malnutrition: will the oig be coming to see you? all you ... · moderate to severe, assign code...
TRANSCRIPT

1
This is the Full Title of a Session
Malnutrition: Will the OIG Be Coming to See You? All You Need to Know and More
Vaughn Matacale, MD, CCDSDirector, Physician AdvisorsVidant HealthGreenville, NC
Kristen Gonzalez, MHA, RHIASenior HIMS AdministratorVidant HealthGreenville, NC
Shelby Humphreys, RHIACorporate Director, Coding and CDIVidant HealthGreenville, NC
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.
2
Learning Objectives
• At the completion of this educational activity, the learner will be able to:– Recognize components of the OIG audit process– Describe the importance of clinical guidelines and definitions to support documentation and coding of malnutrition
– Discuss current coding guidelines and Coding Clinics that are relevant to compliant coding of malnutrition
– Explain the clinical implications and impact of diagnosing and treating malnutrition
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

3
Introduction
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

4
Vidant Health
• 8 hospitals (3 CAHs)• 1,512 all Vidant hospitals • 974 Vidant Medical Center• Affiliated medical school• 1,000+ providers
• 64,388 admissions• 46,544 surgeries• 5 physician advisors• Over 30 IP coders and 15 CDSs• Over 36 quality staff
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.
5
OIG Letter of Engagement
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

6
Rationale for Performing Audit
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

7
Letter of Intent OIG
• Intent to audit inpatient claims with diagnosis code 261 (nutritional marasmus) or 262 (other severe protein‐calorie malnutrition)
• Objective was to determine compliance with Medicare regulations
• Period spanning January 2013–June 2015
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

8
Kwashiorkor Audits
• Between 2014 and 2016, OIG published 25 reports on incorrect use of ICD‐9‐CM code 260 (Kwashiorkor)
• Dates of service span CY 2010–2014• Overpayments of $6,030,135 identified
– Coding classification was unclear on use of code 260• Discrepancy between alpha and tabular index
– Alpha included Kwashiorkor, Malnutrition (calorie) malignant, Malnutrition (calorie) protein, Protein deficiency, Protein malnutrition
– Tabular listed only Kwashiorkor• Coding software led to incorrect code assignment
• Recent report estimates total loss of $102 million during CY 2006–2014 related to Kwashiorkor coding
“CMS Did Not Adequately Address Discrepancies in the Coding Classification for Kwashiorkor”https://oig.hhs.gov/oas/reports/region3/31400010.pdf
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

