management of infertility. introduction primary infertility: the inability to conceive after 1 year...
TRANSCRIPT

Management of Infertility

Introduction
• Primary infertility: The inability to conceive after 1 year of unprotected intercourse for a woman younger than 35, or after 6 months of unprotected intercourse for a woman 35 or older.
• Secondary infertility: The inability of a woman to conceive who previously was able to do so.
• Infertility is more common in older women. However, increased age reduces the efficacy of treatment.
Prevalence and Overview of Treatments
Approximately half of all women who receive fertility care achieve conception leading to a live birth.
Requirements for Conception
• Production of healthy egg and sperm• Unblocked tubes that allow sperm to reach
the egg• The sperms ability to penetrate and fertilize
the egg• Implantation of the embryo into the uterus• Finally a healthy pregnancy

Infertility• Reproductive age for women
– Generally 15-44 years of age– Fertility is approximately halved between 37th and
45th year due to alterations in ovulation– 20% of women have their first child after age 30– 1/3 of couples over 35 have fertility problems
• Ovulation decreases• Health of the egg declines• Health problems develop
• With the proper treatment 85% of infertile couples can expect to have a child
Causes for infertilityMale
• ETOH• Drugs• Tobacco• Health problems• Radiation/Chemotherapy• Age• Enviromental factors
• Pesticides• Lead
Female• Age • Stress• Poor diet• Athletic training• Over/underweight• Tobacco• ETOH• STD’s• Health problems
Causes of Infertility
• Anovulation (10-20%)• Anatomic defects of the female genital tract
(30%)• Abnormal spermatogenesis (40%)• Unexplained (10%-20%)

Evaluation of the Woman
• Primary evaluation components:– Male factor– Ovarian factor– Cervical factor– Tubal factor– Uterine factor
Physical Evaluation
• Obtain a complete health history of both partners
• Assess the woman’s hormone values• Perform a complete pelvic exam• Order the man’s semen analysis

Complete Pelvic Examination• Abnormalities and current pathologies are
ruled out.• Transvaginal ultrasound (TVUS): Used to
examine the uterus, endometrium, ovaries and tubes
• Sonohysteroscopy: Used to identify polyps, fibroid tumors, cysts or other intrauterine masses
• Hysterosalpingogram: Used to evaluate the interior uterus and fallopian tubes
Evaluation of Ovulatory Function
Women can use simple, noninvasive techniques to predict ovulation:
– Daily basal body temperature– Ovulation predictor kits – Salivary predictor tests
Evaluation of Ovulatory Function • TVUS: Evaluates ovarian follicle
development and quality of the endometrial lining
• Clomid Challenge Test (CCT): Assesses ovarian reserve in the older woman or the woman suspected of having early ovarian failure
Evaluation of Ovulatory Function
• Anovulation and oligoovulation:– Among the most common causes of
infertility– More common in women who:
• Have extremes of body weight• Exercise excessively• Struggle with eating disorders
Ovarian Dysfunction and Failure
•Some women fail to ovulate because they have very few or no remaining oocytes.
–Before age 40, this condition is classified as premature ovarian failure or premature menopause.
–Using a donated oocyte or embryo adoption are the only options for affected women who desire to become pregnant.

Factors that Affect Fertility
• Chronic stress related to fertility• Smoking and exposure to secondhand smoke• Excessive alcohol intake• Illicit drug use• Extreme body mass index (BMI)• Eating disorders

Evaluation of the Male
• Male factor contributes to infertility in 50 percent of infertile couples
• Evaluation begins at the initial consultation with the couple.

Evaluation of the Male• Physical examination
– Obesity– Hypothalamic or pituitary failure– Abnormalities of the testes, epididymis,
prostate penis or vas deferens– Degrees of varicocele
• Semen analysis• Endocrine and chromosomal assessment• Anatomical evaluation• Psychological factors
Fertility Treatment: Goals
• To ensure patient safety• To help a couple experience a healthy pregnancy
and birth or an alternative way to build a family• To use as little of a couple’s resources as
necessary

Fertility Treatment: Options
• Correct ovulatory dysfunction• Correct tubal or uterine abnormalities• Overcome subfertile sperm parameters• ART

Ovulation Induction: Clomiphene Citrate (Clomid, Serophene)
• The “first line” of fertility therapy• Used to treat mildly disordered ovulation and luteal-
phase insufficiency• Establish tubal patency and sperm adequacy before
use.• In appropriately selected patients, 80 percent ovulate
and 40 percent conceive with clomiphene.• Multiples rate is about 10 percent.• After 6 months, women should move on to more
aggressive therapy.

Ovulation Induction: Injectable Gonadotropins
• Used:– When women exhibit resistance to
clomiphene – When multiple oocytes are desirable to
ovulate– With IVF and creation of donor oocytes and
embryos– With ovulation induction (OI)
• Multiple pregnancy rates as high as 40 percent.

Ovulation Induction: Pulsatile Gonadotropin-Releasing Hormone
• Anovulation may be due to the failure of the hypothalamus to provide sufficient stimulation to the pituitary gland.
• Gonadotropin-releasing hormone (GnRH) can be directly administered via a small medication pump to induce ovulation.
• The ideal patient is the hypogonadotropic woman.

