managed care aaron liberman, ph.d.. overview of managed care
TRANSCRIPT
Managed CareManaged Care
Aaron Liberman, Ph.D.
Overview of Managed CareOverview of Managed Care
Techniques of Managed Care vs. Techniques of Managed Care vs. Organizations Performing Organizations Performing Managed Care FunctionsManaged Care Functions
Techniques of Managed Care vs. Techniques of Managed Care vs. Organizations Performing Organizations Performing Managed Care FunctionsManaged Care Functions
• Techniques–Financial incentives for providers
–Promotion of wellness
–Early identification of disease
–Patient education
–Self-care
–Utilization management (UR, QI, QM)
Techniques of Managed Care vs. Techniques of Managed Care vs. Organizations Performing Organizations Performing Managed Care FunctionsManaged Care Functions
Techniques of Managed Care vs. Techniques of Managed Care vs. Organizations Performing Organizations Performing Managed Care FunctionsManaged Care Functions
• Organizations– HMO– PPO– EPO– POS Plan – Self-Insured & Experience Rated HMO– Specialty HMO–Managed Care Overlay to Indemnity Plan– PHO
Stages of Managed CareStages of Managed CareStages of Managed CareStages of Managed Care
• Early Years: Before 1970–1792 Shippers of Boston
–1910 Western Clinic of Tacoma Wash.
–1929 Baylor Hospital’s Prepaid Plan for Teachers (BCBS)
–1932 AMA Adopts Stand Anti-Prepaid Group Practices

Stages of Managed CareStages of Managed CareStages of Managed CareStages of Managed Care
• Early Years: Before 1970 (cont.)
–1937 Kaiser Foundation Health Plans
–1937 Group Health Association
–1944 HIP of New York
–1947 Group Health Coop of Puget Sound
–1954 First Individual Practice Association

Stages of Managed CareStages of Managed CareStages of Managed CareStages of Managed Care
• Early Years: Before 1970 (cont.)
–Trends• Providers wanted to ensure flow of
patients & revenues• Employers began using prepaid plans• Consumers sought access to improved &
affordable healthcare

Stages of Managed CareStages of Managed CareStages of Managed CareStages of Managed Care
• Adolescent Years: 1970-1985–1973 HMO Act
–Problems with Federal Legislation

Features of the 1973 HMO Act Features of the 1973 HMO Act Features of the 1973 HMO Act Features of the 1973 HMO Act
• Grants and loans to start HMOs
• State laws against HMOs overridden
• Dual choice provisions– Indemnity vs. HMO
–Employers with 25+ employees must offer 2 HMO plans for every indemnity plan offered

Features of the 1973 HMO ActFeatures of the 1973 HMO ActFeatures of the 1973 HMO ActFeatures of the 1973 HMO Act
• Process to become federally qualified –Minimum benefit package
–Adequate provider network
–QA system in place
–Standards of financial stability
–Enrollee grievance system
1973 HMO Act: Importance of 1973 HMO Act: Importance of Federal QualificationFederal Qualification
1973 HMO Act: Importance of 1973 HMO Act: Importance of Federal QualificationFederal Qualification
• Good Housekeeping Seal–Use as a marketing tool
• Dual choice = access to employer market
• Preemption of state insurance oversight
• Required for receipt of federal grants

1973 HMO Act: Problems with 1973 HMO Act: Problems with Federal LegislationFederal Legislation
1973 HMO Act: Problems with 1973 HMO Act: Problems with Federal LegislationFederal Legislation
• Compromise between Liberals & Conservatives in Congress–Liberals wanted National Health
Insurance• Goal was to increase access to those
without access
–Conservatives wanted competition• Goal was to promote plans which gave
physicians incentives to constrain costs
1973 HMO Act: Problems with 1973 HMO Act: Problems with Federal LegislationFederal Legislation
1973 HMO Act: Problems with 1973 HMO Act: Problems with Federal LegislationFederal Legislation
• Result of the compromise was an open enrollment & community rating system–HMOs were required to accept all
enrollees without regard to their health status
–Limited the ability of HMOs to relate premiums to health status

1973 HMO Act: Problems with 1973 HMO Act: Problems with Federal LegislationFederal Legislation
1973 HMO Act: Problems with 1973 HMO Act: Problems with Federal LegislationFederal Legislation
• Federal government was slow in issuing implementation regulations
• Results of regulation attempts = failures of initial HMOs
Stages of Managed CareStages of Managed CareStages of Managed CareStages of Managed Care
• Coming of Age: 1985-Present– Innovation
–Maturation
–Restructuring

InnovationInnovation InnovationInnovation
• PHO as a Contracting Vehicle– Increased negotiating power of providers
• Development of Carve Outs–Separated the reimbursement of specific
specialized services
• Advances Computer Technology– Increased efficiency• i.e. generation of reports, processing of
claims

Maturation Maturation Maturation Maturation
• HMO & PPO growth– Increased enrollment
• External Quality Oversight–NCQA (most credible), URAC, AAAHC,
JCAHO
• Report Card System–Performance measurement systems• i.e. quality, outcomes, etc.
• Focus on Cost Management

