mainenance, surveillance, and interventions for native ... · 3/17/2009 1 mainenance, surveillance,...
TRANSCRIPT

3/17/2009
1
Mainenance, Surveillance, and Interventions Mainenance, Surveillance, and Interventions for Native Fistulaefor Native Fistulae
Gordon McLennan, MDGordon McLennan, MDInterventional Radiology & BioengineeringInterventional Radiology & Bioengineering
Cleveland ClinicCleveland Clinic
DisclosuresDisclosures
Consultant:Consultant:Consultant:Consultant:Bard, Medtronic, CookBard, Medtronic, Cook
Grant SupportGrant SupportOmnisonicsOmnisonicsCookCookBoston ScientificBoston ScientificBoston ScientificBoston ScientificBardBardMirMedicalMirMedical

3/17/2009
2
ObjectivesObjectives
Discuss ongoing assessment needsDiscuss ongoing assessment needsDiscuss ongoing assessment needsDiscuss ongoing assessment needs
Describe the different tools & processes used to monitor Describe the different tools & processes used to monitor AVFAVF
Explain failure to matureExplain failure to mature
Clinical ScenarioClinical Scenario
50 year old african american female presents to 50 year old african american female presents to y py pemergency room with nausea, decreased appetite, & emergency room with nausea, decreased appetite, & drowsiness which caused her to collapse at home.drowsiness which caused her to collapse at home.
During the Hospitalization, she is diagnosed with During the Hospitalization, she is diagnosed with acute worsening of what was likely chronic renal acute worsening of what was likely chronic renal failure & her serum creatinine is now 6.5. failure & her serum creatinine is now 6.5.
During the hospital course she received a dialysis During the hospital course she received a dialysis catheter to initiate hemodialysis. Incatheter to initiate hemodialysis. In--patient patient education has been limited & she now presents to education has been limited & she now presents to your dialysis unit.your dialysis unit.

3/17/2009
3
GUIDELINE 1. PATIENT PREPARATION FOR PERMANENT HEMODIALYSIS ACCESS GUIDELINE 1. PATIENT PREPARATION FOR PERMANENT HEMODIALYSIS ACCESS Appropriate planning allows for the initiation of dialysis therapy at the appropriate time Appropriate planning allows for the initiation of dialysis therapy at the appropriate time with a permanent access in place at the start of dialysis therapy.with a permanent access in place at the start of dialysis therapy.
1.1 Patients with a glomerular filtration rate (GFR) less than 30 mL/min/1.73 m1.1 Patients with a glomerular filtration rate (GFR) less than 30 mL/min/1.73 m22 (CKD stage (CKD stage 4) should be educated on all modalities of kidney replacement therapy (KRT) options, 4) should be educated on all modalities of kidney replacement therapy (KRT) options, including transplantation, so that timely referral can be made for the appropriate modality including transplantation, so that timely referral can be made for the appropriate modality and placement of a permanent dialysis access, if necessary. (A)and placement of a permanent dialysis access, if necessary. (A)
1.2 In patients with CKD stage 4 or 5, forearm and upper1.2 In patients with CKD stage 4 or 5, forearm and upper--arm veins suitable for placement arm veins suitable for placement of vascular access should not be used for venipuncture or for the placement of intravenous of vascular access should not be used for venipuncture or for the placement of intravenous p pp p(IV) catheters, subclavian catheters, or peripherally inserted central catheter lines (PICCs). (IV) catheters, subclavian catheters, or peripherally inserted central catheter lines (PICCs). (B)(B)
1.3 Patients should have a functional permanent access at the initiation of dialysis therapy.1.3 Patients should have a functional permanent access at the initiation of dialysis therapy.1.3.1 A fistula should be placed at least 6 months before the anticipated start of HD treatments. 1.3.1 A fistula should be placed at least 6 months before the anticipated start of HD treatments. This timing allows for access evaluation and additional time for revision to ensure a working This timing allows for access evaluation and additional time for revision to ensure a working fistula is available at initiation of dialysis therapy. (B) fistula is available at initiation of dialysis therapy. (B) 1.3.2 A graft should, in most cases, be placed at least 3 to 6 weeks before the anticipated start of 1.3.2 A graft should, in most cases, be placed at least 3 to 6 weeks before the anticipated start of HD therapy. Some newer graft materials may be cannulated immediately after placement. (B) HD therapy. Some newer graft materials may be cannulated immediately after placement. (B) 1.3.3 A peritoneal dialysis (PD) catheter ideally should be placed at least 2 weeks before the 1.3.3 A peritoneal dialysis (PD) catheter ideally should be placed at least 2 weeks before the anticipated start of dialysis treatments. A backup HD access does not need to be placed in most anticipated start of dialysis treatments. A backup HD access does not need to be placed in most patients. A PD catheter may be used as a bridge for a fistula in “appropriate” patients. (B) patients. A PD catheter may be used as a bridge for a fistula in “appropriate” patients. (B)
1.4 Evaluations that should be performed before placement of a permanent HD access 1.4 Evaluations that should be performed before placement of a permanent HD access include (Table 1):include (Table 1):
1.4.1 History and physical examination, (B) 1.4.1 History and physical examination, (B) 1.4.2 Duplex ultrasound of the upper1.4.2 Duplex ultrasound of the upper--extremity arteries and veins, (B) extremity arteries and veins, (B) 1.4.3 Central vein evaluation in the appropriate patient known to have a previous catheter or 1.4.3 Central vein evaluation in the appropriate patient known to have a previous catheter or pacemaker. (A) pacemaker. (A)
Ultrasound Access PlanningUltrasound Access Planning
Ultrasound the entire Ultrasound the entire arm with & without arm with & without tourniquettourniquet
Radial artery > 2mmRadial artery > 2mmCephalic Vein Cephalic Vein >> 2.0 mm2.0 mmCephalic Vein should be Cephalic Vein should be continuouscontinuousCentral stenosis Central stenosis evaluated by valsalvaevaluated by valsalvaAlso look at cephalic Also look at cephalic Also look at cephalic Also look at cephalic above elbow, basilic & above elbow, basilic & brachial for possible brachial for possible transfertransfer
Goal: to be able to tell Goal: to be able to tell the surgeon what vein the surgeon what vein to use for an AVFto use for an AVF
Robbin et. al. Radiology 2000; 217: 83-88Mendes et. al. JVS 2002; 36: 460-463

