making social protection work for the informal sector: … making social protection work for the...
TRANSCRIPT

1
Making Social Protection Work for the Informal Sector: The Case of PhilHealth and ALKANSSSYA Program for the Self-Employed
AKI-CBMS Proposal on Social Protection
By: Mitzie Irene P. Conchada and Marites M. Tiongco
April 2015
Abstract: In the DLSU-AKI annual report of Monitoring the Philippine Economy, the Philippines
maintained its growth momentum in 2014, besting other Asian economies. Given this, it is
interesting to find out whether various sectors have benefited from this growth, particularly the
informal sector which includes bulk of the poor who are self-employed and are mostly engaged in
the services sector. The intention of this study aimed to determine the effect of social protection,
particularly PhilHealth and the ALKANSSSYA on informal sector especially those who are poor
and self-employed. By the end of 2014, total benefit payment for all sectors amounted to PhP 78.2
billion (PhP 19.2 billion for the informal sector). Since the government spends so much on the
PhilHealth, especially with its expansion of the indigent program, there is a need to investigate the
effectiveness of the program especially on the poor. Utilizing data from the Community Based
Monitoring Survey (CBMS) collected in2015 from selected provinces in the Philippines, the
propensity score matching method showed that those who availed of PhilHealth(both individual
paying and sponsored member) have a higher total income and income in cash compared to those
who did not avail (PhP288 and PhP595 respectively). PhilHealth beneficiaries are also more likely to
have higher total sales from entrepreneurial activities in the informal sector (PhP69) than non-
beneficiaries. On the other hand, ALKANSSSYA beneficiaries also had higher annual income,
higher total sales from entrepreneurial activities and higher expenditure than non-beneficiaries
(PhP986, PhP18, and PhP304 respectively). The results support the claim that social protection is
indeed effective in improving the income of the poor, especially those who are dependent on the

2
informal sector. Expanding the coverage of the programs for the informal sector, thus, will aid in
increasing social inclusion and in reducing poverty levels.

3
I. INTRODUCTION
In the DLSU-AKI annual report of Monitoring the Philippine Economy, the Philippines
maintained its growth momentum in 2014, besting other Asian economies. Despite doubts over
growth prospects and challenges in the external market, the Philippine economy attained a solid 6.1
percent growth in 2014. Favorable demand and supply side factors combined with improvements in
the global market, particularly a recovering US economy and intensifying demand in Asia, led to the
6.1 percent growth in the country’s Gross Domestic Product (GDP). This brings the year-end
forecast to a higher estimate (Monitoring the Philippine Economy, January 2014). Given this, it is
interesting to find out whether various sectors have benefited from this growth, particularly the
informal sector, which includes bulk of the poor who are self-employed and are mostly engaged in
the services sector.1
Despite the performance of the economy, unemployment still remains one of the major
concerns. By the end of 2014, unemployment rate was recorded at 6.8 percent which implies that
there is still a large number of Filipinos who are unemployed given our population. Moreover, the
Philippine Statistics Authority (PSA)reported that most of the unemployed were males, high school
graduates and belonged to the age group 15 to 24 years old (Philippine Statistics Authority, 2014).
Given fewer stable job opportunities in the country, Filipinos are seeing entrepreneurship as an
alternative to earn income.
1The authors adapt the operational definiton of the informal sector by the Philippine Statistics Authority (PSA),
which shall refer to “household unincorporated enterprises which consist of both informal own-account enterprises and enterprises of informal employers. Informal own-account enterprises are household unincorporated enterprises owned and operated by own-account workers, either alone or in partnership with member/s of the same or other households which may employ unpaid family workers as well asoccasionally /seasonally hired workers but do not employ employees on continuing basis. Enterprises of informalemployers are household unincorporated enterprises owned and operated by own-account workers, either alone or in partnership with members of the same or other household which employ one or more employees on a continuing basis…”

4
As of 2012, there were 940,886 registered micro, small and medium enterprises (MSMEs) in
the Philippines (99.6 percent of the total establishments), majority of which are in the retail and
wholesale industry.Despite this impressive number, there is a huge number of businesses, mostly
belonging to self-employed Filipinos, that are not registered and are part of what is called the
informal sector. There are many barriers as to why many of them are not registered and one of the
reasons is the high opportunity cost of having to register their business especially for micro
establishments such as sari-sari stores, food stalls and other small scale businesses.
More often than not, these businesses belonging to the informal sector are exposed to
different types of shocks, both internal and external such as sickness in the family and natural
disasters. Their vulnerability to shocks hinders the business from realizing its full potential and thus
resources are wasted. To protect the informal sector from shocks, the government invested in social
protection. The definition of social protection in the Philippines was formalized in 2007 and covers
four components namely: social insurance, social welfare, social safety nets, and labor market
interventions (International Labor Organization, 2014). On the other hand, the National Economic
Development Authority (NEDA) is a set of policies and programs that seek to reduce proverty and
vulnerability to risks and to enhance social status and rights of the marginalized. One of the
initiatives on social protection was the passage of the National Health Insurance Act in 1995 which
aims to provide equitable access to quality health care to everyone (International Labor
Organization, 2014). Through the Act, the National Health Insurance System or PhilHealth was
established to implement universal health care by the year 2016. As of the December 2014, there
were a total of 2,023,696 members in the informal sector, which is only 9 percent of the informal
sector (PhilHealth, 2014). Membership has increased by 62,586 by the end of December 2015, but in
terms of proportion, growth has remained at 9 percent of the informal sector (Philhealth, 2015a). It
5
is thus important to increase the coverage of the informal sector since they are more vulnerable to
shocks.
According to the International Labor Organization (2014), social protection is crucial as the
country faces socio-economic factors that affect the population. For one, the Philippines has most
unequal income distribution among East Asian middle-income countries. Second, general and youth
unemployment are high (7.1% and 16.6% respectively). Furthermore, the rapid population growth
at the rate of 1.9% places pressure on the labor market. Third, aside from unemployment, a high
percentage of the employed are considered vulnerable (38.4%). Fourth, a strong service sector is
prevalent which requires more man power. Lastly, the exposure of the country to natural disasters
such as typhoons makes it more vulnerable (International Labor Organization, 2014).
It is the intention of this study to determine the effect of social protection, particularly
PhilHealth and the ALKANSSSYA2 on informal sector especially those who are poor and self-
employed.3By the end of 2014, total benefit payment for all sectors amounted to PhP 78.2 billion
(PhP 19.2 billion for the informal sector).Since the government spends so much on the PhilHealth,
especially with its expansion of the indigent program, there is a need to investigate the effectiveness
of the program especially on the poor.There are many programs aimed towards the informal sector
but there are a few studies on this. This study will focus on answering the research question: ―Are
people in the informal sector better-off availing PhilHealth and the ALKANSSSYAprogram?‖
Specifically, the research aims to address the following objectives:
1. Provide an overview of the coverage of the Philhealthand the ALKANSSSYA program
in the informal sector
2 The AlkanSSSya is an innovative saving mechanism which allows people to pay premiums whenever they can. It
was introduced by Social Security System to address expansion coverage of PhilHealth to include the informal sector.
6
2. Identify barriers to access Philhealth and the ALKANSSSYA program in the informal
employment
3. Determine whether PhilHealth and ALKANSSSYA members experienced an
improvement in the income of the poor who are part of informal sector.

