management of eczema - kenya paediatric...
TRANSCRIPT

Management Of Eczema
GICHINA M. B.MB ChB, MMed Paeds - Nairobi, MSc Derm – London.
CONSULTANT PAEDIATRICIAN AND DERMATOLOGIST
DFMH

DefinitionImpactClinical featuresDiagnosisDifferential diagnosisTreatment

Improve your ability to accuratelydiagnose and manage 90% cases ofAD.Recognize differences in infant,
childhood and adult presentations ofAD Improve ability to diagnose
conditions sometimes confused withAD

A chronic, relapsinginflammatory skin diseasecharacterized by dryness anditching.AD, CD, LSC, discoid, stasis,NP.


Aetiology- unknownFamily studies support a genetic basis.
70%.The mode of inheritance appears
complexEvidence points to AD being due to a
primary barrier defect (filaggrin protein)with inflammation being a secondaryphenomena.
Filaggrins (filament aggregating protein)proteins which bind to keratin fibers in S.Corneum.Hydration and pH regulation of the s.
corneum Mutations in the gene coding for
filaggrin are predisposed to dry skin,ichthyosis vulgaris, and eczema

(Charlesworth, Am J Med, 2002)

IrritantsWoolSoaps/detergentsDisinfectants“Occupational”Tobacco smoke
Microbial agentsStaph aureus, strepViral infectionDermatophytes
Environmental .House dust mites
Aeroallergens -sprays, perfumesClimate
Heat/Sweating,humidityStress
physical, mentalor social stress
Triggers; social, environmental, and biological.

Prevalence 15-25% children. 3%85% of pts develop AD by age 5. 60%.15% Mod to severe - profound effect on
QOL4-6% of adults.40-60% have allergic rhinitis/asthma.
*adapted from Laughter D. J Am Acad Dermatol 2000; 43:649-55.
2



