malnutrition in hospitalized patients; what is it and how
TRANSCRIPT

Malnutrition Problems 0907(1)602
Malnutr i t ion in Hospita l i zed
Pat ients ; what i s i t and how to
manage i t .
Lina Mohamed Hassan, Mai Alaa El-Menebawy,
Mona Mohaseb Hassan Mohaseb, Nancy Ahmed
Nasser, Shereen Mohamed Kamal, 2020

1
Malnutrition Problems 0907(1)602
Table of Contents
1. Abstract ………………………………….……….. 3
2. Definition of Hospital Malnutrition ……………. 4
3. Causes of Hospital Malnutrition ……………….. 4
4. Vulnerable groups ………………………………. .5
5. Risk Factors ……………………………………….5
6. Nutrition Screening and Assessment ……………. 7
7. Diagnosis ………………………………………….. 9
8. Impact of Malnutrition …………………………... 9
9. Prevention ………………………………………... 12
10. Treatment Strategies…………………………… 16
11. Appendices ………………………………..............20
12. References …………………………………………25

2
Malnutrition Problems 0907(1)602
Abstract
Malnutrition is a debilitating and highly prevalent condition in the acute
hospital setting. Malnutrition is associated with many adverse outcomes
including depression of the immune system, impaired wound healing, muscle
wasting, longer lengths of hospital stay, higher treatment costs and increased
mortality. Referral rates for dietetic assessment and treatment of malnourished
patients have proven to be suboptimal, thereby increasing the likelihood of
developing such aforementioned complications. Nutrition risk screening using
a validated tool is a simple technique to rapidly identify patients at risk of
malnutrition, and provides a basis for prompt dietetic referrals. Unidentified
malnutrition not only heightens the risk of adverse complications for patients,
but can potentially result in foregone reimbursements to the hospital through
casemix-based funding schemes. It is strongly recommended that mandatory
nutrition screening be widely adopted in line with published best-practice
guidelines to effectively target and reduce the incidence of hospital
malnutrition.Nutritional screening and assessment are readily available and
inexpensive procedures that provide crucial information to develop nutrition
care plans. These plans should determine the need for dietary modifications,
enteral or parenteral nutrition, strategies for monitoring adverse events and
therapeutic success, and parameters for therapy termination.

3
Malnutrition Problems 0907(1)602
Definition of Malnutrition
Malnutrition is a broad term that can be used to describe any imbalance in nutrition.
Recently, the definition of malnutrition has been clarified by the European Society of
Parenteral and Enteral Nutrition (ESPEN) to highlight the differences between cachexia,
sarcopenia (loss of muscle mass and function) and malnutrition. Cachexia can be defined as a
“multifactorial syndrome characterized by severe body weight, fat and muscle loss and
increased protein catabolism due to underlying disease(s)”. Therefore, malnutrition seen in
hospitalized patients is often a combination of cachexia (disease-related) and malnutrition
(inadequate consumption of nutrients) as opposed to malnutrition alone.
Causes of malnutrition in hospitalized patients
Many patients are already malnourished at the point of admission, while others
become malnourished during their hospital stay. Etiologies include alterations in the intake,
digestion, absorption, and/or metabolism of food. Risks include GI disorders, chronic disease,
malignancies, lower socioeconomic status, psychological disorders, alcohol and drug abuse,
older age, and lower levels of education.
Several disease states and acute events predispose patients to malnutrition, the degree of
which is usually determined by the severity of the illness. The most obvious are those that
prevent oral food intake, such as: oral cancer, tumors or strictures in the throat or esophagus,
stroke, and degenerative neurologic disorders that result in dysphagia. Trauma patients and
others who are ventilator dependent rely on the timely initiation of nutrition support.
Conditions such as chronic obstructive pulmonary disease, chronic infections, and cancer can
result in increased metabolic demand and weight loss due to cachexia and poor oral intake.
Patients with GI disorders are among those who are most prone to developing
malnutrition. Patients with gastroparesis, gastric outlet or bowel obstruction, and motility
disorders present with varied degrees of malnutrition depending on how long they have
waited to seek medical care. Surgical resections of the GI tract for cancer or Crohn’s disease
can result in severe maldigestion and malabsorption of nutrients, as can chronic digestive
disorders such as cystic fibrosis. Gastric bypass procedures, while effective for weight loss,
predispose patients to serious micronutrient deficiencies. Chronic liver disease can contribute
to poor nutrient digestion and absorption, and patients with pancreatitis often present with
malnutrition.
Even for patients who can eat orally, nutritional intake often decreases during
hospitalization. Patients are required to be NPO prior to many tests and procedures, as well as

