major emergency plan - ireland's health services · emergency department clinical nurse ......
TRANSCRIPT

1
Major Emergency Plan
Connolly Hospital
Blanchardstown
Dublin 15
November 2013
Review date: November 2015

2
Table of Contents:
1 Introduction 5
2 Areas of Responsibility 9
2.1 Principal Functions 9
2.2 Persons authorised to activate plan 9
2.3 Responsibility of key individuals 9
2.4 Key roles & location of key areas 10
2.5 Colour Coding/Injury Categories 11
2.6 Patient flow during MEP activation 12
2.7 Dealing with the Media 13
3 Stand by Phase 13
3.1 Purpose of the Standby Phase 13
3.2 Method by which the hospital will be put on stand by 13
3.3 Procedure by which stand by will be upgraded to full activation/stood down 13
4 Activation Procedures 14
5 Stand down 14
6 Recovery 15
7 Training & exercising 15
8 Plan Procedures – in brief 15
Action Cards:
Telephonists 17
Control Team
• Director of Nursing – Nursing Controller 21
• Hospital Manager/Deputy 22
• Clinical Director 24
Medical Staff
• Emergency Medicine Consultant – Role of Triage Officer 26
• Consultant Surgeon on Call (Surgical Incident) – Snr Clinical Doctor & Acute Admitting
Ward Doctor 30
• Consultant Physician on Call (Medical Incident) – Snr Clinical Doctor & Acute Admitting
Ward Doctor 30
• Emergency Medicine Registrar – Triage Officer 32
• Consultant Anaesthetist on call – Resuscitation Lead Doctor 36
• Anaesthetist Registrar on call – Resuscitation Lead Doctor 38
• Consultant Orthopaedic Surgeon on call – member of Resuscitation Team 40
• ED SHO/Orthopaedics SHO & Registrar and Surgical Registrar’s – Resus Doctor 42
• Medical SHO on Call (Surgical Incident) – Minor Injuries Doctor –OPD 44
• Surgical SHO on call (Medical Incident) – Minor Injuries Doctor – OPD 44
• Consultant Histopathologist on Call 46
• Surgical SHO on call (Surgical Incident) – Doctor Acute Admitting Ward – Redwood 47
• Medical SHO on call (Medical Incident) – Doctor Acute Admitting Ward – Elm 47
• Consultant Radiologist on call 49

3
Nursing Staff
• Director of Nursing Office – Senior Nursing Manager 51
• Emergency Dept. Clinical Nurse Manager/Snr Nurse – Emergency Dept. Co-ordinator 53
• Bed Management Department & Patient Flow Team 56
• Clinical Nurse Manager – OPD – Minor Injuries/Green Area 60
• Green Area Discharge Team 62
• Clinical Nurse Manager – Redwood Ward – Acute Admitting Ward (Surgical Incident) 63
• Clinical Nurse Manager – Elm Ward – Acute Admitting Ward (Medical Incident) 65
• Theatre Clinical Nurse Manager/Deputy 67
• ICU – Clinical Nurse Manager 69
• CCU – Clinical Nurse Manager 70
• Clinical Nurse Specialist in Infection Control – Temporary Mortuary – Physio Treatment
Room 71
• CSSD Manager 73
• Cherry/Cypress/Laurel & Maple - Clinical Nurse Manager 74
• Surgical Day – Clinical Nurse Manager 76
• Beech & Rowan - Clinical Nurse Manager 78
• Holly Day Hospital – Clinical Nurse Manager 80
• Woodlands – Clinical Nurse Manager 82
Allied Health Professional Staff
• Head Medical Social Worker 83
• Social Worker – Discharge Team 85
• Laboratory Manager 86
• Radiography Services Manager 88
• Physiotherapy Department – Temporary Mortuary in Physio Treatment Room 90
• Allied Health Professionals – not involved in the first stage of a Major Emergency 91
Administration Staff
• Chief Pharmacist 92
• Emergency Department Clerical/Admin Supervisor 93
• Emergency Department Clerical/Admin Staff 94
• Senior Admin Staff – OPD – Minor/Green Area 95
• Admin Staff – Green Area Discharge Team 97
• Business Managers 98
• Administrative Co-ordinator – Snr Admin Managers 101
• Theatre – Ward Clerk 102
• Cherry/Cypress/Elm/Laurel/Maple & Redwood – Ward Clerk 103
• Information Help Line – Communication Centre – Snr Admin Managers 104
• Radiology Dept. – Admin Supervisor 105
• Chaplaincy Department 107
• Nurse Practice Development Staff & Snr Admin Staff – Scribes 108
• Department of Clinical Engineering 109

4
Support Services
• Security Department 110
• Transport Supervisor 112
• Hospital Driver 113
• Environment Manager 114
• Materials Manager 115
• Catering Manager 117
• Estate’s Manager 118
• Household Services Officer 119
• Contract Cleaners/Derry Court 120
• Portering Services Manager/Shift Leader 121
Appendices
• Appendix 1 – Surge Capacity Plan for ED 123
o Hospital Manager 124
o Director of Nursing 125
o Clinical Director 126
• Information for Staff on duty at the time of MEP Activation 128
• Major Emergency Notification Form 130
• Internal Phone Numbers – during Major Emergency Plan 131
• Addresses & Telephone Numbers for Local Hospitals 133
• Emergency Services Telephone Numbers 134
• Nursing Agencies, Telephone & Faxes 134
• Taxi’s & Private Ambulance’s 134
• Major Emergency Planning Steering Committee 135

5
Section 1: Introduction _____________________________________________________________________
Connolly Hospital has developed this Major Emergency Plan in order to provide hospital
personnel with a plan of action to provide a structured, coordinated and timely response to a
major emergency. The plan uses an “all hazards” approach: it can be applied to a wide range of
possible causes and scenarios. The plan outlines the responsibilities of individuals and
departments, prioritises major emergency requirements / actions and conceptually establishes
how the major emergency should be managed. The hospital’s Major Emergency Plan is a subset of
health service regional and national Major Emergency Plans and is in accordance with emergency
management standards and guidance as outlined in the interagency document “A Framework for
Major Emergency Management”.
The Hospital General Manager has responsibility:
� For implementation of this Major Emergency Plan
� For maintenance of the plan to ensure proper quality, security, integrity, accuracy,
consistency and accessibility
Any queries or suggested amendments should be addressed the Hospital Major Emergency
Management Coordinator for presentation to the Hospital Major Emergency Management
Committee for inclusion in the review process.
Connolly Hospital Major Emergency Plan is issued to:
� Hospital Manager
� Director of Nursing
� All Consultant Medical Staff
� Assistant Director of Nursing/Night Superintendents
� Clinical Nurse Managers III, Site Nurse Managers
� Emergency Department Clinical Nurse Manager
� I.C.U. Clinical Nurse Manager
� C.C.U. Clinical Nurse Manager
� Theatre Clinical Nurse Manager
� Bed Manager
� All Action Card Holders
� Clinical Nurse Manager’s (Wards)
Each of the above should study and familiarise themselves and their staff with the relevant
sections.
NB: No plan can provide for all of the various situations which could arise, but this Plan
should ensure that those involved are aware of their responsibilities and that the
necessary procedures are initiated without delay. It is not intended, nor must it be
interpreted, as a restriction on common sense or initiative in the light of the governing
circumstances.

6
Review/ Update
The Major Emergency Plan will be reviewed and updated:
� Following activation of the plan
� Following hospital structural /organizational / service delivery changes
� Following exercise and / or testing of the Major Emergency Plan
� In light of risk assessments and review of incident reports
� Otherwise on an annual basis
The Major Emergency Plan layout follows the phases of a Major Emergency: Preparation,
Response and Recovery. It includes “Action Cards” for key personnel.
The master Major Emergency Plan will be held centrally on-site by the Hospital Major Emergency
Planning Coordinator and a copy will be kept by all departments / units. It can also be download
from the Connolly Hospital intranet site. Departments must notify the Hospital Major Emergency
Planning Coordinator if any changes and / or alterations occur within their department which
could affect implementation or performance of the Hospital Major Emergency Plan.
The Hospital Major Emergency Planning Coordinator is: Annette Murphy, Business Manager,
Ext: 5640, e-mail: [email protected]
In most major emergencies the hospital will not be responding in isolation: other hospitals,
ambulance services, community services and others will likely activate their major emergency
plans. Some Major Emergencies may require a wider regional or even a national response. The
Hospital Plan facilitates a coordinated health service and wider interagency response through
health service Crisis Management Teams and the interagency Local (or Regional) Coordination
Group.
Hospital Support Structure
Hospital Major Emergency
Control Team
Health Service Regional Crisis
Management Team
Health Service
Site Controller of
Operations
Multiagency Local / Regional
Coordination Group

7
Definition of Major Emergency
Definition of a Major Emergency
“A Major Emergency” can be defined as any event which, usually with little or no warning:
• Causes or threatens:
1. Death or Injury
2. Serious disruption of essential services, or
3. Damage to Property
• Is beyond the normal capabilities of the Health Services, Local Authorities (including Fire
Services) and Gardai Services.
Examples of such emergencies would be:
1. Multiple Motor Vehicle Collision
2. Air Disasters
3. Major Factory Accidents
4. Accidents involving vehicles engaged in transportation of hazardous substances by
road/rail
5. Fires
6. Bombings
It should also be noted that a Major Emergency could arise as a result of flooding and blizzard
conditions.
As far as medical and hospital services are concerned a Major Emergency can be defined as any
event, which produces more casualties than the services can normally cope with.
For the hospital, the definition of a major emergency will be met by the immediate or imminent
arrival of a number of priority 1 or priority 2 patients which necessitates the activation of the
measures contained in this plan.
Identification of a Major Emergency may arise from ED attendance pattern, notification by
Ambulance Control or notification by a Designated Person(s) (see list under “Activation”).

8
Plan Title: Connolly Hospital’s Major Emergency Plan
Plan version Number: 3 Date: November 2013
Issued to: Heads of Department, Consultants & Clinical Nurse Managers
The Major Emergency Planning Co-ordinator of Connolly Hospital has issued this plan to you.
If there are queries with regard to this document please contact the Co-ordinator directly at
telephone ext. 5640.
This hospital operates a policy of version control of its Major Emergency Plan. This is done to
ensure that the relevant personnel/services are always working with the most up to date
version of the plan.
Should this document be copied for others, that copy would be considered invalid.

9
2. Areas of Responsibility _____________________________________________________________________
2.1 Principal Functions
In general the following are the main functions of Connolly Hospital:
• Activation of hospital Major Emergency Plan
• Assessment of casualties and determination of priorities for their treatment
• Provision of appropriate medical services
• The suspension and resumption of routine activity
• Liaison with relevant organisations
• Maintain a level of service to population during a Major Emergency
• Structured review of performance following activation
2.2 Persons authorised to activate the plan or how can the plan be activated
The authority to activate the plan is confined exclusively to the following:
• By notification from Ambulance Control stating they have activated their Major Emergency
Plan due to Major Emergency. A member of the Hospital Control Team will based on the
information provided decide to activate Connolly Hospital’s Major Emergency Plan – see
Major Emergency Message, below
• A member of the Hospital Control Team i.e. Hospital Manager, Director of Nursing or
Clinical Director
• Senior Staff in Emergency Dept. may request via the Control Team that the plan is
implemented
Major Emergency Message
The hospital may be alerted to an event that has occurred, or is imminent, that may require
activation of the Hospital Major Emergency Plan. This can occur by a METHANE message from the
Ambulance Service (METHANE - Major Emergency; Exact Location; Type; Hazards; Access; Number
injured; Emergency Services involved), pattern of self presentation to ED or by contact from the
HSE Regional Crisis Management team.
Only the person(s) designated in the Plan can activate the hospital Major Emergency Plan.
The plan is activated using the following phrase:
“This is ---- (name and designation). Connolly Hospital’s Major Emergency Plan is now activated”.
The Telephone Operator will then implement the Major Emergency Procedures (see page 12)
2.3 Responsibility of key individuals
When the Emergency Plan is activated, there are a number of agreed procedures and
arrangements to be followed to ensure an effective response.

10
The “Hospital Control Team” has full responsibility for the response to the incident.
Hospital Control Team consists of the following:
• Hospital Manager or designate
• Clinical Director or in their absence Consultant Physician on call for a surgical incident or
the Consultant Surgeon on call for incident of medical nature
• Director of Nursing or Ass. Director of Nursing
Location of Control Team-Hospital Manager’s Office, Admin Block
Each member of the group will have their own functions appropriate to their discipline. As a group
they will control and manage the hospital throughout the period of the incident.
Triage Officer
The Consultant in Emergency Medicine or in his/her absence the most senior medical or nursing
staff member present will assess all casualties as soon as they enter the Emergency Department of
the Hospital and decide on the priority (see page 25)
Minor Injuries Doctor
The Minor Injuries Doctor will be the Medical SHO, until 2nd
Medical Consultant arrives in the
event of a surgical emergency or the Surgical SHO, until 2nd
Surgical Consultant arrives in the
event of a medical emergency. (Page 35) An ANP & Physio will be assigned to the Minor Injuries
Area.
Resuscitation Lead Doctor
Anaesthetist NCHD until relieved by Consultant Anaesthetist: Role is to co-ordinate the initial
resuscitation of a large number of undifferentiated patients requiring resuscitation. (Page 27)
Acute Admitting Ward Doctor
Surgical SHO on call for Surgical Incident or Medical SHO on call for Medical Incident, pending
arrival of Consultant Surgeon (Surgical Incident) or Consultant Physician (Medical Incident). (Page
23)
Emergency Department Co-ordinator
Emergency Department Clinical Nurse Manager. (Page 44)
Senior Clinical Lead Doctor
Consultant on call who will lead in Emergency Dept. until 2nd
ED Consultant arrives
2.4 Key Roles and Location of key areas
Control Room: The Control Room is located in the Hospital Manager’s Office. The following
personnel are located in the Control Room.
Hospital Manager or Designate Ext: 5102

11
Director of Nursing/Senior Nurse on Duty Ext: 5179
Clinical Director or Designate Ext: 5178
(All three of the above make up the Hospital Control Team and may be
contacted at any of the extensions listed above)
Triage Officer located at Ambulance Entrance to Emergency Dept.
(Emergency Medicine Consultant or Senior Emergency Dept. staff on duty)
Minor Injuries Officer located in Out Patients Department Ext: 5824/5/6
Emergency Department Co-ordinator located in Emergency Dept. Ext: 6252/3
Senior Clinical Lead Doctor located initially in Emergency Dept. and then in Acute Admitting
Ward (Redwood Ward for Surgical Incident or Elm Ward for Medical Incident)
Resuscitation Lead Doctor located in Red Area, Emergency Dept. Ext: 6258/6259/6261
Acute Admitting Ward during Major Emergency Activation is REDWOOD WARD (Surgical
Incident) Ext: 6300/1/2: ELM WARD (Medical Incident) Ext: 6400/6401/6402
Patients referred to/for X-ray will progress to Acute Admitting Ward i.e. Redwood (Surgical
Incident) or Elm Ward (Medical Incident) and not return to Emergency Dept. unless serious
deterioration. The decision on where the patient goes after x-ray will be made by the treating
Doctor in conjunction with the ED Co-ordinator
If a patient is transferred directly from x-ray to the ward the Doctor in ED needs to call the Acute
Admitting Doctor on the ward for verbal handover.
Communication Centre Ext: 5741/5250
Based in Risk Management Dept.. Ext: 5170/5696
Administration Block Ext: 5089/5098
Media Location Ext: 5455/5459/5458
Nurse Education Centre
Relatives Area Ext: 5112
Staff Restaurant, Administration Block
2.5 Colour Coding/Injury Categories
The Triage Officer will designate the severity of injury. The following colour coding will be used to
identify injury categories and treatment areas.

12
Injury Code Location
Severe Red Emergency Department
Moderate Yellow Emergency Department
Minor Green Out Patients Department
BID White Temporary Mortuary in Physio treatment room-
Dept. of Physical Medicine (following prouncement
of death in Emergency Dept.)
2.6a Crisis Management Structure
When the Emergency Plan is activated, there are a number of agreed procedures and
arrangements to be followed to ensure an effective response.
The “Control Team” has full responsibility for the response to the incident and consists of:
• Hospital Manager or Designate
• Director of Nursing or Asst. Director of Nursing
• Clinical Director or Designate
Upon being notified that the Major Emergency Plan is in operation, members of the Control Team
will go immediately to the Control Room (Hospital Manager’s Office)
2.6b Patient Flow during MEP activation
• All casualties from the incident, all patients waiting in the Emergency Dept. unfit to be
allowed home, and all other (non MEP) patient(s) who present to ED during the activation
period are triaged and incorporated into the MEP response.
• Patients in the ED waiting room will be advised of alternative arrangements.
• Patients deemed suitable for GP assessment will be advised to attend GP.
• Other patients will be urgently accommodated on the wards.
• Unstable patients will remain in ED.
• All casualties will arrive to the Ambulance Entrance of the ED. All other entrances will be
closed to patients.
• Triage: casualties will be diverted to RED, YELLOW, GREEN OR WHITE areas.
• Triage is DYNAMIC and re-diversion will occur if change in patient status occurs.
• This will be coordinated by the ED Coordinator.
• Patients for RED/YELLOW Areas who proceed to the Radiology Dept. will not return to the
Emergency Dept. but proceed to the Acute Admitting Ward (Redwood – Surgical incident
or Elm – Medical incident) for reassessment. If significant deterioration occurs while in x-
ray a patient can be returned to the ED following discussion with the ED coordinator.
• Any patient being discharged MUST be seen by the DISCHARGE TEAM in the GREEN AREA.
• ALL discharged patients will be offered follow up and must have their contact details
recorded so that follow up can be arranged.

13
• All patients triaged as WHITE (Dead) will be removed to the TEMPORARY MORTUARY in
Physio treatment room, Dept. of Physical Medicine.
2.7 Dealings with the Media
Communications with the media is the responsibility of the Hospital Manager and the Health
Services Executive’s Communications Director. Any queries in this regard should be directed to the
Hospital Manager (during MEP activation) who can be contacted at ext: 5102
3. Stand by phase
___________________________________________________________
3.1 Purpose of the Standby Phase
The function of the standby is to inform certain departments that an incident has taken place or is
likely to take place and that the full Major Emergency Plan may need to be activated.
3.2 Method by which the hospital will be put on stand by
• Ambulance control will inform Emergency Department or Switch an incident has occurred
• Confirm incident has taken place by returning call to National Ambulance Control @
6709111 or Dublin Fire Brigade Control via the Red Phone
• Member of Control Team contacted by Switch and informed of incident, decision made by
Control Team to put hospital on stand by
• Staff in Emergency Dept (if call is received in ED) inform Switchboard of incident
• Switchboard staff notify the following:
o Emergency Dept. Consultant on Call
o Emergency Dept. – CNM (if call not received in ED)
o Hospital Manager and Senior Managers
o Director of Nursing or Snr. Nursing Officer
o Clinical Director
o Consultants on call
o All personnel listed in phase 1
• 10 minutes following Major Emergency Alert Telephonist is to inform Hospital Manager
(office hours)/Director of Nursing/Designate (out of hours) of failure to contact personnel
3.3 Procedure by which stand by will be upgraded to full activation or stood down
The authority to upgrade the stand by to full activation of the Emergency Plan is the exclusive
responsibility of one of the following key personnel:
o Member of the Control Team i.e. Hospital Manager, Director of Nursing or Clinical
Director
o Snr. Staff in Emergency Dept. via the Control Team – when a situation that results in
casualties being brought to the hospital, or any situation that puts excess pressure on our
services
o Ambulance Control may request that our Major Emergency Plan is activated

14
o When a Senior Officer of the Gardai or Fire Service contacts the hospital, advising that a
major emergency has occurred. A member of the Control Team will then decide to
activate plan.
The authority to stand down the Major Emergency Plan is confined to the Control Team.
4. Activation Procedures
__________________________________________________________________
When the decision is made to activate the Major Emergency Plan the Switchboard staffs are
informed, who in turn informs everyone on the Phase 2 listing with the following message –
phone:
“The Major Emergency Plan has been activated. Please make your way to the hospital
immediately”.
Contingencies for long-term response
____________________________________________________________________
In the event that the emergency requires a long term response, the control team will issue the
directive that all elective work will be cancelled. This will require extensive communication with
patients. Patients medically fit or suitable may be transferred to another facility or discharged.
The hospital’s Control Team should meet once daily or several times daily, as required.
Control Room will be manned by middle management who is able to call on senior management in
the event of any issues or any escalation of the emergency.
5. Stand down
_____________________________________________________________________
The authority to stand down the Major Emergency Plan is confined to the Control Team. Stand
down will be on a phased basis through the hospital i.e. depending on department activity.
Documentation: All documentation which is used in the event should be stored, following stand
down. No documentation should be destroyed or put into waste bins.
Each department should confirm the name of the person giving the stand down instruction and
prepare a report on their response, activities, lessons learned and should take part in a general de-
brief.
Following stand down – it is essential to update any patients with blood transfusion, ensuring of
the patient has the correct name band with updated patient identifiers.
Send a new group & screen sample to the lab with the updated identifiers.
This sample will be used for future blood components/products.

