lurasidone meeting - ds-pharma.co.jp
TRANSCRIPT

1
June 12, 2009
Dainippon Sumitomo Pharma Co., Ltd.
June 12, 2009
Dainippon Sumitomo Pharma Co., Ltd.
Lurasidone MeetingLurasidone Meeting

2
Lurasidone: Clinical Studies SummaryLurasidone: Clinical Studies Summary
Antony Loebel, MDVice President, Clinical DevelopmentDainippon Sumitomo Pharma America

3
Lurasidone Development Timeline
20082008 200920091990-19951990-1995 200720072002200220002000 20042004 20052005 20062006
First in Man
(Japan)
First in First in ManMan
(Japan)(Japan)
US Schizophrenia IND
US Schizophrenia US Schizophrenia IND IND
US Schizophrenia NDA
US Schizophrenia US Schizophrenia NDANDA
SchizophreniaPhase 3
SchizophreniaSchizophreniaPhase 3Phase 3
SchizophreniaPhase 2
SchizophreniaSchizophreniaPhase 2Phase 2
Schizophrenia Pre-NDA Meeting
Schizophrenia Schizophrenia PrePre--NDA NDA MeetingMeeting
Bipolar Depression Phase 3
Bipolar Bipolar Depression Phase 3Depression Phase 3
EOP 2 FDA Meeting
EOP 2 FDA EOP 2 FDA MeetingMeeting
Lurasidone Discovery
(Japan)
Lurasidone Lurasidone Discovery Discovery
(Japan)(Japan)
20102010 20112011
US Bipolar Depression
sNDA
US Bipolar US Bipolar Depression Depression
sNDAsNDA
MerckOutlicensed

4
Problems with Current Antipsychotic Agents
Lack of efficacy
EPS/akathisia
Prolactin increase
Metabolic syndrome• Weight gain• Lipid increase• Diabetes
QTc prolongation
Sedation
Poor functioning
Reduced adherence to treatment

5
ADA/APA Consensus Statement on Antipsychotic Drugs and Obesity and Diabetes
––+/-ziprasidone*
––+/-aripiprazole*
DD+ +quetiapine
DD+ +risperidone
+++ + +olanzapine
+++ + +clozapine
DyslipidemiaDiabetes RiskWeight GainDrug
+ = increased effect; - = no effect; D = discrepant results. *Newer drugs with limited long-term data.Diabetes Care/J Clin Psych, 2004 and others

6
Olanzapine (n=330) Risperidone (n=333)
Ziprasidone (n=183)Quetiapine (n=329)Perphenazine (n=257)
0.8
0.9
0.7
0.6
0.4
0.3
0.1
0.5
0.2
0.00 3 6 9 12 15 18
1.0
Time to Discontinuation for Any Cause (months)
Prop
ortio
n of
Pat
ient
sC
ontin
uing
Tre
atm
ent
CATIE Schizophrenia Study: Time to Discontinuation for Any Cause
Lieberman JA et al. N Engl J Med. 2005;353:1209-1223.

7
Psychiatrists Perceive the Greatest Unmet Needs in the Treatment of Schizophrenia and Bipolar Disorder to Involve Better/More Consistent Efficacy Balanced with Tolerable Side Effects
Less expensive medications (issue for 10-20% of patients)
Less expensive medications (issue for 30% of patients) Lower Cost
QD medicationsSimple regimen, maybe a combination of meds patients typically take in a single capsule
Simpler Administration
Fewer metabolic effectsLimited side effects
Better performance in terms of metabolic effects and weight gain (effects impact compliance)
Fewer Side Effects
More uniformly effective for depressed phaseDrugs that work alone to treat all stagesControl of agitation
Uniform effectiveness (balanced with side effect burden)Treatment of positive symptoms -violence, loss of self-controlSomething to enhance cognitive functioning of patients, improve intellectual capacityNew alternatives – “There are still a number of patients who are quite sick with available medications. We need new mechanisms, an increased arsenal.”
Better Efficacy
Bipolar DisorderSchizophreniaUnmet Needs
DSP, data on file, 2009

