management of asymptomaticmanagement of ...universe-syllabi.gi.org/acg2011_32_slides.pdf1 management...
TRANSCRIPT

1
Management of AsymptomaticManagement of Asymptomatic Pancreatic Cysts
Manoop S. Bhutani, MD, FACG, FASGE, FACP, AGAF
Professor, Gastroenterology, Hepatology and NutritionUT MD Anderson Cancer Center, Houston, Texas
Why Asymptomatic pancreatic cysts are important for us?
■ Clinical dilemma
■ High prevalence
1% of patients undergoing abdominal CT scan have a cystic lesion in the pancreas
■ Clinical dilemma
Mucinous vs Non-mucinousBenign vs Premalignant or
Malignant

2
Classification
No epithelium Pseudocyst
Serous epithelium
Degenerative h i lid
y
Mucinous epitheliumMucinous cystic neoplasm
epitheliumSerous cystic neoplasm
Squamous epitheliumL h ith li
change in solid tumorCystic ductal adenocarcinomaCystic neuroendocrine tumorcystic neoplasm
Intraductalpapillary mucinous neoplasm
Lymphoepithelial cyst
tumorCystic acinar cell carcinoma
Serous Cystic Neoplasm (SCN)
F>M
6th decade
Sex
Age 6 decadeAge
Anywhere Location
Multicystic/honeycomb appearance.Central scar and calcification.
Morphology/imaging
Glycogen-rich cuboidal cells lining cystic spaces and amorphous stroma.PAS stain (+)
Histopathology
Generally Benign
Malignancy potentialThirabanjasak D, et al. Pancreatology 2009.

3
Varieties of SCNMicrocystic SCN Oligocystic SCN
F (95%)>>M
4th 5th decade
Sex
Age
Mucinous Cystic Neoplasm (MCN)
4th , 5th decadeAge
Body (tail) Location
Unilocular or septatedcyst +/- wall calcifications.MPD communication (-)
Morphology/imaging
Variable cellular atypiaand secretes mucin with ovarian-like stroma.
Histopathology
Yes Malignancy potentialTanaka M, et al. Pancreatology 2006.

4
Varieties of MCN
M (70%) > FSex
Intraductal Papillary Mucinous Neoplasms (IPMN)
6th and 7th decadeAge
HeadLocation
Dilated main duct or pancreatic ductbranches.
Morphology/imaging branches.Solid component (+) →malignancy?
YesMalignancy potential

5
Intraductal Papillary Mucinous Neoplasms (IPMN)
Mucinous secretion
Fish-mouth appearance
MAIN DUCT IPMN
IPMN
Risk factors for malignancy
■Old■Older age
■Presence of symptoms
■Involvement of main pancreatic duct
■Dilation of main pancreatic duct
■Mural nodule
■Size >30mm (side branch type)
6
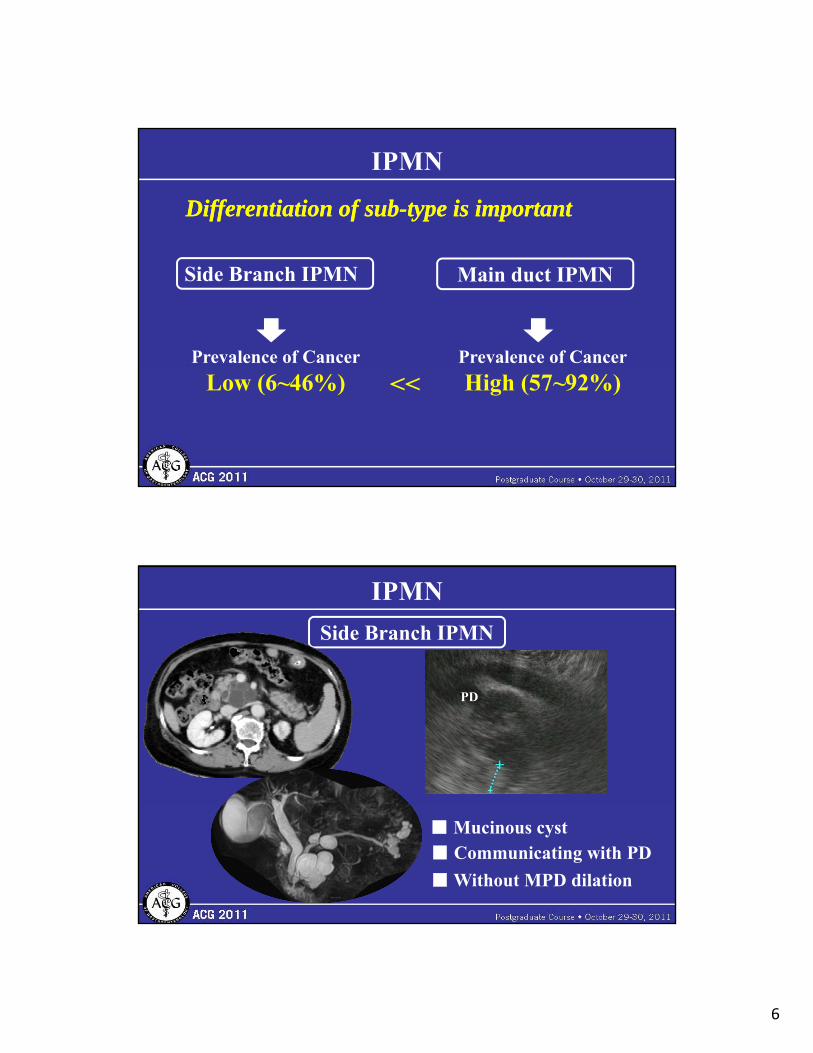
IPMN
Differentiation of subDifferentiation of sub--type is important type is important
Side Branch IPMN Main duct IPMN
Prevalence of Cancer Prevalence of Cancer
Low (6~46%) High (57~92%)<<
IPMN
Side Branch IPMN
PD
■ Mucinous cyst■ Communicating with PD
■ Without MPD dilation

