mahidol study 1: comparison of radiographic and survival...
TRANSCRIPT
Clinical Research
Mahidol Study 1: Comparison of Radiographic andSurvival Outcomes of Immature Teeth Treated with EitherRegenerative Endodontic or Apexification Methods:A Retrospective StudyThanawan Jeeruphan, DDS, Grad Dip in Clin Sc (Endodontics), High Grad Dip in Dentistry(Operative),* Jeeraphat Jantarat, DDS, MDSc, PhD,* Kallaya Yanpiset, DDS, MDSc,*
Lalida Suwannapan, DDS, Grad Dip in Clin Sc (Endodontics),*
Phannarai Khewsawai, DDS, High Grad Dip in Dentistry (Endodontics),†
and Kenneth M. Hargreaves, DDS, PhD‡
Abstract
Introduction: There are numerous challenges in treatingimmature permanent teeth with a diagnosis of pulpnecrosis. Three general treatment options are calciumhydroxide apexification, mineral trioxide aggregate(MTA) apexification, and revascularization. The objectiveof this retrospective study was to evaluate radiographicand clinical outcomes of immature teeth treated with 1of these 3 methods. Methods: Clinical outcome dataand radiographs were collected from 61 cases (ie, 22calcium hydroxide apexification cases, 19 MTA apexifica-tion cases, and 20 revascularization cases). Both toothsurvival and clinical success rates were analyzed. In addi-tion, the preoperative and recall radiographs wereanalyzed to calculate the percentage increase in rootwidth and length. Results: The percentage change ofroot width was significantly greater in the revasculariza-tion group (28.2%) compared with theMTA apexification(0.0%) and calcium hydroxide apexification groups(1.5%). In addition, the percentage increase of rootlength was significantly greater in the revascularizationgroup (14.9%) compared with the MTA (6.1%) andcalcium hydroxide apexification groups (0.4%). More-over, the survival rate of the revascularization-treatedteeth (100%) and MTA apexification�treated teeth(95%) were greater than the survival rates observed inteeth treated with calcium hydroxide (77.2%). Conclu-sions: In this study, revascularization was associatedwith significantly greater increases in root length andthickness in comparison with calcium hydroxide apexifi-cation and MTA apexification as well as excellent overallsurvival rates. (J Endod 2012;38:1330–1336)*Department of Operative Dentistry and Endodontics, Mahidol U‡Department of Endodontics, University of Texas Health Science Ce
Address requests for reprints to Dr Thanawan Jeeruphan, DepartmBangkok 10400, Thailand. E-mail address: [email protected]/$ - see front matter
Copyright ª 2012 American Association of Endodontists.http://dx.doi.org/10.1016/j.joen.2012.06.028
1330 Jeeruphan et al.
Key WordsApexification, calcium hydroxide, immature teeth, mineral trioxide aggregate, regener-ative endodontics, retrospective studies, revascularization
There are numerous challenges that the clinician faces when treating infectedpulp in immature permanent teeth. The cleaning and shaping of the root canal
system is challenging because of the thin dentinal walls. Obturation is also compli-cated because the apex is not fully developed and has a blunderbuss shape. More-over, these teeth may be susceptible to fracture during or after treatment (1).Traditionally, a calcium hydroxide–based apexification procedure has been advo-cated for treating an immature permanent tooth with an open apex (2). Teethtreated with this apexification procedure require a long-term application of calciumhydroxide in order to create an apical barrier to prevent the extrusion of obtura-tion materials. However, there are several drawbacks to this traditional apexificationprocedure, including a potential calcium hydroxide–mediated reduction in rootstrength and the requirement for excellent patient compliance because of theneed for multiple visits scheduled over many months (3, 4).Thus, the traditionalcalcium hydroxide treatment approach for these cases may be less than idealfor many patients.