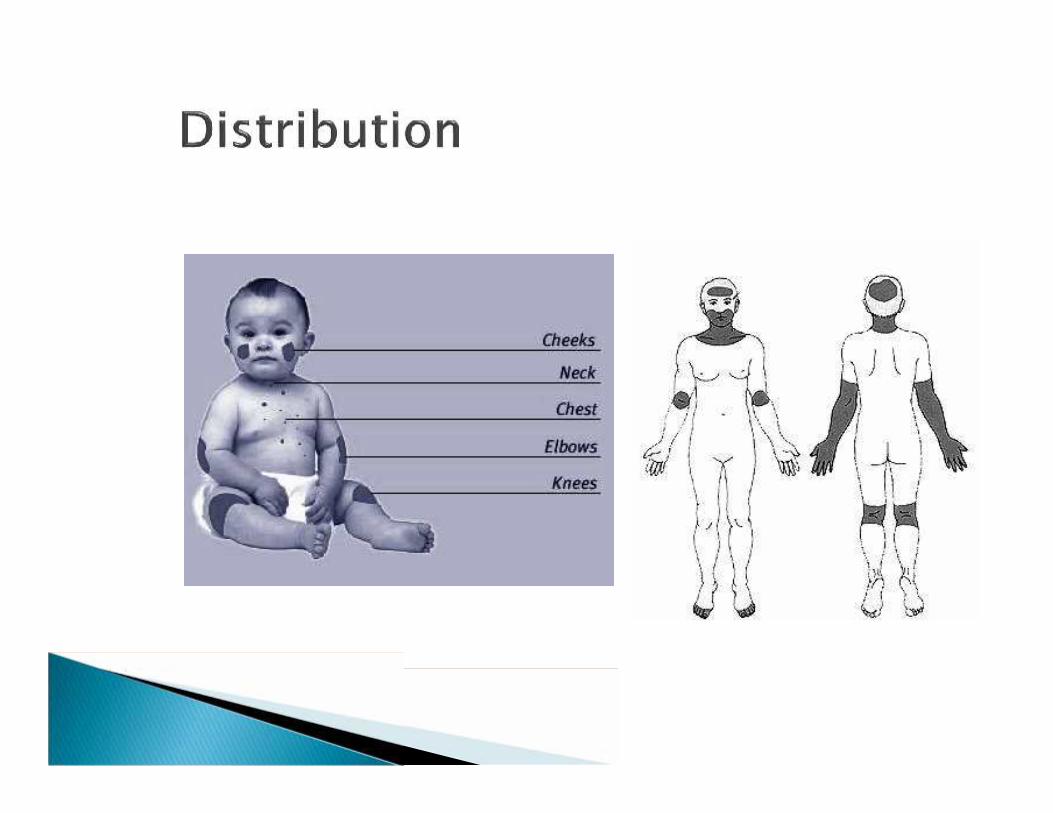
In infants, the face is often affected first,then the hands and feet; dry red patchesmay appear all over the body.In older children, the skin folds are
most often affected, especially the elbowcreases and behind the knees.In adults, the face and hands are more
likely to be involved.
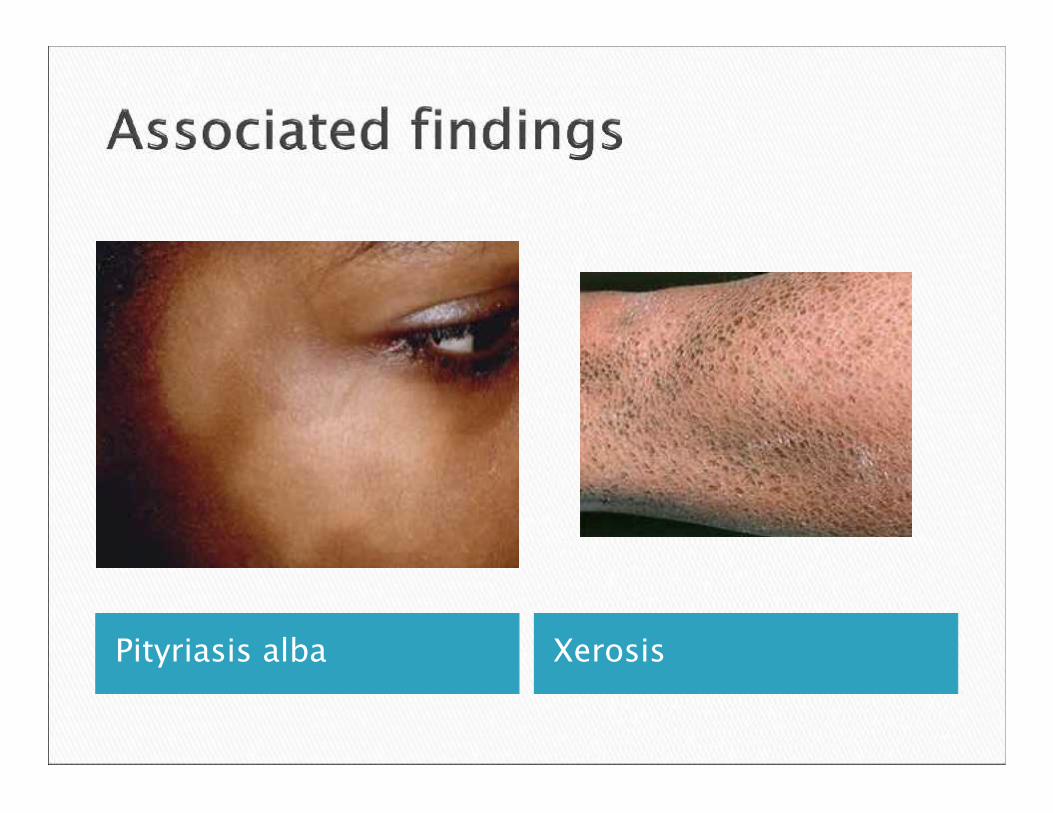
Pityriasis alba Xerosis

Keratosis pilaris Ichthyosis

Children:Moderate-Severe AD have (33% transient) clinically
significant food allergyIncreasing severity of AD ~ increasing risk
of food allergy Adults:Low incidence (<2%)
Foods responsible (~85% of cases):Outgrown: Milk, egg, soy, wheatPersistent: Peanut, nuts, fish, shellfish

Laboratory studiesSpecific IgE -ONLY if clinically indicated!Skin prick testing
Clinical evaluation:Elimination dietsOral food challenges
Physician supervisedOpen, single blind, double-blind,
placebo controlled