7
II. REVIEW OF RELATED LITERATURE
a. Poverty in the Philippines
In an effort to address poverty through the MDGs on human capital development through
education, health and women empowerment, various programs have been implemented. However,
progress has been slow in reducing poverty. Table 2.1 shows that poverty incidence in the
Philippines has not improved that much since the year 2003. Moreover, the magnitude of poor
families has increased from 3.8 million families in 2006 to 4.2 million in 2012 (NSCB, 2012). The
poverty incidence among Filipino families in 2012 was the highest in the regions ARMM, Eastern
Visayas (region 8), and Soccsksargen (region 12) with 48.7 percent, 37.4 percent, and 37.1 percent
respectively. In the region ARMM, Lanao del Sur had the most severe incidence of poverty among
families with 67.3 percent. This was followed by Maguindanao with 54.5 percent families of the
total number of families who are considered poor.
Table 2.1First Semester Poverty Incidence Among Families (%)
Major Island Group
1991
First Semester Poverty Incidence among Families (%)
2003 2006 2009 2012 2015 Increase/Decrease
06-09 09-12 12-15
PHILIPPINES 29.7 22.9 23.4 22.9 22.3 21.1 (0.5) (0.5) (1.3)
Luzon
14.73 15.4 15.0 14.5 13.4 (0.4) (0.5) (1.0)
NCR
2.8 3.7 3.8 4.5 0.9 0.1 0.7
Without NCR
19.3 18.4 17.6 16.1 (0.9) (0.8) (1.5)
Visayas
32.44 31.6 30.7 29.1 28.7 (0.9) (1.6) (0.4)
Mindanao
35.17 36.2 35.6 36.0 33.8 (0.6) 0.4 (2.1)
8
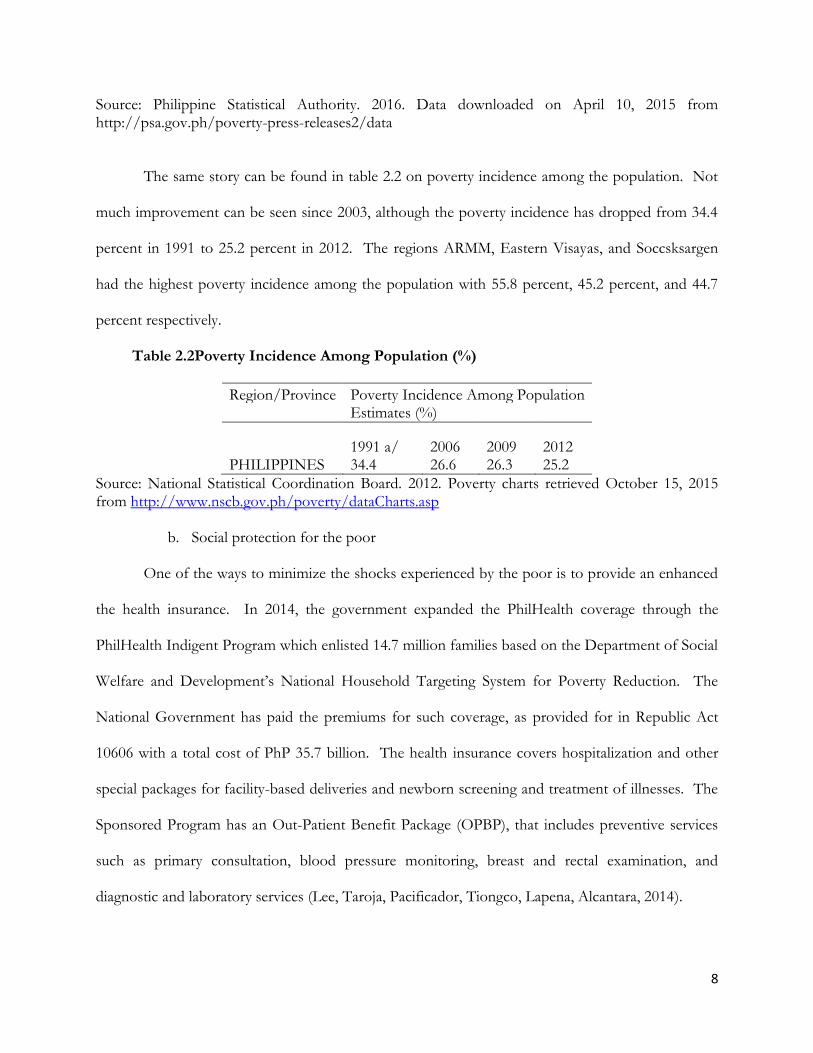
Source: Philippine Statistical Authority. 2016. Data downloaded on April 10, 2015 from http://psa.gov.ph/poverty-press-releases2/data
The same story can be found in table 2.2 on poverty incidence among the population. Not
much improvement can be seen since 2003, although the poverty incidence has dropped from 34.4
percent in 1991 to 25.2 percent in 2012. The regions ARMM, Eastern Visayas, and Soccsksargen
had the highest poverty incidence among the population with 55.8 percent, 45.2 percent, and 44.7
percent respectively.
Table 2.2Poverty Incidence Among Population (%)
Region/Province Poverty Incidence Among Population
Estimates (%)
1991 a/ 2006 2009 2012
PHILIPPINES 34.4 26.6 26.3 25.2
Source: National Statistical Coordination Board. 2012. Poverty charts retrieved October 15, 2015 from http://www.nscb.gov.ph/poverty/dataCharts.asp
b. Social protection for the poor
One of the ways to minimize the shocks experienced by the poor is to provide an enhanced
the health insurance. In 2014, the government expanded the PhilHealth coverage through the
PhilHealth Indigent Program which enlisted 14.7 million families based on the Department of Social
Welfare and Development’s National Household Targeting System for Poverty Reduction. The
National Government has paid the premiums for such coverage, as provided for in Republic Act
10606 with a total cost of PhP 35.7 billion. The health insurance covers hospitalization and other
special packages for facility-based deliveries and newborn screening and treatment of illnesses. The
Sponsored Program has an Out-Patient Benefit Package (OPBP), that includes preventive services
such as primary consultation, blood pressure monitoring, breast and rectal examination, and
diagnostic and laboratory services (Lee, Taroja, Pacificador, Tiongco, Lapena, Alcantara, 2014).

