lymphoid lesion 57 - ed.dent.psu.ac.th
TRANSCRIPT

8/17/2014
sompid/ lymphoid lesions 57 1
Dr. Sompid KintarakDepartment of Stomatology
Prince of Songkla University2557
Lymphoid lesions
Lymph node
http://www.dartmouth.edu
nhscience.lonestar.edu
Barnes Surgical Pathol of HN 3rd ed.
(adenoid)
Waldeyer ring
http://ethesis.helsinki.fi
www.pathology.washington.edu
emedicine.medscape.com
Foliate papillaeLymphadenopathy

8/17/2014
sompid/ lymphoid lesions 57 2
Reactive lymphoid hyperplasia
Barnes Surgical Pathol of HN 3rd ed.
Acute non-specific lymphadenitis
� Acute inflammatory response in a lymph node, normally associated with reactive changes in the follicles
� Cervical region: due to microbial drainage from infections of the head and neck region e.g. teeth or tonsils
� Axillary or inguinal regions: secondary to infections in the extremities
� Mesenteric lymph nodes: draining acute appendicitis
Acute non-specific lymphadenitis
� Macroscopic findings� swollen, gray-red, engorged
� Microscopic findings� prominent lymphoid follicles with large germinal centers� sinus dilation and filled with neutrophils, histiocytes, and a
moderate admixture of red cells� suppurative mass in follicles, within sinus
� Clinical findings� enlarged nodes due to cellular infiltration and edema
� tender due to capsular distention� redness of overlying skin
Chronic non-specific lymphadenitis
� Chronic immunologic reactions can produce several different morphologic alterations, depending on the underlying stimulus
� Morphology:� Reactive follicular lymphoid hyperplasia� Reactive paracortical lymphoid hyperplasia
� Sinus histiocytosis
� Clinical: enlarged lymph node, not tender
Reactive follicular lymphoid hyperplasia
� Increase in size and number of secondary lymphoid follicles
� Caused by stimuli that activate humoralimmune response
� Specific causes: � rheumatoid arthritis� toxoplasmosis
� early stage of HIV infection� cat scratch disease� cytomegalovirus lymphadenitis in immunocompetent hosts
� primary infection by Epstein-Barr virus (EBV)
library.med.utah.edu
Hyperplastic (Inflamed) Submandibular Lymph Node
© Photos: Dr. Charles Halstead, Virginia

8/17/2014
sompid/ lymphoid lesions 57 3
#46 Lesion: Hyperplastic Buccinator Lymph Node Prevalence (# Lesions/1,000) = 0.1 for Males, 0.1 for Females, 0.1 Total
© Photo: Dr. Jerry Bouquot, The Maxillofacial Center, Morgantown, West Virginia
Buccal Mucosa
Reactive paracortical lymphoid hyperplasia
� expansion of the paracortexbetween reactive or atrophic lymphoid follicles
� Characterized by reactive changeswithin the T-cell regions of the lymph node
� Caused by stimuli that trigger cellular immune responses� Causes:
� drugs (esp. dilantin)
� acute viral infection, particularly infectious mononucleosis, following vaccination against certain viral disease
Barnes Surgical Pathol of HN 3rd ed.
Sinus histiocytosis
� expansion of the sinuses by bland-looking histiocytes in the sinuses� distention and prominence of the lymphatic sinusoids
� the sinuses are filled with histiocytes� the endothelial cells are often grossly enlarged
� Nonspecific but prominent in lymph nodes draining cancer� A rare cause of cervical lymphadenopathy
pleiad.umdnj.edu webpathology.com
Sinus histiocytosis with massive lymphadenopathy (Rosai-Dorfman disease)
� Rare
� most cases resolve spontaneously
� marked capsular fibrosis, the sinuses are filled with large histiocytes; some have engulfed lymphocytes (emperipolesis)
� there is reactive plasmacytosis
pathologyoutlines.com ipath-network.com
Reactive lymphoid hyperplasia of extranodal sites in the head and neck
www.anatomyatlases.org
� Reactive lymphoid hyperplasia of the lingual tonsil (foliate papilla)

