management of asthma - trinity college, dublin€¦ · management of asthma & coad oct 2009....
TRANSCRIPT

Management of Asthma &
COADOct 2009


Asthma fatal ity is preventable




Therapy
Quick reliefRescue medications Preventer medications
Short acting inhaled beta 2 agonists
Steroids
Long acting inhaled beta 2 agonists
Leukotriene antagonistsChromoglycate, others
During severe acute exacerbationsIpratropium
Available modalities
• Beta adrenergic receptor agoni sts• Glucocorticoids• Leucotriene receptor antagoni sts/
synthesis inhibitors • Nedocromil Sodium• Anticholinergic agents• Theophyllin

Drug delivery
Quicker onset of actionLesser side effectsGreater bronchodialation

Inhaled medications
LARGER THAN 5 MICRONDIAMETER:DEPOSIT LOCALLY
1-5 MICRON DIAMETER:DEPOSIT IN THE AIRWAYS
SMALLER THAN 0.5 MICRONDIAMETER: EXHALED

Optimising delivery
0102030405060708090
orophy. Deposit
spacer -spacer+
0
10
20
30
40
50
60
70
lung deposit
spacer -spacer+
INHALED MEDICATIONS
• HI LOCAL CONCENTRATION IN THE LUNGS
• MINIMAL SYSTEMIC ADVERSE EVENTS
• MORE THAN 90 % OF ASTHAMA TICS CAN BE MANA GED ON INHALED DEVICES ALONE
• CFC REPLACED BY Hydro-floro-alkane

A, 18 yrs of age, is found to be wheezy, since he moved to Ireland from US, initially symptoms were present in spring time only and of late are more persistant worse on
exercise.Diagnosis = Asthma

Rescue: Beta 2 agonist therapy
SHORT ACTINGSALBUTAMOLTERBUTALINE
5 MIN 4-6HRS
Ø All short acting beta 2 agonists are equipotent in thei r potencyØ Frequent use can reduce the durati on of action but maximal effect
remains unchangedØ A log linear dose response curve up to very high doses
CHECK INHALER TECH NIQUE AND ADD SPACER IF NEEDED.

• Mr A’s symptoms rel ieved completely with inhaler. But he needs frequent rescue meds
Good long term control•Infrequent asthmatic symptoms,•an unrestricted level of activity, •normal or near-normal lung function, • minimial or no asthmatic attacks requiring emergency care

Improving long term control [preventative therapy]
Inhaled glucocorticoids
antiinflammatory activities, Reduced t-cells, b cells,
dendriditic cells
Improved qual ity of lifeReduces acute attacksReduced hospi talisation
Reduced asthma related mortal ity

•Do not “cure “ inflammation which recurs with in 2 weeks of stopping therapy•Less effective in smokers•At doses of >1000micrgms can cause
- Growth retardation of 1 cm/year during the 1 styr - suppression of HPA axis- long term effects on bones and soft tissues

STEROIDS Inhaled steroids• Beclometasone dipropionate
(beclomethasone dipropionate), • budesonide, • fluticasone propionate, • mometasone furoateIV:Hydrocortisone
No major di fferences in long term outcomes at equivalent doses

CAUTIONS
• Paradoxical Bronchospasm
• mucous plugging of the airways causes decreased dose del ivery

Side effects
• adrenal crisis • respiratory tract infections • osteoporosis • glaucoma and catracts• Steroid induced hyperactivity and
insomnia• Cadidia infections (Upper GIT)