Major features;Itchy skin condition in the last yearPlus three or more of the following: Eruption in a typical age-appropriate distributionVisible flexural dermatitisHistory of flexural involvementHistory of generally dry skinPersonal history of atopic disease†
Onset below the age of 2†children under 4 years family history of atopic disease*Mainly clinical.. No need of biopsy, RAST and the allergy tests unless in
severe dse.
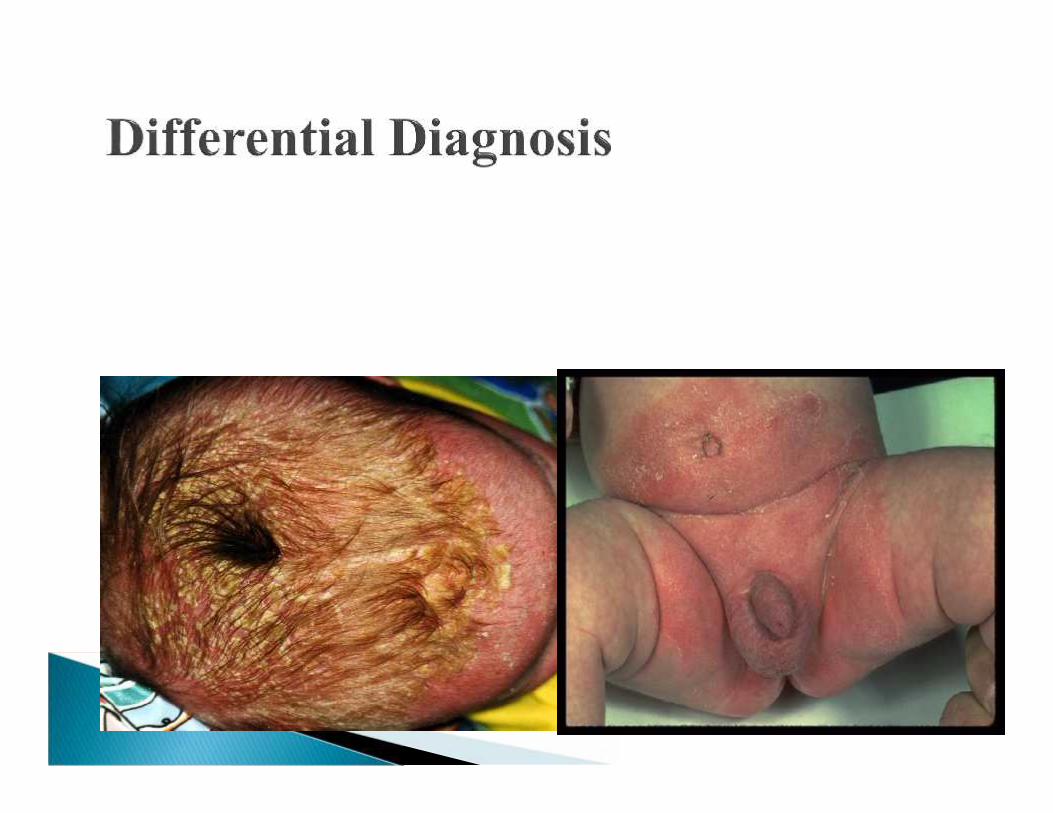

