management of clozapine cardiotoxicity with
TRANSCRIPT
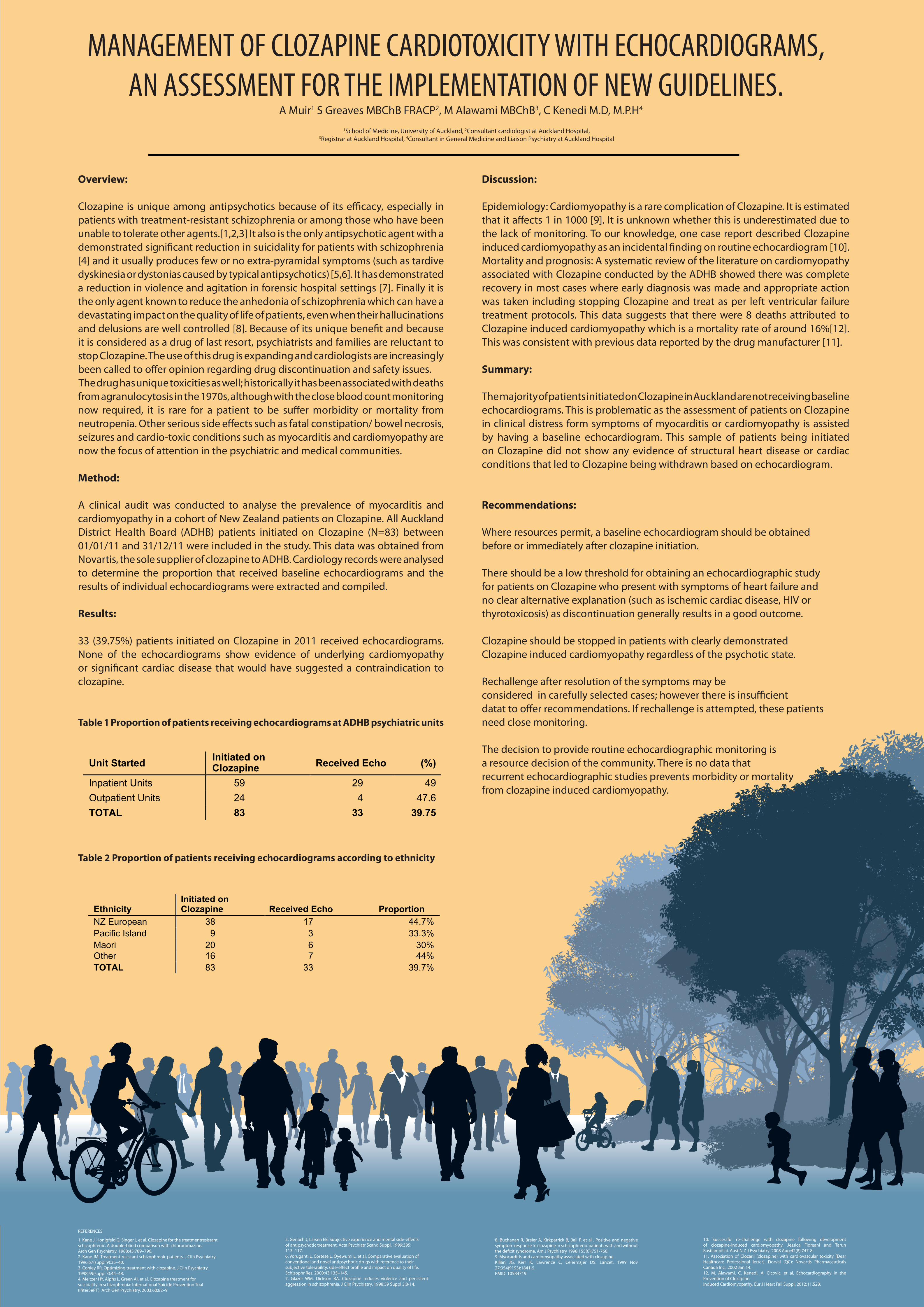
Overview:
Clozapine is unique among antipsychotics because of its efficacy, especially in patients with treatment-resistant schizophrenia or among those who have been unable to tolerate other agents.[1,2,3] It also is the only antipsychotic agent with a demonstrated significant reduction in suicidality for patients with schizophrenia [4] and it usually produces few or no extra-pyramidal symptoms (such as tardive dyskinesia or dystonias caused by typical antipsychotics) [5,6]. It has demonstrated a reduction in violence and agitation in forensic hospital settings [7]. Finally it is the only agent known to reduce the anhedonia of schizophrenia which can have a devastating impact on the quality of life of patients, even when their hallucinations and delusions are well controlled [8]. Because of its unique benefit and because it is considered as a drug of last resort, psychiatrists and families are reluctant to stop Clozapine. The use of this drug is expanding and cardiologists are increasingly been called to offer opinion regarding drug discontinuation and safety issues. The drug has unique toxicities as well; historically it has been associated with deaths from agranulocytosis in the 1970s, although with the close blood count monitoring now required, it is rare for a patient to be suffer morbidity or mortality from neutropenia. Other serious side effects such as fatal constipation/ bowel necrosis, seizures and cardio-toxic conditions such as myocarditis and cardiomyopathy are now the focus of attention in the psychiatric and medical communities.