15
6. Recovery
_____________________________________________________________________
Following stand down, a preliminary de-briefing will be held involving all heads of department.
Decisions are made at this stage on when:
a. Review Clinics are to be held (should be held within 72 hours)Control Team will
advise location of clinics
b. When normal activity can be resumed taking into account capacity and staffing
resources
c. Psychological support for staff will be provided by Critical Incident Stress debriefing
teams from Staff Care
d. A date for a formal debriefing is scheduled
e. Following formal debriefing plan may need to be altered/changed
7. Training and exercising
_____________________________________________________________________
All Heads of Departments and key personnel referred to in this plan should familiarise themselves
with the plan and carry out any preparatory work or make the necessary arrangements as outlined
in the plan.
Plan Procedures – in brief 1. The Hospital Manager is responsible for ensuring that the procedures in this Plan are revised and
updated, and regular staff training exercises are organised.
2. Heads of Departments/Action Card Holders are responsible for ensuring that all staff in their
departments and in particular new staff are familiar with the procedures outlined in this Plan.
3. Each ward and department must hold a copy of this document, which is readily available in the
event of a Major Emergency.
4. The initial contact with the hospital will be through the Telephone Operator or the Health
Authority radio link in the Emergency Department. If the call is received by radio link the Hospital
Telephonist should be contacted to notify senior personnel. The Hospital Manager or a member of
the Hospital Control Team will make the decision to implement the Hospital’s plan.
5. It is essential that once the Major Emergency is declared, traffic outwards on the telephone
system should be curtailed and limited to calls directly related to the Emergency. Standard calls
should not be made through the Telephone 6256.
6. The preparation of the Emergency Department to accept and triage casualties from the site will be
of paramount importance. Patients brought to the Hospital will be received at the Emergency
Department ambulance door only.
7. All Major Emergency Patients being discharged during activation should be seen by Discharge
Teams, based in Green Area (OPD), to ensure follow up appointments are made.
8. All staff alerted must remain at their posts until ‘stand down’ orders are received.
9. All heads of disciplines should contact the Administrative Co-ordinator, Clinical Director’s Office,
Admin Building (ext.5324) upon arrival at the hospital.
10. All heads of disciplines should contact and call in their own staff. It is the responsibility of each
head of department/ward to ensure that they have up to date contact details for all their staff. It is
important to remember staff that have just come off duty, are not available for first contact and
staggering contacting staff in the event incident becoming prolonged is essential.
11. All off duty nursing staff/nursing attendants should report to the Senior Nursing Officer based in
Nursing Administration
12. Medical Staff should report to the Clinical Director in Hospital Manager’s Offices –ext: 5178
13. Relatives will be located in Staff Restaurant, Administration Block.

16
14. The media will be located in the Nurse Education Centre, Academic Centre.
15. The Manager of each ward/department is responsible for keeping a log of events and decisions
made during the incident. This should be given to a member of the Control Team after the
incident.
16. It is the responsibility of the Control Team to ensure a log is kept at the Control Centre and that
all events and decisions are recorded. They are also responsible to ensure all logs and records
kept by the managers are secured after the incident.
17. All staff must wear Connolly Hospital identification badges at all times during a Major
Emergency.
18. Patient confidentially must be respected at all times.
This plan will be reviewed on a bi-annual basis, following an incident or where there are any changes to
hospital/regional policy.

17
Telephonists
Internal Contact No: 5141/5120 and 9
Department Role:
Activate the Hospital call out plan.
Authority to activate the plan is confined exclusively to the following:
• Member of the Control Team i.e. Hospital Manager, Director of Nursing or Clinical Director
• Senior Staff in Emergency Dept. may request via Control Team
Action Card
Phase 1 – Alert Phase
In the event of a Major Emergency Alert notification will be received via Ambulance Control the
Telephone Operator will:
1. Note the details from the call (if received by Switch) on the agreed form - This will occur by
a METHANE message from the Ambulance Service (METHANE - Major Emergency; Exact
Location; Type; Hazards; Access; Number injured; Emergency Services involved)
• Source of Information i.e. Name and contact number of controller
• Date Call Received
• Time Call Received
• Exact location of Incident
• Type of Incident
• Hazards e.g. Radiation
• Number of Casualties
• Estimated time of Arrival at Hospital
2. Verify call by contacting Ambulance Service Tele. 01 6709111 (if not already verified by the
Emergency Department via radio link) or if call from DFB use Red Phone in ED to verify
3. Contact each member of the Control Team i.e. Hospital Manager, Director of Nursing or
Clinical Director, who will decide to put the hospital on alert, based on information
received
4. Contact the following people by bleep/phone with the message:
“The Hospital has received notice of a Major Emergency and has been put on alert”
• Senior Nursing Officer (Director of Nursing/ Ass. Director of Nursing or CNMIII- Site
Nurse Manager)
• Emergency Department
• Emergency Department Clinical Nurse Manager
• Emergency Medicine Consultant
• Hospital Manager
• Clinical Director
• Consultant Surgeon on duty
• Orthopaedic Consultant on duty

18
• Consultant Radiologist on call
• Consultant Physician on duty
• Consultant Anaesthetist
• Consultant Histopathologist
• On call teams
• Theatre Clinical Nurse Manager
• Radiographer on duty
• Laboratory Manager (office hours) Medical Scientist on call (out of hours)
• Medical Physics & Clinical Engineering
• Back up telephonist (if not on duty)/call in receptionist from front desk if on duty
10 minutes following Major Emergency Alert Telephonist is to inform Hospital Manager (office
hours) or Director of Nursing or designate of (out of hours)
• Failure to contact personnel
Phase 2 – Activation Phase
In the Event of a Major Emergency
1. The Hospital Emergency Plan may be implemented by decision of a member of Hospital
Control Team arising from the upgrading of Major Alert Status
NB: Prior notification may not be received and the first contact may be patients arriving in the
Emergency Department from a Major Emergency or notification from one of the other
responding emergency services e.g. Gardai.
If contacted by any source outside the hospital the call should be immediately be referred
to Ambulance Control – 6709111
2. When verification of a Major Emergency is received the Telephonist will re-contact all
people listed in Phase 1 together with the following people. If any telephone number is
engaged the Telephonist will proceed through the list and retry engaged numbers later.
Bleep/Text Message Phase 2 (where appropriate):
“The Major Emergency Plan has been activated. Please make your way to the hospital
immediately.”
• Back up Telephonist/s (Supervisor if not on duty)
• Consultant Pathologist
• Radiographer on duty

19
• All Senior Managers e.g. Business Managers, Human Resource Manager, Risk Manager
• Bed Manager
• Security/Manager
• Head Medical Social Worker
• Clinical Nurse Specialist in Infection Control
• On Call NCHD’s
• Laboratory Manager
• Chaplain
• Chief Pharmacist
• Estates Manager
• Supplies Officer
• Contract Cleaners - Supervisor
• Head of Household Services
• Hospital Driver on duty
• Physiotherapist on call
• CSSD Manager
• Catering Manager
• Portering Services Manager/bleep
• Transport Supervisor
• Head Gardener
• This list is not listed by priority
3. Contact Hospital Manager/Control Centre EXT. 5102/5178/5179 and report any contact
failure.
4. Contact I.C.T. Voice Comms (i.e. John Graham) to inform of plan’s activation (contact
details held at switch)
6. Have contact details of NCHD’s not on call available for Clinical Director if required.
7. Direct all patient enquiries to the Gardai Casualty Enquiry Bureau (Gardai will issue contact
number at an early stage) or Information Help Line in Risk Management Office ext;
5170/5741.
8. Press/Media enquiries should be directed to the Control Team ext. 5102 and 5178 if
Communications Director is not on site
9. Enquiries from relatives should be directed to Risk Management Department @
5170/5741/5089/5250/5098
10. Keep a list of all switchboard staff involved in the incident (including time of arrival and
departure).
11. Document all actions taken, to be sent to Control Centre when activation is stood down
12. Give Stand Down instruction to departments as informed by Control Centre

20
13. Please do not leave your post until the Control Centre has issued stand down.
Location Reporting
It is the responsibility of this department to make a status report of their areas activities in relation
to the functions identified in this section. At any time during the plan activation an incident arises
which could impede the fulfilment of this function contact should be made with the Control
Centre to resolve the issue.
Stand Down
A call will be received in the department via the phone line from the Control Centre stating that
the Hospital Manager has instructed that we now step down from Major Emergency activation
and start the process of returning to normal activities. The staff member who receives this stand
down ensures that the senior member of staff in charge of the department at the time, records
the time of stand down and informs all staff under their control.
It should be noted that activation of Stand Down will not always indicate that the work of the
Department are complete. Ensure that there are sufficient staff to handle the expected workload
and Stand Down the remaining staff.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

21
Director of Nursing
Nursing Controller
Internal Contact No 5123/5121 (during office hours), out of office hours via the Switchboard
During MEP Activation: 5179
Activation Procedure
In the event of Connolly Hospital being put on alert the Director of Nursing, will be contacted by
the Switchboard. He/she based on information received may activate plan.
Action Card
Once second Senior Nursing Manager arrives on site (if out of hours), the Director of Nursing or
most senior of Nurse Manager present becomes a member of the Control Team.
• If Hospital Manager is off site the Director of Nursing (based on information received
from ambulance control) may decide to activate the Hospitals Major Emergency Plan in
conjunction with Emergency Dept. and Senior Manager
o Report to the Control Centre – Hospital Managers Office
o If first member of Control Team to arrive set up the Control Centre
o Liaise with the Bed Manager
o Ensure that the Bed Manager is given all information pertaining to
discharges/admissions/transfers of patients
o Liaise with the Snr. Nursing Manager (administration) and assess staffing needs in the:
o Emergency Department, including Care Attendants
o Theatre
o X-ray
o Ensure that routine operating theatre lists, outpatient clinics and Day Case activity
are suspended
o Ensure that Ward Managers have made contingency plans to staff wards and departments
throughout the Emergency and for the following day
o Contact agency for more staff if required
o Ensure all decisions are documented
o In conjunction with other members of Control Team agree on step down arrangements
o In conjunction with other member of Control Team agree location of Special Review Clinics
& staffing of same (possible location – Surgical Day Ward)
o In conjunction with other members of Control Team agreed for a swift debriefing of staff
o Following stand down visit all departments with the other members of the Control Team:
o Thank staff
o Get up to date information on staffing levels
o Give information on debriefing and follow up
o Collect lists of staff involved in the Emergency
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

22
Hospital Manager/Deputy
Internal Contact No: 5178/5179 (during office hours, out of office hours via the Switchboard)
During MEP Activation: 5102
Function/Role:
• Ensure the Hospital’s efficient response to a Major Emergency
Activation Procedure
In the event of Connolly Hospital being put on alert the Hospital Manager, will be contacted by the
Switchboard. He/she based on information received may activate plan. Ambulance Control may
request that the plan is activated in such cases Hospital Manager will be notified by Switchboard
for an immediate decision.
Action Card
• Based on information received the Hospital Manager, may decide to implement the
Hospital’s Emergency Plan
• Notify Switchboard to implement the plan
• Report to the Control Room, Hospital Managers Office, if first to arrive set up room
• Assign one member of senior staff to take on the role of Administrative Controller, to be
based in Clinical Director’s office, ext: 5324
• Ensure senior administrative staff are being notified by either the Switchboard or
Administrative Controller, including Estates Manager, I.C.T. co-ordinator and Waste
Manager (if required)
• Confirm with Switch via Admin. Co-ordinator that contact was made with Chief Pharmacist,
if unavailable liaise with Clinical Director re staffing of Pharmacy
• Delegate a senior staff member to record all calls and decisions taken during emergency
for each member of the Control Team
• Notify the Regional Director Of Operations, Dublin North East, Health Service Executive of
the Plan’s implementation
• Notify the Gardai in the local Blanchardstown Station of the Plan’s implementation
• Liaise with the Director of Nursing and Medical Director to ensure the efficient
management of the Hospital throughout the Major Emergency
• Establish links with Chief Ambulance Officer and confirm hospital situation regarding bed
availability
• Establish links with the Gardai Liaison Officer based in Emergency Dept.- Ext: 6266
• Ensure all departments are staffed and identify any deficiencies in services
• Confirm all supplies regarding equipment, stores and pharmaceutical are available
• Confirm all patient transfers/discharges are in hand or are completed
• In consultation with HSE, Communication Director, prepare press release and deal with
media enquiries
• Arrange for regular information bulletins to be made to families, press and staff

23
• In conjunction with other members of the Control Team decide on stand down
arrangements for each department on an individual basis
• In conjunction with other members of the Control Team decide date, time, venue and
staffing arrangements for Review Clinic –suggested location, Surgical Day Ward
• Ensure that all documentation is collected from each department following stand down
• In conjunction with other members of Control Team agreed for a swift debriefing of staff
• Following stand down visit all departments with the other members of the Control Team:
o Thank staff
o Get up to date information on staffing levels
o Give information on debriefing and follow up
o Collect lists of staff involved in the Emergency
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

24
Clinical Director
If Clinical Director is not available, Consultant Physician on call will take
on this role in the event of a Surgical Incident, Consultant Surgeon on
call will take on this role in the event of a Medical Incident
During MEP activation contact no: 5178 (Hospital Manager’s
Office)
Function/Role:
Supervise the Hospital’s medical response to a Major Emergency
Activation Procedure
In the event of Connolly Hospital being put on alert Clinical Director will be contacted by the
Switchboard. He/She can based on the information received and in conjunction with other
members of the Control Team, decide to activation of plan.
Action Card
• Report immediately to the Control Room – Hospital Managers Office
• If first to arrive arrange/set up room as necessary
• Arrange for further Consultant Staff to attend as appropriate
• Arrange for NCHD’s not on call to be contacted if required (contact details with
Switchboard)
• It is important to remember staff who have just come off duty, are not available for first
contact and staggering contacting staff in the event incident becoming prolonged is essential
• On advice from Hospital Manager assign a NCHD (non intern) to Pharmacy as Chief
Pharmacist not available
• Contact medical/surgical teams as appropriate to identify patients suitable for
discharge in conjunction with the Bed Manager
• Monitor status in Emergency Department, ICU and Theatre
• Liaise with Snr Nursing Manager/Hospital Manager/Triage Officer/Emergency
Department Clinical Nurse Manager with regard to allocating medical staff to:
o OPD (minor injuries area)
o Surgical Teams
o Theatre Teams
o Emergency Department Teams
• Liaise with Consultants and Snr. Nursing Manager on potential patient discharge
• Assist liaison between ED and other hospitals regarding transfer of patients if required
• In conjunction with Anaesthetist assign medical staff to accompany patients
transferring to other hospitals
• Monitor admissions and injury severity
• Agree Stand Down in conjunction with other members of the Control Team
• Assign Medical Staff to attend Review Clinic (to be held within 72 hours)
• Ensure medical actions taken during an Emergency are documented including dates,
time and signature of staff

25
• In conjunction with other members of Control Team agreed for a swift debriefing of
staff
• Following stand down visit all departments with the other members of the Control
Team:
o Thank staff
o Get up to date information on staffing levels
o Give information on debriefing and follow up
o Collect lists of staff involved in the Emergency

26
Emergency Medicine Consultant
Role of Triage Officer
Emergency Medicine Consultant or Most Senior member of Emergency
Medical/Nursing staff present, if 2nd
Emergency Medicine Consultant is available,
assume the role of Emergency Dept., Lead Doctor – see Consultant Surgeon Action
Card
Role/Function:
• The Triage Team are solely to sort patients into order of clinical priority
• Do not become involved in delivery of care
• Once Triage complete or a 2nd
ED Consultant arrives assume role of ED Lead Doctor
Members of Triage Team:
• Emergency Medicine Consultant or Registrar
• 2nd
most Senior Nurse on duty
• Receptionist from Emergency Department
Activation Procedure
In the event of Connolly Hospital being put on alert the Emergency Medicine Consultant on call
will be contacted by the Switchboard/Emergency Dept. if call received there. If/when full
alert/activation of plan has being implemented the Switchboard will re-contact Emergency
Medicine Consultant.
Action Card
• Assist in vacating Emergency Department
• Establish Triage Point at Ambulance Entrance
• Initially expect a large influx of casualties and use simple Triage Sieve. As MEP evolves you
may be able to proceed to a more advance Triage Sort (see attached).
• Pronounce all Death’s. Ambulance will take them directly to the Temporary Mortuary
(Physio Treatment Room).
• On arrival of patient ensure correct category on cruciform card
• Distribute pre assembled charts and packs
• Ensure patient name band is attached and attach patient identification label to chart
• Monitor numbers of patients arriving
• Determine order of priority and direct patients to appropriate area
• Liaise with Medical Co-ordinator (Control Team – ext. 5178) for
o Allocation of medical staff to Emergency Teams

27
Minimum data set required for unconscious/unknown patient for blood transfusion purposes:
Sample and request card must include:
• Unique MEP number
• Unknown Male/Female (instead of
name, if unknown)
• Signature of person taking sample
• O – (Negative) is a limited resource and
if demand exceeds supply the O – should
be restricted to females of child bearing
age. Other patients can receive O+
positive blood following consultation
with the Consultant Haematologist
Patients referred to/for X-ray will progress to Acute Admitting Ward i.e. Redwood (Surgical
Incident) or Elm Ward (Medical Incident) and not return to Emergency Dept. unless serious
deterioration. The decision on where the patient goes after x-ray will be made by the treating
Doctor in conjunction with the ED Co-ordinator
If a patient is transferred directly from x-ray to the ward the Doctor in ED needs to call the Acute
Admitting Doctor on the ward for verbal handover.
Location Reporting
It is the responsibility of this department to make a status report of their areas activities in relation
to the functions identified in this section. These reports should be made required to the Medical
Co-ordinator in the Control Centre. At any time during the plan activation an incident arises which
could impede the fulfilment of these functions contact should be made with the Control Centre to
resolve the issue.
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
It should be noted that activation of Stand Down will not always indicate that the work of the
Department are complete. Ensure that there is sufficient staff to handle the expected workload
and Stand Down the remaining staff. It may be necessary to leave some staff on duty for a
prolonged period. Arrange a shift cycle to ensure that members of staff are not left on duty for
an excessive period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