9
Flawed Audit Rationale
• OIG suggests that the rationale for incorrect billing of code 260 (Kwashiorkor) could have caused hospitals to incorrectly assign codes 261 and 262
• Code 260 (Kwashiorkor) does not include protein malnutrition– Clarified by AHA Coding Clinic Q3 2009
• “Code 260, Kwashiorkor, is not appropriate since the provider did not specifically document this condition.”
• Codes 261 (Nutritional marasmus) does includes severe malnutrition NOS– Confirmed by AHA Coding Clinic Q3 2012
• “If provider documentation indicates that the malnutrition has progressed from moderate to severe, assign code 261, Nutritional Marasmus, for Severe Malnutrition.”
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.
10
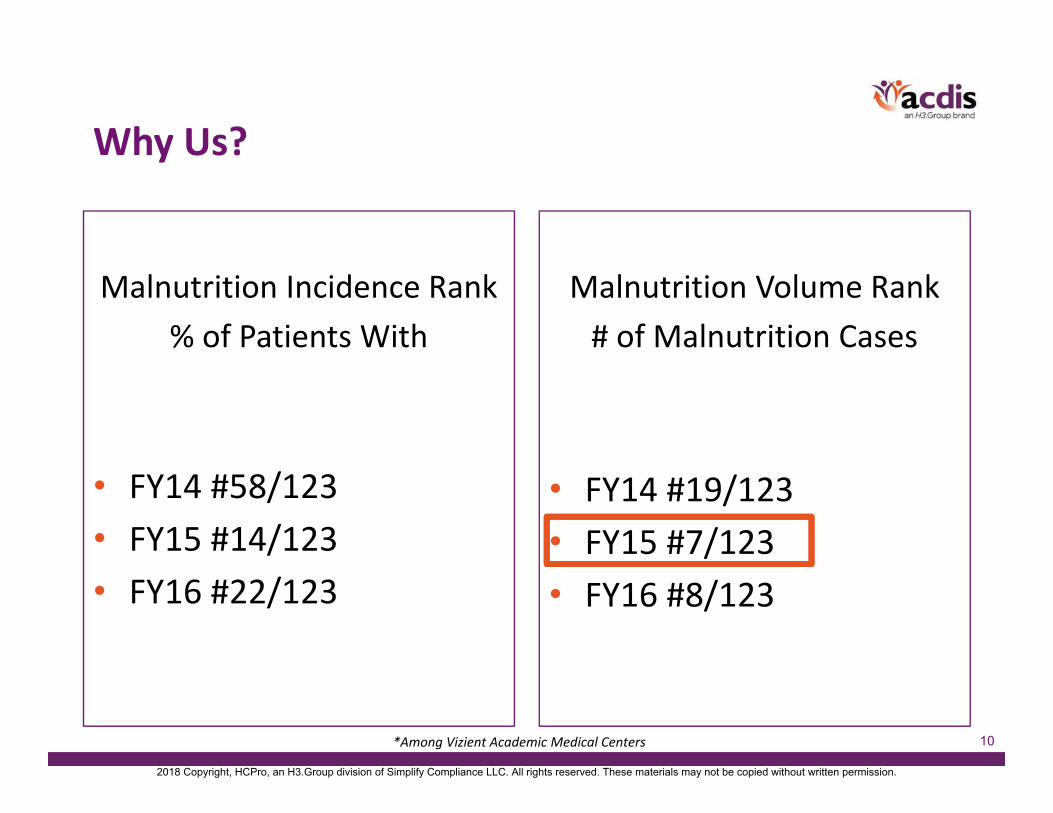
Why Us?
Malnutrition Incidence Rank% of Patients With
• FY14 #58/123• FY15 #14/123• FY16 #22/123
Malnutrition Volume Rank# of Malnutrition Cases
• FY14 #19/123• FY15 #7/123• FY16 #8/123
*Among Vizient Academic Medical Centers
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.
11
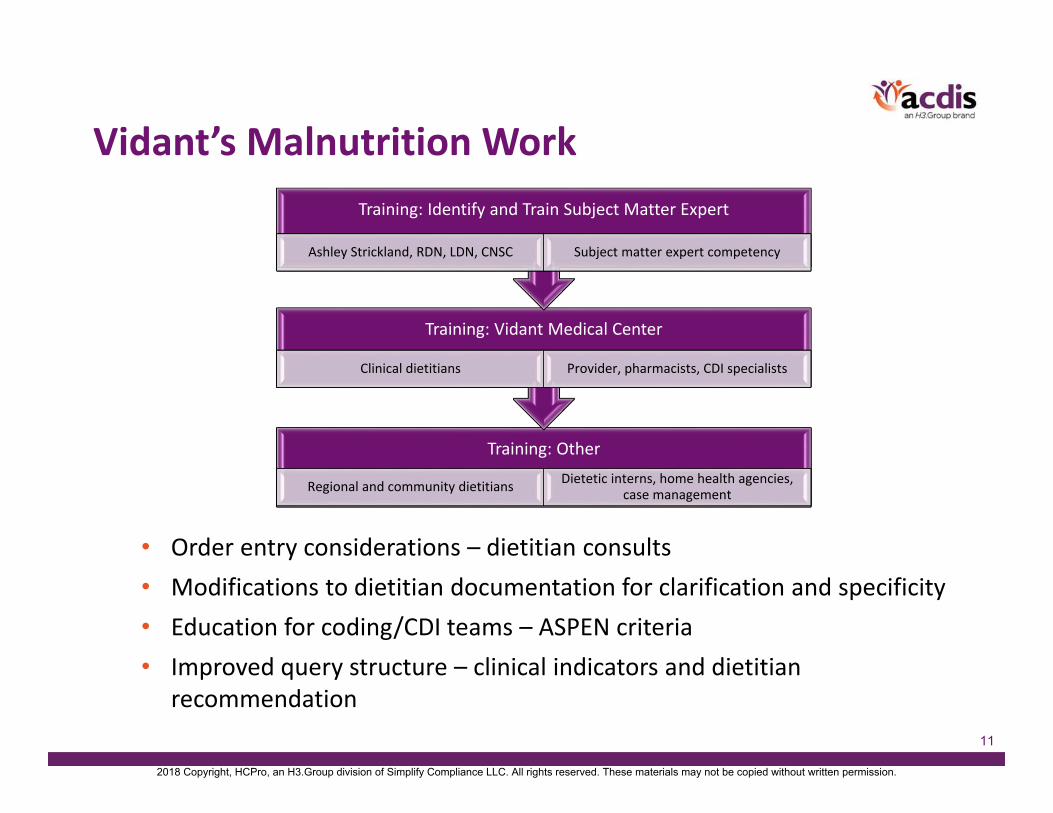
Vidant’s Malnutrition Work
• Order entry considerations – dietitian consults• Modifications to dietitian documentation for clarification and specificity• Education for coding/CDI teams – ASPEN criteria• Improved query structure – clinical indicators and dietitian
recommendation
Training: Other
Regional and community dietitians Dietetic interns, home health agencies, case management
Training: Vidant Medical Center
Clinical dietitians Provider, pharmacists, CDI specialists
Training: Identify and Train Subject Matter Expert
Ashley Strickland, RDN, LDN, CNSC Subject matter expert competency
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

12
Education: Coding and CDI Teams
• External consultant education • Dietitian in‐service with existing coders• Coding academy for new coder staff• Articles for coder monthly focused education time• CDS orientation and preceptor for new CDSs• CDS meeting education for existing CDSs• Pilot program CDS presentation• Dietitian presentation at joint CDS and coder meeting• ASPEN criteria education and references during CDS
orientation• Doc tips• ASPEN material on shared drive
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

