lung function, respiratory muscle strength and effects …589175/fulltext01.pdf · lung function,...
TRANSCRIPT
ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2013
Digital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 857
Lung Function, RespiratoryMuscle Strength and Effects ofBreathing Exercises in CardiacSurgery Patients
CHARLOTTE URELL
ISSN 1651-6206ISBN 978-91-554-8580-1urn:nbn:se:uu:diva-192208
Dissertation presented at Uppsala University to be publicly examined in B:42, BMC,Husargatan 3, Uppsala, Friday, March 1, 2013 at 09:15 for the degree of Doctor of Philosophy(Faculty of Medicine). The examination will be conducted in Swedish.
AbstractUrell, C. 2013. Lung Function, Respiratory Muscle Strength and Effects of BreathingExercises in Cardiac Surgery Patients. Acta Universitatis Upsaliensis. Digital ComprehensiveSummaries of Uppsala Dissertations from the Faculty of Medicine 857. 58 pp. Uppsala.ISBN 978-91-554-8580-1.
Background: Breathing exercises are widely used after cardiac surgery. The duration ofexercises in the immediate postoperative period is not fully evaluated and only limited dataregarding the effects of home-based breathing exercises after discharge from hospital have beenpublished.
Aim: The overall aim of this thesis was to evaluate the effects of deep breathing exercises withpositive expiratory pressure (PEP) and describe lung function and respiratory muscle strengthin patients undergoing cardiac surgery.
Participants and settings: Adult participants (n=131) were randomised to perform either 30or 10 deep breaths with PEP per hour during the first postoperative days (Study I): the mainoutcome was oxygenation, assessed by arterial blood gases, on the second postoperative day. InStudy III, 313 adult participants were randomly assigned to perform home-based deep breathingexercises with PEP for two months after surgery or not to perform breathing exercises with PEPafter the fourth to fifth postoperative day. The main outcome was lung function, assessed byspirometry, two months after surgery. Studies II and IV were descriptive and correlative andinvestigated pre and postoperative lung function, assessed by spirometry, and respiratory musclestrength, assessed by maximal inspiratory pressure, and maximal expiratory pressure.
Results: On the second postoperative day, arterial oxygen tension (PaO2) and arterial oxygensaturation (SaO2) was higher in the group randomised to 30 deep breaths with PEP hourly.There was no improved recovery of lung function in participants performing home-based deepbreathing exercises two months after cardiac surgery, compared to a control group. Subjectiveexperience of breathing or improvement in patient perceived quality of recovery or health-related quality of life did not differ between the groups at two months. Lung function andrespiratory muscle strength were in accordance with predicted values before surgery. A 50%reduction in lung function was shown on the second postoperative day. High body massindex, male gender and sternal pain were associated with decreased lung function on thesecond postoperative day. Two months postoperatively, there was decreased lung function, butrespiratory muscle strength had almost recovered to preoperative values.
Keywords: Breathing exercises, Cardiac surgery, Deep breathing, Lung function,Oxygenation, Physical therapy, Positive expiratory pressure, Spirometry, Respiratory musclestrength
Charlotte Urell, Uppsala University, Department of Neuroscience, Physiotheraphy, Box 593,SE-751 24 Uppsala, Sweden.
© Charlotte Urell 2013
ISSN 1651-6206ISBN 978-91-554-8580-1urn:nbn:se:uu:diva-192208 (http://urn.kb.se/resolve?urn=urn:nbn:se:uu:diva-192208)
List of Papers
This thesis is based on the following studies, which are referred to in the text by their Roman numerals.
I Urell C, Emtner M, Hedenström H, Breidenskog M, Tenling A, Westerdahl E. Deep Breathing Exercises with Positive Expiratory Pressure at a Higher Rate Improve Oxygenation in the Early Period After Cardiac Surgery – A Randomised Controlled Trial. European Journal of Car-diothoracic Surgery 2011;40:162-167
II Urell C, Westerdahl E, Hedenström H, Janson C, Emtner M.
Lung Function Before and Two Days after Open-Heart Surgery. Critical Care Research and Practice, vol.2012, Article ID 291628, Doi: 10.1155/2012/291628
III Westerdahl E, Urell C, Jonsson M, Bryngelsson I L, Hedenström H, Emtner M. Home-Based Deep Breathing Exercises Performed Two Months Following Cardiac Surgery – A Randomised Controlled Trial. Submitted IV Urell C, Emtner M, Hedenström H, Westerdahl E. Respiratory Muscle Strength in Cardiac Surgery Patients Submitted
Reprints were made with permission from the respective publishers.

Contents
Introduction ..................................................................................................... 9
Background ................................................................................................... 10 Postoperative pulmonary impairments and risk factors ........................... 10 Lung function ........................................................................................... 11 Respiratory muscle strength ..................................................................... 11 Physiotherapy treatment in the postoperative period ............................... 12
Deep breathing exercises with PEP ..................................................... 12 Duration and frequency of breathing exercises ................................... 13
Rationale for this thesis ............................................................................ 14 Aims .......................................................................................................... 15
Methods ......................................................................................................... 16 Design ....................................................................................................... 16 Participants and settings ........................................................................... 18 Surgery, postoperative care and physiotherapy ........................................ 21 Study groups, procedures, and intervention ............................................. 21
Studies I-II ............................................................................................ 21 Studies III-IV ........................................................................................ 22 Deep breathing with PEP .................................................................... 22
Measurements ........................................................................................... 24 Spirometry (Studies I-IV) ..................................................................... 24 Arterial blood gas (Study I) ................................................................. 24 Respiratory muscle strength (Study IV) ............................................... 25 Sternal pain (Studies I-IV) ................................................................... 25 Patient-perceived quality of recovery (Study III) ................................ 25 Health-related quality of life (Study III) .............................................. 26 Subjective experience of breathing and oxygen saturation (Studies III and IV) ............................................................................... 26 Thoracic excursion (Study III) ............................................................. 26
Statistical analyses .................................................................................... 28 Sample size calculation ........................................................................ 29 Descriptive statistics ............................................................................ 29 Parametric statistics ............................................................................ 29 Non- parametric statistics .................................................................... 30
Results ........................................................................................................... 31 Lung function (Studies I-IV) .................................................................... 31 Arterial blood gas (Study I) ...................................................................... 33 Respiratory muscle strength (Study IV) ................................................... 33 Sternal pain (Studies I-IV) ........................................................................ 34 Patient-perceived quality of recovery, health-related quality of life (Study III) and subjective experience of breathing (Studies III-IV) ........ 34 Oxygen saturation (Studies III, IV), thoracic excursion (Study III), and postoperative pulmonary infections (Study III) ................................. 35
Discussion ..................................................................................................... 36 Effects of deep breathing exercises with PEP .......................................... 36 Compliance with the breathing exercises ................................................. 38 Preoperative lung function and respiratory muscle strength .................... 39 Postoperative lung function and respiratory muscle strength ................... 40 Methodological considerations ................................................................. 41 External validity ....................................................................................... 42 Clinical implications and further research ................................................ 43
Conclusions ................................................................................................... 45
Sammanfattning på svenska .......................................................................... 46 Lungfunktion, andningsmuskelstyrka och effekter av andningsövningar hos personer som genomgår hjärt-kirurgi ................................................. 46
Acknowledgements ....................................................................................... 48
References ..................................................................................................... 51
Abbreviations
ABG ANOVA ATS BMI CABG CG COPD CPAP ERS FEV1 FRC FVC HRQoL IC ICU IR-PEP IS MEP MIP NRS NIV NYHA PaCO2 PaO2 PEP RCT SaO2 SpO2 SD SF-36 TG VC
Arterial blood gases Analysis of variance American Thoracic Society Body Mass Index Coronary artery bypass grafting Control group Chronic obstructive pulmonary disease Continuous positive airway pressure European Respiratory Society Forced expiratory volume in 1 second Functional residual capacity Forced vital capacity Health-related quality of life Inspiratory capacity Intensive care unit Inspiratory resistance positive expiratory pressure Incentive spirometry Maximal expiratory pressure Maximal inspiratory pressure Numeric rating scale Non-invasive ventilation New York Heart Association classification Arterial carbon dioxide tension Arterial oxygen tension Positive expiratory pressure Randomised controlled trial Arterial oxygen saturation Peripheral oxygen saturation Standard deviation Short form 36 Treatment group Vital capacity


9
Introduction
Coronary heart disease is one of the most common causes of morbidity and mortality globally (1, 2). Although cardiac surgery is an effective treatment for patients with advanced coronary heart disease, it carries a risk for serious non-cardiac complications, such as pulmonary impairments, sepsis, stroke, renal impairments, deep sternum infections, and gastrointestinal complica-tions, all of which prolong the length of hospital stay (3). Pulmonary im-pairments are the single greatest non-cardiac complications and the causes are multifactorial (3-5). In the early postoperative period, lung function, measured as vital capacity (VC) and forced expiratory volume in one second (FEV1), is usually decreased by 35-60% (6-9), and a 6-13% decreased lung function can persist for four months (10). In the first postoperative days a reduced lung function can contribute to impaired gas exchange (11, 12) and respiratory muscle strength decreases during the first days after surgery (13): however, little data on respiratory muscle function months after surgery is reported.
Breathing exercises are widely used in postoperative care for preventing postoperative pulmonary impairments, such as decreased lung volumes, ate-lectasis, decreased oxygenation and pneumonia, and are used in different ways and through a variety of devices and techniques (12, 14-18). In Swe-den, deep breathing exercises with positive expiratory pressure (PEP) is a common postoperative treatment (19), however, it is unclear whether differ-ent duration and frequencies affect lung volumes and oxygenation levels. The challenge of this thesis was to contribute to the increasing knowledge in how to prevent and reduce the negative effects of pulmonary impairments after cardiac surgery by deep breathing exercises with PEP and to describe lung function and respiratory muscle strength in cardiac surgery patients.

10
Background
Postoperative pulmonary impairments and risk factors Cardiac surgery increases the risk of postoperative pulmonary impairments (4, 20). The definition of postoperative pulmonary impairments is still un-clear, but atelectasis, pleura effusion, pulmonary oedema, bronchospasm and pneumonia are reported as pulmonary impairments (21). Clinical manifesta-tions of postoperative pulmonary impairments range from arterial hypox-emia to acute respiratory distress syndrome (22). In the first postoperative week 67-100% of patients have areas of atelectasis (17, 23) and the preva-lence of pneumonia is reported to be 3-12% after cardiac surgery (21, 24). Several risk factors, classified as preoperative-, perioperative- and postop-erative are involved in causing pulmonary impairments, but the pathogenesis is complex and not completely understood. Preoperative risk factors for postoperative pulmonary impairments include general disability, infections in the respiratory passage, lung disease, smok-ing, older age (>80 years), overweight (Body Mass Index, BMI >25), diabe-tes mellitus, malnutrition and dehydration (25, 26). Although chronic ob-structive pulmonary disease (COPD) is conventionally associated with in-creased postoperative morbidity and mortality after cardiac surgery, this association has been challenged (27-29). Postoperative pulmonary impair-ments are two-fold greater in current smokers than in non-smokers and their hospital stay is prolonged (30) and after cardiac surgery obese patients suffer more pulmonary impairments than non-obese patients (25). Perioperative risk factors for postoperative pulmonary impairments include median sternotomy incision, dissection of internal mammary artery, hypo-thermia for myocardial protection, the use of cardiopulmonary bypass, and general anaesthesia (31-34). After sternotomy, changes in the chest wall configuration can reduce chest wall compliance for up to three months post-operatively (35). The retrieval of the internal mammary artery, which typi-cally necessitates pleural dissection, may also contribute to pulmonary im-pairment (36). Topical cooling for myocardial protection causes phrenic nerve dysfunction followed by diaphragm paralysis (33, 37) and almost all anaesthestics generate a reduction in functional residual capacity (FRC) and negatively influence oxygenation (38). One reason for reduced FRC is loss