3/17/2009
4
ElbowElbow 2.72.7
Upper ArmUpper Arm 4.54.5
ShoulderShoulder 3.93.9
Allen TestAllen Test 5 Second 5 Second
VenographyVenography
Get complete imaging Get complete imaging p g gp g gof veins from wrist to of veins from wrist to HeartHeart
Should be performed Should be performed if suspect central if suspect central stenosis or occlusionstenosis or occlusion
Performed in Performed in Performed in Performed in conjunction with conjunction with treatments of failing treatments of failing accesses.accesses.

3/17/2009
5
Ehrman et. al. JVIR 1994; 5:771-775
COCO22 VenographyVenographyCO2 75% accurate for measuring stenoses in 32 patients CO2 75% accurate for measuring stenoses in 32 patients with failing fistulaewith failing fistulae
CO2 & Contrast equivalent for arterial measurements CO2 & Contrast equivalent for arterial measurements compared to IVUScompared to IVUS
McLennan et. al. JVIR 2001; 12:985-989
Nephrogenic Sclerosing Nephrogenic Sclerosing FibrosisFibrosis
FDA Recommendation (2006): FDA Recommendation (2006): When a patient with When a patient with FDA Recommendation (2006): FDA Recommendation (2006): When a patient with When a patient with moderate to endmoderate to end--stage kidney disease needs an imaging stage kidney disease needs an imaging study, select imaging methods other than MRI or MRA study, select imaging methods other than MRI or MRA with a gadoliniumwith a gadolinium--based contrast agent for the study based contrast agent for the study whenever possible.whenever possible. If these patients must receive a If these patients must receive a gadoliniumgadolinium--based contrast agent, prompt dialysis based contrast agent, prompt dialysis following the MRI or MRA should be considered.following the MRI or MRA should be considered.
Gadolinium is not approved for angiography.Gadolinium is not approved for angiography.
215 cases worldwide. 75 investigated215 cases worldwide. 75 investigated——all had Gd & Gd all had Gd & Gd was seen in skin biopsies.was seen in skin biopsies.

