lymphocyte cytotoxicity: a possible in-vitro test for contact dermatitis
TRANSCRIPT
75
positive material was not extracted with cold acetonebut was almost completely extracted with hot acetone.Both the luxol fast blue and the o.T.A.N. stains con-firm this conclusion. The negative o.T.A.N./sodium-hydroxide reaction indicates that sphingomyelin isnot the major phospholipid. The substance is not aglycoprotein because the amount of sialic acid wasnegligible as ascertained by the 1+ alcian bluereaction. Since both the periodic-acid/Schiff andphospholipid reactions are intensely positive, we
conclude that the histiocytic cytoplasm contains a
glycophospholipid complex.Discussion
The major clinical manifestations of the syndromeof the sea-blue histiocyte have been summarised bySilverstein et al.l The pulmonary findings as seen inour propositus have not been emphasised, and thefrequency of such findings is not known. Cogan andFederman’s 6 patient had streaky densities in both
lung fields over at least a 7-year period and the secondpatient of Sawitsky et al. had a persistent right-upper-lobe infiltrate. The pulmonary infiltrate in ourpatient is not dissimilar to that seen in patients withhistiocytosis X. The histologic nature of the lunglesion remains to be determined.With so few bone-marrow examinations in patient’s
relatives, it is not surprising that the genetic aspectsof the disorder have remained unresolved, especiallysince abnormal histiocytes can be found in the absenceof splenomegaly:
Few siblings have been investigated. Two siblingshad normal marrow, and of the six siblings whosespleen size was recorded none has had splenomegaly.Including our family, five males and eight femaleshave been recorded, thus suggesting that it is notX-linked. From our family study it seems most
likely that the sea-blue histiocyte disease is inheritedas an autosomal recessive. The normal bone-marrowsof the parents of our siblings together with the findingof normal marrows in both parents of one case andin the father of another,2 supports the recessive natureof the inheritance pattern. Confirmation of thisconclusion must await further family studies.The exact nature of the disease needs to be deter-
mined by further chemical analysis of the substance(s)accumulating in the histiocytes and identification ofthe presumed enzyme defect. From the data availablewe postulate that the disorder is one of the lipid-storage diseases. Clinically, it is very similar to
Gaucher’s disease, with a variable onset of spleno-megaly. The lipid-filled histiocytes have been foundin splenic tissue of all patients who had such histo-logical examination.1-3,5,6,8 The liver findings have
been less consistent; foam cells were identified inthree 1,4,10 but not in four others.2,5,9
If one postulates an enzyme defect in the degrada-tive pathway of lipids, the substrate in front of theblock would accumulate and be stored in histiocytes.This could account for the variable number of
granules in the histiocytes and perhaps the inconsistentfindings in liver-biopsy specimens. It might also
explain the absence of splenomegaly in one of ourpatients. It is of interest that the ages of the reportedcases vary from 21/2 months to 61 years but the ageat which splenomegaly developed is not known. Thisis analogous to the variable age of onset of clinicalmanifestations of other lipid-storage diseases.
Kattlove et al.12 have questioned the existence ofthe sea-blue histiocyte syndrome as a specific entity,suggesting instead that these histiocytes are secondaryto increased blood destruction. The marrow findingsin the sibling of our patient discounts this hypothesissince she was clinically normal with no history orevidence of chronic disease or organomegaly. We believethis is a distinct genetically determined disorder.
Requests for reprints should be addressed to B. J.REFERENCES
1. Silverstein, M. N., Ellefson, R. D., Ahern, E. J. New Engl. J. Med.1970, 282, 1.
2. Sawitsky, A., Hyman, G. A., Hyman, J. B. Blood, 1954, 9, 977.3. Marshall, A. H. E., Adams, C. W. M. J. Path. Bact. 1958, 76, 159.4. Malinin, T. I. Blood, 1961, 17, 675.5. Silverstein, M. N., Young, D. G., ReMine, W. H. Archs intern.