Alternative apexification methods have recently been proposed. Mineral trioxideaggregate (MTA), used in a 1- or 2-step apexification procedure, has been shown tocreate an artificial apical barrier that permits the compaction of obturating materialand the placement of coronal restoration (5). Several case series have indicated thatMTA apexification treatment has a high success rate with a greatly decreased numberof appointments and time to completion (6–10). Despite these advantages, thesetreatments neither strengthen the root nor foster further root development. Thus,the roots remain thin and fragile, suggesting the need for another treatmentapproach.
A recently proposed alternative treatment is to promote continued hard-tissueformation and root growth. Revascularization is a regenerative treatment that isbiologically based and designed to allow the continuation of root development
niversity, Bangkok, Thailand; †Department of Dentistry, Pasang Hospital, Lamphun, Thailand; andnter at San Antonio, San Antonio, Texas.ent of Operative Dentistry and Endodontics, Mahidol University, 6 Yothi Street, Rajthevi, Payathai,
JOE — Volume 38, Number 10, October 2012

Figure 1. A clinical checklist used for all patients at each recall visit. Clinicians were instructed to check for pain, percussion sensitivity, probing depths, swelling,and fractures, and this information was placed under ‘‘Remarks.’’
Clinical Research
and strengthening of the root structure (11, 12). Many recentlypublished case reports (13–15) indicate that this treatment hasthe potential to promote the continued development of both theroot width and the overall root length in these immature cases.
However, there are no clinical data comparing the outcomes ofthese 3 treatments for the immature tooth with a necrotic pulp. Theobjective of this retrospective study was to compare the outcomes oftreatment in immature teeth with nonvital pulp among calciumhydroxide apexification, MTA apexification, and revascularization andto establish a standard protocol permitting future comparative studies.
Materials and MethodsThe study protocol was approved by the Ethics Committee
of Mahidol University (ref. 2012/009.2501). The dental charts of all
Figure 2. (A) The root length is measured from the CEJ to the radiographic apex.erative root canal length. (C) The pulp space was measured at the same level, and ththe root canal width.
JOE — Volume 38, Number 10, October 2012
patients who had treatment for an immature permanent tooth in theDepartment of Operative Dentistry and Endodontics and the Departmentof Pediatric Dentistry, Mahidol University, Bangkok, Thailand, between1997 and 2009 that fulfilled the following criteria were collected:
1. The immature permanent tooth was treated by either calciumhydroxide apexification, MTA apexification, or revascularization.
2. There was a preoperative, postoperative, and follow-up radiographof at least 6 months after the completion of treatment.
3. Clinical data of signs and symptoms of preoperative and follow-upvisits were recorded.
The data collected included patient age, sex, tooth number, clinicalsymptoms and signs, pulpal and periapical diagnoses, clinical proce-dures, size of apical radiolucency, root length, dentin thickness, the
(B) The root canal width was measured at the level of two thirds of the preop-e remaining dentin thickness was calculated by subtracting the pulp space from
Radiographic and Survival Outcomes of Immature Teeth 1331

TABLE 1. A Summary of Patient Demographics and the Clinical Characteristics of the Study Population
Variable
Revascularization(n = 20) MTA (n = 19)
Calcium hydroxide(n = 22)
Teeth % Teeth % Teeth %
SexFemale 10 50.00 6 31.58 9 40.91Male 10 50.00 13 68.42 13 59.09
Tooth typeIncisor 7 35.00 11 57.89 18 81.82Premolar 13 65.00 8 42.11 4 18.18
Tooth locationMaxilla 7 35.00 12 63.16 18 81.82Mandible 13 65.00 7 36.84 4 18.18
CauseCaries 1 5.00 4 21.05 0 0.00Dens evaginatus 12 60.00 4 21.05 4 18.18Trauma 7 35.00 11 57.89 18 81.82
Signs and symptoms*Absent 3 15.00 5 26.32 1 4.55Present 17 85.00 14 73.68 21 95.45
Apical periodontitisAbsent 1 5.00 6 31.58 8 36.36Present 19 95.00 13 68.42 14 63.64
Age (y) (mean � SD) 12.9 � 5.07 14.6 � 6.17 10.5 � 3.85Follow-up time (mo) (mean � SD) 21.15 � 11.70 14.21 � 7.84 27.32 � 30.47
SD, standard deviation.