13
Vidant Audit
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.
14
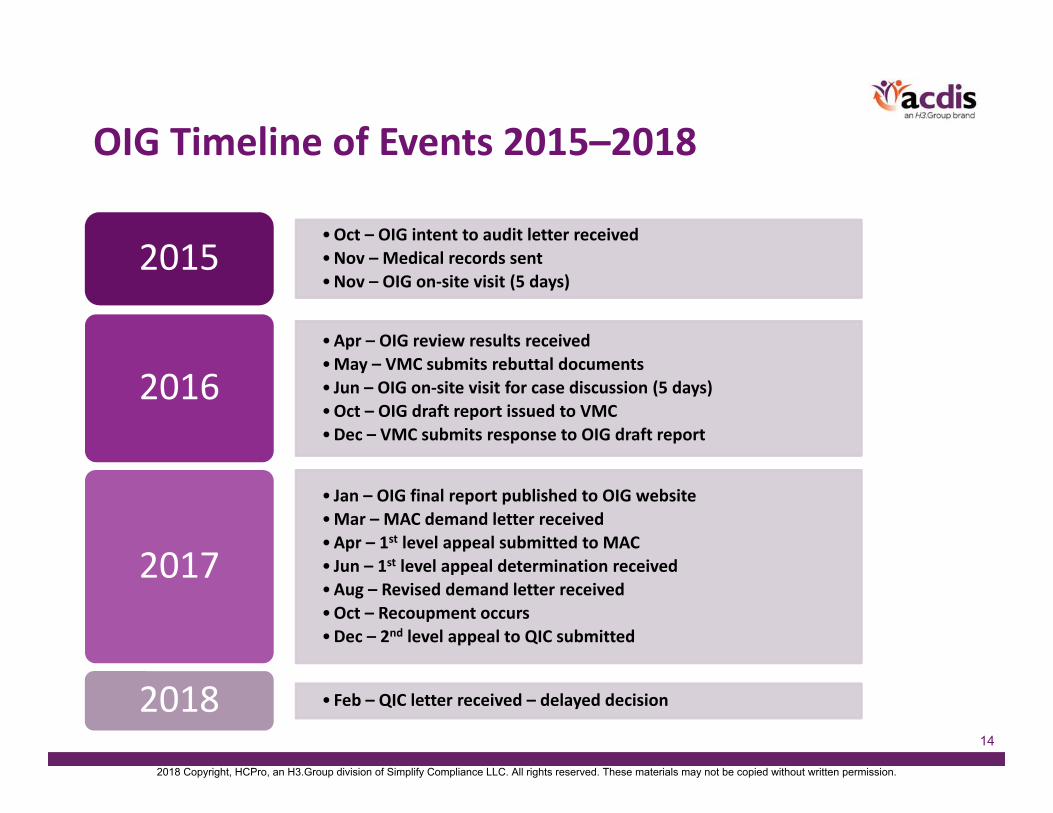
OIG Timeline of Events 2015–2018
•Oct – OIG intent to audit letter received•Nov – Medical records sent•Nov – OIG on‐site visit (5 days)
2015
•Apr – OIG review results received•May – VMC submits rebuttal documents• Jun – OIG on‐site visit for case discussion (5 days)•Oct – OIG draft report issued to VMC•Dec – VMC submits response to OIG draft report
2016
• Jan – OIG final report published to OIG website•Mar – MAC demand letter received•Apr – 1st level appeal submitted to MAC• Jun – 1st level appeal determination received•Aug – Revised demand letter received•Oct – Recoupment occurs•Dec – 2nd level appeal to QIC submitted
2017
• Feb – QIC letter received – delayed decision2018
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

15
OIG Audit Experience
• Initial on‐site visit with OIG (Nov 2015)– Four auditors on‐site for 5 days– Lead auditor with experience in past kwashiorkor reviews– Entrance/exit conferences– Representation from legal, compliance, billing, HIMS, physician advisor teams
– Process interviews conducted• Coding • CDI• Billing
– No reviews of cases during on‐site
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

16
OIG Audit Experience
• Records submitted by due date– OIG contracts with outside review group (Maximus)
• Significant delays in audit completion• Maximus results received late April 2016 • Vidant performs immediate review of findings to prepare for any appeal opportunities
• On‐site case discussion offered by OIG – Week of June 6, 2016– Case‐by‐case rebuttals by internal interdisciplinary team– No intention of overturn by OIG auditors– No opportunity to rebut directly to Maximus review team
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