Seborrheic dermatitis
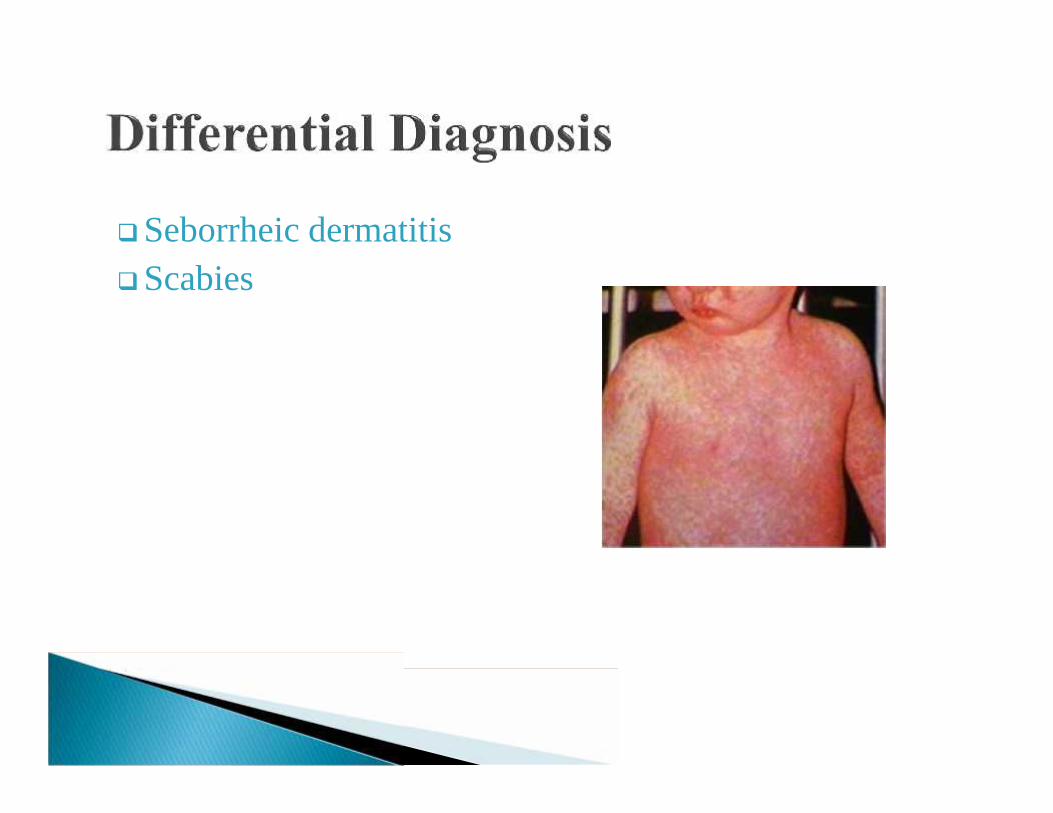
Seborrheic dermatitisScabies
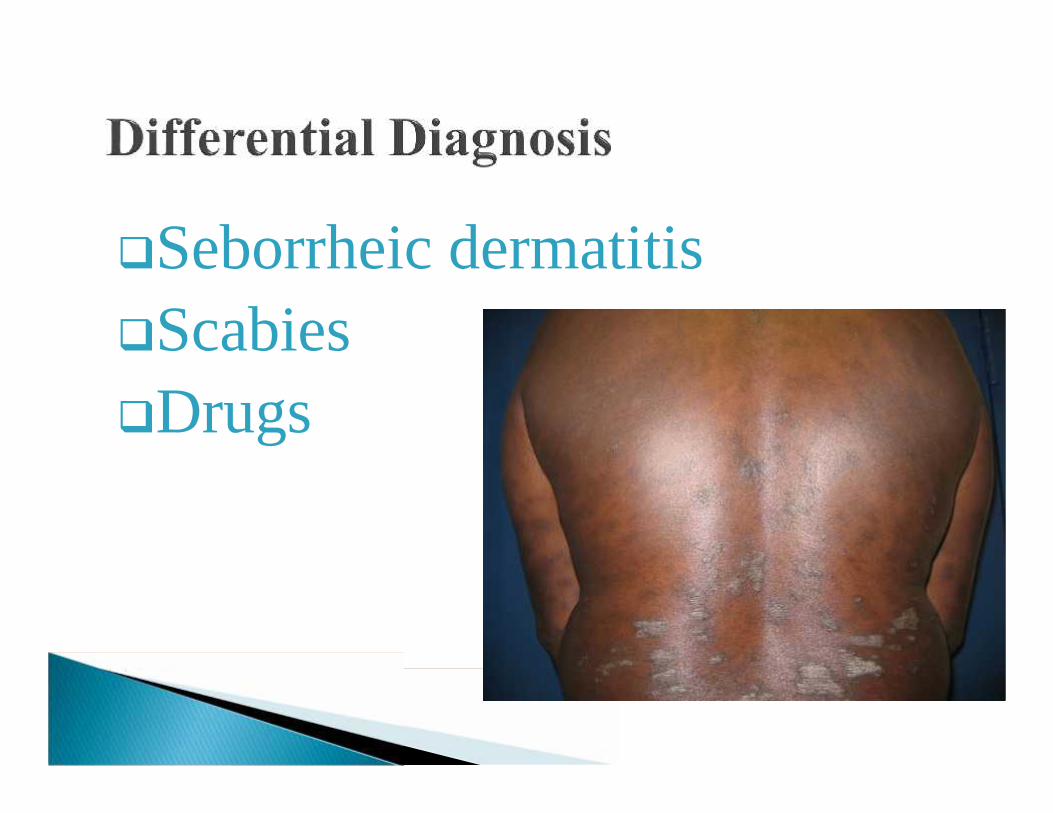