*Signs and symptoms include pain, swelling, sinus opening, percussion, palpation, mobility, or probing depths >3 mm.
Clinical Research
follow-up period, and, if required, the reason for extraction. The collec-tion of these data was standardized by the use of a clinical checklist(Fig. 1) that is completed for all patients at all postoperative visits. Thisstandardized method of assessment has been used at Mahidol Universitysince 1995 and permits the analysis of radiographic, subjective (ie, painand percussion sensitivity), and objective (ie, sinus tract, swelling, andcrown fracture) outcomes after the completion of treatment.
Revascularization was accomplished in a 3-appointment processin which the first appointment consisted of rubber dam isolation, irri-gation with 2.5% NaOCl, and no instrumentation. The triple antibioticmix as described by Hoshino et al (16) was placed for a mean of28.85� 13.08 days between appointments; teeth were closed betweenappointments with a temporary restoration. The second appointmentconsisted of rubber dam isolation, irrigation with 2.5% NaOCl, andlaceration of the apical tissue using either a file or an endo spreader.A blood clot was formed in the canal and a matrix (Collaplug; ZimmerDental, Carlsbad, CA) was placed over the blood clot if the blood clotwas formed below the cementoenamel junction (CEJ). MTA apexifica-tion was accomplished in a 1-appointment procedure and consisted ofthe delivery of an apical plug of at least 3 mm MTA followed by obtura-tion with glass ionomer cement and resin composite. Calciumhydroxide apexification consisted of a rubber dam isolation and intra-canal delivery of Ca(OH)2 spread over a mean of 17 � 12.6 monthsfollowed by obturation with gutta-percha.
The preoperative and postoperative images were scanned witha Microtek scanner (Scanmaker 9800XL; Microtek International Inc,Hsinchu, Taiwan); saved in a JPEG format; and transferred to theimaging program software (Sopro; Acteon, La Cirotat Cedex, France)for measurement and recording the root length, dentin thickness,and the size of the periapical lesions. The size #2 of an intraoral radio-graphic film image in the Sopro software was calibrated by setting thehorizontal dimension to 31 mm and the vertical dimension to 41mm. The calibration process permitted the measurement of changesin root size on a millimeter scale. The root length from both the preop-erative and recall images weremeasured, which weremodified from theprocedure described by Bose et al (17). A straight line from the CEJ to
1332 Jeeruphan et al.
the radiographic apex of the tooth and the increasing root length wascalculated. The dentinal wall thickness for both the preoperative andrecall images were measured at the level of the apical one third ofthe preoperative root canal length measured from the CEJ (Fig. 2).The root canal width and the pulp space were measured at this level,and the remaining dentin thickness was calculated by subtracting thepulp space from the root canal width. The root length and the dentinwall thickness were reported in terms of percentage change in rootlength and percentage change in dentin thickness, respectively. Allradiographic measures were collected by the same investigator, andimages subjected to repeated analysis showed a kappa reliability. Arepeated measure of the same set of radiographs 1 week apart (n =15 cases) produced an intraexaminer agreement of k = 0.9845, indi-cating the reliability of these measures.
Treatment outcomes were assessed using both survival andsuccess as separate analyses. Survival was defined as retention of thetooth in the arch at the time of the postoperative recall. Althoughmany factors can contribute to a lack of survival, in this case series itwas exclusively because of a catastrophic fracture that was deemed non-restorable by the attending clinician. The second outcome analysis wassuccess. This was defined using the same criteria described by Fried-man and Mor (18), which consisted of the following categories:
1. Healed: Both the clinical (subjective and objective) and radio-graphic presentations were normal.
2. Healing: The periapical radiolucency was reduced with a normalclinical presentation.
3. Disease: The radiolucency was either increased or persisted withoutchange even when the clinical presentation was normal or clinicalsigns or symptoms were present regardless of the radiographicpresentation.