17
OIG Audit Experience (OIG to MAC)
• Formal rebuttal to pending OIG final report underway (summer to fall 2016)– OIG draft report shared and reviewed by Vidant
• Interdisciplinary team, legal, and compliance involved• Formal statement submitted
– OIG final report published in January 2017– 1st level appeal prep underway
• Vidant waits for demand letter from MAC– Discussions with CMS action official– Contact made with PGBA representative
• Demand letter received (March 2017)– Validation of information in letter
• Extrapolation amount verified
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.
18
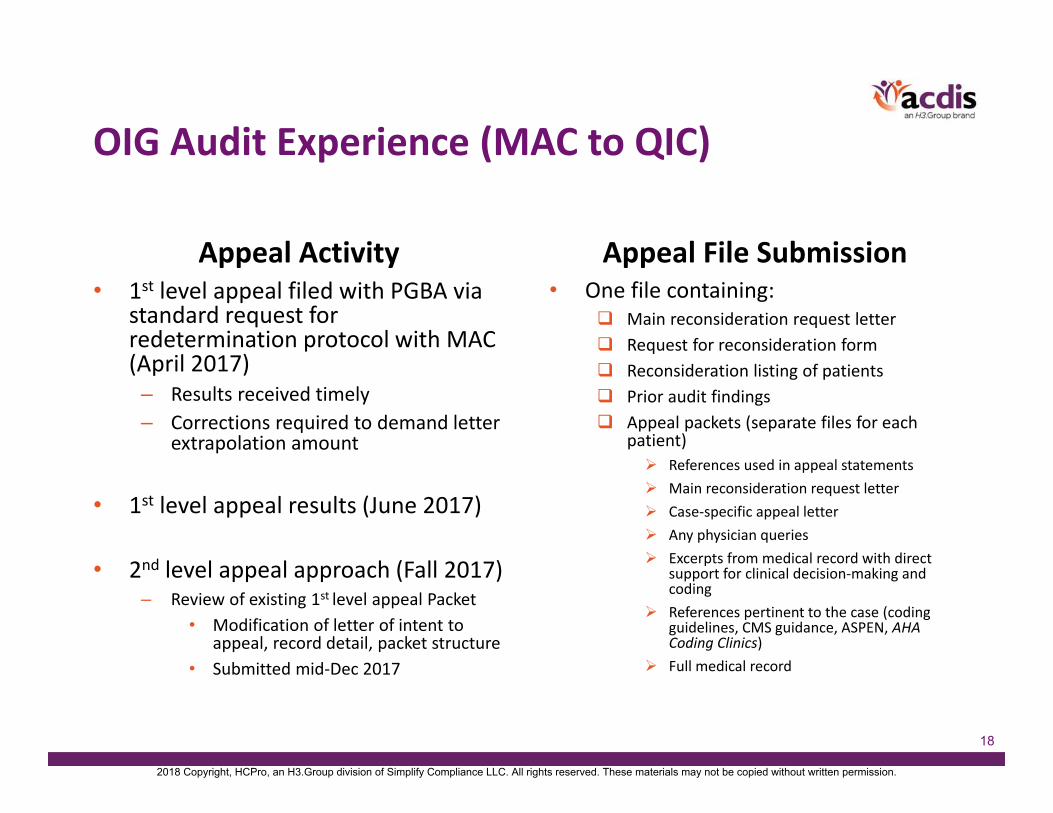
OIG Audit Experience (MAC to QIC)
Appeal Activity• 1st level appeal filed with PGBA via
standard request for redetermination protocol with MAC (April 2017)– Results received timely– Corrections required to demand letter
extrapolation amount
• 1st level appeal results (June 2017)
• 2nd level appeal approach (Fall 2017)– Review of existing 1st level appeal Packet
• Modification of letter of intent to appeal, record detail, packet structure
• Submitted mid‐Dec 2017
Appeal File Submission• One file containing:
Main reconsideration request letter Request for reconsideration form Reconsideration listing of patients Prior audit findings Appeal packets (separate files for each
patient) References used in appeal statements Main reconsideration request letter Case‐specific appeal letter Any physician queries Excerpts from medical record with direct
support for clinical decision‐making and coding
References pertinent to the case (coding guidelines, CMS guidance, ASPEN, AHA Coding Clinics)
Full medical record
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