8
Receptor Binding Profiles:Lurasidone and Other Agents
26
>1000
67
38
10
2.1
34
3.3
Aripip
7
4.9
2.0
16
18
120
9.2
110
Cloz
7
210
9.0
350
310
320
340
200
Quet
2
>1000
510
400
6.0
8.5
0.3
3
Zip
19248α1Orthostatic hypotension, sedation
2101111α2cCognition
1106.60.505-HT7Mood/Cognition
27002606.85-HT1AMood/Cognition
7.6 >1000>1000ACh M1Impair cognition
3.83.5>1000 Histamine H1Impair cognition, sedation, weightgain
5.80.22.05-HT2AAntipsychotic/ Attenuate EPS
142.91.7D2Antipsychotic
OlanzRispLurasidoneBinding Affinities(Ki; nM)
Lurasidone data on file, 2008Bymaster,et al. Neuropsycopharmacology,1996;14:87-96 and others

9
Lurasidone Dose-Dependently Competes with [3H]SB-269970 Binding
5-HT7 Receptor Autoradiographyin Rat
Lurasidone 100 nM Lurasidone 1000 nM
ThHy
AmLurasidone 1 nM Lurasidone 10 nM
Am-AmygdalaHy-HypothalamusTh-ThalamusHi-Hippocampus
Total Non Specific
Hi

10

11
Lurasidone Reverses MK-801 Induced Learning & Memory Impairment
Inescapable shock
+Lurasidone
1 day later
1 day later
1 day later

12
Lurasidone Phase 2 Studies
DSM-IV schizophrenia, requiring hospitalization
6-week, randomized, double-blind,placebo-controlled
All studies involved US sites only
Primary end point: BPRS derived from PANSS (BPRSd)
Hospitalization required for 2-4 weeks

13
Study 006:PANSS Total Score (ITT-LOCF)
†p=0.06 *p≤0.05; **p=0.01 Ogasa et al. ICOSR 2003
-20
-18
-16
-14
-12
-10
-8
-6
-4
-2
00 1 2 3 4 5 6
WeeksM
ean
Cha
nge
from
Bas
elin
e
Placebo (n=49)
†
Lurasidone 40 mg (n=49)
** **
Lurasidone 120 mg (n=47)

14
-16
-14
-12
-10
-8
-6
-4
-2
00 1 2 3 4 5 6
WeeksM
ean
Cha
nge
from
Bas
elin
e
Study 196:PANSS Total Score (ITT-LOCF)
*
* *
*
*
**
Day 3
*p≤0.01Nakamura M et al. J Clin Psych, 2009
Placebo (n=90) Lurasidone 80 mg (n=90)

15J Clin Psychatry June 2, 2009, e1-e8

16
Depressive Symptom Change: Phase 2 Data
Anxiety Depression
PANSS Anxiety/Depression
MADRS
**
n=135n=135 n=135n=135 n=181n=181n=181n=181
-1.0
-0.5
0.0
Mea
n C
hang
e fr
om B
asel
ine
Placebo
*
n=83n=83 n=86n=86
-4
-3
-2
-1
0
Mea
n C
hang
e fr
om B
asel
ine
Studies 006, 196Studies 006, 196Studies 006, 196 Study 196Study 196Study 196
Baseline: Placebo 14.5, Lurasidone 14.2LOCF at end point*p<0.05 using ANCOVA
Lurasidone80mg

17
PANSS Cognitive Subscale
Nakamura M et al. J Clin Psych, 2009
Study 196
-0.5
-2.1
-2.5
-2
-1.5
-1
-0.5
0M
ean
Cha
nge
Placebo
Lurasidone
p = 0.0015
n=90n=90

18
Simpson Angus Scale (SAS):Pooled Phase 2 Studies*
0.230.04
1.24
-0.05
0.49
0.09
-0.5
0.0
0.5
1.0
1.5
2.0
2.5
Placebo Lurasidone20mg
Lurasidone40mg
Lurasidone80mg
Lurasidone120mg
Haloperidol10mg
Mea
n C
hang
e
n=209 n=71 n=114 n=159 n=48 n=72
*Studies 006, 049, 196SAS scored 0-5 on 10 items for max possible score of 50

