macra 071916
TRANSCRIPT
1
The Merit Health
Network
MACRA Overview –
July 2016

Background
2
MACRA permanently eliminates the SGR (and annual rate cuts)
Consolidates Medicare PQRS, MU, VBM reporting programs
Establishes a path to predominant Value-Based payment methodologies
Passed in Senate 92-8; Passed in House 392-37

Fears
3
Medicare projects 70% of rural practices with 2-9 docs will be penalized via MIPS
50% of non-pediatric physicians have never heard of MACRA
MIPS program is budget neutral; penalized providers will pay rewards for other providers
It is widely reported MACRA will force further consolidation

MIPS: National Financial Impact
4
• MIPS is Budget Neutral
• Government expects $833 million will be redistributed
• Additional $500 million in bonuses for top performers

MACRA Progression
5

Today vs. Tomorrow
6
Currently: QRUR MU PQRS/VBMNon-
Existent

QPP: MIPS? APM? Both….
7
Merit Incentive Based Payment
System (MIPS)
Default Program (≈90% of Medicare
Providers): A portion of Medicare
Revenue at the TIN/Individual Provider
Level is at risk based on the following
performance categories:
Alternative Payment Models (APMs)
Generic term for providers who receive
significant revenue through 2-sided risk-
based contracts.
Currently Proposed Options:
• Medicare Shared Savings Program
(MSSP) Tracks 2 & 3
• Next Generation ACO
• Oncology Care Model Two-sided Risk
Arrangement (Available 2018)
• Comprehensive End-Stage Renal Disease
Care (CEC) Model

Ultimate Goal: APM’s
8
• Requires:• “More than nominal” Risk• Quality measurement• Very advanced Value-
Based Design (Technology, Analytics, Workflow, Contracts, etc.)
• Provides:• Prospective 5% Lump-
Sum annual bonus in 2019-2024
• Exemption from MIPS requirements
2019
–
2020
2021–
2022
25% N/A
50%
N/A 25%
50%
OROption 1 Option 2
Required for All
Providers
2023
and
on
75%
N/A 25%
75%
Required Percentage of Revenue
Under Risk-Based Payment Models
Option 1
Medicare Only
Option 2
Medicare +
Commercial
Contracts

Current Focus: MIPS
9
• MIPS is the Default Program; AKA New Medicare FS• CMS anticipates 90% of all
physicians will be paid via MIPS in 1st year of the Quality Payment Program (QPP)
• Adjusts Medicare payments based on performance on a single budget-neutral payment beginning in 2019 (2-year Look-Back)
• Applies to physicians, NPs, clinical nurse specialists, physician assistants, and certified RN anesthetists

MIPS: Composite Performance Scores
10
4 Categories = 100%
1. Quality = 50%
2. Advancing Care Information = 25%
3. Clinical Practice Information Activities = 15%
4. Cost = 10%

11

Components of the MIPS Score
12

MIPS Category: Quality (50% Yr 1 MIPS Score)
13
From 9 PQRS Measures to 6 total Measures
During Open Comment period, many pushed towards specialty and
practice-specific measures
Final Rule to show many changes
Focus today on ability to incorporate 6 measures into workflow

MIPS Category: ACI (25% Yr 1 MIPS Score)
14
Key Takeaways:
High, historical MU compliance does not guarantee a high ACI score.
Unlike Historical MU, ACI Scoring is a CONTINUOUS scale, Not All-Or-Nothing
• Replaces Meaningful Use
• Potential to Participate as a group (If Final Rule allows)
• Advanced Practice Providers – exempt (Midlevels, NPs, PAs, etc.)
• Split Into Base Score & Performance Score
• Proposed Rule = Complicated Scoring (130 total points, only 100
needed to earn full score in ACI category)

ACI Base Score (50 Points)
15
6 Objective and Measure Categories
1. Protect Patient Health Information - Y/N (Required)
2. Patient Electronic Access - N/D
3. Coordination of Care & Patient Education - N/D
4. Electronic Prescribing - N/D
5. Health Information Exchange – N/D
6. Public Health/Registry Reporting – Y/N
*N/D = Numerator/Denominator