8/17/2014
sompid/ lymphoid lesions 57 4
� Lymphoid hyperplasia� Usually <1 cm in diameter� Posterior lateral tongue
(usually bilateral & symmetrical)
� Posterior hard palate
Angiofollicular lymphoid hyperplasia (Castleman’s disease)
� Rare condition, usually affects thorax� 15-20% of cases causes a cervical mass resembling a
lymphoma� unknown cause� Microscopy:
� Hyperplasia of lymphoid follicles
� Concentrically packed lymphocytes surround a vessel with thickened endothelium
� Highly vascular interfollicular tissue� Hyaline vascular type (90%) vs plasma cell type
Angiofollicular lymphoid hyperplasia (Castleman disease)
� Hyaline-vascular type: 90% of cases� young adults� asymptomatic, localized mass, enlarged cervical LN
� abnormal hyaline vascular follicles� hypervascular interfollicular zone� lack of nodal sinuses
� Plasma cell type:� associated with fever, weight loss, skin rash
� early loss of red blood cells (hemolytic anemia)� hypergammaglobulinemia
� commonly abdominal LN� reactive lymphoid follicles, sheet of mature plasma cells
between the follicles
Angiofollicular lymphoid hyperplasia (Castleman disease)
� Multicentric or generalized Castleman disease:� multiple peripheral nodes involvement with systemic symptoms� hepatosplenomegaly
� associated with HIV infection, HHV-8, overproduction of IL-6
� Management: surgery / high dose corticosteroids� Lymphomatous change is rare� Kaposi sarcoma in patients with the acquired immune deficiency
syndrome
webpathology.com
www.pathologyoutlines.com
Angiofollicular lymphoid hyperplasia (Castlemandisease)
Kimura disease � Rare in the West but common in China, Japan, and
Singapore� a mass forming chronic inflammatory condition of
unknown etiology, frequently involving the soft tissues, salivary glands (parotid, submandibular), cervical LNs, ocular adnexa in the HN region
� form deeper masses rather than mucosal nodules� young to middle-aged males� eosinophilia condition and high serum IgE� surgery may not be required except for cosmetic or
diagnostic reasons

8/17/2014
sompid/ lymphoid lesions 57 5
www.webpathology.com/image
www.scielo.br/scielo.php
Dr. Eiichiro Kimura
www.ispub.com/journal
Epithelioid hemangioma(Angiolymphoid hyperplasia with eosinophilia)
� Age 20-40 years; F > M� reactive process > neoplasm� affected skin of the head and neck region� subcutaneous lesions first appear as dull red pruritic
plaques� oral lesions (occasional) may resemble pyogenic
granuloma or may ulcerate� Microscopy:
� vascular proliferation with histiocytoid endothelial cells and stromal inflammatory reaction
� usually not associated with a heavy lymphoid infiltrate
dermatology.cdlib.org
ades.tmu.edu.tw
www.histopathology-india.net/ALHE.htm
� Angiolymphoidhyperplasia with eosinophilia
Drug-associated Lymphadenopathy
� Phenytoin-associated lymphadenopathy� can develop within a few weeks or months, but
more frequently after long-term treatment� not associated with serum-sickness-like
symptoms of fever, rashes, joint pain� cervical LNs are frequently first affected, then
becomes widespread
� Microscopic changes can closely mimic Hodgkin lymphoma
Oral lymphoepithelial cyst� Develops within a benign lymphoid aggregate or
accessary tonsil of oral or pharyngeal mucosa� Clinical presentation:
� yellow to white nodule� asymptomatic, slow growing
� overlying mucosa intact, smooth� most common in floor of mouth, followed by ventral tongue and
posterior lateral tongue
� Microscopy: lymphoid tissue with germinal centers surrounding true cyst lumen filled with epithelial debris
� Clinical DDX: lipoma, minor salivary gland neoplasm or sialolith, mucocele
� No treatment needed unless in traumatized area