7
IPMN
Main duct IPMN
MPD
■ Mucinous cyst■ Dilation of PD (>10mm)
Mucinous cystic neoplasms
Differentiation is important for managementDifferentiation is important for managementCharacreristic MCN Branch duct IPMN
Gender (% female)
Age (decade)
Location (% body/tail)
Common capsule
Calcification
Gross appearance
>95%
4th and 5th
95%
Yes
Rare, curvilinear, in the wall of cyst
Orange-like
~30%
6th and 7th
~30%
No
No
Grape-like
Ovarian-type stroma Positive (76%) Negative
Tanaka M, et al. Pancreatology 2006.
Internal structure
Pancreatic duct communication
Cyst in cyst
Infrequent
p
Cyst by cyst
YesMain pancreatic duct Normal or deviated Normal

8
Imaging diagnosis
■ Computed Tomography (CT)
■ Magnetic Resonance Image (MRI)
■ Endoscopic Ultrasound (EUS)p ( )
Imaging diagnosis -CT-
■ Typical characterization on CT scanS h i DV t l R di l 2006
Unilocular Macrolocular MicrolocularSahani DV, et al. Radiology 2006.
Pseudocyst IPMN, MCN SCA

9
Imaging diagnosis -MRI-
■ Communication with pancreatic duct: IPMN■ Communication with pancreatic duct IPMN
■ Presence of central scar: SCN
MRI may be a feasible tool for surveillance without radiation exposure.
Imaging diagnosis
■ Specific diagnosisp g
CT: Accuracy 61.9 to 76.2%
MRI: Accuracy 55.6% to 76.2%
CT+MRI: Accuracy 73.0% to 77.8% (Lee HJ et al Clinical Radiol 2011)(Lee HJ, et al. Clinical Radiol 2011)

10
Imaging diagnosis -EUS imaging-
HighHigh--resolution images resolution images
Gress F, et al. Am J Gastroenterol 1997.
Koito K, et al. Gastrointest Endosc 2006.
EUS classificationThick wall type Tumor protruding type Thick septal type
Micro cystic type Micro cystic typeThin septa type Simple type
Koito K, et al. Gastrointest Endosc 2006.

11
Imaging diagnosis -EUS imaging-
■ Benign vs Malignant
■ Mucinous vs Non-Mucinous
Accuracy 40% to 93%Accuracy 40% to 93%
Accuracy 51%Accuracy 51%
Thick wallSeptationIntramural nodule/Mass (Ahmad NA, et al. Gastrointest Endosc 2003)
■ Mucinous vs Non Mucinous Accuracy 51% Accuracy 51%
EUS Imaging without FNA not enough as an independent predictor.
Brugge WR, et al. Gastroenterology 2004
Imaging diagnosis -EUS imaging
Cystic fluid analysis with EUSCystic fluid analysis with EUS--FNAFNACystic fluid analysis with EUSCystic fluid analysis with EUS--FNAFNA
■Cytology
■Biochemistry
■Viscosity
■Tumor markers
y
■DNA and others