RestructuringRestructuringRestructuringRestructuring
• Interplay between managed care & delivery system
• Dominance of primary care physicians
• Consolidation
Health Care ReformHealth Care Reform
Factors Driving Health Policy Factors Driving Health Policy FormationFormation
Factors Driving Health Policy Factors Driving Health Policy FormationFormation
• U.S. Budget & Deficit / Surplus
• Medicare Trust Fund Shortfall
• State Budget Shortfalls
• Business Profits & Growth –Excessive
• Public Demand & Appetite for Change
Medicare Payment PoliciesMedicare Payment PoliciesMedicare Payment PoliciesMedicare Payment Policies
• Packaged Pricing –Case rate method = DRGs
–APCs vs. RBRVS
• Risk Based Contracting – Fixed monthly amount
• Provider Sponsored Organization (PSO) –Provider-based integrated delivery system
Medicaid Payment PoliciesMedicaid Payment PoliciesMedicaid Payment PoliciesMedicaid Payment Policies
• Medicaid Managed Care Plans–PCCM
• Summary of Principal Efforts–Arizona effort
–Virginia effort

Ethics in Managed CareEthics in Managed Care(Fraud, Abuse & Emergence (Fraud, Abuse & Emergence
of Federal Legislation)of Federal Legislation)
Ethics in Managed CareEthics in Managed Care(Fraud, Abuse & Emergence (Fraud, Abuse & Emergence
of Federal Legislation)of Federal Legislation)
• Relationship to Managed Care
• Who are Managed Care Stakeholders
• Historical Perspective on Federal Legislation
Historical Perspective: Federal Historical Perspective: Federal LegislationLegislation
Historical Perspective: Federal Historical Perspective: Federal LegislationLegislation
• Hill Burton Act 1946
• First National Mental Health Commission
• CMHC Acts 1963
• Social Security Act 1965 (PL 89-97)–Medicare (Title 18)
–Medicaid (Title 19)

Historical Perspective: Federal Historical Perspective: Federal LegislationLegislation
Historical Perspective: Federal Historical Perspective: Federal LegislationLegislation
• CHP (PL 89-749)
• RMPs (PL 89-239)
• PSROs 1972 (PL 92-603)
• HMO Act 1973 (PL 92-222)
• NHRPD Act 1974 (PL 93-641)
• ERISA 1974
Historical Perspective: Federal Historical Perspective: Federal LegislationLegislation
Historical Perspective: Federal Historical Perspective: Federal LegislationLegislation
• OBRA 1981 –Medicare & Medicaid HMOs
• TEFRA 1983 –PPS
–DRGs
• Peer Review Improvement Act 1982–PSROs
–PROs
Historical Perspective: Federal Historical Perspective: Federal LegislationLegislation
Historical Perspective: Federal Historical Perspective: Federal LegislationLegislation
• DRGs 1985
• COBRA 1985 –Anti-dumping of patients
• HCQIA 1986 –National Health Practitioners Data
Bank
• OBRA 1987 –Nursing home quality care
Historical Perspective: Federal Historical Perspective: Federal LegislationLegislation
Historical Perspective: Federal Historical Perspective: Federal LegislationLegislation
• TEFRA 1988 –Medicare catastrophic coverage• Expanded Parts A & B
• CLIA 1988 –Lab standards classifying the
complexity of labs
• Medicare Coverage Repeal Act 1989–Congressional back peddling
Historical Perspective: Federal Historical Perspective: Federal LegislationLegislation
Historical Perspective: Federal Historical Perspective: Federal LegislationLegislation
• OBRA 1989 –Physician Payment Reform
–Resource Based Relative Value Scales (RBRVS)
• HIPAA 1996–Portability of coverage
–Restrictions on use of preexisting condition limits
–Establishment of MSAs
Contemporary RealizationsContemporary RealizationsContemporary RealizationsContemporary Realizations
• Limits on material resources
• Limits on health expenditures
• Limits on life saving devices
• Choices must be made
• Oregon legislation
• Honest business practices required

