management of labour & fetal assessment king khalid university hospital department of obstetrics...
TRANSCRIPT
Management of labour & fetal assessment
King Khalid University HospitalDepartment of Obstetrics & Gynecology
Course 482

Management of labour & fetal assessment
Objectives:
Managements of the stages of labourPain relief in labourFetal assessment (antenatal & intra-partum)

Management of labour
Definition of labour:Progressive cervical effacement and dilatation resulting from regular uterine contractions that occur at least every 5 minutes and last 30-60 secondsBraxton Hicks: contractions Not associated with cervical changes
Lightening: Descent of the fetal head into the pelvisThere are 4 stages of labour

First stage of labourStart from onset of true labour pain----full dilatation of cervixIn primigravida------ 12 hour durationIn multigravida-----6 hours duration
Chiefly concerned with preparation of the birth canal as to facilitate expulsion of the fetus in the second stage
It has 2 phasesA latent phase up to 3 cm dilatation of cervix
• is variable: up to 8 hours in primi• 4 hours in multi
An active phase from 3 cm to full dilatation of cervixRate of dilatation 1 cm/hour in primigravida
• 1.5 cm/ hour in multigravida

Dilatation of the cervix
Dilatation usually measured by fingers but recorded in cm
Dilatation relates with dilatation of internal os

Effacement or taking up of cervix
Muscle fibers of cervix are pulled upward and merges with the fibers of the lower uterine segment
Cervix becomes thin during first stageIn primi----- effacement precedes dilatation of the cervixIn multi-----both occur simultaneously
Effacement is determined by the length of the cervical canal in the vaginaEffacement is expressed in terms of percentage

Effacement or taking up of cervix

First stage of labour
Maternal system-General condition remains
unaffected-Pulse rate increases by 10-15
bpm during contraction with the settle down to its previous rate in between contractions
-Systolic BP increase by 10 mm Hg during contraction
-Temperature remains unaffected
Fetal system-As so long as the membranes
are intact, usually there is no adverse effect on the fetus BUTHowever, during contraction there may be slowing of FHR by 10-20 bpm which soon returns to its normal as the intensity of contraction diminishes

Management of labour
Initial assessment:History: Onset, strength, frequency of contractionsLeakage of fluidVaginal bleedingFetal movementMedicationsLast oral intakeReview of past obstetric history, prenatal lab tests, gestational age, parity, size of previous infants, any antenatal complications

Management of the first stage of labour
--Informed consent on management of labour & delivery-Maternal position---lateral recumbent position
- Avoid supine hypotension-Partogram:
-Iv fluids & avoid oral intake-Maternal vital signs every 1-2 hours
-Input-output monitoring-Analgesia
- Fetal heart rate monitoring (CTG)-Uterine contractions monitoring
-Vaginal examination for cervical dilatation & poistion in active phase every 2 hours
--Amniotic membranes status & amniotic fluid colour

Monitoring progress of labour (Partogram)

Mechanics of labour
The Power: force generated by uterine contraction

Second Stage of labour
From full dilatation of cervix till delivery of the neonateThe mother has a desire to bear down with each contractionLast from 30 minutes to 3 hours in primigravida
5-30 minutes in multigravida