4
Malnutrition Problems 0907(1)602
before and after surgery. Delays or the need for several procedures result in prolonged periods
without nutrition. Patients’ appetites usually decrease during illness due to pain, nausea,
weakness, and altered mood or mental status, and they can become dissatisfied with repetitive
menu cycles, dietary restrictions, and the food, which may not be the type they prefer.
Vulnerable Groups
There is an increased risk of malnutrition observed in patients with dentures,
gastrointestinal disorders, dementia and depression as well as in patients with high loss of
body fat, decreased food supply, low BMI, bedridden patients, liver disease and
gastrointestinal symptoms.
Malnutrition was also common in hospitalized patients, and resulted in longer
hospitalization and associated lower survival rate. The rate of malnutrition tended to be higher
when the patient was older than 70 years old or hospitalized for medical treatment or
diagnostic work-up compared to elective surgery.
Who are at Risk of malnutrition?
Older people over the age of 65, particularly if they are living in a care home or nursing
home or have been admitted to hospital
People with long-term conditions, such as diabetes, kidney disease, chronic lung disease
People with chronic progressive conditions – for example, dementia or cancer
People who abuse drugs or alcohol
There are also social factors that can increase the risk of malnutrition including:
Poverty
Social isolation
Cultural norms – for example, hospitals and care homes may not always provide food that
meets particular religious or cultural needs and so increase the risk of malnutrition whilst a
person is away from their normal environment
Physical factors can also increase the risk of malnutrition. For example:
Eating may be difficult because of a painful mouth or teeth
Swallowing may be more difficult (a stroke can affect swallowing) or painful
Losing your sense of smell or taste may affect your appetite
Being unable to cook for yourself may result in reduced food intake
Limited mobility or lack of transport may make it difficult to get food

5
Malnutrition Problems 0907(1)602
The etiology of hospital malnutrition is multifactorial and includes causes related to
the disease itself: intake reduction, response to aggression, mechanical obstruction of the
gastrointestinal tract, pharmaceutics, advanced age, an increase in requirements, an increase
of its losses, and inflammatory conditions; causes related to hospitalization: a change in
habits, reactive emotional situations, complementary examinations, surgical treatments,
pharmaceutics, chemotherapy-radiotherapy, hospitality; causes related to the medical team:
misuse of therapeutic fasts, lack of nutritional assessment, lack of intake control, dilution of
responsibilities; causes related to health authorities: lack of nutritionists, absence of nutrition
units, lack of dietician-nutritionist acknowledgement, and lack of a coordinated and
multidisciplinary work.
Hospital malnutrition usually enters a vicious cycle, despite the fact that the patient
has increased requirements, they tend to not be met, causing depletion and exhaustion of
energy and nutrimental reserves and thus increasing his/ her consumption needs. There are
reports confirming that hospitalized patients, in general, do not consume the necessary
amount of energy and nutriments to cover their requirements, which worsens their nutritional
condition.

6
Malnutrition Problems 0907(1)602
Nutrition Screening and Assessment
Numerous nutrition screening and assessment tools exist to identify risk of, and
diagnose, malnutrition.
Nutritional risk screening tools are very helpful in the daily routine to detect potential
or manifest malnutrition in a timely manner. Such tools should be easy to use, quick,
economical, standardized, and validated. Screening tools should be both sensitive and
specific, and if possible, predictors of the success of the nutritional therapy. Nutritional
screening should be part of a defined clinical protocol that results in a plan of action if the
screening result is positive.
Screening should be performed within the first 24–48 h after hospital admission and at
regular intervals thereafter (e.g., weekly), in order to rapidly and accurately identify
individuals who should be referred to the nutrition specialist (e.g., dietitian, expert clinician)
for further assessment.
Nutritional assessment should be performed in patients identified as at nutritional risk
according to the first step (i.e., screening for risk of malnutrition). Assessment allows the
clinician to gather more information and conduct a nutrition-focused physical examination in
order to determine if there is truly a nutrition problem, to name the problem, and to determine
the severity of the problem. The data collected in a nutritional assessment are often similar to
data collected in the screening process, but in more depth. Screening assesses risk whereas
assessment actually determines nutritional status. A nutritional assessment includes four main
components, summarised as ‘ABCD’: Anthropometric Measures, Biochemical and laboratory
measures, Clinical Methods and Dietary Evaluation Methods.
Anthropometric indicators: According to standardized procedures and cutoff points
defined in the literature, the body mass index (BMI) grading was used both for adults and the
elderly. According to Frisancho (1990) and Burr & Phillips (1984), arm circumference (AC),