19
Barnes Akathisia Rating Scale (BARS): Pooled Phase 2 Studies*
*Studies 006, 049, 196BAS scored 0-5 on Global Clinical Assessment of akathisia; maximum score= 5
0.160.31
0.58
0.12
-0.06-0.04
-0.5
0.0
0.5
1.0
1.5
2.0
Placebo Lurasidone20mg
Lurasidone40mg
Lurasidone80mg
Lurasidone120mg
Haloperidol10mg
Mea
n C
hang
e
n=210 n=71 n=114 n=160 n=48 n=72

20
Serum Prolactin:Pooled Phase 2 Studies*
-1.4
1.4
8.5
-2
0
2
4
6
8
10
Placebo Lurasidone Haloperidol
Med
ian
Cha
nge
(ng/
mL)
n=187n=187
n=62n=62n=353n=353
*Studies 006, 049, 196

21
CATIE Schizophrenia Study: Prolactin
-4.5
15.4
-9.3-6.1
0.4
-20.0
-10.0
0.0
10.0
20.0
Ziprasidone Risperidone Quetiapine
Olanzapine Perphenazine
Mea
n ch
ange
from
Bas
elin
e (n
g/dL
)
Ziprasidone Olanzapine
n=143n=143
n=262n=262
n=268n=268 n=286n=286 n=212
Lieberman JA et al. N Engl J Med 2005;353:1209-1223. 20.1 mg/dOlanzapine20.8 mg/dPerphenazine
543.4 mg/dQuetiapine3.9 mg/dRisperidone
112.8 mg/dZiprasidoneMean Modal Dose

22
Weight Gain:Pooled Phase 2 Studies*
0.16
0.46
0.100.0
0.5
1.0
1.5
2.0
Placebo Lurasidone Haloperidol
Mea
n C
hang
e (k
g)
n=208n=208 n=71n=71n=387n=387
*Studies 006, 049, 196

23
Plac
ebo
Molind
one
Zipra
sidon
eFlu
phen
azine
Halope
ridol
Risper
idone
Chlor
prom
azin
eSe
rtind
oleTh
iorida
zine
Olanza
pine
Cloza
pine
–3
–2
–1
0
1
2
3
4
5
6M
ean
Cha
nge
in B
ody
Wei
ght (
kg) Conventional Antipsychotics
Second-generation Antipsychotics
Estimated Mean Weight Gain at 10 Weeks with Antipsychotics
Allison DB et al. Am J Psychiatry. 1999;156:1686-1696

24
-30
-25
-20
-15
-10
-5
0Cholesterol HDL* LDL* Triglycerides
Mea
n C
hang
e (m
g/dL
)
Placebo Lurasidone
Lipid Profile:Pooled Phase 2 Studies#
n=192/381 n=78/76 n=72/70 n=192/381
#Studies 006, 049 and 196*Not measured in study 049 Fasting measures obtained per protocol

25
-18.1
-2.6
19.2
42.9
8.3
CATIE Schizophrenia Study:Triglycerides
Ziprasidone Risperidone Quetiapine Olanzapine Perphenazine
n=143n=143
n=262 n=268n=268 n=286n=286 n=212n=212
20.8 mg/dPerphenazine20.1 mg/dOlanzapine
543.4 mg/dQuetiapine3.9 mg/dRisperidone
112.8 mg/dZiprasidoneMean Modal Dose
Lieberman JA et al. N Engl J Med 2005;353:1209-1223
Mean Change from Baseline (mg/dL)

26
A Randomized, Double-Blind Study Comparing 3 Fixed Doses of Lurasidone to Placebo in Patients With Acute Schizophrenia: A Phase 3 Trial
A Randomized, Double-Blind Study Comparing 3 Fixed Doses of Lurasidone to Placebo in Patients With Acute Schizophrenia: A Phase 3 Trial
Study D1050229 (PEARL 1)

27
PEARL 1:Study Design
Open-Label Extension PhaseDouble-Blind Phase
6 weeks 22 months
Scre
enin
gSc
reen
ing
Scre
enin
g
Bas
elin
eB
asel
ine
Bas
elin
eLurasidone 40 mg/d
n=120Lurasidone 40 mg/dLurasidone 40 mg/d
n=120n=120
Placebon=120
PlaceboPlacebon=120n=120
Lurasidone 80 mg/dn=120
Lurasidone 80 mg/dLurasidone 80 mg/dn=120n=120
Lurasidone 120 mg/dn=120
Lurasidone 120 mg/dLurasidone 120 mg/dn=120n=120
Lurasidone 40-120 mg/dLurasidone 40Lurasidone 40--120 mg/d120 mg/d