19
Audit Results and Analysis
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

20
https://oig.hhs.gov/oas/reports/region3/31500011.asp
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.
21
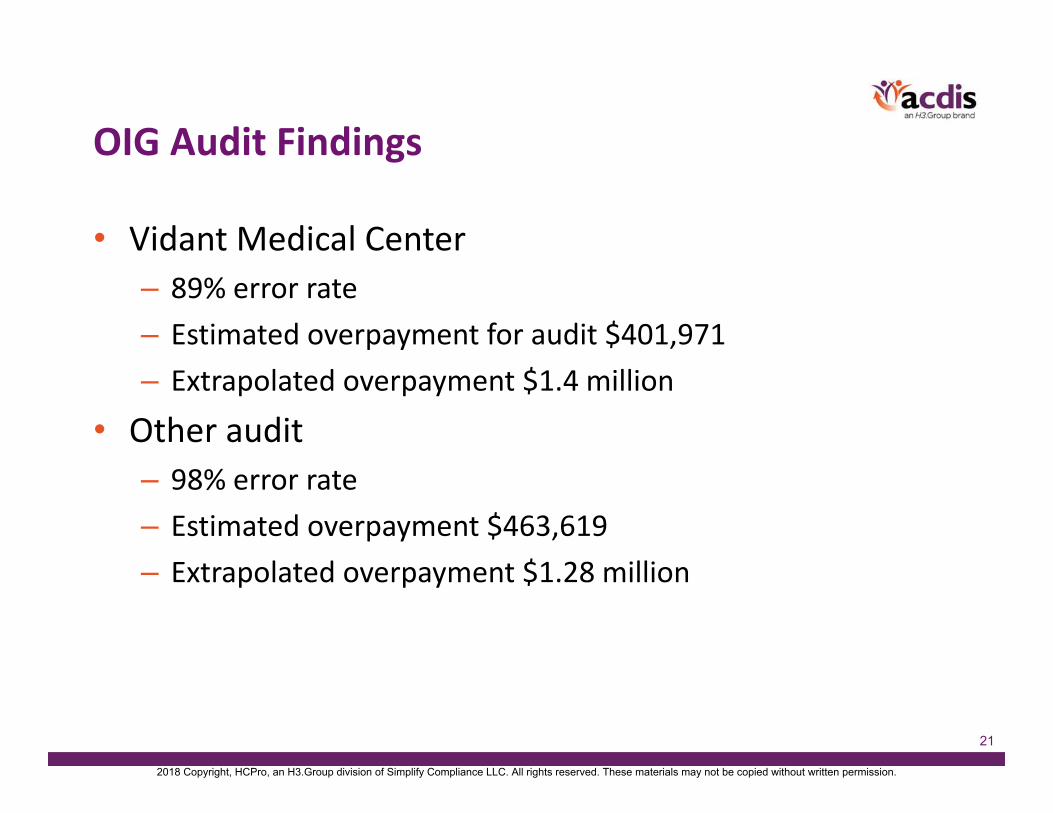
OIG Audit Findings
• Vidant Medical Center– 89% error rate– Estimated overpayment for audit $401,971– Extrapolated overpayment $1.4 million
• Other audit– 98% error rate– Estimated overpayment $463,619– Extrapolated overpayment $1.28 million
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.
22
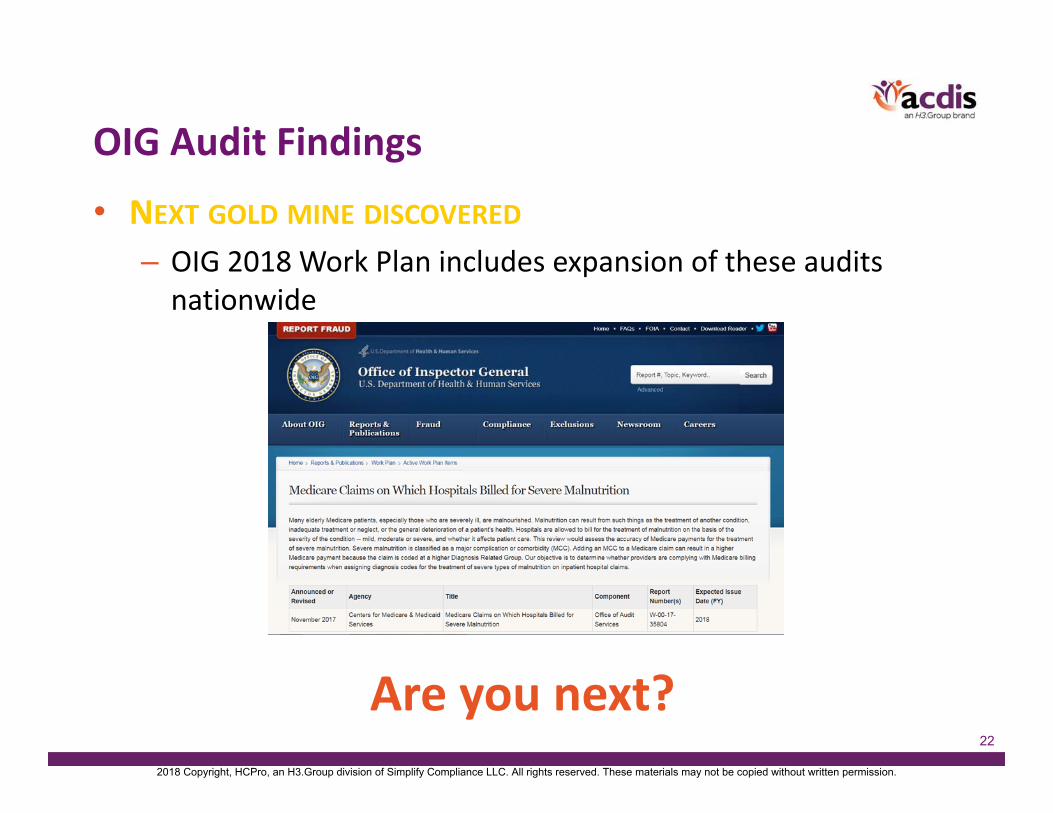
OIG Audit Findings
• NEXT GOLD MINE DISCOVERED
– OIG 2018 Work Plan includes expansion of these audits nationwide
Are you next?2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.
23
Denial Rationale Breakdown
• Coding denials – 45 claims– Code 261 (Nutritional marasmus) was submitted, but the patient
did not have nutritional marasmus– The patient had malnutrition, but it was not treated “enough” or
did not impact the stay enough to be reported as a diagnosis– The patient had malnutrition but it was due to or an integral part
of another condition and should not be separately reported as a diagnosis
• Clinical validation denials – 44 claims– The patient did not have malnutrition in any form– The patient had a form of malnutrition, but not the type of
malnutrition that was coded
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

24
Denial Rationale FrequencyRationale Category Primary
CasesTotal Cases
The patient had malnutrition, but it was not treated “enough” or did not impact the stay enough to be reported as a diagnosis
Coding 30 40
The patient did not have malnutrition in any form Clinical Validation 29 31
Code 261 (Nutritional marasmus) was submitted, but the patient did not have nutritional marasmus Coding 4 22
The patient had a form of malnutrition, but not the type of malnutrition that was coded
Clinical Validation 15 18
The patient had malnutrition but it was due to or an integral part of another condition and should not be separately reported as a diagnosis
Coding 11 18
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.
25
Malnutrition Not Treated or Impactful “Enough”
• Reporting additional diagnoses – “For reporting purposes the definition for “other diagnoses” is interpreted as additional conditions that affect patient care in terms of requiring:• Clinical evaluation; or• Therapeutic treatment; or• Diagnostic procedures; or• Extended length of hospital stay; or• Increased nursing care and/or monitoring”
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

26
Case Example: Not Treated EnoughDENIAL RATIONALE
Did not meet Medicare coverage criteria as billed with diagnosis code 261 (Nutritional marasmus). She had a chronic PEG tube. There was no new intervention, no new treatment beyond using the established PEG, and no impact on the length of stay. Criteria has not been met for the inclusion of marasmus as a secondary diagnosis. The focus of care was on hypoglycemia.
CLINICAL BACKGROUND
Pt with DM, CVA, Dysphagia, and PEG. Weight from 150 lbs to 111 lbs. Not eating well, not taking supplemental tube feeds. PE: Cachectic, thin, frail. Dietitian eval: severe malnutrition. Less than 75% of estimated energy needs for greater than a month, severe loss of subcutaneous fat in the triceps region, weight loss of 14%/6mo. Documented by MD as severe malnutrition in discharge summary.
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