Med. 1964, 114, 251.6. Cogan, D. G., Federman, D. D. Archs Ophthal. 1964, 71, 489.7. Holland, P., Hug, G., Schubert, W. K. Am. J. Dis. Child. 1965,
110, 117.8. Thompson, I. L., Moloney, W. C. Blood, 1966, 27, 49.9. Rosner, F., Kagen, M. D., Dana, M. New Engl. J. Med. 1970,
282, 1100.10. Saidi, P., Azizi, S. P., Sarlati, R., Sayar, N. Blood, 1970, 35, 533.11. Lancet, 1970, i, 459.12. Kattlove, H. E., Gaynor, E., Spivack, M., Gottfried, E. L. New
Engl. J. Med. 1970, 282, 630.
Preliminary Communications
LYMPHOCYTE CYTOTOXICITY:
A POSSIBLE IN-VITRO TEST FOR
CONTACT DERMATITIS
J. DELESCLUSE J. L. TURKDepartment of Immunology, Institute of Dermatology,
St. John’s Hospital for Diseases of the Skin, London E.9
Summary Lymphocytes from guineapigs withcontact sensitivity to dinitrofluoro-
benzene (D.N.F.B.) damaged target cells (chicken redblood-cells) conjugated with D.N.F.B. This pheno-menon is shown only with peripheral circulatinglymphocytes and not with lymph-node lymphocytes.Circulating lymphocytes cytotoxic to carrier cellscoated with the hapten were present in the circulationfrom the twelfth day after one contact with D.N.F.B.
INTRODUCTION
CONTACT dermatitis is an important cause ofindustrial morbidity. Sensitivity to simple chemicalcontact agents has previously been demonstrable onlyby in-vivo patch testing. No technique for demon-strating cell-mediated immunity in vitro has proved
76
applicable to contact-sensitivity tests in man. Theseinclude lymphoblastic transformation by specificantigen and inhibition of migration of macrophagesin vitro. One in-vitro correlate of cell-mediatedimmunity that has not yet been studied is the cytotoxiceffect of specifically sensitised lymphocytes for targetcells.1,2 The introduction of 51Cr-labelled chicken
erythrocytes (R.B.c.s) 3 as carrier target cells to
demonstrate the cytotoxicity of lymphocytes sensi-tised to tuberculin suggested that this approachmight be applicable to the problem of trying to findan in-vitro test for contact sensitivity.
MATERIALS AND METHODS
Contact sensitivity was induced in guineapigs byepicutaneous application of a 10% solution of D.N.F.B. inbenzene, acetone, and olive oil (2/1/1) to the back of theneck and ears. 5-29 days after sensitisation (1 day beforethe experiment) the animals were tested on the flank witha 0-25% solution of D.N.F.B. in acetone/olive-oil (4/1) andexamined after 24 hours.4
Lymph-node lymphocytes were obtained from the
lymph-nodes draining the sensitised regions (axillary andauricular), washed twice in Eagle’s minimal essentialmedium (M.E.M.) (Burroughs Wellcome) supplementedwith penicillin and streptomycin, and 15% heat-inactivatedfetal calf serum. Blood lymphocytes were obtained by thedextran-sedimentation method.5 The cells were washedtwice in M.E.M., supplemented with heat-inactivated fetalcalf serum.
Chicken R.B.C.S were obtained from blood drawn fromthe alar vein of a chicken. 5% suspension of chickenR.B.c.s was conjugated with D.N.F.B. (20 g. per ml.) in
phosphate-buffered saline solution pH 8 at 20°C for 1 hourwith continuous mixing. The cells were then washed fourtimes in Earle’s balanced-salt solution containing glycine(150 tig. per ml.) to remove excess D.N.F.B. Cells were alsoconjugated with 14C-labelled D.N.F.B. to demonstrate thatthey were adequately coated with the sensitiser. It wasfound that 0-03 .mole D.N.F.B. was conjugated to 107chicken R.B.C.S In all experiments, cells used as controlswere treated in the same way, except that D.N.F.B. wasomitted. Chicken R.B.c.s were then labelled with 51Cr.6Finally the cells were washed four times, and diluted inM.E.M. supplemented with antibiotics and 15% heat-inactivated fetal calf serum.