11
of respiratory muscle tone, which allows the elastic forces of the lungs to pull the chest wall (39). Mucociliary clearance is also affected by the general anesthesia, intubation and analgesia. Postoperative risk factors for postoperative pulmonary impairments include immobilisation, pain, pain analgesics and, hyperhydration (40, 41). A supine position during intubation results in decreased FRC and an upward shift of the diaphragm, relaxation of the chest wall, altered chest wall compliance, and a shift in blood volume from the thorax to the abdomen. A combination of these factors results in a mismatch in ventilation-perfusion (32). Sternal pain is commonly reported during hospital stay (31, 41, 42) and a worsening of pain correlates with decreased lung function and maximal inspiratory pressure (MIP) during the first postoperative days (41). Pleural drain is an important cause of postoperative pain and shorter duration of pleural drain renders a shorter length of stay in the intensive care unit (ICU) (43).
Lung function Lung function variables measured in this thesis were vital capacity (VC), forced vital capacity (FVC), inspiratory capacity (IC), forced expiratory volume in one second (FEV1), functional residual capacity (FRC), and total lung capacity (TLC). Lung volume is used synonymously. The majority of patients undergoing cardiac surgery have almost normal lung function preoperatively (44). In comparison to preoperative values, a mean reduction in lung function is reported to be 35-60% in the first postop-erative week (8, 9, 45). Reduced lung function contributes to impaired gas exchange (46). There is an inverse correlation between atelactatic area and arterial oxygenation (PaO2) during the first (11) and second (23) postopera-tive days. Lung function gradually recovers, but even four months after car-diac surgery a reduction of preoperative values with 6-13% is reported (10). Although lung function decreases after cardiac surgery, it is unclear whether breathing exercises can influence lung function several months postopera-tively.
Respiratory muscle strength Evans et al. (47) suggest a maximal inspiratory pressure (MIP) greater than 50 cm H2O is normal, whereas, in the “Statement on Respiratory Muscle Testing (48), a MIP above 80 cm H2O usually excludes patients with clini-cally relevant inspiratory muscle weakness, e.g. dyspnea. According to Ev-ans et al. (47), maximal expiratory pressure (MEP) values greater than 60 cm
12
H2O are considered normal for producing an effective cough. The majority of cardiac surgery patients have both MIP and MEP above these recommen-dations before surgery (13, 44, 49). The first week after cardiac surgery, a 35% reduction is reported, compared to preoperative values (44), and 18 months after surgery recovered values of MIP and MEP are reported (50), but the relation between lung function and respiratory muscle strength is unclear.
Physiotherapy treatment in the postoperative period After cardiac surgery, physiotherapy treatment during hospital stay often consists of early mobilisation, breathing exercises, instruction in efficient coughing techniques and an active range of motions for the shoulder girdle and upper back (19, 51). Breathing exercises are widely used in postoperative care in hospitals to prevent postoperative pulmonary impairments and their effects (7, 12, 18, 52). The main purpose of different breathing exercises during the postopera-tive period is to increase lung volume. During the hospital stay, common breathing exercises/techniques for patients with spontaneous breathing in-clude; deep breathing (17), incentive spirometry (IS) (53, 54), breathing exercises with PEP (12, 23), inspiratory resistance-positive expiratory pres-sure (IR-PEP) (17, 55, 56) and non-invasive ventilation (NIV) (8, 57). The forced expiratory technique and coughing aimed at mucus clearance are used in a clinical setting but are insufficiently evaluated after cardiac sur-gery. In Sweden, during hospital stay, mobilisation and breathing exercises with PEP are the first choices of therapy after non-complicated cardiac sur-gery (19). As no single breathing exercise during the postoperative period has proven superior, there is a lack of consensus regarding the most appro-priate breathing exercises (8, 52, 57, 58). As there is limited evaluation of breathing exercises after discharge (50) it is unclear whether breathing exer-cises, several months after surgery, can influence decreased lung function.
Deep breathing exercises with PEP Deep breaths are an important part of normal breathing. In clinical practice patients do not naturally sigh and yawn after surgery, probably because of pain. Deep breathing with post-inspiratory pause increases FRC, which in turn increases alveolar stability, can justify the use of deep breaths for the prevention of atelectasis (59). Following cardiac surgery, deep breathing exercises are often recommended for reducing areas of atelectasis and im-proving oxygenation (23).
13
The use of PEP in postoperative care specifically aims at increasing lung volume and facilitating mucus clearance. Although the physiological effects of PEP are unknown, the potential increase in FRC is considered essential (60). Deep breathing and PEP can also be used as a mucus clearance tech-nique. As deep breathing increases lung volume, it promotes an effective forced expiratory technique or cough manoeuver. PEP is purported to pro-mote movement of mucus in patients with cystic fibrosis (61), but data on the function of PEP as a mucus clearance technique in postoperative care are limited. Different devices for PEP breathing are used in clinical practice; a mask or a mouthpiece is connected to either a resistance nipple to create positive pres-sure during expiration, or a blow bottle system in which the resistance is created by a water seal. The pressure achieved depends on how the manoeu-ver is performed, the applied resistance, and the patient`s expiratory flow. In postoperative care, expiratory resistance is often regulated to achieve 5-20 cm H2O. Deep breathing exercises with PEP can be performed in different ways. In this thesis the purpose of the breathing exercises with PEP was to increase lung volumes and to facilitate the following deep breath. The deep inhalation was to create a larger lung volume than normal tidal breathing and the hold-ing of the breath after maximal inhalation aimed at improving the possibility of increased gas exchange. Furthermore, PEP during exhalation aimed to stimulate the diaphragm into a favourable position. Deep breathing exercises with PEP performed every hour during the first four postoperative days after cardiac surgery increase lung function (12) and IS in combination with PEP reduce the incidence of pneumonia and length of hospital stay (62). A six-day postoperative rehabilitation program with PEP breathing in combination with walking training is reported to increase respiratory muscle strength, measured as MIP and MEP, after cardiac sur-gery (63). However, the recommendations on duration and frequency of breathing exercises differ in both studies and clinical practice.
Duration and frequency of breathing exercises The duration of treatment sessions range from 4 to 40 minutes (6, 55, 56, 58, 62, 64, 65), and there is a lack of evidence for how long after surgery the breathing exercises should continue. The number of breaths range from 5 to 30 breaths per hour (12, 14, 23, 66) and the frequency of daily sessions rang-es from once an hour to once a day (6, 12, 23, 66). The optimal duration and frequency of breathing exercises after surgery has not been fully investigated, thus, it is unclear if deep breathing exercises
14
with PEP performed after the fourth to fifth postoperative day can influence lung function.
Rationale for this thesis Approximately 6000 adults undergo open cardiac surgery every year in Sweden (2). Postoperative pulmonary impairments are the most common non-cardiac complication after cardiac surgery and increase both morbidity and mortality. Breathing exercises are widely used in the postoperative care for preventing or/and treating already developed impairments. Hourly deep breathing exer-cises with PEP have positive effects on lung function and oxygenation dur-ing hospital stay after cardiac surgery. The optimal duration of breathing exercises is unknown and instructions concerning how long patients should continue the breathing exercises after discharges vary within clinical prac-tice.
As impaired lung function occurs in the first postoperative days after cardiac surgery, the factors that might affect lung function should be investigated in an attempt to identify plausible threats to lung function. Furthermore, respir-atory muscle strength decreases in the first postoperative week, but it is un-known when patients regain muscle strength after cardiac surgery and if respiratory muscle strength correlates with lung function two months after surgery. The hypotheses of the present thesis were:
• a higher rate of deep breathing exercise with PEP during the first postoperative days increases oxygenation and lung function
• deep breathing exercises with PEP, performed during the first two postoperative months, decrease pulmonary impairment and improve patient-perceived quality of recovery and health-related quality of life
• age, obesity, smoking, airflow obstruction, and pain negatively in-fluence lung function on the second postoperative day
• respiratory muscle strength and lung function are decreased two months postoperatively
15
Aims
The overall aim of this thesis was to evaluate the effects of deep breathing exercises with positive expiratory pressure (PEP) and to describe lung func-tion and respiratory muscle strength in patients undergoing cardiac surgery. The specific aims were: Study I To determine the effect of 30 versus 10 deep breaths hourly, while awake, with a PEP-device, on oxygenation and lung function, during the first two days after cardiac surgery. Study II To investigate the pre-,peri-, and postoperative factors influencing lung vo-lumes, measured by spirometry, on the second postoperative day after car-diac surgery. Study III To evaluate the effectiveness of home-based deep breathing exercises per-formed with a PEP-device during the first two months after cardiac surgery. Study IV To describe respiratory muscle strength, measured as maximal inspiratory pressure and maximal expiratory pressure, before and two months after car-diac surgery.

16
Methods
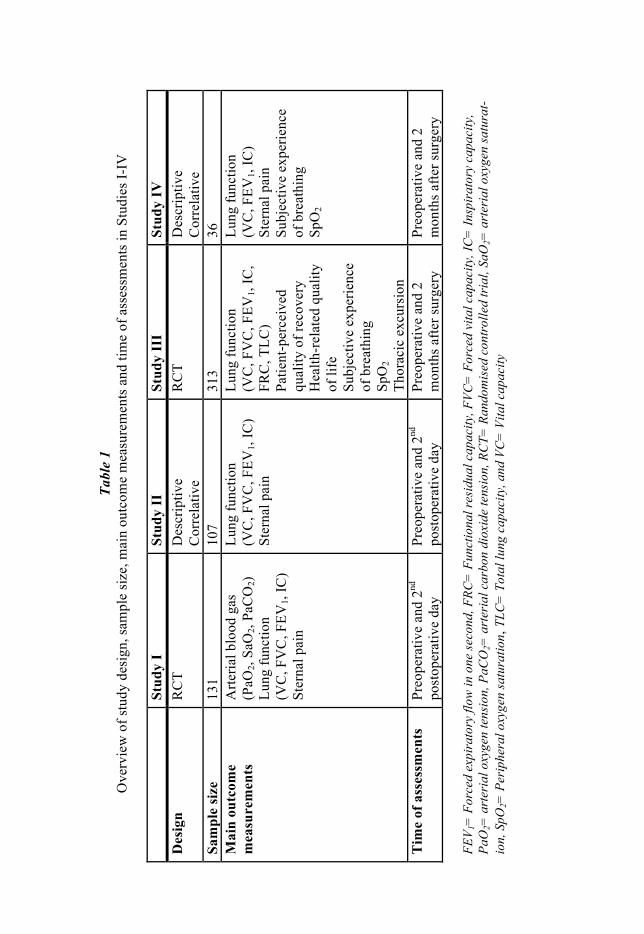
Design This thesis consists of four studies. In Study I 131 patients participated, of which 107, who performed lung function testing, participated in Study II. Study III consisted of 313 participants, of which a subgroup of 36 was in-cluded in study IV. In Studies I, II, and IV the participants were recruited from Uppsala University Hospital, Uppsala, Sweden. In Study III, the par-ticipants were recruited from Uppsala University Hospital and from Örebro University Hospital, Örebro, Sweden. The Regional Ethical Review Board in Uppsala, Sweden approved the studies (Studies I-II Dnr: 2007/044 and Studies III-IV Dnr: 2007/160). Participants were given verbal and written information about the study and informed consent was obtained from each participant. The study design, sample size, main outcome measures and time of assessment are outlined in Table 1.
Tabl
e 1
Ove
rvie
w o
f stu
dy d
esig
n, sa
mpl
e si
ze, m
ain
outc
ome
mea
sure
men
ts a
nd ti
me
of a
sses
smen
ts in
Stu
dies
I-IV
Stud
y I
Stud
y II
St
udy
III
Stud
y IV
D
esig
n R
CT
Des
crip
tive
Cor
rela
tive
RC
T D
escr
iptiv
e C
orre
lativ
e Sa
mpl
e si
ze
131
107
313
36
Mai
n ou
tcom
e
mea
sure
men
ts
Arte
rial b
lood
gas
(P
aO2,
SaO
2, Pa
CO
2)
Lung
func
tion
(VC
, FV
C, F
EV1,
IC)
Ster
nal p
ain
Lung
func
tion
(VC
, FV
C, F
EV1,
IC)
Ster
nal p
ain
Lung
func
tion
(VC
, FV
C, F
EV1,
IC,
FRC
, TLC
) Pa
tient
-per
ceiv
ed
qual
ity o
f rec
over
y H
ealth
-rel
ated
qua
lity
of li
fe
Subj
ectiv
e ex
perie
nce
of b
reat
hing
Sp
O2
Thor
acic
exc
ursi
on
Lung
func
tion
(VC
, FEV
1, IC
) St
erna
l pai
n Su
bjec
tive
expe
rienc
e of
bre
athi
ng
SpO
2
Tim
e of
ass
essm
ents
Pr
eope
rativ
e an
d 2nd
po
stop
erat
ive
day
Preo
pera
tive
and
2nd
post
oper
ativ
e da
y Pr
eope
rativ
e an
d 2
mon
ths a
fter s
urge
ry
Preo
pera
tive
and
2 m
onth
s afte
r sur
gery
FE
V 1=
For
ced
expi
rato
ry fl
ow in
one
seco
nd, F
RC=
Fun
ctio
nal r
esid
ual c
apac
ity, F
VC=
For
ced
vita
l cap
acity
, IC
= In
spir
ator
y ca
paci
ty,
PaO
2= a
rter
ial o
xyge
n te
nsio
n, P
aCO
2= a
rter
ial c
arbo
n di
oxid
e te
nsio
n, R
CT=
Ran
dom
ised
con
trol
led
tria
l, Sa
O2=
art
eria
l oxy
gen
satu
rat-
ion,
SpO
2= P
erip
hera
l oxy
gen
satu
ratio
n, T
LC=
Tot
al lu
ng c
apac
ity, a
nd V
C=
Vita
l cap
acity
18
Participants and settings To be eligible for participation in the four studies, participants had to be >18 years, scheduled for coronary artery bypass grafting (CABG) or valve sur-gery, and literate in Swedish. Participants were not included if they had an-gina at rest before surgery (Studies I-II). Furthermore, the participants were excluded after randomisation (Studies I-II) if they were postoperatively artificially ventilated for >15 hours or used continuous positive airway pres-sure (CPAP) treatment, received aorta balloon treatment, or had a pneumo-thorax requiring drainage treatment. For Studies III and IV, patients who had an emergency operation, previous cardiac or lung surgery, kidney failure requiring dialysis or were participant in other ongoing studies were not included. Criteria for not being random-ised (Studies III-IV) were intubation time > 24 hours, ICU time > 72 h, severe hemodynamic impairment, pulmonary or neurological complications, requiring dialysis, sternum related infections, sternum instability, mental health disorders, or other complications that could affect the patient’s oppor-tunity to participate in the study (perform deep breathing exercises, spirome-try examination and/or respiratory muscle test). Exclusion from the study was determined by the study manager (physical therapist) at each hospital in consultation with the cardiothoracic surgeon or cardiothoracic anaesthesiol-ogist. The recruitment processes for the randomised trials (Studies I and III) are presented in the flow charts in Figure 1 and 2. Reasons for participant withdrawal after randomisation in Study I were arte-rial needle out of order and too tired for spirometry (Figure 1). Reasons for participant withdrawal after randomisation in Study III were haemodynamic instability (n=3), pericardial or pleural effusion (n=5), sternal instabil-ity/infection (n=2), pain (n=1), cough (n=1), fatigue (n=5), other morbidities (n=2), failure to cooperate (n=1), and unwillingness to participate in the fol-low-up (n=24). The characteristics of the participants analysed in Studies I-IV are presented in Table 2.