Method:
A clinical audit was conducted to analyse the prevalence of myocarditis and cardiomyopathy in a cohort of New Zealand patients on Clozapine. All Auckland District Health Board (ADHB) patients initiated on Clozapine (N=83) between 01/01/11 and 31/12/11 were included in the study. This data was obtained from Novartis, the sole supplier of clozapine to ADHB. Cardiology records were analysed to determine the proportion that received baseline echocardiograms and the results of individual echocardiograms were extracted and compiled.
Results:
33 (39.75%) patients initiated on Clozapine in 2011 received echocardiograms. None of the echocardiograms show evidence of underlying cardiomyopathy or significant cardiac disease that would have suggested a contraindication to clozapine.
Table 1 Proportion of patients receiving echocardiograms at ADHB psychiatric units
Table 2 Proportion of patients receiving echocardiograms according to ethnicity
MANAGEMENT OF CLOZAPINE CARDIOTOXICITY WITH ECHOCARDIOGRAMS, AN ASSESSMENT FOR THE IMPLEMENTATION OF NEW GUIDELINES.
Discussion:
Epidemiology: Cardiomyopathy is a rare complication of Clozapine. It is estimated that it affects 1 in 1000 [9]. It is unknown whether this is underestimated due to the lack of monitoring. To our knowledge, one case report described Clozapine induced cardiomyopathy as an incidental finding on routine echocardiogram [10].Mortality and prognosis: A systematic review of the literature on cardiomyopathy associated with Clozapine conducted by the ADHB showed there was complete recovery in most cases where early diagnosis was made and appropriate action was taken including stopping Clozapine and treat as per left ventricular failure treatment protocols. This data suggests that there were 8 deaths attributed to Clozapine induced cardiomyopathy which is a mortality rate of around 16%[12]. This was consistent with previous data reported by the drug manufacturer [11].
Summary:
The majority of patients initiated on Clozapine in Auckland are not receiving baseline echocardiograms. This is problematic as the assessment of patients on Clozapine in clinical distress form symptoms of myocarditis or cardiomyopathy is assisted by having a baseline echocardiogram. This sample of patients being initiated on Clozapine did not show any evidence of structural heart disease or cardiac conditions that led to Clozapine being withdrawn based on echocardiogram.
Recommendations:
Where resources permit, a baseline echocardiogram should be obtained before or immediately after clozapine initiation.
There should be a low threshold for obtaining an echocardiographic study for patients on Clozapine who present with symptoms of heart failure and no clear alternative explanation (such as ischemic cardiac disease, HIV or thyrotoxicosis) as discontinuation generally results in a good outcome.
Clozapine should be stopped in patients with clearly demonstrated Clozapine induced cardiomyopathy regardless of the psychotic state.
Rechallenge after resolution of the symptoms may be considered in carefully selected cases; however there is insufficient datat to offer recommendations. If rechallenge is attempted, these patients need close monitoring.