Mechanism of labour
Management of the second stage of labour
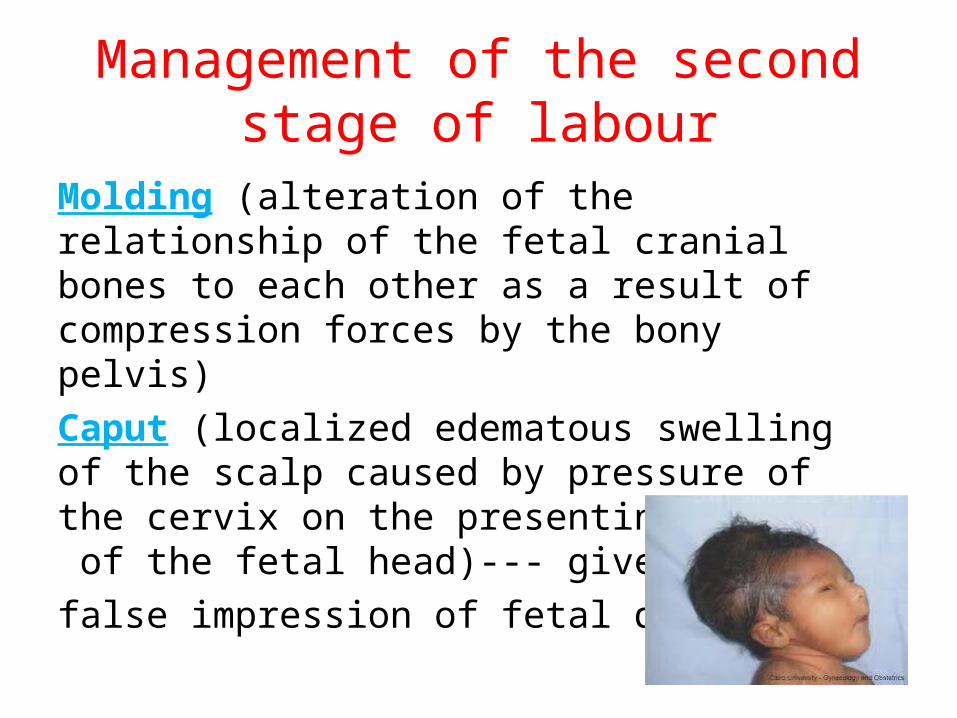
Molding (alteration of the relationship of the fetal cranial bones to each other as a result of compression forces by the bony pelvis)Caput (localized edematous swelling of the scalp caused by pressure of the cervix on the presenting portion of the fetal head)--- gives
false impression of fetal descent

Management of the second stage of labour
Crowning ( when the largest diameter of the fetal head is encircled by the vulvar ring)
-Vaginal examination every 30 minutes-Maternal position– any comfortable position for bearing
down-Bearing down---with each contraction
-Delivery of the fetal head---manual perineal support-Fetal airway clearance
-Umbilical cord clamping-Place the infant under warmer

Episiotomy
Incision in the perineum after crowning to aid delivery and avoid laceration of periniumTypes: Right mediolateral
Left mediolateral Central

PERINEAL LACERATION
4 TYPES:
-First degree: laceration involving the vaginal epithelium or perineal skin
-Second degree: laceration extending into the sub-epithelial tissues of the vagina or perineum with or without involving the perineal bodyThird degree: laceration involving anal sphincterFourth degree: laceration involving rectal mucosa

Third stage of labourThe interval between the delivery of the infant and complete delivery of the placenta & membranes
Duration is 5-30 minutes Signs of placental separation:
1 -Fresh blood show from vagina2 -The umbilical cord lengthens outside the vagina
3 -The fundus of the uterus rises up4 -The uterus becomes firm & globular
The placenta should be examined to ensure that it is completeThe blood loss should be estimated

Forth stage of labour
The hour immediately after the delivery
-Needs close observation of: blood pressure ,pulse rate, uterine blood loss
Watch for post partum hemorrhage

Pain relief in labour
Goal: effective pain relief to the mother that is safe for her & the fetus with minimal side effects on the progress & outcome of labour

Pain relief in labour
Non pharmacological method:
Back massageAcupunctureHypnosisBreathing exercises

Pain relief in labourPharmacological methods:
Narcotic analgesics– cross the placenta – cause fetal respiratory depression (Nitrous oxide, pethidine)Epidural analgesia: The most effectiveContra indicated if-coagulo-pathy, infection at needle site, severe hypo-volemiaSide effects: Hypotension, headache, impaired ability to push, prolonged second stage (15 Minutes)Pudendal block: for S2-S4
for the second stage of labour for instrumental delivery

Fetal assessment
Aim: Ensure fetal wellbeing ( Identify patients at risk of fetal asphyxia)
To prevent prenatal mortality & morbidity

Screening for high risk pregnancy
History *Age
*Social burden*Smoking
*Past medical conditions e.g D.M, HTN*Past Obstetric history

FETAL AND NEONATAL COMPLICATIONS OFANTEPARTUM ASPHYXIA
Stillbirth (Mortality)Metabolic acidosis at birth
Hypoxic renal damageNecrotizing enterocolitisIntracranial haemorrhageSeizuresCerebral palsy