28

29

30
Consultant Surgeon on call (Surgical Incident)
Consultant Physician on call (Medical Incident)
Role: Senior Clinical Doctor and Acute Admitting Ward (AAW) Doctor
Will be relieved in ED by 2nd
Emergency Department Consultant if available
Consultant Surgeon (Surgical Incident)/Consultant Physician (Medical Incident) will
remain responsible for the Acute Admitting Ward i.e. Redwood (Surgical
Incident)/Elm (Medical Incident)
Activation Procedure
The Switchboard will inform the Consultant Surgeon/Consultant Physician if Major Emergency Plan
is “activated” or on “stand by”.
Report to Emergency Department when Full Alert is given via Ambulance Entrance and sign in
using swipe I.D. card at Resus door.
Role/Function: Co-ordinate the Medical Response in the RED/YELLOW AREA and the ACUTE
ADMITTING WARD
Action Card
• Co-ordinate assessment and treatment of all patients admitted to Red/Yellow area in
Emergency Dept. and the Acute Admitting Ward (Redwood-Surgical or Elm – Medical)
• Liaise with
o Triage Officer (ED Consultant)
o Resus Lead Doctor (Consultant Anaesthetist)
o Emergency Department Co-ordinator (CNMII)
• Assign doctors/nurse teams to treatment areas e.g. Red/Yellow/Green
• Prioritise patients for:
o Theatre
o Imaging
o ICU
o Transfer to other hospitals
• On arrival of Surgical Colleagues decide on operating teams
• Liaise with Control Centre regarding hospital capacity – ext: 5102/5179/5178
• Liaise with Control Centre regarding stand down arrangements

31
Minimum data set required for unconscious/unknown patient for blood transfusion purposes:
Sample and request card must include:
• Unique MEP number
• Unknown Male/Female (instead of
name, if unknown)
• Signature of person taking sample
• O – (Negative) is a limited resource and
if demand exceeds supply the O – should
be restricted to females of child bearing
age. Other patients can receive O+
positive blood following consultation
with the Consultant Haematologist
Patients referred to/for X-ray will progress to Acute Admitting Ward i.e. Redwood (Surgical
Incident) or Elm Ward (Medical Incident) and not return to Emergency Dept. unless serious
deterioration. The decision on where the patient goes after x-ray will be made by the treating
Doctor in conjunction with the ED Co-ordinator
If a patient is transferred directly from x-ray to the ward the Doctor in ED needs to call the Acute
Admitting Doctor on the ward for verbal handover.
Location Reporting
It is the responsibility of this department to make a status report of their areas activities. These
reports should be made as required to the Medical Co-ordinator in the Control Centre ext. 5178.
At any time during the plan activation an incident arises which could impede the fulfilment of your
role contact should be made with the Control Centre to resolve the issue.
Stand Down
The decision to Stand Down will be made in conjunction with the Control Centre.
It should be noted that activation of Stand Down would not always indicate that the work of the
Department are complete. Ensure that there is sufficient staffs to handle the expected workload
and Stand Down the remaining staff. It may be necessary to leave some staff on duty for a
prolonged period. Arrange a shift cycle to ensure that members of staff are not left on duty for
an excessive period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

32
Emergency Medicine Registrar
Role of Triage Officer
Until relieved by 1st
Emergency Medicine Consultant.
Once relieved assume role assigned by ED Consultant
Role/Function:
• The Triage Team are solely to sort patients into order of clinical priority
• Do not become involved in delivery of care
• Once Triage complete or a 2nd
ED Consultant arrives assume role assigned by ED Consultant
Members of Triage Team:
• Emergency Medicine Consultant or Registrar
• 2nd
most Senior Nurse on duty
• Receptionist from Emergency Department
Activation Procedure
In the event of Connolly Hospitals Major Emergency Plan being put into operation the Emergency
Medicine Registrar will be notified from Emergency Dept.
Action Card
• Vacate Emergency Department
o Patient suitable for GP assessment should be redirected there
o Patients requiring further investigations/admission should be moved to the
Endoscopy Suite
o Unstable patients remain in ED
• Establish Triage Point at Ambulance Entrance
• Initially use simple Triage Sieve. As MEP evolves move to Triage Sort (see attached)
• Pronounce all BID’s then Ambulance to take them directly to the Temporary Mortuary
(Physio treatment room via entrance opposite ED)
• On arrival of patient review cruciform card
• Distribute pre assembled charts and packs
• Ensure patient wrist band is attached (X2) and attach patient identification label to chart
• Monitor numbers of patients arriving
• Determine order of priority and direct patients to appropriate area
o Red Patients to Resus & clinical decision unit
o Yellow Patients to major & minor cubicles
o Green Patients to Out Patients Dept.
o Dead/White patients to temporary Mortuary (Physio treatment room)
• Liaise with Medical Co-ordinator (Control Team - 5178) for
o Allocation of medical staff to Emergency Teams

33
Ensure the Patient’s medical chart stays with the Patient at all times
Minimum data set required for unconscious/unknown patient for blood transfusion purposes:
Sample and request card must include:
• Unique MEP number
• Unknown Male/Female (instead of
name, if unknown)
• Signature of person taking sample
• O – (Negative) is a limited resource and
if demand exceeds supply the O – should
be restricted to females of child bearing
age. Other patients can receive O+
positive blood following consultation
with the Consultant Haematologist
Patients referred to/for X-ray will progress to Acute Admitting Ward i.e. Redwood (Surgical
Incident) or Elm Ward (Medical Incident) and not return to Emergency Dept. unless serious
deterioration. The decision on where the patient goes after x-ray will be made by the treating
Doctor in conjunction with the ED Co-ordinator
If a patient is transferred directly from x-ray to the ward the Doctor in ED needs to call the Acute
Admitting Doctor on the ward for verbal handover.
Location Reporting
• Report on number & status of patients in your area to the Control Team regularly @ ext
5178
• Identify potential risks & obstacles to Control Team early @ ext 5178
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there is sufficient staff to handle the expected workload and Stand Down the
remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

34

35

36
Consultant Anaesthetist on call
Role of Resuscitation Lead Doctor
This role can be performed by Anaesthetist NCHD until arrival of Consultant
Anaesthetist. As MEP progresses if a 2nd
Consultant Anaesthetist is available,
assign staff to ICU, Theatre and Acute Admitting Ward
Activation Procedure
In the event of Connolly Hospitals Major Emergency Plan being put into operation the Consultant
Anaesthetist on Call will be notified when the Hospital is put on alert, by the Switchboard. When
the MEP is activated or when Full Alert is given the Switchboard will inform the Consultant
Anaesthetist on call.
Role/Function:
o Proceed to Red Area – Emergency Dept. and assume role of Resus Lead Doctor
o Co-ordinate the initial resuscitation of a large number of undifferentiated patients
requiring resuscitation
o Will attempt to ensure 2nd
Anaesthetist is available to:
� Complete surgery in progress
� Ensure the stoppage of elective work
� Review ICU bed state
Action Card
• Will attempt to endeavour adequate Anaesthetic staffing to Resuscitation Room in ED to
Co-ordinate the initial resuscitation of a large number of undifferentiated patients
requiring resuscitation from the incident
• Call in extra staff if required
• It is important to remember staff that have just come off duty, are not available for first contact
and staggering contacting staff in the event incident becoming prolonged is essential
• As colleagues arrive assign to:
o Emergency Resus: Assume Role of Resus Lead Doctor
o Theatre: stop elective work and complete surgery in progress
o ICU: review ICU bed state
o Acute receiving ward i.e. Redwood/Elm
o Liaise with lead resus nurse to arrange Doctor/Nurse teams
o Triage will have been performed by ED Consultant and you will receive the most critically
injured into the Red Area (ED Resus and Observation Area)
o Category 1(Red): Patients will have major hemodynamic or respiratory compromise. They
are likely to require emergency surgical or intensive care intervention after standard
resuscitation
o Liaise with Senior Clinical Lead Doctor (Consultant Surgeon or Physician) regarding order of
theatre list

37
o In consultation with Senior Clinical Lead Doctor decide on priority for
o Theatre
o Imaging etc.
o Assess the availability of theatre and the skill mix of staff available in conjunction with
Theatre Nurse Manager
o Liaise with Clinical Director or designate (Control Centre @ 5178) regarding the availability
of theatre space and the likelihood of delays etc.
o Liaise with Radiology re availability of diagnostic imaging
o Liaise with Bed Management re the possibility of using CCU beds as discharge point for ICU
patients
o Liaise with Control Team regarding any potential risks and obstacles as early as possible at
ext. 5178
o Liaise with Control Team regarding Stand Down
o
M Minimum data set required for unconscious/unknown patient for blood transfusion
purposes:
Sample and request card must include:
• Unique MEP number
• Unknown Male/Female (instead of
name, if unknown)
• Signature of person taking sample
• O – (Negative) is a limited resource and
if demand exceeds supply the O – should
be restricted to females of child bearing
age. Other patients can receive O+
positive blood following consultation
with the Consultant Haematologist
Patients referred to/for X-ray will progress to Acute Admitting Ward i.e. Redwood (Surgical
Incident) or Elm Ward (Medical Incident) and not return to Emergency Dept. unless serious
deterioration. The decision on where the patient goes after x-ray will be made by the treating
Doctor in conjunction with the ED Co-ordinator
If a patient is transferred directly from x-ray to the ward the Doctor in ED needs to call the Acute
Admitting Doctor on the ward for verbal handover.
38
Anaesthetist Registrar on call
Role of Resuscitation Lead Doctor
Will be relieved by Consultant Anaesthetist upon his/her arrival. Once relieved
assume role assigned by Consultant Anaesthetist
Action Card
• Will attempt to endeavour adequate Anaesthetic staffing to Resuscitation Room in ED to
Co-ordinate the initial resuscitation of a large number of undifferentiated patients
requiring resuscitation from the incident
• Call in extra staff if required
• It is important to remember staff that have just come off duty, are not available for first contact
and staggering contacting staff in the event incident becoming prolonged is essential
• As colleagues arrive assign to:
o Emergency Resus: Assume Role of Resus Lead Doctor
o Theatre: stop elective work and complete surgery in progress
o ICU: review ICU bed state
o Acute receiving ward i.e. Redwood/Elm
o Liaise with lead resus nurse to arrange Doctor/Nurse teams
o Triage will have been performed by ED Consultant and you will receive the most critically
injured into the Red Area (ED Resus and Observation Area)
o Category 1(Red): Patients will have major hemodynamic or respiratory compromise. They
are likely to require emergency surgical or intensive care intervention after standard
resuscitation
o Liaise with Senior Clinical Lead Doctor (Consultant Surgeon or Physician) regarding order of
theatre list
o In consultation with Senior Clinical Lead Doctor decide on priority for
o Theatre
o Imaging etc.
o Assess the availability of theatre and the skill mix of staff available in conjunction with
Theatre Nurse Manager
o Liaise with Clinical Director or designate (Control Centre @ 5178) regarding the availability
of theatre space and the likelihood of delays etc.
o Liaise with Radiology re availability of diagnostic imaging
o Liaise with Bed Management re the possibility of using CCU beds as discharge point for ICU
patients
o Liaise with Control Team regarding any potential risks and obstacles as early as possible at
ext. 5178
o Liaise with Control Team regarding Stand Down

39
Minimum data set required for unconscious/unknown patient for blood transfusion purposes:
Sample and request card must include:
• Unique MEP number
• Unknown Male/Female (instead of
name, if unknown)
• Signature of person taking sample
• O – (Negative) is a limited resource and
if demand exceeds supply the O – should
be restricted to females of child bearing
age. Other patients can receive O+
positive blood following consultation
with the Consultant Haematologist
Patients referred to/for X-ray will progress to Acute Admitting Ward i.e. Redwood (Surgical
Incident) or Elm Ward (Medical Incident) and not return to Emergency Dept. unless serious
deterioration. The decision on where the patient goes after x-ray will be made by the treating
Doctor in conjunction with the ED Co-ordinator
If a patient is transferred directly from x-ray to the ward the Doctor in ED needs to call the Acute
Admitting Doctor on the ward for verbal handover.

40
Consultant Orthopaedic Surgeon on Call
Role: Initially Member of Resuscitation Team in RED/YELLOW area but you will
proceed to GREEN (Minors) Area (OPD) and Acute Admitting Ward (Redwood –
Surgical or Elm –Medical) as MEP progresses/and/or when colleague become
available
Activation Procedure
The Consultant Orthopaedic Surgeon on call will be notified when Hospital is put on the alert by
the Switchboard, when Full Alert or MEP is activated the Switchboard will re-contact the
Consultant on call.
Report to Emergency Department when full Alert is given via ambulance entrance,
use ID card to record attendance by swiping at Resus door.
Role: Assist your colleagues (Resus Lead Doctor and ED Lead Doctor) in the assessment and
resuscitation undifferentiated casualties
Action Card
• Confirm with Control Team (ext 5178) if Orthopaedic colleagues have been contacted
• Liaise with: o Triage Officer (ED Consultant or Reg) o Resus Lead Doctor (Consultant Anaesthetist or Reg) o Emergency Department Co-ordinator (CNM II)
• Supervise NCHD/Nursing Teams in the resuscitation of patients
• With your Surgical, Anaesthetist & Radiology Colleagues, prioritise patients for: o Theatre o Imaging o ICU o Transfer to other hospitals
As incident evolves progress to reviewing orthopaedic casualties in
Red/Yellow/Green Area and AAW (Acute Admitting Ward)
• Once colleagues arrive, assign staff to Theatre
• Liaise with Control Centre regarding hospital capacity
• Liaise with Control Team regarding any potential risks and obstacles as early as possible
at ext. 5178
• Liaise with Control Centre regarding requirements follow up Fracture/Review Clinics • Liaise with Control Team regarding Stand Down

41
Minimum data set required for unconscious/unknown patient for blood transfusion purposes:
Sample and request card must include:
• Unique MEP number
• Unknown Male/Female (instead of
name, if unknown)
• Signature of person taking sample
• O – (Negative) is a limited resource and
if demand exceeds supply the O – should
be restricted to females of child bearing
age. Other patients can receive O+
positive blood following consultation
with the Consultant Haematologist
Patients referred to/for X-ray will progress to Acute Admitting Ward i.e. Redwood (Surgical
Incident) or Elm Ward (Medical Incident) and not return to Emergency Dept. unless serious
deterioration. The decision on where the patient goes after x-ray will be made by the treating
Doctor in conjunction with the ED Co-ordinator
If a patient is transferred directly from x-ray to the ward the Doctor in ED needs to call the Acute
Admitting Doctor on the ward for verbal handover.
All Major Emergency patients being discharged during activation should be seen by Discharge
Teams in Green Area (OPD) to ensure follow up appointments etc. are made.

42
ED SHO, Orthopaedics SHO and Registrar and Surgical Registrar’s
Role: Resus Doctor
Activation Procedure
In the event of Connolly Hospitals Major Emergency Plan being put into operation all on call
NCHD’s will be contacted by Switchboard, remaining teams will be contacted by Medical Co-
ordinator
Reporting location
All NCHD’s should report to Emergency Department Co-ordinator (CNM) for assignment of role
during Major Emergency
Action Card
o Immediately, assist with disposal of all patients currently in department.
o Form part of Nurse/Doctors teams
o Assess and treat of Red/Yellow patients under supervision of Resus Lead Doctor
o Reassess patients as often as possible and change their priority as necessary
o Manage patients according to ATLS guidelines e.g. airway, breathing, circulation
o Use Major Emergency folders for documentation
o Ensure patient has being given the correct category on Cruciform cards, leave card with
patients while in Emergency Dept.
o Use pre-printed labels
o Once Resuscitation area is fully staffed you may be reassigned to another area e.g. Minor
Injuries Area
o Do Not leave your post without informing lead Resus Doctor
Minimum data set required for unconscious/unknown patient for blood transfusion purposes:
Sample and request card must include:
• Unique MEP number
• Unknown Male/Female (instead of
name, if unknown)
• Signature of person taking sample
• O – (Negative) is a limited resource and
if demand exceeds supply the O – should
be restricted to females of child bearing
age. Other patients can receive O+
positive blood following consultation
with the Consultant Haematologist
Patients referred to/for X-ray will progress to Acute Admitting Ward i.e. Redwood (Surgical
Incident) or Elm Ward (Medical Incident) and not return to Emergency Dept. unless serious
deterioration. The decision on where the patient goes after x-ray will be made by the treating
Doctor in conjunction with the ED Co-ordinator
If a patient is transferred directly from x-ray to the ward the Doctor in ED needs to call the Acute
Admitting Doctor on the ward for verbal handover.

43
All Major Emergency patients being discharged during activation should be seen by Discharge
Teams in Green Area (OPD) to ensure follow up appointments etc. are made.

44
Medical SHO on Call (Surgical Incident)
Surgical SHO on Call (Medical Incident)
Role: Minor Injuries Doctor – until relieved by 2nd
Consultant Orthopaedic Surgeon or other
senior ED or Surgical staff when available
Location: Out Patients Dept.
Activation Procedure
On call teams will be notified when Hospital is put on Alert by the Switchboard, when MEP
activated or Full Alert is given the Switchboard will re-contact the teams on call.
Action Card
o Brief Liaise with Ward Staff to identify patients:
o Who can go home
o Who can be transferred elsewhere on Connolly Hospital campus
o During activation of the Hospital Major Emergency Plan, Registrar can discharge
patients from all specialities
o Nominate intern to liaise with GPs on cases who may need more immediate out patient
follow up e.g. medication/blood testing
o Keep Bed Management ext 5216 & 5217 and Medical Consultant on call informed of bed
state
o Proceed to Minor Injuries Area (Out Patients Department) and assume role
of Minor Injuries Officer o Immediate provision of medical care to minor casualties of the emergency
o Reassess patient’s clinical status using triage sieve/sort & re-assign cruciform card if
necessary
o Liaise with the Snr. Nurse – Green Area re medical needs
o Emergency Nurse Practitioner can assess and treat patients independently
• Further medical staff will be assigned as they become available
• Receive all minor injuries from Triage
• Stabilise patients prior to transfer
• Priorities:
o Assess all injuries and provide analgesia
o Arrange wound cleaning and dressing
o Request x-rays if required (all glass wounds must be imaged)
o Check Tetanus status
• If in doubt re: patient management await arrival of more experienced staff
• Liaise with Green Area-Senior Nurse
• Establish and co-ordinate immediate treatment by minor treatment teams
• Document and identify all patients for registration from major emergency in your area, in
co-operation with administration staff assigned to Green Area
• On instruction from Control Centre stand down all staff

45
Minimum data set required for unconscious/unknown patient for blood transfusion purposes:
Sample and request card must include:
• Unique MEP number
• Unknown Male/Female (instead of
name, if unknown)
• Signature of person taking sample
• O – (Negative) is a limited resource and
if demand exceeds supply the O – should
be restricted to females of child bearing
age. Other patients can receive O+
positive blood following consultation
with the Consultant Haematologist
Patients referred to/for X-ray will progress to Acute Admitting Ward i.e. Redwood (Surgical
Incident) or Elm Ward (Medical Incident) and not return to Emergency Dept. unless serious
deterioration. The decision on where the patient goes after x-ray will be made by the treating
Doctor in conjunction with the ED Co-ordinator
If a patient is transferred directly from x-ray to the ward the Doctor in ED needs to call the Acute
Admitting Doctor on the ward for verbal handover.
All Major Emergency patients being discharged during activation should be seen by Discharge
Teams in Green Area (OPD) to ensure follow up appointments etc. are made.
46
Consultant Histopathologist On Call
Ext: 5397/5353
During MEP Activation ext: 5256
Activation Procedure
Consultant Histopathologist on Call will be contacted by the Switchboard, if/when the decision is
made to activate the MEP or the Major Alert Status is upgraded to Full Alert the Consultant
Histopathologist will be re-contacted by the Switchboard.
Action Card
• Inform the Control Centre via Administrative Co-ordinator at ext: 5324 of your arrival
• Assume responsibility for the temporary Mortuary (Physio Treatment Room)
• Call in Mortuary Staff if required
• Close all blinds in the department
• Turn on air conditioning/fans
• It is important to remember staff that have just come off duty, are not available for first contact
and staggering contacting staff in the event incident becoming prolonged is essential
• Liaise with Clinical Nurse Specialist in Infection Control with regard to additional staffing
needs
• Prepare area in conjunction with Clinical Nurse Specialist to receive the deceased
• Pronounce the patient dead
• Liaise with Clinical Nurse Specialist in Infection Control, Social Worker, Coroner, Gardai
representative and administrative staff assigned to mortuary
• Contact Medical Co-ordinator (Control Centre – ext 5178) if extra medical staff are
required
• Liaise with Control Centre regarding step down arrangements
NB: Remains of casualties pronounced dead on arrival would be placed in Physio Treatment
Room. These remains should be placed in a body bag as soon as possible after arrival. No
attempt should be made to remove effects or to clean the remains, as this could be vital
evident in establishing the cause of death and in making a formal identification. The
identification of these casualties is the responsibility of the Dublin City Coroner and the
Gardai. It is the responsibility of the Coroner to arrange the post mortems of these
casualties.