Ovulation Induction: Pulsatile GnRH
• Overall ovulation rates are between 50 percent and 80 percent. The chance of pregnancy is 10 percent to 30 percent per ovulatory cycle, depending on the couple’s other fertility factors.
• The risk of multiples is low.

Artificial Insemination
• Used to treat:– Male-factor infertility – Retrograde ejaculation– Neurologic impotence – Sexual dysfunction
• Sperm used for insemination may be the male partner’s or donated.
Artificial Insemination
• Methods of insemination– Intracervical insemination (ICI) – Intrauterine insemination (IUI)
• Success rates vary from 6 percent to 24 percent per cycle

Assisted Reproduction
• Assisted hatching of the embryo
Images provided by author. Reprinted with permission. (Figure 8)
Assisted Reproduction
• Indications for ART:– Tubal disease– Male-factor infertility– Endometriosis– Premature ovarian failure– Polycystic ovarian syndrome– Immunologic infertility– Unexplained infertility
Assisted Reproduction
• IVF: Placing the gametes and subsequent embryo into the uterus
• ZIFT (zygote intrafallopian transfer): Placing the gametes and subsequent embryo into the fallopian tubes
• GIFT (gamete intrafallopian transfer): Placing the unfertilized oocyte and sperm into the fallopian tube
Assisted Reproduction
• Stimulation type, dosage and duration depends on patient characteristics, diagnoses and the fertility center.
• Monitoring is usually by serial TVUS, usually over four to five visits.
Assisted Reproduction
• Cleavage of the embryos and other subjective indicators of embryo health help the clinician decide timing and number of embryos to transfer.
• The usual timing of transfer of embryos is on day 3, 4 or 5 after retrieval.
Assisted Reproduction: Cryopreservation
• Freezing, thawing and using:– Sperm– Embryos– Oocytes
Pre-implantation Genetic Diagnosis
• Used only with IVF• One or two cells removed from the embryo
and analyzed for defects before transfer to the uterus

Pre-implantation Genetic Diagnosis
• May be helpful for:– Women older than 35 years– Couples who have experienced recurrent
pregnancy loss – Couples with one partner known to carry a
balanced chromosomal translocation• Up to 85 percent accurate for detecting the
most common chromosomal abnormalities

Third-party Reproduction
• Donor gametes • Donor embryos • Surrogacy
– Gestational carrier: Carries other people’s oocyte and sperm
– Traditional surrogate: Inseminated with the male partner’s sperm
ART Risks and Complications
• Ovarian hyperstimulation syndrome (OHHS)• Multiple gestation

Male-factor Infertility
• ART may help men with:– Sperm counts between 1 and 10 million with
poor motility and morphology scores– Failed previous inseminations– Obstructive or nonobstructive azoospermia
where sperm can be successfully extracted from the epididymis or testes
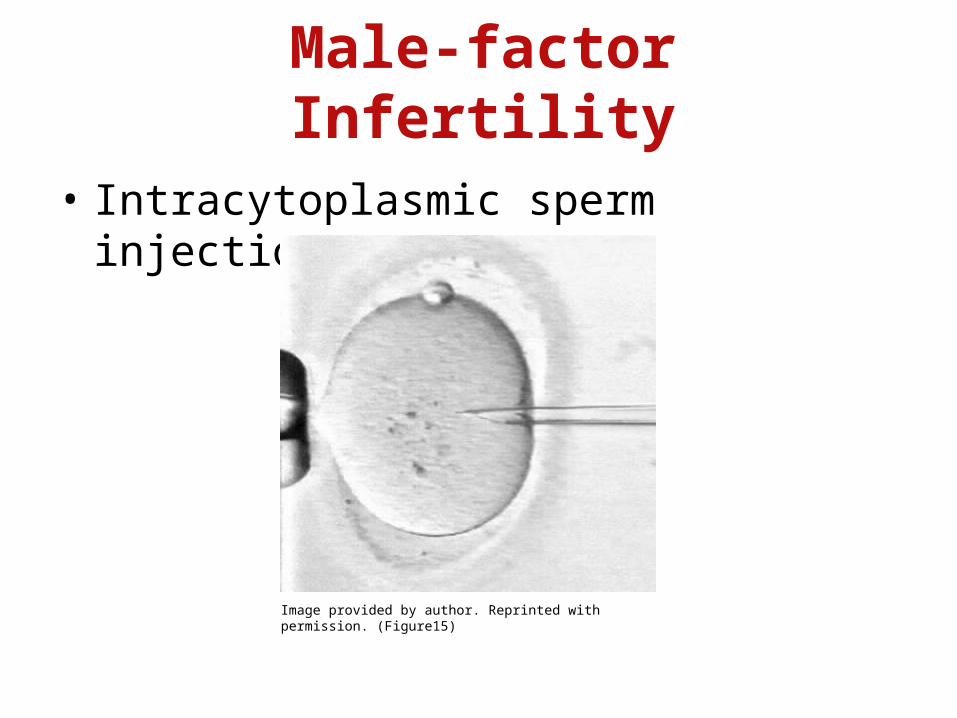
Male-factor Infertility
• Intracytoplasmic sperm injection (ICSI)
Image provided by author. Reprinted with permission. (Figure15)