8/17/2014
sompid/ lymphoid lesions 57 6
Benign lymphoepithelial lesion (myoepithelial sialadenitis)
� Microscopic features of lymphocytic infiltrate with an associated epimyoepithelial island
� Clinical features:� mostly develop as a component of Sjögren’s
syndrome (bilateral lesions): women� those not associated with Sjögren’s syndrome are
usually unilateral� may occur in association with other salivary gland
pathologic conditions e.g. sialoliths, benign or malignant epithelial tumors
Benign lymphoepithelial lesion (myoepithelial sialadenitis)
� Clinical features:� most often develops in adults, mean age 50 y� female (60% to 80% of cases)� parotid glands (85%), submandibular glands, minor
glands� usually appears as firm, diffused swelling of the
affected gland� asymptomatic or associated with mild pain
Benign lymphoepithelial lesion (myoepithelial sialadenitis)
� Histopathologic features:� a heavy lymphocytic infiltrate associated with the
destruction of the salivary acini� germinal centers may or may not be seen� ductal cells and surrounding myoepithelial cells
become hyperplastic, forming ‘epimyoepithelialislands’ throughout the lymphoid proliferation
www.brown.edu/Courses/Digital_Pa...lel.html
www.nature.com/modpathol/journal...2f1.html
Benign lymphoepithelial lesion (myoepithelial sialadenitis)
� Treatment and prognosis:� surgical removal with good prognosis in most cases� increased risk for lymphoma, either within the affected
gland or in an extrasalivary site (uncertain risk but one study showed the risk in patients with Sjögrensyndrome to be ~44 times greater than expected in general population – Kassan, et al. Ann Intern Med. 1978 Dec;89(6):888-92.
○ Extranodal marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue (MALT lymphoma)
Benign lymphoepithelial lesion (myoepithelial sialadenitis)
� Treatment and prognosis: (continue)� a rare malignant counterpart of this lesion: malignant
lymphoepithelial lesion or lymphoepithelial carcinoma○ poorly differentiated salivary carcinoma with a
prominent lymphoid stroma○ most cases have occured in Inuits (Eskimos) and
Asians and appear to have arisen de novo as carcinomas
○ Epstein-Barr virus is the possible causative agent (not definite proof)
○ guarded prognosis (Asian patients have had a better survival rate)

8/17/2014
sompid/ lymphoid lesions 57 7
www.forpath.org/0201/html/case_9_10.htm
www.pathologyoutlines.com/lungtumor.html
Low-grade marginal zone B cell lymphoma of MALT
Hematolymphoid neoplasia� Hodgkin lymphoma� Non-Hodgkin lymphoma (more common)
Hematolymphoid neoplasia
� The most common hematolymphoid neoplasm in the HN region are � diffuse large B-cell lymphoma (DLBCL), follicular
lymphoma, classical Hodgkin lymphoma for LNs� DLBCL, extranodal marginal zone lymphoma of
mucosa-associated lymphoid tissue (MALT lymphoma), extranodal NK/Tcell lymphoma, and extramedullary plasmacytoma for extranodal sites
� mantle cell lymphoma of extranodal sites� Burkitt lymphoma of the jaw in children of central
Africa, and the sporadic form can affect the tonsils and lymph nodes of children and young adults
Hematolymphoid neoplasia
� Etiology: � Etiology of most types is unknown� Chromosomal translocations and oncogenes� Inherited genetic factors� Immunosuppression: posttransplant lymphoproliferative
disorder (PTLD), HIV/AIDS� Viruses: HTLV-1, EBV, KSHV/HHV-8� Environmental agents� Iatrogenic factors Regezi’s Oral Pathology. 6th ed.