7
Malnutrition Problems 0907(1)602
triceps skinfold (TSF) and arm muscle circumference (AMC) were classified by percentiles
grades. Calf circumference (CC) was classified according to WHO definition.
Laboratory indicators:There is no single parameter that can thoroughly assess
nutritional status or monitor nutritional therapy. However, a set of laboratory parameters in
the clinical routine (e.g., complete blood count, lipid profile, electrolytes, liver parameters)
may provide valuable information about a patient’s nutritional status (e.g., proof of nutrient
deficiency, information about the etiology of malnutrition, follow-up nutritional therapy),
about the severity and activity of the disease, and about changes in body composition.
Laboratory values are mostly delayed and costly, and largely dependent on the
analytic method and the analyzing laboratory. Additionally, numerous non-nutrition-related
factors may influence the laboratory parameters (e.g., inflammatory markers such as CRP),
leading to distorted values. Thus, laboratory values must always be interpreted within the
clinical context. (Appendix table 1.)
Nutrition Screening and Assessment tools
The Malnutrition Universal Screening Tool (MUST)
The MUST is a reliable screening tool to identify malnourished individuals in all care
settings (hospitals, nursing homes, home care, etc.); however, it has not been validated in
children or renal patients. (Appendix figure 1.)
The Mini Nutrition Assessment (MNA)
MNA was developed specifically for use among elderly patients (≥65 years) in
hospitals, nursing homes and the community as it is more likely to identify risk of developing
undernutrition, and undernutrition at an early stage, since it also includes physical and mental
aspects that frequently affect the nutritional status of the elderly, as well as a dietary
questionnaire. (Appendix figure 2.)
Nutritional Risk Screening (NRS-2002)
The purpose of the NRS-2002 system is to detect the presence of undernutrition and
the risk of developing undernutrition in the hospital setting. It contains the nutritional
components of MUST, and in addition, a grading of severity of disease as a reflection of
increased nutritional requirements. (Appendix table 2.)
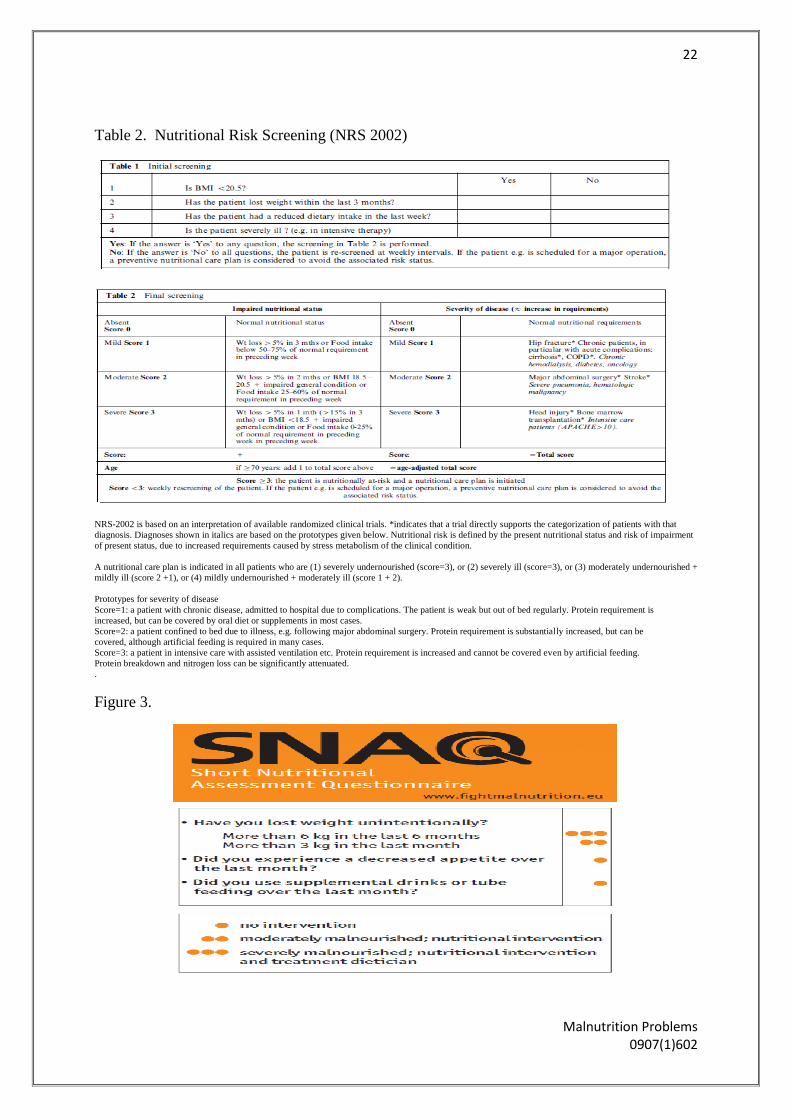
The four item Short Nutrition Assessment Questionnaire (SNAQ)
SNAQ was developed to diagnose malnutrition in hospitalised patients.It is a
Quick and easy-to-use screening tool for hospitalized patients. (Appendix figure 3.)
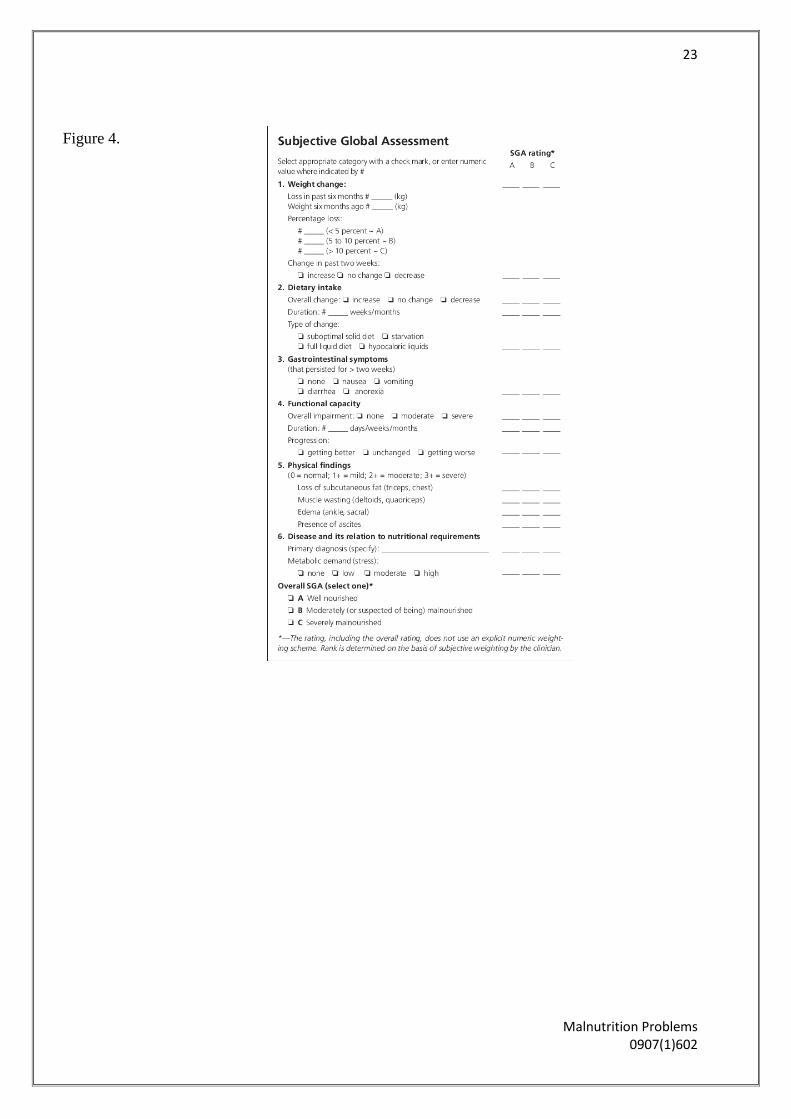
Subjective Global Assessment (SGA)