9
Aside from the Indigent Program, PhilHealth also has a specific program for those who are
part of the informal sector. This includes street hawkers, market vendors, pedicab and taxi drivers,
small-time construction workers, and home-based industries and services. They also cover
dependents such as the legitimate spouse, child or children below 21 years old and are still
unmarried, children above 21 years old but are suffering from physical or mental disability, and
parents who are 60 year old and above (Philhealth, 2015b).
Another social protection program from the government is Social Security System’s (SSS)
program for self-employed people. The program includes self-employed professionals, owners of
business, farmers and fisherfolk, and workers in the informal sector such as market and ambulant
vendors, public utility transport drivers, tourism industry-related workers, and others in a similar
situation (https://www.sss.gov.ph/sss/appmanager/pages.jsp?page=selfemployedcoverage).
Launched in 2011, AlkanSSSya is a micro-savings program intended for self-employed members in
the informal sector, particularly those who have irregular income such as tricycle drivers and market
vendors. It is designed to fit the way of life of informal sector workers and to make saving for
monthly SSS premiums as affordable as only P11.00 per day for a minimum SSS monthly
contribution of Php330. The informal sector groups are organized and are registered as SSS Self-
employed members that must meet the monthly salary of Php3,000. Those who have a higher
month salary can contribute a higher monthly contribution.
Prior to AlkanSSSya, there were already several affordable saving schemes through commercial
banks introduced by SSS. However, there was very low participation from the informal sector
because saving was difficult to do for those who had highly irregular incomes in addition to being
risk averse to formal banking transactions.
TheAlkanSSSya derived its concept from a piggy bank, and makes use of large metal safety box with
secure individual compartments in which members can put their savings to pay for their monthly
10
contribution. The money saved will be picked up by SSS authorized collectors by the end of the
month and will be credited to their monthly contribution. This does away with the hassle of having
to go to a bank or the SSS office to remit their money, which is often of the hindrances that
members experience. The program was initially conceptualized for tricycle drivers in Las Pinas but
has spread nationwide because of its effectivity and popularity. This has deemed to be successful
because of the benefits of the micro-savings program
(http://www.philstar.com/business/2013/06/09/951731/sss-expands-alkansssya-program-inmates-
drivers. The program has more than 80 partners across the country that service the self-employed
and the informal sector workers.
These social security programs are aimed at minimizing the negative impact of internal and
external shocks that may affect families who are dependent on self-employment and informal sector
activities. Very few studies have shown theeffectivity of social security programs for the informal
sector thus this study aims to look deeper into how the program works and what benefits do the
beneficiaries receive compared to non-members.

11
III. EMPIRICAL MODEL AND METHODOLOGY
In assessing whether the social security programs of PhilHealth and SSS are effective, the
study will employ and impact evaluation. Usui (2011) discussed the various approaches to
conducting an impact evaluation study. The basic idea behind an impact evaluation study is to
compare the indicators before and after the implementation of the program. Setting up time-bound
and measurable performance indicators is very important because this will allow proper monitoring
and evaluation. Usui (2011) identifies the first step as setting up an ex-ante target for each
performance indicator with a specific time frame. To determine the impact of the program, the
actual value of the indicator is measured at a certain stage after completion of the project (Usui,
2011). The baseline value is usually used as a point of comparison. This baseline could be the initial
characteristics of the household before implementation of the program.
The study will evaluate the impact of the programs on the informal sector using propensity
score matching. Propensity score matching, as developed by Rosenbaum and Rubin (1983), is a
statistical technique that tries to estimate the effect of an intervention or treatment given certain
covariates that predict receiving the treatment. The PSM technique is used for observational data to
estimate the impact of an intervention and helps answer the question ―what is the treatment effect
on the treated.‖ In the case of this study, we answer the question what is the impact of PhilHealth
and Social Security System’s AlkanSSSyaon income and health expenditures of the beneficiaries.
Moreover, the PSM technique establishes the counterfactual, that is what would have happened to
the beneficiaries had they not received the social protection program. Through the PSM a proper
counterfactual can be found by matching a beneficiary to a non-beneficiary with similar pre-
intervention characteristics (also called covariates). For the households with matched characteristics,
each has an equal chance of becoming a beneficiary or non-beneficiary (Capuno, 2013).

