maggie mcnally, james curtain, kirsty o’brien, borislav d dimitrov, and tom fahey hrb centre for...
TRANSCRIPT

Maggie McNally, James Curtain, Kirsty O’Brien, Borislav D Dimitrov, and Tom Fahey
HRB Centre for Primary Care Research
Department of General Practice
Royal College of Surgeons in Ireland
Predicting severity of pneumonia
in general practice: a meta-
analysis of the CRB-65 criteria

Outline
• What is a clinical prediction rule?
• Assessment of clinical prediction rules
• CRB-65: a clinical prediction rule
• Statistical methods in meta-analysis
• Results
• Conclusions
• Future work

Clinical Prediction Rule
• Clinical tool that quantifies contribution of:– History– Examination– Diagnostic tests
• Stratify patients according to probability of having target disorder
• Outcome can be in terms of diagnosis, prognosis, referral or treatment
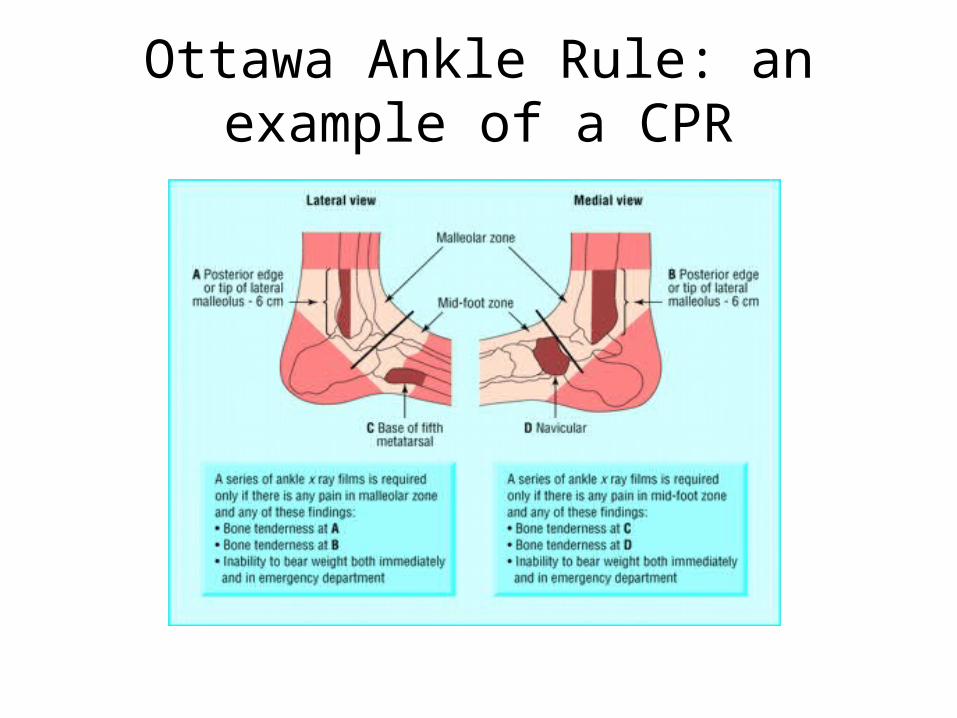
Ottawa Ankle Rule: an example of a CPR
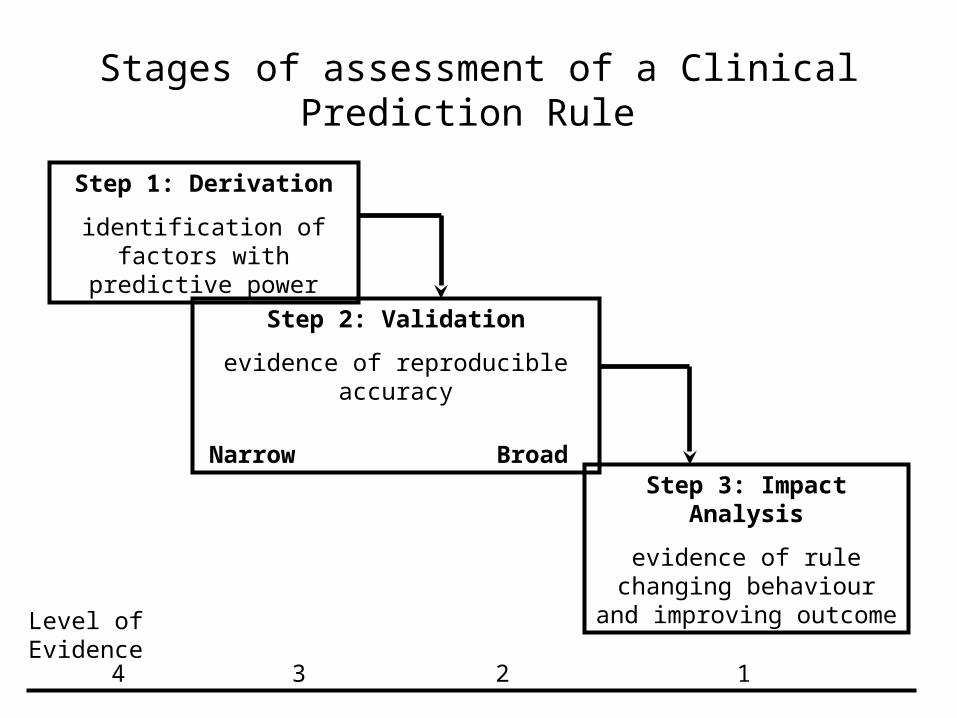
Stages of assessment of a Clinical Prediction Rule
Step 1: Derivation
identification of factors with predictive power
Step 2: Validation