47
Surgical SHO on call (Surgical Incident)
Medical SHO on call (Medical Incident)
Role: Doctor assigned to Acute Admitting Ward i.e. Redwood (Surgical
Incident)/Elm (Medical Incident) until relieved by more Senior Staff
Function:
• Receive all patients admitted to ward from incident who have not been diverted to ICU or
Theatre
• Receive all patients from X-ray (all patients sent to x-ray from Red/Yellow areas will
proceed directly to Acute Admitting Ward (Redwood-Surgical Incident/Elm- Medical
Incident) from x-ray – following handover from treating Doctor in ED
• Full review of patients (ATLS principles) will be required including review of blood and x-ray
results
• During a Major Emergency a patient may still be in the unstable phase of
their injury when arriving to the Acute Admitting Ward
Activation Procedure
On call teams will be notified when Hospital is put on Alert by the Switchboard, when MEP
activated or Full Alert is given the Switchboard will re-contact the teams on call.
Action Card
• Assist CNM in clearing Acute Admitting Ward (Redwood – Surgical Incident/Elm – Medical
Incident)
• Liaise with Emergency Department Co-ordinator ext- 6252/6253
• Assess patients on arrival from Emergency Department and X-ray
• Review blood reports and x-rays (including CT or US if performed)
• Decide on treatment priorities
• Liaise with Consultant Surgeons/Physicians and Anaesthetists re priorities for Theatre
• Patients who develop life/limb threatening deterioration will need to be identified and
dealt with rapidly
• Document assessment and decisions in chart
Minimum data set required for unconscious/unknown patient for blood transfusion purposes:
Sample and request card must include:
• Unique MEP number
• Unknown Male/Female (instead of
name, if unknown)
• Signature of person taking sample
• O – (Negative) is a limited resource and
if demand exceeds supply the O – should
be restricted to females of child bearing
age. Other patients can receive O+
positive blood following consultation
with the Consultant Haematologist

48
Patients referred to/for X-ray will progress to Acute Admitting Ward i.e. Redwood (Surgical
Incident) or Elm Ward (Medical Incident) and not return to Emergency Dept. unless serious
deterioration. The decision on where the patient goes after x-ray will be made by the treating
Doctor in conjunction with the ED Co-ordinator
If a patient is transferred directly from x-ray to the ward the Doctor in ED needs to call the Acute
Admitting Doctor on the ward for verbal handover.

49
Consultant Radiologist on call
Department Role/Function
• In conjunction with Senior Clinical Lead prioritise patients from Emergency with regard to
radiological requirements
Activation Procedure
In the event of Connolly Hospitals Major Emergency Plan being put into operation the Consultant
Radiologist on call will be notified when Hospital is put on the alert by the Switchboard, when Full
Alert is given the Switchboard will re-contact the Consultant Radiologist on duty
Action Card
• Call in remaining Consultant Radiologists if required
• Liaise with Radiographer on call regarding consulting with Emergency Department re likely
requirements
• Liaise with Radiography Services Manager regarding cancelling of the remainder of
scheduled work (if in normal working hours)
• Liaise with Senior Clinical Lead regarding diagnostic imaging
• Keep Emergency Department Co-ordinator (6252/6253) informed of situation in X-ray
Dept.
• If patient has serious clinical deterioration, contacting Emergency Department Co-
ordinator on 6252/6253 concerning returning patient to Emergency Department for
further assessment.
• Liaise Radiography Services Manager and Administrative Supervisor re department needs
• Stand down when requested
Minimum data set required for unconscious/unknown patient for blood transfusion purposes:
Sample and request card must include:
• Unique MEP number
• Unknown Male/Female (instead of
name, if unknown)
• Signature of person taking sample
• O – (Negative) is a limited resource and
if demand exceeds supply the O – should
be restricted to females of child bearing
age. Other patients can receive O+
positive blood following consultation
with the Consultant Haematologist
Patients referred to/for X-ray will progress to Acute Admitting Ward i.e. Redwood (Surgical
Incident) or Elm Ward (Medical Incident) and not return to Emergency Dept. unless serious
deterioration. The decision on where the patient goes after x-ray will be made by the treating
Doctor in conjunction with the ED Co-ordinator
If a patient is transferred directly from x-ray to the ward the Doctor in ED needs to call the Acute
Admitting Doctor on the ward for verbal handover.

50
Location Reporting
• Report on number & status of patients in your area to the Control Team regularly @ ext
5178
• Identify potential risks & obstacles to Control Team early @ ext 5178
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the works of the Department are
complete.
• Ensure that there is sufficient staff to handle the expected workload and Stand Down the
remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

51
Director of Nursing Office
Senior Nursing Manager
Director of Nursing, Ass. Director of Nursing, Night Superintendent or CNMIII – Site
Nurse Manager
Internal Contact No: 5121/5123 or relevant bleep
Department Function/role:
• To ensure nursing care is provided to all patients
• Facilitate the reception of a large number of undifferentiated patients
• Until arrival of Bed Manager, carry out their duties (out of hours)
Activation Procedure
The Hospital’s plan can then be activated by,
� Based on the information received (from Ambulance Control and the Emergency Dept.) the
Director of Nursing may decide in conjunction with other members of the Control Teams to
activate plan, in this case both the Emergency Dept. and the Switchboard must be
informed immediately.
Department Activation Procedure
Outside normal working hours when plan is activated it is your responsibility to contact
immediately a second Senior Nurse Manager/Staff Nurse.
Staff Reporting Location
Second Senior Nurse Manager reports directly to the Director of Nursing’s office.
Action Card
Following decision to activate the Major Emergency Plan the senior Nursing Manager will:
After 5 p.m. /Out of Hours
• Call in 2nd
A/Director of Nursing immediately for assistance
• One Snr. Nurse Manager will remain as operational Manager and one joins the Control
Team
• Inform ICU, CCU, Surgical Day Ward, Redwood, Laurel, Cypress, Cherry, Elm, Maple and
Oak that the Major Emergency Plan has being activated
• Inform outlining wards of plan’s activation i.e. Woodlands, Sycamore & Silver Birch
• Contact CNM of OPD
• Contact CNM Surgical Day Ward if required
• Collect rosters and contact information
• Identify bed availability if there is no Bed Manager on duty
• Inform Clinical Nurse Manager Emergency Dept. and Control Centre (ext 5179) of bed
availability

52
• In the absence of the Bed Manager communicate bed availability with wards
Office Hours
• Inform OPD, Holly Day Hospital, ICU, CCU, Surgical Day Ward, Redwood, Laurel, Cypress,
Cherry, Elm, Maple and Oak that the Major Emergency Plan has being activated. Also
inform Woodlands, Sycamore, Silver Birch and Unit 6 of plan’s activation
• Identify potential staff availability and areas where extra staff may be required
• Contact nursing staff as necessary: groups available
o Tutorial Staff
o Nurse Practice Development Staff
o Specialised Nursing Staff e.g. OPD, CPR Training Officers and Endoscope staff
• Review with Emergency Department Clinical Nurse Manager/Medical Co-ordinator
situation in Emergency Department, Theatre, ICU and CCU
• Document all proceedings
• Liaise with ED Co-ordinator as required – ext 6252/6253
• Liaise with Control Centre on regular basis throughout Emergency – ext 5890
• Liaise with Control Centre regarding Step Down
Outside of normal working hours Nursing Administration will transfer charge of the Hospital to
the Hospital Manager/Deputy when they arrive on site.
It is important to remember staff that have just come off duty, are not available for first contact and
staggering contacting staff in the event incident becoming prolonged is essential
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

53
Emergency Dept. Clinical Nurse Manager (Snr. Nurse)
Emergency Dept. Co-ordinator
Internal Contact No: 6252/6253
Department Role:
• Immediate provision of medical care to causalities of the Emergency
• Prepare for the arrival of a large number of undifferentiated patients
• Liaise with entire hospital via Control Centre to ensure that the Emergency
Department receives all necessary support
• On going communication with Ambulance Liaison Officer, who will provide
information from the scene
Activation Procedure
CNM, Emergency Department will be notified when Hospital is put on the alert by the
Switchboard (if call does not come into Emergency Department itself), when Full Alert or Plan is
activated the Switchboard will re-contact the CNM or Snr Nurse on duty.
Ward/Department Activation Procedure
When Full Alert is given the CNM or Senior Nurse on duty will contact his/her staff directly or will
instruct a junior member of nursing staff to do so on their behalf.
Action Card
• Record all details of call (if received in the Emergency Dept.)
• Source of Information
• Date Call Received
• Time Call Received
• Exact location of Incident
• Type of Incident
• Hazards e.g. Radiation
• Number of Casualties
• Estimated time of Arrival at Hospital
• Verify call by contacting Ambulance Services (01 6709111)-if call is received in ED
• Notify Telephonist and Snr Nursing Officer 5121/5123 or relevant bleep if call is received in
the Emergency Department
• Contact on call Consultant in Emergency Medicine
• Brief all staff in Emergency Department
• Vacate Emergency Department of Patients and Relative, possible options
o Admit to ward – Day Ward/Endoscopy Suite
o Advise patients in waiting room to attend their GP or attend a hospital which is not
involved in the Emergency (name will be available)
o Incorporate patients into Major Emergency
o Transfer to Minor Injuries Area (OPD)

54
• Assign Nursing Staff and issue relevant action cards
o Red Nurse - Resuscitation Room/CPOU/Obs.
o Yellow Nurse – Cubicles 1-10/POP: 1 and 2
o Green Nurse – Minors
o Blue Nurse –
� Drugs Nurse
� Blood Nurse
� Equipment Nurse
� Triage Nurse
o Florescent Yellow– Emergency Dept. Co-ordinator (Clinical Nurse in charge)
• Nursing staff to Red area until support staff arrive
• Triage Point – Assign Snr Nurse to triage point
• Triage Officer – most senior member of staff present to be designated as Triage Officer
• Emergency Staff call out – assess extra staff required and assign junior nursing staff to
make contact
• Request from Snr. Nurse Manager (Asst. D of N at ext: 5121/5123 or relevant bleep) extra
staff as required
• Ensure walk in doors are locked and blinds on windows closed
• Ambulance entrance only to be used
• Liaise with
o Triage Officer
o Senior Nursing Officer
o Medical Co-ordinator
o Hospital Manager
• Check-
o Trolleys
o Bed state
o Supplies
o Nursing Staff (additional requirements)
o Unauthorised personnel
• Ensure a record is kept of all equipment/supplies lent/borrowed from other wards
• Document all decisions made during the Emergency (nominate a scribe), including staff
involved in the incident. Send copy to Control Centre when stand down is called
• Assign Doctor/Nurse pairs to receive patients (refer to individual action cards)
• On instruction from Control Centre stand down all staff
It is important to remember staff that have just come off duty, are not available for first contact and
staggering contacting staff in the event incident becoming prolonged is essential
Location Reporting
• Report on number & status of patients in your area to the Control Team regularly @ ext
5179
• Identify potential risks & obstacles to Control Team early @ ext 5179
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.

55
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there is sufficient staff to handle the expected workload and Stand Down the
remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

56
Bed Management Department & Patient Flow Team
Ext. 6269 in ED / Ext. 6365 in SDW / Ext. 5216 & 5217 in Patient Flow Office &
Ext: 5288 in Waiting List Coordinator’s Office
Bleep: 110
Department Role / Function:
o Arrange for the immediate transfer of admitted patients in Emergency Department to
appropriate beds to clear the ED
o Organize transfers from specialized units i.e. ICU, CCU, Cypress and Acute Admitting Wards
(Redwood & Elm Wards) to ensure adequate number of acute beds vacant
o Arrange transfers of non acute patients occupying acute beds to Non Acute Units
o Monitor total number of discharges & transfers from acute beds through liaison with
Consultant Surgeon and Physician on call
o Cancel all scheduled In Patient, Day Case & OPD appointments still pending for the day and
the following days as indicated by Control Team
o Keep Emergency Department and Control Centre informed of patient flow, number &
location of available beds
Activation Procedure
If / when a decision is made to activate the MEP or the Major Alert Status is upgraded to Full Alert
the Head of Bed Management Department will be contacted by Switchboard.
Department Activation Procedure
Outside of normal working hours, the Head of Bed Management Department will call in his / her
staff directly. When contact is made with first staff member they may be instructed to contact
remaining staff
Staff Reporting Location
All staff from the Bed Management Department & Patient Flow will report directly to the following
locations:
• All Patient Flow Team to Patient Flow Office initially to obtain Operational folder, bleep &
documentation required
• 1st
Patient Flow Team Member with bleep 110 to Emergency Department at ext. 6269
• 2nd
Patient Flow Team Member to the Surgical Day Ward, CNM II Office – ext. 6365
• 3rd
Patient Flow Team member, Discharge, Fair Deal & Patient Flow Coordinators to
Patient Flow Office – ext 5216 & 5217 as their base in their role as Discharge Coordinating
Team
• Waiting List Coordinator, Waiting List Officers (In Patient & Out Patient) & Hospital
Statistician to the Waiting List Coordinator’s Office – ext 5288
57
Action Card
Patient Flow Team
Consisting of One or Two Patient Flow Team Members as available
1st
Patient Flow Team Member:
Located in Emergency Department: ext. 6269
o Inform Snr. Nursing Officer (Ext. 5123 / 5121) and Hospital Manager, Control Centre via
ext: 5552 on arrival
o Call in staff as required and proceed to the Emergency Department with bleep 110 o It is important to remember staff that have just come off duty, are not available for first contact
and staggering contacting staff in the event incident becoming prolonged is essential
o Coordinate Patient Flow and locate at ext 6269 in the ED. Confirm current bed status with
Control Centre: ext. 5555 / 5890 / 5891
o Transfer admitted patients in the ED immediately to acute beds & clear the department
o Confirm bed status of Specialized Units, (ICU, CCU and Cypress) including number of
patients on ventilators and patients suitable for transfer from Cypress and inform 2nd
Patient Flow Team Member of totals
o Inform Control Centre ext. 5178/5179/5102 and ED Coordinator ext. 6252 / 6253 on
ongoing basis of bed status and availability
o Receive updates from 2nd
Patient Flow Team Member & Discharge Coordinating Team on
bed status and allocate new admissions to Acute Admitting Wards
o Ensure a constant and timely patient flow from the Emergency Department
o Communicate scheduled appointment cancellation timeframes to Waiting List Coordinator
as received from Control Team
o Ensure complete and accurate recording of patient flow to and from the Emergency
Department
o Remain at location in Emergency Department
2nd
Patient Flow Team Member:
Located at CNM Office, Surgical Day Ward: ext. 6365
- Confirm bed status with Major Acute Admitting Wards, (Redwood ext. 6301 & Elm ext.
6401), SDW, Endoscopy Day Unit & all other Acute Wards and communicate to 1st
Patient
Flow Team Member
- Receive information of Specialized Units from 1st
Patient Flow Team Member
- Organize transfers of non ventilated patients & non telemetry patients from specialized
units: ICU, CCU & Cypress Ward
- Initiate transfers from the Acute Admitting Wards (Redwood & Elm) to the Surgical Day
Ward and other available acute beds after consultation with the Consultant Surgeon and
Physician on duty. Ensure as many as possible vacant beds on all Acute Admitting Wards
- Keep 1st
Patient Flow Team member in Emergency Department up to date with available
beds in Acute Admitting Wards and Specialized Units
- Ensure four to six available beds on Elm Ward to be used for Non Invasive Ventilation (Bi
PAP & CPAP) if required
58
- Liaise with Discharge Coordinating Team as to patient numbers that can transfer from
acute in patient beds to Day Wards & Non Acute Units
- Ensure complete & accurate recording of all inter departmental transfers
- Remain at location in Surgical Day Ward
Discharge Coordinating Team:
Located in Patient Flow Office: ext. 5216
- Liaise with the Consultant Surgeon & Physician on call as to the amount, patient names,
location & clinical acuity of patients who
□ can be discharge home immediately,
□ can be transferred to Non Acute Units
- Confirm patients for immediate discharge with CNM’s on acute wards
- Confirm current bed status with CNM of Non Acute Units: Silver birch, Beech & Woodlands
and enquire about additional surge capacity available within units
- Communicate information immediately to 1st
Patient Flow Team Member in Emergency
Department
- Assist all patients discharged of acute wards as required with vacation of beds, contacting
of relatives & arranging of transport
- Initiate immediate transfer of non acute patients (stable medically discharged, listed LTC
patients) to Non Acute Units
- Ensure complete & accurate recording of all discharges & transfers to Non Acute Units
- Keep 1st
Patient Flow Team Member in Emergency Department informed
- Liaise with 2nd
Patient Flow Team Member as required
- Remain at location in Patient Flow Office
Waiting List Coordinator, In-Patient waiting List Officers, OCRO Staff & Hospital Statistician:
Located in Waiting List Coordinator’s Office: ext. 5288 initially for a briefing, then continuing to
own desk & extension
- Cancel all unresolved, elective in-patients, day cases & scheduled Out Patient Services
immediately for the day. Inform patients that a new appointment will be posted out to
them in due time
- Print PAS Reports of all scheduled patient appointments as elective in-patients, day cases &
scheduled Out Patient Services for the following day and cancel their appointments. Inform
patients that a new appointment will be posted out to them in due time.
- Following on advise form the Control Team, print PAS Reports of all above mentioned
category of patients for the next few days and cancel as appropriate or requested by
Control Team
- Keep clear records of all patients cancelled
Remain within Bed Management Department & offer clerical support to Patient Flow
Team & Discharge Coordinating Team
Location Reporting
• Report on number & status of patients in your area to the Control Team regularly @ ext
5179
• Identify potential risks & obstacles to Control Team early @ ext 5179

