management of acute right ventricle failure in the icu
DESCRIPTION
Management of acute right ventricle failure in the ICU. Dr Vincent Ioos Medical ICU Pakistan Institute of Medical Sciences. Introduction. Neglected medical condition RV connected to pulmonary circulation: low pressure system Anatomical specificities of RV: thin wall (1/3 LV), crescent shape - PowerPoint PPT PresentationTRANSCRIPT

Management of acute right ventricle failure in
the ICU
Dr Vincent IoosMedical ICU
Pakistan Institute of Medical Sciences

Introduction
• Neglected medical condition• RV connected to pulmonary circulation:
low pressure system• Anatomical specificities of RV: thin wall
(1/3 LV), crescent shape• RV considered a passive conduit between
systemic and pulmonary circulation

Definition
« The clinical syndrome resulting from the inability of the right ventricle to provide adequate blood flow to the pulmonary circulation at a normal central venous filling pressure »

Main circumstances in ICU
• Severe pulmonary embolism• ARDS• Sepsis induced RV dysfunction• Exacerbation of medical conditions
leading to chronic pulmonary hypertension
• Right ventricle infarction• Pericardial diseases• RV failure after cardiac surgery• After cardiac transplant

Context
• Cardiac versus pulmonary causes
• RV previously healthy (Acute)
• Chronically impaired RV function (Acute on Chronic): RV hypertrophy / dilatation

Pulmonary hypertension: Venice 2003 classification
• Pulmonary arterial hypertension (PAH)– Idiopathic (iPAH)– Familial (FPAH)– Associated with (APAH) : Collagen vascular disease, Congenital
systemic-to-pulmonary shunts, Portal hypertension, HIV infection Drugs and toxins, …
– Associated with significant venous or capillary involvement– Persistent pulmonary hypertension of the newborn
• Pulmonary hypertension with left heart disease• Pulmonary hypertension associated with lung
diseases and/or hypoxemia• Pulmonary hypertension due to chronic
thrombotic and/or embolic disease• Miscellaneous (Sarciodosis, histiocytosis X, lymphangiomatosis,
compression of pulmonary vessels)
Simmoneau G, Galiè N, Rubin LJ, et al: Clinical classification ofpulmonary hypertension. J Am Coll Cardiol 2004; 43:10S.

Physiology of the normal pulmonary circulation
• Low pressure system: Prv (syst) = 25 mmHg / Plv (syst) = 120 mmHg
• The pressure in the pulmonary system depends on cardiac ouput, resistance and compliance
• The pulmonary vascular resistance has a particular dependency on alveolar oxygen tension, whereby alveolar hypoxia leads to pulmonary arterial vasoconstriction
• High compliance of the pulmonary vessels with large diameter and thin wall

O2 requirements and blood supply to the RV
• Less O2 requirements than the LV : less myocardic mass, less pre load and after load .
• During stress, extraction reserve is greater.• Vascularisation : 2/3 RCA, 1/3 left branches• RV perfused in both systolic and diastolic
phases as a result of the low systolic pressure (25 mmHg), which does not occlude the vessel that has a systemic pressure.
• If afterload , pressure necessary to contract the RV successfully , partial occlusion of the RCA may occur ischaemia.

Pathophysiology of failing RV
Piazza, G. et al. Chest 2005;128:1836-1852

Ventricular interdependence
• During systole, LV protrudes in RV• Surrounding pericardium with limited distensibility• Compliance of one ventricle can modify the other = Diastolic ventricular interaction
Right to left shunting
• Increase in RA pressure due to RVF• Reopening of patent foramen ovale• Right to left shunting• Secondary hypoxemia• Can be improved by improving RV function• Hypoxemia usually not improved by mechanical
ventilation in case of RVF due to pulmonary hypertension due to pulmonary vascular disease (PAH, CTEPH)

Vicious cycle of auto-aggravation

Management
• Control of trigerring factors
• Supportive treatment:– Optimization of preload– Improving contractility– Pulmonary vasodilators
• Specific therapies addressing the cause of RVF