12
Cystic fluid analysis-Cytology-
■ Mucinous versus non mucinous■ Mucinous versus non-mucinous
■ Mucinous vs Non-Mucinous
Accuracy 59 %
(Thosani N, et al. Dig Dis Sci 2010)
Brugge WR, et al. Gastroenterology 2004.
( , g )
Systemic review and meta-analysis of 11 studiesSensitivity 63 %, Specificity 88%
■ Indirect measurement of mucin, glycoprotein, DNA
Cystic fluid analysis-Viscosity-
contents
■ Viscosity≧1.6 is highly suggestive for mucinous lesion
Brugge WR, et al. Gastroenterology 2004
Linder JD, et al. Gastroenterol Endosc 2006.
Predicted cyst Cyst fluid analysis formula Sensitivity Specificity Accuracy
PC
SCyA
MCyA
MCyA-CA
VIS<1.6 or lipase UL>6000 and CEA ng/ml <480VIS<1.6 and lipase UL<6000
VIS≧1.6 and CEA ng/ml <6000
VIS≧1.6 and CEA ng/ml ≧6000
91.3
100
85.7
100
100
100
100
92
97.2
100
97.2
94.3

13
■ String sign:
Cystic fluid analysis-Viscosity-
■ String sign:
Non-mucinous 0 mm vs Mucinous 3.5 mm (median)Leung KK, et al. Ann Surg Oncol 2009
CPC Study
Cystic fluid analysis-CEA-
C C Study
(Cooperative Pancreatic Cyst Study)
■ Prospectively enrolled 371 patients
■ Histopathology was gold standard
Brugge WR, et al. Gastroenterology 2004.
p gy g
■ EUS, cytology and various fluid tumor markers were evaluated.

14
CPC Study
Cystic fluid analysis--
Receiver operator curve
Sensitivity 73%Specificity 84%
Mucinous vs Non-Mucinous p
analysis of the tumor markers demonstrated that cyst fluid CEA (optimal cutoff of 192 ng/mL) demonstrated the greatest area under the
Accuracy 79%curve (0.79) for differentiating mucinous vs. nonmucinous cystic lesions
Cystic fluid analysis-CEA-
• Pooled analysis of 12 studies, 450 patients.C t ith l t ti 250 U/L• Cysts with an amylase concentration <250 U/L were SCA, MCA, or MCAC (sensitivity 44%, specificity 98%) and, thus, virtually excluded PC.
• A carcinoembryonic antigen (CEA) <5 ng/mL suggested a SCA or PC (sensitivity 50%, specificity 95%)
Van der Waaij LA, et al. Gastrointest Endosc 2005.
95%). • CEA >800 ng/mL strongly suggested MCA or MCAC
(sensitivity 48%, specificity 98%).

15
Cystic fluid analysis-DNA Quantification and Allelic Loss-
PANDA Study
■ 391 patients (Final cohort was 113)
■ Mucinous vs Non-Mucinous
■ Prospective, multicenter trial
■ Malignant vs Pre-malignant
Khalid A, et al. Gastrointest Endosc 2009.
PANDA STUDY
• The study cohort consisted of 113 patients with 40 malignant, 48 premalignant, and 25 benign cysts.premalignant, and 25 benign cysts.
• Cyst fluid k-ras mutation was helpful in the diagnosis of mucinous cysts (odds ratio 20.9, specificity 96%).
• Components of DNA analysis detecting malignant cysts included allelic loss amplitude over 82% (AUC 0.9) and high DNA amount (optical density ratio >10, AUC 0.79). The criteria of a high amplitude k-rasmutation followed by allelic loss showed maximum specificity (96%)mutation followed by allelic loss showed maximum specificity (96%) for malignancy.
• All malignant cysts with negative cytologic evaluation (10/40) could be diagnosed as malignant by using DNA analysis.

16
DNA analysis to the rescue!
Cystic fluid analysis-DNA Quantification and Allelic Loss-
y
1
23
456
Pathological findings
IPMC-NI
MCACLiver met
IPMC-IIPMC-NIIPMC-NI
ALA% if >82%
Yes
Yes
Yes
OD if >10
YesYesYesYes
Cycle threshold value if <25
YesYes
K-ras followed by allelic loss
Yes
Yes
Yes
(Adapted from Ref. 24)
78
9
10
IPMC-NIIPMC-NI
IPMC-NI
IPMC-I
YesYes
Yes
Yes
Yes
Yes
YesYes Yes
The most important clinical tools areThe most important clinical tools are
ACG Guidelines
■ Cross sectional imaging
■ Endoscopic ultrasound
■ Cystic fluid analysis
The most important differential isThe most important differential isThe most important differential is The most important differential is
Mucinous or Non-Mucinous
Khalid A, et al. Am J Gastroenterol 2007.