F
igur
es 1
and
2. R
ecru
itmen
t pro
cess
for t
he ra
ndom
ised
tria
ls (S
tudi
es I
and
III)
. *Fo
r cau
ses o
f los
t to
follo
w-u
p in
Stu
dy II
I, se
e te
xt. A
BG=
art
e-ri
al b
lood
gas
Ass
esse
d fo
r elig
ibili
ty n
=216
Not
mee
ting
incl
usio
n cr
iteria
or
exc
lude
d af
ter s
urge
ry (n
=35)
- D
eclin
ed to
par
ticip
ate
(n=4
) - I
ntub
atio
n >1
5h o
r CPA
P (n
=31)
Ran
dom
ised
(n=1
81)
Allo
cate
d to
trea
tmen
t g
roup
(n=8
9)
Allo
cate
d to
con
trol
gro
up (n
=92)
Lost
to fo
llow
-up:
A
BG
: arte
rial n
eedl
e ou
t of
ord
er (n
=26)
Lu
ng fu
nctio
n: T
oo ti
red
for s
piro
met
ry (n
=41)
Lost
to fo
llow
-up:
A
BG
: arte
rial n
eedl
e ou
t of
orde
r (n=
24)
Lung
func
tion:
Too
tire
d fo
r sp
irom
etry
(n=3
3)
Ana
lyse
d: A
BG
(n=6
3)
Lung
func
tion
(n=4
8)
Ana
lyse
d: A
BG
(n=6
8)
Lung
func
tion
(n=5
9)
Lost
to fo
llow
-up:
Lost
to fo
llow
-
Ana
lyse
d: A
BG
(n=6
8)A
naly
sed:
AB
G (n
=63)Stud
y I
Ass
esse
d fo
r elig
ibili
ty (n
=407
)
Not
mee
ting
incl
usio
n cr
iteria
or
excl
uded
afte
r sur
gery
(n=5
0)
- Dec
lined
to p
artic
ipat
e (n
=19)
- C
ould
not
per
form
spiro
met
ry (n
=4)
- Ino
pera
ble
patie
nt (n
=2)
- Int
ubat
ion
>24
h/IC
U>7
2h (n
=14)
- N
euro
logi
cal s
ympt
oms
(n=5
) - S
tern
al in
stab
ility
(n=1
) - M
orta
lity
(n=4
) - M
issi
ng d
ata
(n=1
)
Ran
dom
ised
(n=3
57)
Allo
cate
d to
trea
tmen
t gr
oup
(n=1
80)
Allo
cate
d to
con
trol
grou
p (n
=177
)
Lost
to fo
llow
up
(n=2
1)*
Lost
to fo
llow
up
(n=2
3)*
Ana
lyse
d lu
ng
func
tion
(n=1
59)
Ana
lyse
d lu
ng
func
tion
(n=1
54)
ed (n
=357
)
Allo
cate
d to
trea
tmen
t A
lloca
ted
to c
ontro
l
Lost
to fo
llow
up
(n=2
3)Lo
st to
follo
w u
p (n
=21)
Ana
lyse
d lu
ng
Ana
lyse
d lu
ng
Stud
y II
I
20
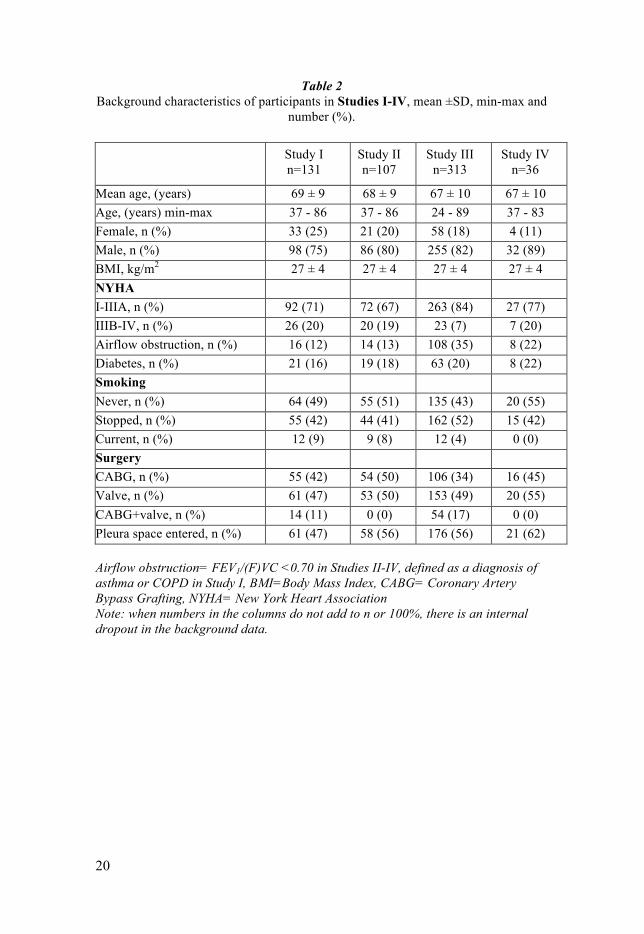
Table 2 Background characteristics of participants in Studies I-IV, mean ±SD, min-max and
number (%).
Study I n=131
n
Study II n=107
Study III n=313
Study IV n=36
n=36 Mean age, (years)
69 ± 9 68 ± 9 67 ± 10 67 ± 10
Age, (years) min-max 37 - 86 37 - 86 24 - 89 37 - 83 Female, n (%) 33 (25) 21 (20) 58 (18) 4 (11) Male, n (%) 98 (75) 86 (80) 255 (82) 32 (89) BMI, kg/m2 27 ± 4 27 ± 4 27 ± 4 27 ± 4 NYHA I-IIIA, n (%) 92 (71) 72 (67) 263 (84) 27 (77) IIIB-IV, n (%) 26 (20) 20 (19) 23 (7) 7 (20) Airflow obstruction, n (%) 16 (12) 14 (13) 108 (35) 8 (22) Diabetes, n (%) 21 (16) 19 (18) 63 (20) 8 (22) Smoking Never, n (%) 64 (49) 55 (51) 135 (43) 20 (55) Stopped, n (%) 55 (42) 44 (41) 162 (52) 15 (42) Current, n (%) 12 (9) 9 (8) 12 (4) 0 (0) Surgery CABG, n (%) 55 (42) 54 (50) 106 (34) 16 (45) Valve, n (%) 61 (47) 53 (50) 153 (49) 20 (55) CABG+valve, n (%) 14 (11) 0 (0) 54 (17) 0 (0) Pleura space entered, n (%) 61 (47) 58 (56) 176 (56) 21 (62)
Airflow obstruction= FEV1/(F)VC <0.70 in Studies II-IV, defined as a diagnosis of asthma or COPD in Study I, BMI=Body Mass Index, CABG= Coronary Artery Bypass Grafting, NYHA= New York Heart Association Note: when numbers in the columns do not add to n or 100%, there is an internal dropout in the background data.

21
Surgery, postoperative care and physiotherapy All participants received general anaesthesia and artificial ventilation with a positive end-expiratory pressure of 5-12 cm H2O. During anaesthesia and after surgery, all patients inspired oxygen with a concentration of 35-80%. After extubation, all participants received supplemental oxygen (1-5 litres) for maintaining arterial oxygen saturation (SaO2) above 90%. The partici-pants underwent aortic-, mitral- or tricuspidal valve replacement, CABG, or a combination of these: in Studies II and IV, no participants underwent combination surgery. All participants were administrated analgesics for pain and care according to standard routines at Uppsala University Hospital and Örebro University Hospital. Preoperatively, the physiotherapists orally informed all participants about the importance of early postoperative mobilisation, deep breathing exercises with PEP, and daily active exercises of the shoulder girdle and upper back. The participants met the physiotherapist once or twice daily during the first postoperative days in hospital. All participants were mobilised according to clinical routine: assisted to sitting as early as possible after surgery and were sitting out of bed and/or standing on the first postoperative day, walking in the room or a short distance in the corridor on the second postoperative day, and walking a longer distance in the corridor on the third postoperative day. Before discharge, all participants were orally informed about the importance of starting physical activity gradually.
Study groups, procedures, and intervention
Studies I-II Preoperatively, sealed envelopes were used to randomly allocate the partici-pants either to a treatment group (TG) or a control group (CG) for perform-ing deep breathing exercises with PEP with two different durations hourly in the two first postoperative days. The deep breathing exercises with PEP started approximately one hour after extubation and continued during day-time until the morning of the second postoperative day. The TG was in-structed to perform 30 deep breaths with PEP hourly (three sets of 10 con-secutive deep breaths) and the CG was instructed to perform one set of 10 consecutive deep breaths with PEP hourly. Each set was documented in the medical records by the nursing staff.
22
Studies III-IV On the fourth postoperative day participants were randomly allocated, either to a treatment group (TG) or a control group (CG), through sealed enve-lopes. From the fourth to fifth postoperative day, the TG was instructed to continue with 30 deep breaths with PEP (three sets of 10 consecutive deep breaths) five times a day for two months. The CG was instructed to end the deep breathing exercises with PEP after the fourth to fifth postoperative day. All participants were contacted at home by telephone one month postopera-tively. The TG documented each training session in an exercise diary and was contacted and coached by a physiotherapist ten days after surgery for coaching of the breathing exercises.
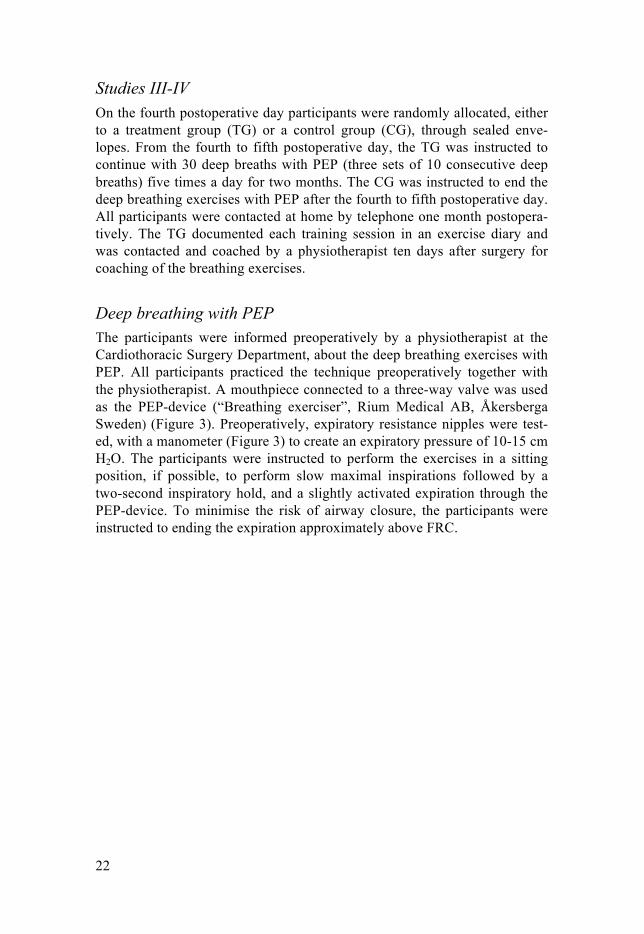
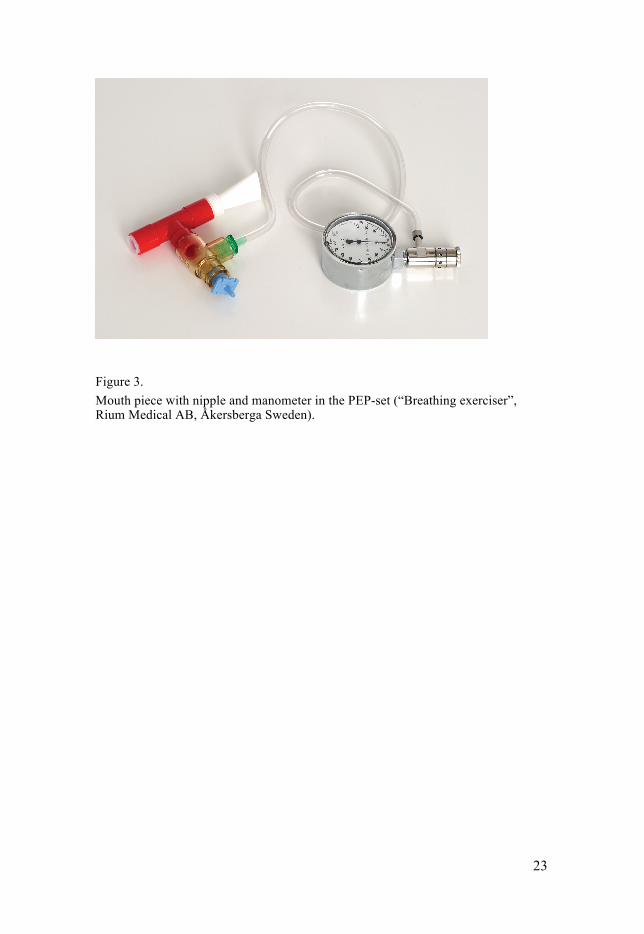
Deep breathing with PEP The participants were informed preoperatively by a physiotherapist at the Cardiothoracic Surgery Department, about the deep breathing exercises with PEP. All participants practiced the technique preoperatively together with the physiotherapist. A mouthpiece connected to a three-way valve was used as the PEP-device (“Breathing exerciser”, Rium Medical AB, Åkersberga Sweden) (Figure 3). Preoperatively, expiratory resistance nipples were test-ed, with a manometer (Figure 3) to create an expiratory pressure of 10-15 cm H2O. The participants were instructed to perform the exercises in a sitting position, if possible, to perform slow maximal inspirations followed by a two-second inspiratory hold, and a slightly activated expiration through the PEP-device. To minimise the risk of airway closure, the participants were instructed to ending the expiration approximately above FRC.
23
Figure 3. Mouth piece with nipple and manometer in the PEP-set (“Breathing exerciser”, Rium Medical AB, Åkersberga Sweden).
24
Measurements
Spirometry (Studies I-IV) In Studies I and II, lung function (VC, FVC, FEV1, IC) was measured pre-operatively and on the second postoperative day with a portable dynamic spirometry (Cardio Perfect dynamic spirometry, Welch Allyn, New York, USA). The measurements were performed at the bedside by two physiother-apists, who were unaware of the participant’s group allocation. The equip-ment was volume-calibrated every morning prior to measurement. The par-ticipants were in a sitting position and used a nose clip. The highest value of three technically satisfactory manoeuvres was retained for VC, FVC and FEV1, and the mean of three values was used for IC. The highest value of VC and FVC was used for VC in Study II.
In Studies III and IV, lung function (VC, FVC, FEV1, IC, functional residu-al capacity (FRC) and total lung capacity (TLC)) was performed preopera-tively and two months postoperatively with a Jaeger MasterScreen PFT/Bodybox (Intramedic AB, Bålsta, Sweden). The measurements were taken at the Department of Clinical Physiology, Uppsala University Hospital and Örebro University Hospital by medical laboratory technicians, who were unaware of the participant’s group allocation. The equipment was calibrated every morning prior to measurements, and during calibration room tempera-ture and barometric pressure were updated. The highest value of three tech-nically satisfactory attempts was retained.
The spirometry was standardised as described in American Thoracic Socie-ty/European Respiratory Society (ATS/ERS) ”Standardization of spirome-try” (67, 68). Predicted values for lung function were related to age, sex, height, and weight in some variables, according to the reference values re-ported by Hedenström et al. (69, 70).
Arterial blood gas (Study I) On the second postoperative day, arterial blood gas samples were drawn from arteria radialis. The participants had been without supplementary oxy-gen and did not perform the deep breathing exercises with PEP for at least 10 minutes before measurement. The analyses were performed immediately after the blood gas samples were taken. Arterial oxygen tension (PaO2),
arterial carbon dioxide tension (PaCO2), and arterial oxygen saturation (SaO2) were evaluated through ABG analyses (ABL 725, Triolab Sollen-tuna, Sweden) by a nurse at the Department of Cardiothoracic Surgery,
25
Uppsala University Hospital, and who was unaware of the participant’s group allocations.
Respiratory muscle strength (Study IV) Maximal respiratory muscle strength (measured as MIP and MEP, expressed in cm H2O) was measured preoperatively and two month postoperatively. The measurements were performed at the Department of Clinical Physiology at Uppsala University Hospital by medical laboratory technicians. The par-ticipants were in a sitting position and used a mouthpiece. The participants were instructed to hold the mouthpiece tightly in the mouth to prevent air leakage. MIP was measured near residual volume after a maximal exhalation and MEP was measured near TLC after maximal inhalation. The highest value from three technically acceptable manoeuvres was recorded. The in-spiratory- and expiratory muscle tests were standardised as described in ATS/ERS Statement on Respiratory Muscle Testing (48) and assessed by Jaeger Respiratory drive/Muscle strength (Intramedic, Bålsta, Sweden). Pre-dicted values for MIP and MEP were adjusted for age and gender (47).
Sternal pain (Studies I-IV) Sternal pain was quantified on a numeric rating scale (NRS) (71) on the se-cond postoperative day (Studies I-II) and two months after surgery (Studies III-IV). The NRS rates were from 0 (no pain) to 10 (the worst imaginable pain). In Studies I and II the participants rated their sternal pain at rest, while taking a deep breath, while performing deep breathing exercises with PEP, while coughing, and while moving from lying to sitting. In Studies III and IV, the participants rated their pain at rest, while taking a deep breath and while coughing. The validity of NRS for pain intensity has good sensi-tivity with expected pain intensity change (72).
Patient-perceived quality of recovery (Study III) Patient-perceived quality of recovery was assessed through a Swedish ver-sion of quality of recovery score (QoR-40), which is designed to measure the patient’s recovery after surgery and anaesthesia. QoR-40 was measured on the fourth postoperative day and two months after surgery. The QoR-40 is a self-administrated 40-item score measuring five dimensions: physical com-fort, emotional status, physical independence, psychological independence and pain. Each item is rated on a five-point Likert scale (for positive items: 1=none of the time, 5= all of the time: for negative items, the scoring was reversed). The possible score on QoR-40 is from 40 (extremely poor quality of recovery) to 200 (excellent quality of recovery) (73, 74). The validity,