Treatment of triggering factors
(acute on chronic)
• Arrhytmias• Infections• Pulmonary embolism• Thyroïd dysfunction

Optimization of preload
Frank-Starling relationship between preload and stroke volume: preload dependance (A) and preload independance (B)

Fluid therapy
Diuretics
• Frequent volume overload• At a point of Frank-Starling curve where
there is no more reserve on contractility• Ventricular interdependance• Diuretics to be considered• Sometimes with continuous high dose
infusion• If fails, consider CVVHF

• Prospective, controlled, randomized, animal study • 22 dogs underwent transient PA constriction
(90mn)• Dobutamine 5 and 10 g/kg/mn, norepinephrine
0.1 to 0.5 g/kg/mn• A transient increase in PA pressure persistently
worsens PA hemodynamics, RV contractility, RV-PA coupling, and cardiac output.
• Dobutamine restores RV-PA coupling and cardiac output better than norepinephrine because of its more pronounced inotropic effect

Dobutamine
1 adrenergic stimulation CI PVR at 5 g/kg/mn• At higher dose HR without subsequent
in PVR• Experimental models Dobutamine
Norepinephrine to improve right-ventricular – pulmonary artery coupling
• Improves CI, PVR and PaO2/FiO2 in combination with Inhaled nitric oxyde

Norepinephrine
1 and 1 adrenergic stimulation• Increases mPAP and PVR• But marked improvement in CO• Useful in combination with Dobutamine
for hypotensive patients• Causes less tachycardia than other
inotropes• Second choice after Dobutamine in
normotensive patients
Levosimendan
• Calcium sentitizer: increases the sensitivity of troponin C for Ca2+ within cardiac myocyte
• Dilatation of pulmonary vasculature by activation of adenosin tri-phosphate potassium channel
• Animal studies and pilot studies support its efficacy in right ventricle failure associated with pulmonary hypertension

• 35 ICU patients with ARDS and sepsis randomized to receive placebo or levosimendan 0.2g/kg/mn
• Mean arterial pressure 80 to 90 mmHg (sustained by norepinephrine infusion)
• Improvement of right ventricle performance:– CI (from 3.8 1.1 to 4.2 1.0 L/min/m2)– PAPm (from 29 3 to 25 3 mm Hg) RVESV, RVEF, SvO2

Addressing the cause of the RV failure, if possible
• Treatment of Pulmonary Arterial Hypertension
• Pericardiotomy/ drainage• Thrombolysis / embolectomy• Thrombolysis / angioplasty• Thromboendarteriectomy• Atrial septostomy• Transplantation