evidence of reproducible accuracy
Narrow Broad
Step 3: Impact Analysis
evidence of rule changing behaviour and improving
outcome
Level of Evidence
4 3 2 1
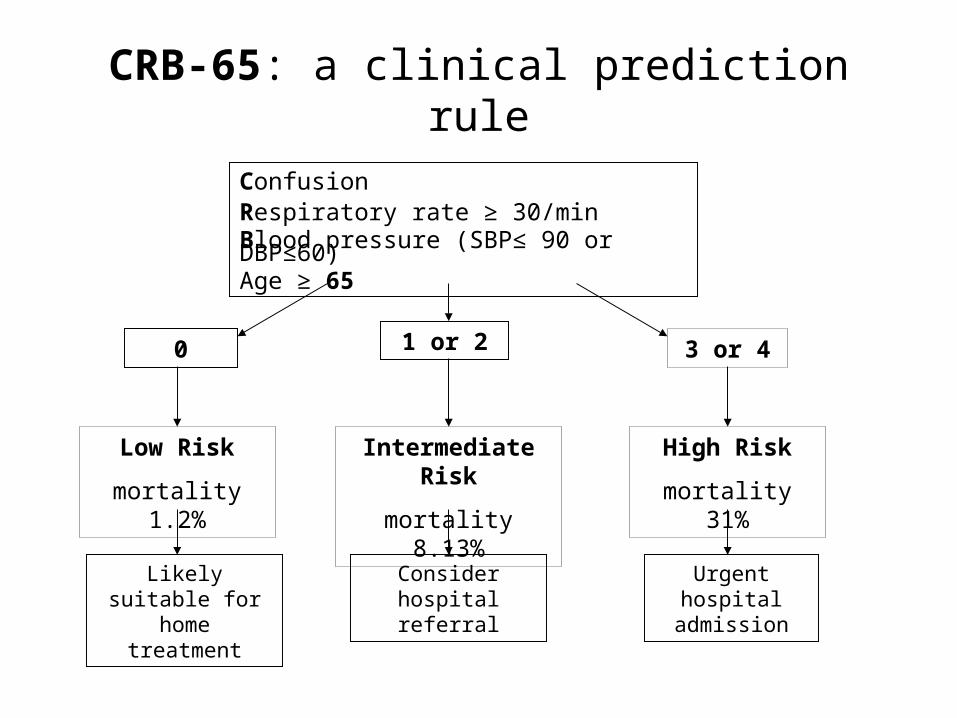
ConfusionRespiratory rate ≥ 30/min Blood pressure (SBP≤ 90 or DBP≤60)Age ≥ 65
0 1 or 2 3 or 4
Low Risk
mortality 1.2%
Intermediate Risk
mortality 8.13%
High Risk
mortality 31%
CRB-65: a clinical prediction rule
Likely suitable for home treatment
Consider hospital referral
Urgent hospital admission
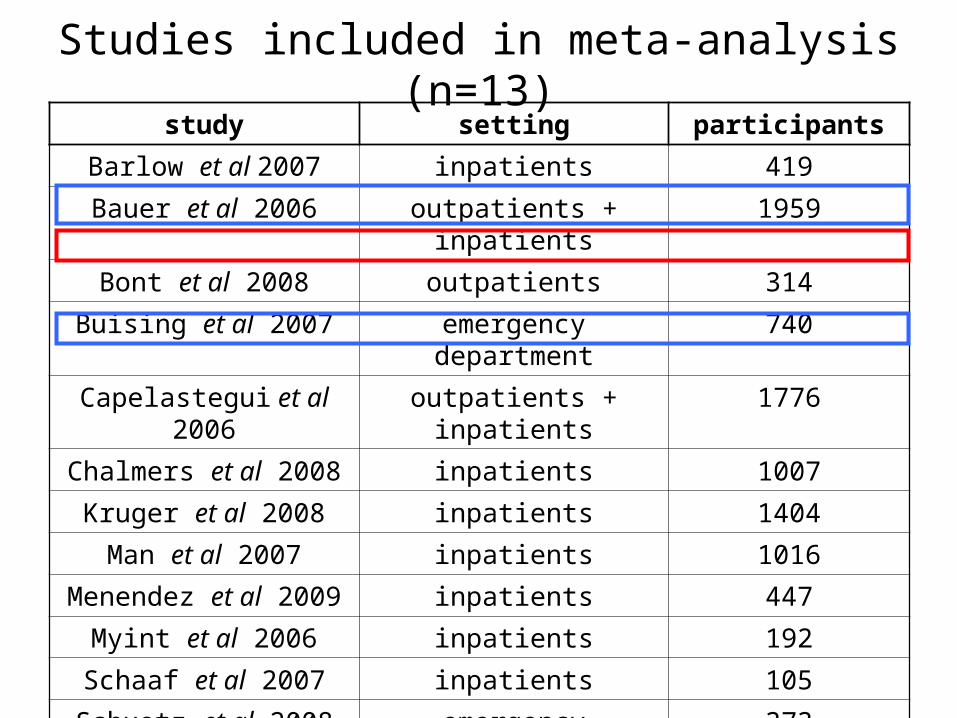
Studies included in meta-analysis (n=13)study setting participants
Barlow et al 2007 inpatients 419
Bauer et al 2006 outpatients + inpatients 1959
Bont et al 2008 outpatients 314
Buising et al 2007 emergency department 740
Capelastegui et al 2006 outpatients + inpatients 1776
Chalmers et al 2008 inpatients 1007
Kruger et al 2008 inpatients 1404
Man et al 2007 inpatients 1016
Menendez et al 2009 inpatients 447
Myint et al 2006 inpatients 192
Schaaf et al 2007 inpatients 105
Schuetz et al 2008 emergency department 373
Zuberi et al 2008 inpatients 137
TOTAL 9889