26
reliability, and clinical acceptability of QoR-40 are reported to be good in patients undergoing surgery and general anaesthesia (74).
Health-related quality of life (Study III) Health-related quality of life (HRQoL) was measured through a Swedish version of Short Form-36 (SF-36) (first version) both preoperatively and two months after surgery (75-77). The SF-36 compromising 36 items across eight dimensions: physical functioning (PF), role limitation due to physical problems (RP), bodily pain (BP), general health (GH), vitality (VT), social functioning (SF), role limitation due to emotional problems (RE) and mental health (MH). The responses to each question within one dimension are com-bined to generate a score from 0 to 100, with higher scores indicating better health. In addition, the questionnaire comprises two main domains physical health (PF, RP, BP, GH) and mental health (VT, SF, RE, MH). SF-36 is a self- administrated questionnaire and is widely used in various countries (78). The Swedish version of SF-36 has good reliability and construct validi-ty across general populations (75). Furthermore, SF-36 has established relia-bility and validity for patients with coronary artery disease (79).
Subjective experience of breathing and oxygen saturation (Studies III and IV) The participants were asked to describe their breathing ability two months after surgery compared to their preoperative breathing ability (improved, unaltered or impaired) (Studies III-IV). Two months postoperatively, the participants in the treatment group in Study III, were asked to score their subjective benefit and/or discomfort of the breathing exercises performed during the postoperative period. Answers were recorded on an arbitrary scale from 0 (not at all) to 3 (very much). The participants were asked to give in-formation on assumed respiratory tract infections/pneumonia and antibiotic treatments during the study period.
Saturation of peripheral oxygen (SpO2) was measured by a handheld pulse-oximetry (Rad-5v Handheld, Masimo, Irvine, USA) with a probe on the par-ticipant’s finger preoperatively and two months after surgery in Studies III and IV.
Thoracic excursion (Study III) Thoracic excursions were measured with a tape (marked in mm) around the circumference of the chest to provide a measure of chest expansion or mobil-ity preoperatively and at two months after surgery. Thoracic excursions were

27
measured at the level of the xiphoid process, performed with the participants standing with their hands placed on their head and given the instructions ‘Breathe in maximally and make yourself as big as possible’ and ‘Breathe out maximally and make yourself as small as possible’ (80). Thoracic excur-sion measured as difference in size of thorax between inspiration and expira-tion was recorded. This method of measuring thoracic excursion is shown to be reliable in healthy volunteers (81). Demographic and descriptive data were collected from medical record or reported by the participant.
28
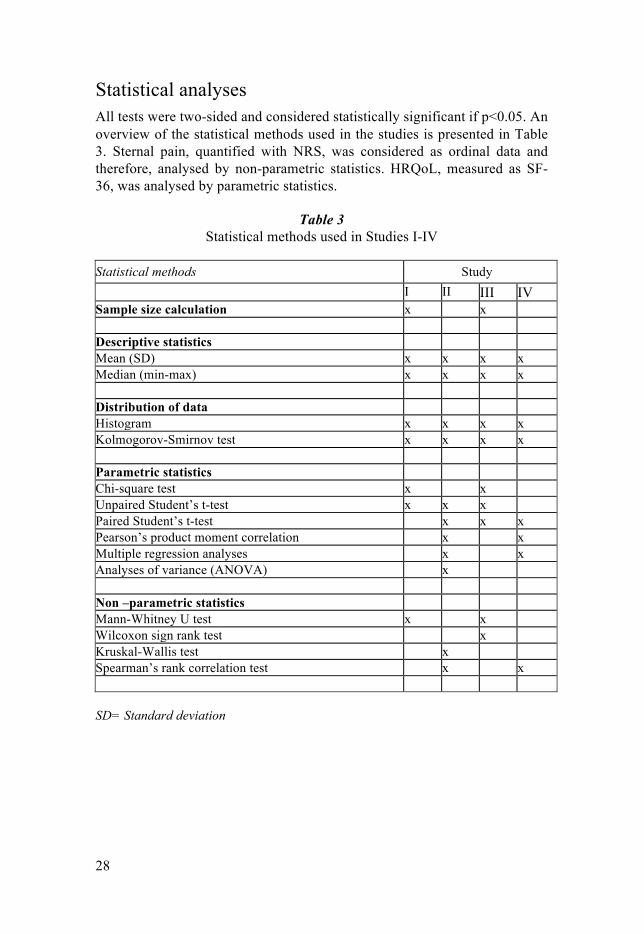
Statistical analyses All tests were two-sided and considered statistically significant if p<0.05. An overview of the statistical methods used in the studies is presented in Table 3. Sternal pain, quantified with NRS, was considered as ordinal data and therefore, analysed by non-parametric statistics. HRQoL, measured as SF-36, was analysed by parametric statistics.
Table 3
Statistical methods used in Studies I-IV Statistical methods Study I II III IV Sample size calculation x x Descriptive statistics Mean (SD) x x x x Median (min-max) x x x x Distribution of data Histogram x x x x Kolmogorov-Smirnov test x x x x Parametric statistics Chi-square test x x Unpaired Student’s t-test x x x Paired Student’s t-test x x x Pearson’s product moment correlation x x Multiple regression analyses x x Analyses of variance (ANOVA) x Non –parametric statistics Mann-Whitney U test x x Wilcoxon sign rank test x Kruskal-Wallis test x Spearman’s rank correlation test x x SD= Standard deviation
29
Sample size calculation To obtain a power of 80% in Study I, a sample size of 63 participants in each group was needed to detect a difference of 0.5 kPa in PaO2 between groups, assuming an SD of 1 kPa. The mean difference between groups in Study I was based on absolute values of PaO2, on the second postoperative day.
To obtain a power of 80% in Study III, a sample size of 160 participants in each group was needed to detect a 10% difference in FEV1, assuming a SD of 25% two months after surgery. The mean difference between groups in Study III was based on the relative change (postoperative value in % of preoperative value) in each group.
Descriptive statistics In all studies, descriptive statistics were used for demographic data. Contin-uous variables were presented as mean and standard deviation (SD). For ordinal data, the median, minimal and maximal values were presented. For nominal data, absolute or relative numbers (%) or both were described. The distribution of data, was evaluated with the Kolmogorov-Smirnov test and histograms.
Parametric statistics Chi-Square tests were used when analysing groups of nominal data at base-line (Studies I and III). Unpaired Student’s t-test was used in Studies I and III when analysing continuous variables between treatment and control group, and in Study II when calculating the stratified analyses between two subgroups (Gender, BMI >25 versus ≤ 25). In Studies II, III and IV, paired Student’s t-test was used for analyses of paired observations of continuous variables. The univariate analyses of continuous data in Studies II and IV were calculated with Pearson’s product moment correlation. In Study II, dependent variables were postoperative VC, FEV1 and IC and independent variables were both pre-, peri- and of postoperative character. If an inde-pendent variable was associated with impairment in VC, FEV1 or IC in the univariate analyses with a p≤0.1, it was included in the forward multiple regression analyses in Study II. The dependent variable in Study IV was postoperative MIP and the independent variables were age and BMI. ANO-VA was used to analyse differences between more than two subgroups (age and pain groups) in Study II.

30
Non- parametric statistics Mann-Whitney U test was used to analyse ordinal data between groups in Studies I and III, Wilcoxon sign rank test was used for analysing of paired observations of ordinal data (Study III), and Kruskal-Wallis test was used for analysing differences between different age groups and sternal pain (Study II). Correlation between ordinal data variables was assessed by Spearman’s rank correlation test (Studies II and IV).
31
Results
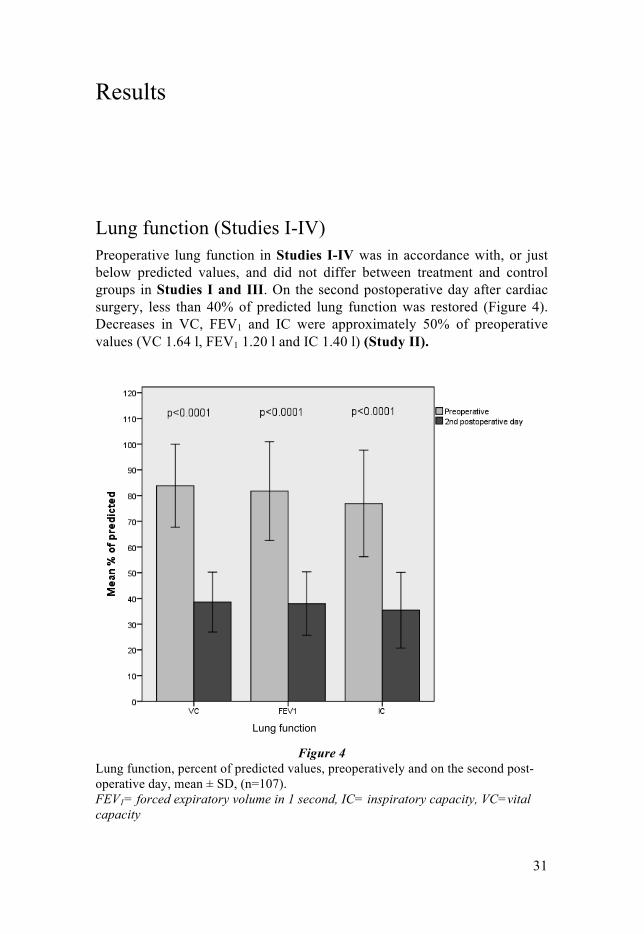
Lung function (Studies I-IV) Preoperative lung function in Studies I-IV was in accordance with, or just below predicted values, and did not differ between treatment and control groups in Studies I and III. On the second postoperative day after cardiac surgery, less than 40% of predicted lung function was restored (Figure 4). Decreases in VC, FEV1 and IC were approximately 50% of preoperative values (VC 1.64 l, FEV1 1.20 l and IC 1.40 l) (Study II).
Figure 4 Lung function, percent of predicted values, preoperatively and on the second post-operative day, mean ± SD, (n=107). FEV1= forced expiratory volume in 1 second, IC= inspiratory capacity, VC=vital capacity
Lung function
32
Lung function values on the second postoperative day did not differ between the treatment group performing 30 deep breaths with PEP hourly and the control group performing 10 deep breaths with PEP (Study I).
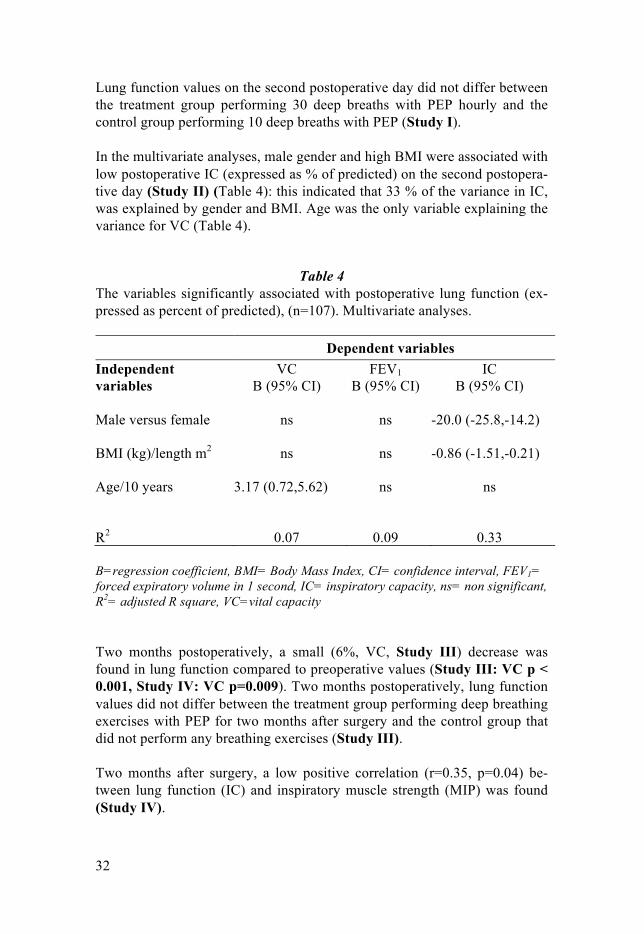
In the multivariate analyses, male gender and high BMI were associated with low postoperative IC (expressed as % of predicted) on the second postopera-tive day (Study II) (Table 4): this indicated that 33 % of the variance in IC, was explained by gender and BMI. Age was the only variable explaining the variance for VC (Table 4).
Table 4
The variables significantly associated with postoperative lung function (ex-pressed as percent of predicted), (n=107). Multivariate analyses. Dependent variables Independent variables
VC B (95% CI)
FEV1 B (95% CI)
IC B (95% CI)
Male versus female ns ns -20.0 (-25.8,-14.2)
BMI (kg)/length m2 ns ns -0.86 (-1.51,-0.21)
Age/10 years 3.17 (0.72,5.62) ns ns
R2 0.07 0.09 0.33 B=regression coefficient, BMI= Body Mass Index, CI= confidence interval, FEV1= forced expiratory volume in 1 second, IC= inspiratory capacity, ns= non significant, R2= adjusted R square, VC=vital capacity Two months postoperatively, a small (6%, VC, Study III) decrease was found in lung function compared to preoperative values (Study III: VC p < 0.001, Study IV: VC p=0.009). Two months postoperatively, lung function values did not differ between the treatment group performing deep breathing exercises with PEP for two months after surgery and the control group that did not perform any breathing exercises (Study III).
Two months after surgery, a low positive correlation (r=0.35, p=0.04) be-tween lung function (IC) and inspiratory muscle strength (MIP) was found (Study IV).
33
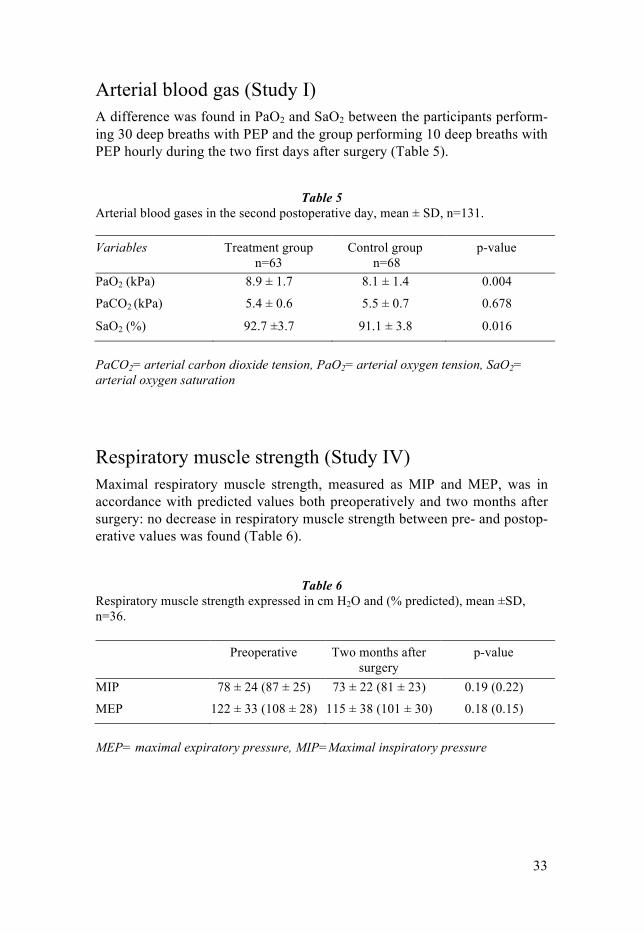
Arterial blood gas (Study I) A difference was found in PaO2 and SaO2 between the participants perform-ing 30 deep breaths with PEP and the group performing 10 deep breaths with PEP hourly during the two first days after surgery (Table 5).
Table 5
Arterial blood gases in the second postoperative day, mean ± SD, n=131. Variables
Treatment group n=63
Control group n=68
p-value
PaO2 (kPa)
8.9 ± 1.7 8.1 ± 1.4 0.004
PaCO2 (kPa)
5.4 ± 0.6 5.5 ± 0.7 0.678
SaO2 (%)
92.7 ±3.7 91.1 ± 3.8 0.016
PaCO2= arterial carbon dioxide tension, PaO2= arterial oxygen tension, SaO2= arterial oxygen saturation
Respiratory muscle strength (Study IV) Maximal respiratory muscle strength, measured as MIP and MEP, was in accordance with predicted values both preoperatively and two months after surgery: no decrease in respiratory muscle strength between pre- and postop-erative values was found (Table 6).
Table 6 Respiratory muscle strength expressed in cm H2O and (% predicted), mean ±SD, n=36. Preoperative Two months after
surgery p-value
MIP 78 ± 24 (87 ± 25) 73 ± 22 (81 ± 23) 0.19 (0.22) MEP 122 ± 33 (108 ± 28) 115 ± 38 (101 ± 30) 0.18 (0.15)
MEP= maximal expiratory pressure, MIP=Maximal inspiratory pressure
34
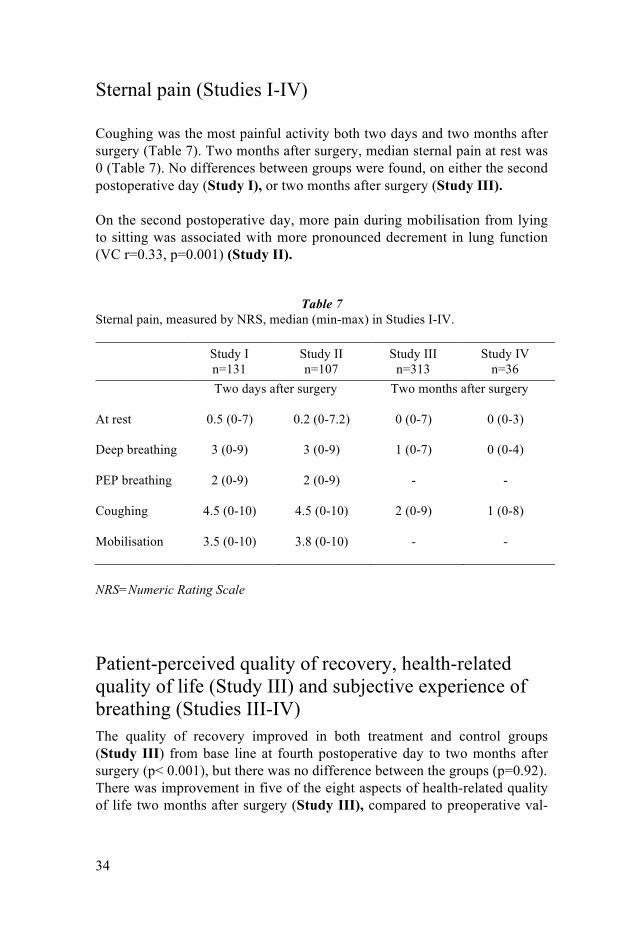
Sternal pain (Studies I-IV) Coughing was the most painful activity both two days and two months after surgery (Table 7). Two months after surgery, median sternal pain at rest was 0 (Table 7). No differences between groups were found, on either the second postoperative day (Study I), or two months after surgery (Study III).
On the second postoperative day, more pain during mobilisation from lying to sitting was associated with more pronounced decrement in lung function (VC r=0.33, p=0.001) (Study II).
Table 7 Sternal pain, measured by NRS, median (min-max) in Studies I-IV. Study I
n=131 Study II n=107
Study III n=313
Study IV n=36
Two days after surgery Two months after surgery At rest 0.5 (0-7) 0.2 (0-7.2) 0 (0-7) 0 (0-3)
Deep breathing 3 (0-9) 3 (0-9) 1 (0-7) 0 (0-4)
PEP breathing 2 (0-9) 2 (0-9) - -
Coughing 4.5 (0-10) 4.5 (0-10) 2 (0-9) 1 (0-8)
Mobilisation 3.5 (0-10) 3.8 (0-10) - -
NRS=Numeric Rating Scale
Patient-perceived quality of recovery, health-related quality of life (Study III) and subjective experience of breathing (Studies III-IV) The quality of recovery improved in both treatment and control groups (Study III) from base line at fourth postoperative day to two months after surgery (p< 0.001), but there was no difference between the groups (p=0.92). There was improvement in five of the eight aspects of health-related quality of life two months after surgery (Study III), compared to preoperative val-
35
ues, but no differences between the treatment and the control groups were found (p=0.14-0.74).
Experience of breathing ability improved two months after surgery com-pared to before surgery, in approximately 50% of the participants (Studies III-IV).
In the treatment group, 72% experienced subjective benefit from the exercis-es, 5% found no benefit and 23% of participants had no opinion. Discomfort related to the breathing exercises was reported by 2% to a high degree and 17% to some extent. The adverse experience given were related to increased pain and dizziness (Study III).
Oxygen saturation (Studies III, IV), thoracic excursion (Study III), and postoperative pulmonary infections (Study III) Oxygenation, measured as SpO2, was above 97% both before surgery and two months postoperatively (Studies III and IV) and there was no differ-ence between treatment and control groups in study III (p=0.66).
There were no differences regarding thoracic excursion, either within groups from pre- to two months postoperatively, or between groups at the two-month follow-up (p=0.55) (Study III).
Two months after surgery, 13 participants in the treatment group and 15 participants in the control group reported respiratory infection or pneumonia after surgery (p= 0.60). The self-reported use of antibiotic treatment for res-piratory infection/pneumonia was n=6 in the treatment group, and n=13 in the control group (p= 0.07) (Study III). In Study I, compliance with the breathing exercises did not differ between the treatment and control groups, and on average, 65 ± 5% of the possible sessions were carried out. In Study III, the participants in the treatment group reported they performed the breathing exercises 4 ± 3 times (min-max 3-5) a day postoperatively and each session consisted of 23 ± 12 (min-max 3-60) breaths.