Pulmonary vasodilators

Inhaled nitric oxyde
• Dilate pulmonary vessels in ventilated units of the lung
• Reverses hypoxic pulmonary vasoconstriction
• In acutely decompensated RV improves PVR, increase CO improve PaO2/FiO2 (Benker KA et Al. Am J Crit Care. 1997
Mar;6(2):127-31) • Beware of methemoglobinemia (high
concentraton, prolonged use)
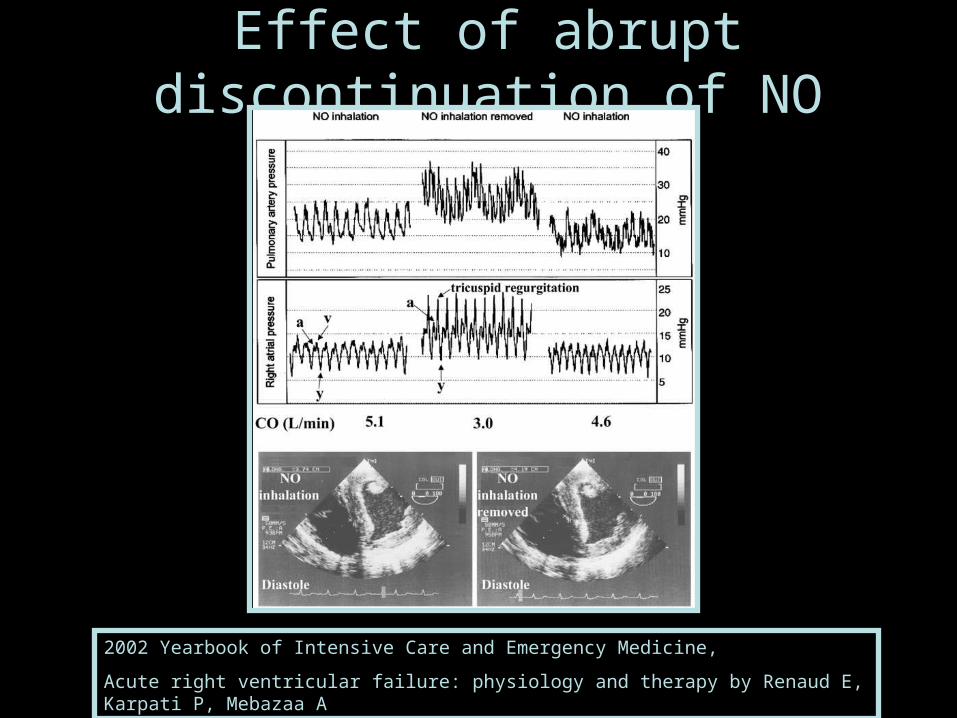
Effect of abrupt discontinuation of NO
2002 Yearbook of Intensive Care and Emergency Medicine,
Acute right ventricular failure: physiology and therapy by Renaud E, Karpati P, Mebazaa A

Prostanoids
• Intravenous Epoprostenol• Effect on survival in stable patients with PAH• Reduces mPAP and improves CO• Systemic side effects• Worsening PaO2/FiO2• Systemic effects (hypotension)• Inhaled prostacyclin / nebulized iloprost: case
series (Shock associated with PAH, Olschewski H. Intensive Care Med. 1998 Jun;24(6):631-4)

Sidenafil
• Phosphodiesterase-5 inhibitor• Approved for treatment of PAH (stable patients)• Only case reports for use in critically ill (RVF
after transplant: De Santo LS et Al.Transplant Proc. 2008 Jul-Aug; 40(6): 2015-8)
• May be useful for weaning from inhaled nitric oxyde
• Effect start 15mn after administration, peak effects within 30-60mn
• Systemic hypotension

Effects of mechanical ventilation
• Increased RV afterload due to positive pressure ventilation
• Hemodynamic failure frequently refractory in PAH patient put on MV
• In ARDS increase in mPAP while increasing tidal volume and PEEP
• Permissive hypercapnia is deleterious (increase in mPAP)
•
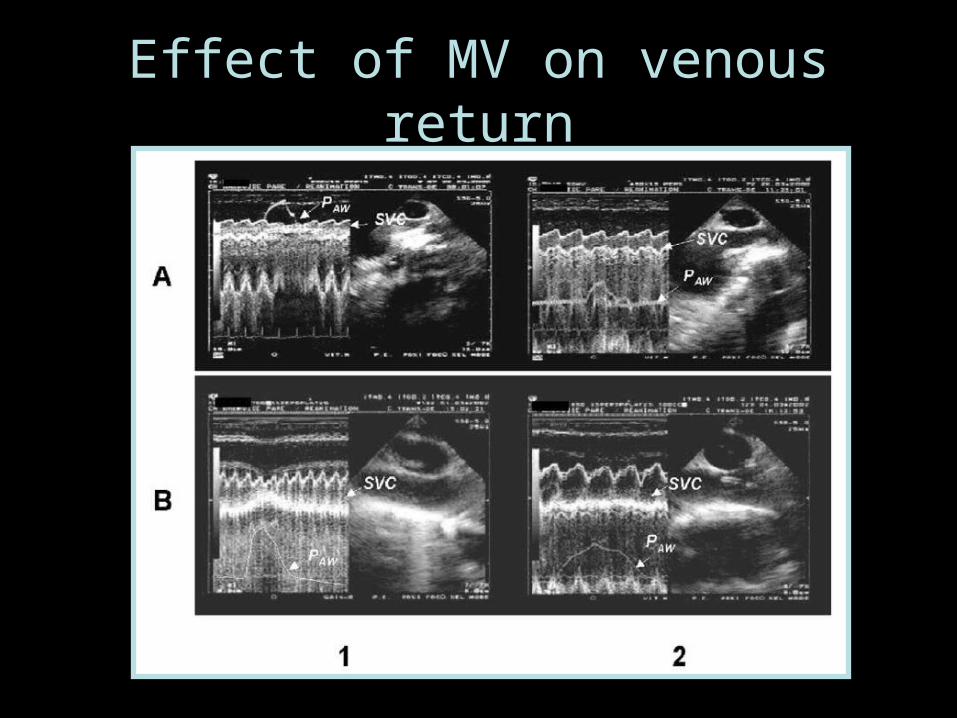
Effect of MV on venous return

