lower gastrointestinal bleeding endovascular treatment claudio rabbia
TRANSCRIPT

LOWER GASTROINTESTINAL BLEEDING
Endovascular treatment
Claudio Rabbia

Endovascular treatment
• Vasopressin infusion
• Selective embolization

Colonic embolization for LGI bleeding was attempt as early as the 1970s by Rosch and Brookstein
The catheters and the embolic materials available then were primitive, and initial efforts led to unacceptably high rates of ischemia and infarction ranging from 13% to 33%
Throughout the 1980s, colonic embolization was generally abandoned in favor of vasopressin infusion
The high rates of infarction in these early series were probably due to the relatively larger catheters (5 - 6.5F) used and more limited embolic agents (autologous clot and gelatine sponge)
Rosch I, Dotter CT, Antonovic R. Selective vasoconstrictor infusion in the management of arteriocapillary gastrointestinal hemorrhage, AJR Radium Ther Nucl Med 1972
The history

Vasopressin infusion has important limitations including a failure rate greater than 20% and a rebleeding rate greater than 15%.
It’s very labor intensive and time consuming due to management of an indwelling arterial catheter.
Dissatisfaction with catheter directed vasocostriction led to renewed interest in embolization in the late 1980s and early 1990s when coaxial microcatheter become available.
These catheters typically range in size from 2.5 to 3 F in diameter and can be advanced through a 5 F catheter
The history

LGI bleedingvasopressin versus embolization
• In the 70’ and 80’ vasopressin was the recommended therapy for LGI bleeding and embolotherapy was promoted for UGI bleeding.
• Since the 90’ there is a less clear anatomic delineation of where to apply these treatments

The catheter just needs to be placed selectively into the main trunk of SMA or IMA
The devices are less complex than those for embolization: a single 5 F catheter is all the equipment required
Rarely, vasopressin infusion into a single vessel may fail to terminate bleeding if the lesion is near a junction of 2 arterial distributions, such as the splenic junction.
In these cases, 2 catheters may be required to simultaneously infuse into SMA and IMA
Vasopressin infusion
Vasopressin infusionfirst step
Typical vasopressin therapy involves an initial 20-minute infusion at a rate of 0.2U/min followed by repeated arteriography to determine that bleeding has stopped and that the artery is not overconstricted
If bleeding continues, the infusion may increase to 0.3 U/min and than 0.4U/min followed by a waiting period for the increased drug dose to take effect and than another arteriogram to assess the effect
THEREFORE, INTRAPROCEDURAL TIME MAY BE SIMILAR TO THAT FOR EMBOLIZATION

Vasopressin infusionsecond step
Diverticularbleeding
After 24 hoursof vasopressin
infusion 0.1 U/min
Vasopressin therapy requires a longer committment of catheter management. When the proper dose is determined, the vasopressin is infused at that rate for 6-12 hours.
The dose is than reduced by half and the infusion is continued for another 12-24 hours.
The catheter is than removed if there are no clinical signs of bleeding but, at this time, the catheter has been in place for 1-2 days.
Prolonged catheterization may also increase the risk of groin complication like hematoma or thrombosis

Vasopressin infusiongeneral limitations
ability to catheterize the main SMA and IMA trunk
coagulopathy
atherosclerosis: atherosclerotic arteries do not constrict in response to vasopressin despite successful catheterization

Vasopressin infusionsuccess rate
Vasopressin therapy is a particularly effective therapy when applied to LGI hemorrhage
General series of LGI bleeding with mixed locations (small bowel and colon) and varied etiologies report success rates ranging from 59% and 90%
One study who segregated small bowel from colonic sources found a slightly better response in the colon at 83%, vs 71% in the small bowel
Pennoyer WP. Management of angiogram positive lower gastrointestinal hemorrhage: long term follow-up of non-operative treatments. Int J Colorectal Dis 1996
Vasopressin infusioncomplications
Vasopressin infusion is associated with major complications in 0-21% of cases and, in many as 9%, the results were fatal
Minor complications are more common with reported frequency ranging from 10 to 41%
puncture site complications: hematoma (7%) thrombosis pseudoaneurysm spasm catheter sepsis
complications at the infusion catheter: thrombosis dissection
Eckstein MRGastric bleeding: therapy with intraarterial vasopressin and transcatheter embolization, Radiology 1984

sistemic effect (21%): arrhythmias hypotension angina cardiac arrest spontaneous bacterial peritonitis
intestinal infarction: thrombosis end organ ischemia (overconstriction)
Eckstein MR Gastric bleeding: therapy with intraarterial vasopressin and transcatheter embolization. Radiology 1984
Vasopressin infusioncomplications

