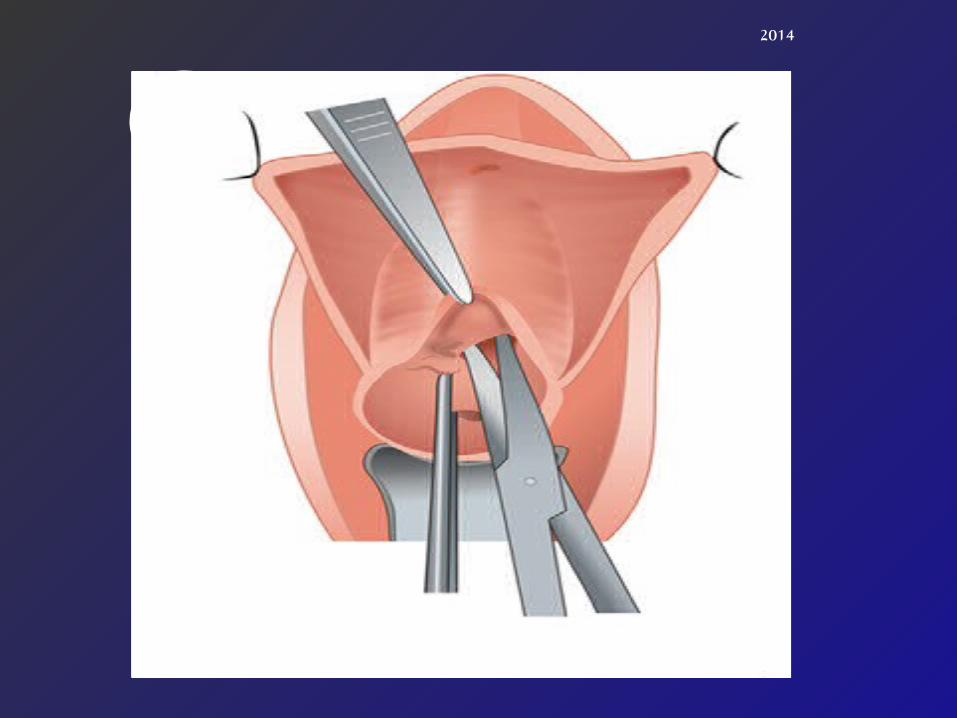
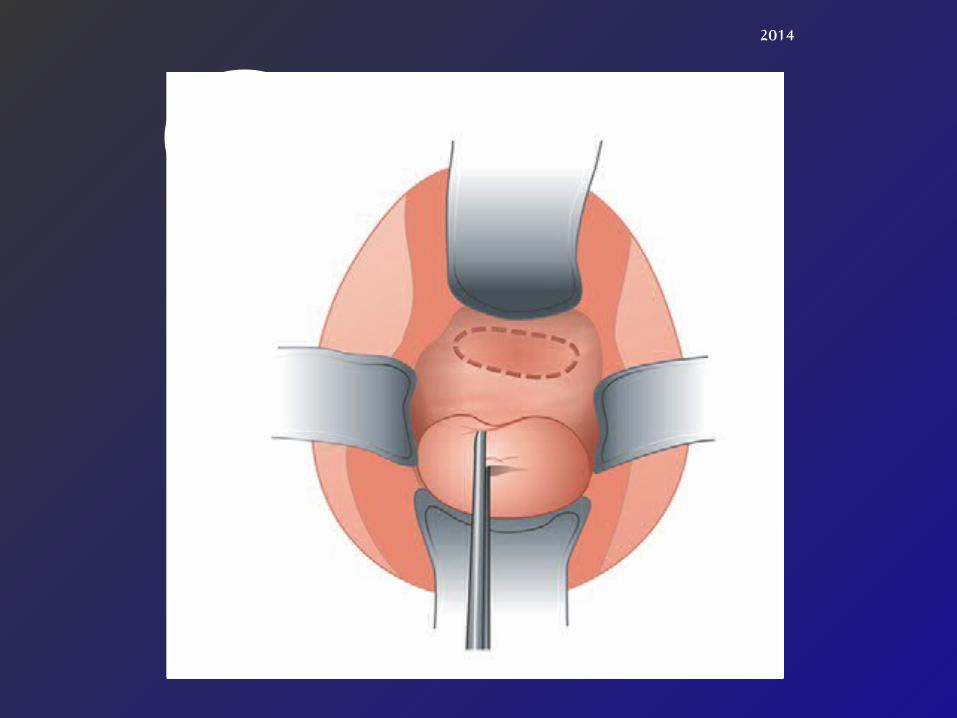
Steps of vaginal bilateral uterine artery ligation
operation:
1- The posterior vaginal wall was retracted with a Sims speculum, and the anterior lip of the cervix was held with a vulsellum.

