management acute peritonitis - pmj.bmj.com · intestinal tract, a diffuse andoften fatal...
TRANSCRIPT

631
THE MANAGEMENT OF ACUTEGENERAL PERITONITIS
By C. R. SAVAGEResident Assistant Surgeon, St. Thomas's Hospital, London
IntroductionInflammation of the peritoneal cavity is usually
due to bacterial infection which may be precededin certain instances by an initial chemical peri-tonitis. Infection most often commences locally insome part of the peritoneal cavity and particularlywith early and efficient treatment frequently re-mains confined to that area. It may, however,become widespread and it is to this condition thatthe term acute general peritonitis is applied. Inmany cases when the cause of this infection isremoved at an early stage, inflammation althoughwidespread, never becomes established in theperitoneum. This distinction between a generalperitonitis which has, and one which has not,become established, although largely a matter ofdegree is one of great importance as regardstreatment. In the former -case such measures asthe parenteral administration of fluids and the useof gastrointestinal aspiration may well be essential,while in the latter, in the majority of cases, theyare quite unnecessary. The causes of generalperitonitis are many and varied, but the mostcommon are acute appendicitis and perforationsof the stomach and duodenum; a not inconsider-able number of instances occur after electivesurgery on the gastrointestinal tract and these carrya very high mortality. There are a number ofprinciples underlying efficient management andthese will now be considered.
Early Elimination of the Source of InfectionIn the majority of instances organisms gain
access to the peritoneal cavity through perfora-tions in the walls of hollow viscera. Where thesource of infection can be dealt with at an earlystage either by closure of a perforation, as inperforated peptic ulcer or. by removal of the in-fected organ as in acute appendicitis, the peri-toneum is usually well able to overcome any in-fection which remains. Where, however, apersistent leakage of infected material occurs intothe peritoneal cavity either as a result of delay intreatment of an acute abdominal condition oroccasionally following an operation on the gastro-
intestinal tract, a diffuse and often fatal peritonitismay ensue. Considerable efforts on the part ofthe body may be made in an attempt to seal offthe area of such perforations and these are onoccasion successful. Diversion of the intestinalcontents from the site of the perforation willcertainly assist in this process. It may take theform of gastric aspiration in cases of perforatedpeptic ulcer or of proximal colostomy above thesite of a colonic perforation. It is seldom wise,however, to rely on this measure alone to controlcontinued peritoneal contamination, for in theformer instance it may not be possible to keep thestomach completely empty and even if this issuccessful, duodenal reflux may still occur, whilein the latter intestinal contents below the level ofthe colostomy may still continue to dischargethrough the perforation. Good results have,however, been obtained in the conservative treat-ment of perforated gastric and duodenal ulcers bygastric aspiration (Hermon Taylor), but it is con-sidered that early surgical closure is still the treat-ment of choice except in those cases in which theoperative risks are considered to be unduly high.Diversion of the stream of intestinal contents re-mains a valuable adjuvant measure.Removal of infected material which has already
accumulated in the peritoneal cavity should becarried out at operation with suction and thegentle use of gauze swabs. All methods ofirrigation have long since been abandoned becauseof their disastrous effect of spreading infection andbecause of the severe shock that they produced.It has long been realized also that attempts todrain the general peritoneal cavity are quite futileowing to the rapid sealing off of the drain track.In addition there are certain positive dangers anddisadvantages associated with the use of drainagetubes, such as the formation of adhesions, theerosion of surrounding structures (if the tube istoo rigid), the giving of unnecessary pain, and thepossible formation of an avenue of infection to theperitoneal cavity from without. Used, however,with certain definite objectives in mind, drainagemay be of very great value. Such is the case when
by copyright. on 16 M
arch 2019 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.28.326.631 on 1 D
ecember 1952. D
ownloaded from

632 POSTGRADUATE MEDICAL JOURNAL December 1952
doubt is felt about the integrity of a suture line,when it is not possible to remove an infected organor infected material which forms part of an in-flammatory mass or the wall of an abscess cavity,or when adequate haemostasis cannot be ensured.In these cases the presence of a drainage tube tothe site rapidly forms an exit for infected dis-charges which might otherwise form a localabscess or spread elsewhere within the peritonealcavity.