CONDITIONS ASSOCIATED WITH INCREASEDPERINATAL MORBIDITY/MORTALITY
Small for gestational age fetusDecreased fetal movementPostdates pregnancy (>294 days)Pre-eclampsia/chronic hypertensionPre-pregnancy diabetesInsulin requiring gestational diabetesPreterm premature rupture of membranesChronic (stable) abruption

When to start fetal Assessment antenatally
**Risk assessed individually**For D.M. fetal assessment should start from 32
weeks onward if uncomplicated***If complicated D.M. start at 24 weeks onward
**For Post date pregnancy start at 40 weeks**For any patient with decrease fetal movement
start immediately **Fetal assessment is done once or twice weekly

Antenatal Fetal Assessment
Fetal movement countingNon stress test
Contraction stress test
Ultrasound fetal assessment
Umbilical Doppler Velocimetry

Fetal movement counting
Cardiff technique:
*Done in the morning, patient should:
calculate how long it takes to have 10 fetal movement
**10 movements should be appreciated in 12 hours

Fetal movement counting
Sadovsky technique:
-For one hour after meal the woman should lie down and concentrate on fetal movement
-4 movement should be felt in one hour-If not , she should count for another hour
-If after 2 hours four movements are not felt, she should have fetal monitoring

Non stress test
*Done using the cardiotocometry with the patient in left lateral position
**Record for 20 minutes

Non stress test
*The base line 120-160 beats/minute*Reactive:
At least two accelerations from base line of 15 bpm for at least 15 sec within 20 minutesNon reactive:
No acceleration after 20 minutes- proceed for another 20 minutes
Non stress test
If non reactive in 40 minutes---proceed for contraction stress test or biophysical profile
The positive predictive value of NST to predict fetal acidosis at birth is 44%

NST

NST

Contraction stress test
Fetal response to induced stress of uterine contraction and relative placental insufficiency
Should not be used in patients at risk of preterm labor or placenta previa
Should be proceeded by NST

Contraction stress test
Contraction is initiated by nipple stimulation or by oxytocin I.V.
The objective is 3 contractions in 10 minutes
If late deceleration occur-----positive CST

Interpretation of CTG
Normal Baseline FHR 110–160 bpm –Moderate bradycardia 100–109 bpm –Moderate tachycardia 161–180 bpm
–Abnormal bradycardia < 100 bpm –Abnormal tachycardia > 180 bpm