28
Key Entry Criteria
DSM-IV schizophrenia• Acute exacerbation ≤2 months• ≤2 weeks hospitalization prior to screening• No significant improvement between screening and baseline
Age 18-75 yrs
Baseline Assessments• PANSS score ≥80; ≥4 (moderate) on at least 2 positive
psychotic items • CGI-S ≥4
Medically stable
Not treatment resistant• Based on failure to respond to ≥2 prior antipsychotic trials

29
Efficacy Endpoints
Primary endpoint• Baseline to 6-week/endpoint change in PANSS
Total Score, using mixed model repeated measures (MMRM) analysis adjusted by Hommel procedure for multiple comparisons (dose/endpoints)
• ANCOVA LOCF used for sensitivity analysis
Key secondary endpoint• CGI-S change

30
PANSS Total (MMRM)
-25
-20
-15
-10
-5
0Baseline Day 4 Wk 1 Wk 2 Wk 3 Wk 4 Wk 5
Wk 6Endpoint
Placebo (n=124) 40 mg Lurasidone (n=118) 80 mg Lurasidone (n=123) 120 mg Lurasidone (n=121)
LS M
ean
Cha
nge
from
Bas
elin
e
*0.031
*0.018
*0.017 *
0.010 *0.011
*
*

31
PEARL 1:PANSS Total ≥30% Responder Analysis
38%
50%52%46%
0%
10%
20%
30%
40%
50%
60%
70%
Lur 40 mg/d Lur 80 mg/d Lur 120 mg/d Placebo
Perc
enta
ge o
f Sub
ject
s
n=122 n=119 n=124 n=124
*p=0.058
†P=0.028

32
-30
-25
-20
-15
-10
-5
0
PANSS Total:Per Protocol Population
LS M
ean
Cha
nge
(LO
CF)
n=19 n=26 n=13 n=29
n=100 n=89 n=94 n=102
* *p=0.004
Lur 40 mg Lur 80 mg PlaceboLur 120 mg
p=0.032

33
PANSS Positive Subscale (MMRM)
-10
-5
0Baseline Day 4 Wk 1 Wk 2 Wk 3 Wk 4 Wk 5
Wk 6Endpoint
Placebo (n=124) 40 mg Lurasidone (n=118) 80 mg Lurasidone (n=123) 120 mg Lurasidone (n=121)
LS M
ean
Cha
nge
from
Bas
elin
e
*
* **
* *** **
* *** **
* **
* *** **
* *** ** *
* ** *
*p<0.05**p<0.01***p<0.001

34
CGI-S (MMRM)
-1.5
-1.2
-0.9
-0.6
-0.3
0.0Baseline Day 4 Wk 1 Wk 2 Wk 3 Wk 4 Wk 5
Wk 6Endpoint
Placebo (n=124) 40 mg Lurasidone (n=122) 80 mg Lurasidone (n=119) 120 mg Lurasidone (n=124)
*0.025
*0.029
*0.009 *
0.006*
0.005
* 0.048
* 0.029
LS M
ean
Cha
nge
from
Bas
elin
e

35
0.3
0.00.0
0.5
1.0
1.5
Lurasidone Placebo
PEARL 1:Weight Change (LOCF)
Med
ian
Cha
nge
from
Bas
elin
e (k
g)
(N=124)
n=364

36SAS scored 0-5 on 9 items for max possible score of 45
PEARL 1:Simpson Angus Scale (SAS)
-0.01
0.06
0.010.03
-0.05
0.00
0.05
0.10
0.15
0.20
Lur 40 mg/d Lur 80 mg/d Lur 120 mg/d Placebo
LS M
ean
Cha
nge
n=122 n=119 n=124
n=124