The Assistance ofthe Natural Processes oftheBody in the Resolution and Localization ofthe Infection
Widespread infection of the peritoneal cavitymay terminate in one of the following ways. Itmay undergo resolution with complete absorptionof the inflammatory exudate with or without theformation of adhesions. It may result in the deathof the patient usually by causing a general toxaemiawith peripheral circulatory failure due to a com-bination of factors amongst which continuedsepsis, interference with the water, electrolyte andprotein balances of the body and paralytic ileus arethe most important. It may localize into one ormore areas with the formation of abscesses whichmay in their turn either be absorbed, extend invarious directions and discharge either spon-taneously or with surgical aid into the lumen ofthe intestine, externally or, on rare occasions, intothe general peritoneal cavity.
It cannot be emphasized too strongly that amost important part of the management of thesecases consists in repeated clinical examination toascertain the presence and site of these residualabscesses and in their efficient treatment. Wherethe bowel forms part of the wall of the abscesscavity, discharge frequently occurs into thelumen, but when this process is delayed, withdeterioration in the general condition of thepatient, when the abscess points externally orwhere anatomical factors preclude this termination(e.g. subphrenic abscess) surgical evacuation isnecessary. If for any reason such treatment isdelayed for too long, sepsis may spread eitherlocally or widely in the peritoneal cavity withdisastrous results. On rare occasions due either tothe effect of antibiotics, to high resistance on thepart of the individual or to low resistance of theorganisms concerned, a chronic septic peritonitismay ensue with multiple plastic adhesions andscattered collections of pus and fibrin between theloops of intestine. In such cases either as theresult of leakage of air from the bowel at some un-known site or due to the presence of gas-formingorganisms, a form of spontaneous pneumo-peritoneum may occur with multiple encystedcollections of gas and fluid which on radiography
may closely resemble distended segments of bowel.Fig. i shows the X-rays of such a case. An opera-tion for the relief of intestinal obstruction had beenperformed three weeks previously and had beenfollowed by general peritonitis and paralytic ileus.Three days after the abdomen had returned tonormal size following resumption of bowel activity,it again became grossly distended, but this timewith gas and fluid outside the lumen of the bowel.Further operation confirmed these X-ray findings.The process of localization of infection within
the peritoneal cavity is brought about by the
FIG. i.-X-ravs in erect and horizontal lateral positionsshowing encysted intraperitoneal collections offluid and gas followina acute general peritonitis.(The dense shadows in the horizontal film are due tomercury in the bowel lumen following rupture ofthe balloon of a Miller Abbott tube.)
FIG. Ia.-Horizontal lateral X-ray. Spontaneouspneumoperitoneumn.
...............
FIG. Ib.-X-ray in erect position. From the samepatient as in Fig. ia.
by copyright. on 16 M
arch 2019 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.28.326.631 on 1 D
ecember 1952. D
ownloaded from
December I95 SAVAGE: The Management of .4cuite General Peritonitis 633
k/IV
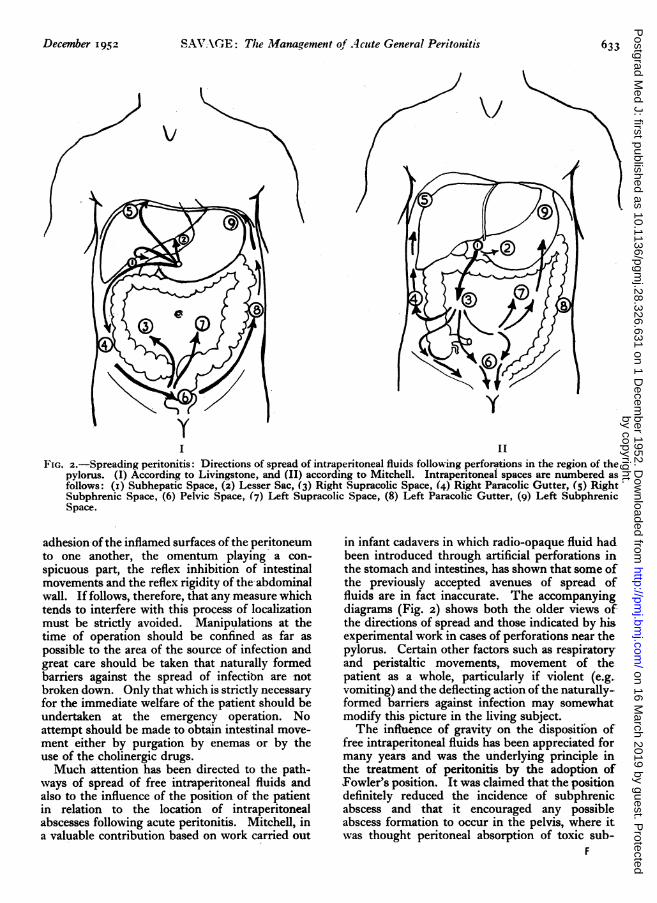
I IFIG. Z.-Spreading peritonitis: Directions of spread of intraperitoneal fluids following perforations in the region of the
pylorus. (I) According to Livingstone, and (II) according to Mitchell. Intraperitoneal spaces are numbered asfollows: (i) Subhepatic Space, (2) Lesser Sac, (3) Right Supracolic Space, (4) Right Paracolic Gutter, (5) RightSubphrenic Space, (6) Pelvic Space, (7) Left Supracolic Space, (8) Left Paracolic Gutter, (g) Left SubphrenicSpace.