EmbolizationA conventional 5 F catheter may be used to select a first-order vessel (SMA or IMA)
A microcatheter can be advanced through this catheter to more distal, smaller vessels
In the mesenteric circulation, the marginal artery or vasa recta can be selectively catheterized very close to the site of bleeding. This has been termed SUPERSELECTIVE CATHETERIZATION
Once the bleeding vessel has been superselectively catheterized, embolic material can be deployed to arrest hemorrhage.
Superselective embolization limits the segment of bowel at risk for ischemia or most often obviate the risk altogether

EmbolizationChoice of embolic material
spongostanspongostanautologous clotautologous clot
absolute absolute alcohol alcohol
Montoya 2004Montoya 2004
cyanoacrylate cyanoacrylate Cantasdemir Cantasdemir
20032003
detachable balloons
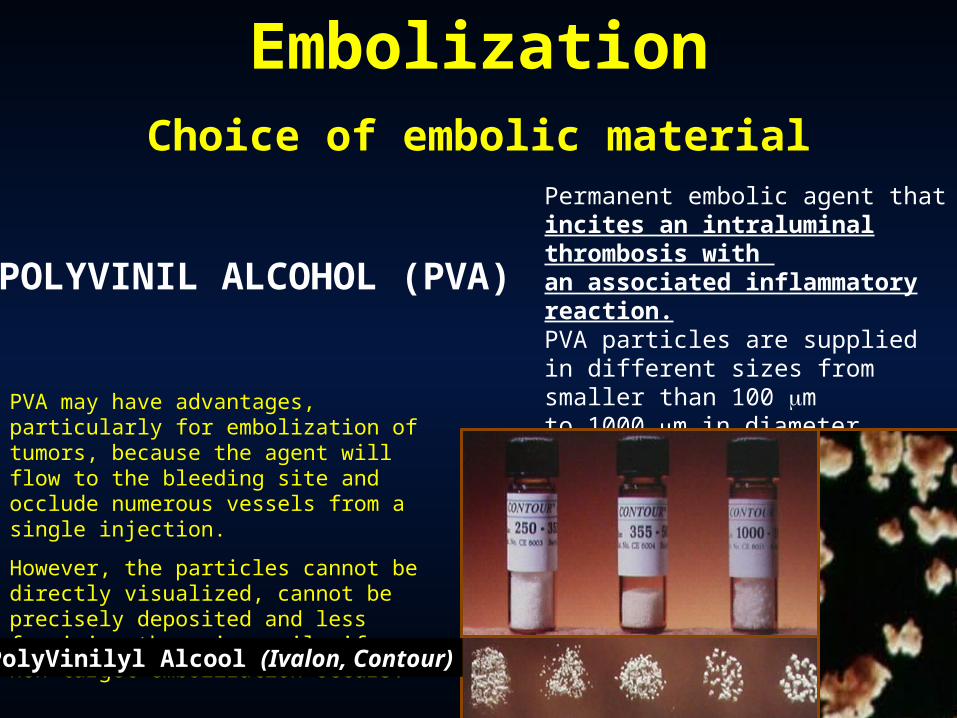
POLYVINIL ALCOHOL (PVA)
Permanent embolic agent that incites an intraluminal thrombosis with an associated inflammatory reaction.PVA particles are supplied in different sizes from smaller than 100 mto 1000 m in diameter
PVA may have advantages, particularly for embolization of tumors, because the agent will flow to the bleeding site and occlude numerous vessels from a single injection.
However, the particles cannot be directly visualized, cannot be precisely deposited and less forgiving than microcoils if non-target embolization occurs.
PolyVinilyl Alcool (Ivalon, Contour)
EmbolizationChoice of embolic material