59
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

60
Clinical Nurse Manager – OPD
Out Patient Department – Minor Injuries – Green Area
Ext: Suite A-5834/5836: Suite C-5833/5837 Suite D-5849
Department Role/Function
• Evacuate Out Patients Department if in use
• Accept minor injuries from Emergency Department
• Re-assesses patients as required
Activation Procedure
If/when a decision is made to activate the MEP or the Major Alert Status is upgraded to Full Alert
the Clinical Nurse Manager or Snr. Nurse will be contacted by Director of Nursing’s Office or Night
Superintendent.
Ward/Department Activation Procedure
Outside normal working hours the Clinical Nurse Manager will call in staff.
Staff Reporting Location
Staff will report directly to their own department, unless otherwise informed on contact.
Action Card
• CNM/Nurse in charge informs Nursing Administration (ext: 5121/5123 or relevant bleep) of
your arrival (if out of hours)
• Call in extra staff including Health Care Assistant/Portering staff as required
• It is important to remember staff who have just come off duty, are not available for first contact
and staggering contacting staff in the event incident becoming prolonged is essential
• If OPD is in use in conjunction with Administrative supervisor
o Vacate all patients in Department waiting for transport to main Concourse Area
• Options available to patients are: (as stated in pre-designed letter)
o Ring the following working day and make a new appointment
o If necessary go to G.P.
• Remove all charts and x-rays to chart room and lock same
• Lock main OPD doors (to prevent entrance). Access via Suite D, one way system in
operation
• Prepare consulting rooms for reception of minor injuries
• Accept minor injuries as they arrive
• Review patients x-rays on return from x-ray – on NIMIS system
• As Doctor discharges patients they are referred to Discharge Team in Waiting Area, Suite D
• Instruction sheets for minor injury patients are distributed to patients on discharge from
Green Area and return appointments for patients involved in MEP are given on discharge
or contact will be made the next day when dates of review clinics are available
• All Advance Nurse Practitioners (ANP) can treat and discharge patients independently
• Liaise with the Consultant at all times

61
• Ensure patient details are recorded on the Symphony system under Major Emergency:
Code – Major Incident Primary/Secondary/Trauma
Location Reporting
• Report on number & status of patients in your area to the Control Team regularly @ ext
5179
• Identify potential risks & obstacles to Control Team early @ ext 5179
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

62
Green Area Discharge Team
Location: Out Patients Department, Suite D – Ext:5849
Role: Review all patients being discharged from Green Area
Members of discharge team:
• Social Worker
• Administrative staff
• Nursing staff
Action Card
• Ensure all patients discharged from Green Area are comfortable and safe
• Ensure wounds are cleaned and dressed
• Ensure splints/crutches are provided if required
• Tetanus status of patients is confirmed
• Analgesics/antibiotics are provided if required
• Advice Sheets are provided as appropriate
• Transport/collection by family are arranged, via Social Worker assigned to discharge team
• Contact details of all patients being discharged are correct
• All patients need to return for review in Special Review Clinics – Control Team will decide
on location for Review Clinics- within 3 days/72 hours
• Document discharge details of each patients
• If it is not possible to make appointments at this time all patients will be contacted the
next day
• Ensure complete list of discharged patients and contact details are compiled and given to
the Emergency Department Co-ordinator and the Control Team
Location Reporting
• Report on number & status of patients in your area to the Control Team regularly @ ext
5179
• Identify potential risks & obstacles to Control Team early @ ext 5179
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

63
Clinical Nurse Manager –Redwood Ward
Acute Admitting Ward – Surgical Incident - Ext: 6301
Department Role/Function
• Identify potential patients for discharge
• Arrange transfer of remaining patients to adjacent wards
• Prepare to receive patients from Emergency Department
Activation Procedure
If/when a decision is made to activate the MEP the Clinical Nurse Manager or Snr. Nurse on duty
will be contacted by Director of Nursing’s Office or Night Superintendent.
Ward/Department Activation Procedure
• Request any staff about to go off duty to remain on duty
• Contact will be made with off duty staff by either Junior Member of Staff or Ward Clerk (if
in attendance)
• Contact details for all staff should be kept up to date at all times
Staff Reporting Location
All staff should report directly to their own wards. A sign in book recording all staff present during
a Major Emergency should be kept.
Action Card
• Call in the Ward Clerk if necessary
• Instruct Ward Clerk or junior member of staff to call in extra staff as required
• It is important to remember staff that have just come off duty, are not available for first contact
and staggering contacting staff in the event incident becoming prolonged is essential
• Ask all visitors on the ward to leave the premises as the MEP has being activated
• In conjunction with Medical teams identify potential discharge patients and delegate a
nurse to transfer patients to Patients TV lounge
• Vacate beds of ambulant patients - to Patients TV lounge
• Relocate remaining patients to adjacent wards ensuring adequate records are maintained
of all transfers in and out of ward
• Nominate staff member to co-ordinate transfers:
o Discharge home
o Within hospital campus
o To Surgical Day Ward
• Liaise with Bed Management regarding bed availability
• Prepare to receive incident patients
• Accept transfers from ICU

64
Location Reporting
• Report on number & status of patients in your area to the Control Team regularly @ ext
5179
• Identify potential risks & obstacles to Control Team early @ ext 5179
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

65
Clinical Nurse Manager –Elm Ward
Acute Admitting Ward – Medical Incident - Ext: 6401
Department Role/Function
• Identify potential patients for discharge
• Arrange transfer of remaining patients to adjacent wards
• Prepare to receive patients from Emergency Department
Activation Procedure
If/when a decision is made to activate the MEP the Clinical Nurse Manager or Snr. Nurse on duty
will be contacted by Director of Nursing’s Office or Night Superintendent.
Ward/Department Activation Procedure
• Request any staff about to go off duty to remain on duty
• Contact will be made with off duty staff by either Junior Member of Staff or Ward Clerk (if
in attendance)
• Contact details for all staff should be kept up to date at all times
Staff Reporting Location
All staff should report directly to their own wards. A sign in book recording all staff present during
a Major Emergency should be kept.
Action Card
• Call in the Ward Clerk if necessary
• Instruct Ward Clerk or junior member of staff to call in extra staff as required
• It is important to remember staff that have just come off duty, are not available for first contact
and staggering contacting staff in the event incident becoming prolonged is essential
• Ask all visitors on the ward to leave the premises as the MEP has being activated
• In conjunction with Medical teams identify potential discharge patients and delegate a
nurse to transfer patients to Patients TV lounge
• Vacate beds of ambulant patients - to Patients TV lounge
• Relocate remaining patients to adjacent wards ensuring adequate records are maintained
of all transfers in and out of ward
• Nominate staff member to co-ordinate transfers:
o Discharge home
o Within hospital campus
o To Surgical Day Ward
• Liaise with Bed Management regarding bed availability
• Prepare to receive incident patients
• Accept transfers from ICU

66
Location Reporting
• Report on number & status of patients in your area to the Control Team regularly @ ext
5179
• Identify potential risks & obstacles to Control Team early @ ext 5179
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

67
Theatre Clinical Nurse Manager
Or Deputy on Duty
Ext: 6315/6329
Department Role/Function
• Finish surgery in progress
• Do not commence any new surgery until Stand Down is given
• Inform Control Centre of Theatre and staff availability
• Assess status of recovery room
Activation Procedure
Theatre Clinical Nurse Manager/Snr. Nurse Manager on duty will be notified when the hospital is
put on alert by the Switchboard, when Full Alert is given the Switchboard will re-contact the
Theatre Clinical Nurse Manager/Snr. Nurse Manager on duty.
Department Activation Procedure
Outside of normal working hours when Full Alert is given the Snr. Nurse Manager on duty contacts
Clinical Nurse Manager who in turn will contact his/her staff directly or will instruct the Snr. Nurse
Manager on duty to do so on their behalf.
Staff Reporting Location
All staff will report directly to Theatre. (On Major Disaster Board, there is a template for allocation
of staff etc.)
Action Card
• Contact Clinical Nurse Manager (if not on duty)
• On site Snr. Nurse calls in staff as required, including Ward Clerk
• It is important to remember staff that have just come off duty, are not available for first contact
and staggering contacting staff in the event incident becoming prolonged is essential
• Inform Surgeons who are in Theatre
• Assess the situation in the Recovery Room and make provision for the transfer of patients
from same if necessary
• Deploy staff as they become available
o 3 Staff Nurses and one attendant to each Theatre
o 2 Staff Nurses to Anaesthetic and 2 Staff Nurses to Recovery Areas
o Third recovery Staff Nurse to remain on standby
• Liaise with Anaesthetist and Surgeon regarding co-ordination of operation scheduling
• Liaise with the Anaesthetist and Bed Manager regarding transfer of patients from Recovery
Room

68
• Release department porter for reassignment to hospital pool if/when they are no longer
required
• Co-ordinate with the Radiography Service Manager the need for assignment of
Radiographer to Theatre i.e. depending on the nature of Emergency
• Ensure that a system for the care of patient’s property and for the preservation of
specimens or foreign bodies is in place
• Keep Control Centre informed of Theatre availability
• Assign Scrub Nurse to setting up trolleys
• Stock, drugs, IV fluids and blood availability to be checked when appropriate staff arrive on
duty
• Liaise with Control Centre regarding stand down arrangements
Location Reporting
• Report on number & status of patients in your area to the Control Team regularly @ ext
5179
• Identify potential risks & obstacles to Control Team early @ ext 5179
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

69
ICU
(Clinical Nurse Manager/Nurse in Charge)
Contact No: 6384/6380/6381
Activation Procedure
If/when a decision is made to activate the MEP or the Major Alert Status is upgraded to Full Alert
the ICU CNM/Nurse in charge will be contacted by Nursing Administration.
Action Card
• In consultation with the Consultant Anaesthetist review ICU patients for suitability for
discharge to surgical/medical wards
• Inform Bed Manager/Snr Nursing Officer of patients to be moved and therefore bed
availability
• Co-ordinate and allocate staff for admission and transfer of patients
• Call in extra staff as required
• It is important to remember staff that have just come off duty, are not available for first contact
and staggering contacting staff in the event incident becoming prolonged is essential
• Deploy staff as they arrive:
o Two Staff Nurses per patient
o One Staff Nurse to set up necessary equipment
• Ensure there are sufficient staff to handle the expected workload and arrange stand down
with Control Centre
Location Reporting
• Report on number & status of patients in your area to the Control Team regularly @ ext
5179
• Identify potential risks & obstacles to Control Team early @ ext 5179
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

70
CCU
(Clinical Nurse Manager/Nurse in Charge)
Contact No: 6200/6201/6204
Activation Procedure
If/when a decision is made to activate the MEP or the Major Alert Status is upgraded to Full Alert
the CCU CNM/Nurse in charge will be contacted by Nursing Administration.
Action Card
• In consultation with the Consultant Cardiologist/Cardiac Registrar review CCU patients for
suitability for discharge to medical ward i.e. Cypress
• Inform Bed Manager/Snr Nursing Officer of patients to be moved and therefore bed
availability
• Co-ordinate and allocate staff for admission and transfer of patients
• Call in extra staff as required
• It is important to remember staff that have just come off duty, are not available for first contact
and staggering contacting staff in the event incident becoming prolonged is essential
• Deploy staff as they arrive
• Ensure there are sufficient staff to handle the expected workload and arrange stand down
with Control Centre
Location Reporting
• Report on number & status of patients in your area to the Control Team regularly @ ext
5179
• Identify potential risks & obstacles to Control Team early @ ext 5179
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

71
Clinical Nurse Specialist in Infection Control
Location: Temporary Mortuary- Physio Treatment Room
Internal Contact No: Bleep 191
During MEP Activation ext: 5256
Activation Procedure
If/when a decision is made to activate the MEP or the Major Alert Status is upgraded to Full Alert
the Clinical Specialist in Infection Control will be contacted by the Switchboard.
Action Card
• Liaise with Consultant Histopathologist on call regarding staffing needs
• Contact Nursing Administration regarding calling in additional Specialist Nurses if required
• Liaise with Consultant Histopathologist regarding calling in Mortuary staff
• Prepare temporary mortuary (Physio Treatment Room)
• Place bodies including all effects in body bags
• Co-ordinate in conjunction with Garda assigned to mortuary visitors/relative for
identification purposes or otherwise
• Liaise with Consultant Histopathologist, Social Worker, Coroner, Gardai representative and
administrative support staff assigned to mortuary
• Establish a register of patient information
• Liaise with the Control Centre regarding step down arrangements
NB: Remains of casualties pronounced dead on arrival would be placed in Physio-treatment
room. These remains should be placed in a body bag as soon as possible after arrival. No
attempt should be made to remove effects or to clean the remains, as this could be vital
evidence in establishing the cause of death and in making a formal identification. The
identification of these casualties is the responsibility of the Dublin City Coroner and the
Gardai. It is the responsibility of the Coroner to arrange the post mortems of these
casualties.
Location Reporting
• Report on number & status of patients in your area to the Control Team regularly @ ext
5179
• Identify potential risks & obstacles to Control Team early @ ext 5179
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.

72
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

73
CSSD Manager
Contact No: 5212/5209
Department Role/Function
o To provide decontamination and sterile services to facilitate the efficient treatment of
casualties in theatre and clinical areas.
Activation Procedure
If/when a decision is made to activate the MEP or the Major Alert Status is upgraded to Full Alert
the CSSD Manager will be contacted by Switchboard.
Action Card
• Inform Control Centre via Administrative Co-ordinator ext: 5324 of your arrival (if out of
hours)
• Assess the likely workload in consultation with Theatre
• Call in staff as required
• It is important to remember staff that have just come off duty, are not available for first contact
and staggering contacting staff in the event incident becoming prolonged is essential
• Liaise with Theatre Manager to assess the availability of sterile equipment
• Liaise with Emergency Department Co-ordinator –ext 6252/6253 re extra requirements for
ED
• Allocate staff and prioritise sets
• Liaise with Control Centre regarding step down arrangements
Location Reporting
• Report on number & status of patients in your area to the Control Team regularly @ ext
5179
• Identify potential risks & obstacles to Control Team early @ ext 5179
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

74
Clinical Nurse Manager or Senior Nurse on duty
Wards – Cherry (Ext: 6271), Cypress (Ext: 6213), Laurel (Ext: 6340) and Maple (Ext:
6239)
Department Role/Function
• Identify potential patients for discharge
• Prepare to receive patients from Acute Admitting Ward: Redwood Ward – Surgical incident
or Elm – Medical incident
Activation Procedure
If/when a decision is made to activate the MEP or the Major Alert Status is upgraded to Full Alert
the Clinical Nurse Manager or Snr. Nurse on duty will be contacted by Director of Nursing’s Office
or Night Superintendent.
Ward/Department Activation Procedure
• Request any staff about to go off duty to remain on duty
• Contact will be made with off duty staff by either Junior Member of Staff or Ward Clerk (if
in attendance)
• Contact details for all staff should be kept up to date at all times
Staff Reporting Location
All staff should report directly to their own wards. A sign in book recording all staff present during
a Major Emergency should be kept.
Action Card
• Call in the Ward Clerk if necessary
• Instruct Ward Clerk or junior member of staff to call in extra staff as required
• It is important to remember staff that have just come off duty, are not available for first contact
and staggering contacting staff in the event incident becoming prolonged is essential
• Vacate beds of ambulant patients - to Patients TV lounge
• Ask all visitors on the ward to leave the premises as the MEP has being activated
• In conjunction with Medical teams identify potential discharge patients and delegate a
nurse to transfer patients to the Patients TV lounge
• Relocate remaining patients to one/or more room
• Liaise with Bed Management regarding bed availability
• Prepare to receive patients from Acute Admitting Ward i.e. Redwood Ward or Elm Ward
• Nominate staff member to co-ordinate transfers:
o Discharge home
o Within hospital campus
o To Surgical Day Ward
• Ensure adequate records are maintained of all transfers in and out of ward

75
Location Reporting
• Report on number & status of patients in your area to the Control Team regularly @ ext
5179
• Identify potential risks & obstacles to Control Team early @ ext 5179
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

76
Clinical Nurse Manager or Snr. Nurse on duty
Surgical Day Ward
Ext: 6363/6366
Department Role/Function
• Vacate Day Beds
• Prepare to accept pre-discharged patient
Activation Procedure
If/when a decision is made to activate the MEP or the Major Alert Status is upgraded to Full Alert
the Clinical Nurse Manager or Snr. Nurse will be contacted by Director of Nursing’s Office or Night
Superintendent.
Ward/Department Activation Procedure
Outside of normal working hours, Nursing Administration will contact Surgical Day Ward staff.
Staff Reporting Location
All staff from Surgical Day Ward will report directly to their department unless told otherwise
when contact is made.
Action Card
• Call in extra staff as required
• It is important to remember staff that have just come off duty, are not available for first contact
and staggering contacting staff in the event incident becoming prolonged is essential
• Vacate day beds
• Finish procedures in progress. Do not commence any new procedures until Stand Down is
given
• Explain to all patients awaiting procedures that MEP has being activated and take contact
details for new appointments following step down
• Prepare Ward for accepting pre-discharge patients
• Contact pharmacy, stores and CSSD for extra supplies if required
• Keep Bed Manager informed of bed situation
Location Reporting
• Report on number & status of patients in your area to the Control Team regularly @ ext
5179
• Identify potential risks & obstacles to Control Team early @ ext 5179
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.

77
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

78
Clinical Nurse Manager or Senior Nurse on duty
Beech (Ext: 5540) and Rowan (Ext: 5551)
Department Role/Function
• Vacate beds
• Prepare to accept patients transferred
Activation Procedure
If/when a decision is made to activate the MEP or the Major Alert Status is upgraded to Full Alert
the Clinical Nurse Manager or Snr. Nurse will be contacted by Director of Nursing’s Office or Night
Superintendent.
Ward/Department Activation Procedure
Outside of normal working hours, Clinical Nurse Manager or Snr. Nurse on Duty will call in his or
her own staff.
Staff Reporting Location
All staff will report directly to their own ward/department
Action Card
• Vacate beds of ambulant patients
• Request all visitors to leave the Ward due to the MEP being activated
• Report bed situation to Bed Manager (ext. 5289 or bleep 110)/ Senior Nursing Officer
• Identify patients for discharge home and arrange same
• Ensure listing is available of patients discharged following Emergency
• Keep Bed Manager informed on bed state
• Call in extra staff as required
• It is important to remember staff that have just come off duty, are not available for first contact
and staggering contacting staff in the event incident becoming prolonged is essential
Location Reporting
• Report on number & status of patients in your area to the Control Team regularly @ ext
5179
• Identify potential risks & obstacles to Control Team early @ ext 5179
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.

79
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

80
Clinical Nurse Manager – Holly Day Hospital
Ext: 5550/5555
Department Role/Function
• Evacuate Holly Day Hospital if in use
Activation Procedure
If/when a decision is made to activate the MEP or the Major Alert Status is upgraded to Full Alert
the Clinical Nurse Manager or Snr. Nurse will be contacted by Director of Nursing’s Office (if during
working hours).
Staff Reporting Location
Staff will report directly to their own department, unless otherwise informed on contact.
Action Card
• Call in extra staff including Health Care Assistant/Portering staff as required
• It is important to remember staff who have just come off duty, are not available for first contact
and staggering contacting staff in the event incident becoming prolonged is essential
• If Holly Day Hospital is in use in conjunction with Nursing & Administration Staff
o Vacate all patients in Department waiting for transport to main Concourse Area
• Options available to patients are: (as stated in pre-designed letter)
o Ring the following day and make a new appointment
o If necessary go to G.P.
• Remove all charts and x-rays to safe location and lock if possible
• Close all doors to the Holly Day Hospital. Access via ambulance entrance only
• Liaise with Nursing Administration regarding any further duties to be assigned
Location Reporting
• Report on number & status of patients in your area to the Control Team regularly @ ext
5179
• Identify potential risks & obstacles to Control Team early @ ext 5179
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.