interactions
• Hypokalaemia• Antihypertensive agents• Vaccines• Reduced concentrati on with hepatic
enzyme inducers– Barbiturates– Benzodiazepines
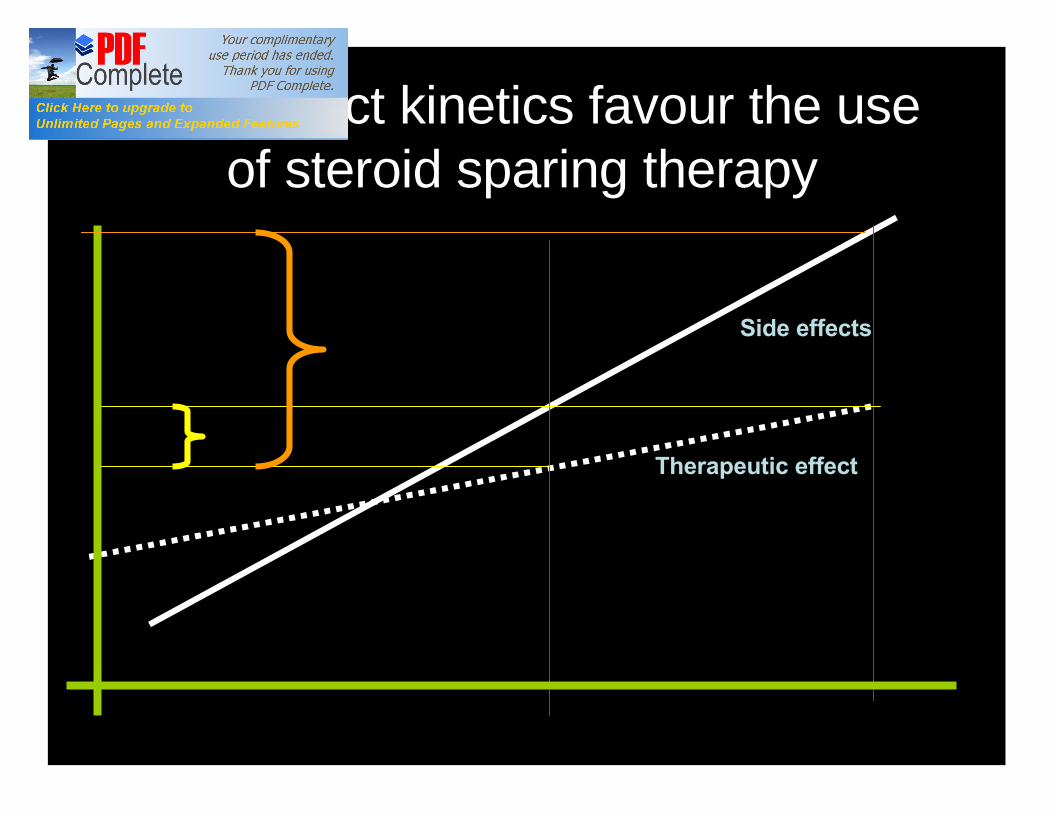
Dose effect kinetics favour the use of steroid sparing therapy
Therapeutic effect
Side effects

Adrenergic antagonistsBronchodilation and relief of
asthma symptoms
Non selective Selective beta 2 agonistsAdrenaline
EphidrineOrciprenaline
Potiential for serious cardiac arrythmiasNOT ADVISED
LONG ACTINGFormoterol (eformoterol) salmeterol

Long acting beta 2 agonists
12 HRS
• The bronchoprotective effect of long-acting β-agonists (i.e., their inhibition of exercise-induced bronchoconstriction) rapidly wanes with regular use
•Do not have anti -inflammatory effects hence may fail to provide effec tive relief •SHOULD ALWAYS BE USED W ITH INFLAMMATION REDUCING AGENTS•Combination therapy wi th steroids provides better cover and can be steroid sparing.•Concomitant use of short acting beta 2 agents does not interfere with efficacy.

Beta2 agonists should be used with caution in
• hyperthyroidism,• cardiovascular disease, • arrhythmias, • susceptibility to QT-interval prolongation,• hypertension.

Special precautions
• If high doses are needed duri ng pregnancy they should be given by inhalation because a parenteral beta2 agonist can affect the myometrium
• with caution in diabetes—monitor blood glucose (risk of ketoacidosis, especially when beta2 agon ist given intravenously).
Beta agonists and K +
• Hypokalaemia (Particularly in severe asthma)
potentiated by concomitant treatment wi th • theophylline and its derivatives, • corticosteroids,• diuretics,• hypoxia. Plasma-potassium concentration should
therefore be moni tored in severe asthma
Indications
• Reversible airway obstruction• COAD• Emergency treatment of hyperkalaemia• Myometrial relaxants

Side-effects of the beta2 agonists
• fine tremor (particularly in the hands), • Anxiety, • headache,• muscle cramps, • and palpitation. Less commonly• tachycardia, arrhythmias, peripheral
vasodilation, and disturbances of sleep and behaviour.
• Paradoxical bronchospasm, urticaria, angioedema, hypotension,

Interactions
• Hypokalaemia
• Reduced effecti veness with Beta- blocker therapy !!!