12
For observational studies such as this, the assignment of treatments to subjects is not
randomized and the PSM thus mimics an experiment by creating a sample of units that received the
treatment that is comparable on all observed covariates to a sample of units that did not receive the
treatment. The propensity scores that will be generated will be used to match a beneficiary to a non-
beneficiary, which is better than using covariates to match the two groups because the latter has too
many dimensions which may result in the failure of common support (Capuno, 2013).
In carrying out the PSM in this study, the following steps will be implemented. First,
covariates (independent variables) that simultaneously influence participation into the program as
well as the outcome will be selected. The covariates and outcome will then used in the probit model
that would help estimate the propensity score.
In the absence of pre-treatment data, we will use time invariant observable variables in the
study. We will use household characteristics such as gender of the household head (1 if male, 0
otherwise), highest educational attainment of the household, age of the household head, and family
size. The treatment variable shall be whether the household is a beneficiary or not of the two social
security programs. The model will be regressed against several outcome variables such as income
and health expenditures.
The model is described as:
Pr 𝑆𝑆 = 1 = 𝐹(𝛽1 + 𝛽2𝑖𝑛𝑑𝑖𝑣𝑖𝑑𝑢𝑎𝑙 𝑐ℎ𝑎𝑟𝑎𝑐𝑡𝑒𝑟𝑖𝑠𝑡𝑖𝑐𝑠𝑖 + 𝛽3ℎ𝑜𝑢𝑠𝑒ℎ𝑜𝑙𝑑 𝑐ℎ𝑎𝑟𝑎𝑐𝑡𝑒𝑟𝑖𝑠𝑡𝑖𝑐𝑠𝑖 +
𝛽4𝑤𝑒𝑎𝑙𝑡ℎ 𝑖𝑛𝑑𝑒𝑥𝑖 + 𝜀𝑖)
The equation was used for both the PhilHealth and Social Security System’s AlkanSSSya.
The equation above describes the relationship of the independent variables which are the
characteristics of the household, characteristics of the individual and wealth index to whether they
are beneficiaries or non-beneficiaries of PhilHealth and AlkanSSSya programs using the latest

13
Community Based Monitoring System which includes questions on unemployment, social protection
and entrepreneurship.
The outcomesincluded in the study were total income, total income in cash, wage in cash,
total sales from entrepreneurial activities, and total expenditure in cash.

14
IV. RESULTS AND ANALYSIS
Making PhilHealth and SSS accessible to the informal sector might be a challenge in itself as
contribution is not mandatory and accessibility might post a cost to the contributor. Despite the
long term benefits that could be drawn from the program, the short-sightedness and lack of
foresight of some individuals can hinder them from availing of the program (SOURCE?).
PhilHealth
According to Sifverberg (2016), Philhealth coverage rates were at 56-58%, indicating that
over 40% of people who did not qualify as dependents and are unemployed did not have healthcare.
The study also noted that Bicol and Eastern Visayas Regions had some of the lowest rates at 23.85%
and 28.95% respectively, although Sulu and Tawi-tawi posted even worse rates of 3% (Silfverberg,
2016).
Sifverberg (2016) mentioned in that the availability of health care resources in the area
seemed to be an essential factor in the ensuing level of coverage in the province, with more private
hospitals making it more likely for a province to have higher coverage rates. Moreover, Sifverberg
(2016)stated that the problem may have to do with informal sector workers sometimes classifying
themselves as members of the formal sector. Sifverberg (2016) therefore recommended that the
government channel funds into the health insurance system instead of public providers and examine
the depth of Philhealth coverage, especially the Individually Paying Program, since some people may
perceive that coverage will end up accounting for only a minute part of their medical expenses.
AlkanSSSya
According to SSS’ 2014 Annual Report, the AlkanSSSya Program was conceived by the SSS
as a service to informal sector workers like public utility vehicle drivers, market vendors, farmers,
fishermen, and prison detainees, who face demands to focus on basic needs in addition to 12-14

15
hour work days, and thus do not have the time to learn about and exercise financial planning. It
allows for members to save as little as P12 day or around P330 a month; it serves just like a literal
piggy bank for savings for the future (SSS, 2014).
Since the implementation of the AlkanSSSya Program in 2011 until December 2014, it has
covered 122,387 members of 1,236 informal sector groups (ISGs), collecting P167m in
contributions. The program experienced an improvement in 2014, achieving a coverage of 63,758
members from 673 ISGs, more than half of all cumulative members and reached ISGs since 2011;
total contributions also reached P66.2m in 2014, accounting for 40% of the cumulative
contributions since 2011
https://www.sss.gov.ph/sss/DownloadContent?fileName=SSS2014_Annual_Report.pdf).
Barriers to Social Security
Based on the survey results, the common barriers identified were: 1) no regular income to
sustainably contribute; 2) low income that is not enough to allow contribution; 3) no necessary
requirements to become a member; 4) not aware of benefits; 5) lack of information on how to
become a member; 6) offices not available; 7) others (Table 4.1). The other reasons include 1) too
young to contribute; 2) not able to take care of it; 3) too far/not accessible; 4) well enough or okay
not to avail of SSS; 5) no money/resources (Table 4.2).
Table 4.1 Barriers to avail of SSS
Reasons Percent
No regular income to sustainably contribute 25.4
Low income that is not enough to include contribution 25.4
Does not have necessary requirements to become a member 7.5
Not aware of benefits 7.4
Lack of information how to register or become member 6.3
Offices are not accessible 4.6
Only GSIS is applicable 22.9
Others 0.4
Source: CBMS database 2015

16
In general, most of the respondents identified no regular income and low income (15.5 %
for both) as the top reasons why they are able to continue on being a member. For those who
answered others, the top answers were: 1) ok not to contribute (34%); and 2) no time to take care of
it (25%).
Table 4.2 Other reasons for non-membership in SSS
Other Reasons Percent
Too young to contribute 6.25 Not able to take care of it 25
Too far/not accessible 21.88 Well enough or okay not to avail of SSS 34.38
No money/resources 12.5
Source: CBMS database 2015
Having no regular source of income or low income makes it difficult for them to contribute
regularly. Regular employees do not have to make a conscious effort to set aside money since their
social security contributions are deducted already from their income. But this is not the case for
those who are working in the informal sector. Before they can set aside their contribution for social
security, they have to think about their other expenses which make it difficult to prioritize the
contribution. Moreover, some are resigned to the idea that they are ok with not having a social
security because of the high opportunity cost for them to contribute. The conscious effort to set
aside money and to go to the nearest SSS office every month is quite taxing on their part as they
have to take care of other pressing matters.