3/17/2009
6
Referral to SurgeonReferral to SurgeonMany types of fistulae can be created.Many types of fistulae can be created.
Simple AV FistulaeSimple AV FistulaeSimple AV FistulaeSimple AV FistulaeRadialRadial--Cephalic (forearm)Cephalic (forearm)BrachialBrachial--Cephalic (arm)Cephalic (arm)Proximal RadialProximal Radial--Median antebrachial (forearm)Median antebrachial (forearm)
TranspositionsTranspositionsCephalic vein (forearm) Radial artery to Cephalic veinCephalic vein (forearm) Radial artery to Cephalic veinBasilic vein (forearm) Radial artery to Basilic veinBasilic vein (forearm) Radial artery to Basilic veinCephalic vein (arm) Brachial artery to Cephalic veinCephalic vein (arm) Brachial artery to Cephalic veinCephalic vein (arm) Brachial artery to Cephalic veinCephalic vein (arm) Brachial artery to Cephalic veinBasilic vein (arm) Brachial artery to Basilic veinBasilic vein (arm) Brachial artery to Basilic veinSaphenous vein (thigh) Femoral artery to saphenous veinSaphenous vein (thigh) Femoral artery to saphenous veinFemoral vein (thigh) Femoral artery to Femoral veinFemoral vein (thigh) Femoral artery to Femoral vein
Vein TranslocationsVein Translocations
Many types of fistulas can Many types of fistulas can be createdbe created
Simple AV FistulaeSimple AV FistulaeRadialRadial Cephalic (forearm)Cephalic (forearm)RadialRadial--Cephalic (forearm)Cephalic (forearm)BrachialBrachial--Cephalic (arm)Cephalic (arm)Proximal RadialProximal Radial--Median antebrachial (forearm)Median antebrachial (forearm)
TranspositionsTranspositionsCephalic vein (forearm) Radial artery to Cephalic veinCephalic vein (forearm) Radial artery to Cephalic veinBasilic vein (forearm) Radial artery to Basilic veinBasilic vein (forearm) Radial artery to Basilic veinCephalic vein (arm) Brachial artery to Cephalic veinCephalic vein (arm) Brachial artery to Cephalic veinp ( ) y pp ( ) y pBasilic vein (arm) Brachial artery to Basilic veinBasilic vein (arm) Brachial artery to Basilic veinSaphenous vein (thigh) Femoral artery to saphenous veinSaphenous vein (thigh) Femoral artery to saphenous veinFemoral vein (thigh) Femoral artery to Femoral veinFemoral vein (thigh) Femoral artery to Femoral vein
Vein TranslocationsVein Translocations
3/17/2009
7
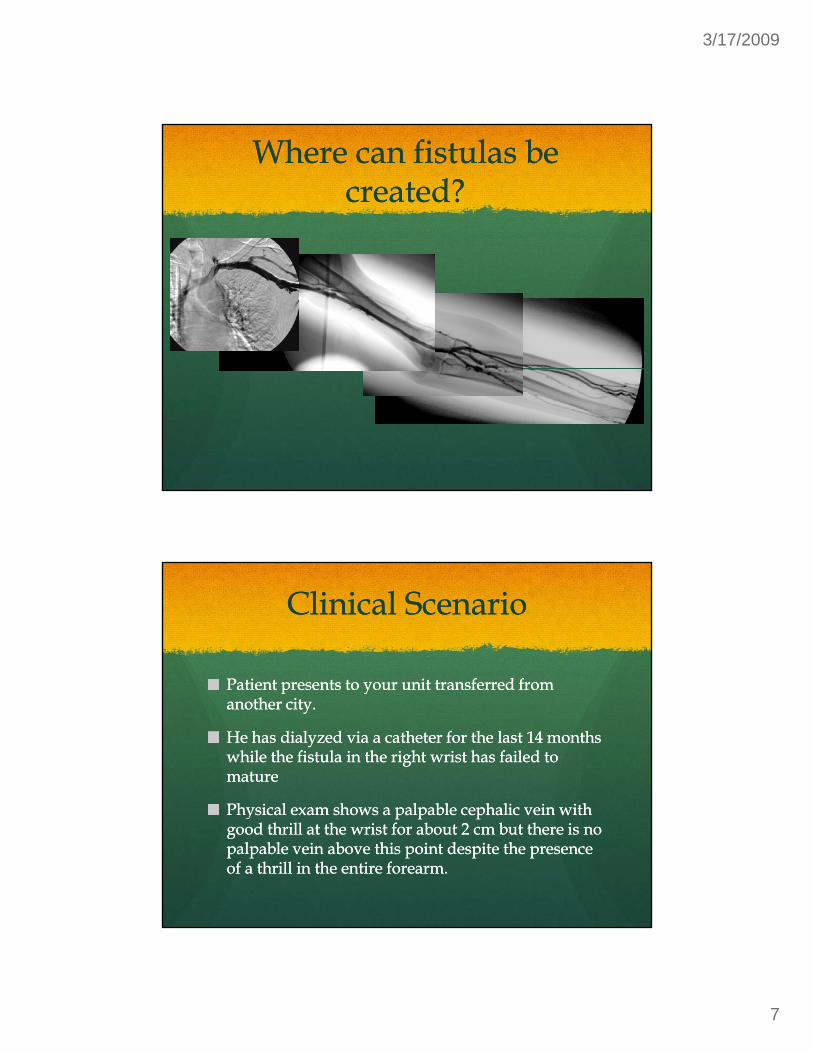
Where can fistulas be Where can fistulas be created?created?
�� ��
�� �
�
Clinical ScenarioClinical Scenario
Patient presents to your unit transferred from Patient presents to your unit transferred from Patient presents to your unit transferred from Patient presents to your unit transferred from another city.another city.
He has dialyzed via a catheter for the last 14 months He has dialyzed via a catheter for the last 14 months while the fistula in the right wrist has failed to while the fistula in the right wrist has failed to maturemature
Ph i l h l bl h li i ith Ph i l h l bl h li i ith Physical exam shows a palpable cephalic vein with Physical exam shows a palpable cephalic vein with good thrill at the wrist for about 2 cm but there is no good thrill at the wrist for about 2 cm but there is no palpable vein above this point despite the presence palpable vein above this point despite the presence of a thrill in the entire forearm.of a thrill in the entire forearm.