36
Discussion
Participants performing 30 deep breaths with a PEP device hourly had higher PaO2 and SaO2 than participants performing 10 deep breaths with a PEP device hourly the two fist days after cardiac surgery. Participants who con-tinued the breathing exercises for two months after surgery had no positive effects on lung function, oxygenation, HRQoL, quality of recovery or sub-jective breathing ability, compared to a control group without breathing in-structions after the fourth to fifth postoperative day.
Preoperatively, lung function and respiratory muscle strength were in ac-cordance with predicted values. Two days after surgery, the lung function was reduced to 50% of preoperative values and two months after surgery a small, 6%, reduction of preoperative values was found. Two months after surgery, respiratory muscle strength was in accordance with predicted val-ues.
Effects of deep breathing exercises with PEP The deep breathing exercises with PEP used in this thesis, were considered to slow down expiration and increase lung volume, and might have prevent-ed or reduced airway collapse. However, there is scarce scientific evidence that breathing exercises with PEP are superior to other breathing exercises in patients undergoing abdominal or thoracic surgery (82). A combination of initial deep inspiration with an expiratory resistance could possibly extend the time with higher lung volume, which may help expand and maintain alveolar and airway patency and re-expansion of atelectasis, as previously demonstrated in the in-hospital phase (12, 23). After cardiac surgery the PEP technique has been combined with incentive spirometry (IS) with positive outcomes on lung function, a 6-minute walking distance, and postoperative pulmonary impairments as well as dyspnea and HRQoL (SF-36) both one, and 18 months after cardiac surgery (50, 62). The hypothesis in Study I was that a duration of 30 deep breaths (treatment group) with PEP hourly during the two first days after surgery increased oxygenation and lung function, compared to 10 deep breaths hourly (control group). This statement was based on a previous study in which 30 deep

37
breaths with PEP reduced the atelectatic area and improved the lung function compared to no deep breathing exercises during the first days after cardiac surgery (12). As expected, the treatment group had higher levels of oxygena-tion than the control group. The duration of 10 and 30 deep breaths with PEP was chosen according to ordinary routines in Sweden (19). Although the absolute difference in PaO2 between the groups was 0.8 kPa and the impair-ment could be considered small, it could be important because it was posi-tioned in the steep part of the oxygen dissociation curve. Thus, the difference was considered clinically relevant. Alveolar recruitment and re-expansion of lung tissue, due to a longer period at higher volumes, could be a possible explanation as of why an intensified intervention can increase oxygenation. Rothen et al. (83) demonstrate instant re-expansion of collapsed lung tissue with one VC manoeuvre in anaesthetised subjects, however arterial oxygena-tion can be influenced by non-pulmonary factors, such as cardiac output and efficiency of hypoxic pulmonary vasoconstriction, even if this was not the focus of the present study. Although oxygenation (PaO2, SaO2) differed between the groups in Study I, lung function did not differ. One explanation could be the dynamic spirome-try measured maximal lung function capacity (VC, FVC, FEV1, IC) but oxy-genation reflected the volume patient breaths within each breath (tidal vol-ume). A second explanation could be hyperhydration, which might influence oxygenation but not the lung function. A third explanation could be reduced reliability of the spirometry, which requires cooperation from the partici-pants. Currently, there is no scientific documentation of how long after the surgery patients should continue breathing exercises, or which kind of breathing exercises are most beneficial: the recommendations between hospitals vary (19). The aim of Study III was to evaluate the effectiveness of home-based deep breathing exercises performed with a PEP device during the first two months after cardiac surgery. The hypothesis was deep breathing exercises performed during the first two months after cardiac surgery would decrease pulmonary impairments and improve patient-perceived quality of recovery and HRQoL. The results from the present study indicated home-based deep breathing exercises two months after cardiac surgery had no effect on pul-monary impairments and improve patient-perceived quality of recovery and HRQoL, compared to a regime without breathing exercises after the fourth to fifth postoperative day.
Two studies have evaluated breathing exercises performed after discharge (50, 62). Haeffener et al. (62) and Ferreira et al. (50) have evaluated incen-tive spirometry (IS) combined with PEP from the first postoperative day to one month postoperatively and found improvement in lung function (62),

38
sensation of dyspnea after 6 minute walking test, and improved HRQoL, measured as the physical dimension of SF-36 (50). The positive effects achieved in the studies by Haeffener et al. (62) and Ferreira et al (50) could be attributed to the use of IS, which helps the patient visualise the inspiratory volume. However, Hirschorn et al. (84) found no effects of a walk-ing/breathing exercise intervention on vital capacity or HRQoL four weeks after discharge. Deep breathing exercises in the early postoperative period have positive effects on atelectasis (12, 23), oxygenation (23), lung function (12) and length of in-hospital stay (18). As a gradual spontaneous recovery of lung function occurs after surgery, breathing exercises might not provide any additional effect two months after surgery. The gradual increase in daily activities expected after cardiac surgery might also lower the effects of breathing exercises. An increased frequency or intensity in exercises is likely to be more efficacious, but as 150 breaths a day were performed if the pa-tients followed the instructions, the recommendation of frequency was con-sidered feasible. However, subgroups of patients who are not able to be as physically active as recommended, i.e. patients with a lung disease, smoking history, advanced age, or obesity need to be investigated. Two months postoperatively, there was improvement in five of the eight aspects of SF-36 in both groups (Study III) compared to preoperative values. However, there were no differences between the treatment and control groups after two months for HRQoL (Study III). These results are in accord-ance with healthy people of the same age (77). Although physical and mental components of HRQoL (SF-36) are reported to improve from before surgery to three months postoperatively in cardiac surgery patients (85), further stud-ies are needed to investigate the relationship between HRQoL and lung func-tion in these patients.
Compliance with the breathing exercises During the two first days after surgery (Study I), compliance with breathing exercises did not differ between the groups: on average, 65 ± 5% of the pos-sible sessions were carried out. The participants were instructed and remind-ed to perform the breathing exercises every hour they were awake. If a par-ticipant was unable to perform the deep breathing exercises, or had a feeling of sickness, a member of the staff returned to the patient 15 min later to coach the participant to perform the breathing exercises again. With this kind of supervised treatment, an expected high level of compliance was found. The most common reason for not performing the breathing exercises was tiredness. One limitation might be the non-control of the intensity of the

39
deep breaths. Even though participants had sternal pain in the first days after surgery compliance with the breathing exercises was good.
In Study III, the participants were supposed to perform the breathing exer-cises at home for two months. The participants stated they had performed the deep breathing exercises 4 ± 3 times a day postoperatively and each session had consisted of 23 ± 12 breaths. Almost all participants in the treatment group reported the breathing technique was easy to perform. One reason for the lack of effect of the home-based exercises may be compliance with the breathing exercises. Even though participants in the treatment group docu-mented compliance with treatment in an exercise diary, the overall extent of individual training was not possible to monitor. The breathing exercises might have had an effect if they were actually performed according to the protocol. On discharge, participants were instructed in the deep breathing performance but they were not supervised on how to perform the deep breathing exercises at home, and this might contribute to the lack of differ-ences between the groups. Unsupported home-based training could be diffi-cult to comply. In home-based pulmonary rehabilitation programs for pa-tients with COPD 23-31% of participants drop out (86). In Study III, all par-ticipants in the treatment group were contacted by telephone by a physical therapist 2 times during the treatment period. In a study by Ferreira et al (50), the patients were weekly contacted by telephone during the study peri-od, in order to emphasize the importance of executing the exercises. Telep-hone supporting appeared to be an effective strategy to improve adherence in home-based cardiac rehabilitation (87). In the future, telemedicine could perhaps help to individualise the breathing exercises for participants.
Preoperative lung function and respiratory muscle strength Preoperative lung function in the present studies was in accordance with predicted values (69, 70). The importance of preoperative lung function on the development of postoperative pulmonary impairment is unclear. Mortali-ty rate associated with cardiac surgery is not influenced by the presence and severity of airflow obstruction in patients with COPD, but the incidence of pneumonia and length of hospital stay increase in patients with severe air-flow obstruction (28, 88). For respiratory muscle strength, MIP was 87% and MEP was 108% (ex-pressed as percent of predicted value before surgery) (47). Previous studies have reported similar preoperative values for MIP (13, 44) but lower levels for MEP (13, 44, 49). The variation in MEP values between studies could be

40
due to differences between the groups studied and the way in which the tests were performed. Few data is reported about the impact of respiratory muscle strength in the preoperative period (49). Rodrigues et al. (49) report an asso-ciation between MIP or MEP below 70% of predicted value (89) and the need for prolonged invasive mechanical ventilation after cardiac surgery. In elective thoracotomy and laparotomies of the upper abdomen preoperative respiratory muscle strength above 75% of predicted values (89) appears to be protective against postoperative pulmonary complications (90). However, further studies are needed to investigate whether preoperative respiratory muscle strength can be used to identify risk patients for postoperative pul-monary impairments.
Although it is possible to increase the respiratory muscle strength preopera-tively in cardiac surgery patients (91-93), the postoperative benefits are un-clear. In addition, it is unclear whether inspiratory muscle training (IMT) for patients with verified inspiratory muscle weakness would be more beneficial than for patients without muscle weakness. Thus, further studies investigat-ing if, how, and in which cardiac surgery patients, preoperative IMT would be of benefit are needed.
Postoperative lung function and respiratory muscle strength Reduced lung function affects gas exchange, and there is an inverse correla-tion between atelectasis area and arterial oxygenation (PaO2) during the first postoperative days after cardiac surgery (11, 12). Pulmonary impairments after cardiac surgery create problems and are an important cause of postop-erative morbidity.
On the second postoperative day, the 50% decrease in lung function was in accordance with previous studies (8, 9). The causes of reduced lung function are multifactorial and involve a combination of surgery, anaesthesia, immo-bilisation and pain (31-33, 36). The levels of sternal pain in the first postop-erative days were lower than reported in previous studies (31, 40, 42), possi-ble because of the individual pain analgesics regime and early mobilisation. Postoperative pain may be associated with changes in the thorax mechanism, although changes in thoracic excursion were not evaluated on the second postoperative day. Increased sternal pain was associated with more pro-nounced decrement in lung function, which was in accordance with another study (41).