17
Descriptive Statistics
The next section discusses variables that were used in the study based on the propensity
score model. There were a total of 283 respondents for the AlkanSSSya program, 138 were
beneficiaries and 145 non-beneficiaries. For the PhilHealth individual paying and sponsored
programs, there were a total of 10,483 individuals: 5,233 were beneficiaries and 5,250 were non-
beneficiaries.
Table 4.3 Descriptive statistics for PHILHEALTH
Variable Definition Mean Std. dev Min Max
Dependent variable Availprog Availed of PHILHEALTH 0.4992 0.5000 0 1
Independent variables wi_simple Wealth index 1 (simple) 0.2318 0.1571 0 0.9565
educal1 Grade school 0.3269 0.4691 0 1
educal2 College 0.0551 0.2283 0 1
educal3 Technical vocation 0.0096 0.0977 0 1
sex Male or female 0.5038 0.5000 0 1
internet Access to internet 0.0315 0.1746 0 1
unemp Unemployed 0.0198 0.1395 0 1
Outcomes totin Total income 76,482 46,819 0 401,000
totincsh Total income in cash 61,012 44,062 0 365,000
wagcsh Wage in cash 41,597 43,773 0 365,000
totexp Total expenditures 138 3,221 0 190,000
Number of observations 10,438 Income and expenditure are in current prices (Philippine pesos) and represent annual figures.
Table 4.3 provides some information about the characteristics of individuals who are
beneficiaries and non-beneficiaries of PhilHealth in the CBMS 2015. The beneficiaries and non-
beneficiaries were from NCR: Manila and Marikina, Batangas, Cavite, Negros Occidental, and
Misamis Occidental. Almost half of the individuals who are part of the informal sector are females.
18
Most of them are married, have high school as their highest educational attainment, and belong to a
family with an average size of 6 members. When it comes to the economic profile of the
individuals, the average annual total income (in cash) is PhP61,012 while the average wage is
PhP41,597.Only a few of them are unemployed as most are self-employed in different kinds of
economic activities, especially those related to the services sector. Since all of the respondents are
poor, access to household appliances, land, and a vehicle is very low: only less than ¼ or 23% have
access to such wealth variables. Moreover,access to internet which measures social connectedness is
also very low: only 3% of the respondents have access. The next table describes the profile of the
respondents who availed of the ALKANSSSYA program.
The profile of those who availed of ALKANSSSYA is almost similar to the PhilHealth
beneficiaries except that all the respondents are from Marikina. Most of the respondents are females
(54%) and are married, and have high school as their highest educational attainment. Only 9 percent
have finished college and 3 percent have finished a technical/vocational course. Most of them
belong to a family of 6 and rely on self-employment activities. The individuals who are engaged in
activities in the informal sector are mostly in the retail business (44%): sari-sari store, food vendors;
and are engaged in the services sector (25%) - either drivers, carpenters, work in the parlor as a
stylist, manicurist, etc.
19
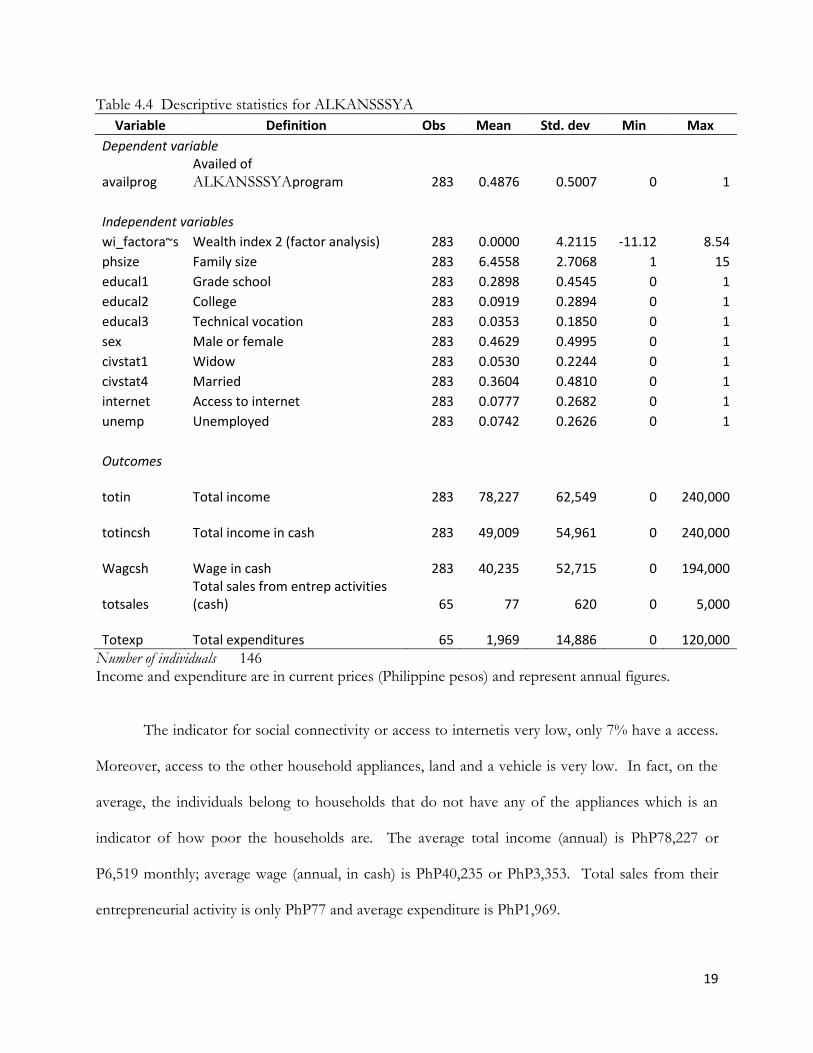
Table 4.4 Descriptive statistics for ALKANSSSYA
Variable Definition Obs Mean Std. dev Min Max
Dependent variable
availprog Availed of ALKANSSSYAprogram 283 0.4876 0.5007 0 1
Independent variables wi_factora~s Wealth index 2 (factor analysis) 283 0.0000 4.2115 -11.12 8.54
phsize Family size 283 6.4558 2.7068 1 15
educal1 Grade school 283 0.2898 0.4545 0 1
educal2 College 283 0.0919 0.2894 0 1
educal3 Technical vocation 283 0.0353 0.1850 0 1
sex Male or female 283 0.4629 0.4995 0 1
civstat1 Widow 283 0.0530 0.2244 0 1
civstat4 Married 283 0.3604 0.4810 0 1
internet Access to internet 283 0.0777 0.2682 0 1
unemp Unemployed 283 0.0742 0.2626 0 1
Outcomes
totin Total income 283
78,227
62,549 0
240,000
totincsh Total income in cash 283
49,009
54,961 0
240,000
Wagcsh Wage in cash 283
40,235
52,715 0
194,000
totsales Total sales from entrep activities (cash) 65
77
620 0
5,000
Totexp Total expenditures 65
1,969
14,886 0
120,000
Number of individuals 146 Income and expenditure are in current prices (Philippine pesos) and represent annual figures.
The indicator for social connectivity or access to internetis very low, only 7% have a access.
Moreover, access to the other household appliances, land and a vehicle is very low. In fact, on the
average, the individuals belong to households that do not have any of the appliances which is an
indicator of how poor the households are. The average total income (annual) is PhP78,227 or
P6,519 monthly; average wage (annual, in cash) is PhP40,235 or PhP3,353. Total sales from their
entrepreneurial activity is only PhP77 and average expenditure is PhP1,969.
20
Both beneficiaries and non-beneficiaries of the PhilHealth and AlkanSSSya programs are
poor and almost have no ownership to property such as land and other assets. Their main source of
income is from self-employment activities that yields a very low income and may not be enough to
meet the needs of the family. Given their economic status, being a member of the PhilHealth and
Alkansssya programs would help augment their expenses especially in health care.
Propensity score matching results
To determine the impact of the PhilHealth and Alkansssya programs, the study compared
the impact on beneficiaries and non-beneficiaries. The study made sure that the characteristics of
the two groups were the same in order to find out the counterfactual: what have happened if the
program was not implemented?Controlling for the characteristics of the two groups would really
point out the impact of the programs. For the PhilHealth program, there were a total of 10,438
individuals: 5,233 were beneficiaries and 5,250 were non-beneficiaries. For the AlkanSSSya
program, there were a total of 283 respondents: 138 were beneficiaries and 145 non-beneficiaries.
The non-beneficiaries were randomly chosen from a pool of non-beneficiaries who had the same
characteristics as those with the beneficiaries.
The following results are based on the Community Based Monitoring System 2015 database.
The study used the Propensity Score Method (PSM) which is an impact evaluation tool used when
no baseline survey has been conducted and the only data available are the characteristics of the
beneficiaries. The aforementioned method is a quasi-experiment that tries to determine what would
have happened if the program was not implemented. The model used in the study is described as:
𝑃𝑟𝑆𝑆 = 𝐹(𝛽1 + 𝛽2𝑤𝑒𝑎𝑙𝑡ℎ 𝑖𝑛𝑑𝑒𝑥𝑖 + 𝛽3ℎ𝑜𝑢𝑠𝑒ℎ𝑜𝑙𝑑 𝑠𝑖𝑧𝑒𝑖 + 𝛽4𝑠𝑒𝑥𝑖 + 𝛽5𝑒𝑑𝑢𝑐𝑖 + 𝛽6𝑖𝑛𝑡𝑒𝑟𝑛𝑒𝑡𝑖
+ 𝛽7𝑢𝑛𝑒𝑚𝑝𝑖 + 𝛽8𝑐𝑖𝑣𝑠𝑡𝑎𝑡𝑖 + 𝜀𝑖
where: Wealth index – index durable assets such as land, housing, etc to capture personal
21
security and privacy
Household size – number of family members
Sex – whether male or female (with value equal to 1 if male, 0 if female)
Educal – highest educational attainment as proxy for living standards — the higher the
education the more likely to raise living standards
Internet – internet connection; proxy for social connectedness as dimensions for well-
being/welfare
Unemp – dummy variable for whether the individual is unemployed or not (1 if
unemployed, 0 if employed)
Civstat – dummy variables for various civil status (with value equal to 1 if married, 0 if
not married 0; widowed, 1, not widowed, 0; live-in, 1, not live-in, 0; and
separated, 1, not separated 0)
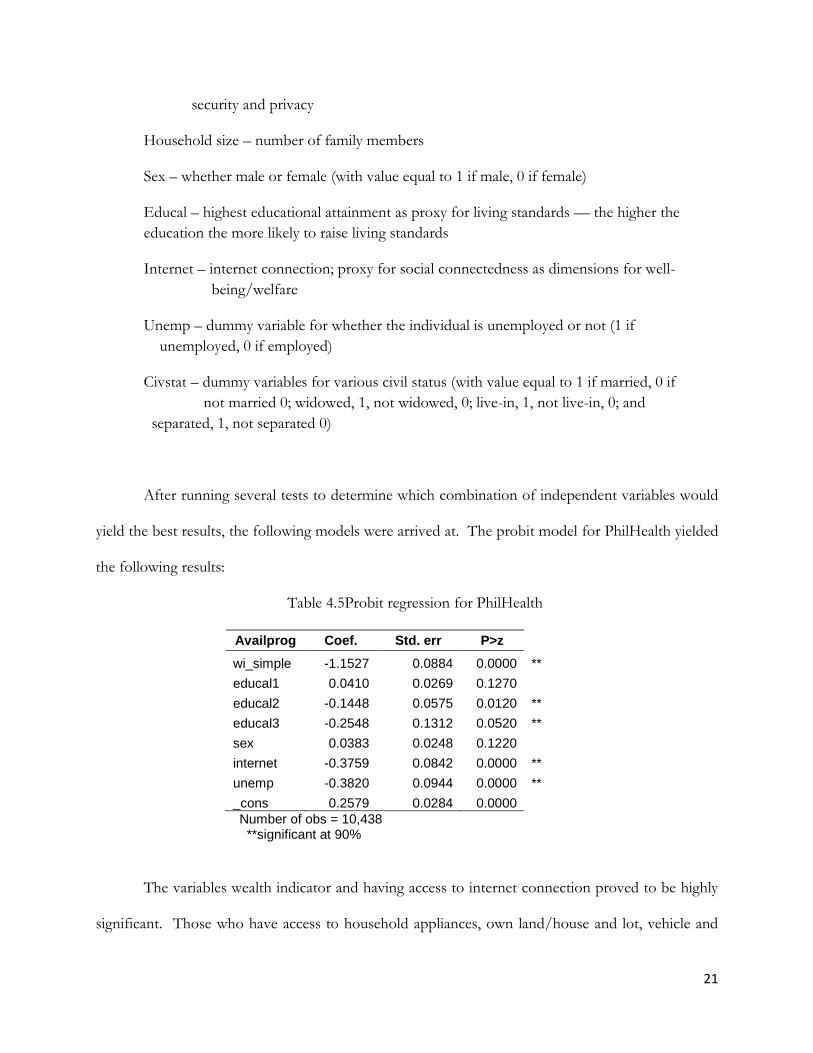
After running several tests to determine which combination of independent variables would
yield the best results, the following models were arrived at. The probit model for PhilHealth yielded
the following results:
Table 4.5Probit regression for PhilHealth
Availprog Coef. Std. err P>z
wi_simple -1.1527 0.0884 0.0000 **
educal1 0.0410 0.0269 0.1270 educal2 -0.1448 0.0575 0.0120 **
educal3 -0.2548 0.1312 0.0520 **
sex 0.0383 0.0248 0.1220 internet -0.3759 0.0842 0.0000 **
unemp -0.3820 0.0944 0.0000 **
_cons 0.2579 0.0284 0.0000 Number of obs = 10,438
**significant at 90%
The variables wealth indicator and having access to internet connection proved to be highly
significant. Those who have access to household appliances, own land/house and lot, vehicle and