37
PEARL 1: Barnes Akathisia Rating Scale (BAS)
BAS scored 0-5 on Global Clinical Assessment of akathisia for a maximum possible score of 5
0.0
0.3
0.10.1
0.0
0.5
1.0
Lur 40 mg/d Lur 80 mg/d Lur 120 mg/d Placebo
LS M
ean
Cha
nge
n=124 n=122 n=119 n=124
Global Clinical Assessment

38
0.70
0.35
0.0
0.5
1.0
1.5
2.0
2.5
3.0
Lurasidone Placebo
Med
ian
Cha
nge
(ng/
mL)
PEARL 1:Serum Prolactin
n=361n=361 n=122n=122

39
-14
-12
-10
-8
-6
-4
-2
0Cholesterol HDL LDL Triglycerides
Med
ian
Cha
nge
(mg/
dL)
Placebo Lurasidone
PEARL 1:Lipid Profile
n=108/343 n=108/343 n=108/343 n=108/343
LOCF endpoint values; fasting per protocol; includes all subjects

40
2.11.91.2 1.8
0.0
2.0
4.0
6.0
8.0
10.0
Lur 40 mg/d Lur 80 mg/d Lur 120 mg/d Placebo
PEARL 1:QTcF Interval Change (LOCF)
Mea
n C
hang
e (m
sec)
n=120n=120n=122n=122n=117n=117n=120n=120

41
6.2%
6.5%
4.7%
4.1%
11.2%
10.8%
8.7%
11.2%
12.8%
12.8%
10.6%
14.9%
11.6%
6.5%
13.3%
21.4%
Sedation
Nausea
Somnolence
Akathisia
Placebo (n=339)Lurasidone 40 mg (n=241)Lurasidone 80 mg (n=282)Lurasidone 120 mg (n=173)
Treatment-Emergent Adverse Event Rates (Incidence ≥10%)
Phase 2 and 3 DataStudies 006/049/196/PEARL 1
Cucchiaro J, et al. Efficacy and Safety of Lurasidone in Phase 2/3 Acute Schizophrenia Trials. Poster.American Psychiatric Association, San Francisco, CA, May 16-21, 2009,

42
Lurasidone Efficacy:Summary
Consistent efficacy
40, 80 and 120 mg/d shown effective across 3 placebo-controlled trials
Rapid onset (day 3 or 4) with subsequent sustained improvement noted in placebo-controlled trials
Potential for improvement of cognitive deficits, based on preclinical and clinical data
43
Lurasidone Safety:Summary
Lurasidone is well tolerated
Low rates of EPS and akathisia
Minimal prolactin change
Neutral effects on weight, lipids and glucose
Modest change in QTc interval
Self-reported AEs are generally mild and transient
Potential for Ongoing Adherence to TreatmentPotential for Ongoing Adherence to TreatmentPotential for Ongoing Adherence to Treatment

44
Lurasidone Development ProgramLurasidone Development Program

45
PEARL 1 and 2 Trials:Lurasidone in Acute Schizophrenia
Lurasidone 40 mgLurasidone 40 mgLurasidone 40 mg
Lurasidone 80 mgLurasidone 80 mgLurasidone 80 mg
Lurasidone 120 mgLurasidone 120 mgLurasidone 120 mg
PlaceboPlaceboPlacebo
Lurasidone 40-120 mgLurasidone 40Lurasidone 40--120 mg120 mg
Open-label, 2 years
Study 229PEARL #1Study 229Study 229PEARL #1PEARL #1
Double-blind, 6 weeks
Lurasidone 40 mgLurasidone 40 mgLurasidone 40 mg
Lurasidone 120 mgLurasidone 120 mgLurasidone 120 mg
Olanzapine 15 mgOlanzapine 15 mgOlanzapine 15 mg
PlaceboPlaceboPlacebo
Lurasidone 40-120 mgLurasidone 40Lurasidone 40--120 mg120 mg
Open-label, 6 months
Study 231PEARL #2Study 231Study 231PEARL #2PEARL #2
Double-blind, 6 weeks
N=480/studyLurasidone: QD dosing schedule