EmbolizationChoice of embolic material
embospheres

MICROCOILSMade of platinum or stainless steel, when deployed function in a similar manner to a surgical ligation. They are biocompatible but high thrombogenic due to addiction of sinthetic fibers attached to the coil.
Kessaris 1995 Martin 2000
Treiber 2003 Vignali 2004
spirali
EmbolizationChoice of embolic material
EmbolizatioEmbolization n
with coilswith coils
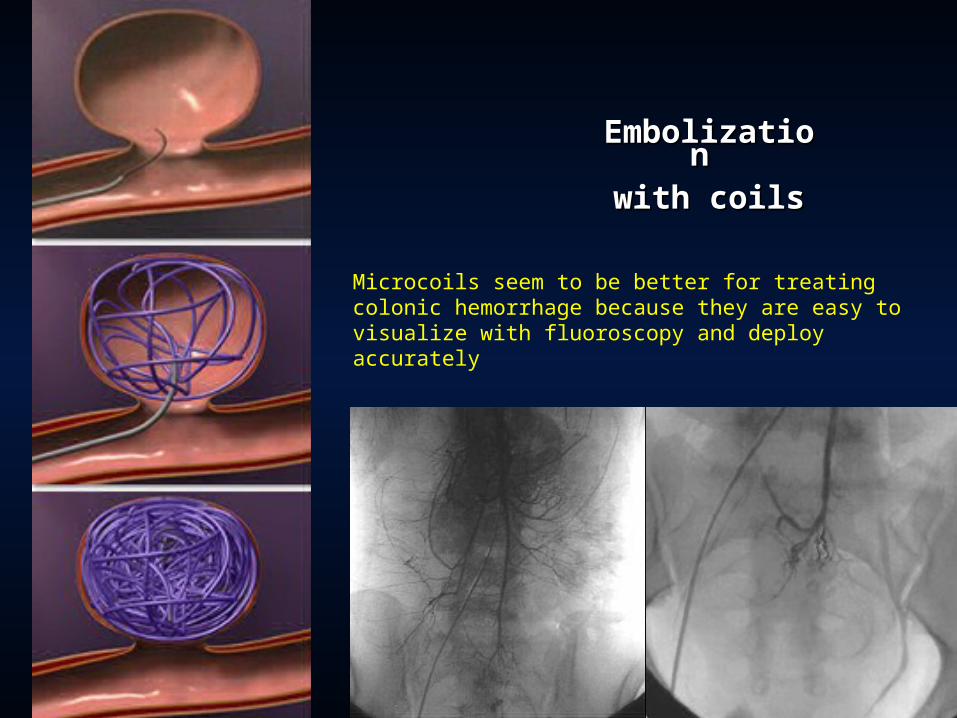
Microcoils seem to be better for treating colonic hemorrhage because they are easy to visualize with fluoroscopy and deploy accurately
Embolization decrease perfusion pressure enough to arrest hemorrhage but notto the extent of total devascularization.
Due to the limited collateral blood flow in the colon, overly aggressive embolization must be avoided.
The mechanism of embolization depends on the embolic agent used.
Microcoils decrease perfusion pressure and induce local vasospasm.This enables the patient to more effectively form clot, leading to hemostasis.
Superselective embolization limits the segment of bowel at risk for ischemia.
Mechanism of embolization
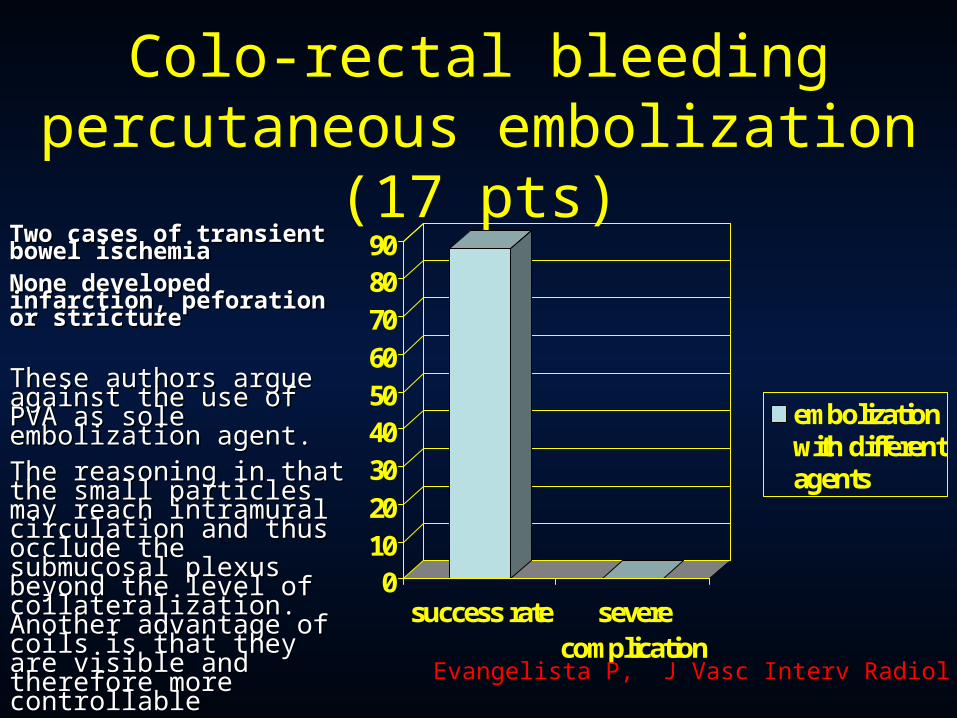
Colo-rectal bleedingpercutaneous embolization (17 pts)
0102030405060708090
success rate severecomplication
embolizationwith differentagents
Two cases of transient Two cases of transient bowel ischemiabowel ischemiaNone developed None developed infarction, peforation or infarction, peforation or stricturestricture
These authors argue against the These authors argue against the use of PVA as sole use of PVA as sole embolization agent. embolization agent.
The reasoning in that the small The reasoning in that the small particles may reach intramural particles may reach intramural circulation and thus occlude the circulation and thus occlude the submucosal plexus beyond the submucosal plexus beyond the level of collateralization. level of collateralization. Another advantage of coils is Another advantage of coils is that they are visible and that they are visible and therefore more controllabletherefore more controllable
Evangelista P, J Vasc Interv Radiol 2000Evangelista P, J Vasc Interv Radiol 2000
Limitations of embolization
Different disorders will vary in responsiveness to embolization.Angiodysplasia is more difficult to treat with embolization.
The most important limitations of endovascular therapy is the inability to diagnoseand treat patients who are not actively bleeding.
Embolization is morely treating a symptom of the underlying disorder than thedisease itself. Patients with multifocal disease are at risk for repeatedhemorrhage from other affected sites (11% and 19% in old and more recent series, respectively)
Other limitations include the inability to perform superselective catheterization in patients with difficult vascular anatomy or severe atherosclerotic disease