Leukotriene receptor antagonists


Leukotriene receptor antagonists
• montelukast and zafirlukast• Orally administered• No role in acute exacerbati on
• Inferior to steroid therapy• May be used in selected patients to
maintain a lower steroid dose

Leukotriene receptor antagonists
• Rarely eosinophilic vasculitic syndrome– Rash– Eosinophilia– Neuropathy– Worsening respiratory symptoms

• Possible worsening of l iver enzymes• Close monitoring of warfarin therapy• Reduced clearance of warfarin• Very rare systemic adverse effects
– GI disturbances– Thirst
Leukotriene receptor antagonists


Omalizumab anti IgE
• Reduces IgE levels by 90%• moderate and severe persi stent asthma
with raised IgE when – inhaled corticosteroids, – long-acting β-agonists, – leukotriene modifiers have not provided
adequate control

If you don’t mind ,I will ask for a second opinion

Antimuscrinic effects
•Bronchodilation•Reduced bronchial secretions
Blocked vagal activity Heart (tachycardia)Pupil dialationLens muscles - blurred visionInhibited micturitionGI motility decreased

Antimuscarinic bronchodilators: used mainly in COAD and severe
acute asthma attacks
• Ipratropium– Only mild bronchodilator– Peak effects at 30 min– Duration 4-6 hours
• Tiotropium– Long acting agent routine use in asthma not
advised

Cautions
• Prostatic hyperplasia• Bladder outflow obstruction• Glaucoma

Adverse effects
• Dry mouth • GI effects :nausea, Consti pation, • tachycardia, palpitation, paradoxical
bronchospasm, • urinary retention, blurred vision, angle-
closure glaucoma, • hypersensitivity reactions including rash,
urticaria, and angioedema occur rarely.

Interactions
• Increased anti -muscrinic effects– Antidepressants Tricyclics,Clozapine,MAO-I– antihistamines
• Reduced serum concentrati on– Levodopa– Ketoconazole
– Decrease effects of Metoclopramide / dompreidone


Theophylline
•ADENOSINE ANT AGONISTS
BronchoConstriction
Immune related mediator release

Theophyllin concentrations
INCREASED IN •Chronic Liver Disease•Heart failure•Drugs that inhibit livermetabolism
DECREASED IN•Smokers•Alcohol Excess•Drugs that induceliver metabolism
there is considerable variation in plasma-theophyllineconcentration particularly in smokers,

Intravenous use
• Aminophylline• Very slow administration (20 min)• Concentration between 10–20 mg/litre• Too irritant for IM use• Measurement of pl asma levels is essential
if patients already on theophyllin

Side effects
• tachycardia, palpitation,• nausea and other gastro -intestinal
disturbances, • CNS stimulation, headache, insomnia, • arrhythmias, and convul sions especially if
given rapidly by intravenous injection;

Caution
• SMOKERS / AL COHOL EXCESS/ LIVER DISEASE
• cardiac disease, • hypertension, • hyperthyroidism; • peptic ulcer; • epilepsy; • elderly;

Cromoglycate and related therapy
• Prophylactic agents (NO ROLE IN ACUTE ASTHMA)
• Sodium Cromoglicate and Nedocromil• asthma with an allergic basis• exercise-induced asthma• less effective than prophylaxis with
corticosteroid inhalations