46
PEARL 3:Lurasidone in Acute Schizophrenia
Lurasidone 80 mgLurasidone 80 mgLurasidone 80 mg
Lurasidone 160 mgLurasidone 160 mgLurasidone 160 mg
Quetiapine XR 600 mgQuetiapine XR 600 mgQuetiapine XR 600 mg
PlaceboPlaceboPlacebo
Lurasidone 40-160 mgLurasidone 40Lurasidone 40--160 mg160 mg
Quetiapine XR 200-800 mgQuetiapine XR 200Quetiapine XR 200--800 mg800 mg
Double-blind, flexible dose, 1 year
Studies 233/234
PEARL #3
Studies Studies 233/234233/234
PEARL #3PEARL #3
Double-blind, 6 weeks
N=480/studyLurasidone: QD dosing schedule

47
Open-Label Continuation PhaseDouble-Blind Phase
12 months 6 months
Scre
enin
gSc
reen
ing
Scre
enin
g
Bas
elin
eB
asel
ine
Bas
elin
e
Lurasidone 40-120mg/dN=400(200 for sub-study)Lurasidone 40Lurasidone 40--120mg/d120mg/d
N=N=440000(200 for sub(200 for sub--study)study)
Risperidone 2-6mg/dN=200(100 for sub-study)
Risperidone 2Risperidone 2--6mg/d6mg/dN=N=220000(100 for sub(100 for sub--study)study)
Lurasidone 40-120mg/dLurasidone Lurasidone 4040--120mg/d120mg/d
Long-Term Safety Study With Cognitive Sub-Study
6 MonthsMCCB UPSA-B
Cognition Sub-Study
MCCB: MATRICS Consensus Cognitive BatteryUPSA-B: UCSD Performance-Based Skills Assessment - Brief Version

48
Atypical Use Has and Will Continue to Expand
AcuteManiaAcuteMania MaintenanceMaintenance
Treatment-Resistant
Depression
Treatment-Resistant
DepressionDepression/
AnxietyDepression/
AnxietyBipolar
DepressionBipolar
Depression
DepressionSchizophrenia Bipolar
AtypicalsAtypicals
AntidepressantsAntidepressants
Mood StabilizersMood Stabilizers

49
PREVAIL: Lurasidone in Bipolar Depression

50
PREVAIL Add-On Design (Study 235) PREVAIL Monotherapy Design (Study 236)
PREVAIL Extension
Study
PREVAIL PREVAIL Extension Extension
StudyStudyPlacebo + Lithium or Valproate
Placebo Placebo + Lithium or + Lithium or ValproateValproate
Lurasidone 20-120 mg/d+ Lithium or Valproate
Lurasidone 20Lurasidone 20--120 mg/d120 mg/d+ Lithium or + Lithium or ValproateValproate
ScreeningScreeningScreening
Bas
elin
eB
asel
ine
Bas
elin
e3-28 days
Day 0
Double-Blind Phase
6 weeksEnrollment Initiated 2Q ’09Enrollment Initiated 2Q ’09
PREVAIL Extension
Study
PREVAIL PREVAIL Extension Extension
StudyStudyPlacebo Placebo Placebo
ScreeningScreeningScreening
Lurasidone 20-60 mg/dLurasidone 20Lurasidone 20--60 mg/d60 mg/d
3-28 days
Day 0
Lurasidone 80-120 mg/dLurasidone 80Lurasidone 80--120 mg/d120 mg/d
n=504
(Study 235)
(Study 236)
Total n=504 (n=168/arm).
Total n=340 (n=170/arm).
Bas
elin
eB
asel
ine
Bas
elin
e

51
Lurasidone Commercial OverviewLurasidone Commercial Overview
Joseph Yen LinVice President, MarketingDainippon Sumitomo Pharma America

52
Agenda
I. Market and Disease State Overview
II. Competitive Landscape

53
$0
$2
$4
$6
$8
$10
$12
$14
Market OverviewOverall Growth
Sale
s ($
Bill
ions
)
Source: IMS NSP Data, 2004-2008
The atypical antipsychotic market is large and continues to grow at a robust rate
$14.1B
$12.7B
$11.3B$10.1B
$9.3B
+8.6%
+11.9%
+12.4%
+11.0%
2004 2005 2006 2007 2008