3/17/2009
8
KK--DOQIDOQI
5 1 2 A program should be in place to detect early 5 1 2 A program should be in place to detect early 5.1.2 A program should be in place to detect early 5.1.2 A program should be in place to detect early access dysfunction, particularly delays in access dysfunction, particularly delays in maturation. The patient should be evaluated no maturation. The patient should be evaluated no later than 6 weeks after access placement. (B) later than 6 weeks after access placement. (B)
Is it hopeless?Is it hopeless?

3/17/2009
9
PTA 8mmPTA 8mm
Functional AccessFunctional Access

3/17/2009
10
Take home pointsTake home points
Have an algorithm to assess all fistulas as they Have an algorithm to assess all fistulas as they Have an algorithm to assess all fistulas as they Have an algorithm to assess all fistulas as they maturemature
Don’t let catheters stay more than 2 monthsDon’t let catheters stay more than 2 months
Assess accesses frequently as they mature & if they Assess accesses frequently as they mature & if they don’t mature by 2 months send them to be evaluated don’t mature by 2 months send them to be evaluated b fi t l hb fi t l hby fistulography.by fistulography.
Clinical ScenarioClinical Scenario
45 year old male is in your CKD clinic & has been 45 year old male is in your CKD clinic & has been 45 year old male is in your CKD clinic & has been 45 year old male is in your CKD clinic & has been followed for the last 3 months.followed for the last 3 months.
GFR at initial visit was 42 & it has slowly decreased GFR at initial visit was 42 & it has slowly decreased every month to 38, 34, & now it is 31.every month to 38, 34, & now it is 31.
What do you do?What do you do?

3/17/2009
11
Ultrasound MappingUltrasound MappingUltrasound MappingUltrasound Mapping
Surgical Referral for fistula placementSurgical Referral for fistula placement
Reaffirm vein protection principlesReaffirm vein protection principlesNo Ivs or blood draws above the handsNo Ivs or blood draws above the handsNo picc lines in the armsNo picc lines in the armsNo Subclavian linesNo Subclavian linesDialysis catheters are temporary bridges not Dialysis catheters are temporary bridges not permanent accesses. permanent accesses. Goal will be to have a functioning fistulaGoal will be to have a functioning fistula
Clinical ScenarioClinical Scenario
Patient in your unit has had a forearm loop graft for Patient in your unit has had a forearm loop graft for Patient in your unit has had a forearm loop graft for Patient in your unit has had a forearm loop graft for the last 3 years. It has had one prior declot about 8 the last 3 years. It has had one prior declot about 8 months ago in which it was noted that the venous months ago in which it was noted that the venous anastamosis was stenotic & needed angioplasty. anastamosis was stenotic & needed angioplasty.
Now you are having alarms on the machine Now you are having alarms on the machine indicating High venous pressures.indicating High venous pressures.

3/17/2009
12
PTA 8mmPTA 8mm
What to do?What to do?

3/17/2009
13
Look for suitable veins in Look for suitable veins in patients with graftspatients with grafts
This patient has an arterialized upper arm cephalic This patient has an arterialized upper arm cephalic This patient has an arterialized upper arm cephalic This patient has an arterialized upper arm cephalic veinvein
Conversion to upper arm fistula can be performedConversion to upper arm fistula can be performed
Access could then be used immediatelyAccess could then be used immediately
Physical exam & Physical exam & MonitoringMonitoring
Important to examine the arms regularly with the Important to examine the arms regularly with the Important to examine the arms regularly with the Important to examine the arms regularly with the sleeves up to look for additional veins that could be sleeves up to look for additional veins that could be converted to fistulas.converted to fistulas.
In patients with fistulas, the physical exam can In patients with fistulas, the physical exam can identify changes in the fistula above & below the identify changes in the fistula above & below the elbowelbow