Compliance: Federal Statutory Compliance: Federal Statutory RequirementsRequirements
Compliance: Federal Statutory Compliance: Federal Statutory RequirementsRequirements
• Purposes of Compliance Programs–Detect & prevent violations
– Identify areas of vulnerability
–Reduce vulnerability
Compliance: Federal Statutory Compliance: Federal Statutory RequirementsRequirements
Compliance: Federal Statutory Compliance: Federal Statutory RequirementsRequirements
• Objectives of Compliance Program–Decrease risk of culpable actions by
employees
–Reaffirm key organization themes• Quality• Superior Service• Cost effectiveness
–Meet legal & statutory requirements
Compliance: Federal Statutory Compliance: Federal Statutory RequirementsRequirements
Compliance: Federal Statutory Compliance: Federal Statutory RequirementsRequirements
• Seven Key Steps for Compliance Programs–Establish compliance standards &
procedures
–Appoint a Corporate Compliance Officer
–Delegate discretionary authority
–Monitoring, auditing, & reporting• Use of employee hot line
Compliance: Federal Statutory Compliance: Federal Statutory RequirementsRequirements
Compliance: Federal Statutory Compliance: Federal Statutory RequirementsRequirements
• Seven Key Steps for Compliance Programs (cont.)
–Communicate standards to employees
–Consistent appropriate disciplinary procedure
–Consistent appropriate responses to violations
Excesses of Managed Care Excesses of Managed Care Organizations as Reflected in Organizations as Reflected in State Actions to Limit PowersState Actions to Limit Powers
Excesses of Managed Care Excesses of Managed Care Organizations as Reflected in Organizations as Reflected in State Actions to Limit PowersState Actions to Limit Powers
• 14 States: Guaranteed issue & renewal for individual insured
• 37 States: Guaranteed I & R group market• 33 States: Restrict pre-ex limits• 20 States: Authorized MSAs• 10 States: Laws increasing consumer access
to ER services• 13 States: Require range of added services
Excesses of Managed Care Excesses of Managed Care Organizations as Reflected in Organizations as Reflected in State Actions to Limit PowersState Actions to Limit Powers
Excesses of Managed Care Excesses of Managed Care Organizations as Reflected in Organizations as Reflected in State Actions to Limit PowersState Actions to Limit Powers
• 15 States: Prohibit Gag Rules• 17 States: Direct access to OB/GYNs

What About the Immediate What About the Immediate FutureFuture
What About the Immediate What About the Immediate FutureFuture
• Legislation on Patient Bill of Rights
• Personal Responsibility of Insureds
• Individual Ethical Code
Types of Managed Care Types of Managed Care OrganizationsOrganizations
HMOHMO
• Both an Insurer & a Delivery System
• Primary point of differentiation among HMOs:–How the HMO relates to its physicians
HMOHMOHMOHMO
• Staff HMO–Doctors are employees• Form a closed panel
–Advantage: • Easier to control
–Disadvantages:• Costly & expensive• Limited choice of doctors• Productivity problems

HMOHMOHMOHMO
• Group Practice HMO–Contracts with groups of doctors to
provide all services to members• Doctors are not employees of the HMO
–Captive vs. Independent Model• Captive = doctors provide services
exclusively for the HMO• Independent = doctors provide services
for both HMO & non-HMO patients
HMOHMOHMOHMO
• Group Practice HMO (cont.)
–Advantages:• Easier to conduct UM• Lower capital needs than Staff Model
–Disadvantages:• Limited choice• Limited locations• Perception of inferior care
HMOHMOHMOHMO
• Network HMO–Contracts with more than one practice
to provide services
–Advantage:• Broader physician participation
–Disadvantage:• Still limited choice
HMOHMOHMOHMO
• Individual Practice Association (IPA)–Contracts with an association of doctors
–Advantages:• Less capital requirements• Broad choice of doctors• Marketing advantages
–Disadvantages:• IPA becomes a de facto union for doctors• UM is difficult because doctors have
remained in private practice
HMOHMOHMOHMO• Direct Contract HMO–Works directly with large number of
doctors
–Advantage: • Eliminates possibility of physician bargaining
unit by contracting directly with each doctor
–Disadvantages:• May assume too much financial risk on
behalf of doctors• Difficult to recruit doctors because no clear
cut leader
PPOPPOPPOPPO• Common Characteristics of PPOs–Select provider panel
–Negotiated payment rates• Typically discounted 20-60%
–Rapid payment terms
–Utilization management• Failure to comply with plan requirements =
financial penalty to physician
–Consumer Choice• Higher cost sharing if choose non-panel
physician or hospital
PPOPPOPPOPPO
• Advantages:– Independence of providers &
consumers
–Flexibility of plan
• Disadvantages:–Little cost control
–Lack of provider concern for fiscal integrity of purchaser
EPOEPOEPOEPO
• Like PPO except patients may only use panel providers
• Advantage:–Control over provider behavior
• Disadvantages:–Potentially greater liability exposure
for EPO
–Disaffection of plan providers
POS PlansPOS PlansPOS PlansPOS Plans
• Uses primary care physician as gatekeeper
• Primary care physicians are capitated
• Withhold is prominently used
• Member can use non-panel provider but will pay much higher deductible
POS PlansPOS PlansPOS PlansPOS Plans
• Advantage:–Choice accorded patients
• Disadvantages:–Added cost to patients
–Lack of cost & underwriting control for POS Plan
Self-Insured & Experience Self-Insured & Experience Rated HMOsRated HMOs
Self-Insured & Experience Self-Insured & Experience Rated HMOsRated HMOs
• Fixed payments for period of time
• Followed by a settlement process
• Advantage:–Significant cost control
• Disadvantages:–Failure to reserve for IBNR
–Failure to underwrite conservatively
–Uncontrolled aggregate losses
Specialty HMOsSpecialty HMOsSpecialty HMOsSpecialty HMOs
• Dental & Vision
• Also called Single Specialty HMOs
• Advantage:–Low cost
• Disadvantages:–Generally disinterested providers
–Poor quality care
Managed Care OverlaysManaged Care OverlaysManaged Care OverlaysManaged Care Overlays
• Utilization management for general & specialty services
• Large case management for shock loss
• WCN utilization management
PHOPHOPHOPHO
• Simple vs. complex PHOs
• Advantages:–Greater negotiating clout
–Provided vehicle for risk sharing
–Clearinghouse for credentialling & utilization management
–Organized approach for physicians & hospitals to work together
PHOPHOPHOPHO
• Problems:–Difficulty competing against large
MCOs
–Large MCO making money with utilization management & do not want to capitate as way of laying off risk to PHO while UM is profitable
Integrated Healthcare Integrated Healthcare Delivery SystemsDelivery Systems
(IDS)
Three Categories of IDSThree Categories of IDSThree Categories of IDSThree Categories of IDS
• Only physicians are integrated– Individual Practice Association
–Physician Practice Management Organization
–Group Practice Without Walls
–Consolidated Medical Group
Three Categories of IDSThree Categories of IDSThree Categories of IDSThree Categories of IDS
• Physician & hospital integration–Physician Hospital Organization
–MSOs
–Foundation Model
–Physician Ownership Model
–Virtual Integration
• Full integration of physicians, hospitals, & insurance
Individual Practice Association Individual Practice Association (IPA)(IPA)
Individual Practice Association Individual Practice Association (IPA)(IPA)
• Negotiates fees on behalf of members
• Advantages:–Greater ability to share risk than PHO
–Easily understood
–Requires less startup capital
–Greater motivation to participating physicians
Individual Practice Association Individual Practice Association (IPA)(IPA)
Individual Practice Association Individual Practice Association (IPA)(IPA)
• Disadvantages:–Unwieldy
–Unable to change physician behavior
–Cannot accept high degree of risk without being classified as an insurance company & without having to be licensed
–Too many specialists creates upward utilization & cost pressures