8/17/2014
sompid/ lymphoid lesions 57 8
Hodgkin lymphoma
� Nodular lymphocyte-predominant Hodgkin lymphoma
� Classical Hodgkin lymphoma:� Nodular sclerosis classical Hodgkin lymphoma� Mixed cellularity classical Hodgkin lymphoma� Lymphocyte-rich classical Hodgkin lymphoma� Lymphocyte depleted classical Hodgkin lymphoma
Classical Hodgkin lymphoma
� predominantly a nodal-based disease (75% of cases) � mediastinal, supraclavicular, cervical LNs� Males, bimodal age distribution: 15-35 and >50 years� persistent enlarging, non-tender, discrete mass or
masses in one LN region� a better prognosis if no systemic signs & symptoms
(fever, night sweat, and weight loss)� characterized by neoplastic Reed–Sternberg cells and
their variants scattered in an appropriate inflammatory background
� ~40% of cases of classical Hodgkin lymphoma are associated with EBV
www.healthoma.com
www.wgabinecie.pl
Hodgkin’s lymphoma� CD45-, CD30+, CD15+/-
library.med.utah.edu
www.pathconsultddx.com
� Reed-sternberg cells and variants
Nodular lymphocyte-predominant Hodgkin lymphoma� Rare B-cell neoplasm� usually children to middle-aged adults, with marked
male predominance� most patients present with solitary enlarged lymph node
in the cervical, axillary, or inguinal region (stage I/II disease)
� large neoplastic cells (lymphocytic and histiocytic cells or L&H cells) have been nicknamed ‘‘popcorn cells’’ because of the characteristic lobulation of the nuclei with multiple deep notches.
� Large cells: CD45+, CD20+, CD30-, CD15-, EBV-
www.pathconsultddx.com
� Popcorn-like L&H cell
www.webpathology.com

8/17/2014
sompid/ lymphoid lesions 57 9
2008 WHO classification of lymphoma and histiocytic/dentritic cell tumors
� Precursor lymphoid cell neoplasms� B-lymphoblastic leukemia/lymphoma� T-lymphoblastic leukemia/lymphoma
� Mature B-cell neoplasms� Chronic lymphocytic leukemia/small lymphocytic lymphoma� B-cell prolymphocytic leukemia� Lymphoplasmacytic lymphoma� Splenic B-cell marginal zone lymphoma� Splenic lymphoma-leukemia, unclassifiable� Hairy cell leukemia� Plasmacytoma� Extranodal marginal zone lymphoma of MALT (MALT lymphoma)� Nodal marginal zone lymphoma� Follicular lymphoma� Primary cutaneous follicle center lymphoma� Mantle cell lymphoma
2008 WHO classification of lymphoma and histiocytic/dentritic cell tumors
� Mature B-cell neoplasms� Diffuse large B-cell lymphoma (DLBCL), not otherwise specified� DLBCL, distinct subtypes:
○ Primary mediastinal (thymic) large B-cell lymphoma○ Intravascular large B-cell lymphoma○ Primary effusion lymphoma○ T-cell/histiocyte-rich large B-cell lymphoma○ Plasmablastic lymphoma○ ALK-positive large B-cell lymphoma○ EBV+ diffuse large B-cell lymphoma of the elderly○ DLBCL associated with chronic inflammation○ Primary DLBCL of the central nervous system○ Primary cutaneous DLBCL, leg-type○ Large B-cell lymphoma arising in HHV8-associated multicentric
Castleman disease
2008 WHO classification of lymphoma and histiocytic/dentritic cell tumors
� Mature B-cell neoplasms� Lymphomatoid granulomatosis
� Burkitt lymphoma� B-cell lymphoma, unclassifiable, with features intermediate between
DLBCL and Burkitt lymphoma� B-cell lymphoma, unclassifiable, with features intermediate between
DLBCL and classical Hodgkin lymphoma
2008 WHO classification of lymphoma and histiocytic/dentritic cell tumors
� Mature T-cell and NK-cell neoplasms� T-cell prolymphocytic leukemia� T-cell large granular lymphocytic leukemia� Adult T-cell leukemia/lymphoma� Aggressive NK-cell leukemia� Chronic lymphoproliferative disorder of NK cells� EBV+ T-cell lymphoproliferative disease of childhood
○ Systemic EBV+ T-cell lymphoproliferative disease of childhood○ Hydroa vacciniforme-like lymphoma
� Extranodal NK/T-cell lymphoma, nasal type � Enteropathy-associated T-cell lymphoma � Hepatosplenic T-cell lymphoma � Angioimmunoblastic T-cell lymphoma � Peripheral T-cell lymphoma, not otherwise specified
2008 WHO classification of lymphoma and histiocytic/dentritic cell tumors
� Mature T-cell and NK-cell neoplasms� Anaplastic large cell lymphoma, ALK+� Anaplastic large cell lymphoma, ALK-� Mycosis fungoides/ Sézary syndrome � Subcutaneous panniculitis-like T-cell lymphoma � Primary cutaneous CD30-positive T-cell lymphoproliferative disorders
○ Lymphomatoid papulosis○ Primary cutaneous anaplastic large cell lymphoma
� Primary cutaneous CD8+ aggressive epidermotropic cytotoxic T-cell lymphoma
� Primary cutaneous γδT-cell lymphoma� Primary cutaneous CD4+ small/medium T-cell lymphoma
2008 WHO classification of lymphoma and histiocytic/dentritic cell tumors� Immunodeficiency-associated lymphoproliferative disorders
� Lymphoproliferative diseases associated with primary immune disorders� HIV-related lymphomas� Posttransplant lymphoproliferative disorders� Methotrexate-associated lymphoproliferative disorders
� Histiocytic and dendritic cell neoplasms� Histiocytic sarcoma� Langerhans cell histiocytosis� Langerhans cell sarcoma� Follicular dendritic cell sarcoma� Interdigitating dendritic cell sarcoma� Indeterminate dendritic cell tumor� Fibroblastic reticular cell tumor� Disseminated juvenile xanthogranuloma� Blastic plasmacytoid dendritic cell neoplasm (formerly ‘‘blastic NK-cell
lymphoma’’)