81
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

82
Clinical Nurse Manager or Senior Nurse on duty
Woodlands
Ext: 5560/5561
Department Role/Function
• Prepare to accept pre-discharged patients transferred
Activation Procedure
If/when a decision is made to activate the MEP or the Major Alert Status is upgraded to Full Alert
the Clinical Nurse Manager or Snr. Nurse will be contacted by Director of Nursing’s Office or Night
Superintendent.
Ward/Department Activation Procedure
Outside of normal working hours, Clinical Nurse Manager or Snr. Nurse on Duty will call in his or
her own staff.
Staff Reporting Location
All staff will report directly to their own ward/department
Action Card
• Prepare Day Room for transfer of pre-discharge patients
• Keep Bed Manager informed on bed state
• Call in extra staff as required
• It is important to remember staff that have just come off duty, are not available for first contact
and staggering contacting staff in the event incident becoming prolonged is essential
Location Reporting
• Report on number & status of patients in your area to the Control Team regularly @ ext
5179
• Identify potential risks & obstacles to Control Team early @ ext 5179
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

83
Head Medical Social Worker
(Ext. 5280/5281 – Bleep 119/220)
Department Role/Function
• Provide support and counselling to relatives
• Complete the relative’s enquiry form (which will assist with identification)
• Assist in giving accurate information to individual families
• Assist in discharge planning of patients in Minor (Green) area in conjunction with Discharge
Team
Activation Procedure
If/when a decision is made to activate the MEP or the Major Alert Status is upgraded to Full Alert
the Head Medical Social Worker will be notified by Switchboard.
Ward/Department Activation Procedure
Outside of normal working hours, Head Medical Social Worker will call in her/his staff directly.
When contact is made with the first staff member they may be instructed to contact remaining
staff.
Staff Reporting Location
All staff from Social Work Department will report directly to their own department from where
they will be assigned.
Action Card
• Inform Administrative Co-ordinator ext. 5324 of your arrival
• Call in staff as required, including clerical support (if not already called by Business
Manager)
• It is important to remember staff that have just come off duty, are not available for first contact
and staggering contacting staff in the event incident becoming prolonged is essential
• Assign Social Worker to the following areas:
o Relative’s area (Staff Restaurant) – assist relatives to complete the relative inquiry
form in conjunction with Administration staff assigned to this area
o Assign Medical Social Worker discharge teams from wards and minor injuries area,
Suite D, Out Patients Dept. (see separate action card)
o Ensure a Medical Social Worker is available to relatives of the deceased whose
remains have been transferred to the temporary mortuary – Physio Treatment
Room
o Assign a Medical Social Worker to the Communications Centre to help in dealing
with particularly distressed telephone callers
• Ensure refreshments are available for relatives
• Ensure relatives have access to phones if necessary
• In conjunction with representative from Directorates, collate names and enquiries from
relatives. Cross reference these with the Emergency Dept. admission list
• Liaise with the Control Centre regarding step down arrangements

84
• Co-ordinate a Critical Incident Stress Debriefing service with Staff Care for staff post
incident
Location Reporting
• Status report of each areas activities in relation to the functions identified should be made
to the Control Team via Admin Co-ordinator regularly @ ext 5324
• Identify potential risks & obstacles to Control Team early @ ext 5324
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

85
Social Worker
Green Area Discharge Team –Ext:5849
Location: Out Patients Department, Suite D
Role: Review all patients being discharged from Green Area
Members of discharge team:
• Social Worker
• Nurse
• Administrative staff
Action Card
• Ensure all patients discharged from Green Area are comfortable and safe
• Ensure wounds are cleaned and dressed
• Ensure splints/crutches are provided if required
• Tetanus status of patients is confirmed
• Analgesics/antibiotics are provided if required
• Advice Sheets are provided as appropriate
• Transport/collection by family are arranged, via Social Worker assigned to discharge team
• Contact details of all patients being discharged are correct
• All patients need to return for review in Special Review Clinics, Control Team will identify
location of Review Clinics - within 72 hours
• Document discharge details of each patients
• If it is not possible to make appointments at this time all patients will be contacted the
next day
• Ensure complete list of discharged patients and contact details are compiled and given to
the Emergency Department Co-ordinator and the Control Team
Location Reporting
• Status report of each areas activities in relation to the functions identified should be made
to the Control Team via Admin Co-ordinator regularly @ ext 5324
• Identify potential risks & obstacles to Control Team early @ ext 5324
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

86
Laboratory Manager
Ext. 5394
Or Medical Scientist on duty (Bleep 158 out of hours)
Department Role/Function:
• Ensure requests from the Emergency Department are dealt with as quickly and efficiently
as possible
Activation Procedure:
The Laboratory Manager (during normal working hours) or Medical Scientist on duty (if outside
normal working hours) Bleep 158 will be notified when Hospital is put on alert by the Switchboard.
When Full Alert is given the Switchboard will re-contact the Laboratory Manager.
Ward/Department Activation Procedure
Outside of normal working hours either the Laboratory Manager or his/her deputy will make
contact with staff.
Staff Reporting Location
All staff from this department will report directly to the Laboratory.
Action Card
• Call in Laboratory Manager (if not on duty)
• Inform Administrative Co-ordinator (Ext: 5324), of your arrival
• Assess staffing needs and call in staff if required
• It is important to remember staff that have just come off duty, are not available for first contact
and staggering contacting staff in the event incident becoming prolonged is essential
• Liaise with Clinical Director @ ext. 5178 on need for blood and blood products
• Release staff as the workload decreases following liaison with the Control Centre
• Liaise with Control Team regarding stand down
Minimum data set required for unconscious/unknown patient for blood transfusion purposes:
Sample and request card must include:
• Unique MEP number
• Unknown Male/Female (instead of
name, if unknown)
• Signature of person taking sample
• O – (Negative) is a limited resource and
if demand exceeds supply the O – should
be restricted to females of child bearing
age. Other patients can receive O+
positive blood following consultation
with the Consultant Haematologist
87
Location Reporting
• Status report of departments activities in relation to the functions identified should be
made to the Control Team via Admin Co-ordinator regularly @ ext 5324
• Identify potential risks & obstacles to Control Team early @ ext 5324
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

88
Radiography Services Manager
(Ext. 5297)
(or Radiographer on duty)
Department Role/Function
• Prioritise patients from Emergency with regard to radiological requirements
Activation Procedure
The Radiography Services Manager / Radiographer on duty (if outside normal working hours) will
be notified when Hospital is put on the alert by the Switchboard, when Full Alert is given the
Switchboard will re-contact the Radiography Services Manager or Radiographer on duty
Ward/Department Activation Procedure
Outside of normal working hours when Full Alert is given the Radiographer on duty contacts
Radiography Services Manager who in turn will contact his/her staff directly or will instruct
Radiographer on duty to do so on their behalf.
Staff Reporting Location
All staff will report to the Department from where they will be assigned.
Action Card
• Call in Radiography Services Manager (if not on duty)
• Liaise with Clerical Supervisor/ Business Manager on clerical assistance needed
• Contact Clerical Supervisor and ask that they call in their staff
• Inform Administrative Co-ordinator (Ext. 5324), of your arrival if out of hours
• Consult with Emergency Department re likely requirements ext. 6252/6253
• In conjunction with Clerical Supervisor cancel the remainder of scheduled work (if in
normal working hours)
• Contact radiology nurse
• Call in extra staff as required, as staff arrive deploy them appropriate
• It is important to remember staff that have just come off duty, are not available for first
contact and staggering contacting staff in the event incident becoming prolonged is
essential
• Patients for admission will progress directly to Acute Admitting Ward i.e. Redwood
(Surgical Incident) or Elm (Medical Incident)
• If Patient deteriorates clinically contact Emergency Department Co-ordinator at 6252/6253
to discuss patients return to Emergency Department
• All patients from Green Area i.e. minors (based in OPD) to be directed back to Out Patients
for completion of examination process
• Liaise with Theatre Nurse Manager ext. 6315/6329 re – need for assignment of
Radiographer to Theatre i.e. depending on nature of Emergency

89
Patients referred to/for X-ray will progress to Acute Admitting Ward i.e. Redwood (Surgical
Incident) or Elm Ward (Medical Incident) and not return to Emergency Dept. unless serious
deterioration. The decision on where the patient goes after x-ray will be made by the treating
Doctor in conjunction with the ED Co-ordinator
If a patient is transferred directly from x-ray to the ward the Doctor in ED needs to call the Acute
Admitting Doctor on the ward for verbal handover.
Location Reporting
• Status report of departments activities in relation to the functions identified should be
made to the Control Team via Admin Co-ordinator regularly @ ext 5324
• Identify potential risks & obstacles to Control Team early @ ext 5324
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

90
Physiotherapy Department
Ext: 5296/5276
(Temporary Mortuary in Physio Treatment Room)
Department Role/Function
• Vacate the treatment room and prepare same
Activation Procedure
The Physiotherapist on call (if outside normal working hours) will only be notified when Full Alert
is given, and will be notified by Switchboard.
Action Card
If plan is activated while Physiotherapy Department is in use – normal working hours:
• Vacate all patients in department and waiting area-issuing instructions to patients. Options
open to patients are:
o Ring the following day and make a new appointment
o If returned to ward a new appointment will be made on the following day
• Remove all items from treatment room and lock in a secure area
• Assist in the preparation of the treatment room
• Assign Physio to Green (Minor) Area – Out Patients Dept. to assist with any treatment
required
Location Reporting
• Status report of departments activities in relation to the functions identified should be
made to the Control Team via Admin Co-ordinator regularly @ ext 5324
• Identify potential risks & obstacles to Control Team early @ ext 5324
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

91
Allied Health Professionals
Not involved in the first stages of a Major Emergency
Role/Function
• Support Control Team in what every manner required
Activation Procedure
During normal working day: If/when the decision is made to activate the MEP the Allied Health
Professional Departments will be contacted by the Director of Allied Health Professionals
Outside normal hours: If/when the decision is made to activate the MEP each head of department will be
contacted if needed by the Administrative Co-ordinator and they in turn will contact their staff as required.
Reporting Location
Staff whose attendance is requested should report to the office of Clinical Director’s office (1st
floor,
opposite Hospital Manager’s, Admin Building) for assignment
Action Card
• Contact staff as requested
• Report to Admin. Co-ordinator for assignment – based in Clinical Director’s Office, 1st
Floor, Admin Building
• Assignment may be as Scribe, Communication Centre or where needed
• Ensure all actions taken during activation are documented, including dates, time and
signature of staff
• It should be noted that individual Allied Health Dept.’s role may come into play
following stand down, therefore each department may need to develop an action card
to cover this eventuality

92
Chief Pharmacist
(Ext:6010/6062/6013)
Department Role/Function
• Supply pharmaceutical stocks to wards as required
Activation Procedure
If Major Emergency Plan is activated the Chief Pharmacist will be notified by Switchboard. If the
Chief Pharmacist is not available the switchboard should contact another pharmacist.
Ward/Department Activation Procedure
The Chief Pharmacist will contact her/his own staff if outside normal working hours.
Staff Reporting Location
All staff will report directly to the Pharmacy Department
Action Card
• Inform Administrative Co-ordinator (Ext. 5324) of your arrival (if outside normal working
hours)
• On arrival at Pharmacy ensure availability of medication – as per departmental protocol
• Assess the situation and contact other staff if required
• Organise supply of drugs including controlled drugs upon receipt of requests by phone.
Each request should include details of the item required, the name of the
Ward/Department and the name of the person making request
• Liaise with the Control Team regarding Stand Down arrangements
Location Reporting
• Status report of departments activities in relation to the functions identified should be
made to the Control Team via Admin Co-ordinator regularly @ ext 5324
• Identify potential risks & obstacles to Control Team early @ ext 5324
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

93
Emergency Department Clerical Supervisor
(Ext: 6250)
Department Role/Function
o Ensure patient tracking system is in place
o Assist Business Manager or representative in maintaining Registration of Patient
Information
Activation Procedure
The Emergency Department Supervisor will only be notified (outside of normal working hours)
when Full Alert is given, and will be notified by his/her staff on duty.
Department Activation Procedure
Outside of normal working hours, the Supervisor will instruct staff on duty to make immediate
contact with off duty staff.
Staff Reporting Location
All Emergency Department Clerical Staff will report directly to their department.
Action Card (Snr. Clerical Staff)
o Assign an experienced clerical person to the Triage team immediately (see receptionist
triage action card)
o Call in Emergency Department Clerical Supervisor and remaining staff as required,
including secretaries of dept.
o It is important to remember staff that have just come off duty, are not available for first
contact and staggering contacting staff in the event incident becoming prolonged is
essential
o Assign an experienced clerical person to the Minor Area (OPD) to ensure details are being
entered correctly
o Assign Clerical person to Temporary Mortuary i.e. Physio treatment room
o Assign a member of the Clerical Team to act as Scribe for Emergency Dept. Co-ordinator
o Collect folders containing: MRN numbers, Name bands, Blood labels and Addressograph
labels
o Ensure registration details are completed correctly and being entered onto the Symphony,
system using the correct code (Major Incident Primary/Secondary/Trauma)
o As further details become available on patients prepare to update registration
o Assist Business Manager or representative in maintaining Central Registration of Patient
Information
o Liaise with Control Team regarding step down arrangements

94
Emergency Dept. Clerical Staff
Role: Triage Team – Clerical Support
Action Card
• Retrieve folders from Snr. Clerical Staff containing: MRN numbers, Name bands, Blood
labels and Addressograph labels
• Don appropriate Tabard
• Form team at ambulance entrance with members of Triage Team i.e. Triage doctor and
nurse
• Give chart to nurse who will attach wristband to patient and label to Cruciform card
• Record as much detail as possible e.g. name, sex, obvious injury onto data sheet
• When details are accumulated on 5 patients pass information to Clerical staff at computer
station to enter details onto the system
• Start collating information on the next 5 patients
• As further staff arrive, assistance will be given
• Stay with the Triage team until all patients have being triaged
Location Reporting
• Status report of departments activities in relation to the functions identified should be
made to the Control Team via Admin Co-ordinator regularly @ ext 5324
• Identify potential risks & obstacles to Control Team early @ ext 5324
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

95
Senior Administrative Staff - OPD
Out Patients Dept. – Minor Injuries – Green Area
Ext: 5823/5824/5825
Department Role/Function
• Evacuate Out Patients Department if in use
• Accept minor injuries from the Major Emergency
Activation Procedure
If/when a decision is made to activate the MEP the Administrative Staff will be contacted by one
of the Business Managers or designate.
Department Activation Procedure
Outside normal working hours a Dept. Supervisor will call in the remainder of the department
staff.
Staff Reporting Location
Staff will report directly to their own department, unless otherwise informed on contact.
Action Card
• If out of hour- inform Business Manager -mobile number will be distributed or @ ext: 5074
of your arrival
• If OPD is in use in conjunction with Clinical Nurse Manager
o Vacate all patients in Department awaiting transport to main Concourse Area
o Ensure listing is kept of attending patients
• Options available to patients are: (as stated in pre-designed letter)
o Ring the following day and make another appointment
o If necessary go to G.P.
• Assist CNM in
o Removing all charts to chart storage room and lock same
o Lock main OPD doors (to prevent entrance)
• Call in extra staff as required
• Document and identify all patients for registration from ME in your area
• Ensure patient details are recorded on the Symphony system under Major Incident
Primary/Secondary/Trauma Code
• Assign a member of staff to the discharge team based in Suite D (see separate action card)
• Assign senior experienced staff to temporary mortuary (physio treatment room) until
requested otherwise
• Liaise with Control Team regarding Stand Down
Location Reporting
• Status report of departments activities in relation to the functions identified should be
made to the Control Team via Admin Co-ordinator regularly @ ext 5324
• Identify potential risks & obstacles to Control Team early @ ext 5324

96
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

97
Green Area Discharge Team
Location: Out Patients Department, Suite D @ ext. 5849
Role: Review all patients being discharged from Green Area
Members of discharge team:
• Social Worker
• Nurse
• Administrative staff
Action Card
• Ensure all patients discharged from Green Area are comfortable and safe
• Ensure wounds are cleaned and dressed
• Ensure splints/crutches are provided if required
• Tetanus status of patients is confirmed
• Analgesics/antibiotics are provided if required
• Advice Sheets are provided as appropriate
• Transport/collection by family are arranged, via Social Worker assigned to discharge team
• Contact details of all patients being discharged are correct
• All patients need to return for review in Special Review Clinics, location to be decided by
Control Team, within 72 hours
• Document discharge details of each patients
• If it is not possible to make appointments at this time all patients will be contacted the
next day
• Ensure complete list of discharged patients and contact details are compiled and given to
the Emergency Department Nurse Co-ordinator and the Control Team
Location Reporting
• Status report of departments activities in relation to the functions identified should be
made to the Control Team via Admin Co-ordinator regularly @ ext 5324
• Identify potential risks & obstacles to Control Team early @ ext 5324
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

98
Business Managers
(Ext. 5074/5640)
Department Role/Function
o To co-ordinate and ensure clerical support is available to all relevant wards/department as
required
Activation Procedure
The Business Managers will be notified when the Hospital is put on Alert, by the Switchboard, if
MEP is activated or due to the upgrading of Major Alert the Business Managers will be re-
contacted by Switchboard.
Action Card
o Inform Administrative Co-ordinator (Ext: 5324), of your arrival
o Call in Snr. Administrative Staff if required, i.e. Health Care Records Manager and/or
Cardiac Services Co-ordinator
o Contact supervisor’s in X-ray and OPD (if not already contacted)
o Assign role of OPD Supervisor if necessary
o Contact Ward Clerk, Supervisors
o Prepare sign in sheets for staff
o Assess clerical staffing levels needed at:
o Emergency Department
o X-ray
o Laboratory
o Medical Records
o Ward Clerks
o Relative Centre (Staff Restaurant in Administration Block)
o OPD-Minor Injuries Area (Green Area)
o Physio Treatment Room (temporary mortuary)
o Call in extra staff if required
o Collate names and enquiries received from Relatives Centre and Communication Centre.
Cross reference these with the Emergency Department admission list
o Ensure coding cards are completed correctly
o Establish a Central Register of Patient Information (this can be accessed from Symphony
system)
o Advise Senior Managers on telephone help line of location of patients
o Liaise Control Team regarding Stand Down
Location Reporting
• Status report of departments activities in relation to the functions identified should be
made to the Control Team via Admin Co-ordinator regularly @ ext 5324
• Identify potential risks & obstacles to Control Team early @ ext 5324

