long-acting risperidone injection: efficacy, safety, … · 109 articole originale long-acting...
TRANSCRIPT
109
ARTICOLE ORIGINALE
LONG-ACTING RISPERIDONE INJECTION: EFFICACY, SAFETY, AND COST-EFFECTIVENESS OFTHE FIRST LONG-ACTING ATYPICAL ANTIPSYCHOTIC
Pierre Chue*
INTRODUCTION
The long-acting injectable antipsychotics weredeveloped in the 1960s as an additional method of drugdelivery aimed specifically at improving treatmentcompliance in patients with schizophrenia, as well assimplifying the medication process. Long-acting
antipsychotics are convenient for the patients and theirfamilies, in that patients no longer have the burden ofremembering to take daily medication, and families nolonger have to regularly monitor and remind theirfamily member about their medication. Moreover,from the clinician’s point of view, a critical advan-
* Department of Psychiatry University of Alberta, Edmonton, Alberta, Canada
Rezumat:Obiectiv: trecerea în revistã a farmacocineticii,
eficacitãþii, siguranþei ºi cost-eficienþei risperidonei cuacþiune prelungitã.
Metode: A fost efectuatã o cerectare a bazelorMedline ºi EMBAS ºi evaluate studiile publicate întreIanuarie 2000 ºi Octombrie 2006 care au cercetat far-macocinetica, eficacitatea, sigurtanþa ºi costeficienþarisperidonei cu acþiune prelungitã. Au fost evaluate ºirezumatele ºi posterele prezentate în cadrul congreselorpsihiatrice importante ºi aflate în domeniul public.
Rezultate: Profilul farmacocinetic unic al risperi-donei cu acþiune prelungitã derivã din incapsularearisperidonei într-o matrice glicolid/lactidicã subformã de microsfere astefel încât, dupã o singurãinjecþie intramuscularã, se ating niveluri plasmaticesemnificative dupã a treia sãptãmâna. Nivelul deechilibru, în condiþii de administrare repetatã la 2 sãp-tãmâni, este atins dupã 3 cicluri de injectare. Studiilepe termen scurt ºi lung au demonstrat cã risperidonacu acþiune prelungitã (25, 37.5, or 50 mg) este eficien-tã ºi bine toleratã de catre o mare varietate de pacienþicu schizofrenie ºi alte tulburãri psihotice. Majoritateapacienþilor suportã trecerea de la alte antipsihoticeorale ºi depot fãrã a se face un compromis la adresaeficacitãþii ºi siguranþei. Risperidona cu acþiune pre-lungitã ar putea reduce costurile generale datorateîngrijirilor medicale prin scãderea ratelor recãderilorºi spitalizãrilor.
Concluzie: Administrarea sigurã a unui antipsi-hotic atipic conþinând risperidonã cu acþiune prelun-gitã prezintã implicaþii importante pentru complianþapacienþilor, menþinerea stabilitãþii ºi regularitãþii tra -ta mentului ºi îmbunatãþirii rezultatelor, inclusiv atin-gerea remisiunii
Cuvinte cheie: risperidonã cu acþiune prelungitã,eficacitate, siguranþã, farmacocineticã, farma-coeconoomie, schizofrenie.
Abstract:Objective: To review the pharmacokinetics, effi-
cacy, safety, and cost-effectiveness of long- actingrisperidone.
Methods: Studies published between January2000 and October 2006 evaluating the pharmacoki-netics, efficacy, safety, and cost-effectiveness of long-acting risperidone were reviewed, as identified from lit-erature searches using Medline and EMBASE. Abstractsand posters on long-acting risperidone presented at keypsychiatry congresses and available in the publicdomain during this time period were also reviewed.