Physician Practice Physician Practice Management OrganizationManagement Organization
Physician Practice Physician Practice Management OrganizationManagement Organization
• Provides management of all support services
• Advantages:–Purchasing power
–Specialists in managing practices
–Provide greater sense of ownership
Physician Practice Physician Practice Management OrganizationManagement Organization
Physician Practice Physician Practice Management OrganizationManagement Organization
• Disadvantages:–Too often focused on the next deal
• e.g. Phycor, Medpartners
–Not always engaged fully in essentials of the business

Group Practice Without WallsGroup Practice Without WallsGroup Practice Without WallsGroup Practice Without Walls
• Leverages negotiating strength with MCOs & hospitals
• Key Advantage:– Income is a function of group
performance
• Key Disadvantage:–Physicians remain as independent
practitioners
Consolidated Medical GroupConsolidated Medical GroupConsolidated Medical GroupConsolidated Medical Group
• True group practice with income sharing
• Advantages:–Economies of scale
–Negotiating leverage
–Can actually influence physician behavior
– Investment required of physicians serves as an exit barrier
Consolidated Medical GroupConsolidated Medical GroupConsolidated Medical GroupConsolidated Medical Group
• Disadvantages:– Inflated opinion of worth
–Rigid & unable to change
–Utilization patterns reflecting overhead pressures on group
Physician Hospital Physician Hospital Organization Organization (PHO)(PHO)
Physician Hospital Physician Hospital Organization Organization (PHO)(PHO)
• Actively manages relationship of principals–Ownership should be equally balanced
between physicians & hospitals
Physician Hospital Physician Hospital Organization Organization (PHO)(PHO)
Physician Hospital Physician Hospital Organization Organization (PHO)(PHO)
• Advantage:–Can negotiate effectively on behalf of
principals
• Disadvantage:–Often fails to achieve needed
improvements in contracts

Management Service Management Service Organizations Organizations (MSOs)(MSOs)
Management Service Management Service Organizations Organizations (MSOs)(MSOs)
• Service bureau
• Advantage:–Binds physician closer to hospital
• Disadvantage:–Physician remains too independent
Foundation ModelFoundation ModelFoundation ModelFoundation Model• Can either own provider organizations
or contract for services• Governed by Board & not dominated
by any provider group• Advantages:–High level of structural integration–Exerts considerable influence over
providers–Has resources to recruit & compensate
needed providers