22
internet connection are not likely to be poor thus will not enroll in the individual paying or
sponsored program. The poor who are usually not employed and rely only on economic activities in
the informal sector are less likely to avail of the PhilHealth program due to several reasons. One of
them is not having extra income/profit to pay for the monthly premium. This goes to say that
individuals who are unemployed are not likely to avail of PhilHealthindividual paying or sponsored
program. The barriers which is mainly lack of income, especially when they are unemployed,
prevents them from being a member. The educational attainment of the individual was also
significant, particularly those who were college and technical/vocational graduates. Those who have
finished college and technical/vocational courses are (14% and 25% respectively) not likely to avail
of the PhilHealth individual paying program. These individuals are more likely to have a full time
job, thus wouldn’t require availing of PhilHealth’s individual paying program.
The next table describes the probit regression results for the AlkanSSSya program.
Table 4.6Probit regression for AlkanSSSya
availprog Coef. Std. err P>z
wi_factora~s 0.0224 0.0209 0.2830
phsize 0.0107 0.0286 0.7070
educal1 0.0360 0.1760 0.8380
educal2 0.1465 0.2790 0.5990
educal3 0.0910 0.4227 0.8290
sex 0.0789 0.1573 0.6160
civstat1 0.3163 0.3526 0.3700
civstat4 0.1899 0.1717 0.2690
internet -0.8213 0.3348 0.0140 **
unemp 0.0403 0.3001 0.8930
_cons -0.1511 0.2393 0.5280
Number of obs = 283 **significant at 90%
The probit regression results reveal that there is only one variable that turned out to be
significant: access to internet. Access to internet, which measures social connectivity, decreases the
probability (82%) of availing the AlkanSSSya program. An individual who has access to internet is