Seborrheic dermatitisScabiesDrugs
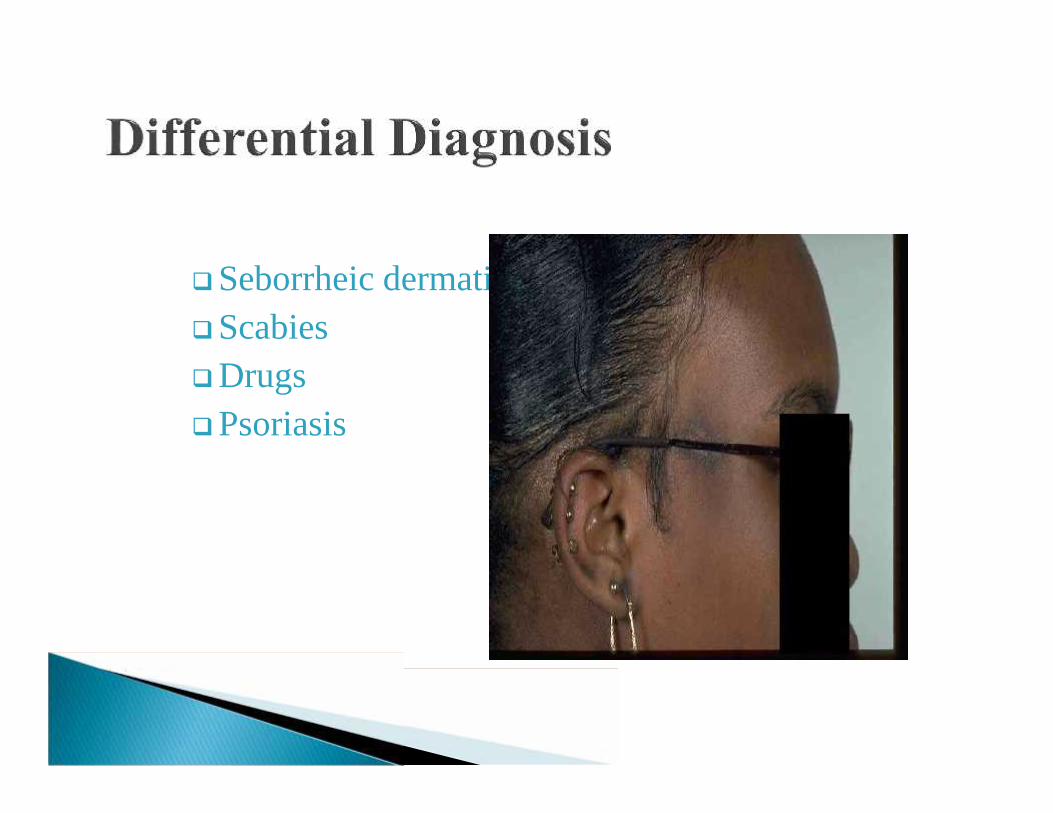
Seborrheic dermatitisScabiesDrugsPsoriasis