8
Malnutrition Problems 0907(1)602
SGA is one of the most commonly used nutrition assessment tools, and assesses
nutrition status via completion of a questionnaire.
A limitation of using SGA is that it only classifies subjects into three general groups,
and it does not reflect subtle changes in nutritional status. Furthermore, it is subjective, does
not account for biochemical values (e.g., visceral protein levels) (appendix figure 4.)
How to diagnose malnourished patients?
According to the A.S.P.E.N clinical characteristics:
Energy intake
Interpretation of weight loss
Physical findings
Body fat
Muscle mass
Fluid accumulation
Reduced grip strength
Malnutrition and Its Impact :
Malnutrition has often been referred to as the “skeleton in the hospital closet”, as it is often
overlooked, undiagnosed and untreated. Despite this, the negative consequences of

9
Malnutrition Problems 0907(1)602
malnutrition have been widely reported in the literature, and can be separated into two main
categories: consequences for the patient and consequences for the health care facility.
Consequences for the Patient:
Malnutrition has been shown to cause impairment at a cellular, physical and
psychological level This impairment is dependent on many factors, including the patient’s age,
gender, type and duration of illness, and current nutritional intake. On a cellular level,
malnutrition impairs the body’s ability to mount an effective immune response in the face of
infection, often making infection harder to detect and treat It also increases the risk of pressure
ulcers, delays wound healing, increases infection risk, decreases nutrient intestinal absorption,
alters thermoregulation and compromises renal function
On a physical level, malnutrition can cause a loss of muscle and fat mass, reduced
respiratory muscle and cardiac function, and atrophy of visceral organs It has been shown that
an unintentional 15% loss of body weight causes steep reductions in muscle strength and
respiratory function, while a 23% loss of body weight is associated with a 70% decrease in
physical fitness, 30% decrease in muscle strength and a 30% rise in depression.
At a psychological level, malnutrition is associated with fatigue and apathy, which in
turn delays recovery, exacerbates anorexia and increases convalescence time.
It is widely reported in the literature that malnutrition is associated with an increased
length in hospital stay One study conducted in the United States looked at adult patients
hospitalised for more than 7 days and examined the impact nutritional decline had on
outcomes, including LOS The results showed that patients who were admitted with some
degree of malnutrition, and those patients who experienced a decline in nutritional status
during their admission, had significantly longer hospital stays (by an average of 4 days) than
patients both admitted and discharged as well nourished. Similarly, a study conducted in
Australia found a significantly greater difference of 5 days between the LOS of malnourished
and well-nourished patients
In addition to a longer LOS, malnourished patients are more prone to experiencing
complications during their period of hospitalisation than patients who are in a well-nourished
state .Complications can occur when an unexpected accident or disease adds to a pre-existing
illness without being specifically related to the illness . For example, one study that assessed
the nutritional status of patients preoperatively found that malnourished patients had
significantly higher rates of both infectious and non-infectious complications . Following on