Foundation ModelFoundation ModelFoundation ModelFoundation Model
• Disadvantages:–Primary: physicians only linked
indirectly to mission of Foundation
–Conflicts frequently occur between Foundation & providers
–Non-profit status of Foundation
•Must constantly prove it is a benefit to community to retain non-profit status
Physician Ownership ModelPhysician Ownership ModelPhysician Ownership ModelPhysician Ownership Model• Physicians hold significant portion of
ownership• Functions like an MSO & a Staff Model
HMO• Advantage:–Total alignment of goals of the group &
the IDS
• Disadvantage:–Amount of resources required to develop
& operate the system
Virtual IntegrationVirtual IntegrationVirtual IntegrationVirtual Integration
• Independent parties pretending to be integrated to maximize reimbursement potential
• Advantage:–“Virtually” none
• Disadvantage:–Conflicts & dishonesty
–“Virtually” non-existent relationship
Assuming An Insurance Assuming An Insurance FunctionFunction
Assuming An Insurance Assuming An Insurance FunctionFunction
• IDS becomes both a provider & a licensed payer (insurer)
• Can employ capitation &/or negotiated rates
• Advantage:–“One stop shopping”
Assuming An Insurance Assuming An Insurance FunctionFunction
Assuming An Insurance Assuming An Insurance FunctionFunction
• Disadvantage:–May not possess insurance experience
• Potentially disastrous
–Anti-trust implications
–Must maintain licensure
–Regulated by State Government’s Insurance Department
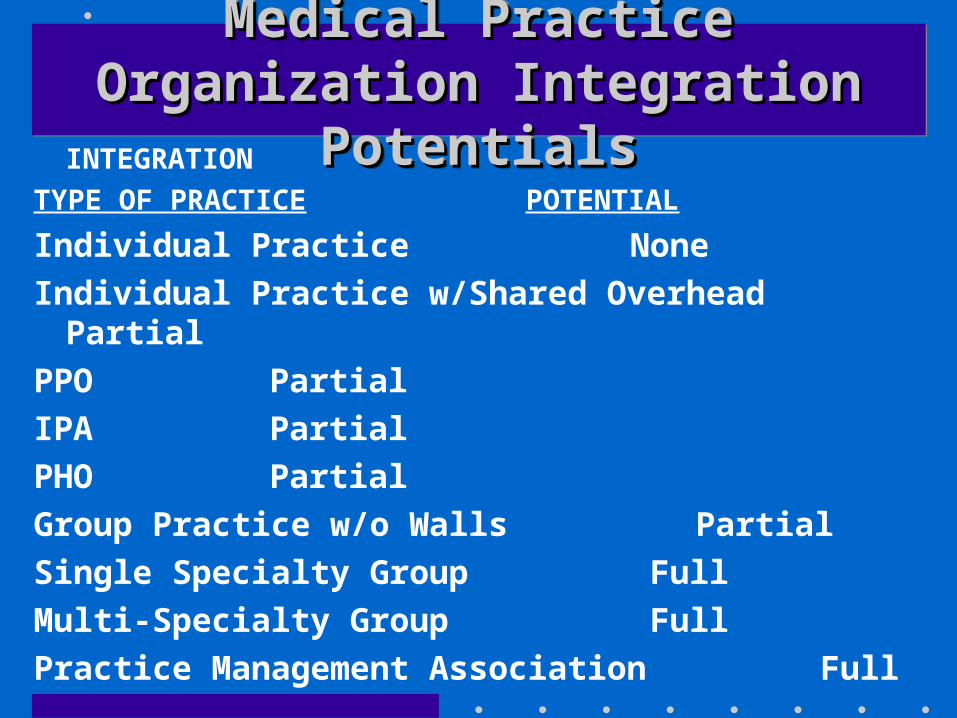
Medical Practice Organization Medical Practice Organization Integration PotentialsIntegration Potentials
Medical Practice Organization Medical Practice Organization Integration PotentialsIntegration Potentials
INTEGRATION
TYPE OF PRACTICE POTENTIAL
Individual Practice None
Individual Practice w/Shared Overhead Partial
PPO Partial
IPA Partial
PHO Partial
Group Practice w/o Walls Partial
Single Specialty Group Full
Multi-Specialty Group Full
Practice Management Association Full
Governance & Management Governance & Management ControlControl
Functions of the Governing Functions of the Governing BoardBoard
Functions of the Governing Functions of the Governing BoardBoard
• Stakeholder v. Shareholder
• Fiduciary Duty of For-Profit vs. Not For Profit Governing Board–The Stern Case (1963)• Board members diverted hospital funds to
finance their own business venture
–Duty of trust• Not for profit governing board has a
higher duty of trust

Functions of the Governing Functions of the Governing BoardBoard
Functions of the Governing Functions of the Governing BoardBoard
• Special duties of MCO governance–Quality management
–Employment of CEO
Functions of the Governing Functions of the Governing BoardBoard
Functions of the Governing Functions of the Governing BoardBoard
• Essential committee functions–Operations
–Personnel
–Planning
–CQI
–Compliance
–Pharmacy & therapeutics
• Liability Exposures of MCOs
Primary Care In Open & Primary Care In Open & Closed Panel PlansClosed Panel Plans