54
$2.9 $3.6 $3.2 $3.4 $3.8
$0.6$0.4 $0.6 $0.6
$0.6$1.4$1.3 $1.3 $1.5 $1.3
$2.1$2.2 $2.8 $2.8
$3.3$2.3
$2.6$3.4
$4.4$5.0
$0
$2
$4
$6
$8
$10
$12
$14
Market OverviewGrowth by Diagnosis
Sale
s ($
Bill
ions
)$14.1B
$12.7B
$11.3B
$10.1B$9.3B
Source: Estimated from IMS NSP Data, 2004-2008 and NDTI 2004 to 2008
Growth in the atypical antipsychotic category is being driven by use in bipolar disorder and schizophrenia
2004 2005 2006 2007 2008
Bipolar Disorder
Schizophrenia
Depression
Anxiety
Other

55
Schizophrenia Disease State OverviewPatient Flow
U.S. lifetime prevalence of schizophrenia is 1%; approximately 2.5 million affected
Origination
Diagnosis/ Evaluation
Treatment
Continuation High rates of patient discontinuation and switching • Lack of efficacy• Side effects• Need for new treatment options
High rates of diagnosis (80%) and treatment (85%)
Atypical antipsychotics considered the gold standard for schizophrenia

56
Schizophrenia Disease State OverviewLandmark CATIE Trial
“…patients with chronic schizophrenia in this study discontinued their antipsychotic study medications at a high rate, indicating
substantial limitations in the effectiveness of the drugs.”
Effectiveness of Antipsychotic Drugs in Patients with Chronic Schizophrenia
Jeffrey A. Lieberman, M.D., T. Scott Stroup, M.D., M.P.H., Joseph P. McEvoy, M.D., Marvin S. Swartz, M.D., Robert A. Rosenheck, M.D., Diana O. Perkins, M.D., M.P.H., Richard S.E. Keefe,
Ph.D., Sonia M. Davis, Dr.P.H., Clarence E. Davis, Ph.D., Barry D. Lebowitz, Ph.D., Joanne Severe, M.S., John K. Hsiao, M.D., for the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE)
Investigators

57
Bipolar Disease State OverviewPatient Flow
U.S. lifetime prevalence of bipolar disorder is 2.6%; over 6 million affected
Origination
Diagnosis/ Evaluation
Treatment
Continuation
Relatively lower rates of diagnosis (45%) and treatment (80%) as compared to schizophrenia
Multiple agents currently used in treatment – lithium, antiepileptic agents
Atypicals increasingly used to treat bipolar depression
Only 1 atypical currently approved for bipolar depression (Seroquel)

58
Key Takeaways
Large, growing market for atypical antipsychotics
High rate of dissatisfaction and switch; need for new treatment options
Increasing use for the treatment of bipolar disorder is a significant driver of atypical antipsychotic market growth
ChallengesOpportunities

59
Agenda
I. Market and Disease State Overview
II. Competitive Landscape

60
0%
5%
10%
15%
20%
25%
30%
35%
40%
Jan-0
3Ju
l-03
Jan-0
4Ju
l-04
Jan-0
5Ju
l-05
Jan-0
6Ju
l-06
Jan-0
7Ju
l-07
Jan-0
8Ju
l-08
Atypical Antipsychotic MarketCurrent Competitive Environment
SEROQUEL
RISPERIDONE
ABILIFY
ZYPREXA
GEODONCLOZARILINVEGARIS CONSTA
Seroquel is the clear market leader; impact of generic risperidone not yet evident
Source: IMS DataView
TRx
Shar
e