10
Malnutrition Problems 0907(1)602
from a higher complication risk, as mentioned prior malnutrition has also been shown to be
associated with an increase in mortality rates.
Despite the multitude of evidence indicating that patients who are nutritionally
compromised suffer worse outcomes, it is difficult to control for disease severity in the clinical
setting and thus definitively conclude that malnutrition alone is a cause of these outcomes. The
fact that numerous studies internationally, in a wide variety of clinical settings and patient
groups, all report similar findings lends strength to the premise that malnutrition is detrimental
in terms of clinical outcome. The high prevalence rates of malnutrition in the hospital setting
indicate that such negative outcomes as longer hospital stay, higher complication and infection
rates, and mortality would be highly prevalent also. It is therefore not surprising that
malnutrition has significant secondary effects to health care facilities.
Consequences for the Health Care Facility:
Malnutrition places additional stress on acute health care facilities. As previously
stated, malnourished patients often have higher rates of infections and pressure ulcers (and
consequently require greater nursing care), require more medications, are less independent due
to muscle loss and consequently have longer lengths of hospital stay .All these issues
combined indirectly increase hospital costs associated with treating the patient, secondary to
the management of their primary medical reason for admission.
Malnutrition also has an indirect effect on health care costs by way of the casemix
funding system, as exists in much of Australia and other countries around the world. Under
casemix-based funding, once a patient is discharged, their medical notes are audited by
medical coders and their major diagnosis, surgeries, co-morbidities, complications and other
interventions are recorded and a Diagnosis Related Group (DRG) is assigned. In Australia at
least, hospitals are subsequently reimbursed for the patient admission based on the DRG.
Malnutrition, when documented as a co-morbidity or complication, has the ability to influence
a DRG, often resulting in a “higher’ classification which has the potential to attract greater
hospital reimbursement
Two Australian studies have reported estimates of unclaimed reimbursements from
patient admissions where malnutrition was not recorded as a co-morbidity as part of the DRG.
In Melbourne in 2009, a study used SGA to diagnose malnutrition across a large hospital-
based population and estimated an annualised deficit to the hospital in reimbursements of
AUD1,850,540 for undiagnosed or undocumented cases of malnutrition. Similarly, a study
conducted in Brisbane also used SGA to determine nutrition status in a hospital population and

11
Malnutrition Problems 0907(1)602
estimated an annualised financial loss to the hospital of AUD1,677,235 due to undiagnosed
and documented malnutrition
Two international studies, one in Germany and one in the United States, both reported
financial losses to the hospital due to unrecognised malnutrition based on a DRG funding
system. In the German study, SGA was used to define malnutrition and reported a 19% rate of
malnutrition in the patient population, an increased LOS of 4 days in the malnourished patient
group, and an annual financial shortfall of €35,280 due to unrecognised malnutrition
.Similarly, the American study reported a loss of greater than USD86,000 after conducting a
retrospective audit of patient medical charts
Other studies have also shown increased financial costs to health care facilities due to
untreated malnutrition based simply on the increased LOS associated with malnutrition. To
illustrate, one study found that patients at risk of malnutrition had a 6-day longer LOS than
those not at nutritional risk, resulting in treatment costs for malnourished patients increasing
by USD1,633 per patient per hospital stay Taking the opposite approach, a similar study
looked at the cost-benefit associated with nutritional intervention in patients at risk of
malnutrition and found that early intervention using specialised nutritional products and
frequent reviews was more cost-effective than either early intervention or frequent review
alone, with an estimated saving to the health care facility of USD1,064 per patient
It seems evident by the number of researchers who have examined the relationship between
malnutrition and its effect on both patients and treatment costs, that benefits to both
individuals and hospitals exist if malnutrition is correctly identified and treated.
Prevention
Maintaining normal nutrition and preventing malnutrition from occurring during
hospitalization can be accomplished by early risk assessment, ensuring adequate nutrient
intake and escalating the need for intervention. In order to promote nutrition, decrease the risk
of developing malnutrition and actively participate in the treatment of malnutrition the
Clinical Nurse Specialist (CNS) must be prepared to intervene and develop a system that
ensures: (1) recognition of malnutrition; (2) intervention to prevent and treat malnutrition; (3)
evaluation of nutrition interventions; and (4) provision of continuity of nutrition therapy
through care transitions, at discharge, and beyond.
Patients who enter the health care system may be well nourished or may have varying
degrees of malnutrition. Regardless of a patient’s nutrition level, the risk of developing

12
Malnutrition Problems 0907(1)602
malnutrition is a threat to the majority of patients who are hospitalized. Individuals, who are
already malnourished, are at even greater risk of worsening their malnutrition state.
To prevent future harm, it is a key for care providers to quickly recognize
malnutrition, implement appropriate treatments and recognize intervening variables (personal
risk factors and/or pre-disposing factors) that may contribute to developing malnutrition.
Examples of intervening variables that contribute to malnutrition are grouped into categories
and include: 1) the duration of the illness, 2) physiological processes, 3) organ system
dysfunction, and 4) socioeconomic and environmental conditions
Malnutrition Screening
Screening for malnutrition enables the early identification of individuals at risk and an
action plan for its management to be developed. Screening should be undertaken on the
individual’s admission to a hospital ward and on a weekly basis thereafter, unless there is a
change in the patients’ clinical condition requiring this sooner. A commonly used tool in the
UK is the Malnutrition Universal Screening Tool (MUST), which was developed to identify
the risk of malnutrition in all adult patients across all healthcare settings. The tool has five
steps to be completed by ward staff.
To improve patients’ nutritional status in the hospital setting, action plans should be
implemented. The following box outlines the action plans to be implemented based on an
individual’s MUST score.
Malnutrition Universal Screening Tool (MUST) action plans
MUST score 0 = low risk of malnutrition
Repeat nutritional screening weekly
MUST score 1 = medium risk of malnutrition
Document the patient’s dietary intake for three days
If their dietary intake is adequate, repeat screening weekly
If their dietary intake is inadequate, follow local policy, set goals,
and improve and increase nutritional intake
MUST score 2 or more = high risk of malnutrition
Refer the patient to the dietician or nutrition support team
Set goals to improve and increase their overall nutritional intake
Monitor and review their care plan weekly
(Adapted from British Association for Parenteral and Enteral Nutrition 2011)