Statistical AnalysisAll radiographic measurements were repeated after 1 week, and
the mean of the 2 sets was considered as the final value. The data of
JOE — Volume 38, Number 10, October 2012

Figure 3. (A) A preoperative radiograph of calcium hydroxide apexification treatment of tooth #11 and (B) a recall radiograph at 12 months. (C) A preoperativeradiograph of MTA apexification treatment of tooth #34 and (D) a recall radiograph at 24 months. (E) A preoperative radiograph of revascularization treatment oftooth #45 and (F) a recall radiograph at 29 months.
Clinical Research
dentin thickness and root length were calculated as the percentagechange from the preoperative values. The radiographic data wereanalyzed initially for normality and were found to be nonnormallydistributed. The percentage change in root length and the percentagechange in the dentin of thickness were analyzed by the nonparametricKruskal-Wallis analysis of variance test, and the Mann-Whitney U test
Figure 4. (A) The percentage increase in root width after treatment with revascu(Ca(OH)2). (B) The percentage increase in root length after treatment. ***P < .0
JOE — Volume 38, Number 10, October 2012
was used to identify the difference among groups. A P value <.05 wasconsidered to be significant, and the mean values were reported.
ResultsThe retrospective chart review found 79 cases meeting the
eligibility criteria, of which 61 had documented recall
larization (Revasc) or with apexification by either MTA or calcium hydroxide01 vs all other groups. **P < .01 vs all other groups.
Radiographic and Survival Outcomes of Immature Teeth 1333
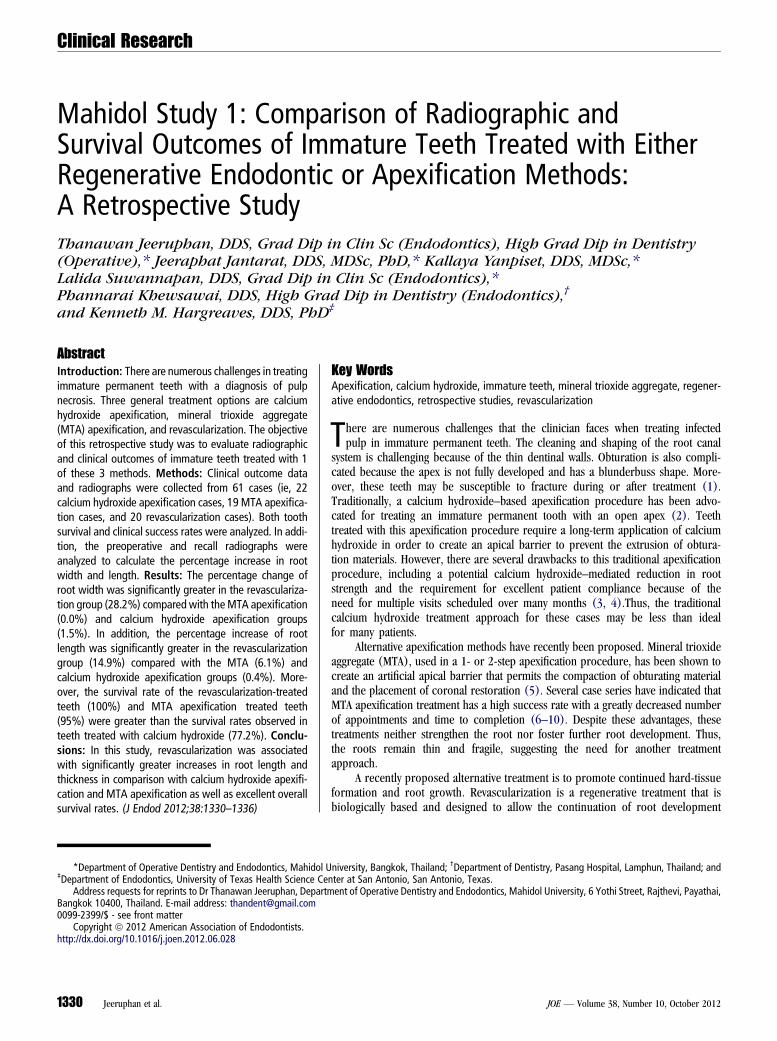
Figure 5. An evaluation of the contribution of patient age and sex to radiographic changes in (A) root width and (B) root length after revascularization treatment.Numbers at each bar indicate the number of patients per age group.