27
Case Example: Not Treated Enough
Clinical evaluation; or
This patient underwent a nutritional consult on 4/23/15 in which the nutritionist stated the patient met criteria for severe malnutrition in the setting of chronic illness based on energy < 75% of estimated energy needs for > 1 month along with severe loss of subcutaneous fat in the triceps region and a 67% weight loss over the past 2 years
In the H&P the physician documented the patient to have malnutrition with a documented weight loss of 14% in 6 months (wt. 11/4/14 was 55.6 kg with wt. 4/22/15 at 47.492 kg)
Therapeutic treatment; or PEG feedings with recommendations
Medication changes for appetite stimulation
Diagnostic procedures; or
Extended LOS; or
Increased nursing care and/or monitoring
Monitoring performed by dietetics team
Reportability Standards
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

28
AHA Letter of Support
• “Neither the ICD‐9‐CM classification, the ICD‐9‐CM Official Guidelines for Coding and Reporting, nor Coding Clinic for ICD‐9‐CM specify a required level of treatment to warrant code assignment for diagnosis code 261 or any other diagnosis code as long as the condition meets the definition of a reportable diagnosis. As stated in the ICD‐9‐CM Official Guidelines for Coding and Reporting:
For reporting purposes the definition for “other diagnoses” is interpreted as additional conditions that affect patient care in terms of requiring:• clinical evaluation; or• therapeutic treatment; or• diagnostic procedures; or• extended length of hospital stay; or• increased nursing care and/or monitoring.”
(Reference: Official Guidelines 2011, page 91, and 2002, page 48)
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.
29
Patient Did Not Have Any Form of Malnutrition
• Confusion around basis for denials– Clinical criteria, if any, used by reviewer was not disclosed– OIG didn’t know either– CMS has not adopted a particular clinical guideline for evaluation, identification, and diagnosis of malnutrition
– CMS has not published any clarifying guidance on the use of 261 and 262
• What are hospitals to do in absence of published guidance?
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

30
Case Example: Without Any Form of MalnutritionDENIAL RATIONALE
The patient was admitted due to diarrhea. Management was focused on diarrhea with colonoscopy and stool studies. She was provided dietary support consistent with poor intake and dialysis but not specific to her nutrition state. Hospitalization was a consequence of her diarrhea and her nutrition state did not complicate the course. She was made nothing by mouth during her stay and no intervention was done to address the nutrition. Nutrition should not be part of the secondary diagnosis.
CLINICAL BACKGROUND
67 yo. Admitted with fall and weakness, has diabetes, and ESRD (end stage renal disease) status post renal transplant with rejection. She was recently discharged for failure to thrive, started back on dialysis. Complained of diarrhea for several weeks. PE: cachectic with BMI of 15.56. Patient was noted to have a 10 lb weight loss, consuming only 50% of meals. Nutrition focused physical exam: severe muscle depletion in the temporalis, clavicle, and interosseous regions. The patient was continued on Megace. Had hypokalemia, hypomagnesemia, and hypophosphatemia, concerning for refeeding syndrome. Monitored and repleted. Treated with high calorie nutritional supplements, vitamin and minerals, electrolyte supplements. PEG was considered but declined at that time.
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

31
Case Example: Without Any Form of MalnutritionASPEN‐AND Severe Malnutrition Criteria Met in the Context of Chronic Illness:
2 of 6 Required for the Diagnosis of Severe Malnutrition
Category Criteria Present Documentation
Weight Loss
>5% over 1 month >7.5% over 3 months >10% over 6 months >20% over 1 year
Energy Intake≤ 75% of estimated energy requirement for ≥ 1 month
YesPt consuming less than 75% of energy needs for greater than 1 month – RDN notes 11/20/14; 11/24/14
Body Fat Severe Depletion
Muscle Mass Severe Depletion YesSevere muscle wasting assessed in the temporalis, clavicles, and interosseous muscles – RDN notes 11/20/14; 11/24/14
Fluid Accumulation
Severe
Grip Strength Reduced for Age/Gender
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

32
Coding Denials• The patient had malnutrition but it was due to or an integral
part of another condition and should not be separately reported as a diagnosis– Section I. A. 6. of the ICD‐9‐CM Official Guidelines for Coding and
Reporting states: • Certain conditions have both an underlying etiology and multiple body system manifestations due to the underlying etiology. For such conditions, the ICD‐9‐CM has a coding convention that requires the underlying condition be sequenced first followed by the manifestation. Wherever such a combination exists, there is a “use additional code” note at the etiology code, and a “code first” note at the manifestation code. These instructional notes indicate the proper sequencing order of the codes, etiology followed by manifestation.1
– No published direction from UHDDS or AHA Coding Clinic that malnutrition is integral to other disease processes and should not be reported separately
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

33
Coding Denials• The patient had a form of malnutrition but not the type of
malnutrition that was reported– Reviewers claimed that another code for malnutrition was more
appropriate• Suggestion to review codes to unspecified or lower degree of specificity
ICD‐9‐CM Official Guidelines for Coding and Reporting dictate that diagnoses must be coded to the highest degree of specificity.
CMS also clarified this requirement, stating: The physician should code the ICD‐9‐CM code that provides the highest degree of accuracy and completeness. In the context of ICD‐9‐CM coding, the “highest degree of specificity” refers to assigning the most precise ICD‐9‐CM code that most fully explains the narrative description of the symptom or diagnosis.
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