Effects of transpulmonary presure on RV outflow
impedance
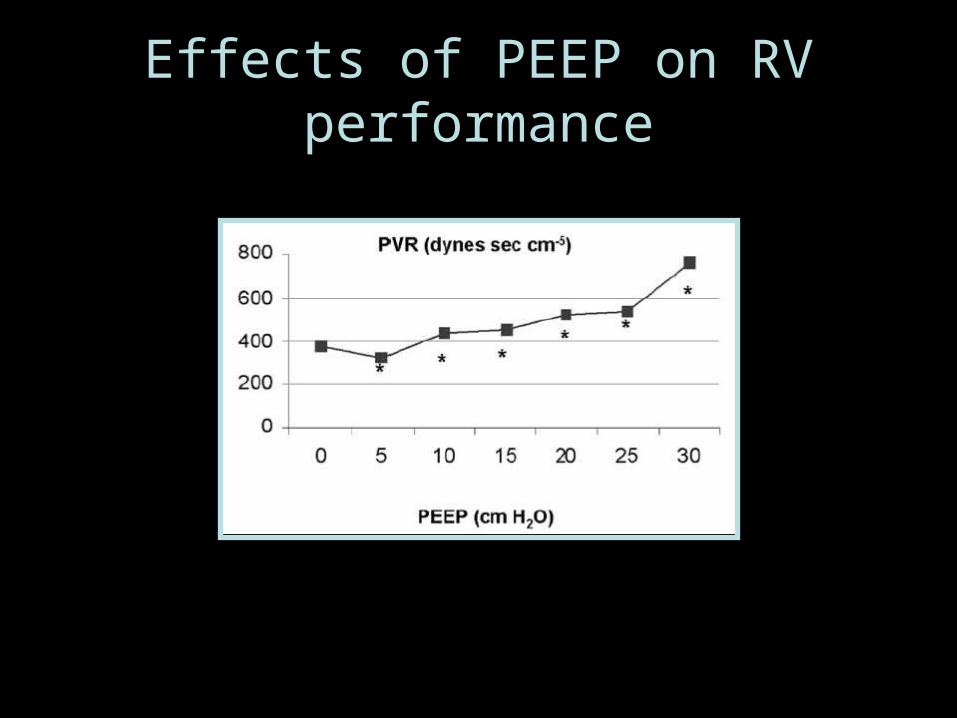
Effects of PEEP on RV performance