adhesion of the inflamed surfaces of the peritoneumto one another, the omentum playing a con-spicuous part, the reflex inhibition of intestinalmovements and the reflex rigidity of the-abdominalwall. If follows, therefore, that any measure whichtends to interfere with this process of localizationmust be strictly avoided. Manipulations at thetime of operation should be confined as far aspossible to the area of the source of infection andgreat care should be taken that naturally formedbarriers against the spread of infectibn are notbroken down. Only that which is strictly necessaryfor the immediate welfare of the patient should beundertaken at the emergency operation. Noattempt should be made to obtain intestinal move-ment either by purgation by enemas or by theuse of the cholinergic drugs.Much attention has been directed to the path-
ways of spread of free intraperitoneal fluids andalso to the influence of the position of the patientin relation to the location of intraperitonealabscesses following acute peritonitis. Mitchell, ina valuable contribution based on work carried out
in infant cadavers in which radio-opaque fluid hadbeen introduced through artificial perforations inthe stomach and intestines, has shown that some ofthe previously accepted avenues of spread offluids are in fact inaccurate. The accompanyingdiagrams (Fig. 2) shows both the older views ofthe directions of spread and those indicated by hisexperimental work in cases of perforations near thepylorus. Certain other factors such as respiratoryand peristaltic movements, movement of thepatient as a whole, particularly if violent (e.g.vomiting) and the deflecting action of the naturally-formed barriers against infection may somewhatmodify this picture in the living subject.The influence of gravity on the disposition of
free intraperitoneal fluids has been appreciated formany years and was the underlying principle inthe treatment of peritonitis by the adoption ofFowler's position. It was claimed that the positiondefinitely reduced the incidence of subphrenicabscess and that it encouraged any possibleabscess formation to occur in the pelvis, where itwas thought peritoneal absorption of toxic sub-
F
by copyright. on 16 M
arch 2019 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.28.326.631 on 1 D
ecember 1952. D
ownloaded from

634 POSTGRADUATE MEDICAL JOURNAL December I952
stances was less active than in the subdiaphrag-matic area. Whereas large collections of fluid willcertainly be influenced in this way, it is notnecessarily true of smaller ones. Spalding hasmaintained that the Fowler position so far fromdiscouraging may, in fact, predispose to subphrenicabscess formation. He has emphasized the partplayed 'by respiratory movement in promoting aconstant flow of a thin film of peritoneal fluid inan upward direction towards the subdiaphragmaticarea under normal conditions, where it is absorbedtogether with any. small, particles w7hich may bepresent into the diaphragmatic lymphatics. Whenair is present within the peritoneal cavity (e.g.after laparotomy) this mechanism ceases tofunction so efficiently. Un&er' these' conditions heconsiders that, in the sitting position, a pocket ofair forms beneath the diaphragm which under theinfluence of respiratory movement may aspirateinfected fluid from the subhepatic pouch (whichdoes not empty in)'that position) into the sub-phrenic spaces.