34
Coding Denials• Code 261 (Nutritional marasmus) was submitted, but the
patient did not have nutritional marasmus– The OIG failed to recognize and acknowledge that code 261 (Nutritional
marasmus) includes additional malnutrition conditions:
An example of direction for coding severe malnutrition with code 261 can be found in AHA Coding Clinic, Third Quarter 2012, Page 10, effective with discharges September 15, 2012, which states:
“If provider documentation indicates that the malnutrition has progressed from moderate to severe, assign code 261, Nutritional Marasmus, for Severe Malnutrition.”
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

35
Clinical Perspective and Directing Guidance
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

36
Clinical Impact of Identifying and Treating Malnutrition
• 1 in 3 patients enter a hospital malnourished
• Malnourished patients:– 2x more likely to develop a pressure ulcer in a hospital– Hospitalized an average of 2 days longer than those screened and treated early– Comprise 45% of patients that fall in a hospital– Have 3x the risk for surgical site infection
• Benefits of nutrition intervention:– 25% reduction in pressure ulcer incidence– 28% decrease in avoidable readmissions– 14% fewer overall complications– ~2 day reduction in average length of stay
Recommended further reading:• Tappenden KA, Quantara B, Parkhurst ML, Malone AM, Fanjiang G, Ziegler TR. Critical role of nutrition in improving quality of care:
an interdisciplinary call to action to address adult hospital malnutrition. JPEN J Parenter Enteral Nutr. 2013;37(4):482‐497. • The Facts on Malnutrition. Available from: http://malnutrition.com/getinspired/factsheet. Accessed January 13, 2016.
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.
37
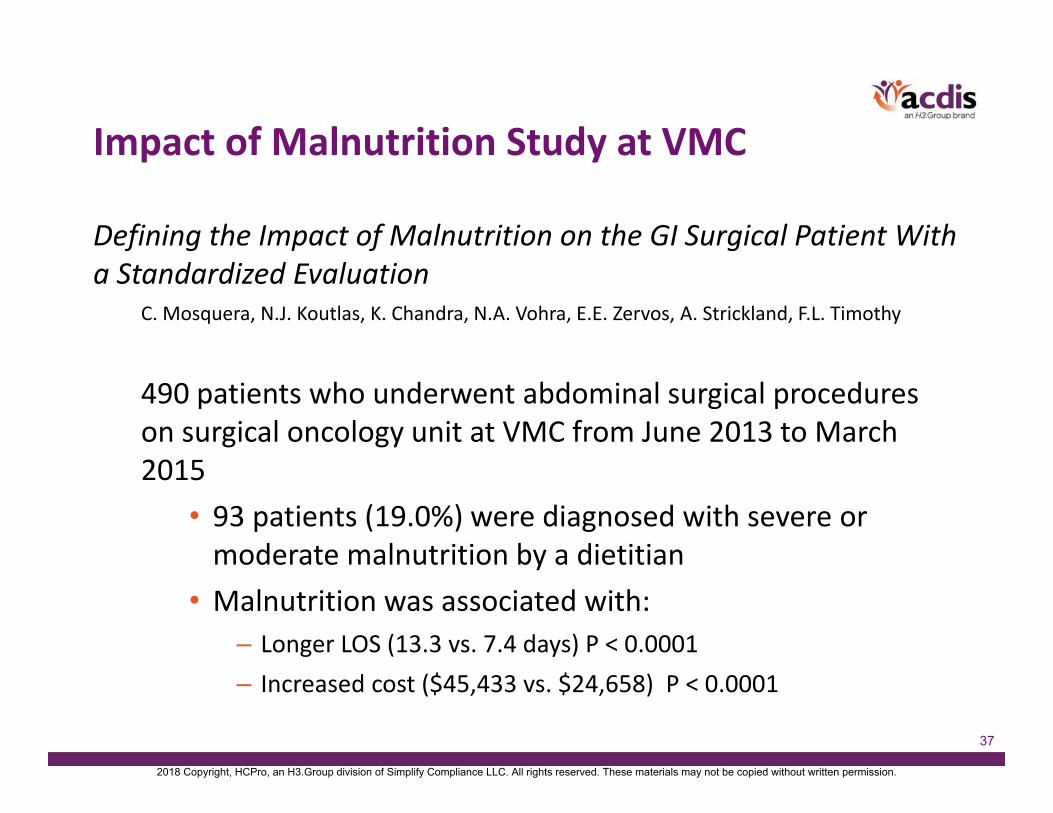
Impact of Malnutrition Study at VMC
Defining the Impact of Malnutrition on the GI Surgical Patient With a Standardized Evaluation
C. Mosquera, N.J. Koutlas, K. Chandra, N.A. Vohra, E.E. Zervos, A. Strickland, F.L. Timothy
490 patients who underwent abdominal surgical procedures on surgical oncology unit at VMC from June 2013 to March 2015
• 93 patients (19.0%) were diagnosed with severe or moderate malnutrition by a dietitian
• Malnutrition was associated with: – Longer LOS (13.3 vs. 7.4 days) P < 0.0001– Increased cost ($45,433 vs. $24,658) P < 0.0001
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