ACI Performance Score (80 Points)
16
3 Objective and Measure Categories
1. Patient Electronic Access - N/D
2. Coordination of Care & Patient Education – N/D
3. Health Information Exchange – N/D
** Immunization Registry – Mandatory
** Bonus Point – Pub Health reporting beyond immunizations
* N/D = Numerator/Denominator
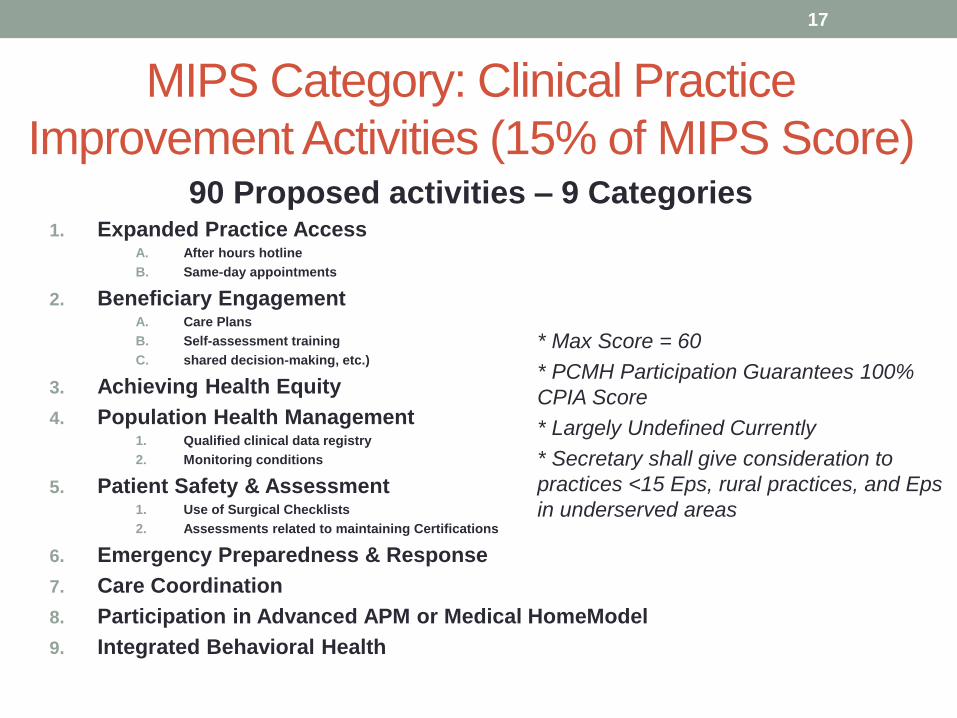
MIPS Category: Clinical Practice
Improvement Activities (15% of MIPS Score)
17
* Max Score = 60
* PCMH Participation Guarantees 100%
CPIA Score
* Largely Undefined Currently
* Secretary shall give consideration to
practices <15 Eps, rural practices, and Eps
in underserved areas
90 Proposed activities – 9 Categories1. Expanded Practice Access
A. After hours hotline
B. Same-day appointments
2. Beneficiary Engagement A. Care Plans
B. Self-assessment training
C. shared decision-making, etc.)
3. Achieving Health Equity
4. Population Health Management 1. Qualified clinical data registry
2. Monitoring conditions
5. Patient Safety & Assessment1. Use of Surgical Checklists
2. Assessments related to maintaining Certifications
6. Emergency Preparedness & Response
7. Care Coordination
8. Participation in Advanced APM or Medical HomeModel
9. Integrated Behavioral Health

MIPS Category: Cost (10% 1st Yr MIPS Score)
18
1. Replaces cost component / resource use of VBMP.
2. Scored on Medicare claims = NO REPORTING.
3. 40 specific episode measures – among specialists.
4. Must see at least 20 patients in respective category.
5. Each cost measure max out at 10 points.

Score Summary Recap
19

Key Questions & Suggestions
20
Key Questions
1. Do you use CEHRT (Certified EHR Technology)?
2. Do you feel comfortable with your reporting process? (Proposed Full-year
reporting)
3. Do you know the measures your EHR is capable of reporting? (These metrics will
become public under MACRA) http://oncchpl.force.com/ehrcert
Key Suggestions
1. Stay familiar with CMS’ Core Measures as CMS & AHIP agree to harmonize
metrics
2. Improving your PQRS reporting process will pay dividends
3. 2017 Reporting Year will be 50 % PQRS & 25% ACI (Formerly Meaningful Use)
4. Download QRUR
5. Prepare to adjust workflows
6. Focus resources on specific PQRS measures. Identify workflow adjustments
7. Assess EHR/technological capability to comply

Strategic Plan
21
1. Short-run: Focus on Coding, PQRS Workflow, Care-Coordination
(CCM 99490), Chronic Care management, CPC+*, analytics
2. Long-Term: Learn via MIPS; Prepare APM contracts by expanding
to MA plans, then commercial FFV arrangements
3. Educate staff on initiatives
A. Many metrics involve strong communication & non-physician
reporting processes
B. Cultural change management in pursuit of Triple Aim
4. Establishing a CIN provides the architecture to strategically step
towards value-based payments to shift from MIPS to APMs & receive
further incentive-rewards
* CPC+ (Comprehensive Primary Care Plus) Regions are to be announced August 1, 2016

Sample Roadmap
22

Acronyms Reference Guide
23
• ACO – Accountable Care
Organization
• APM – Advanced Alternative
Payment Model
• CMS – Centers for Medicare &
Medicaid Services
• CPC+ – Comprehensive
Primary Care Plus
• EHR – Electronic Health
Record
• EP – Eligible Professional
• HHS – U.S. Department of
Health & Human Services
• MACRA – The Medicare Access
and CHIP Reauthorization Act of
2015
• MIPS – Merit-Based Incentive
Payment System
• MSSP – Medicare Shared
Savings Program
• PQRS – Physician Quality
Reporting System
• QPP – Quality Payment Program
• QRUR – Quality and Resource
Use Report
• VBPM – Value-Based Payment
Modifier

Summary: Merit Health QPP Plan
24
1. More education for members
2. Continue CIN objectives
3. Analytics implementation
4. More clinical workgroups
5. Analytics support
6. Partnership

25