CTG
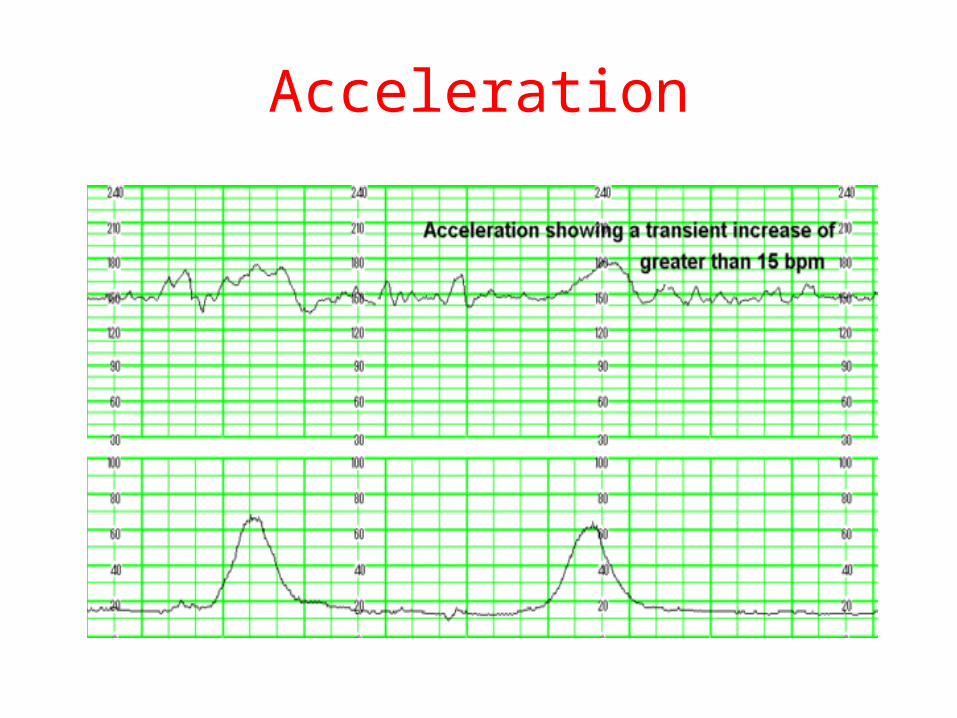
Acceleration

Deceleration
EARLY : Head compression
LATE : U-P Insufficiency
VARIABLE : Cord compression Primary CNS dysfunction

Early deceleration

Late deceleration

Variable Deceleration

Reduced Variability

TachycardiaHypoxia
ChorioamnionitisMaternal fever B-Mimetic drugs
Fetal anaemia,sepsis,ht failure,arrhythmias

Ultrasound fetal assessment
Assessment of growth
Biophysical profile (BPP)

Assessment of fetal growth by ultrasound
Biometry:
Biparietal diameter (BPD)Abdominal Circumference (AC)Femur Length (FL)Head Circumference (HC)Amniotic fluidPlacental localization

Assessment of fetal growth by ultrasound
BPD
AC
FL
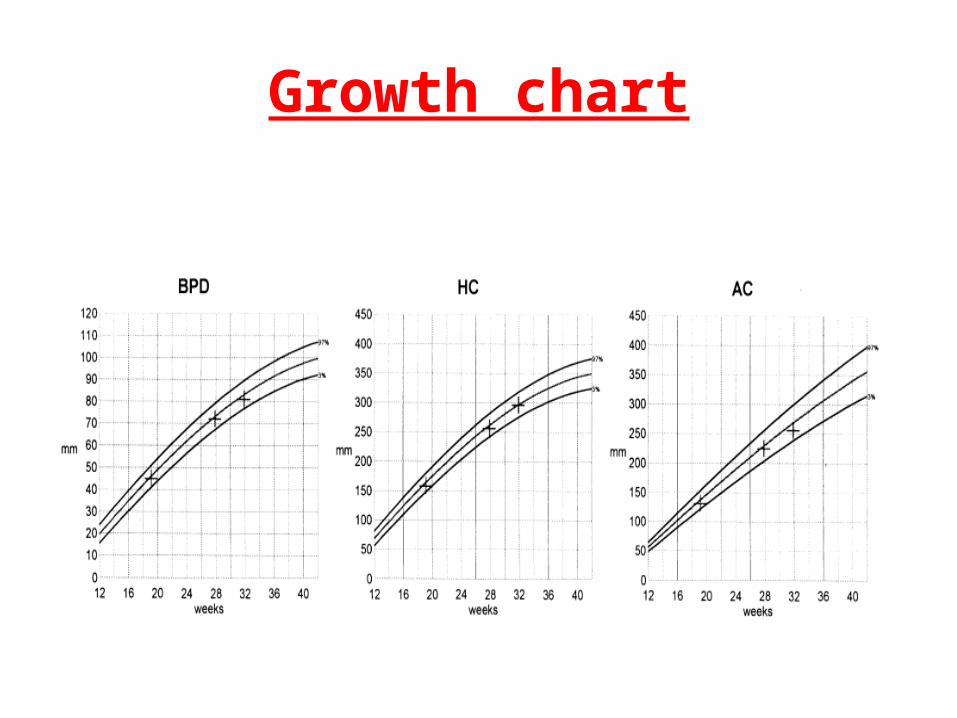
Growth chart

Placental localization

Amniotic fluid

Fetal Biophysical profileBiophysical Variable
Normal (score=2) Abnormal (score= 0)
Fetal breathing movements
1 episode FBM of at least 30 s duration in 30 min
Absent FBM or no episode >30 s in 30 min
Fetal movements
3 discrete body/limb movements in 30 min
2 or fewer body/limb movements in 30 min
Fetal tone 1 episode of active extension with return to flexion of fetal limb(s) or trunk. Opening and closing of the hand considered normal tone
Either slow extension with return to partial flexion or movement of limb in full extension Absent fetal movement
Amniotic fluid volume
1 pocket of AF that measures at least 2 cm in 2 perpendicular planes
Either no AF pockets or a pocket<2 cm in 2 perpendicular planes