2-. Transverse incision was made at the cervicovaginal junction. The bladder is
separated from the cx and reflected upward for 3 cm.
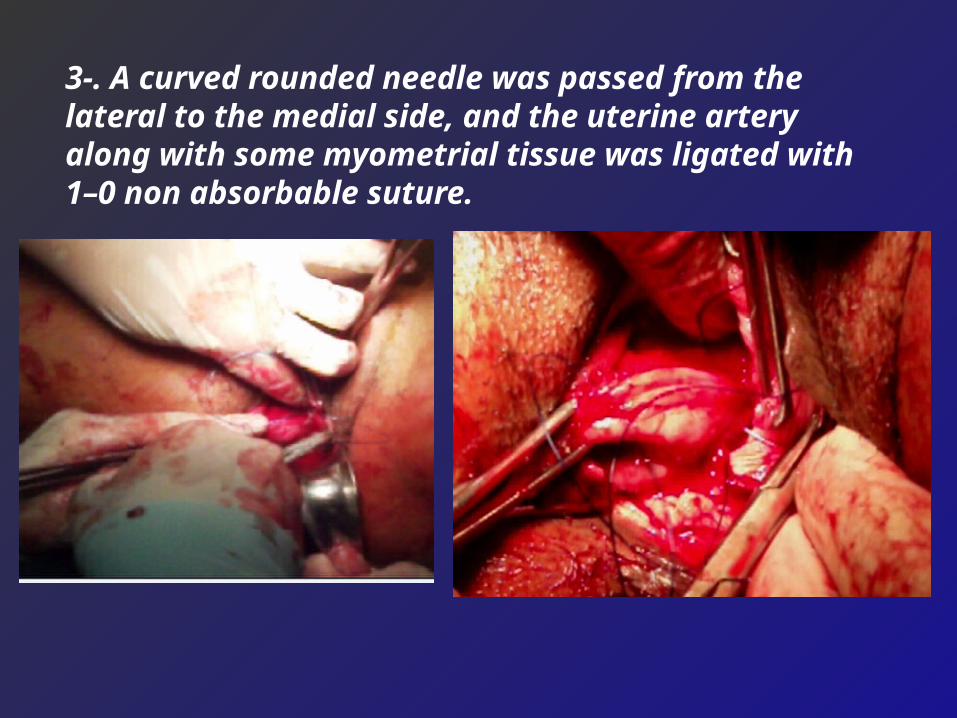
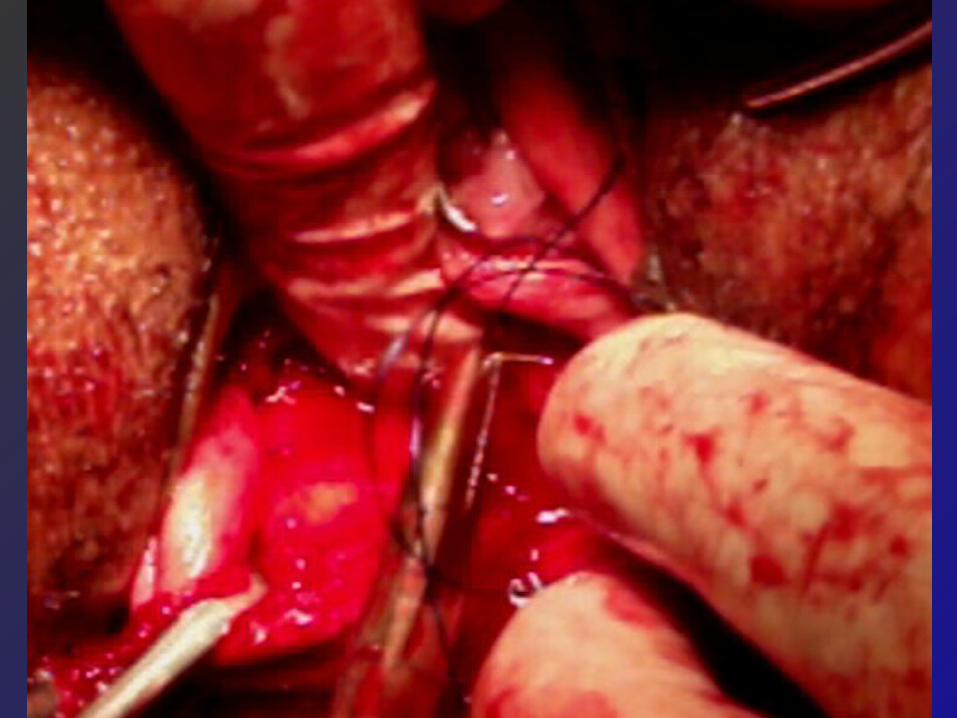
3-. A curved rounded needle was passed from the lateral to the medial side, and the uterine artery along with some myometrial tissue was ligated with 1–0 non absorbable suture.