It is certainly quite evident that a number offactors are involved in the localization of infectionwithin the subphrenic area and very difficult toassess which will, in fact, be predominant in anyparticular instance. In practice, moreover, factorsother than the location of residual abscesses willmodify opinion as to the correct position forthe patient with general peritonitis. The, im-portance of rest, both general and local, has longbeen realized in the treatment of acute inflam-matory conditions, but only more recently has itbeen appreciated that rest is not synonymous withimmobility and that the latter may have certainvery serious consequences. Important amongstthese are the liability to chest comnplications andthe tendency to peripheral vein thrombosis andpulmonary embolism. These dangers far out-weight the doubtful possibilities of influencing thesite of abscesses. It is now considered that move-iment and frequent change of position are of thegreatest importance to the patient, and that thereis no such thing as a correct or an incorrectposition. Constant attention must be -paid toimprovement of the pulmonary ventila'tion, to theexpectoration of bronchial secretions and to theprevention of circulatory stasis.
Destruction of Infecting OrganismsThe introduction first of all of the sulphonamide
group of drugs and later of the antibiotics has beenone of the most important advances in the treat-ment of peritonitis in recent years. Most cases ofperitonitis are due to the combined activities of anumber of different types of organisms and manyof these organisms are sensitive to one or other ofthe antibiotics. Failure of the antibiotics to over-
come the infection may be due to the presence ofinsensitive organisms, to persistent reinfection ofthe peritoneal cavity, to failure of the drugs topenetrate into infected and necrotic tissue whoseblood supply has been impaired and occasionallyto failure of the patient's normal resources againstinfection to play their necessary part. In rareinstances it may be due to inadequate dosage.
Parenteral administration of antibiotics isnormally'relied upon and is in most cases satis-factory. Attempts to control infection by oraladministration' in cases of persistent reinfectionfrom the" alimentary tract are likely to be un-successfui owing to the'loss of peristaltic activityof the intestine and the frequent necessity ofgastrointestinal aspiration. Local use 'within theperitoneal cavity is unwise in view of the formationof foreign body granulomas and adhesions. Owingto their wide range of activity, antibiotics havealmost entirely superseded the sulphonamides inthe treatment of peritonitis. It seems doubtful iftoxins produced by infecting bacteria themselvesare of much importance in contributing to thegeneral toxaemia and circulatory failure that maybe present. It is more likely that other substancesformed as a result of inflammatory destruction oftissue (perhaps of the nature of toxic amino-acids) may be responsible by exerting a directaction on the bowel wall and on the medullarycentres. The enormous area of peritoneal. surfaceavailable for absorption is obviously of importancebut it seems doubtful whether this absorbtivecapacity differs significantly in the various parts ofthe peritomeal cavity.
Correction of the Disturbed Water, Electro-lyte and Protein Balance of the Body
There is no doubt that a large part of the circu-latory collapse which is so marked a feature in thelater stages of peritonitis, especially if complicatedby paralytic ileus, is dependent upon the losses ofwater, electrolytes and protein that occur and toan alteration of their distribution within thecellular, extracellular and vascular compartmentsof the body. These losses may in fact be ofenormous dimensions and occur by vomiting orsuction from the upper intestinal tract, in somecases by diarrhoea from the lower, from the lungs,from the' kidneys and by sweating. In additionlarge quantities which cannot be, in fact, accuratelymeasured, are lost to the body in the formation ofinflammatory exudates and into the lumen ofdistended bowel. The normal intake of fluid mayin addition be grossly reduced.The aim in management in peritonitis must
therefore be to' restore the normal balance ofwater, electrolytes and protein in the body and tomaintain it once this has been achieved. In many
by copyright. on 16 M
arch 2019 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.28.326.631 on 1 D
ecember 1952. D
ownloaded from

December 1952 SAVAGE: The -Management of Acute General Peritonitis 635
early cases where peritonitis has not becomeestablished, this may be accomplished by oralintake alone or supplemented by' the rectal route.Where, ho'wever, infectioTi has advanced beyondthis stage as indicated by operative findings, bynausea, or vomiting (excluding post anaesthetic),by abdominal distension and terrderness and by arising or sustained high pulse' rate, dehydration islikely to be more severe and other measures willbe necessary. The main method' of administra-tion of fluid'must now be the intravenous route,and large amounts may be required to begin with.Careful records of the intake and output of fluidmust be kept in all cases. Estimation of the exactrequirements is not alw*ys easy as allthe relevantinformation necessary is never- available. Inpractice, guidance should be obtained from carefulclinical examination of the patient for evidence ofunder- or over-hydration, from study of the fluidbalance charts with special reference to the urinaryoutput and by daily' estimation of the urinarychlorides. Progress may be checked periodicallyby appropriate blood examinations. It is mostimportant to realize that' at all times the findings ofclinical examination are of primary importance andinformation gained by other means interpretedstrictly in relation-to these.The importance of protein deficiency which may
result from loss into inflammatory exudates, intothe lumen of the distended intestine, into theintestinal wall and from diminished intake has-been emphasized by Rob, who recommended theadministration of plIsna, sometimes in largequantities, for the prevention and treatment of-peripheral circulatory failure in 'all cases ofperitonitis of sufficient severity to require intra--venous fluids.