8/17/2014
sompid/ lymphoid lesions 57 10
Non-Hodgkin’s lymphoma
� MALT lymphoma� Diffuse large B-cell lymphoma� Burkitt lymphoma
Non-Hodgkin lymphoma� relatively common in head & neck region� most common in middle-aged and older� non-tender, diffuse swelling with boggy consistency or
mass of reddish blue tissue with ulceration, pain� paresthesia particularly with a mandibular lesion (numb
chin syndrome)� initial presentation in oral cavity is uncommon (2%)� may rise within LNs or extranodal in soft tissue:
� Waldeyer ring, buccal vestibule, posterior hard palate, soft palate, gingiva, tongue
� Ill-defined radiolucency in bone, loss of lamina dura, uniform widening PDL space, displaced teeth, malocclusion and/or exfoliation
Lymphoma
MALT lymphoma
� Extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue type
� accounts for 8% of all non-Hodgkin lymphomas� an indolent lymphoma � occurs in various mucosal and extranodal sites� most commonly involved salivary gland, thyroid gland,
and ocular adnexa� most patients have early stage disease (stage I/II) at
presentation
Diffuse large B-cell lymphoma
� a rapidly growing neck mass (lymph node), but 30% of patients present with extranodal disease and 71% have extranodal involvement during the course of disease
� about half of the patients have stage I/II disease� about 50% of cases express BCL2 protein� an aggressive but potentially curable disease, usually
treated by multiagent chemotherapy together with anti-CD20 (Rituximab)
� relatively common in head & neck region
Neville’s Oral Pathology. 3rd ed.
NHL of the palateRegezi’s Oral Pathology. 6th ed.