4- Cystoscopic examination was performed to confirm bilateral ureteric patency

2014
4
2014
3
2014
5

2014
7
• The operative time without cystoscopy
was 22 minutes.
• The mean hospital stay time was 3hours.
Results

Serial post operative follow up every 2 months
then applied for 3 years to record the response to
the operation as regard bleeding cycles regularity
degree of pain with TVS;CD , niche
width,pregnancy rate with its outcome and
uterine volume measurement.
90

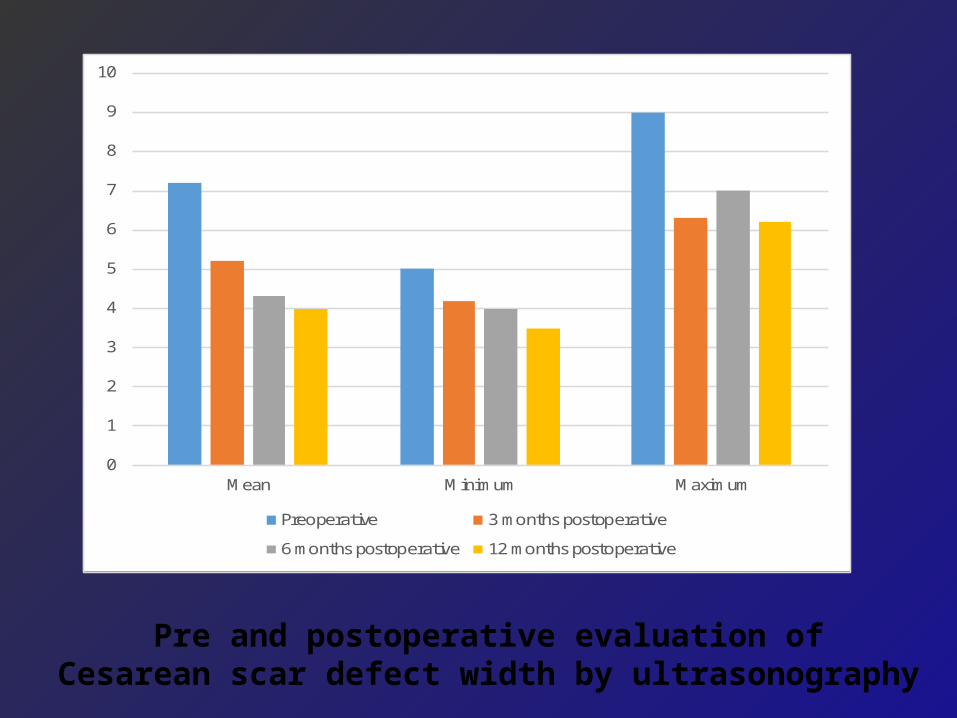