Recent work suggests that potassium loss is alsoimportant and any defiiciency must be rectifiedwith due regard to the dangers of over-dosage.
Control of Gastrointestinal DistensionReflex depression of gastrointestinal activity of
varying degree follows every laparotomy and may,in fact, be initiated reflexly on rare occasions bytrauma to more distant parts of the body. Thedepression of activity is accompanied by a dis-organization of the gas and fluid balancingmechanisms of the intestine. In the majority ofcases it is of a temporary nature only, but in certaininstances a self-perpetuating vicious circle ofevents is set up and paralytic ileus becomesestablished. This is particularly likely to occurin diffuse peritonitis. Careful and repeated clinicalexamination is necessary if the early symptoms andsigns of the onset of the condition are to be recog-nized. These are increasing abdominal distension,absent or altered bowel sounds, nausea and
vomiting and a rapid pulse rate. In most casesthere is no bowel movement and no flatus ispassed per rectum. It is important, however, torealize that nausea and vomiting may on occasionsbe entirely absent, that distension may pass un-noticed in the lax abdomen (e.g. after parturitionor in the obese) and that the only warning signsmay then be an otherwise unexplained rising pulserate in an anxious ill-looking patient. Symptomsof peripheral circulatory failure may follow rapidly.Paralytic ileus may affect either the whole or onlya part of the gastro-intestinal tract and diarrhoeamay occur in the presence of gross distensionparticularly in cases where infection is most markedin the pelvis. When in these cases the diarrhoea isaccompanied by a gradually rising pulse rate, itappears to. be of very ominous significance. Themost important causative factors appear to be thefailure of the normal gas and fluid balancingmechanisms of the bowel, the disorganization ofthe propulsive element of peristaltic activity,toxic paralysis of the bowel wall, circulatory stasisand hypoproteinemia. The fluid'in the distendedbowel is. derived from intake by mouth, gastric,intestinal, biliary and pancreatic secretions, andfluid diffused from the blood through the oedema-tous inflamed and ill-nourished bowel' wall.According to Wangensteen the gas is derivedlargely from swallowed air, the normal absorptivemechanism having broken down and, to a muchlesser extent, from diffusion from the blood andfrom digestive processes.
Mgaiagemrnt.should be directed to the relief ofdistension and to the maintenance of a satisfactorycirculation to the distended bowel as only if thisis ensured can there be hope of resumption ofnormal activity. Gastrointestinal aspiration hasbeen of the greatest value in achieving theseobjects. Introduced originally for diagnosticpurposes its therapeutic possibilities were 'soonrealized. The Miller Abbott double lumen tube,acting as a progressing internal enterostomy, wasan additional advance on this principle. Difficultyin introduction of the end of this tube into theduodenum despite careful attention to detail is notinfrequent, particularly in those cases in which itmight be expected to be of; most benefit. Oncepast the pylorous, however, its progress is4usuallymost satisfactory. It is fortunate that' in themajority of cases gastric intubation appears to beefficient in preventing vomiting and in ensuringadequate decompression. It is certainly seldomadvisable to persist in repeated attempts to passthe Miller Abbott tube into the duodenum in a'serioisly ill patient. Even when' this ttibe, 'haspassed into the small intestine it may on occa3ionfail to function satisfactorily even when its patencvis undoubted. It scems probable that this may be
by copyright. on 16 M
arch 2019 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.28.326.631 on 1 D
ecember 1952. D
ownloaded from

636 POSTGRADUATE NIEDICAL JOURNAL. December 1952
due either to the necessarily small caljbre of thetube in relation to thick intestinal contents some-times encountered, to further distention occurringin the bowel above the level of the end of thetube, as suggested by the increased aspirate whichmay be obtained on withdrawing the tube to ahigher level or to the arrest of the tube above anangulated distended loop of bowel. This additionalfactor of mechanical superimposed upon functionalobstruction, caused by angulation of distendedbowel is very important and arises in all cases inwhich distension becomes severe. Multiple pointsof obstruction are produced and attempted sur-gical relief is never indicated as these angulationsrapidly become reduced once normal peristalticactivity is resumed. Obstruction by adhesions ata single site certainly occurs following peritonitis,but it is seldom seen in the early post-operativeperiod. At one time it was considered that, insome cases, obstruction might be due to a localizedloop of small intestine becoming paralyzed byimmersion in a collection of pus in the pelvis (theileus duplex of Sampson Handley), but it seemsdoubtful if this is ever really so although the reliefof obstruction which may follow the drainage of anintraperitoneal abscess tends to support it. It maybe, in fact, that the inteptine has become angulatedand oedematous by becoming involved in theforma,tion of the wall ofNthe abscess and that thisis relieved when the pus has been evacuated.