Cytotoxicity was determined as follows: 1 ml. of the
lymphocyte suspension (effector cells), containing 107 cellswas added to 0-4 ml. of the 51Cr-labelled chicken R.B.C.S(106 per ml.) (target cells) in roller tubes. 0-1 ml. of mediumwas added so that the total volume should be 1-5 ml. Themedium used throughout was M.E.M. supplemented withantibiotics and 15% heat-inactivated fetal calf serum.Before incubation at 37°C for 20-48 hours, the tubes weregassed with 90% air and 10% carbon dioxide. In each
experiment control tubes were included containing 51Cr-labelled chicken R.B.C.S without added lymphocytes, as acontrol. In these tubes 108 unlabelled cells were addedbefore incubation to avoid spontaneous release of the61Cr label. At the end of incubation, first the total radio-activity of every sample was counted in a well-type scin-tillation counter, then the tubes were centrifuged at 700gfor 20 minutes and 1 ml. of the cell-free supernatant wascarefully withdrawn and counted. The cytotoxicity wasexpressed as a percentage of the total radioactivity releasedinto the supernatant.
RESULTS
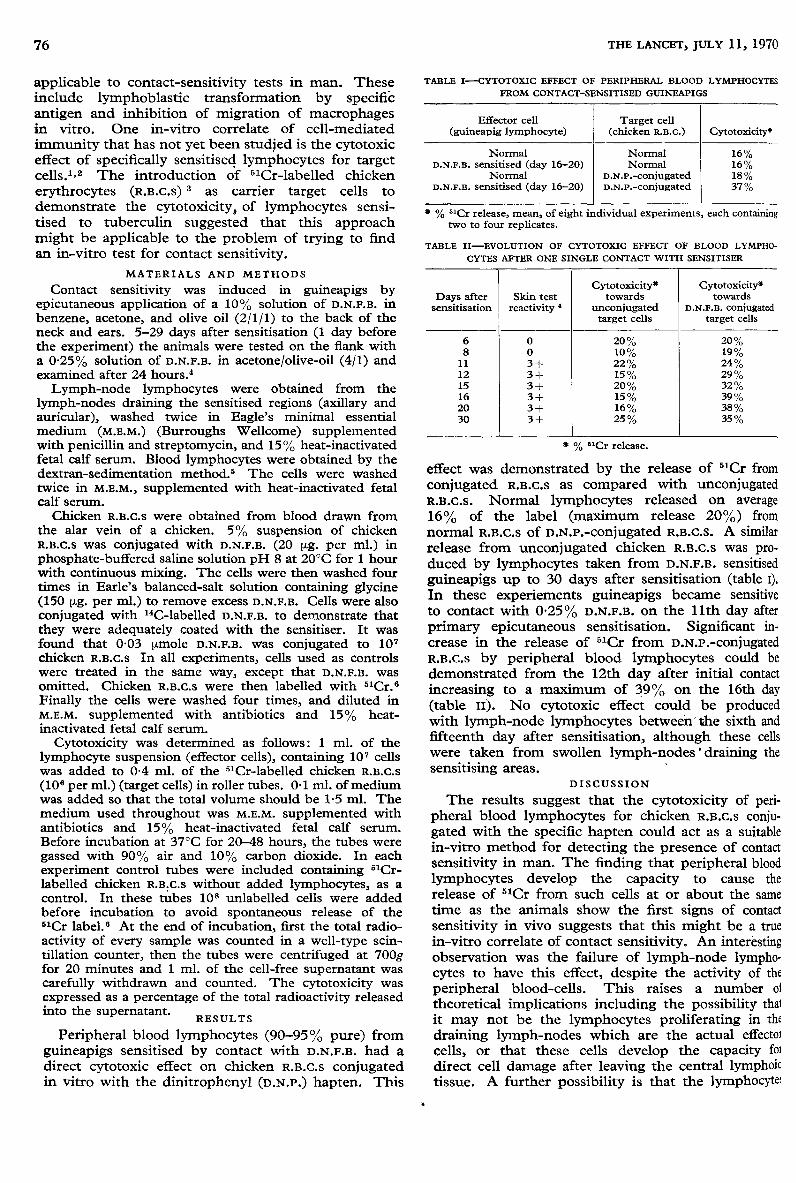
Peripheral blood lymphocytes (90-95% pure) fromguineapigs sensitised by contact with D.N.F.B. had adirect cytotoxic effect on chicken R.B.C.S conjugatedin vitro with the dinitrophenyl (D.N.P.) hapten. This
TABLE I--CYTOTOXIC EFFECT OF PERIPHERAL BLOOD LYMPHOCYTES
FROM CONTACT-SENSITISED GUINEAPIGS
* % 5’Cr release, mean, of eight individual experiments, each containingtwo to four replicates.