Scar defect width (mm)MeanSDMinimumMaximum
Preoperative 7.2
2.259
3 months postoperative 5.21.84.26.3
6 months postoperative 4.31.747
12 months postoperative 3.01.205
Paired comparison Preoperative vs 3 months; t = 12.15, p < 0.001*
Preoperative vs 12 months; t= 16.31, p <0.001*
Pre and postoperative evaluation of Cesarean scar defect width (mm) by ultrasonography
0
1
2
3
4
5
6
7
8
9
10
Mean Minimum Maximum
Preoperative 3 months postoperative
6 months postoperative 12 months postoperative
Pre and postoperative evaluation of Cesarean scar defect width by ultrasonography
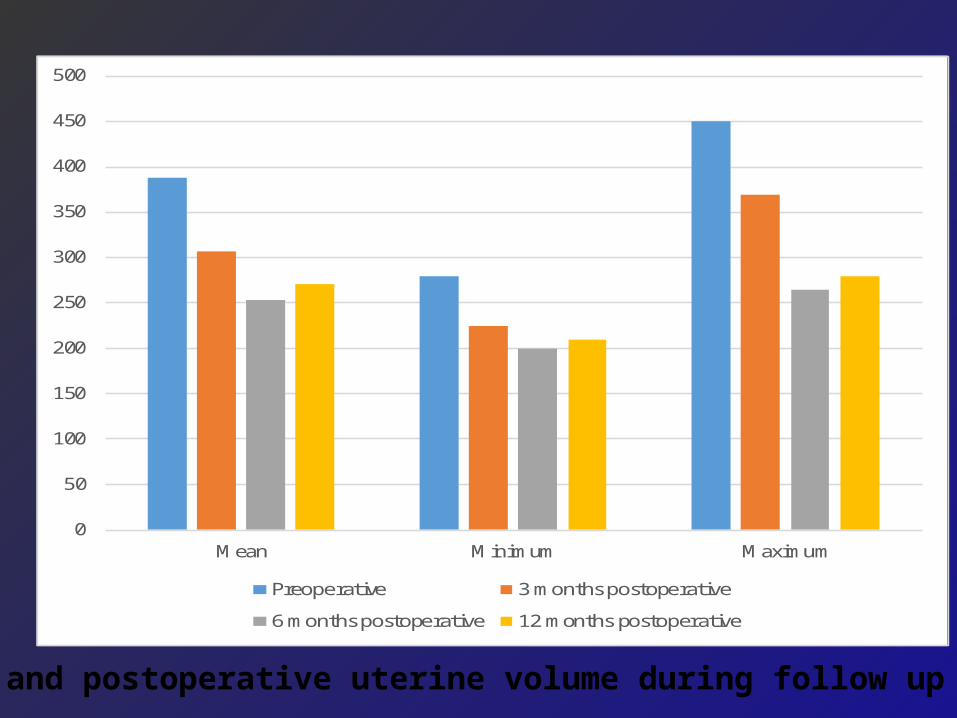
0
50
100
150
200
250
300
350
400
450
500
Mean Minimum Maximum
Preoperative 3 months postoperative
6 months postoperative 12 months postoperative
pre and postoperative uterine volume during follow up period
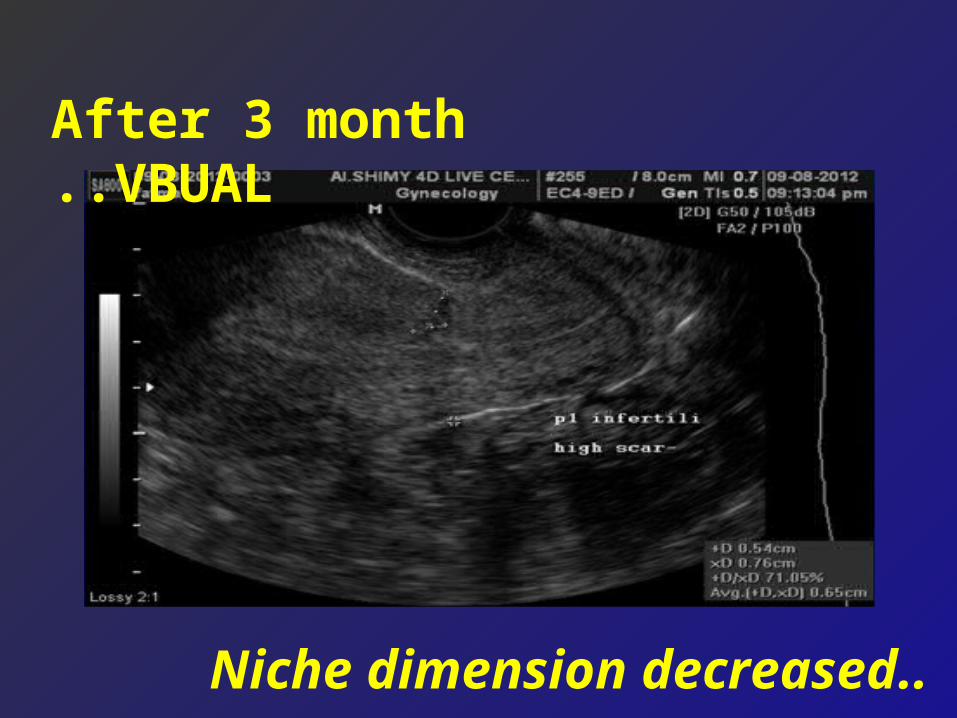
After 3 month VBUAL..
..Niche dimension decreased
05/15/13
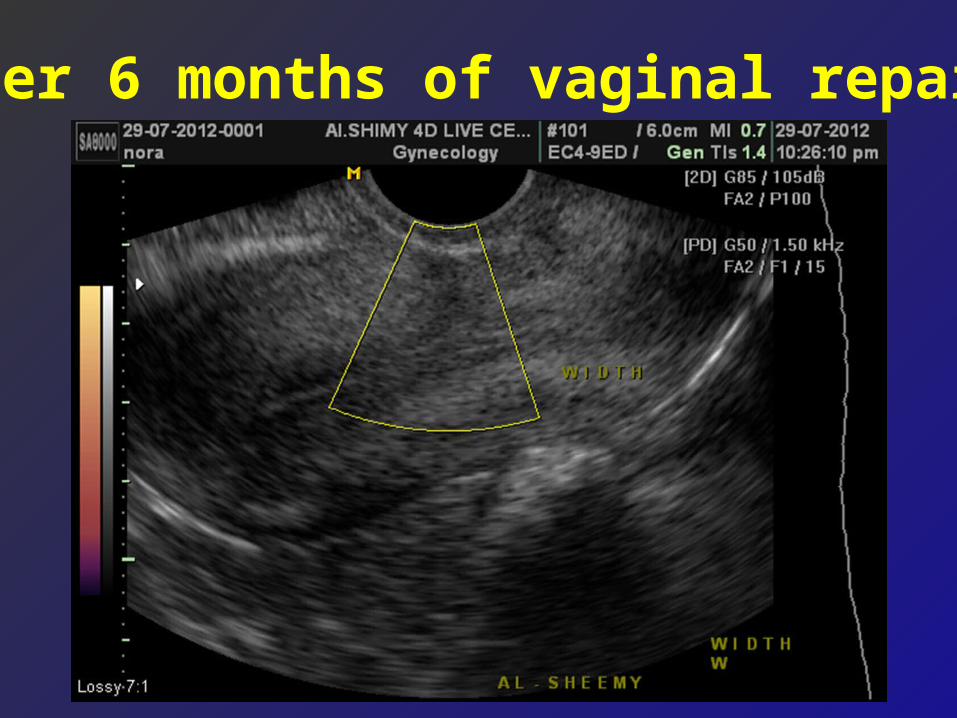
After 6 months of vaginal repair
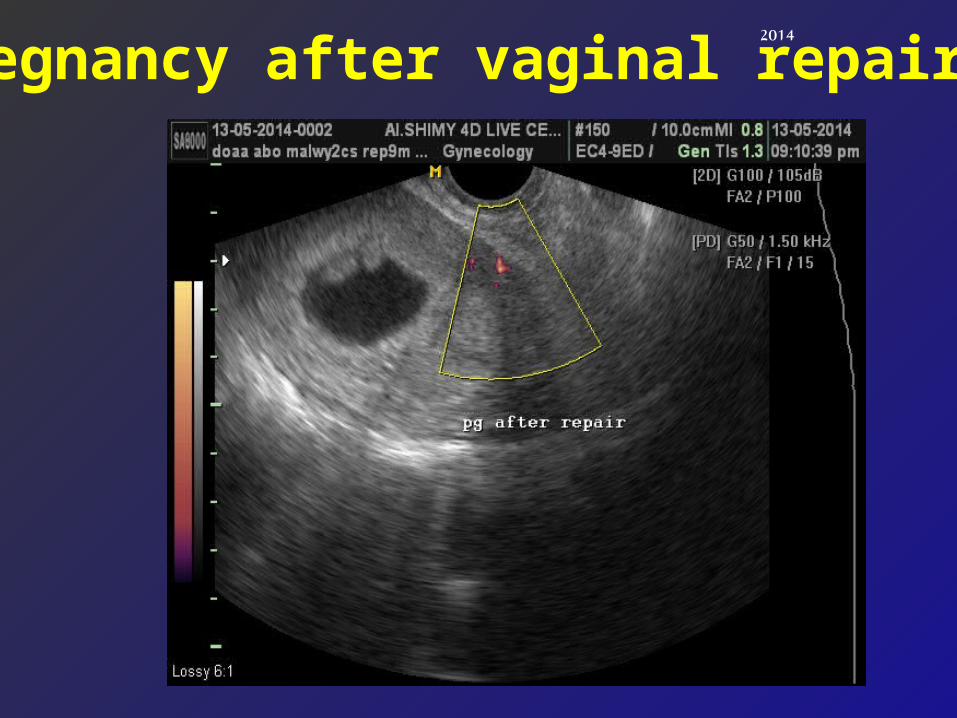
2014
Pregnancy after vaginal repair