23
more likely to be non-poor and would more likely to have a regular job where his SSS contributions
are automatically deducted.
After performing balancing tests and robustness of the PSM, the last step performed was to
estimate the average treatment effect (ATT) using the beneficiaries (poor individuals who are part of
the informal sector who availed of PhilHealth and ALKANSSSYA) versus the non-beneficiaries.
The results are summarized in the table below:
Table 4.7PSM results: For PhilHealth beneficiaries and non-beneficiaries
Treated Control ATT Std. Err. t-value
Total income per capita 5233 5031 607.58 104.57 5.81 **
Total income in cash per capita 5233 5031 992.96 102.45 9.69 **
Wage in cash per capita 5233 5031 146.33 114.09 1.28 *
Total expen cash per capita 5233 5031 4155.98 509.51 8.15 **
*statistically significant at p<0.10 **statistically significant at p<0.05
To check the robustness of the ATT results, the study used Nearest Neighbor Matching
(NNM). If any of these tests appeared significant (based on the bootstrapped standard errors), then
it means that the results are robust.
The results for PhilHealth reveal that those who availed of the program have a higher annual
income than those who did not avail – by PhP608. Furthermore, annual income in cash is PhP993
higher than those who did not avail. Wage is also higher for beneficiaries as they get to enjoy
PhP146 compared to non-beneficiaries. Lastly, individuals who are PhilHealth members have
higher annual expenditures: PhP4,155. The results are consistent with the a-priori expectations that
individuals who have access to social security insurance such as PhilHealthgives them more savings
which they can use for more important expenses such as education and food.

24
The next table shows the results the ALKANSSSYA program. All of the outcome variables
turned out to be significant. This implies that the impact of the program is effective in improving
the welfare of the beneficiaries, especially in terms of their income, wage, total sales from
entrepreneurial activities and total expenses.
Table 4.8PSM results: For AlkanSSSya beneficiaries and non-beneficiaries
Treated Control ATT Std. Err. t-value
Total income per capita
138 78 1,890.65 1145.58 1.65 *
Total income in cash per capita 138 78 1,472.31 1096.41 1.34 *
Wage in cash per capita 138 78 1,349.66 1094.97 1.23 *
Total sales from entrep per capita 138 18 18.38 18.471 0.99
Total expen cash per capita 138 78 317.23 237.86 1.33 *
*statistically significant at p<0.10
Those who availed of the AlkanSSSya program in Marikina enjoy higher total income of
(PhP1,890) and higher wage (PhP1,349) than non-members. Moreover, those individuals who are
engaged in a small business enjoy higher sales of PhP18. Though this is a small amount, if this is
summed up through a longer period of time, it would create a bigger difference. In addition to that,
members are able to have extra to spend more on other essential goods (PhP317) such as food and
other basic goods.
Given the benefits of being a member of PhilHealth and AlkanSSSya programs, there is
more than enough reason to believe that the money paid for the premium (PhP2,400/year for
PhilHealth, and PhP330/month for AlkanSSSya) will go a long way. It helps the individual augment
its expenses for health and other investment generating activities through the benefits that they get
from being a member. Being part of the informal sector makes them vulnerable to shocks such as

25
sudden changes in prices and one of the ways to minimize the negative economic impact of this is
there is access to social security such as in this case, the PhilHealth individual paying and sponsored
program and the AlkanSSSya program.