41
Even though lung function was decreased two months after cardiac surgery, respiratory muscle strength was not: There was a non-significant reduction in MIP and MEP to 94% of preoperative values. In the early postoperative period, decrement in respiratory muscle strength is reported: Riedi et al. (94) demonstrate an 11% reduction in MIP five days after surgery, and Morsch et al. (44) report a 36% reduction of MIP six days after surgery, compared to preoperative values. One month after cardiac surgery, Stein et al. (63) evalu-ated a six-day rehabilitation program and found almost recovered MIP. One explanation for the reduced respiratory muscle strength in the early postop-erative period after cardiac surgery might be sternal pain, which affects the possibility of performing the muscle strength test properly. The finding of recovered respiratory muscle strength two months after cardiac surgery agreed with results one and 18 months after surgery (50, 63): however, it is still unclear if, and how, muscle strength is affected by surgery. One expla-nation for the recovery of muscle strength at the two month follow-up might be decreased sternal pain levels or an assumed less sedentary behaviour. A positive correlation between the level of activity in daily life and respiratory muscle strength is reported in healthy elderly population (95). Participants had less pain at the two month follow-up, however, physical level or seden-tary behaviour was not assessed.
Although, there was a small reduction in respiratory muscle strength (6%), and the values were in accordance with predicted values at the two months follow-up. This decrease was not statistically significant, but might be useful when treating patients with severe lung function impairment or other mor-bidities. The low correlation between MIP and VC, FEV1, IC, two months after sur-gery supported respiratory muscle strength and lung function are interrelat-ed: a linear association between MIP and FVC is also reported in healthy men (96) and patients two weeks after cardiac surgery (97). However, fur-ther studies are needed to investigate the relationship between lung function and respiratory muscle strength.
Methodological considerations In evaluation the effects of breathing exercises the focus was primarily on lung function and oxygenation, as in previous studies (7, 12, 13, 18, 62, 98). For practical reasons, lung function was evaluated at the bedside with dy-namic spirometry (Study I). However, with dynamic spirometry, FRC could not be measured, which might have been the most important parameter to measure, as it might reflect the normal breathing in each breath. Further-more, the evaluation of oxygenation through arterial blood gas (ABG), was
42
chosen because this is a direct measure of PaO2, SaO2, and PaCo2 (Study I). ABG was measured two days after cardiac surgery and compared between the groups. ABG before surgery was not practical, as the arterial needle was inserted before surgery when sedation already started. As the between-individual difference in ABG is small, only postoperative measurement was considered appropriate. Puls-oximetry was chosen to measure SpO2, as both the pre and postopera-tive SpO2 values were measured outside of the ICU (Studies III and IV). Pulse-oximetry is accurate in the 70-100% saturation range, where readings do not usually vary more than 1-2% from the measurements obtained by blood gas analysis (99). An uncertainty, of magnitude of 2%, in the 80-100% SpO2 interval has been reported (100). The reference values chosen for lung function were developed by Hedenstrom et al (69, 70) and are used in Sweden: these values are based on gender, age and height, and weight in some variables (69, 70). The reference values for MIP and MEP (Study IV) were based on Evans et al (47). Evans et al (47), who combined results from other published refer-ence values (89, 101-103) to obtain one regression equation for MIP and one for MEP depending on age, but separate for gender. However, it is important to consider that “normal values” differ between different reference values particularly with MIP and MEP where the normal range is wide (48). The first and second days after cardiac surgery are critical, and avoiding a return to mechanical ventilation is important. Mobilisation in bed and to sitting and walking is vital for preventing pulmonary impairment in the im-mediate postoperative care (104). Breathing exercises are important for re-covery especially for immobilised patients, and maybe necessary for a quicker rehabilitation. Therefore, evaluation of the duration of deep breath-ing exercises with PEP on the second postoperative day was chosen (Study I). In studies III and IV, home-based breathing exercises and respiratory muscle strength were evaluated. As both lung function and respiratory muscle strength are influenced by postoperative pain and restricted thoracic move-ment (31, 35, 41) and because the healing of the sternum these values were evaluated two months postoperatively. External validity Participant characteristics in the four studies were similar to the Swedish population of cardiac surgery patients (2): therefore the external validity of
43
the results were considered to be good. In international studies (6, 49, 62) the samples included younger adults and a greater part of smoking participants. In all four studies, the seriously unwell patients were not included, as the aim was to describe and evaluate deep breathing exercises with PEP in uncom-plicated patients, and the selection should be representative. As none of the studies was designed to evaluate subgroups additional studies are required to study groups of special interest.
Clinical implications and further research The findings from these studies suggest a higher duration of deep breathing exercises with PEP in the first days after cardiac surgery to improve oxygen-ation. Therefore, duration of 30 deep breaths is recommended as a part of standard care for elective cardiac surgery patients, in addition to mobilisation in the first postoperative days. In clinical practice, and to improve the com-pliance, the staff has an important role in reminding patients to perform the breathing exercises every hour, it is recommended that each session is rec-orded in a diary. The breathing exercises with PEP were well tolerated and PEP is a cheap breathing device to use. The home-based breathing exercise program was also well tolerated, but did not demonstrate any difference in lung function, oxygenation, HRQoL, qual-ity of recovery or subjective breathing ability, compared to a control group two months after cardiac surgery. Further studies are needed to investigate the effects of breathing exercises after discharge, as contra indicative results of home-based breathing exercises have been presented (50, 62). Further studies of subgroups i.e. patients with lung disease, smoking history, ad-vanced age, or obesity would be beneficial for evaluating whether postopera-tive home-based breathing exercises are beneficial for these groups. Im-provements in anaesthesiological and surgical techniques may result in shorter hospital stay (105) and therefore a greater responsibility for the reha-bilitation is likely to be home-based. The growing number of older and chronically ill patients is a challenge to surgery and postoperative rehabilita-tion, and further research should be designed to identify patients who would benefit the most from breathing interventions after discharge. High BMI and pain are risk factors for decreased lung function on the se-cond postoperative day: therefore, patients with high BMI should receive extra attention during postoperative care. As pain is related to a larger de-crease in postoperative lung function, optimal pain relief is important. Cardiac surgery patients have respiratory muscle strength in accordance with predicted values both before and two months after surgery. Two months

44
after surgery, there is a low correlation between maximal inspiratory strength and lung function. However, further studies are needed to investigate wheth-er patients with low respiratory muscle strength benefit from inspiratory muscle training and for further analysis of the relationship between respira-tory muscle strength and lung function.
45
Conclusions
• After cardiac surgery, performing 30 deep breaths hourly with PEP during the first two postoperative days improves oxygenation more than performing 10 deep breaths with PEP hourly.
• Home-based deep breathing exercises with PEP performed five times a day (30 breaths every session) for two months after cardiac surgery does not improve lung function, oxygenation, health-related quality of life, quality of recovery, or subjective breathing ability.
• Lung function is decreased by 50%, and is less than 40% of predictive values on the second postoperative day after cardiac surgery. Patients with high BMI are a risk group for decreased postoperative lung function and pain is related to a larger decrease in lung function two days after surgery.
• Respiratory muscle strength is not impaired either before or two months after cardiac surgery. Two months postoperatively, there is a low correlation between maximal inspiratory muscle strength and lung function.
46
Sammanfattning på svenska
Lungfunktion, andningsmuskelstyrka och effekter av andningsövningar hos personer som genomgår hjärt-kirurgi Sjukgymnastiska insatser i vården av patienter som genomgår hjärtkirurgi handlar om att förebygga och lindra effekterna av de lungfunktionsned-sättningar som uppstår i samband med operationen. Mobilisering lyfts ofta fram som förstahandsalternativ och till detta adderas andningsövningar, framförallt under den första postoperativa perioden.
En av de vanligast förekommande andningsövningarna, i det postoperativa förloppet, i Sverige, är djupandningsövningar med motstånd på utandningen (Positive Expiratory pressure, PEP). Det är oklart med vilken duration, under de första postoperativa dagarna, andningsövningarna bör utföras. Inte heller är det klarlagt hur länge patienterna bör fortsätta utföra andningsövningar efter de fyra första postoperativa dagarna. Lungfunktionen är nedsatt initialt efter det kirurgiska ingreppet men också flera månader efteråt. Andningsmuskelstyrkan har rapporterats vara nedsatt den första veckan efter operationen men endast ett fåtal studier har studerat andningsmuskelstyrkan i efterförloppet efter hjärtoperation. Det övergripande syftet med avhandlingen var att utvärdera effekten av dju-pandningsövningar med PEP och beskriva lungfunktion och andningsmus-kelstyrka hos personer som genomgått hjärtkirurgi. I det första delarbetet utvärderades effekten av olika duration av djup-andningsövningar med PEP de två första dagarna efter operationen. I delar-bete II beskrevs lungfunktionen samt faktorer som påverkat lungfunktionen två dagar efter operationen. I delarbete III utvärderades effekten av djup-andningsövningarna med PEP utförda från och med den 4-5:e postoperativa dagen och under två månader. I delarbete IV studerades andningsmuskel-styrkan före och två månader efter operationen.