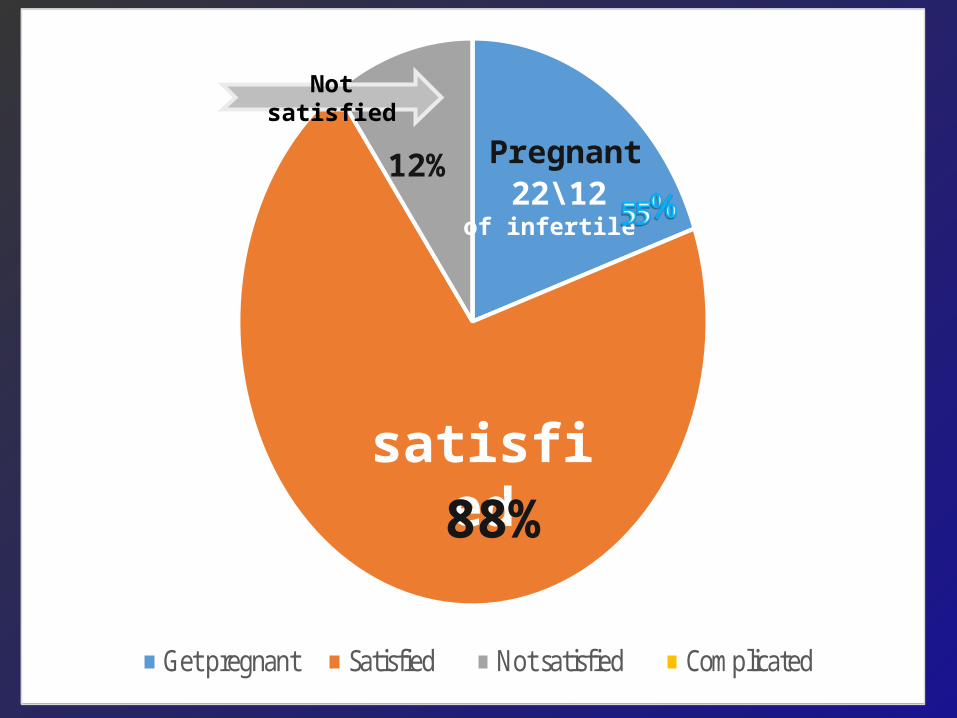
Get pregnant Satisfied Not satisfied Complicated
satisfied
Not satisfied
Pregnant12\22
of infertile
12%
88%
• VBUAL and Vaginal repair are simple safe, minimally invasive and not time consuming and can be applied before deciding histerectomy specially in young women
• Clinical and sonographic results of both are promising specially as regard patient satisfaction.
• Our primary results indicate that unremarkable pregnancy can occur with good pregnancy outcome .
99
Conclusion of three studies