13
Malnutrition Problems 0907(1)602
It is essential for nurses to become engaged with patients’ mealtimes to assess how the
patient is managing with their eating and drinking and to ensure any potential issues are
identified quickly. However, the competing pressures of acute environments can make this
challenging. The National Patient Safety Agency introduced protected mealtimes to
encourage staff to prioritize mealtimes as an essential aspect of patient care. Its
recommendations include:
All ward staff should be involved with handing out meals and assisting patients as
required.
All non-urgent clinical activities on wards should stop during mealtimes, such as ward
rounds and dressing changes, to reduce interruptions while patients are eating.
Patients identified as being at risk of malnutrition should be monitored on a weekly
basis. Food diaries should be used for this, as well as fluid balance charts to monitor
patients’ fluid intake and output. Oral nutritional supplements and high-protein menus
should be available to increase the nutritional value of what patients consume orally.
Support from therapy services
The prevention and management of malnutrition requires a multidisciplinary team
approach to improve the patient’s nutritional status. Support from therapy services can be
beneficial in meeting specific patient needs. For example, involving speech and language
therapists (SLTs) is essential if it has been identified that dysphagia is affecting the patient’s
ability to eat and drink. SLTs may recommend exercises, swallowing techniques or texture-
modified foods and drinks to aid with eating and drinking. If an SLT has assessed a patient, it
is essential that nurses are aware of their recommendations and the level of assistance the
patient requires.
Dietetic input is important to accurately assess the patient’s nutritional requirements
and any nutritional support required. Oral nutritional supplements or enteral nutrition may be
commenced if malnutrition cannot be corrected orally. Dieticians may use anthropometric
measurements such as grip strength, triceps fold thickness and mid-upper arm circumference
to estimate how much muscle mass has been lost. This will be repeated at regular intervals to
determine any losses or gains in the patient’s muscle mass.
Occupational therapists can assist in assessing issues that prevent patients from
feeding themselves, such as reduced dexterity. There is a range of equipment and adapted
cutlery and crockery available to assist in these situations. These aids are essential in enabling
patients to maintain their independence when eating.
14
Malnutrition Problems 0907(1)602
Physiotherapists may be able to support patients who require assistance with positioning
during mealtimes. This assistance may involve moving the patient into an appropriate chair or
into the optimal sitting position in bed, if appropriate.
Catering facilities
Nurses should be aware of their healthcare organization's catering facilities. For
example, this needs to be considered for patients who have religious or cultural beliefs that
influence their diet. If certain menus, such as halal, kosher or vegan, cannot be provided
easily or do not have sufficient variety, patients are less likely to eat. Appropriate menus must
be used for any texture-modified food recommendations from SLTs or for those on special
diets such as gluten-free. Nurses should also be aware of snack menus and if there is a 24-
hour menu available. These facilities are important for patients who miss meals or prefer to
snack or eat little and often.
Volunteers
Some hospitals have introduced a programme where volunteers become dining
companions for patients who do not eat and drink because they are on their own or for those
who require encouragement. The purpose of dining companions is not only to assist patients
with eating and drinking, but also to provide social interaction. Patients’ relatives and friends
should be encouraged to do this when dining companions are not available. The aim of the
volunteers is to provide patients with additional time to prepare for their meals and provide
support at mealtimes. It is important to remember that the responsibility for delegated tasks,
such as assisting patients to eat and drink, remains with the nurse.
Disease –related malnutrition
Duration, severity and type of illness can directly influence the development of
malnutrition. For example, an acute illness that is sustained and unable to be treated
effectively can cause malnutrition. Likewise, a chronic illness, although treated, may result in
malnutrition.
Disease related malnutrition is difficult to prevent. What is preventable is the
additional burden and cost of hospital-acquired malnutrition resulting from provider
inattention to patients’ nutritional intake during hospital stay.
Nutritional therapy and counseling
A special challenge for clinical dietician in the nutritional therapy andnutritional
counselling, which is a central part of the nutritional support inthe elderly, that is the use of
effective nutrition and other strategies (motivational, educational, psychological, social, etc.).

15
Malnutrition Problems 0907(1)602
Also, the implementation ofevidence-based nutritional therapy in practice is a challenge,
becauseknowledge in thisfield is developing rapidly and there are obstacles which can slow
down or hinder theuse of the new knowledge in the practice of nutritional support.
Treatment strategies
1) Improving oral nutrition
Patients experiencing nausea should be offered anti-emetics.
Patients with dysphagia (eg, from an oesophageal stricture) may be able to eat sloppy or
liquid meals.
Swallowing disorders from neurological causes benefit from more viscous liquids, and
thickeners can be added.
Adequate pain relief may improve appetite.
Enough time should be dedicated to feeding patients who have difficulty in feeding
themselves. This can be done by nurses, healthcare assistants or relatives.
After individual evaluation and treatment of underlying causes, the next step is an
individual nutritional clinical history with changes made to patients’ diets with consideration
of patients’ individual wishes using easy-to-digest, high-energy options. Also, there are many
other general measures established in practice, such as the use of special flavor enhancers,
eating in pleasant surroundings and good company, special nutritional education for family
members providing care, encouraging physical activity between meals, or prescribing small,
frequent portions of high-energy food between meals (finger food, snacks, high-energy
drinks) throughout the day. Extra energy can also be added to patients’ diets using
economical, energy-rich additives with no odor or flavor, such as maltodextrin or specific
protein concentrates.