Seborrheic dermatitisScabiesDrugsPsoriasisAllergic contact
dermatitisCutaneous T-cell
lymphoma

No cure but AIM:control of symptoms,improve QOL
General and specificpalliative measures

Irritants Hot water Lukewarm baths Dust Rough fibres Detergents, cosmetics,
soaps Gloves for chemicals
Allergens HDM Moulds Grass pollen Pets dander
Special diets will not help most individuals b/c little evidence that food is majorculprit.
Key adjuvant. Moisturize, moisturize,
moisturize Soften, hydrates and reduce itch. Ointments> Creams > lotions Ct in maintenance when no
longer inflamed Apply liberally -250-500g/week. Apply immediately after bath. V need for cts. Many times daily.
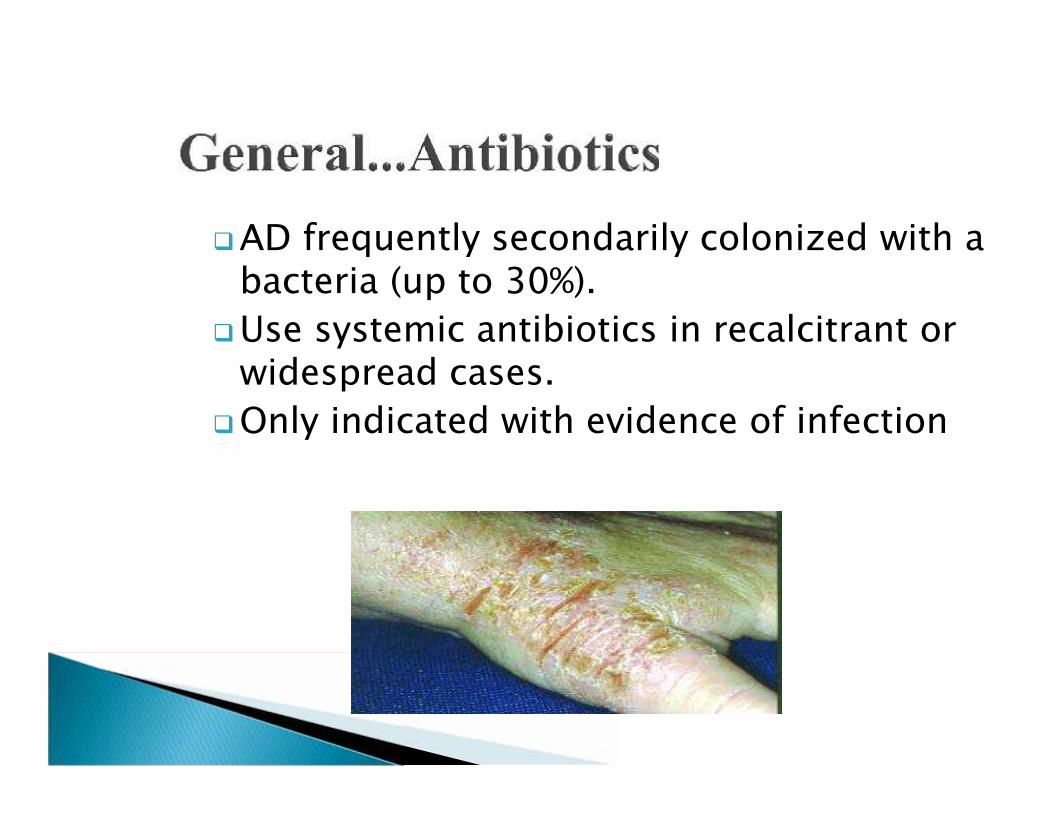
AD frequently secondarily colonized with abacteria (up to 30%).
Use systemic antibiotics in recalcitrant orwidespread cases.
Only indicated with evidence of infection

Reduce urticaria & itchNon-sedating less sideeffects but more expensiveSedative effect ofhydroxyzine &diphenhydramine helpful1st generation > 2nd

Topical cts- Mainstay.Ointments for dry or lichenified skinCreams for weeping skin or body
folds.Lotions for hairy -areas.Considerations - age, site, severity
and potencyStrengths . OD

•Dermovate
Ultrapotent
•Elocon, cutivatePotent
•Eumovate, betamethasoneModeratelypotent
•1% Hydrocortisone
Mildly potent

Second lineTacrolimus / pimecrolimusMild to moderate eczemaSteroid sensitive areas.Steroid fear.Transient stinging possible.Cost higher cc potency steroids.
(Ruzicka, N Engl J Med, 1997)

Severe disease
NbUVB, UVB, UVA PUVA
Can help delay need for systemic therapy.
Useful in skin type V/VI, severe disease.
Systematic review showed benefit (Meduri et al)
Relapse can be quick

Severe flareup diseaseExplore reason for treatment failure. Do
baselines before initiating. Corticosteroids; Systemic: a short course suppress acute
flare-ups. Intra-lesional steroids : plaques not responding totopical agents
Cyclosporine (off label)AZAMTXMMF

Filaggrin technology.
Biologics been tested off-label as a potential therapy
for severe AD

When the diagnosis is uncertainFailed response to appropriate therapyIf treatment of the face or skin folds with
high potency TCS is being contemplatedIf treatment with systemic
immunosuppressive agents is beingconsidered

There is evidence that for infants at high risk ofdeveloping atopy, breastfeeding for at least 4 monthsor breastfeeding with supplements of hydrolyzedinfant formula decreases the risk of eczema and cowmilk allergy in the first 2 years of life.
There is modest evidence that the onset of atopicdisease may be delayed or prevented by the use ofhydrolyzed formulas compared with formula madewith intact cow milk protein.
Effects of Early Nutritional Interventions on the Development of Atopic Disease in Infants and Children: The Role of Maternal DietaryRestriction, Breastfeeding, Timing of Introduction of Complementary Foods, and Hydrolyzed Formulas PEDIATRICS Volume 121, Number 1,January 2008

Educate parents thatThe goal isCONTROL not CURE