www.prof-shimy.8m.com
Not yet Classified?

Thank [email protected]

4- Design large future controlled studies that will include large sample size for more validation and confirmation of the results.
5- Design further studies to compare VBUAL operation with other methods of operative uterine artery occlusion as laparoscopic BUAL, Doppler -assisted trans-vaginal uterine artery clamping as treatment options for refractory menorrhagia

Discarded Terminology
Menorrhagia, Hypermenorrhea. Hypomenorrhea Menometrorrhagia Polymenorrhea ,Polymenorrhagia Oligomenorrhea
DISCARDED TERMINOLOGY CONT.
Dysfunctional uterine bleeding Functional uterine bleeding Metropathica hemorrhagica Amenorrhea – retained term
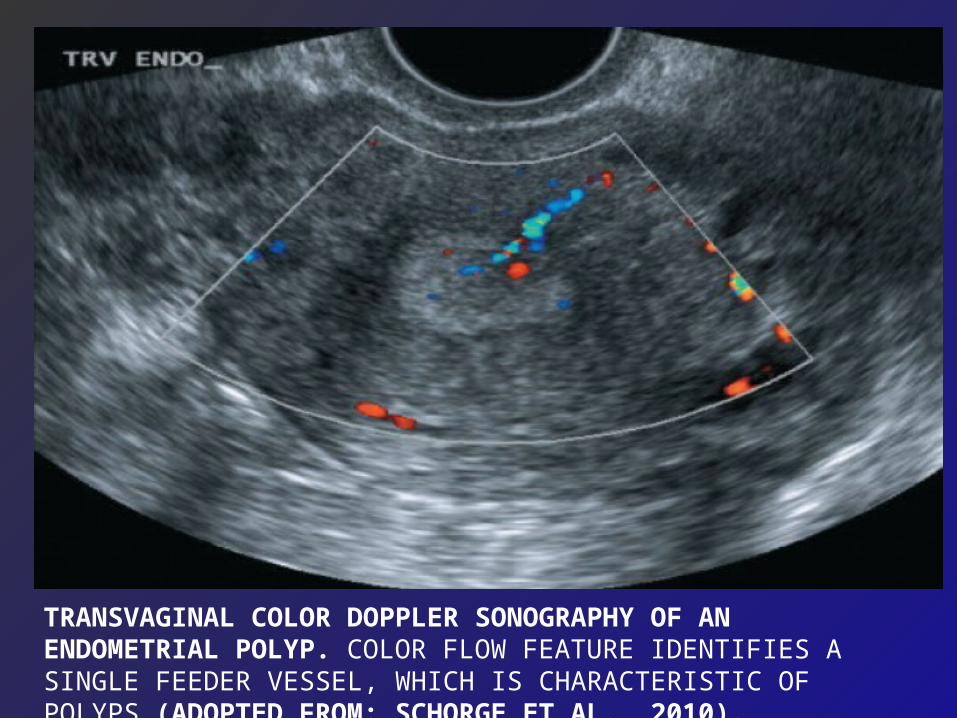
TRANSVAGINAL COLOR DOPPLER SONOGRAPHY OF AN ENDOMETRIAL POLYP. COLOR FLOW FEATURE IDENTIFIES A SINGLE FEEDER VESSEL, WHICH IS CHARACTERISTIC OF POLYPS (ADOPTED FROM: SCHORGE ET AL., 2010).