47
De huvudsakliga fynden i de två randomiserade delarbetena (I och III) var att 30 djupa andetag med utandning mot motstånd (PEP) varje vaken timme, förbättrar PaO2 och SaO2 i jämförelse med om 10 djupa andetag med PEP genomfördes varje vaken timme under de två första dagarna efter operation-en. En högre duration av djupandningsövningar med PEP kan rekommende-ras de två första dagarna efter hjärtkirurgi till patienter som genomgår elektiv hjärtkirurgi.
Vidare kunde ingen skillnad i lungfunktion, SpO2, hälsorelaterad livskvalitet, återhämtning efter operation eller upplevelse av andningen påvisas hos den grupp som fortsatt med andningsövningarna efter den fjärde postoperativa dagen och två månader framöver i jämförelse med en icke-behandlad kon-trollgrupp. Fler studier behövs för att utvärdera effekterna av andningsöv-ningar efter att patienterna har lämnat sjukhuset, eftersom motstridiga resul-tat har rapporterats. De huvudsakliga fynden i de två deskriptiva delarbetena (II och IV) i av-handlingen visar att personer som genomgått elektiv hjärtkirurgi har en sänkt lungfunktion med 50 % och att endast 40 % av de förväntade värdena åter-står två dagar efter operationen. Personer med högt BMI eller smärta från bröstbenet har en mer uttalad lungfunktionsnedsättning än andra. Vidare påvisar resultaten att andningsmuskelstyrkan är i nivå med de förväntade värdena både före och två månader efter operationen. En svag korrelation mellan andningsmuskelstyrka och lungfunktion påvisades två månader post-operativt.
48
Acknowledgements
Jag vill rikta ett stort tack till alla personer som hjälpt mig under forskarutbildningen och i genomförandet av denna avhandling. Tack också alla patienter som deltagit i studierna. Det har varit en otroligt lärorik period på många sätt. Tack …..mina tre handledare: Margareta Emtner, Elisabeth Westerdahl och Hans Hedenström. Ni har tillsammans delat med er, på ett mycket generöst sätt, av er tid och er stora vetenskapliga kunskap. Ni har alltid visat stort engagemang! Margareta, Du har med Din energi, driftighet och alltid posi-tiva syn på vad jag presterat stärkt mig i att våga driva själv och tänka stort. Elisabeth, Du har i den vetenskapliga processen visat mig vikten av nog-grannhet, eftertänksamhet och detaljerna. Hans, Du har med Ditt lugn, Din ödmjukhet och Ditt stora kunnande inom lungfunktionsområdet alltid gjort att jag känt mig tillfreds då jag lämnat våra träffar. Utan er hade detta givetvis inte varit möjligt! …..all personal på avdelning 50B och 50D, Akademiska sjukhuset under ledning av Marie Foconi och Maria Holwaster. Ni har alltid varit positiva till att genomföra forskning i vardagsarbetet. Speciellt tack till underskö-terska Ulrika Eriksson som alltid funnits till hands på 50D. Du har givit mig ovärderlig hjälp under datainsamlingsperioderna och alltid varit klok och enormt pålitlig. …..alla BMA på avdelningen för Klinisk Fysiologi, Akademiska sjukhu-set, som genomfört lungfunktionsundersökningar i studie III och IV. Ni har alltid på ett positivt sätt bemött mig och deltagarna i studierna. ….. personalen på Enheten för Lungmedicin och Allergologi, Uppsala Universitet, för bra arrangemang kring våra gemensamma konferensresor. …..Sektionen för Logopedi, Sjukgymnastik och Arbetsterapi, Akad-emiska sjukhuset under ledning av Marianne Christensen som möjliggjort för mig att förena kliniskt arbete med forskning. Jag vill rikta ett speciellt tack till ”Akutgruppen” under ledning av Ulrika Lindelöf och där i synner-
49
het min avdelningskollega tillika medförfattare, Marie Breidenskog, som lärt mig mycket och alltid varit positiv till att inkludera patienter i studierna. …..Christer Janson, medförfattare, för Din generositet att dela med Dig av Din kunskap kring analysmetoder i studie II. Tack också för att Du alltid fanns till hands för frågor och snabbinsatta möten. …..Arne Tenlig, medförfattare, för att Du delat med Dig av Ditt kliniska kunnande kring intensivvårdpatienter och givit kloka synpunkter i studie I. …..arbetsgruppen för de ”Nationella riktlinjerna inom respiration i samband med kirurgi”, LSR, Maria Antonsson, Monika Fagevik-Olsen, Henrik Johansson, Lena Sandström, Malin Wiklund och Elisabeth Westerdahl för mycket intressanta och lärorika diskussioner. …..Institutionen för Neurovetenskap, Sjukgymnastik, under ledning av biträdande prefekt Cathrin Martin, för en mycket bra forskarutbildning. De förutsättningar, den organisation och det arbetsklimat som finns för doktoranderna är fantastiskt. Tack till studierektor Lena Zetterberg, som möjliggjort för mig att förena undervisning, kliniskt arbete och forskning. Tack till alla seniora forskare som delger oss doktorander kunskap och utmanar oss på seminarier.
Tack också alla tidigare och nuvarande kollegor på sjukgymnastpro-grammet Uppsala Universitet, som hela tiden lockar mig tillbaka till det jag älskar, att ta mig an pedagogiska utmaningar. …..Lena Zetterberg och Annika Bring mina kära vänner, kollegor och rumskamrater under delar av forskarutbildningen. Tack för alla utvecklande diskussioner om våra projekt men också kring allt annat i livet. …..doktorandgruppen, Institutionen för Neurovetenskap, Sjukgymnastik, Mikael Andersson, Christina Emilson, Carina Hagman, Sara Holm, Helena Igelström, Henrik Johansson, Åsa Revenäs, Sören Spörndly-Nees, Birgit Vahlberg. Tack för den fantastiska lärmiljö vi tillsammans skapat men energi och drivkraft. Utan er hade det absolut inte varit så roligt att genomföra denna utbildning! …..mina kära vänner Mona-Lisa Kredner, Karin Kraft, Bodil Grantinger och Torborg Hoppe. Tack för ett allt stöd i vardagen och alla springrundor vi avverkat tillsammans. Ni har alltid aktivt lyssnat på vardagens möjligheter och utmaningar. Tack också för alla roliga middagar och fester vi haft tillsammans!
50
…..min kära mamma, Anita som med outtröttliga energi och en enormt positiva syn på livet alltid trott på mig och hejat på då jag ställts inför nya utmaningar. …..min kära pappa, Per, som inte hann vara med på min disputationsdag. Jag vet att Du skulle varit stolt idag. Tillsammans gav ni mig grunden till att alltid göra mitt bästa och tro på mig själv. …..min stora lycka i livet, min man Jocke och våra barn, Carl och Edith. Ni ger mig kärlek, stöttar mig och gör livet roligt att leva. Ni lär mig att fästa blicken på det som är viktigt i livet. Våra projekt drivs iland tack vare vårat teamarbete.
51
References
1. Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Borden WB, et al. Executive Summary: Heart Disease and Stroke Statistics--2013 Update: A Report From the American Heart Association. Circulation. 2013;127(1):143-52. Epub 2013/01/04.
2. Friberg O, Nilsson, J. Årsrapport SWEDEHEART 2011. 2012. 3. Rahmanian PB, Adams DH, Castillo JG, Carpentier A, Filsoufi F. Predicting
hospital mortality and analysis of long-term survival after major noncardiac complications in cardiac surgery patients. Ann Thorac Surg.90(4):1221-9. Epub 2010/09/28.
4. Apostolakis E, Filos KS, Koletsis E, Dougenis D. Lung dysfunction following cardiopulmonary bypass. Journal of cardiac surgery. 2010;25(1):47-55. Epub 2009/06/25.
5. Schuller D, Morrow LE. Pulmonary complications after coronary revascularization. Curr Opin Cardiol. 2000;15(5):309-15. Epub 2000/12/29.
6. Borghi-Silva A, Mendes RG, Costa Fde S, Di Lorenzo VA, Oliveira CR, Luzzi S. The influences of positive end expiratory pressure (PEEP) associated with physiotherapy intervention in phase I cardiac rehabilitation. Clinics (Sao Paulo). 2005;60(6):465-72. Epub 2005/12/17.
7. Renault JA, Costa-Val R, Rosseti MB, Houri Neto M. Comparison between deep breathing exercises and incentive spirometry after CABG surgery. Rev Bras Cir Cardiovasc. 2009;24(2):165-72. Epub 2009/09/22.
8. Matte P, Jacquet L, Van Dyck M, Goenen M. Effects of conventional physiotherapy, continuous positive airway pressure and non-invasive ventilatory support with bilevel positive airway pressure after coronary artery bypass grafting. Acta Anaesthesiol Scand. 2000;44(1):75-81. Epub 2000/02/11.
9. Nicholson DJ, Kowalski SE, Hamilton GA, Meyers MP, Serrette C, Duke PC. Postoperative pulmonary function in coronary artery bypass graft surgery patients undergoing early tracheal extubation: a comparison between short-term mechanical ventilation and early extubation. J Cardiothorac Vasc Anesth. 2002;16(1):27-31. Epub 2002/02/21.
10. Westerdahl E, Lindmark B, Bryngelsson I, Tenling A. Pulmonary function 4 months after coronary artery bypass graft surgery. Respir Med. 2003;97(4):317-22. Epub 2003/04/16.
11. Tenling A, Hachenberg T, Tyden H, Wegenius G, Hedenstierna G. Atelectasis and gas exchange after cardiac surgery. Anesthesiology. 1998;89(2):371-8. Epub 1998/08/26.
12. Westerdahl E, Lindmark B, Eriksson T, Friberg O, Hedenstierna G, Tenling A. Deep-breathing exercises reduce atelectasis and improve pulmonary function after coronary artery bypass surgery. Chest. 2005;128(5):3482-8. Epub 2005/11/24.
52
13. Savci S, Degirmenci B, Saglam M, Arikan H, Inal-Ince D, Turan HN, et al. Short-term effects of inspiratory muscle training in coronary artery bypass graft surgery: a randomized controlled trial. Scand Cardiovasc J. 2011;45(5):286-93. Epub 2011/07/29.
14. Brasher PA, McClelland KH, Denehy L, Story I. Does removal of deep breathing exercises from a physiotherapy program including pre-operative education and early mobilisation after cardiac surgery alter patient outcomes? Aust J Physiother. 2003;49(3):165-73. Epub 2003/09/04.
15. Crowe JM, Bradley CA. The effectiveness of incentive spirometry with physical therapy for high-risk patients after coronary artery bypass surgery. Phys Ther. 1997;77(3):260-8. Epub 1997/03/01.
16. Stiller K, Montarello J, Wallace M, Daff M, Grant R, Jenkins S, et al. Efficacy of breathing and coughing exercises in the prevention of pulmonary complications after coronary artery surgery. Chest. 1994;105(3):741-7. Epub 1994/03/01.
17. Westerdahl E, Lindmark B, Almgren SO, Tenling A. Chest physiotherapy after coronary artery bypass graft surgery--a comparison of three different deep breathing techniques. J Rehabil Med. 2001;33(2):79-84. Epub 2001/07/28.
18. Herdy AH, Marcchi PL, Vila A, Tavares C, Collaco J, Niebauer J, et al. Pre- and postoperative cardiopulmonary rehabilitation in hospitalized patients undergoing coronary artery bypass surgery: a randomized controlled trial. Am J Phys Med Rehabil. 2008;87(9):714-9. Epub 2008/08/22.
19. Westerdahl E, Olsen MF. Chest physiotherapy and breathing exercises for cardiac surgery patients in Sweden--a national survey of practice. Monaldi archives for chest disease = Archivio Monaldi per le malattie del torace / Fondazione clinica del lavoro, IRCCS [and] Istituto di clinica tisiologica e malattie apparato respiratorio, Universita di Napoli, Secondo ateneo. 2011;75(2):112-9. Epub 2011/09/22.
20. Taggart DP, el-Fiky M, Carter R, Bowman A, Wheatley DJ. Respiratory dysfunction after uncomplicated cardiopulmonary bypass. Ann Thorac Surg. 1993;56(5):1123-8. Epub 1993/11/01.
21. Jensen L, Yang L. Risk factors for postoperative pulmonary complications in coronary artery bypass graft surgery patients. Eur J Cardiovasc Nurs. 2007;6(3):241-6. Epub 2007/03/10.
22. Asimakopoulos G, Smith PL, Ratnatunga CP, Taylor KM. Lung injury and acute respiratory distress syndrome after cardiopulmonary bypass. Ann Thorac Surg. 1999;68(3):1107-15. Epub 1999/10/06.
23. Westerdahl E, Lindmark B, Eriksson T, Hedenstierna G, Tenling A. The immediate effects of deep breathing exercises on atelectasis and oxygenation after cardiac surgery. Scand Cardiovasc J. 2003;37(6):363-7. Epub 2003/12/12.
24. Hortal J, Giannella M, Perez MJ, Barrio JM, Desco M, Bouza E, et al. Incidence and risk factors for ventilator-associated pneumonia after major heart surgery. Intensive care medicine. 2009;35(9):1518-25. Epub 2009/06/27.
25. Akdur H, Yigit Z, Sozen AB, Cagatay T, Guven O. Comparison of pre- and postoperative pulmonary function in obese and non-obese female patients undergoing coronary artery bypass graft surgery. Respirology. 2006;11(6):761-6. Epub 2006/10/21.
26. Hulzebos EH, Van Meeteren NL, De Bie RA, Dagnelie PC, Helders PJ. Prediction of postoperative pulmonary complications on the basis of preoperative risk factors in patients who had undergone coronary artery bypass graft surgery. Phys Ther. 2003;83(1):8-16. Epub 2002/12/24.
53
27. Fuster RG, Argudo JA, Albarova OG, Sos FH, Lopez SC, Codoner MB, et al. Prognostic value of chronic obstructive pulmonary disease in coronary artery bypass grafting. Eur J Cardiothorac Surg. 2006;29(2):202-9. Epub 2005/12/27.
28. Manganas H, Lacasse Y, Bourgeois S, Perron J, Dagenais F, Maltais F. Postoperative outcome after coronary artery bypass grafting in chronic obstructive pulmonary disease. Can Respir J. 2007;14(1):19-24. Epub 2007/02/23.
29. Lizak MK, Nash E, Zakliczynski M, Sliwka J, Knapik P, Zembala M. Additional spirometry criteria predict postoperative complications after coronary artery bypass grafting (CABG) independently of concomitant chronic obstructive pulmonary disease: when is off-pump CABG more beneficial? Pol Arch Med Wewn. 2009;119(9):550-7. Epub 2009/09/25.
30. Arabaci U, Akdur H, Yigit Z. Effects of smoking on pulmonary functions and arterial blood gases following coronary artery surgery in Turkish patients. Jpn Heart J. 2003;44(1):61-72. Epub 2003/03/08.
31. Baumgarten MC, Garcia GK, Frantzeski MH, Giacomazzi CM, Lagni VB, Dias AS, et al. Pain and pulmonary function in patients submitted to heart surgery via sternotomy. Rev Bras Cir Cardiovasc. 2009;24(4):497-505. Epub 2010/03/23.
32. Bruells CS, Rossaint R. Physiology of gas exchange during anaesthesia. Eur J Anaesthesiol.28(8):570-9. Epub 2011/06/29.
33. Canbaz S, Turgut N, Halici U, Balci K, Ege T, Duran E. Electrophysiological evaluation of phrenic nerve injury during cardiac surgery--a prospective, controlled, clinical study. BMC Surg. 2004;4:2. Epub 2004/01/16.
34. Massoudy P, Zahler S, Becker BF, Braun SL, Barankay A, Meisner H. Evidence for inflammatory responses of the lungs during coronary artery bypass grafting with cardiopulmonary bypass. Chest. 2001;119(1):31-6. Epub 2001/02/07.
35. Kristjansdottir A, Ragnarsdottir M, Hannesson P, Beck HJ, Torfason B. Respiratory movements are altered three months and one year following cardiac surgery. Scand Cardiovasc J. 2004;38(2):98-103. Epub 2004/06/19.
36. Bonacchi M, Prifti E, Giunti G, Salica A, Frati G, Sani G. Respiratory dysfunction after coronary artery bypass grafting employing bilateral internal mammary arteries: the influence of intact pleura. Eur J Cardiothorac Surg. 2001;19(6):827-33. Epub 2001/06/19.
37. Siafakas NM, Mitrouska I, Bouros D, Georgopoulos D. Surgery and the respiratory muscles. Thorax. 1999;54(5):458-65. Epub 1999/04/22.
38. Wahba RW. Perioperative functional residual capacity. Canadian journal of anaesthesia = Journal canadien d'anesthesie. 1991;38(3):384-400. Epub 1991/04/01.
39. Hedenstierna G. Oxygen and anesthesia: what lung do we deliver to the post-operative ward? Acta Anaesthesiol Scand. 2012;56(6):675-85. Epub 2012/04/05.
40. Milgrom LB, Brooks JA, Qi R, Bunnell K, Wuestfeld S, Beckman D. Pain levels experienced with activities after cardiac surgery. Am J Crit Care. 2004;13(2):116-25. Epub 2004/03/27.