Technical versus clinical success of embolization
Technical success
• Successful delivery of embolizing agent
• Absence of extravasation at completion angiography
Clinical success
• Termination of bloody output from the bowel
• Stabilization of hematocrit level
• Lack of further transfusions
Clinical success rates are often slightly lower than technical success rates because bleeding can continue despite successful placement of emboli.
This may be caused by collateral perfusion around the emboli or coagulopathy that prevents formation of thombus despite blockade of arterial flow.

Complications of embolization

Complications of embolizationIn the colon, it’s probably best to place coils as far peripherally as possible
The small intestine has a different vascular pattern with a more extensive collateral arcade in the bowel wall. This make the small bowel more resistant to infarction.
The embolic material used can also affect the risk of infarction.Small embolic particles that occlude the arteries very peripherally (at the arteriolar level or beyond) increase the chance of infarction.For these reason microcoils and larger PVA particles are most commonly used.
Overall (major and minor) intestinal ischemic complication rates in the modern series range from 0% to 70% (average 15%) with majority being minor complication, most of these not requiring any therapy
Funaki B, Kostelic JK, Lorenz I et Al. Superselective microcoil embolization of colonic hemorrhage. AJR 2001
Vasopressin versus embolization
• Most of literature on both consists of very small restrospective series with little or no control for anatomic location, lesion pathology or patient demographics and clinical characteristics
• Most of vasopressin literature is older ( no combination with nitroglycerin to reduce complications)
• Single institutional series or controlled trials comparing these therapies are nearly nonexistent
Vasopressin versus embolization
• Embolization has become a relatively safe option for treating LGI hemorrhage
• Despite more technically challenging, it has advantage of quicker completion of therapy, decreased recurrence of bleeding and some decreased complications
• Choice of therapy is institution-dependent, but where the expertise on both modalities exists, embolization is preferable

conclusions• Endovascular treatment plays a definite role in
controlling LGI bleeding• Vasopressin infusion seems to provoke higher
rate of severe complications• Embolotherapy with superselective
catheterization is currently the best endovascular modality of treatment
• Operator skill is mandatory