Prolonged inhalation of oxygen in high con-centrations has been advocated in an attempt toreduce distension by displacing the nitrogen in thebowel. It is very difficult to judge clinically of itsefficacy, but this does not seem to be very great,certainly not sufficient to justify the additionaldiscomfort and manipulation that it entails.
Stimulation of the bowel by various methods hasalso been advised on many occasions in the treat-ment of paralytic ileus, but as far as that com-plicating peritonitis is concerned it is contra-indicated. There is no convincing evidence thatenemas can induce reflex peristalsis in the smallintestine and they may, in fact, add to distensionby being retained and fail to relieve even largebowel ileus when this is present. Cholinergicdrugs may cause contraction of the bowel but thiscontraction does not seem to be of the co-ordinatedpropulsive type necessary for the forward trans-
mission of the intestinal contents. They may, in-fact, stimulate further secretion from the bowelwall and where the mechanical obstructive elementhas supervened there are other possible dangers.
Certain other factors which have already beendealt with, such as the control of infection and ofthe water, electrolyte and protein balance of thebody will have a direct effect on improving thecirculation of the bowel wall and maintaining itin such a condition that its normal function mayreturn. They constitute an essential part oftreatment.
Provision of Rest and Relief of PainThe importance of ensuring adequate rest in
the form of sleep and relief of pain and anxiety ingeneral peritonitis has already been mentioned,and this is even more true when paralytic ileus hasensued. Many conflicting accounts have beengiven of the effects of morphine on the motility ofthe alimentary tract. Even if it were proved con-clusively, however, that it had inhibitory effects onthe intestinal muscle, its enormously valuablegeneral effects would continue to justify its use.
ConclusionImprovement in the prognosis of general
peritonitis has been very marked in recent years.The most important factors responsible are theintroduction of the antibiotics, the fuller under-standing of the fluid, electrolyte and proteinbalances of the body, the use of gastrointestinaldecompression and the earlier diagnosis and treat-ment of the acute abdomen. More powerful anti-biotics with an increased range of activity maybecome available in the future, but in the absenceof the most careful pre- and post-operativemanagement, attention to general surgical prin-ciples and to the details of surgical technique, it isdoubtful if the outlook in this condition can befurther improved to any great extent.
BIBLIOGRAPHYTAYLOR, HERMON (I946), Lancet, ii, 44i.ROB, C. G. ('947), Proc. Roy. Soc. Med., 40, 123.SPALDING, J. E. (1946), Lancet, 1, 643.MITCHELL, G. A. G. (I94I), B.J.S., 28, 291.WANGENSTEEN, 0. H. (1942), Int. Obs. Springfield: Charles
C. Thomas. 2nd Edition.LIVINGSTONE, E. M. (1932), 'A Clinical Study of Abdominal
Cavity and Peritoneum ' (Hoeber's Surgical Monographs No. x),New York: Paul B. Hoeber, Inc.
CORRECTIONWe Mmust apologise for the Printer's error which appears on p. 583 of the November issue,
this acknowledgment should read (Figs. 2, 3, 5 and 6 reproduced by kind permission of The Medical Press).
by copyright. on 16 M
arch 2019 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.28.326.631 on 1 D
ecember 1952. D
ownloaded from