3/17/2009
14
Monitoring Monitoring TechniquesTechniques
4.1 Physical examination (monitoring): Physical examination should be used to detect 4.1 Physical examination (monitoring): Physical examination should be used to detect dysfunction in fistulae and grafts at least monthly by a qualified individual. (B)dysfunction in fistulae and grafts at least monthly by a qualified individual. (B)4.2 4.2 Surveillance of grafts:Surveillance of grafts:
4.2.1 Preferred: 4.2.1 Preferred: 4.2.1.1 Intra4.2.1.1 Intra--access flow by using 1 of several methods that are outlined in access flow by using 1 of several methods that are outlined in Table 7 using Table 7 using sequential measurements with trend analysis. (A) sequential measurements with trend analysis. (A) 4.2.1.2 Directly measured or derived static venous dialysis pressure by 1 of several methods. 4.2.1.2 Directly measured or derived static venous dialysis pressure by 1 of several methods. (A)(A)
4.2.1.3 Duplex ultrasound. (A)4.2.1.3 Duplex ultrasound. (A)4.2.2 Acceptable: 4.2.2 Acceptable:
4.2.2.1 Physical findings of persistent swelling of the arm, presence of collateral veins, 4.2.2.1 Physical findings of persistent swelling of the arm, presence of collateral veins, prolonged bleeding after needle withdrawal, or altered characteristics of pulse or thrill in a prolonged bleeding after needle withdrawal, or altered characteristics of pulse or thrill in a graft. (B) graft. (B)
4.2.3 Unacceptable:4.2.3 Unacceptable:4.2.3.1 Unstandardized dynamic venous pressures (DVPs) should not be used.4.2.3.1 Unstandardized dynamic venous pressures (DVPs) should not be used.
4.3 Surveillance in fistulae: Techniques, not 4.3 Surveillance in fistulae: Techniques, not mutually exclusive, that may be used in mutually exclusive, that may be used in surveillance for stenosis in AVFs include:surveillance for stenosis in AVFs include:
4.3.1 Preferred:4.3.1 Preferred:4.3.1.1 Direct flow measurements. (A) 4.3.1.1 Direct flow measurements. (A) 4.3.1.2 Physical findings of persistent swelling of the 4.3.1.2 Physical findings of persistent swelling of the arm, presence of collateral veins, prolonged bleeding arm, presence of collateral veins, prolonged bleeding after needle withdrawal, or altered characteristics of after needle withdrawal, or altered characteristics of pulse or thrill in the outflow vein. (B) pulse or thrill in the outflow vein. (B) 4.3.1.3 Duplex ultrasound. (A)4.3.1.3 Duplex ultrasound. (A)
4.3.2 Acceptable: 4.3.2 Acceptable: 4.3.2.1 Recirculation using a non4.3.2.1 Recirculation using a non––ureaurea--based based dilutional method. (B) dilutional method. (B) 4.3.2.2 Static pressures (B), direct or derived. (B) 4.3.2.2 Static pressures (B), direct or derived. (B)

3/17/2009
15
Physical ExaminationPhysical Examination
Need to assess all patients monthlyNeed to assess all patients monthlyAll patients with fistulae:All patients with fistulae:
Assess current functionAssess current function
All patients without fistulae:All patients without fistulae:Is there a vein that can be used to convert graft or catheter Is there a vein that can be used to convert graft or catheter to fistula?to fistula?Communicate which vein to use to surgeonCommunicate which vein to use to surgeon
Examine all patients with tourniquet & look for Examine all patients with tourniquet & look for Examine all patients with tourniquet & look for Examine all patients with tourniquet & look for cephalic veincephalic vein
If cephalic is poor, is there an alternative?If cephalic is poor, is there an alternative?Do I need imaging to find the vein?Do I need imaging to find the vein?
Supplement exam with flow screening if thrombosis Supplement exam with flow screening if thrombosis rates highrates high
Physical Physical ExaminationExamination
Thrill throughout = Normal accessThrill throughout = Normal accessPulsatile = Outflow stenosisPulsatile = Outflow stenosisNo thrill and no pulse = Access thrombosisNo thrill and no pulse = Access thrombosisExamine weeklyExamine weeklyFollow trendsFollow trends
h ll h d f d l fh ll h d f d l fThrill at the venous end of dialysis grafts is Thrill at the venous end of dialysis grafts is predictive of successful outcome following predictive of successful outcome following intervention*intervention*
* Ponce P, et. al JVIR 14 (2) pt 2, Feb 2003; S28-29