Definition of Primary CareDefinition of Primary CareDefinition of Primary CareDefinition of Primary Care
• Internal medicine
• Family practice
• Pediatrics
• OB/GYN–Represents a hybrid between primary
& specialty care
Sources of Candidates for Sources of Candidates for Open & Closed Panel Plans Open & Closed Panel Plans Sources of Candidates for Sources of Candidates for
Open & Closed Panel Plans Open & Closed Panel Plans
• Personal Relationships
• Physicians with privileges at panel authorized hospitals
• Physicians working for competitors
• Local/County Medical Society
Sources of Candidates for Sources of Candidates for Open & Closed Panel PlansOpen & Closed Panel PlansSources of Candidates for Sources of Candidates for
Open & Closed Panel PlansOpen & Closed Panel Plans
• Yellow Pages
• Health Claims Data to Eliminate Docs With Undesirable Traits
–i.e. overbilling, double billing, excess billings
Types of Contracting Types of Contracting SituationsSituations
Types of Contracting Types of Contracting SituationsSituations
• Individual Physician –Most common in open panels
–Advantages:• Direct relationship with physicians• Loss of 1 physician not consequential

Types of Contracting Types of Contracting SituationsSituations
Types of Contracting Types of Contracting SituationsSituations
• Small Group–Advantage:• Efforts net multiples of physicians
–Disadvantage:• Ending relationship costs multiple losses
of physicians–Particularly sticky with groups having
several competent physicians & 1 incompetent physician
Types of Contracting Types of Contracting SituationsSituations
Types of Contracting Types of Contracting SituationsSituations
• Multi Specialty–Advantage:• Obtain expertise in several areas
–Disadvantage:• Costs of retaining usually high
Types of Contracting Types of Contracting SituationsSituations
Types of Contracting Types of Contracting SituationsSituations
• Individual Practice Association –Advantage:• Large number of physicians can be
secured in one effort
–Disadvantages:• Functions as a bargaining unit • Often have to accept some less adequate
physicians
Types of Contracting Types of Contracting SituationsSituations
Types of Contracting Types of Contracting SituationsSituations
• IDS–Advantage:• Have network in rapid order
–Disadvantage:• Goals of physicians often not consistent
with IDS

Types of Contracting Types of Contracting SituationsSituations
Types of Contracting Types of Contracting SituationsSituations
• Medical School Faculty Practice Plans –Advantage:• Practice top quality medicine
–Disadvantages: • Less cost effective• Use of interns, residents, & medical
students• Not adept at case management
Reasons For Dissatisfaction Of Reasons For Dissatisfaction Of Physicians In Open & Closed Physicians In Open & Closed
Panel PlansPanel Plans
Reasons For Dissatisfaction Of Reasons For Dissatisfaction Of Physicians In Open & Closed Physicians In Open & Closed
Panel PlansPanel Plans
• Autonomy Issues
• Stress of dealing with demanding Patients
• High demands for productivity
• On-call requirements
• Spousal unhappiness
Reasons for Removing Reasons for Removing Physicians From PanelsPhysicians From PanelsReasons for Removing Reasons for Removing
Physicians From PanelsPhysicians From Panels• Physician unable to work within
system
• Panel too large
• Costly practice style
• Practices poor medicine
Compensation of Compensation of PhysiciansPhysicians