Clinical Research
information for a recall rate of 77%. These 61 cases included20 revascularization cases, 19 MTA apexification cases, and 22calcium hydroxide apexification cases. Table 1 summarizes thepatient demographics and the clinical characteristics of thisstudy population.
An analysis of the radiographic outcomes indicated a significanteffect (P < .0001) for revascularization treatment on the overallroot width at the apical third. Representative cases are presentedin Figure 3, and group analyses are presented in Figure 4. As de-picted in Figure 4A, the treatment of immature teeth with the revas-cularization protocol produced significantly greater percentageincreases in root width (28.2%) compared with teeth treated byeither MTA apexification (0.00%) or calcium hydroxide apexifica-tion (1.52%, P < .0001 for both comparisons). There were no
1334 Jeeruphan et al.
statistically significant differences between the calcium hydroxideapexification and the MTA apexification groups.
The treatment groups also differed significantly (P < .001) inthe development of the root length (Fig. 4B). Teeth treated withrevascularization showed a significantly greater percentage increasein root length (14.9%) compared with teeth treated by either MTAapexification (6.1%) or calcium hydroxide apexification (0.4%, P< .01 for both comparisons).
We next conducted a subset analysis to determine whether therewere any effects of patient age or sex on radiographic changes inroot development after the revascularization procedure (Fig. 5).Although the sample size was small, there was no trend for differencesin outcome for either increased root width (Fig. 5A) or increased rootlength (Fig. 5B) in this study population.
JOE — Volume 38, Number 10, October 2012

TABLE 2. The Survival Rate of Immature Permanent Teeth after Treatment
Outcome
Treatment
Revascularization(n = 20) MTA (n = 19)
Calciumhydroxide(n = 22)
Teeth % Teeth % Teeth %
Survivalrate
20 100.00 18 94.70 17 77.30
Clinical Research
We next evaluated clinical outcomes by both tooth survivalanalysis and a clinical success analysis. In terms of tooth survival(Table 2), revascularization had similar survival rates (20/20 teeth[100%]) compared with teeth treated with MTA apexification(18/19 teeth [95%]) although the follow-up times were nearly50% longer in the revascularization cases. Both of these treatmentsproduced greater survival rates (P < .05) compared with teethtreated with calcium hydroxide apexification (17/22 teeth [77%]).
The second clinical outcome analysis was based on successdefined by radiographic, objective, and subjective findings (Table 3).Teeth treated with the revascularization protocol had rates of completehealing (16/20 cases [80%]) similar to teeth treated with either theMTA (13/19 [68%]) or calcium hydroxide (17/22 [77%]) apexifica-tion methods. Alternatively, when using a looser outcome of ‘‘healed +healing,’’ teeth treated with the revascularization protocol had similaroverall rates (20/20 teeth [100%]) compared with teeth treated withMTA apexification (18/19 teeth [95%]), and both of these treatmentsproduced greater rates (P < .05) compared with teeth treated withcalcium hydroxide apexification (17/22 teeth [77%]).
DiscussionThe recent demonstration of good radiographic outcomes after
revascularization treatments applied to immature permanent teethhas greatly stimulated interest in this method. Although most of thedata are derived from case reports or relatively small case series, 1retrospective study has shown a significantly greater increase inroot width and length after revascularization compared with MTAapexification or traditional nonsurgical root canal treatment (17).The present study provides an independent replication of this priorretrospective study and extends this finding by analyzing calciumhydroxide apexification and performing an outcome analysis ofboth tooth survival and clinical success.