99
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

100
Administrative Co-ordinator
Snr. Administrative Manager i.e. Human Resource Manager, Director of Allied
Health Professionals
Location during activation: Clinical Director’s Office, Admin Building– Ext: 5324
Role/Function
• Support Hospital Manager and other members of the Control Team as required
• Collation and distribution of information
• Ensure catering and supplies are mobilised
• Ensure manning of Relatives Area, Media Centre and Communication Centre
Activation Procedure
All Snr. Administrative Managers will be contacted by the Switchboard if Major Emergency Plan is
activated requesting them to attend the hospital.
Staff Reporting Location
All Senior Staff should report directly to Hospital Manager’s office for assignment. First Senior Staff
member on site, takes the role of Admin Co-ordinator
Action Card
• Inform Hospital Manager of your arrival – ext. 5102
• First Senior Staff to arrive takes the role of Administrative Co-ordinator
• Ensure adequate senior staff are attending, including ICT Co-ordinator and Environmental
Manager if required
• Call in any extra senior staff who are required
• Record names, time etc. of each department manager as they arrive and make contact
• Assign first 3 senior staff to act as Scribes to the Control Team
• Confirm with Business Managers (ext. 5074) that each key area is adequately staffed e.g.
E.D., OPD (minor injuries area), Radiology etc.
• Assign senior staff to the Communications Centre in the Risk Management Dept.
• Assign senior staff to Media Centre i.e. Nurse Education Centre
• Assign senior staff to assist Head Medical Social Worker in the Relative Area i.e. Staff
Restaurant
• Ensure catering arrangements have being put in place by contacting Catering Officer – ext
5157/5126
• Assign runners and scribes from bank of administration staff available and allied health
professional staff who are not directly effected in the first instance of a Major Emergency
i.e. Physios, O.T. s, Speech and Language Therapists etc.
• Liaise with Control Centre regarding Stand Down

101
Location Reporting
• Status report of departments activities in relation to the functions identified should be
made to the Control Team @ ext 5102
• Identify potential risks & obstacles to Control Team early @ ext 5102
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

102
Ward Clerk – Theatre
Ext: 6315
Activation Procedure
If Major Emergency Plan is activated the Theatre Ward Clerk will be contacted by Theatre, CNM or
Snr. Nurse on duty at CNM’s request Or may also be contacted by Business Manager or her/his
representative.
Reporting Location
Report directly to Theatre.
Action Card
• Contact staff as requested
• Liaise with laboratory regarding relevant reports/blood requested etc
• Man phones and take any relevant action
• Ensure there is a ready supply of labels
• Ensure all actions taken during the Emergency are documented, including dates, time
and signature of staff
• Stand down when requested by Clinical Nurse Manager or Business Manager
Location Reporting
• At any time during the plan activation an incident arises which could impede the fulfilment of these
functions (Ward Clerks) contact should be first made with CNM or Business Manager – mobile
number or at ext. 5074 if directly related to the Ward Clerk.
Stand Down
The decision to Stand Down will be made in conjunction with the CNM & Control Team.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.
103
Ward Clerk for all Wards – Cherry, Cypress, Elm, Laurel, Oak, Maple and Redwood
Role/Function of Ward Clerk
• Assist nursing staff with the call in of off duty staff
• Assist with the discharge of patients identified for discharge
Activation Procedure
If MEP is activated the Clinical Nurse Manager/ Snr. Nurse or a Business Manager will contact each
Ward Clerk.
Staff Reporting Location
Ward clerks should report directly to their own wards. When a representative from Business
Manager’s contacts ward please make it know to him/her of your attendance.
Action Card
• Contact staff nominated by CNM to attend hospital stating the Major Emergency Plan has
being activated
• Contact relatives of patients identified to be discharged home
• Contact transport – bleep 131/132 to arrange transfer of identified patients to other areas
on campus
• Co-ordinate post hospital (OPD) follow up of patients discharged due to MEP activation
• Ensure listing of discharges is available for Consultants and bed management in the
aftermath of the Emergency
• Liaise with CNM/Snr. Nurse on duty regarding patients numbers for census report
• Prepare charts for admissions
• Check stationery needs – place order if necessary
• Update patient status board
• Direct relatives of Major Emergency to Staff Restaurant, Administration Building
• Assist the CNM in making the location report
Location Reporting
At any time during the plan activation an incident arises which could impede the fulfilment of these
functions (Ward Clerks) contact should be first made with CNM or Business Manager – mobile number or at
ext. 5074 if directly related to the Ward Clerk.
Stand Down
A call will be received in the department via the phone line stating that the Hospital Manager has
instructed that we now step down from Major Emergency Activation and starts the process of returning to
normal activities. The staff member who receives this stand down ensures that the senior member of staff
in charge of the department at the time records the time of stand down and informs all staff under their
control.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

104
Information Help Line- Communication Centre
(Risk Management Dept.) Ext: 5741/5170/5089/5098
Snr. Administrative Staff
Activation Procedure
In the event of Connolly Hospitals Major Emergency Plan being put into operation all senior
admin staff will by Hospital Manager or designate.
Role/Function
• Complete the enquiry form, which will assist with identification
• Assist in giving accurate information
Action Card
• Inform Administrative Co-ordinator (ext; 5324) of your arrival
• Liaise with Business Managers – mobile number will be distributed or @ ext. 5074 and
Head Social Worker (bleep –119) regarding patient information
• Collate names and enquiries received via the phone lines
• In conjunction with representative from Directorates cross reference these details with the
Emergency Department admission list
• Return and document all calls as soon possible
• Liaise with Control Team regarding step down arrangements
Location Reporting
• Status report of departments activities in relation to the functions identified should be
made to the Control Team via Admin Co-ordinator @ ext 5324
• Identify potential risks & obstacles to Control Team via Admin Co-ordinator early @ ext
5324
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

105
Administrative Supervisor – Radiology Dept.
Ext: 5232/5235
Department Role/Function:
• Clear Radiology Dept. if in use • Cancel all elective x-rays • Accept injuries from the Major Emergency
Activation Procedure
Administrative Supervisor for the Radiology Dept. will only be notified when Full Alert is given, by
either the Business Manager for Radiology or representative or the Radiography Service Manager.
Ward/Department Activation Procedure
Outside normal working hours the Administrative Supervisor will call in or designate a staff
member to contact staff.
Staff Reporting Location
Staff will report directly to their own department, unless otherwise informed on contact.
Action Card
• If out of hours inform Business Manager – mobile number will be distributed, of your
arrival
• Call in extra staff as required
• Assign staff to main reception immediately
• If Radiology Dept. is in use in conjunction with Radiography Services Manager
o Vacate all patients
o Ensure listing is kept of attending patients
• Ensure RIS registration details are completed as accurately as possible
• Date of Birth to be used with unconscious patients: 18-08-1988
• Update patient details on RIS when correct details become available
• Liaise with the Radiography Service Manager and Consultant Radiologist regarding
managing the incident
• Update the Business Manager on regular basis regarding status of department
Location Reporting
• Status report of departments activities in relation to the functions identified should be
made to the Business Manager @ ext 5074 or on mobile
• Identify potential risks & obstacles to Business Manager early @ ext 5074 or on mobile
number
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.

106
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

107
Chaplaincy Department
(Ext: 6208/6209/Bleep - 209)
Department Role:
• Provide spiritual guidance
• Assist the Medical Social Work Department in the Relatives Area
Activation Procedure
If the Major Emergency Plan is activated the Chaplain on call will be contacted by the Hospital
Switchboard.
Action Card
• Contact as many Chaplains as required, including local clergy from all denominations
• Assign a senior member of staff to the Relative’s Centre (Staff Restaurant, Administration
Block)
• The Senior Social Worker will assign an office close to the Relative’s Centre for use by the
Chaplaincy Dept.
• Co-ordinate care of relative’s in conjunction with the Snr. Social Worker
• Assign a member of staff to the Temporary Mortuary, Physio Treatment Room
• Liaise with the Control Team regarding any area, which may require the services of the
Chaplaincy Dept.
• Co-ordinate support necessary following incident to patients, relatives and staff
• Liaise with the Control Team regarding step down
Location Reporting
• Status report of departments activities in relation to the functions identified should be
made to the Control Team via Admin Co-ordinator @ ext 5124
• Identify potential risks & obstacles to Control Team via Admin Co-ordinator early @ ext 512
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

108
Nurse Practice Development Staff & Senior Admin staff who do not have
an assigned role - Scribes
Role/Function of Scribe
• Document all actions taken by the members of the Control Team/Emergency Department
team to whom you are assigned during a Major Emergency
Activation Procedure
If Major Emergency Plan is activated a designate on behalf of Hospital Manager will contact all
Senior Administrative personnel. Nursing Administration will contact Nurse Practice
Development Staff.
Reporting Location
All senior administrative staff should report to Admin Co-ordinator in the Clinical Director’s Office,
1st
Floor, Admin Building, from where they will be assigned e.g. Scribe to a member of the Control
Team or the Communications Centre.
All Nurse Practice Development staff should report to Nursing Administration from where they will
be assigned e.g. Scribe to a member of the Emergency Dept. or the Communications centre.
Action Card
• When assignment is given ensure all actions taken by the members of the team to whom
you are assigned are documented
• Assist in whatever way possible during the Emergency
Location Reporting
• It is the responsibility of each area to which you are assigned to make a status report of
their areas activities in relation to the functions identified in this section.
• These reports should be made as required to the Hospital Manager via Admin Co-ordinator
@ ext. 5324.
• If any time during the plan activation an incident arises which could impede the fulfilment
of these functions contact should be made with the Control Team via the Admin Co-
ordinator to resolve the issue.
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

109
Department of Clinical Engineering
Ext: 5073
Department Role
• Facilitate the provision of life support equipment for designated key areas
• Assess and provide other medical device needs for designated key areas
• Co-ordinate and provide medical device needs for all wards
• Liaise with other Hospitals and/or suppliers to source medical devices as required
• Provide Clinical Engineering and Medical Physics support where required
Activation Procedure
When Major Emergency Plan is activated the Clinical Engineer will be contacted by the Hospital
Manager or designate.
Action Card
• Inform Administrative Co-ordinator (Ext: 5324) of your arrival
• Carry out any assessment of equipment as required
• Perform any duties that may be assigned to the department by the Control Team
• Liaise with the Control Centre regarding step down arrangements
Location Reporting
• Status report of departments activities in relation to the functions identified should be
made to the Control Team @ ext 5102
• Identify potential risks & obstacles to Control Team early @ ext 5102
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

110
Security Department
Ext: 5641/5294/5438 (Bleep 134)
Department Role/Function
• The Security functions are primarily concerned with providing access to certain areas,
controlling access to specified buildings and departments, maintaining order and providing
assistance to Emergency Department and Control Centre Team.
Activation Procedure
In the event of Connolly Hospitals Major Emergency Plan being put into operation the Security
Department will be put on alert to the possibility of it occurring and will be notified by
switchboard when it is implemented.
Ward/Department Activation Procedure
Outside of normal working hours when Full Alert is given the Head Security Staff on duty contacts
Security Manager who in turn will give instructions regarding contacting other staff.
Staff Reporting Location
All staff will report to Security Managers Office and will be assigned from there.
Action Card
• Inform Admin Co-ordinator of your arrival @ ext 5324
• Contact Blanchardstown Garda Station and inform them that Connolly Hospital Emergency
Plan has being activated (if Hospital Manager has not already informed same)
• Open OPD and Staff Restaurant if out of hours
• Ensure outer door to Main Hospital Entrance is supervised and prevent unauthorised
entrance
• Assist with vacating all visitors from the premises
• Assign staff to entrance of the department of Physical Medicine, i.e. Physio entrance to
prevent unauthorised access
• Assign staff to rear entrance to Emergency Dept. on Hospital Street to prevent
unauthorised access
• Liaise with the following regarding their security needs
o Director of Nursing –ext. 5179
o Hospital Manager – ext. 5102
o Emergency Department Co-ordinator –ext. 6252/6253
• Assign staff to hospital vehicular entrance (bridge) and direct visitors vehicles to main
public car park
• Open barriers at rear entrance to allow for the free movement of Emergency vehicles
• Control traffic at Emergency Department until Gardai arrives. It is expected that the Gardai
will manage traffic upon their arrival
• Assign staff to Emergency Department to prevent unauthorised entrance
• Assign staff to vicinity of Control Centre (Hospital Managers Office) to prevent
unauthorized entry
• Keep Control Centre appraised of any pertinent information and any deficiencies in the
services

111
Location Reporting
• Status report of departments activities in relation to the functions identified should be
made to the Control Team via Admin Co-ordinator @ ext 5124
• Identify potential risks & obstacles to Control Team via Admin Co-ordinator early @ ext
5124
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

112
Transport Supervisor
Ext: 5125 – Bleep 130
Department Role
• Facilitate patient transfer
Activation Procedure
If Major Emergency Plan is activated the Transport Supervisor will be contacted by the Hospital
Switchboard.
Action Card
• Inform Administrative Co-ordinator (Ext: 5324) of your arrival
• Call in extra staff as required
• Ensure Major Emergency Signs are placed correctly
• Transfer patients as requested
• Perform any duties that may be assigned to the department
• Liaise with the Control Centre regarding step down arrangements
Location Reporting
• Status report of departments activities in relation to the functions identified should be
made to the Control Team via Admin Co-ordinator @ ext 5124
• Identify potential risks & obstacles to Control Team via Admin Co-ordinator early @ ext
5124
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

113
Hospital Driver
Bleep – 132
Department Role
• Ensure correct signage is available at all times
• Co-ordinate hospital transfers
Activation Procedure
If Major Emergency Plan is activated the Hospital Driver on duty will be contacted by the Hospital
Switchboard.
Action Card
• Inform Transport Supervisor immediately (Ext: 5125/Bleep 130)
• Post Major Emergency Signs
o Emergency Department Access Route-Emergency Vehicles only (X3)
o Relatives Waiting Area (Staff Restaurant, Administration Block) (X1)
o Media Centre – Nurse Education Centre (X1)
• In conjunction with Transport Supervisor co-ordinate transfers
• Perform any other duties which may be assigned to you
Location Reporting
• Status report of departments activities in relation to the functions identified should be
made to the Control Team via Admin Co-ordinator @ ext 5124
• Identify potential risks & obstacles to Control Team via Admin Co-ordinator early @ ext
5124
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

114
Environment Manager
Ext: 5078
Department Role
• Ensure continued supply of Oxygen is available
Activation Procedure
When a decision is made to activate the MEP the Environment Manager will be contacted by
Hospital Manager or designate.
Action Card
• Inform Administrative Co-ordinator (ext: 5324) of your arrival
• Liaise with Transport Supervisor, bleep 130 regarding supply of Oxygen
• Perform any other duties which may be assigned to you
Location Reporting
• Status report of departments activities in relation to the functions identified should be
made to the Control Team via Admin Co-ordinator @ ext 5124
• Identify potential risks & obstacles to Control Team via Admin Co-ordinator early @ ext
5124
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

115
Materials Manager
Ext: 5190/5111
Department Role
• Ensure all first line departments receive any stock requests as soon as possible
Activation Procedure
If/when a decision is made to activate the MEP the Materials Manager will be contacted by the
Hospital Switchboard.
Action Card
• Inform Administrative Co-ordinator (ext: 5324) of your arrival
• Ensure stores is open
• Call in extra staff as required
• Ensure plans are in place for extra ventilators if required
• Contact Medical Gases Suppliers informing them of Major Emergency – extra supply may
be needed. Relevant telephone numbers are:
o Supplies: 4091 901/2 – Collection Dept.
o 4091800 or 1890 355 255 (Direct Line)
o 4091 800 or 1890 344 244 (after hours)
o 2694800 (pager no. for BOC Gases)
• Repairs and Services: 4501 444 (after hours)
• 4571 211 (office hours)
• Liaise with Environmental Manager on collection of cylinders from Medical Gases
• Monitor pattern of demand for supplies
o Medical Disposables
o Replace stocks promptly
• Record all stock supplied during MEP activation
• Liaise with Control Team regarding step down arrangements
Location Reporting
• Status report of departments activities in relation to the functions identified should be
made to the Control Team via Admin Co-ordinator @ ext 5124
• Identify potential risks & obstacles to Control Team via Admin Co-ordinator early @ ext
5124
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.

116
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

117
Catering Department
Ext: 5157/5126
Department Role
• Provide hot meals on a continuous basis for staff, free of charge
• Provide catering services for relatives – Staff Restaurant
• Provide catering services for all front line area
Activation Procedure
If/when a decision is made to activate the MEP the Catering Manager will be contacted by the
Hospital Switchboard.
Action Card
• Inform Administrative Co-ordinator (ext: 5324) of your arrival
• Call in extra staff as required
• Arrange to have tea/coffee and refreshments provided to:
o Relatives Area – Staff Restaurant, Administration Block
o OPD, Minor Injuries, Green Area
o Emergency Department, if requested
• Hot meals should be provided where requested/possible
• Liaise with Control Team regarding step down arrangements
Location Reporting
• Status report of departments activities in relation to the functions identified should be
made to the Control Team via Admin Co-ordinator @ ext 5124
• Identify potential risks & obstacles to Control Team via Admin Co-ordinator early @ ext
5124
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

118
Estate’s Manager
Ext: 5400
Department Role
• Ensure there is no interruption to vital services
Activation Procedure
If/when a decision is made to activate the MEP the Estate Manager will be contacted by the
Hospital Switchboard or Hospital Manager or delegate.
Action Card
• Inform Administrative Co-ordinator (ext: 5324) on your arrival
• Call in the following staff if required:
� Electrician
� Plumber
� Additional Tradesmen if required
� Works Manager or Foremen if required
• Base operations at Estates Department
• Report any problems to Control Centre
• Liaise with Control Team regarding Step Down arrangements
Location Reporting
• Status report of departments activities in relation to the functions identified should be
made to the Control Team via Admin Co-ordinator @ ext 5124
• Identify potential risks & obstacles to Control Team via Admin Co-ordinator early @ ext
5124
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.
119
Household Services Officer
Ext: 5693/5084 – Bleep 222
Department Role
� Ensure that there is an adequate cleaning and laundry service
Activation Procedure
If/when a decision is made to activate the MEP the Household Services Officer will be contacted by
the Hospital Switchboard.
Action Card � Inform Administrative Co-ordinator (ext: 5324) on arrival
� Confirm with Contract Cleaners situation update on bleep 297
� Assess staffing needs and call in staff as required
� Ensure that there is an adequate
o Cleaning Service
o Laundry Service
� Liaise with laundry if necessary
� Liaise with cleaning contractors, Derry Court Supervisor, bleep 297 if necessary
� Liaise with Control Centre regarding step down arrangements
Location Reporting
• Status report of departments activities in relation to the functions identified should be
made to the Control Team via Admin Co-ordinator @ ext 5124
• Identify potential risks & obstacles to Control Team via Admin Co-ordinator early @ ext
5124
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

120
Contract Cleaners/Derry Court
Duty Household Supervisors
Bleep 297
Department Role
� Ensure that there is an adequate cleaning and laundry service
Activation Procedure
If/when a decision is made to activate the MEP the Derry Court Supervisor on site will be
contacted by the Hospital Switchboard.
Action Card
� Inform Administrative Co-ordinator (ext: 5324) on arrival
� Assess staffing needs and call in staff as required
� Ensure that there is an adequate
o Cleaning Service
� Liaise with Household Services Officer, ext. 5693 if necessary
� Liaise with Control Team regarding step down arrangements
Location Reporting
• Status report of departments activities in relation to the functions identified should be
made to the Control Team via Admin Co-ordinator @ ext 5124
• Identify potential risks & obstacles to Control Team via Admin Co-ordinator early @ ext
5124
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

121
Contract Portering Services Manager/Shift Leader (via Contract
Supervisor) – Bleep 297 or 313/182 after hours
Role/Function:
• Assist with the movement of patients as requested
• Assist with requests to/from Laboratory
Activation Procedure
During normal working hours:
In the event of Major Emergency Plan activation the Portering Services Manager will be notified by the
Switchboard via bleep or mobile phone.
Outside normal working hours:
In the event of Major Emergency Plan activation the Portering Services Manager (contract Cleaning
Supervisor) will be notified by the Switchboard via his/her on call number.
Reporting location:
• Porter assigned to Emergency Dept. report to this department
• All other porters report to Services Manager for assignment – location Emergency Department
door in main Concourse Area
Action Card
• Call in all off duty staff
• Report activation of plan to Agency, requesting back up porters as soon as possible
• 2 porters assigned to Theatre remain in their department
• Porter assigned to Emergency Department remain in this department
• All other porters will report to Services Manager, who will be based in Emergency Department –
Reporting location Emergency Department door in Hospital Street, for assignment
• Assign porters to assist in the evacuation of Acute Admitting Ward i.e. Redwood (Surgical incident)
or Elm (Medical incident)
• Assign porter to assist in the movement of blood etc. to Laboratory
• Any other duties, which may be requested by the Control Team
• Keep a record of all request for assistance and assignment of staff
• Keep a list of all staff involved in the incident (including time of arrival and departure)
Location Reporting
• Status report of departments activities in relation to the functions identified should be
made to the Control Team via Admin Co-ordinator @ ext 5124
• Identify potential risks & obstacles to Control Team via Admin Co-ordinator early @ ext
5124
Stand Down
The decision to Stand Down will be made in conjunction with the Control Team.
Activation of Stand Down does not always indicate that the work of the Department is complete.