MYOMET HYPERTROPHY (DIFFUSE)

ETIOLOGY OF HEAVY MENSTRUAL BLEEDING
(R. Hurskainen et al., 2007)
Systemic causesLocal uterine causes
Treatment–related causes
Idiopathic causes
HypothyroidismPolypPoor execution of
anticoagulant therapy
Increased fibrinolysis
DiabetesMyomaCopper IUDOverproduction of
prostacyclin or prostaglandin E2
Chronic cardiac or renal disease
Lack of
thromboxane
Chronic hepatic disease
Adenomyosis Lack of
prostaglandin F2alfa
Systemic lupus erythematosus
Infection Lack of endothelin
ObesityCarcinoma Disorder in
vasoactive peptide hormones
Coagulation disorderspelvic arteriovenous
malformation
Delayed endometrial regeneration
Disorder in endometrial angiogenesis
overproduction of nitrogen oxide

Transvaginal sonography showed localized posterior wall lesion (localized adeno myosis ).(AUB-A) P0 A1 L0 M0 - C0 O0 E0 I0 N0
Uterine arteriovenous malformation (AVM) is a rare but potentially life-threatening source of bleeding. Dubreil and Loubat described the first clinical case involving a uterine AVM in 1926. The true incidence is unknown, but with increased use of ultrasound to evaluate abnormal vaginal bleeding, O’Brien et al propose a rough predicted incidence of 4.5% .AVMs have been reported in patients from 18 to 72 years old but only rarely in nulliparous women .

AVMs are characterized by multiple communications of varying sizes between arteries and veins in the same vicinity. Uterine AVMs have been classified as congenital or acquired Congenital uterine AVMs arise from an abnormality in the embryological development of primitive vascular structures, resulting in multiple abnormal communications between arteries and veins. Acquired uterine AVMs are usually traumatic, resulting from prior dilation and curettage (D&C), uterine surgery, or direct uterine trauma,

2014
2

ItemN
Studied
Decrease in the mean uterine volume. 18 cases 35. 5 %
Mean niche diameters. 8 cases 70.1%
Peak systolic velocity in intra myometrial arteries 18 cases 32 cm/s
Pregnancy in infertile group 12 cases 75%
*R I: Resistance Index.
Results Of Sonographic And Color Doppler
Study During The First Year Of Operation.
Results
117

Levo Norgesterol Intrauterine SystemThe Levonorgesterol Intrauterine System (ius; Mirena) Provides Another Great Option For Aub Therapy. This New Ius Produces A Dramatic Decline In Menstrual Blood Loss By 65% To 98%
Within 12 Months Of Use .There Is Little Systemic Absorption Of Progesterone
(Hurskainen et al., 2001 )and ) Bilian, 2002(.


ENDOMETRIAL DYSFUNCTION (AUB-E) A DIAGNOSIS OF EXCLUSION PATIENT HAS PREDICTABLE AND CYCLIC BLEEDING TYPICAL OF
OVULATORY CYCLES MECHANISM: A PRIMARY DISORDER OF THE ENDOMETRIUM
DISTURBANCES OF METABOLIC MOLECULAR PATHWAYS – TISSUE FIBRINOLYTIC ACTIVITY, PROSTAGLANDINS, INFLAMMATORY AND VASOACTIVE MEDIATORS NO

DIAGNOSIS OF(AVM)Traditionally, uterine AVMs were diagnosed after hysterectomy with histopathologic evidence of the arteriovenous fistulas. (Fleming et al 1989). Several imaging methods, such as Doppler ultrasonography, computed tomography, magnetic resonance imaging (MRI), and angiography, have been employed to diagnose AVMs. Angiography is the gold standard for diagnosis, whereas Doppler ultrasonography and MRI are the modalities of choice for the evaluation of a suspected AVM. Ultrasonography and MRI can not only define

angiography is an invasive procedure, and should be reserved for cases in which surgical intervention or therapeutic embolization of the lesion is planned . Gray-scale and color and duplex Doppler ultrasound (US) and the magnetic resonance (MR) imaging are noninvasive methods for diagnosis of uterine arteriovenous malformations (AVMs) at gray-scale US, uterine AVMs were nonspecific and manifested as subtle myometrial in homogeneity, tubular spaces within the myometrium, intramural uterine mass, endometrial mass,