TABLE 3. The Success Rate of Immature Permanent Teeth after Treatment
Outcomes
Treatment
Revascularization(n = 20)
MTA(n = 19)
Calciumhydroxide(n = 22)
Teeth (%) Teeth (%) Teeth (%)
Healed* 16 (80.00) 13 (68.42) 17 (77.27)Healing† 4 (20.00) 5 (26.32) 0 (0.00)Disease‡ 0 (0.00) 1 (5.26) 5 (22.73)
*Both the clinical and radiographic presentations are normal.†The periapical radiolucency reduced combined with normal clinical presentation.‡The radiolucency was either increased or persisted without change even when the clinical presen-
tation was normal or the clinical signs or symptoms were present regardless of the radiographic
presentation.
JOE — Volume 38, Number 10, October 2012
There are several pertinent issues related to the present study.First, the routine use of a standardized clinical checklist for all recallpatients (Fig. 1) permits the evaluation of subjective and objectiveclinical outcomes that greatly expands an analysis of only radio-graphic outcomes. Second, the overall recall rate (77%) is higherthan that reported in many clinical studies, suggesting that theanalyzed data may reflect the actual outcomes observed in this patientpopulation. Third, the radiographic outcomes of the percentageincrease in root width and length for revascularization (28.2% and14.9%, respectively) and MTA apexification (0% and 6.0%, respec-tively) show the dramatic effect of this new treatment approach.Moreover, these data are similar to the results of the Bose et al study(17) in terms of relative effects (increases in radiographic root width>increases in length) and the magnitude of the effects. Although theBose et al data reported median effects because of the heterogeneityof variance in their clinical material, a reanalysis of their raw data formean effects reveals similar relative percentage increases in rootwidth and length for both revascularization (48% and 11%, respec-tively) and MTA apexification (0.2% and �0.2%, respectively) asseen in the present study. Collectively, these studies provide indepen-dent assessments of the efficacy of revascularization methods. Fourth,to our knowledge, this is the first study to quantitatively analyze bothtooth survival and clinical success after revascularization treatment.Taken together, these factors show the clinical usefulness of revascu-larization protocols and establish a framework for future studies inthis field.
This study does have issues that limit the interpretation of thedata. First, it is a retrospective study, and patients were not randomlyallocated to treatment. Second, the radiographs were not collectedusing standardized methods. However, we attempted to minimizethis particular issue by controlling central beam angulation by usingparallel technique films and a computer program to calibrate theimages.
Another clinically significant finding in this study was the clinicaloutcomes observed in teeth treated with calcium hydroxide apexifica-tion. This study found that the clinical and radiographic success ratefor calcium hydroxide apexification was 77.3% (healed), and forMTA apexification it was 68.4% (healed). This result was somewhatlower than that reported by El-Meligy and Avery (19), who reporteda success rate for calcium hydroxide apexification of 87% and forMTA apexification 100%. Another finding in the present study wasdifferences in tooth survival. The tooth survival after calcium hydroxideapexification was less than the other 2 treatments in this study. Thereason for extraction was nonrestorable root fracture. The durationof calcium hydroxide apexification can range from 3 to 21 months(19). During that time of treatment, the tooth is susceptible to reinfec-tion from coronal leakage and may be prone to fracture because theimmature tooth with an open apex has a thin dentin wall and a shortroot. In addition, Andreasen et al (3) found that long-term calciumhydroxide dressing in the root canal weakens the root structure. Inthis study, the time of a calcium hydroxide dressing in the root canalof the calcium hydroxide apexification group was 14.5 months.However, there were other factors that may have had an impact onthis outcome, such as restoration.
In conclusion, the present study provides an independent confir-mation of the findings of Bose et al (17) and indicates that revascular-ization protocols offer the potential for treating the immaturepermanent tooth with resulting resolution of signs and symptoms andthe initiation of continued root development. Moreover, the methodsdescribed in this study, including standardized clinical follow-up check-lists, provide the framework for continuing this study with both longerfollow-up periods and increased numbers of treated patients.
Radiographic and Survival Outcomes of Immature Teeth 1335

Clinical Research
AcknowledgmentsThe authors wish to thank Assistant Professor Panit Bandits-
ing, Department of Pediatric Dentistry, Mahidol University, forproviding cases for this study and Assistant Professor ChulalukKomoltri, Faculty of Medicine, Siriraj Hospital, for her help in statis-tical analysis.