122
• Ensure that there are sufficient staffs to handle the expected workload and Stand Down
the remaining staff.
• It may be necessary to leave some staff on duty for a prolonged period.
• Arrange a shift cycle to ensure that members of staff are not left on duty for an excessive
period.
Please ensure all actions taken during an Emergency are documented, including dates, time and
signature of staff.

123
Appendix 1:
Internal Emergency - Surge Capacity Plan for Emergency Department
due to unexpected influx of Patients:
• Assessment of circumstances/situation is undertaken by:
o Hospital Manager/Designate (if office hours)
o Director of Nursing/Designate (if office hours)
o Night Superintendent/Site Manager (if out of hours)
o Consultant in Emergency Medicine (on duty)
o CNM in Emergency Dept. o Note: This assessment can be conducted via telephone conference if necessary
• The decision can be made to activate full MEP or a Surge Capacity Plan for ED may be needed
• If activation of MEP then contact a member of the Control Team i.e. Hospital Manager, Director
of Nursing or Clinical Director or their designates including, Night Superintendent/Site Manager
or Senior Staff in Emergency Dept. contacts Switchboard to activate plan
• If Surge Capacity Plan is required the following actions should be taken:

124
Hospital Manager
Action Card – for Surge Capacity Plan (ED)
• Contact Clinical Director regarding Medical needs in conjunction with ED Consultant-this
can be conducted via telephone conference if necessary
• If necessary liaise with Clinical Director re staffing of Pharmacy
• Call in any Senior Staff required i.e. Security Manager
• Assess if extra staff are required in Catering Dept., Household Dept. etc
• Establish links with Chief Ambulance Officer and confirm hospital situation regarding bed
availability. Also to assess as much information regarding source of surge of patients as
possible
• Notify the Regional Director Of Operations, Dublin North East, Health Service Executive of
the plan’s implementation
• Notify the Gardai in the local Blanchardstown Station if necessary
• Liaise with ED to assess staffing immediate, intermediate and long term staffing
requirements
• Reassign staff from within the Hospital until extra staffing can be sourced/called on duty
• Patients likely to require admission should be reviewed directly by the speciality team
• All on call teams should be in bleeped to ED and assist actively in patient flow
• Patients on wards suitable for discharge should be identified
• Low acuity patients suitable for transfer should be identified and moved if demand
requires to Surgical Day Ward or Endoscopy Suite – whichever is opened/staffed
• Confirm all patient transfers/discharges are in hand or are completed
• Prepare press release and deal with media enquiries if necessary
• In conjunction with other members of the Control Team decide on stand down
arrangements
• In conjunction with other members of Control Team agreed for a swift debriefing of staff
• Following stand down visit ED and other departments as involved with the other members
of the Control Team:
o Thank staff
o Get up to date information on staffing levels
o Give information on debriefing and follow up
• In conjunction with Clinical Director & Director of Nursing a decision can be made at any
stage to upgrade to full MEP activation

125
Director of Nursing
Nursing Controller - for Surge Capacity Plan (ED)
Internal Contact No 5123/5121 (during office hours), out of office hours via the Switchboard
Action Card
• If Hospital Manager is off site the Director of Nursing (based on information received
from ambulance control) may decide to activate the Hospitals Major Emergency Plan in
conjunction with Emergency Dept. and Senior Manager
• Follow action card for full activation if MEP is activated
• If decision is made to activate Surge Capacity Plan, call in Senior Nurse Manager to assist
if necessary
• If decision made to activate Surge Capacity Plan – Liaise with ED Clinical Nurse Manager to
assess staffing immediate, interim mediate and long term staffing requirements for the
department
o Liaise with the Bed Manager
o Ensure that the Bed Manager is given all information pertaining to
discharges/admissions/transfers of patients
o In conjunction with Hospital Manager & Clinical Director reassign staffing from elsewhere
in the Hospital until extra staffing can be sourced/called on duty
• Contact agency for more staff if required
• Liaise with the Hospital Manager and Medical Director to ensure the efficient management
of the ED and Hospital throughout this Surge
• Confirm all patient transfers/discharges are in hand or are completed
• In conjunction with Hospital Manager & Director of Nursing a decision can be made at any
stage to upgrade to full MEP activation
• In conjunction with other members of the Control Team decide on stand down
arrangements
• In conjunction with other members of Control Team agreed for a swift debriefing of staff
• Following stand down visit ED and other departments as involved with the other members
of the Control Team:
o Thank staff
o Get up to date information on staffing levels
o Give information on debriefing and follow up
Please ensure all actions taken during The Surge are documented, including dates, time and
signature of staff.

126
Clinical Director
If Clinical Director is not available, Consultant Physician on call will take
on this role in the event of a Surgical Incident, Consultant Surgeon on
call will take on this role in the event of a Medical Incident
Function/Role:
Supervise the Hospital’s medical response to a Major Emergency
Action Card
• Based on information received from ED and in conjunction with other members of the
Control Team decide on if activation of the MEP is required or if the Surge Capacity Plan
(ED) is required
• Follow action card for full activation if MEP is activated
• If decision is made to activate Surge Capacity Plan, call in extra ED Consultants if required
• If decision made to activate Surge Capacity Plan – Liaise with ED Consultant to assess
immediate, interim mediate and long term staffing requirements for the department
• On advice from Hospital Manager assign a NCHD (non intern) to Pharmacy as Chief
Pharmacist not available
• Contact medical/surgical teams as appropriate to identify patients suitable for discharge in
conjunction with the Bed Manager
o Ensure that the Bed Manager is given all information pertaining to
discharges/admissions/transfers of patients
o In conjunction with Hospital Manager & Director of Nursing reassign staffing from
elsewhere in the Hospital until extra staffing can be sourced/called on duty
o Arrange for NCHD’s not on call to be contacted if required (contact details with
Switchboard)
• Contact agency for more staff if required
• Monitor status in Emergency Department, ICU and Theatre
• Liaise with Consultants and Snr. Nursing Manager on potential patient discharge
• Assist liaison between ED and other hospitals regarding transfer of patients if required
• In conjunction with Anaesthetist assign medical staff to accompany patients transferring to
other hospitals
• Monitor admissions and injury severity
• Liaise with the Hospital Manager and Director of Nursing to ensure the efficient
management of the ED and Hospital throughout this Surge
• In conjunction with Hospital Manager & Director of Nursing a decision can be made at any
stage to upgrade to full MEP activation
• Confirm all patient transfers/discharges are in hand or are completed
• In conjunction with other members of the Control Team decide on stand down
arrangements
• In conjunction with other members of Control Team agreed for a swift debriefing of staff
• Following stand down visit ED and other departments as involved with the other members
of the Control Team:

127
o Thank staff
o Get up to date information on staffing levels
o Give information on debriefing and follow up
Please ensure all actions taken during The Surge are documented, including dates, time and
signature of staff.

128
Information for Staff on duty at the time of Major Emergency Plan Activation
Dealing with a major incident can be an emotional experience for hospital staff. A large spectrum of
feelings can be experienced ranging from excitement and interest to shock, concern and grief.
The information in this appendix is designed to help you understand the normal response to crises. It aims
to provide information on maintaining wellbeing having worked during a major incident.
IT MAY HELP YOU TO KNOW
o That an experience which is highly intense has the capacity to imbalance at an emotional,
psychological and physical level o That the common symptoms are a manifestation of one’s system attempting to rebalance o That understanding the symptoms can be helpful and minimise any feelings of isolation or fears
about one’s reaction. Symptoms are: o Physical: dizziness, nausea, muscle tension and pain o Psychological: feeling numb, hyper alertness o Behavioural: Poor concentration, withdrawn or over talkative
o It is important to remember it is the event that is abnormal and unusual, not you o That talking through is helpful
YOU MAY EXPERIENCE
o A sense of disbelief or “numbness” o Anxiety as the reality of what occurred becomes evident o Feelings of helplessness that you could not alter the situation o Feelings of anger o Restimulation of previous experiences of stress o Feelings of isolation and concern that your reactions are unique and therefore abnormal o Fears that if you seek “support” now or in the future you will be labelled as not coping
TAKING CARE OF YOURSELF
o Seek support from your family and friends o Attend one of the Critical Incident Stress Debriefing Sessions delivered by teams from Staff Care
(individual sessions will also be provided) o Do not increase your alcohol intake or any other substances o Ensure you eat healthily o Take regular exercise o Work on relaxation o Accept this is an abnormal incident and that subsequent stress is normal o Remember it will take time to recover o Be aware accidents are more common after severe stress o Drive more carefully and be more careful around the house and at work
OF INTEREST
The Mayday Hospital in Surrey has a staff support system in place. Following a train crash the staff received
support and gave feedback. The feedback informs us of the impact on hospital personnel who worked with
the victims of the crash. They described their initial responses as follows:

129
o Initial feelings of calm while dealing with the emergency
o Feelings of being overwhelmed by the injuries and suffering of patients but also how “good” people
where
o Feeling stressed by the enormity of the event and perhaps going home alone with no one to share
the details with
o Feelings of helplessness, inadequacy and uselessness
o Feelings of embarrassment at their reactions
o Prone to outbursts of tears a few days post the event trigged by unrelated incidents
o Difficulty switching off
o Dreams and nightmares
o Nurses reported feeling angry with the media, whereby they were aware patients had consented to
speak, they felt the there was an invasion of privacy

130
Major Emergency Notification Form
• Source of Information ___________________________
• Date Call Received ___________________________
• Time Call Received ___________________________
• Exact Location of Incident ______________________
• Type of Incident _________________________________
• Hazards (e.g. Radiation) ____________________________
• Number of Injured (Approx.) ________________________
• Estimated time of Arrival at Hospital ___________________
Action taken by Emergency Department Staff or Switchboard Staff
• Confirmed incident has taken place by returning call to Ambulance Control
• Informed Switchboard/Emergency Dept. of Incident

131
Major Emergency Plan Internal Phone Numbers: Department Location Number
Acute Admitting Ward - Redwood (Surgical Incident)
Elm (Medical Incident)
6301
6401
Administrative Co-
ordinator
Clinical Director’s Office, 1st
Floor, Admin Building
5324
Ambulance Control 6709111
Bed Manager Emergency Dept. 5288/5217/5216
Bleep 110
Business Managers Business Managers Office,
Connolly Wing
5074
Mobile number will be distributed
Catering Dept. 5157/5126
CCU 6200/6201/6204
Chaplains Bleep 209
Cherry Ward 6271
Contract Cleaners Bleep 297 or 276 (out of hours)
Control Team Hospital Managers
Office
5102- Hospital Manager
5178 – Medical Director
5179 – Director of
Nursing
CSSD CSSD 5212/5209
Cypress 6213
Elm 6401
Emergency Dept. Co-
ordinator – CNM ED
Emergency Dept. 6252/6253
Environment Manager Bleep 135 Ext: 5409
Hospital Driver Bleep 132
Household
Services/Contract
Cleaners
Bleep 222/ 276 (after hours)
5693/5084
ICU 6384/6380/6381
Information Help Line Risk Management Dept. 5741/5250/5179/5696/5089/5098
Laboratory 5353/5375/5304/5303
Bleep 158 (out of hours)
Laurel 6340
Estate Manager Ext: 5400
Maple 6239
Medical Social Worker Bleep 119/220
5281/5280/5545
Dept. of Clinical
Engineering
Ext: 5073
Minor/Green Area Out Patients Dept. 5829/5834/5836
Mortuary – temporary
Physio Treatment Room
Physiogym Bleep 191
Ext: 5256

132
Nursing Manager D of N Office 5121/5123
Pharmacy 6010
Portering Services Emergency Dept. Bleep 297
Security Bleep 134 :ext:5438/5641
Supplies Officer Stores 5111
Theatre 6315/6316
Transport Supervisor Bleep 130
Ext: 5125
Silver Birch 5510/5511
Sycamore 5530/5531
Woodlands 5560/5561
X-ray Dept. Bleep 298 5248/5298
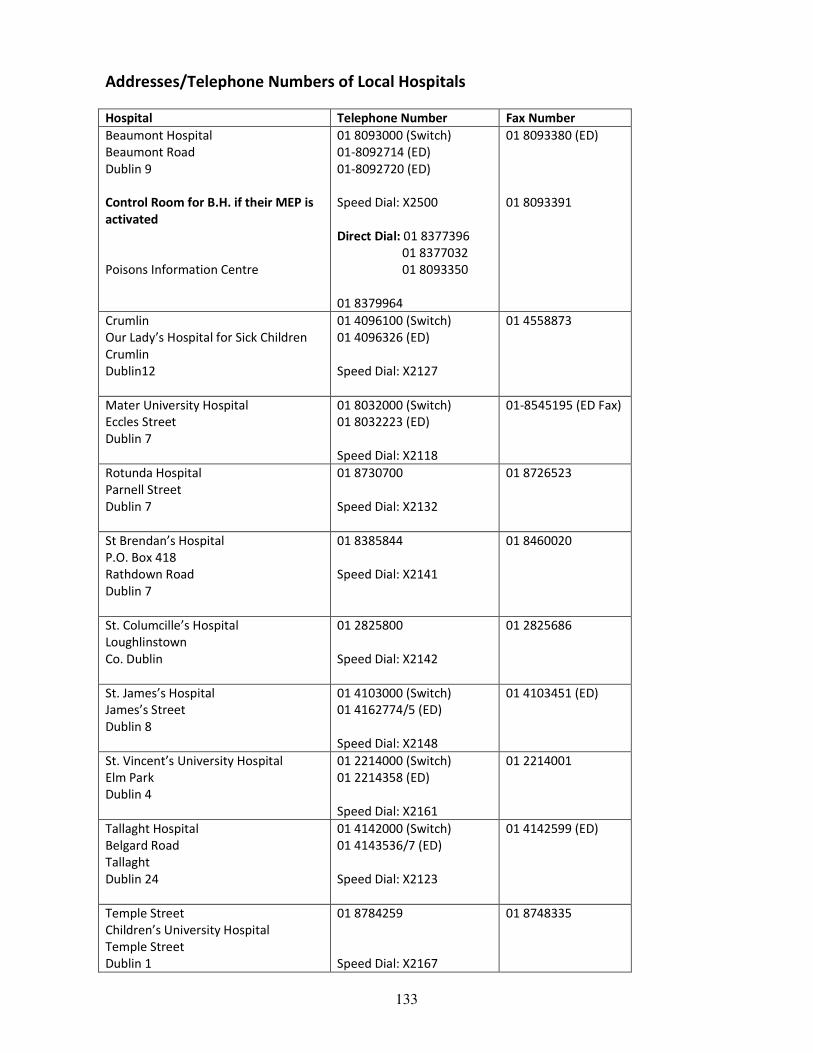
133
Addresses/Telephone Numbers of Local Hospitals
Hospital Telephone Number Fax Number
Beaumont Hospital
Beaumont Road
Dublin 9
Control Room for B.H. if their MEP is
activated
Poisons Information Centre
01 8093000 (Switch)
01-8092714 (ED)
01-8092720 (ED)
Speed Dial: X2500
Direct Dial: 01 8377396
01 8377032
01 8093350
01 8379964
01 8093380 (ED)
01 8093391
Crumlin
Our Lady’s Hospital for Sick Children
Crumlin
Dublin12
01 4096100 (Switch)
01 4096326 (ED)
Speed Dial: X2127
01 4558873
Mater University Hospital
Eccles Street
Dublin 7
01 8032000 (Switch)
01 8032223 (ED)
Speed Dial: X2118
01-8545195 (ED Fax)
Rotunda Hospital
Parnell Street
Dublin 7
01 8730700
Speed Dial: X2132
01 8726523
St Brendan’s Hospital
P.O. Box 418
Rathdown Road
Dublin 7
01 8385844
Speed Dial: X2141
01 8460020
St. Columcille’s Hospital
Loughlinstown
Co. Dublin
01 2825800
Speed Dial: X2142
01 2825686
St. James’s Hospital
James’s Street
Dublin 8
01 4103000 (Switch)
01 4162774/5 (ED)
Speed Dial: X2148
01 4103451 (ED)
St. Vincent’s University Hospital
Elm Park
Dublin 4
01 2214000 (Switch)
01 2214358 (ED)
Speed Dial: X2161
01 2214001
Tallaght Hospital
Belgard Road
Tallaght
Dublin 24
01 4142000 (Switch)
01 4143536/7 (ED)
Speed Dial: X2123
01 4142599 (ED)
Temple Street
Children’s University Hospital
Temple Street
Dublin 1
01 8784259
Speed Dial: X2167
01 8748335

134
Emergency Services Telephone Numbers
Dublin Fire Brigade
Mobilisation Officer:
01 6778221
01 6734000
6703198/673
Speed Dial: X2240
Gardai, Blanchardstown 01 6667000
Speed Dial: X2242
Pelican House 01 4322800
Speed Dial: X2245
St. James Ambulance 01 670944
Speed Dial: X244
Private Ambulance
Lifeline
01 6014704
Nursing Agencies, Telephone and Faxes
Name Telephone Fax
Alliance Nurses Agency 01 6787333 01 6787281
Life Line Nurses Agency 01 8681065
Medical Recruitment
Specialist
01 6146063 01 6146011
Nurses On Call 01 4126569
Taxi’s and Private Ambulance’s
Name Number
Castleknock and Blanchardstown Cabs 01 8225048
City Cabs 01 8727272 and 01 4732226
Clonee Cabs 01 8207465
D. 15, Cabs 01 8829996
Fitzers Cabs 01 8200300
National Radio Cabs 01 6772222
Pony Cabs 01 8202020
Lifeline Ambulance 01 6014704
Medical Ambulance 1890 666999

135
Major Emergency Planning Steering Committee
Ms Marlize Barnard, Bed Manager
Ms Fiona Brady, CNMIII, Emergency Dept.
Ms Maria Clarke, Head Medical Social Worker
Dr Niamh Collins, Consultant in Emergency Medicine
Mr Joe Feely, Chief Medical Scientist
Ms Theresa Heller, Human Resource Manager
Ms Mairead Lyons, A/Director of Nursing
Ms Annette Murphy, Major Emergency Planning Coordinator/Business Manager
Dr Andrew Tierney, Consultant Anaesthetist
Ms Mary Walshe, Hospital Manager