41. Sasseron AB, Figueiredo LC, Trova K, Cardoso AL, Lima NM, Olmos SC, et al. Does the pain disturb the respiratory function after open heart surgery? Rev Bras Cir Cardiovasc. 2009;24(4):490-6. Epub 2010/03/23.
42. Mueller XM, Tinguely F, Tevaearai HT, Revelly JP, Chiolero R, von Segesser LK. Pain location, distribution, and intensity after cardiac surgery. Chest. 2000;118(2):391-6. Epub 2000/08/11.
54
43. Mueller XM, Tinguely F, Tevaearai HT, Ravussin P, Stumpe F, von Segesser LK. Impact of duration of chest tube drainage on pain after cardiac surgery. Eur J Cardiothorac Surg. 2000;18(5):570-4. Epub 2000/10/29.
44. Morsch KT, Leguisamo CP, Camargo MD, Coronel CC, Mattos W, Ortiz LD, et al. Ventilatory profile of patients undergoing CABG surgery. Rev Bras Cir Cardiovasc. 2009;24(2):180-7. Epub 2009/09/22.
45. Shenkman Z, Shir Y, Weiss YG, Bleiberg B, Gross D. The effects of cardiac surgery on early and late pulmonary functions. Acta Anaesthesiol Scand. 1997;41(9):1193-9. Epub 1997/11/21.
46. Hachenberg T, Tenling A, Hansson HE, Tyden H, Hedenstierna G. The ventilation-perfusion relation and gas exchange in mitral valve disease and coronary artery disease. Implications for anesthesia, extracorporeal circulation, and cardiac surgery. Anesthesiology. 1997;86(4):809-17. Epub 1997/04/01.
47. Evans JA, Whitelaw WA. The assessment of maximal respiratory mouth pressures in adults. Respir Care. 2009;54(10):1348-59. Epub 2009/10/03.
48. ATS/ERS Statement on respiratory muscle testing. American journal of respiratory and critical care medicine. 2002;166(4):518-624. Epub 2002/08/21.
49. Rodrigues AJ, Mendes V, Ferreira PE, Xavier MA, Augusto VS, Bassetto S, et al. Preoperative respiratory muscle dysfunction is a predictor of prolonged invasive mechanical ventilation in cardiorespiratory complications after heart valve surgery. Eur J Cardiothorac Surg. 2011;39(5):662-6. Epub 2010/10/05.
50. Ferreira GM, Haeffner MP, Barreto SS, Dall'Ago P. [Incentive spirometry with expiratory positive airway pressure brings benefits after myocardial revascularization]. Arq Bras Cardiol. 2010;94(2):230-5, 46-51, 3-8. Epub 2010/04/30.
51. Westerdahl E, Moller M. Physiotherapy-supervised mobilization and exercise following cardiac surgery: a national questionnaire survey in Sweden. J Cardiothorac Surg.5:67. Epub 2010/08/27.
52. Renault JA, Costa-Val R, Rossetti MB. Respiratory physiotherapy in the pulmonary dysfunction after cardiac surgery. Rev Bras Cir Cardiovasc. 2008;23(4):562-9. Epub 2009/02/21.
53. Freitas ER, Soares BG, Cardoso JR, Atallah AN. Incentive spirometry for preventing pulmonary complications after coronary artery bypass graft. Cochrane Database Syst Rev. 2012;9:CD004466. Epub 2012/09/14.
54. Dias CM, Vieira Rde O, Oliveira JF, Lopes AJ, Menezes SL, Guimaraes FS. Three physiotherapy protocols: effects on pulmonary volumes after cardiac surgery. Jornal brasileiro de pneumologia : publicacao oficial da Sociedade Brasileira de Pneumologia e Tisilogia. 2011;37(1):54-60. Epub 2011/03/11.
55. Ingwersen UM, Larsen KR, Bertelsen MT, Kiil-Nielsen K, Laub M, Sandermann J, et al. Three different mask physiotherapy regimens for prevention of post-operative pulmonary complications after heart and pulmonary surgery. Intensive care medicine. 1993;19(5):294-8. Epub 1993/01/01.
56. Richter Larsen K, Ingwersen U, Thode S, Jakobsen S. Mask physiotherapy in patients after heart surgery: a controlled study. Intensive care medicine. 1995;21(6):469-74. Epub 1995/06/01.
57. Pasquina P, Merlani P, Granier JM, Ricou B. Continuous positive airway pressure versus noninvasive pressure support ventilation to treat atelectasis after cardiac surgery. Anesth Analg. 2004;99(4):1001-8, table of contents. Epub 2004/09/24.
55
58. Romanini W, Muller AP, Carvalho KA, Olandoski M, Faria-Neto JR, Mendes FL, et al. The effects of intermittent positive pressure and incentive spirometry in the postoperative of myocardial revascularization. Arq Bras Cardiol. 2007;89(2):94-9, 105-10. Epub 2007/09/18.
59. Bartlett RH, Gazzaniga AB, Geraghty TR. Respiratory maneuvers to prevent postoperative pulmonary complications. A critical review. JAMA : the journal of the American Medical Association. 1973;224(7):1017-21. Epub 1973/05/14.
60. Garrard CS, Shah M. The effects of expiratory positive airway pressure on functional residual capacity in normal subjects. Crit Care Med. 1978;6(5):320-2. Epub 1978/09/01.
61. Falk M, Kelstrup M, Andersen JB, Kinoshita T, Falk P, Stovring S, et al. Improving the ketchup bottle method with positive expiratory pressure, PEP, in cystic fibrosis. European journal of respiratory diseases. 1984;65(6):423-32. Epub 1984/08/01.
62. Haeffener MP, Ferreira GM, Barreto SS, Arena R, Dall'Ago P. Incentive spirometry with expiratory positive airway pressure reduces pulmonary complications, improves pulmonary function and 6-minute walk distance in patients undergoing coronary artery bypass graft surgery. American heart journal. 2008;156(5):900 e1- e8. Epub 2008/12/09.
63. Stein R, Maia CP, Silveira AD, Chiappa GR, Myers J, Ribeiro JP. Inspiratory muscle strength as a determinant of functional capacity early after coronary artery bypass graft surgery. Archives of physical medicine and rehabilitation. 2009;90(10):1685-91. Epub 2009/10/06.
64. Jenkins S, Soutar S, Loukota J, LC J, Moxham J. A comparison of breathing exercises, incentive spirometry and mobilisation after coronary artery surgery. Physiotherapy theory and practice. 1990;6:117-26.
65. Savci S, Sakinc S, Inal Ince D, Arikan H, Can Z, Buran Y, et al. Active cycle of breating techniques and incentive spirometer in coronary artery bypass graft surgery. Fizioterapi Rehabilitasyon. 2006;17(2):61-9.
66. Dull JL, Dull WL. Are maximal inspiratory breathing exercises or incentive spirometry better than early mobilization after cardiopulmonary bypass? Phys Ther. 1983;63(5):655-9. Epub 1983/05/01.
67. Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, et al. Standardisation of spirometry. The European respiratory journal : official journal of the European Society for Clinical Respiratory Physiology. 2005;26(2):319-38. Epub 2005/08/02.
68. Wanger J, Clausen JL, Coates A, Pedersen OF, Brusasco V, Burgos F, et al. Standardisation of the measurement of lung volumes. The European respiratory journal : official journal of the European Society for Clinical Respiratory Physiology. 2005;26(3):511-22. Epub 2005/09/02.
69. Hedenstrom H, Malmberg P, Agarwal K. Reference values for lung function tests in females. Regression equations with smoking variables. Bull Eur Physiopathol Respir. 1985;21(6):551-7. Epub 1985/11/01.
70. Hedenstrom H, Malmberg P, Fridriksson HV. Reference values for lung function tests in men: regression equations with smoking variables. Ups J Med Sci. 1986;91(3):299-310. Epub 1986/01/01.
71. Williamson A, Hoggart B. Pain: a review of three commonly used pain rating scales. J Clin Nurs. 2005;14(7):798-804. Epub 2005/07/08.
72. Turk D MR. Hand-book of Pain Assessment. New York and London: Guilford; 1992.
56
73. Myles PS, Hunt, J.O, Fletcher, H, Solly, R, Woodward, D, Kelly, S. Relation between quality of recovery in hospital and quality of life at 3 months after cardiac surgery. Anesthesiology. 2001;95:862-7.
74. Myles PS, Weitkamp B, Jones K, Melick J, Hensen S. Validity and reliability of a postoperative quality of recovery score: the QoR-40. Br J Anaesth. 2000;84(1):11-5. Epub 2000/03/31.
75. Sullivan M, Karlsson J, Ware JE, Jr. The Swedish SF-36 Health Survey--I. Evaluation of data quality, scaling assumptions, reliability and construct validity across general populations in Sweden. Soc Sci Med. 1995;41(10):1349-58. Epub 1995/11/01.
76. Persson LO, Karlsson J, Bengtsson C, Steen B, Sullivan M. The Swedish SF-36 Health Survey II. Evaluation of clinical validity: results from population studies of elderly and women in Gothenborg. Journal of clinical epidemiology. 1998;51(11):1095-103. Epub 1998/11/17.
77. Sullivan M, Karlsson J. The Swedish SF-36 Health Survey III. Evaluation of criterion-based validity: results from normative population. Journal of clinical epidemiology. 1998;51(11):1105-13. Epub 1998/11/17.
78. Schlenk EA, Erlen JA, Dunbar-Jacob J, McDowell J, Engberg S, Sereika SM, et al. Health-related quality of life in chronic disorders: a comparison across studies using the MOS SF-36. Quality of life research : an international journal of quality of life aspects of treatment, care and rehabilitation. 1998;7(1):57-65. Epub 1998/03/03.
79. Failde I, Ramos I. Validity and reliability of the SF-36 Health Survey Questionnaire in patients with coronary artery disease. Journal of clinical epidemiology. 2000;53(4):359-65. Epub 2000/04/29.
80. Fagevik Olsén Monika LL, Lind Broberg Jenny, westerdahl Elisabeth. Measuring chest expansion; A study comparing two different instructions. Advances of Pysical Therapy. 2011;13:128-32.
81. Bockenhauer SE, Chen H, Julliard KN, Weedon J. Measuring thoracic excursion: reliability of the cloth tape measure technique. The Journal of the American Osteopathic Association. 2007;107(5):191-6. Epub 2007/06/29.
82. Orman J, Westerdahl E. Chest physiotherapy with positive expiratory pressure breathing after abdominal and thoracic surgery: a systematic review. Acta Anaesthesiol Scand. 2010;54(3):261-7. Epub 2009/11/03.
83. Rothen HU, Neumann P, Berglund JE, Valtysson J, Magnusson A, Hedenstierna G. Dynamics of re-expansion of atelectasis during general anaesthesia. Br J Anaesth. 1999;82(4):551-6. Epub 1999/09/03.
84. Hirschhorn AD, Richards D, Mungovan SF, Morris NR, Adams L. Supervised moderate intensity exercise improves distance walked at hospital discharge following coronary artery bypass graft surgery--a randomised controlled trial. Heart Lung Circ. 2008;17(2):129-38. Epub 2007/12/07.
85. Grady KL, Lee R, Subacius H, Malaisrie SC, McGee EC, Jr., Kruse J, et al. Improvements in health-related quality of life before and after isolated cardiac operations. Ann Thorac Surg. 2011;91(3):777-83. Epub 2011/03/01.
86. Garrod R, Ford K, Daly C, Hoareau C, Howard M, Simmonds C. Pulmonary rehabilitation: analysis of a clinical service. Physiotherapy research international : the journal for researchers and clinicians in physical therapy. 2004;9(3):111-20. Epub 2004/11/25.
57
87. Guiraud T, Granger R, Gremeaux V, Bousquet M, Richard L, Soukarie L, et al. Telephone support oriented by accelerometric measurements enhances adherence to physical activity recommendations in noncompliant patients after a cardiac rehabilitation program. Archives of physical medicine and rehabilitation. 2012;93(12):2141-7. Epub 2012/07/21.
88. Angouras DC, Anagnostopoulos CE, Chamogeorgakis TP, Rokkas CK, Swistel DG, Connery CP, et al. Postoperative and long-term outcome of patients with chronic obstructive pulmonary disease undergoing coronary artery bypass grafting. Ann Thorac Surg.89(4):1112-8. Epub 2010/03/27.
89. Neder JA, Andreoni S, Lerario MC, Nery LE. Reference values for lung function tests. II. Maximal respiratory pressures and voluntary ventilation. Brazilian journal of medical and biological research = Revista brasileira de pesquisas medicas e biologicas / Sociedade Brasileira de Biofisica [et al]. 1999;32(6):719-27. Epub 1999/07/21.
90. Bellinetti LM, Thomson JC. Respiratory muscle evaluation in elective thoracotomies and laparotomies of the upper abdomen. Jornal brasileiro de pneumologia : publicacao oficial da Sociedade Brasileira de Pneumologia e Tisilogia. 2006;32(2):99-105. Epub 2007/02/03.
91. Ferreira PE, Rodrigues AJ, Evora PR. Effects of an inspiratory muscle rehabilitation program in the postoperative period of cardiac surgery. Arq Bras Cardiol. 2009;92(4):275-82. Epub 2009/07/01.
92. Hulzebos EH, Helders PJ, Favie NJ, De Bie RA, Brutel de la Riviere A, Van Meeteren NL. Preoperative intensive inspiratory muscle training to prevent postoperative pulmonary complications in high-risk patients undergoing CABG surgery: a randomized clinical trial. JAMA : the journal of the American Medical Association. 2006;296(15):1851-7. Epub 2006/10/19.
93. Weiner P, Zeidan F, Zamir D, Pelled B, Waizman J, Beckerman M, et al. Prophylactic inspiratory muscle training in patients undergoing coronary artery bypass graft. World journal of surgery. 1998;22(5):427-31. Epub 1998/05/02.
94. Riedi C, Mora CT, Driessen T, Coutinho Mde C, Mayer DM, Moro FL, et al. Relation between respiratory muscle strength with respiratory complication on the heart surgery. Rev Bras Cir Cardiovasc. 2010;25(4):500-5. Epub 2011/02/23.
95. Freitas FS, Ibiapina CC, Alvim CG, Britto RR, Parreira VF. Relationship between cough strength and functional level in elderly. Rev Bras Fisioter. 2010;14(6):470-6. Epub 2011/02/23.
96. Sachs MC, Enright PL, Hinckley Stukovsky KD, Jiang R, Barr RG. Performance of maximum inspiratory pressure tests and maximum inspiratory pressure reference equations for 4 race/ethnic groups. Respir Care. 2009;54(10):1321-8. Epub 2009/10/03.
97. Chetta A, Bobbio A, Aiello M, Del Donno M, Castagnaro A, Comel A, et al. Changes in lung function and respiratory muscle strength after sternotomy vs. laparotomy in patients without ventilatory limitation. European surgical research Europaische chirurgische Forschung Recherches chirurgicales europeennes. 2006;38(5):489-93. Epub 2006/09/30.
98. Barros GF, Santos Cda S, Granado FB, Costa PT, Limaco RP, Gardenghi G. Respiratory muscle training in patients submitted to coronary arterial bypass graft. Rev Bras Cir Cardiovasc. 2010;25(4):483-90. Epub 2011/02/23.
99. Hess D. Noninvasive respiratory monitoring during ventilatory support. Critical care nursing clinics of North America. 1991;3(4):565-74. Epub 1991/12/01.
58
100. Jensen LA, Onyskiw JE, Prasad NG. Meta-analysis of arterial oxygen saturation monitoring by pulse oximetry in adults. Heart Lung. 1998;27(6):387-408. Epub 1998/12/04.
101. Hautmann H, Hefele S, Schotten K, Huber RM. Maximal inspiratory mouth pressures (PIMAX) in healthy subjects--what is the lower limit of normal? Respir Med. 2000;94(7):689-93. Epub 2000/08/05.
102. Vincken W, Ghezzo H, Cosio MG. Maximal static respiratory pressures in adults: normal values and their relationship to determinants of respiratory function. Bull Eur Physiopathol Respir. 1987;23(5):435-9. Epub 1987/09/01.
103. Windisch W, Hennings E, Sorichter S, Hamm H, Criee CP. Peak or plateau maximal inspiratory mouth pressure: which is best? The European respiratory journal : official journal of the European Society for Clinical Respiratory Physiology. 2004;23(5):708-13. Epub 2004/06/05.
104. Chulay M, Brown J, Summer W. Effect of postoperative immobilization after coronary artery bypass surgery. Crit Care Med. 1982;10(3):176-9. Epub 1982/03/01.
105. Kehlet H, Dahl JB. Anaesthesia, surgery, and challenges in postoperative recovery. Lancet. 2003;362(9399):1921-8. Epub 2003/12/12.


Acta Universitatis UpsaliensisDigital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 857
Editor: The Dean of the Faculty of Medicine
A doctoral dissertation from the Faculty of Medicine, UppsalaUniversity, is usually a summary of a number of papers. A fewcopies of the complete dissertation are kept at major Swedishresearch libraries, while the summary alone is distributedinternationally through the series Digital ComprehensiveSummaries of Uppsala Dissertations from the Faculty ofMedicine.
Distribution: publications.uu.seurn:nbn:se:uu:diva-192208
ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2013