TABLE II-EVOLUTION OF CYTOTOXIC EFFECT OF BLOOD LYMPHO-
CYTES AFTER ONE SINGLE CONTACT WITH SENSITISER
’" % 6’Cr release.
effect was demonstrated by the release of 5’Cr fromconjugated R.B.c.s as compared with unconjugatedR.B.C.S. Normal lymphocytes released on average
16% of the label (maximum release 20%) fromnormal R.B.C.S of D.N.p.-conjugated R.B.c.S. A similarrelease from unconjugated chicken R.B.c.s was pro-duced by lymphocytes taken from D.N.F.B. sensitisedguineapigs up to 30 days after sensitisation (table i).In these experiements guineapigs became sensitiveto contact with 0-25% D.N.F.B. on the llth day afterprimary epicutaneous sensitisation. Significant in-crease in the release of 51Cr from D.N.P.-conjugatedR.B.c.s by peripheral blood lymphocytes could bedemonstrated from the 12th day after initial contactincreasing to a maximum of 39% on the 16th day(table 11). No cytotoxic effect could be producedwith lymph-node lymphocytes between the sixth andfifteenth day after sensitisation, although these cellswere taken from swollen lymph-nodes’ draining thesensitising areas.
’
DISCUSSION
The results suggest that the cytotoxicity of peri-pheral blood lymphocytes for chicken R.B.C.S conju-gated with the specific hapten could act as a suitablein-vitro method for detecting the presence of contactsensitivity in man. The finding that peripheral bloodlymphocytes develop the capacity to cause therelease of 5lCr from such cells at or about the sametime as the animals show the first signs of contactsensitivity in vivo suggests that this might be a truein-vitro correlate of contact sensitivity. An interestingobservation was the failure of lymph-node lympho-cytes to have this effect, despite the activity of theperipheral blood-cells. This raises a number oftheoretical implications including the possibility thatit may not be the lymphocytes proliferating in thedraining lymph-nodes which are the actual effector
cells, or that these cells develop the capacity for
direct cell damage after leaving the central lymphoidtissue. A further possibility is that the lymphocytes

77
which proliferate in the lymph-node under antigenstimulation need the cooperation of other cells alreadypresent in the peripheral blood to produce effectivecell damage. Further work is in progress to charac-terise the nature of this reaction in animals and to
apply these findings to the development of an in-vitrotest for contact sensitivity in man.We thank the Gillette Foundation and the Medical Research
Council for their financial support, and Dr. Edgar Pick, Dr.Gerald Levene, Dr. Darien Parker, and Dr. Jan Krejci for theirhelpful discussions.
Requests for reprints should be addressed to J. L. T.
REFERENCES
1. Govaerts, A. J. Immun. 1960, 85, 516.2. Perlmann, P., Holm, G. Adv. Immun. 1969, 11, 117.3. Perlmann, P., Perlmann, H., Wasserman, J., Packalen, T. L.
Int. Archs Allergy, 1970, 38, 204.4. Parker, D., Turk, J. L. ibid. 1970, 37, 440.5. DaGuillard, F., Richter, M. J. exp. Med. 1969, 130, 1187.6. Perlmann, P., Perlmann, H., Holm, G. Science, 1968, 160, 306.