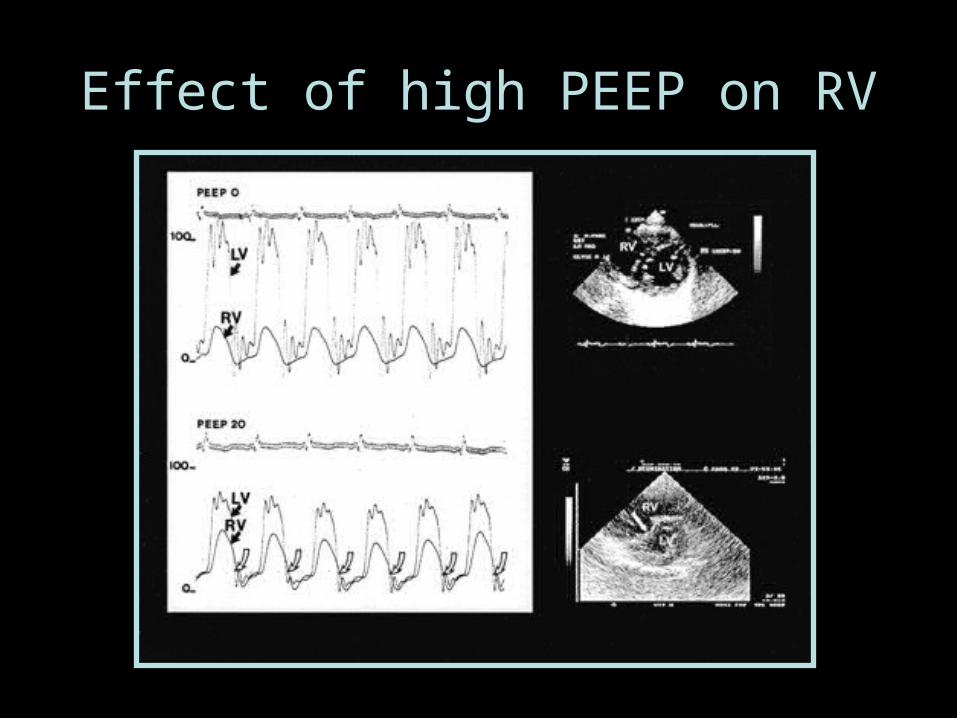
Effect of high PEEP on RV
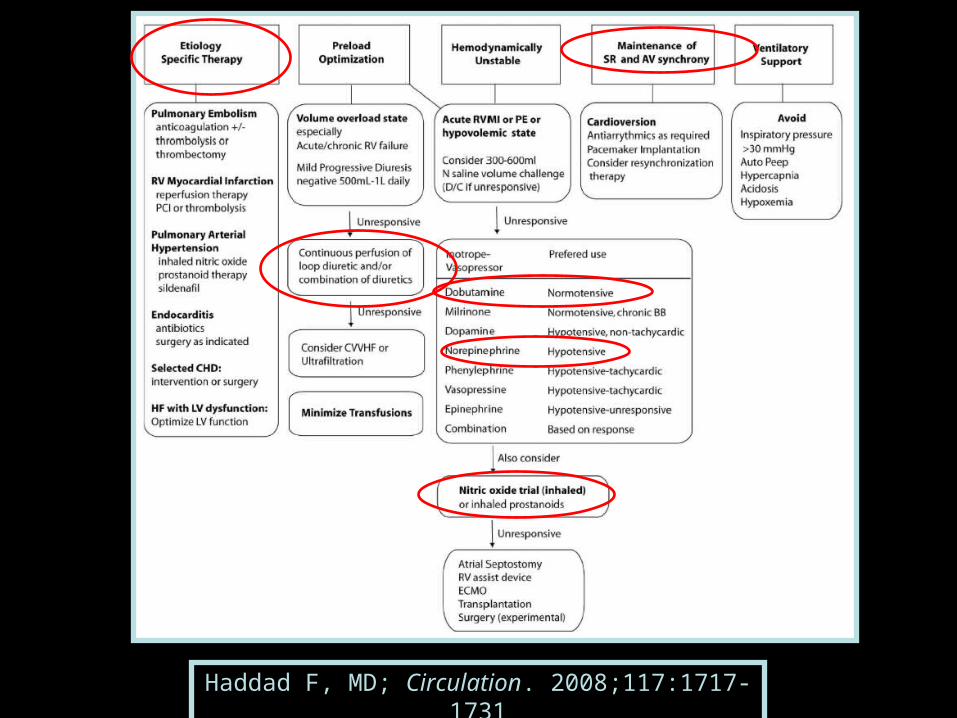
Haddad F, MD; Circulation. 2008;117:1717-1731