Reasons To CapitateReasons To CapitateReasons To CapitateReasons To Capitate
• From standpoint of MCO–Puts physician at risk• Most powerful reason
–Eliminates FFS incentive to overutilize
–Easier & less costly to administer
Reasons To CapitateReasons To CapitateReasons To CapitateReasons To Capitate
• From standpoint of provider–Ensures cash flow• Most powerful reason
–Profit margin under capitation often greater
–Eliminates fee disagreements
Problems With CapitationProblems With CapitationProblems With CapitationProblems With Capitation
• Adverse selection–Most common problem
• Perception that capitation income is “passive income”
• Inappropriate underutilization
Determination Of FeesDetermination Of FeesDetermination Of FeesDetermination Of Fees
• Percentage of usual, customary, & reasonable rates–Advantage:• Easy to obtain
–Disadvantage:• Physicians can greater fees by same
percent
• Relative Value Scales
• Global Fees
Determination Of FeesDetermination Of FeesDetermination Of FeesDetermination Of Fees
• APGs/APCs
• FFS–Losing ground due to churning &
upcoding
Determination Of FeesDetermination Of FeesDetermination Of FeesDetermination Of Fees• Incentives–Bonus based on production• Most common method
–Advantages:• Rewards productive physician• Helps modify bad habits• Documents low productive capacity
–Disadvantages:• Illegal & unethical behavior (churning,
buffing, turfing, upcoding, phantom billing, unbundling)
Contracting With HospitalsContracting With Hospitals
Types of Reimbursement Types of Reimbursement ArrangementsArrangements
Types of Reimbursement Types of Reimbursement ArrangementsArrangements
• % of charges
• Discounts
• Per Diems
• Sliding Scales
• Differential as a function of # of days in hospital
• DRGs
Types of Reimbursement Types of Reimbursement ArrangementsArrangements
Types of Reimbursement Types of Reimbursement ArrangementsArrangements
• Service type differential–Simple vs. Complex
• Case Rates
• Capitation
• % of premium revenue
• Bed leasing–Distinct part
Types of Reimbursement Types of Reimbursement ArrangementsArrangements
Types of Reimbursement Types of Reimbursement ArrangementsArrangements
• Periodic Interim payments
• Performance based incentives–Withholds
–Quality incentives
• Outpatient procedures–APGs/APCs
–Bundled rates
–Discounts
Managed Care in Academic Managed Care in Academic Health CentersHealth Centers
External Challenges To External Challenges To Academic Health CentersAcademic Health CentersExternal Challenges To External Challenges To
Academic Health CentersAcademic Health Centers• Changes in market mechanisms–Managed care has rendered AHCs non-
competitive
–PPS (DRGs) has cut into revenue base
• Employers now select health plans as a function of cost
External Challenges To External Challenges To Academic Health CentersAcademic Health CentersExternal Challenges To External Challenges To
Academic Health CentersAcademic Health Centers
• Diminished revenues as a function of failed health reform in 1993
• Loss of federal support for residency training
Internal Challenges To AHCsInternal Challenges To AHCsInternal Challenges To AHCsInternal Challenges To AHCs• Traditional culture–Physician is main focus which is at
odds with managed care which emphasizes extenders
–AHCs de-emphasize primary care
–AHCs are contra-positioned to outcomes-based treatment decisions
–AHCs do not emphasize sound business practices
–“Quality” patient care is a battle cry
Internal Challenges To AHCsInternal Challenges To AHCsInternal Challenges To AHCsInternal Challenges To AHCs
• Transition market–AHCs see themselves as a revenue
producer
–Manage care sees AHCs as a cost center
Internal Challenges To AHCsInternal Challenges To AHCsInternal Challenges To AHCsInternal Challenges To AHCs
• Information structure–Dearth of contemporary cost
information is a barrier to competitiveness
–Cannot assume financial risk because costs largely are not controlled
Learning From The Few Learning From The Few Successful AHCsSuccessful AHCs
Learning From The Few Learning From The Few Successful AHCsSuccessful AHCs
• Must find ways to maintain patient base–Network with non-academic hospitals
–Develop cost effective primary care programs
–Tie specialty services as support to primary care
Learning From The Few Learning From The Few Successful AHCsSuccessful AHCs
Learning From The Few Learning From The Few Successful AHCsSuccessful AHCs
• Transform traditional culture–Physicians must be held accountable
– Identify & compete for funding streams
–Centralize capital allocations • Autonomy failed
–Develop outcomes based treatment

Learning From The Few Learning From The Few Successful AHCsSuccessful AHCs
Learning From The Few Learning From The Few Successful AHCsSuccessful AHCs
• Reestablish education & research–Maintain cost effectiveness as a
requirement
–Network with MCOs• Linking point could be outcomes research• Tertiary care

Learning From The Few Learning From The Few Successful AHCsSuccessful AHCs
Learning From The Few Learning From The Few Successful AHCsSuccessful AHCs
• Reestablish education & research (cont.)
–Network with traditional health insurance carriers• Development competitive treatment
programs • Form specialty treatment networks
Managing Basic Medical-Managing Basic Medical-Surgical UtilizationSurgical Utilization

Purpose of Managed CarePurpose of Managed CarePurpose of Managed CarePurpose of Managed Care
Manage utilization & thereby reduce health care costs
Methods To Achieve Control Methods To Achieve Control Of Physician ServicesOf Physician Services
Methods To Achieve Control Methods To Achieve Control Of Physician ServicesOf Physician Services
• Single visit authorizations
• Prohibit secondary referrals & authorizations
• Review reasons for referrals
• Control self referrals by plan members
Methods To Achieve Control Methods To Achieve Control Of Physician ServicesOf Physician Services
Methods To Achieve Control Methods To Achieve Control Of Physician ServicesOf Physician Services
• LCM by specialty physicians–LCM process & relationship to specific
stop loss
• Compensation & financial incentives for specialists
Methods Of Decreasing Methods Of Decreasing UtilizationUtilization
Methods Of Decreasing Methods Of Decreasing UtilizationUtilization
• Precertification–Notice to concurrent review system
case occurring
–Ensure care occurs in most appropriate setting
–Capture data for financial accruals
• Preadmission testing & same day surgery
Methods Of Decreasing Methods Of Decreasing UtilizationUtilization
Methods Of Decreasing Methods Of Decreasing UtilizationUtilization
• Concurrent review–UM nurse: case manager
–Primary care physician
–Hospitalier
• Retrospective review–After case is concluded
Methods Of Decreasing Methods Of Decreasing UtilizationUtilization
Methods Of Decreasing Methods Of Decreasing UtilizationUtilization
• Alternatives to acute care hospitalization–SNF
– Intermediate Nursing Facility
–Subacute Facility

Disease ManagementDisease Management
Goals of DMGoals of DMGoals of DMGoals of DM
• Control cost of care per episode
• Reduce morbidity
• Improve functional status of patient
• Improve patient & physician satisfaction
• Acquire more meaningful outcome data
Goals of DMGoals of DMGoals of DMGoals of DM
• Develop improved ability to accept financial risk
• Control cost