HISTOCOMPATIBILITY TESTING FOR
LEUCOCYTE TRANSFUSION
ROBERT G. GRAW, JR.HARMON J. EYRE
IRA M. GOLDSTEIN
PAUL I. TERASAKI
Human Tumor Cell Biology Branch, and Medicine Branch,Leukemia Service, Chemotherapy, National Cancer Institute,
Bethesda, Maryland; and University of California,Los Angeles, California
Summary HL-A typing was done on elevendonors and twenty-eight recipients of
chronic-myelogenous-leukæmia leucocyte transfusionsin an attempt to clarify what relationship leucocyte-antigen compatibility has to the response to granulo-cyte transfusion. The degree of histocompatibilitybetween donor and recipient was correlated with per-centage recovery of leucocytes after transfusion.
INTRODUCTION
FOR many years leucocyte-replacement transfusiontherapy has been used without reference to leucocyte-antigen compatibility between donor and recipient.1,2 2These antigens are a major influence on the survival oftissue allografts; and, in alloimmunised recipients, are,responsible for most of the non-haemolytic febriletransfusion reactions associated with erythrocyte-compatible whole-blood transfusions.3 Alloimmunisa-tion to many of the histocompatibility antigens presenton leucocytes is common among potential recipients ofleucocyte transfusions since they are very likely to havehad multiple transfusions of random-donor blood
components. To see whether the degree of histo-
compatibility between donors and recipients correlateswith leucocyte-transfusion responses, we have typeddonor-recipient pairs in the HL-A series and examinedrecipients’ sera for preformed antileucocyte antibodies.
MATERIALS AND METHODS
Ninety-two patients with acute leukaemia were given 318transfusions of leucocytes obtained from twenty-fourdonors with chronic myelogenous leukaemia (C.M.L.). 99 ofthe transfusions were studied by typing lymphocytes fromeleven donors and twenty-eight recipients for 8-12 antigenspecificities comprising the HL-A system.4 The number ofantigen specificities on donor cells but not present in the
recipient was used as a measure of the degree of histo-compatibility between donor and recipient. Each recipient’sserum was studied for antileucocyte antibody against thedonor’s leucocytes using the lymphocytotoxicity cross-
match 4 and leucoagglutination technique.5 The percentrecovery of transfused leucocytes (w.B.C.s) in the recipients’circulation 1 hour after trasnfusion (% W.B.C. recovery) wasused to compare individual transfusion responses:
If the presence of preformed leucocyte antibodies inrecipients’ sera is ignored, the median 1-hour post-transfusion % W.B.c. recoveries were similar (5-5%)for each donor-recipient group whether mismatched by1, 2, or 3 HL-A antigen specificities (fig. 1). When thetransfusions administered to patients without detect-able leucocyte antibody were recorded separately(fig. 2) we noted a striking fall in % w.B.c. recoveryas the number of HL-A antigen mismatches increased,suggesting that the HL-A antigens may influence
leucocyte-transfusion response. The median transfusionrecoveries resulting from transfusions into patientswithout antibody ranged between 5-5% and 24%, witha median recovery of 15% for the entire group. Theseresults are not statistically significant.
DISCUSSION
Leucocyte transfusions have been considered to beuseful adjuncts in the therapy of infection associatedwith granulocy1openia,1,2,6 even though transfusion
responses have often been confusing and uninterpret-
Fig. 1-Leucocyte-transfusion response, measured as % W.B.C.recovery, for donor-recipient pairs typed for HL-A antigens;no reference to preformed leucocyte antibody."Matched donor-recipient " refers to donors who had no
HL-A antigen specificity not detected in the recipient." HL-A antigen group mismatch " refers to donors who had
1, 2, or 3 antigen specificities not found on the recipient’slymphocytes.
" Random donor CML Tx " refers to 219 C.M.L. transfusions
given to non-HL-A typed recipients.