61
Atypical Antipsychotic MarketPerceptual Mapping in Schizophrenia
Safe
ty/T
oler
abili
ty
Efficacy
Better-Tolerated Medications (i.e.
limited weight gain, metabolic issues);Less Efficacious
More Efficacious Medications; Less Well-tolerated (i.e.
weight gain, metabolic issues, EPS)
Cognitive Functioning
New product opportunity
62
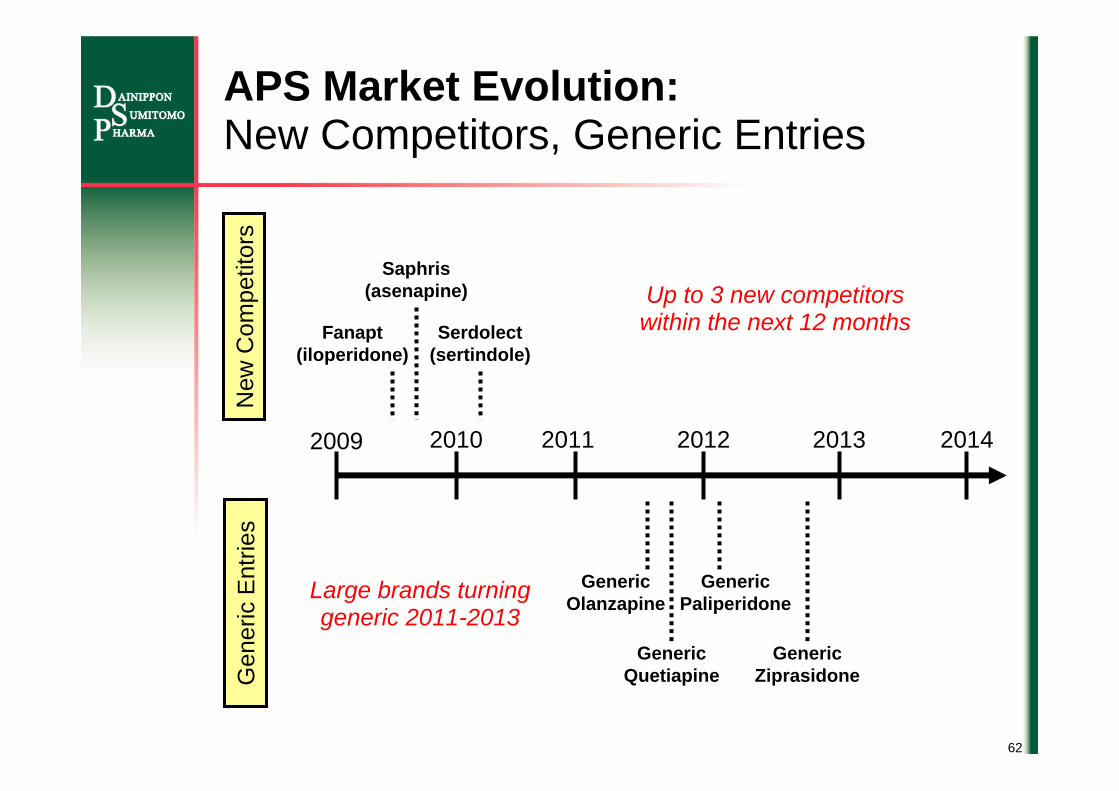
APS Market Evolution:New Competitors, Generic Entries
2009 2010 2012 2013 20142011
Fanapt(iloperidone)
Saphris(asenapine)
Serdolect(sertindole)
New
Com
petit
ors
Up to 3 new competitors within the next 12 months
Generic Olanzapine
Generic Quetiapine
Generic Ziprasidone
Generic Paliperidone
Gen
eric
Ent
ries
Large brands turning generic 2011-2013

63
Antipsychotic Payer Mix
Dual Eligibles7%
Medicaid23%
Medicare Part D17%
CommercialManaged Care
39%
Public and private payers likely to increase control over utilization of branded products when more generics become available
Source: IMS
Other14%
Manage access through tiered co-payments
(higher co-pay for more restricted medications)
Manage access through preferred drug lists (PDLs);
manufacturers provide supplemental rebates to
gain access to PDL

64
Key Takeaways
Highly competitive market with large brands
New competitor launches pending
Genericization of market beginning in 2011 will change market dynamics payers more likely to control utilization of branded products
Large, growing market for atypical antipsychotics
High rate of dissatisfaction and switch; need for new treatment options
Increasing use for the treatment of bipolar disorder is a significant driver of atypical antipsychotic market growth
Market opportunity for more efficacious, better tolerated medications
ChallengesOpportunities

65
Disclaimer Regarding Forward-looking Statements
The statements made in this presentation material are forward-looking statements based on management’s assumptions and beliefs in light of information available up to the day of announcement, and involve both known and unknown risks and uncertainties.
Actual financial results may differ materially from those presented in this document, being dependent on a number of factors.
Information concerning pharmaceuticals (including compounds under development) contained within this material is not intended as advertising or medical advice.