3/17/2009
16
Clinical ScenarioClinical Scenario
63 year old chronic dialysis patient has been 63 year old chronic dialysis patient has been 63 year old chronic dialysis patient has been 63 year old chronic dialysis patient has been dialyzing via left Breciadialyzing via left Brecia--Cimino fistula for the last 12 Cimino fistula for the last 12 years without a problem.years without a problem.
On dialysis, the machine alarms & shuts down. On dialysis, the machine alarms & shuts down. Small clots are noted in the arterial line.Small clots are noted in the arterial line.
Th dl i iti d b t l t Th dl i iti d b t l t The needle is repositioned by an expert cannulator The needle is repositioned by an expert cannulator & the dialysis session still is terminated by “pulling & the dialysis session still is terminated by “pulling clots”clots”
What does “pulling clots” What does “pulling clots” meanmean
The most common cause of death on the dialysis The most common cause of death on the dialysis The most common cause of death on the dialysis The most common cause of death on the dialysis machine is . . .machine is . . . DisconnectionWhen a disconnection occurs, air gets into the line & When a disconnection occurs, air gets into the line & to prevent a massive air embolus, the machine is to prevent a massive air embolus, the machine is shut down by an air bubble sensor.shut down by an air bubble sensor.
Small clots in the arterial line will look like a bubble Small clots in the arterial line will look like a bubble Small clots in the arterial line will look like a bubble Small clots in the arterial line will look like a bubble to the sensor and shut the machine down.to the sensor and shut the machine down.
Clots will be visible in the lineClots will be visible in the line

3/17/2009
17
What is happening?What is happening?
Is the needle in clot?Is the needle in clot? Maybe check the accessIs the needle in clot?Is the needle in clot?
Is the access clotted?Is the access clotted?
Maybe—check the access
Not if there is still a thrillMost commonly “pulling clots” is an indication of Most commonly “pulling clots” is an indication of arterial inflow stenosisarterial inflow stenosis
When flow is decreased When flow is decreased in the artery, there is in the artery, there is increased turbulence at increased turbulence at the anastamosisthe anastamosis
Clots form from decreased Clots form from decreased arterial flowarterial flow
Turbulence Turbulence Turbulence Turbulence activates activates thrombomodulin thrombomodulin locally & can locally & can cause small clots cause small clots to form in the to form in the access that get in access that get in access that get in access that get in the tubing the tubing

3/17/2009
18

3/17/2009
19
PTA 7mmPTA 7mm
Another Case of “Pulling Another Case of “Pulling Clots”Clots”

3/17/2009
20
Access TributariesAccess Tributaries
Ultrasound CorrelationUltrasound Correlation

3/17/2009
21
Clinical ScenarioClinical Scenario
PrePre ESRD patient with 8 month old fistulaESRD patient with 8 month old fistulaPrePre--ESRD patient with 8 month old fistulaESRD patient with 8 month old fistula
While the fistula was previously palpable to above While the fistula was previously palpable to above the elbow, now the fistula is only palpable just the elbow, now the fistula is only palpable just above the wrist and it is pulsatile. The patient is not above the wrist and it is pulsatile. The patient is not on dialysis yet.on dialysis yet.
4/28/04 Gadolinium
Fistula not functioning anymore
4/28/04 Gadolinium
6/9/04

3/17/2009
22
Cephalic Vein!!Cephalic Vein!!
3/17/2009
23
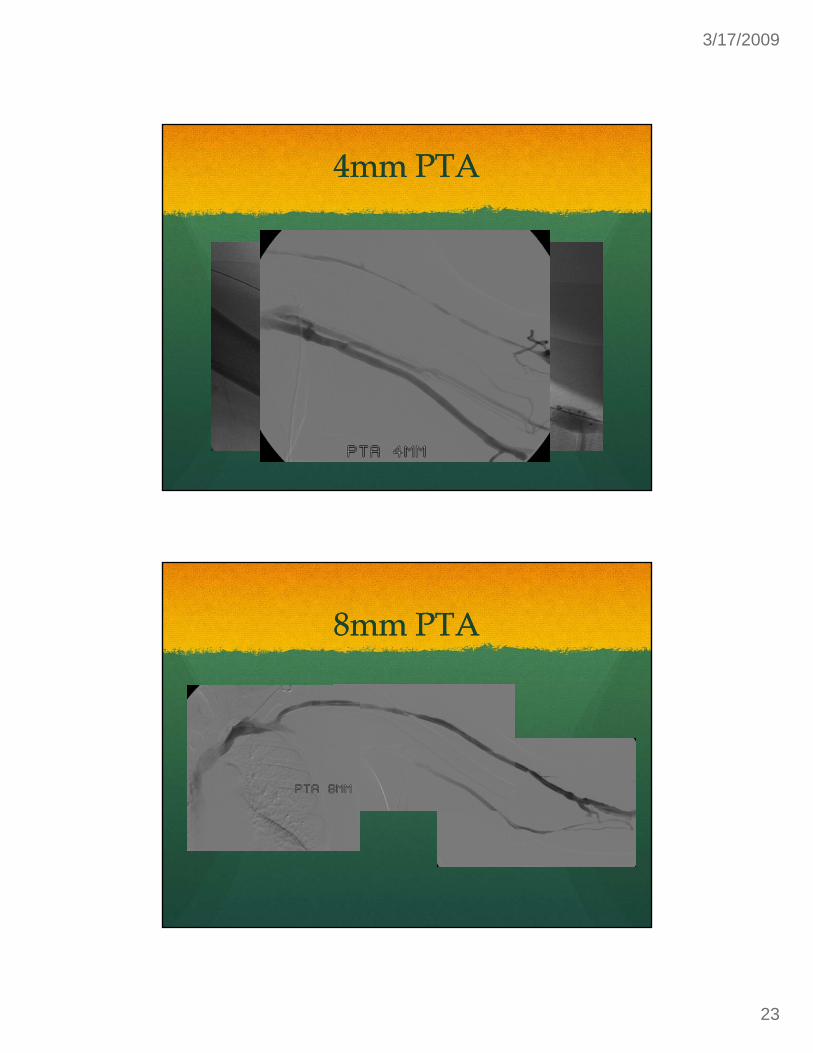
4mm PTA4mm PTA
8mm PTA8mm PTA