16
Malnutrition Problems 0907(1)602
2) Nutritional drinks/oral nutritional supplements
The addition of nutritional drinks to the diets of patients with under-/malnutrition
significantly reduced both the complication rate and mortality. These significant effects are
also seen in malnourished patients who receive additional nutritional drinks or oral nutritional
supplements during short hospital stays.
Nutritional drinks and oral nutritional supplements are available in more than 30
different flavors. They should be given between rather than at mealtimes, or even better in the
evening as supplements to patients’ diets. If a patient is only able to eat a little (e.g. geriatric
patients, tumor patients), high-calorie nutritional drinks with an enriched calorie content of
1.5 to 2.7 kcal/mL can also be offered.
3) Artificial nutrition
If all the measures mentioned above have been tried with no lasting therapeutic
benefit, supportive artificial nutrition must be considered In addition to medical indications
(underlying disease, patients’ individual health status, any comorbidities, expected prognosis,
mental/psychological status, individual patients’ wishes), ethical issues (particularly in the
case of elderly patients with multiple disorders and tumor patients in advanced stages of
illness) must also be considered on an individual basis. Clinical trials show significantly better
quality of life, in addition to a significant improvement in nutritional status, reduced
complication rates, and improved individual prognosis
Short-term access is usually achieved using nasogastric (NG) or nasojejunal (NJ) tubes at an
initial continuous feeding rate of 30 mls per hour. Percutaneous endoscopic gastrotomy (PEG)
or jejunostomy placement should be considered if feeding is planned for longer than one
month.
NG tubes:
These are the most commonly used delivery routes but depend on adequate gastric
emptying.
They allow the use of hypertonic feeds, high feeding rates and bolus feeding into the
stomach reservoir.
NJ tubes:

17
Malnutrition Problems 0907(1)602
These reduce the incidence of gastro-oesophageal reflux and are useful in the presence
of delayed gastric emptying.
Post-pyloric placement can be difficult but may be aided by intravenous prokinetics or
fibre-optic observation.
PEG tubes:a procedure in which a flexible feeding tube is placed through the
abdominal wall and into the stomach
Indications for gastrostomy include stroke, motor neurone disease, Parkinson's disease
and oesophageal cancer.
Relative contra-indications include reflux, previous gastric surgery, gastric ulceration
or malignancy and gastric outlet obstruction.
They are inserted directly through the stomach wall endoscopically or surgically,
under antibiotic cover.
Percutaneous jejunostomy tubes:
They permit early postoperative feeding and are useful in patients at risk of reflux.
They are inserted through the stomach into the jejunum, using a surgical or endoscopic
technique.
This can be difficult and has more complications
Monitoring should include the general observations and laboratory schedule
recommended for all forms of nutritional support, particularly if the patient is at high risk of
re-feeding syndrome. Consideration should also be given to:
The position of nasally inserted tubes, which should be checked before each feed by
obtaining tube aspirate of pH <5.5 on pH paper.
The function of nasal tubes and the development of erosions, which should be assessed
daily.
Gastrostomy and jejunostomy stoma sites, which should be checked each day for tube
position and signs of infection.
Feed preparations
Various nutritionally complete pre-packaged feeds are available:
Standard enteral feeds:
These contain all the carbohydrate, protein, fat, water, electrolytes, micronutrients
(vitamins and trace elements) and fibre required by a stable patient.
'Pre-digested' feeds:
18
Malnutrition Problems 0907(1)602
These contain nitrogen as short peptides or free amino acids and aim to improve
nutrient absorption in the presence of pancreatic insufficiency or inflammatory bowel
disease
The fibre content of feeds is variable and some are supplemented with vitamin K,
which may interact with other medications.
If there are contraindications against enteral nutrition, which is rare, parental catheter
systems (Broviac or Hickman catheters) can also be used.
Peripheral lines may be used to deliver short-term nutritional support, but central access is
necessary for parenteral feeding of more than two weeks' duration. Lines should be dedicated
to feeding and must not be used for drug administration or blood sampling:
Central catheters and ideally tunnelled subclavian vein central lines, inserted using the full
aseptic technique are the optimal method of access:
Parenteral nutrition solution is thrombogenic and an irritant to veins.
Central access allows delivery of more concentrated formulations into high-flow
vessels.
Peripheral administration is achieved through peripherally inserted central catheters (PICCs)
or standard cannulae, inserted with an aseptic technique:
Tolerance to peripheral lines is increased with feeds of low osmolality and neutral pH
and the use of soft paediatric cannulae.
Feed preparations
TPN solutions contain a balanced mix of essential and non-essential amino acids, glucose, fat,
electrolytes and micronutrients:
Iso-osmotic lipid emulsions are used to provide an energy-rich solution and reduce
irritation of veins.
Such preparations also permit a lower concentration of glucose to prevent hyperglycaemia
or hyperosmolar dehydration.
A wide selection of preparations are produced under sterile conditions and are available as 3-
litre bags of prepackaged solution.
Parenteral nutrition should be introduced at a low rate and gradually increased:
TPN is usually delivered at a continuous flow rate but cyclical regimens may suit longer
use.
Vitamins including folic acid are infused with the solution, but vitamin B12 must be
prescribed separately