The authors deny any conflicts of interest related to this study.
References1. Trope M. Treatment of immature teeth with non-vital pulps and apical periodontitis
endotopic. Endod Topics 2006;14:51–9.2. Rafter M. Apexification: a review. Dent Traumatol 2005;21:1–8.3. Andreasen JO, Farik B, Munksgaard EC. Long-term calcium hydroxide as a root
canal dressing may increase risk of root fracture. Dental Traumatol 2002;18:134–7.
4. Sheehy EC, Roberts GJ. Use of calcium hydroxide for apical barrier formation andhealing in non-vital immature permanent teeth: a review. Br Dent J 1997;183:241–6.
5. Torabinejad M, Chivian N. Clinical applications of mineral trioxide aggregate.J Endod 1999;25:197–205.
6. Witherspoon DE, Small JC, Regan JD, Nunn M. Retrospective analysis of openapex teeth obturated with mineral trioxide aggregate. J Endod 2008;34:1171–6.
7. Holden DT, Schwartz SA, Kirkpatrick TC, Schindler WG. Clinical outcomes of arti-ficial root-end barriers with mineral trioxide aggregate in teeth with immatureapices. J Endod 2008;34:812–7.
1336 Jeeruphan et al.
8. Mente J, Hage N, Pfefferle T, et al. Mineral trioxide aggregate apical plugs in teethwith open apical foramina: a retrospective analysis of treatment outcome. J Endod2009;35:1354–8.
9. Nayar S, Bishop K, Alani A. A report on the clinical and radiographic outcomes of 38cases of apexification with mineral trioxide aggregate. Eur J Prosthodont RestorDent 2009;17:150–6.
10. Annamalai S, Mungara J. Efficacy of mineral trioxide aggregate as an apical plug innon-vital young permanent teeth: preliminary results. J Clin Pediatr Dent 2010;35:149–55.
11. Hargreaves K, Law A. Regenerative endodontics. In: Hargreaves K, Cohen S, eds.Pathways of the Pulp. 10th ed. St Louis: Mosby Elsevier; 2011:602–19.
12. Huang GT. Apexification: the beginning of its end. Int Endod J 2009;42:855–66.13. Iwaya SI, Ikawa M, Kubota M. Revascularization of an immature permanent tooth
with apical periodontitis and sinus tract. Dent Traumatol 2001;17:185–7.14. Banchs F, Trope M. Revascularization of immature permanent teeth with apical peri-
odontitis: new treatment protocol? J Endod 2004;30:196–200.15. Thibodeau B, Trope M. Pulp revascularization of a necrotic infected immature
permanent tooth: case report and review of the literature. Pediatr Dent 2007;29:47–50.
16. Hoshino E, Kurihara-Ando N, Sato I, et al. In vitro antibacterial susceptibility ofbacteria taken from infected root dentine to a mixture of ciprofloxacin, metronida-zole, and minocycline. Int Endod J 1996;29:125–30.
17. Bose R, Hargreaves K, Nummikoski P. A retrospective evaluation of radiographicoutcomes in immature teeth with necrotic root canal systems treated with regener-ative endodontic procedures. J Endod 2009;35:1343–9.
18. Friedman S, Mor C. The success of endodontic therapy: healing and functionality.J Calif Dent Assoc 2004;32:493–503.
19. El-Meligy OA, Avery DR. Comparison of apexification with mineral trioxide aggregateand calcium hydroxide. Pediatr Dent 2006;28:248–53.
JOE — Volume 38, Number 10, October 2012

本文献由“学霸图书馆-文献云下载”收集自网络,仅供学习交流使用。
学霸图书馆(www.xuebalib.com)是一个“整合众多图书馆数据库资源,
提供一站式文献检索和下载服务”的24 小时在线不限IP
图书馆。
图书馆致力于便利、促进学习与科研,提供最强文献下载服务。
图书馆导航:
图书馆首页 文献云下载 图书馆入口 外文数据库大全 疑难文献辅助工具