Test Score Result Interpretation Management
10 of 10
8 of 10 (normal fluid)
8 of 8 (NST not done)
Risk of fetal asphyxia extremely rare
Intervention for obstetric and maternal factors
8 of 10 (abnormal fluid) Probable chronic fetal compromise
Determine that there is functioning renal tissue and intact membranes. If so, delivery of the term fetus is indicated. In the preterm fetus less than 34 weeks, intensive surveillance may be
preferred to maximize fetal maturity.
6 of 10 (normal fluid) Equivocal test, possible
fetal asphyxia
Repeat test within 24 hr
6 of 10 (abnormal fluid) Probable fetal asphyxia Delivery of the term fetus. In the preterm fetus less than 34 weeks, intensive surveillance may be preferred to maximize fetal maturity
4 of 10 High probability of fetal asphyxia
Deliver for fetal indications
2 of 10 Fetal asphyxia almost certain
Deliver for fetal indications
0 of 10 Fetal asphyxia certain Deliver for fetal indications

Umbilical Doppler Velocimetry
Indication:
IUGRPETD.M.
Any high risk pregnancyUse a free loop of umbilical cord to measure blood flow in it

Umbilical cord


Umbilical Artery Doppler

Umbilical Artery Doppler

Umbilical cord doppler

Reverse flow in umbilical artery

Management of Abnormal Doppler
Depends on:
Fetal maturity
Gestational ageObstetric history
Management of Doppler results
Reverse flow or absent end diastolic flow--- Immediate delivery
High resistance index---- repeat in few days or delivery
Normal flow---- repeat in 2 week if indicated

Assessment for Chromosomal Abnormality
Ultrasound ----- nuchal translucency (N.T)Biochemical markers ---
1st trimester---PAPPA&βHCG
AmniocentesisChorionic villus sampling

Assessment for Chromosomal Abnormality
General Facts:•The general incidence of Down is 1:1000•The risk by maternal age: at the age of 35 -----------1:365 at the age of 40-----------1:109 at the age of 45-----------1:32•Risk of recurrence is 1% ( 0.75% higher than maternal age related risk•** In case of parental aneuploidy---- 30% risk of Trisomy in offspring

Methods available for screening for chromosomal abnormality
• Maternal age• Biochemical---1st trimester---PAPPA&β HCG,
• 2nd trimester---Triple & quadruple Test
• Ultrasound NT + Other markers
• Fetal DNA

Ultrasound screening for chromosomal abnormality
•Nuchal translucency(N.T)•Skin fold thickness behind the fetal cervical spine
• Timing: 11-13 +6days weeks of pregnancy
• 75-80% of trisomy 21
• 5-10% normal karyotype ( but could be associated with cardiac defects, diaphragmatic hernia, Exomphalos)

Nuchal translucency

Amniocentesis
Obtaining a sample of amniotic fluid surrounding the fetus during pregnancy ”.
Indications:
•Diagnostic (at 11- 20 weeks)•Therapeutic( at any time)

Indications of amniocentesis:•Genetic amniocentesis:
Chromosomal analysis (Down syndrome)Chromosomal analysis (Down syndrome)Spina bifida (Alpha fetoprotein)Spina bifida (Alpha fetoprotein)Inherited diseases (muscular dystrophy)Inherited diseases (muscular dystrophy)Bilirubin level in isoimmunizationBilirubin level in isoimmunizationFetal lung maturation (L/S ratio)Fetal lung maturation (L/S ratio)
Therapeutic amniocentesis:
•Reduce maternal stress in polyhydramnios
•Mainly in twin-twin transfusion or if abnormality associated

Amniocentesis
Chorionic villus sampling
Sampling is done to the cyto-trophoblastsSampling is done to the cyto-trophoblasts
done between 10-14 weeks of pregnancydone between 10-14 weeks of pregnancy


CVS
Recommended books
Essential of obstetrics & gynecology (p 91- 119)
Current diagnosis & treatment Obstetrics & gynecology (p 203-211 & p249-258 & p 441-460)