17
Management
Cost effectiveness for asymptomatic pancreatic cyst Cost effectiveness for asymptomatic pancreatic cyst 26)26)
■ Strategy 2: an aggressive surgical intervention
■ Strategy 1: no specific intervention
■ Strategy 3: EUS-guided FNA with cystic fluid analysis
Compared them in Markov-based clinical model
Das A, et al. Gastrointest Endosc 2009.
Management
Cost effectiveness for asymptomatic pancreatic cyst Cost effectiveness for asymptomatic pancreatic cyst
A strategy based on risk stratification of malignant potential by EUS-guided FNA and cyst fluid analysis is thecyst fluid analysis is the most cost-effective strategy.
Das A, et al. Gastrointest Endosc 2009.

18
Surgery
SCN MCN IPMN
Malignant potential?
No Yes Yes
9 28)
Surgery-MCN-
■ Malignancy: 17.5% 9, 28)
■ The prognosis is excellent
if resected before invasion.
Resection is recommended
Tanaka M, et al. Pancreatology 2006.
Clippa S, et al. Ann Surg 2007.

19
Side-branch IPMN
Surgery -IPMN-
Main duct IPMN
Prevalence of cancer
57% to 92%
Good surgical candidate should be offered surgical Good surgical candidate should be offered surgical resection. resection.
Tanaka M, et al. Pancreatology 2006.
Side-branch IPMN
Surgery -IPMN-
Main duct IPMN
Prevalence of cancer
6% to 46%
Lower prevalence of malignancyLower prevalence of malignancyTreatment should be individualized Treatment should be individualized
Tanaka M, et al. Pancreatology 2006.

20
Surgery -For IPMN-
International consensus guidelineInternational consensus guideline
■ Symptoms attributable to the cyst (e.g., pancreatitis)
■ Dilation of the main pancreatic duct (≥10 mm)
■ Cyst size ≥30 mm
■ Presence of intramural nodules
■ Cyst fluid cytology suspicious/positive for malignancy
Tanaka M, et al. Pancreatology 2006.
Management of asymptomatic cysts
Cyst size
<1<1cm
EUS Monitor
High risk stigmataHigh risk stigmata
MonitorEUS+FNA
Yes No

21
Management of asymptomatic cystsCyst size
1 to 3cm >3cm
EUS+FNA
Consistent with mucinous
Yes
EUS+FNA
Consistent with mucinous
Resection
?
NoHigh risk stigmataPositive cytology
Monitor
No Yes
Yes
Monitor
No
Pancreatic cysts-Injection of alcohol
EUS id d h l l fGan et al, GIE 2005
Dewitt et al, GIE 2009
EUS-guided ethanol lavage lt i t• EUS guided ethanol lavage for
ablation of pancreatic cystic lesions. 23/25 patients with complete follow-up, 8 patients (35%) had complete resolution of their cysts on follow-up imaging
Dimaio et al, Pancreas 2011
results in a greater decrease in pancreatic cyst size compared with saline solution lavage with a similar safety profile.Overall CT-defined
• Two sessions of EUS guided lavage versus only one session.
• 38% had complete resolution after two sessions of ethanol lavage.
Overall CT defined complete pancreatic cyst ablation was 33.3%.

22
Panc.cysts-EUS guided Chemo.
• EUS guided ethanol lavage with Paclitaxel injection in 14 pts cystic pancreatic tumors Oh GIE 2008pts.-cystic pancreatic tumors.Oh,GIE,2008
• Complete resolution in 11/14 patients(78%)
Alcohol injection or alcohol with paclitaxel are promising but not ready for prime time routinepromising but not ready for prime time routine clinical application.
28 months follow up
■ Size <3 cm71 patients
■ Solitary cyst
■ No septationNo solid component
■ Normal PD caliber
45/71 (63%) with f/u studies 26/71 (37%) no f/u studies
31/45 (69%) reviewed 14/45 (31%) not available
■ Normal PD caliber
■ CEA < 192 ng/ml
Pausawasdi N, et al. Surgery 2010.
31/31 (100%) no progression

23
Follow up
Wh t i th ti l i t l f ill ?Wh t i th ti l i t l f ill ?What is the optimal interval of surveillance?What is the optimal interval of surveillance?
2 year follow up from the baseline study for cyst size<3cm, no intracystic growth
Das et al, Am J Gastro 2008
My current practice:First follow up may be at 12 months with MRI and if no change repeat another MRI in one year.
MRI may be better test for follow up than CT
My current practice:
Take home message
■ There are variety of pancreatic cystic lesions.
Mucinous vs Non- mucinous.
Malignant vs Non-malignant.
■ A strategy based on risk stratification of malignant potential by EUS-guided FNA and g p y gcyst fluid analysis is the most cost-effective strategy.

24
The EndThank you for your attentionThank you for your attention