Level of evidence for CRB-65
Step 1: Derivation
identification of factors with predictive power
Step 2: Validation
evidence of reproducible accuracy
Narrow Broad
Step 3: Impact Analysis
evidence of rule changing behaviour and improving
outcome
Level of Evidence
4 3 2 1

Statistical Methods
• Derivation study used as predictive model
• Results presented as ratio measurement:
predicted deaths by CRB-65 rule
observed deaths in validation study

Results

ConfusionRespiratory rate ≥ 30/min Blood pressure (SBP≤ 90 or DBP≤60)Age ≥ 65
0 1 or 2 3 or 4
Low Risk
mortality 1.2%
Intermediate Risk
mortality 8.13%
High Risk
mortality 31%
CRB-65

RR 1.25 (CI 0.60 – 2.59)
RR 9.63 (CI 1.23 – 75.63)
n = 799
events = 0 (0%)
n = 1887
events = 14 (0.74%)

ConfusionRespiratory rate ≥ 30/min Blood pressure (SBP≤ 90 or DBP≤60)Age ≥ 65
0 1 or 2 3 or 4
Low Risk
mortality 1.2%
Intermediate Risk
mortality 8.13%
High Risk
mortality 31%
CRB-65

n = 647
events = 10 (1.5%)
n = 5674
events = 455 (8.0%)
RR 4.92 (CI 2.39 – 10.11)
RR 0.99 (CI 0.80 – 1.23)

ConfusionRespiratory rate ≥ 30/min Blood pressure (SBP≤ 90 or DBP≤60)Age ≥ 65
0 1 or 2 3 or 4
Low Risk
mortality 1.2%
Intermediate Risk
mortality 8.13%
High Risk
mortality 31%
CRB-65

n = 26
events = 5 (19.2%)
n = 869
events = 257 (29.6%)
RR 1.58 (CI 0.59 – 4.19)
RR 1.04 (CI 0.88 – 1.23)
Conclusions

ConfusionRespiratory rate ≥ 30/min Blood pressure (SBP≤ 90 or DBP≤60)Age ≥ 65
0 1 or 2 3 or 4
Low Risk
mortality 1.2%
Intermediate Risk
mortality 8.13%
High Risk
mortality 31%
Hospital Based Patients
Community Based Patients
• General trend towards over-prediction
• However,– Low cohort numbers– Low event numbers

Future Work
Step 1: Derivation
identification of factors with predictive power
Step 2: Validation
evidence of reproducible accuracy
Narrow Broad
Step 3: Impact Analysis
evidence of rule changing behaviour and improving
outcome
Level of Evidence
4 3 2 1
Acknowledgements
• RCSI Research Institute
• Grainne McCabe, RCSI Library