3/17/2009
24
FinalFinal
Clinical ScenarioClinical Scenario
44 y/o male who has dialyzed via left BCF for 2 44 y/o male who has dialyzed via left BCF for 2 44 y/o male who has dialyzed via left BCF for 2 44 y/o male who has dialyzed via left BCF for 2 years presents to dialysis unit with no thrill in the years presents to dialysis unit with no thrill in the fistula. fistula.
There is a small pulse at the anastamosisThere is a small pulse at the anastamosis
The normally plump outflow veins higher in the The normally plump outflow veins higher in the ti ll ll d ti ll ll darm appear partially collapsed.arm appear partially collapsed.

3/17/2009
25
Thrombosed AVFThrombosed AVF
ProcedureProcedure3000 U Heparin3000 U Heparin PTA 6mm3000 U Heparin3000 U Heparin
PTDPTD
OTW FogartyOTW Fogarty
Treat stenosesTreat stenoses
PTA 6mm
PTA 8mm

3/17/2009
26
Post PTDPost PTD
4 months 4 months LaterLater
Pt returns for Pt returns for high venous high venous pressurespressures

3/17/2009
27
PTPTAA
9mm
10mm10mm

3/17/2009
28
AlgorithmsAlgorithms
Venography or Venography or ultrasound in all ultrasound in all ultrasound in all ultrasound in all catheter & graft catheter & graft patientspatients
Look for Look for conversionsconversions
Algorithms to Algorithms to evaluate veins at evaluate veins at St 3 & 4St 3 & 4Stage 3 & 4Stage 3 & 4
Physical ExamPhysical ExamUltrasoundUltrasoundVenography where Venography where neededneeded
When to Refer for ImagingWhen to Refer for Imaging
4.4 When to refer for evaluation (diagnosis) and treatment:4.4 When to refer for evaluation (diagnosis) and treatment:( g )( g )
4.4.1 One should not respond to a single isolated abnormal value. With 4.4.1 One should not respond to a single isolated abnormal value. With all techniques, prospective trend analysis of the test parameter has all techniques, prospective trend analysis of the test parameter has greater power to detect dysfunction than isolated values alone. (A) greater power to detect dysfunction than isolated values alone. (A)
4.4.2 Persistent abnormalities in any of the monitoring or surveillance 4.4.2 Persistent abnormalities in any of the monitoring or surveillance parameters should prompt referral for access imaging. (A) parameters should prompt referral for access imaging. (A)
4.4.3 An access flow rate less than 600 mL/min in grafts and less than 400 4.4.3 An access flow rate less than 600 mL/min in grafts and less than 400 to 500 mL/min in fistulae. (A) to 500 mL/min in fistulae. (A)
4.4.4 A venous segment static pressure (mean pressures) ratio greater 4.4.4 A venous segment static pressure (mean pressures) ratio greater than 0.5 in grafts or fistulae. (A) than 0.5 in grafts or fistulae. (A)
4.4.5 An arterial segment static pressure ratio greater than 0.75 in grafts. 4.4.5 An arterial segment static pressure ratio greater than 0.75 in grafts. (A) (A)