38
Joint Commission Stance on Malnutrition
In 1995 The Joint Commission partnered with ASPEN, the American Society of Clinical Nutrition (now the American Society of Nutrition [ASN]), and the American Dietetic Association (now the Academy of Nutrition and Dietetics) to develop survey accreditation standards that emphasized interdisciplinary delivery of nutrition care and required that all patients have a nutrition screening within 24 hours of admission.
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

39
Joint Commission Stance on Malnutrition
The Joint Commission Journal on Quality and Patient Safety
ForumAddressing Disease‐Related Malnutrition in
Hospitalized Patients: A Call for a National Goal
October 2015, Volume 41, Number 10
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.
40
Joint Commission Stance on Malnutrition
Actions to Take1. Each clinician on the interdisciplinary care team should participate in the execution of the nutrition care plan. • Teams should include a physician, dietitian, nurse, and
pharmacist, at a minimum.2. Develop systems to quickly diagnose all malnourished patients and those at risk. • If malnutrition is present, it should be included as one of the
patient’s coded diagnoses.3. Develop nutrition care plans in a timely fashion and implement comprehensive nutrition interventions (optimally within 48 hours of identification of the malnourished patient).
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

41
CMS IPPS Final Rule May 2015
We believe that RDs (clarified as qualified nutrition professional) are the professionals who are best qualified to assess a patient’s nutritional statusand to design and implement a nutritional treatment plan in consultation with the patient’s interdisciplinary care team. In order for the patient to receive timely nutritional care the RD must be viewed as an integral member of the hospital interdisciplinary care team, one who, as the team’s clinical nutrition expert, is responsible for the patient’s nutritional diagnosis and treatment in light of the patient’s medical diagnosis.”
“All patient diets including therapeutic diets must be ordered by a practitioner responsible for the care of the patient, or by a qualified dietitian … hospitals that choose to grant these privileges to RDs may achieve a higher quality of care for their patients by allowing these professional to fully and efficiently function as important members of the hospital patient care team in the role for which they were trained.”
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

42
IPPS Final Rule 2018 Proposed VBP Measures
National Quality Forum (NQF) Number
Centers for Medicare & Medicaid
Services (CMS) Number
Electronic Clinical Quality Measure (eCQM)
NQF #3087 MUC16‐294 Completion of a Malnutrition Screening Within 24 Hours of Admission
NQF #3088 MUC16‐296Completion of a Nutrition Assessment for Patients Identified as At‐Risk for Malnutrition Within 24 Hours of a Malnutrition Screening
NQF #3089 MUC16‐372Nutrition Care Plan for Patients Identified as Malnourished After a Completed Nutrition Assessment
NQF #3090 MUC16‐344 Appropriate Documentation of a Malnutrition Diagnosis
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

43
Appropriate Documentation of Malnutrition Diagnosis MeasureThe Appropriate Documentation of a Malnutrition Diagnosis measure (MUC16‐344) assesses whether patients age 65 years and older, who are found to be malnourished on the nutrition assessment, have adequate documentation of a malnutrition diagnosis in their medical record. This measure is important because there is often a disconnect between screening for malnutrition and documentation of a diagnosis of malnutrition, which is necessary for appropriate follow‐up after hospital discharge. Data analyzed from the Healthcare Cost and Utilization Project (HCUP), a nationally representative data set describing U.S. hospital discharges, indicated that approximately 3.2% of hospital discharges in 2010 included malnutrition as a diagnosis. However, this same research article notes that the prevalence of a malnutrition diagnosis may be significantly higher as past researchers, using validated screening tools, indicate a significantly higher prevalence of undiagnosed malnutrition in the hospital, ranging from 33% to 54%.
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

44
Joint Commission Comments
The Joint Commission appreciates the opportunity to submit comments in support of inclusion of this suite of malnutrition measures in the Hospital Inpatient Quality Reporting Program (MUC16‐294, MUC16‐296, MUC16‐344, and MUC16‐372) addressing malnutrition developed by Avalere and the Academy of Nutrition and Dietetics. Joint Commission standards have long reflected the importance of nutrition screening, assessment of at‐risk hospitalized patients, diagnosis of malnutrition, and appropriate intervention. Malnutrition is an ongoing healthcare issue with demonstrated impacts on patient outcomes. The Joint Commission welcomes the advent of performance measures to quantify the degree to which these best practices are carried out.
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

45
Summary
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.
46
Where Do We Stand Today?
• Appeal status• Clinical initiatives have continued• Coding education and compliance remains a high priority
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.
47
Key Points and Takeaways
• Develop and maintain a multidisciplinary approach to diagnosing and coding malnutrition
• Maintain a current and consistent definition of malnutrition
• Educate coding and clinical staff• Maintain coding compliance and consistency for malnutrition
• Prepare for the long haul if you are audited• DO WHAT IS BEST FOR PATIENTS
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

48
Want More In‐Depth Information?
• ACDIS May 2016 presentation link (ACDIS members only): – https://acdis.org/resources/2016‐conference‐track‐1‐malnutrition‐pairing‐your‐dietitians‐diagnose‐document‐and‐capture
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.

49
Thank you. Questions?
[email protected]@[email protected]
In order to receive your continuing education certificate(s) for this program, you must complete the online evaluation. The link can be found in the continuing education section at the front of the program guide.
2018 Copyright, HCPro, an H3.Group division of Simplify Compliance LLC. All rights reserved. These materials may not be copied without written permission.