Indications
• Exercise induced asthma• Food allergy• Allergic conjunctivitis



Percent Change in Age-Adjusted Death Rates, U.S., 1965-1998Percent Change in Age-Adjusted Death Rates, U.S., 1965-1998
00
0.50.5
1.01.0
1.51.5
2.02.0
2.52.5
3.03.0Proportion of 1965 Rate Proportion of 1965 Rate
1965 - 19981965 - 1998 1965 - 19981965 - 1998 1965 - 19981965 - 1998 1965 - 19981965 - 1998 1965 - 19981965 - 1998
–59%–59% –64%–64% –35%–35% +163%+163% –7%–7%
CoronaryHeart
Disease
CoronaryHeart
Disease
StrokeStroke Other CVDOther CVD COPDCOPD All OtherCauses
All OtherCauses
Source: NHLBI/NIH/DHHSSource: NHLBI/NIH/DHHS


Four Components of COPD ManagementFour Components of COPD Management
1. Assess and monitor disease
2. Reduce risk factors
3. Manage stable COPDl Educationl Pharmacologicl Non-pharmacologic
4. Manage exacerbations
1. Assess and monitor disease
2. Reduce risk factors
3. Manage stable COPDl Educationl Pharmacologicl Non-pharmacologic
4. Manage exacerbations

57
Management of Stable COPD
Manage Stable COPD: Key Points
§ individualized to address symptoms and improve quality of life.
§ health education (smoking cessation)
§ None of the existing medications for COPD have been shown to modify the long-term decline in lung function that is the hallmark of this disease (Evidence A).
§ Therefore, pharmacotherapy for COPD is used to decrease symptoms and/or complications.

58
Management of Stable COPD
Pharmacotherapy: Bronchodilators
§ Bronchodilator medications are central to the symptomatic management
§ PRN basis or on a regular basis to prevent or reduce symptoms.
§ The principal bronchodilator treatments are ß2- agonists, anticholinergics, and methylxanthines used singly or in combination (Evidence A).
§ Regular treatment with long-acting bronchodilators is more effective and convenient than treatment with short-acting bronchodilators (Evidence A).

59
Management of Stable COPD
Pharmacotherapy: Glucocorticosteroids
§ The addition of regular treatment with inhaledglucocorticosteroids to bronchodilator treatment is appropriate for symptomatic COPD patients with an FEV1 < 50% predicted (Stage III: Severe COPD and Stage IV: Very Severe COPD) and repeated exacerbations (Evidence A).
§ An inhaled glucocorticosteroid combined with a long-acting ß2-agonist is more effective than the individual components (Evidence A).

60
Management of Stable COPD
Pharmacotherapy: Vaccines
§ In COPD patients influenza vaccines can reduce serious illness (Evidence A).
§ Pneumococcal polysaccharide vaccine is recommended for COPD patients 65 years and older and for COPD patients younger than age 65 with an FEV1 < 40% predicted (Evidence B).

IV: Very SevereIII: SevereII: ModerateI: Mild
Therapy at Each Stage of COPD
§ FEV1/FVC < 70%
§ FEV1 > 80% predicted
§ FEV1/FVC < 70%
§ 50% < FEV1 < 80%predicted
§ FEV1/FVC < 70%
§ 30% < FEV1 < 50% predicted
§ FEV1/FVC < 70%
§ FEV1 < 30% predicted
or FEV1 < 50% predicted plus chronic respiratory failure
Add regular treatment with one or more long-acting bronchodilators (when needed); Add rehabilitation
Add inhaled glucocorticosteroids if repeated exacerbations
Active reduction of risk factor(s); influenza vaccinationAdd short-acting bronchodilator (when needed)
Add long term oxygen if chronic respiratory failure. Consider surgical treatments

62
Management of Stable COPD
Non-Pharmacologic Treatments
§ Rehabilitation: All COPD patients benefit from exercise training programs, improving with respect to both exercise tolerance and symptoms of dyspnea and fatigue (Evidence A).
§ Oxygen Therapy: The long-term administration of oxygen (> 15 hours per day) to patients with chronic respiratory failure has been shown to increase survival (Evidence A).

63
lobal Initiative for Chronicbstructiveungisease
lobal Initiative for Chronicbstructiveungisease
GOLD
GOLD

GOLD Website Address
http://www.goldcopd.org