3/17/2009
29
When to treat fistulaeWhen to treat fistulaeGUIDELINE 5. TREATMENT OF FISTULA COMPLICATIONSGUIDELINE 5. TREATMENT OF FISTULA COMPLICATIONS
Appropriate interventions for access dysfunction may result in an Appropriate interventions for access dysfunction may result in an i d d i f i l f h AVFi d d i f i l f h AVFincreased duration of survival of the AVF.increased duration of survival of the AVF.
5.1 Problems developing in the early period after AVF 5.1 Problems developing in the early period after AVF construction (first 6 months) should be promptly addressed.construction (first 6 months) should be promptly addressed.
5.1.1 Persistent swelling of the hand or arm should be expeditiously 5.1.1 Persistent swelling of the hand or arm should be expeditiously evaluated and the underlying pathology should be corrected. (B) evaluated and the underlying pathology should be corrected. (B) 5.1.2 A program should be in place to detect early access dysfunction, 5.1.2 A program should be in place to detect early access dysfunction, particularly delays in maturation. The patient should be evaluated particularly delays in maturation. The patient should be evaluated no later than 6 weeks after access placement. (B)no later than 6 weeks after access placement. (B)5 2 Intervention Intervention on a fistula should be performed for 5 2 Intervention Intervention on a fistula should be performed for 5.2 Intervention Intervention on a fistula should be performed for 5.2 Intervention Intervention on a fistula should be performed for the presence of:the presence of:5.2.1 Inadequate flow to support the prescribed dialysis blood flow. 5.2.1 Inadequate flow to support the prescribed dialysis blood flow. (B)(B)5.2.2 Hemodynamically significant venous stenosis. (B) 5.2.2 Hemodynamically significant venous stenosis. (B) 5.2.3 Aneurysm formation in a primary fistula. Postaneurysmal 5.2.3 Aneurysm formation in a primary fistula. Postaneurysmal stenosis that drives aneurysm also should be corrected. The stenosis that drives aneurysm also should be corrected. The aneurysmal segment should not be cannulated. (B)aneurysmal segment should not be cannulated. (B)5.2.4 Ischemia in the access arm (B).5.2.4 Ischemia in the access arm (B).
5.3 Indications for preemptive PTA:5.3 Indications for preemptive PTA:
A fistula with a greater than 50% stenosis in either the venous outflow A fistula with a greater than 50% stenosis in either the venous outflow or arterial inflow, in conjunction with clinical or physiological or arterial inflow, in conjunction with clinical or physiological abnormalities, should be treated with PTA or surgical revision. (B)abnormalities, should be treated with PTA or surgical revision. (B)
5.3.1 Abnormalities include reduction in flow, increase in static pressures, 5.3.1 Abnormalities include reduction in flow, increase in static pressures, access recirculation preempting adequate delivery of dialysis, or abnormal access recirculation preempting adequate delivery of dialysis, or abnormal physical findings. (B)physical findings. (B)p y g ( )p y g ( )
5.4 Stenosis, as well as the clinical parameters used to detect it, should 5.4 Stenosis, as well as the clinical parameters used to detect it, should return to within acceptable limits following intervention. (B)return to within acceptable limits following intervention. (B)5.5 5.5 Thrombectomy of a fistula should be attempted as early as possible Thrombectomy of a fistula should be attempted as early as possible after thrombosis is detected, but can be successful even after several after thrombosis is detected, but can be successful even after several days. (B)days. (B)5.6 Access evaluation for ischemia:5.6.1 Patients with an AVF 5.6 Access evaluation for ischemia:5.6.1 Patients with an AVF should be assessed on a regular basis for possible ischemia. (B) 5.6.2 should be assessed on a regular basis for possible ischemia. (B) 5.6.2 Patients with new findings of ischemia should be referred to a vascular Patients with new findings of ischemia should be referred to a vascular access surgeon emergently. (B)access surgeon emergently. (B)
5 7 Infection:5 7 Infection: Infections of primary AVFs are rare and should be treated Infections of primary AVFs are rare and should be treated 5.7 Infection:5.7 Infection:Infections of primary AVFs are rare and should be treated Infections of primary AVFs are rare and should be treated as subacute bacterial endocarditis with 6 weeks of antibiotic therapy. as subacute bacterial endocarditis with 6 weeks of antibiotic therapy. Fistula surgical excision should be performed in cases of septic emboli. Fistula surgical excision should be performed in cases of septic emboli. (B)(B)

3/17/2009
30
SummarySummary
Examine your patients at least monthly with sleeves Examine your patients at least monthly with sleeves Examine your patients at least monthly with sleeves Examine your patients at least monthly with sleeves upup
Use algorithmic monitoring scheme to find:Use algorithmic monitoring scheme to find:NonNon--maturing fistulae (within 2 months)maturing fistulae (within 2 months)Fistulas with problems that need interventionFistulas with problems that need interventionGrafts that can be converted to fistulaeGrafts that can be converted to fistulaeGrafts that can be converted to fistulaeGrafts that can be converted to fistulae
Algorithms & Formalized processes will improve Algorithms & Formalized processes will improve the speed of referral & improved patient outcomesthe speed of referral & improved patient outcomes