Candidates for DMCandidates for DMCandidates for DMCandidates for DM
• Asthma
• Diabetes (Type 1)
• AIDS
• CA
• Behavioral care
• ESRD
• Hypertension
Steps In The Start Up Process Steps In The Start Up Process For DMFor DM
Steps In The Start Up Process Steps In The Start Up Process For DMFor DM
• Prioritize disease selection–Benchmarking
• Flowchart care processes–Case finding & preventive efforts
–Education & morbidity reduction
–Management of emergencies
–Hospitalization
–Ambulatory care follow-up
Steps In The Start Up Process Steps In The Start Up Process For DMFor DM
Steps In The Start Up Process Steps In The Start Up Process For DMFor DM
• Determine patient needs & preferences
• Discover cost drivers–Benchmarking
• Identify clinical outcome measures–Benchmarking

Steps In The Start Up Process Steps In The Start Up Process For DMFor DM
Steps In The Start Up Process Steps In The Start Up Process For DMFor DM
• Conduct value optimization studies to document evidence–Benchmarking
• Prepare for major information system investment
• Define episode duration–Benchmarking
Steps In The Start Up Process Steps In The Start Up Process For DMFor DM
Steps In The Start Up Process Steps In The Start Up Process For DMFor DM
• Use data to motivate & train physicians–Benchmarking
• Restructure financial incentives for physicians as deemed appropriate
Managing Utilization of Managing Utilization of Emergency & Ancillary Emergency & Ancillary
ServicesServices
Two Types Of Ancillary Two Types Of Ancillary ServicesServices
Two Types Of Ancillary Two Types Of Ancillary ServicesServices
• Diagnostic
• Therapeutic
Emergency ServicesEmergency ServicesEmergency ServicesEmergency Services
• Importance of emergency room services to a hospital
Managed Behavioral Care Managed Behavioral Care ServicesServices
Special Challenges Posed by Special Challenges Posed by BCSBCS
Special Challenges Posed by Special Challenges Posed by BCSBCS
• Destigmatization–#1 on most lists
• Erosion of Social Support System
• Increased Societal Complexity & Stress
• Advances in Medication & Psycho-therapeutic Methods
Special Challenges Posed by Special Challenges Posed by BCSBCS
Special Challenges Posed by Special Challenges Posed by BCSBCS
• Proliferation of Private Hospitals
• Tightening of Public Sector BCS Funding
• Use of BCS for Personal Development
4 Key Principles of Clinical 4 Key Principles of Clinical TreatmentTreatment
4 Key Principles of Clinical 4 Key Principles of Clinical TreatmentTreatment
• Finding Alternatives to Psychiatric Hospitalization
–PHP (day, night, & weekend programs)
• Finding Alternatives to Restrictive Treatment of Substance Abuse
–PHP & intensive outpatient care
Key Principles of Clinical Key Principles of Clinical TreatmentTreatment
Key Principles of Clinical Key Principles of Clinical TreatmentTreatment
• Goal Directed Psychotherapy
–Cognitive therapy
• Crisis Intervention
–EAP

Key Services in Community Key Services in Community Based ProgramsBased Programs
Key Services in Community Key Services in Community Based ProgramsBased Programs
• Acute inpatient services
• Outpatient therapy services–Non-physician directed
• Day treatment services–Also evenings & weekends
• Emergency services–Triage & referral
Key Services in Community Key Services in Community Based ProgramsBased Programs
Key Services in Community Key Services in Community Based ProgramsBased Programs
• Medication clinics–Physician directed
• Halfway (3/4) house residential services

Key Risk DeterminantsKey Risk DeterminantsKey Risk DeterminantsKey Risk Determinants
• Sufficiency of information
• Extent of services demand–Degree of chronicity
• Large claim risk factors–Adverse selection of group
Major Risk Factors In BCS Major Risk Factors In BCS Capitation Capitation
Major Risk Factors In BCS Major Risk Factors In BCS Capitation Capitation
• Restricted access = underservice• Cost shifting–From BCS to medical
• Preparedness to handle capitated care model–Case management
• Lack or insufficiency of information– Ill-prepared for capitation
• Substandard quality of care

Method Of Developing BCS Method Of Developing BCS Provider NetworkProvider Network
Method Of Developing BCS Method Of Developing BCS Provider NetworkProvider Network
• Establish size & scope of network
• Assess & determine fees & reimbursement rates
• Identify targeted providers
• Contact providers
• Obtain needed biographical information via applications
Method Of Developing BCS Method Of Developing BCS Provider NetworkProvider Network
Method Of Developing BCS Method Of Developing BCS Provider NetworkProvider Network
• Conduct site visits & interviews
• Select providers for network

Emerging Issues In BCSEmerging Issues In BCSEmerging Issues In BCSEmerging Issues In BCS
• Horizontal integration to achieve comprehensive service structure
• Develop data to validate service necessity
• Legal & ethical values must be established
• Control of costs is essential to acceptance

Emerging Issues In BCSEmerging Issues In BCSEmerging Issues In BCSEmerging Issues In BCS
• Financial incentives adjusted to promote cost effective & quality services
• Services accessible to persons of all cultures