8/17/2014
sompid/ lymphoid lesions 57 11
� Diffuse large B-cell lymphoma - spleen
Robbin’s Pathology. 8th ed.
LCA
CD20CD3
Diffuse large B cell lymphoma
Burkitt’s lymphoma
� Highly aggressive B-cell lymphoma � Genetic mutations: C-MYC, p53 � Three forms:
� an endemic type in Africa� a sporadic form occurring in North America and Europe
� a form associated with immunodeficiency
� EBV associated (strong with African Burkitt)� Jaw involvement is characteristic of endemic BL; up to
50% of those afflicted have lesions of the maxilla or mandible
Burkitt’s lymphoma
� Children with peak prevalence ~ 7 y, male� Maxilla > mandible (2:1): posterior segments� Jaw involvement related to the age of patients� X-ray: ill-defined bone destruction
Neville’s Oral Pathology. 3rd ed.
Histopathology: � diffuse infiltration by monotonous
medium-sized cells with a starry-sky pattern
� tumor cells have round or molded nuclei, clumped chromatin, and multiple nucleoli
� numerous mitoses� almost 100% of tumor cells are in
reprication process� Over expression of c-myc resulted from
t(8;14)Treatment:� Death within 4-6 m if not treated� Intensive, multiagent chemotherapeutic
protocols � event-free survival rate 3 to 5 y after treatment ~ 85% to 95% with stage I or II disease, and 75% to 85% with stage III and IV
CD20CD3
8/17/2014
sompid/ lymphoid lesions 57 12
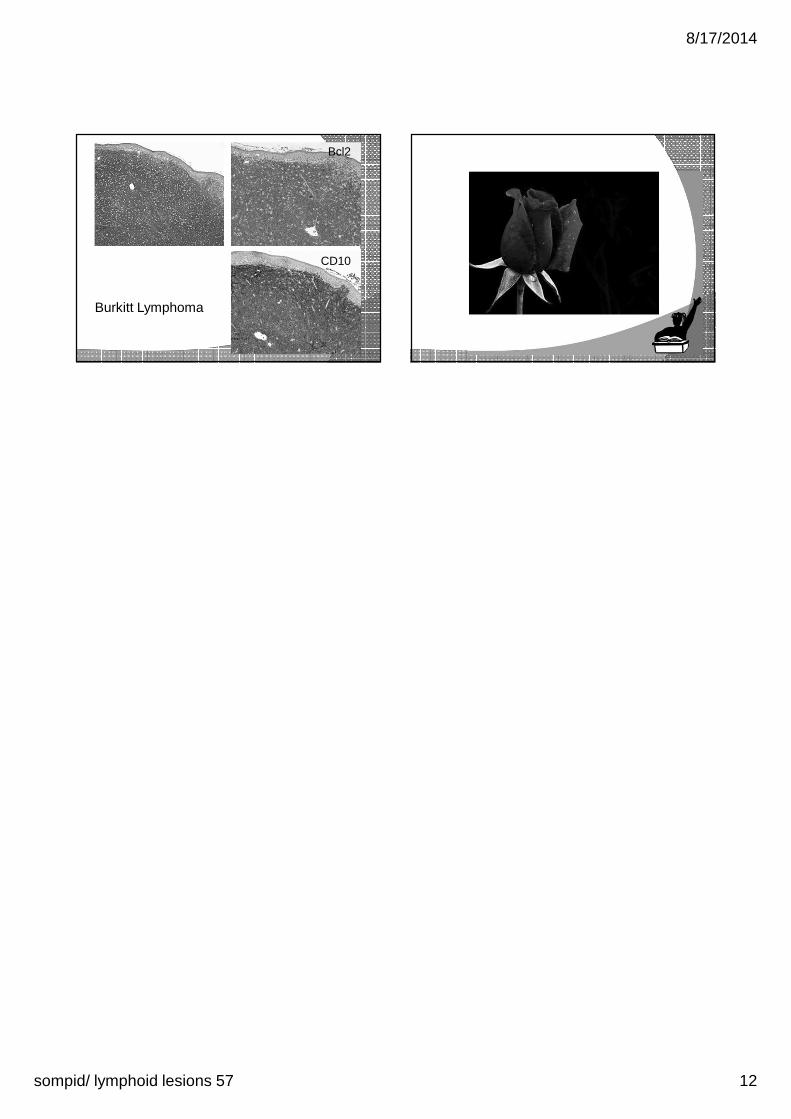
CD10
Bcl2
Burkitt Lymphoma