The decision to provide routine echocardiographic monitoring is a resource decision of the community. There is no data that recurrent echocardiographic studies prevents morbidity or mortality from clozapine induced cardiomyopathy.
1. Kane J, Honigfeld G, Singer J, et al. Clozapine for the treatmentresistantschizophrenic. A double-blind comparison with chlorpromazine.Arch Gen Psychiatry. 1988;45:789–796.2. Kane JM. Treatment-resistant schizophrenic patients. J Clin Psychiatry.1996;57(suppl 9):35–40.3. Conley RR. Optimizing treatment with clozapine. J Clin Psychiatry.1998;59(suppl 3):44–48.4. Meltzer HY, Alphs L, Green AI, et al. Clozapine treatment forsuicidality in schizophrenia: International Suicide Prevention Trial(InterSePT). Arch Gen Psychiatry. 2003;60:82–9
REFERENCES
5. Gerlach J, Larsen EB. Subjective experience and mental side-effectsof antipsychotic treatment. Acta Psychiatr Scand Suppl. 1999;395:113–117.6. Voruganti L, Cortese L, Oyewumi L, et al. Comparative evaluation ofconventional and novel antipsychotic drugs with reference to theirsubjective tolerability, side-effect profile and impact on quality of life.Schizophr Res. 2000;43:135–145.7. Glazer WM, Dickson RA. Clozapine reduces violence and persistent aggression in schizophrenia. J Clin Psychiatry. 1998;59 Suppl 3:8-14.
8. Buchanan R, Breier A, Kirkpatrick B, Ball P, et al . Positive and negative symptom response to clozapine in schizophrenic patients with and without the deficit syndrome. Am J Psychiatry 1998;155(6):751-760.9. Myocarditis and cardiomyopathy associated with clozapine.Kilian JG, Kerr K, Lawrence C, Celermajer DS. Lancet. 1999 Nov 27;354(9193):1841-5.PMID: 10584719
10. Successful re-challenge with clozapine following development of clozapine-induced cardiomyopathy. Jessica Floreani and Tarun Bastiampillai. Aust N Z J Psychiatry. 2008 Aug;42(8):747-8.11. Association of Clozaril (clozapine) with cardiovascular toxicity [Dear Healthcare Professional letter]. Dorval (QC): Novartis Pharmaceuticals Canada Inc.; 2002 Jan 14.12. M. Alawami, C. Kenedi, A. Cicovic, et al. Echocardiography in the Prevention of Clozapineinduced Cardiomyopathy. Eur J Heart Fail Suppl. 2012;11,S28.
Unit Started Initiated on Clozapine Received Echo (%)
Inpatient Units 59 29 49 Outpatient Units 24 4 47.6 TOTAL 83 33 39.75
Ethnicity Initiated on Clozapine Received Echo Proportion
NZ European 38 17 44.7% Pacific Island 9 3 33.3% Maori 20 6 30% Other 16 7 44% TOTAL 83 33 39.7%
Unit Started Initiated on Clozapine Received Echo (%)
Inpatient Units 59 29 49 Outpatient Units 24 4 47.6 TOTAL 83 33 39.75
Unit Started Initiated on Clozapine Received Echo (%)
Inpatient Units 59 29 49 Outpatient Units 24 4 47.6 TOTAL 83 33 39.75
Ethnicity Initiated on Clozapine Received Echo Proportion
NZ European 38 17 44.7% Pacific Island 9 3 33.3% Maori 20 6 30% Other 16 7 44% TOTAL 83 33 39.7%
Ethnicity Initiated on Clozapine Received Echo Proportion
NZ European 38 17 44.7% Pacific Island 9 3 33.3% Maori 20 6 30% Other 16 7 44% TOTAL 83 33 39.7%
A Muir1 S Greaves MBChB FRACP2, M Alawami MBChB3, C Kenedi M.D, M.P.H4
1School of Medicine, University of Auckland, 2Consultant cardiologist at Auckland Hospital, 3Registrar at Auckland Hospital, 4Consultant in General Medicine and Liaison Psychiatry at Auckland Hospital