26
V. CONCLUSION AND POLICY RECOMMENDATIONS
This study has shown some initial evidence on the effectiveness of some social protection
programs such as the PhilHealth and ALKANSSSYA program for those who are involved in the
informal sector. Being part of the informal sector implies that the individual has no permanent
source of income, thus there is no financial security. The PhilHealth and ALKANSSSYA programs
aim to provide health and insurance security.
The results show that both programs are effective for poor individuals involved in the
informal sector in terms of gaining more income. The programs help augment the financial needs
by allowing them to use their income for expanding their business instead of using it for emergency
purposes such as hospitalization or other health needs.
Given the results of this exercise, it is recommended to increasethe low coverage in terms of
membership among the informal sector. This can be done by promoting enrollmentthat can be
initiated by the local chief executives andlocal government units in partnership with civil society and
non-government organizations. However, there isinadequate dataon the number of people in the
informal sector so theproblem lies on how toidentify individuals and households that are poor,
vulnerable and marginalized within the informal sector.It is expected that the informal sector will be
more visible and will be identified efficiently as potential beneficiaries of social protection
programsin the new database from DSWD’s National Household Targeting System for Poverty
Reduction or ―Listahanan‖. The Listahanan is an information management system that assesses and
identifies who the poor are and where they are located in order to maximize the social proteciton
programs.
The use of CBMS data can also help provide baseline information with its rider
questionnaire on social protection by expanding its coverage to all provinces and municipalities.
27
With CBMS data, the informal sector will no longer be invisible and thus better profiling of this
sector will be achieved.
Promoting enrolment and increasing the coverage would also mean increasing the budget for
health at the local government level. One sources of funds would be revenues from the sin tax, in
which 85% of the total revenue is earmarked to fund universal health care, which could also be used
to cover the poor informal sector who can not afford heatlh care.
Another possible policy implication is to improve the accessibility of a payment facility. The
local chief executives and local government units can facilitate in information campaigns on what
services are offerred by Philhealth and ALKANSSSYA. Another one is identifying partners that can
assist in the payment of contributions, for example, in partnership with a telecom networkthrough
the use of an e-load facility or mobile phones in remitting one’s contribution. An individual would
simply purchase a load and have a choice to remit part of it or all of it to his PhilHealth and SSS
contributions. Another possible way of making payment more accessible is through retail
pawnshops (Cebuana or Palawan Express etc.) that are very prevalent in provinces. Exploring more
avenues in partnership with the private sector can make payment facilities more accessible and less
costly on the part of the contributor, especially in geographically isolated areas.
Though it is difficult to reach individuals in the informal sector since most are
undocumented, it is best to involve the participation of the local chief executives and local
government units in identifying, monitoring and providing support for the informal
sector.Community support such as providing assistance in filling out registration forms or creating
opportunities for livelihood and job-creating enterprises that will sustain their incomes. A
sustainable employment will help encourage the poor to set aside a few pesos daily as they can now
afford to save and seek for better health care.

28
REFERENCES
Angelo King Institute. (2014). Monitoring the Philippine Economy Annual Report. BusinessWorld. Retrieved February 19, 2016, from
http://www.bworldonline.com/content.php?section=Economy&title=health-insurance-coverage-rates-56%-58%-for-informal-sector----pids&id=122149
Capuno, J. (2012). Household decisions and child health : Estimating the links between water
treatment and the incidence of diarrhea using non-recursive two-equation causal models. UPSE Discussion Paper No. 2012-02
International Labor Organization. (2014). www.ilo.org Lee, R., Tarroja, C., Pacificador, A., Tiongco, M., Lapena, M., and Alcantara, M. (2014). ―How the
Department of Health and Other Interventions Close the Gap in Health Outcome Disparities among Local Government Units.‖ Inception Report prepared for the Department of Health and the European Union.
National Statistical Coordination Board. 2012. Poverty charts retrieved October 15, 2015 from
http://www.nscb.gov.ph/poverty/dataCharts.asp National Statistics Office. (2014). Census on Population and Housing 2010. Retrieved from
http://census.gov.ph/content/statistical-tables-sample-variables-results-2010-census-population-and-housing-%E2%80%93-bataan on March 3, 2015.
PhilHealth. (2014). www.philhealth.gov.ph Philhealth. (2015a). Philhealth Stats & Charts. http://www.philhealth.gov.ph/about_us/statsncharts/snc2015_2nd.pdf . Downloaded on April 12, 2015. PhilHealth. (2015b). http://www.philhealth.gov.ph/members/informal/dependent.html Rosenbaum, P.R. & D.B. Rubin. (1983). The central role of the propensity score in observational
studies for causal Silfverberg, D.V. (2016). PhilHealth coverage in the informal sector: Identifying determinants of
enrollment. PIDS Policy Notes. No. 2016-02 (January 2016). Philippine Institute of Development Studies.
Social Security System.(2014) SSS Annual Report (Rep.) Retrieved February 19, 2016, from SSS
website: https://www.sss.gov.ph/sss/DownloadContent?fileName=SSS2014_Annual_Report.pdf
Social Security System. (2015). https://www.sss.gov.ph/sss/appmanager/pages.jsp?page=selfemployedcoverage

29
Tubadeza, K. P. (2016, January 26). Health insurance coverage rates 56%-58% for informal sector --
PIDS. Usui, N. (2011). Searching for effective poverty interventions: Conditional cash transfers in the
Philippines. Asia Development Bank.