19
Malnutrition Problems 0907(1)602
Appendices
Table 1. Laboratory values to detect malnutrition and monitor nutritional status

20
Malnutrition Problems 0907(1)602
Figure 1. Malnutrition Universal Screening Tool (MUST) for adults

21
Malnutrition Problems 0907(1)602
Figure 2.
22
Malnutrition Problems 0907(1)602
Table 2. Nutritional Risk Screening (NRS 2002)
NRS-2002 is based on an interpretation of available randomized clinical trials. *indicates that a trial directly supports the categorization of patients with that
diagnosis. Diagnoses shown in italics are based on the prototypes given below. Nutritional risk is defined by the present nutritional status and risk of impairment
of present status, due to increased requirements caused by stress metabolism of the clinical condition.
A nutritional care plan is indicated in all patients who are (1) severely undernourished (score=3), or (2) severely ill (score=3), or (3) moderately undernourished +
mildly ill (score 2 +1), or (4) mildly undernourished + moderately ill (score 1 + 2).
Prototypes for severity of disease
Score=1: a patient with chronic disease, admitted to hospital due to complications. The patient is weak but out of bed regularly. Protein requirement is
increased, but can be covered by oral diet or supplements in most cases.
Score=2: a patient confined to bed due to illness, e.g. following major abdominal surgery. Protein requirement is substantially increased, but can be
covered, although artificial feeding is required in many cases.
Score=3: a patient in intensive care with assisted ventilation etc. Protein requirement is increased and cannot be covered even by artificial feeding.
Protein breakdown and nitrogen loss can be significantly attenuated.
.
Figure 3.
23
Malnutrition Problems 0907(1)602
Figure 4.

24
Malnutrition Problems 0907(1)602
References:
1. American dietetic association
2. Nutritional screening and prevalence of hospital malnutrition risk. University Hospital
of the UANL, Monterrey byPatricia R. Áncer-Rodrígueza, Carmen Porrata-Mauri &
etal
3. Bapen , link : www.bapen.org.uk/how-good-is-your-nutritional-care
4. Malnutrition In Hospitalized Adult Patients, The Role of the Clinical Nurse Specialist,
National Association of clinical Nurse Specialists, January 2017
5. Malhi H (2018), Assessing and managing malnutrition in adults in hospital. Nursing
Standard, doi: 10.7748/ns.2018.e11180 published online October 2018
6. Lisa L. Kirkland, Erin Shaughnessy, Recognition and Prevention of Nosocomial
Malnutrition: a Review and a Call to Action! The American Journal of Medicine
(2017), http://dx.doi.org/doi:10.1016/j.amjmed.2017.07.034.
7. Volume 14, P54-55, August 01, 2016, Challenges for dietitians in nutritional support
of elderly, Denis Mlakar Mastnak, RN, RD , Mila Terčelj, RD
,DOI:https://doi.org/10.1016/j.clnesp.2016.04.023
8. Managing malnutrition to improve lives and save money, Rebecca Stratton,Trevor
Smith and Simon Gabe,Chair of Malnutrition Action Group, BAPEN ;Chair of British
Artificial Nutrition Survey Committee, BAPEN, President Elect of BAPENPresident
of BAPEN, October 2018
9. Prevalence of Malnutrition in Hospitalized Patients: a Multicenter Cross-sectional
Study, the Korean Society for Parenteral and Enteral Nutrition (KSPEN) Clinical
Research Groups, J Korean Med Sci. 2018 Jan 8; 33(2): e10. Published online 2017
Nov 17. doi: 10.3346/jkms.2018.33.e10, PMCID: PMC5729651
10. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3084475/?fbclid=IwAR1xbzJnAhEA
zPHeJN2BCDGXltcpRVKWoIdm2Ljg4UlR1MYnypINB5UeErQ#b37-ijerph-08-
00514
11. https://espen.info/documents/Screening.pdf?fbclid=IwAR0Dn9gn8HPfpE-
zyOlMEmAb0SOljZe8O3SAgOjv3PQWJk63EUaWjaEl0dc
12. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6679209/?fbclid=IwAR1-
P_P_bcueon3AW0kwMy8hF97ZUFjIx8BK-
8i5eMdxdxAUAOMsKBrXE1k#!po=0.537634
13. Hospital Malnutrition: Prevalence, Identification and Impact on Patients and the
Healthcare System https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3084475/
14. https://www.researchgate.net/publication/336531005_NUTRITIONAL_INDICATOR
S_OF_MALNUTRITION_IN_HOSPITALIZED_PATIENTS
15. Stratton RJ, Green CJ, Elia M. Oxon: CABI Publishing; 2003. Disease-related
malnutrition: an evidence-based approach to treatment.
16. National Institute for Health and Clinical Excellence (NICE) National Institute for
Health and Clinical Excellence (NICE) London: 2006. Nutrition support in adults: oral
nutrition support, enteral tube feeding and parenteral nutrition (clinical guideline 32)
17. https://gi.md/procedures/peg-pej
18. https://patient.info/doctor/enteral-feeding
19. https://www.todaysdietitian.com/newarchives/063008p44.shtml