Results: The unique pharmacokinetic profile oflong-acting risperidone is derived from the encapsula-tion of risperidone in a glycolide/lactide matrix in theform of microspheres such that after a single intra-muscular injection, significant plasma levels of thedrug are achieved after week 3. Steady state, afterrepeated administration at 2-week intervals, isachieved after 3 injection cycles. Short- and long-termstudies have demonstrated that long-acting risperi-done (25, 37.5, or 50 mg) is both efficacious and welltolerated in a wide variety of patients with schizophre-nia and related psychoses. Most patients can beswitched from other oral and long- acting antipsychot-ic agents without compromising efficacy and safety.Long-acting risperidone may also reduce overallhealthcare costs by decreasing rates of relapse andhospitalization. Conclusion: The assured delivery ofan atypical antipsychotic medication with long-actingrisperidone has important implications for patientcompliance, main tenance of stability, consistency oftreatment, and improving patient outcomes includ-ing the achievement of remission.
Keywords: long-acting injectable risperidone, effi-cacy, safety, pharmacokinetics, pharmacoeconomics,schizophrenia.

Pierre Chue: Long-acting risperidone injection
110
tage of long-acting antipsychotics is that if a patientdoes become non-compliant, the clinical team willknow immediately (because an injection has beenmissed) and will be able to initiate efforts to deal effec-tively with the problem before symptoms reappear(Valenstein et al 2001). Long-acting injectable antipsy-chotics are not associated with “first-pass metabolism”and can be adjusted more reliably to the lowest effec-tive dose, thereby further reducing the risk of adverseeffects (Ereshefsky et al 1984; Ereshefsky andMascarenas 2003). A less well recognized benefit oflong-acting therapy is the regular contact betweenpatients and treatment teams, which provides theopportunity for greater therapeutic alliance and psy-chosocial interventions.
Consistent with this, data from a number of indi-vidual trials and meta-analyses have shown that,compared with oral antipsychotics, long-actingantipsychotics reduce relapse frequency and rehospi-talization rates (Davis et al 1994; Gerlach 1994) andlower annual treatment costs (Glazer and Ereshefsky1996). However, despite the attractiveness of this treat-ment option, the use of long-acting antipsychotics hasfallen in recent years particularly in North America,likely as the result of the introduction and widespreaduse of the oral atypical antipsychotics. The develop-ment of the atypical antipsychotic agents over the lastdecade was a major step forward in the pharmaco-logical management of schizophrenia, with numerousstudies demonstrating that atypical agents improvenegative symptoms (Lindenmayer et al 1994;Marder and Meibach 1994; Boyer et al 1995; Beasleyet al 1996) and cognitive function (Meyer-Lindenberget al 1997; Keefe et al 1999; Bilder et al 2002; Barkicet al 2003) and exert a beneficial effect on affectivesymptoms (Tollefson et al 1998; Peuskens et al 2000,2002; Buckley 2004). In addition, the atypical agentshave also been shown to enhance quality of life,functional status, and patient satisfaction comparedwith conventional antipsychotics (Meltzer 1990; Franzet al 1997; Revicki et al 1999; Colonna et al 2000;Hamilton et al 2000). This is of particular relevancesince patient satisfaction has been recognized as animportant determinant of treatment success (Kane2001; Lambert and Naber 2004). Furthermore, a num-ber of meta-analyses have demonstrated that, com-pared with conventional agents, the use of atypicalantipsychotics is associated with a lower incidence ofextrapyramidal side effects (EPS) (Leucht et al 1999;Geddes et al 2000; Bagnall et al 2003). However,despite their identified benefits, the issue of non- andpartial compliance with therapy has not been fullyresolved with the newer atypical agents. More than35% of patients begin to demonstrate complianceproblems during their first 4–6 weeks of treatment andby 2 years, 75% are partially compliant (Weiden andZygmunt 1997). Moreover, results from a study byDolder et al, which compared compliance rates with
oral atypical vs oral conventional antipsychotics,reported similar, low levels of compliance in bothgroups after 12 months (54.9±26.0% vs 50.1±30.6%;p=0.11) (Dolder et al 2002).
It is only recently, with the introduction of long-acting risperidone launched in North America in2004, that clinicians have had access to a long-act-ing atypical antipsychotic. Since an earlier studyreported that psychiatrists would be persuaded to usethese agents if any atypical long-acting antipsychoticswere available (Patel et al 2003), the introduction oflong-acting risperidone raises new questions regardingthe treatment of patients with schizophrenia. Theaim of this review is to provide an evaluation of thepharmacokinetics, efficacy, safety and cost- effective-ness of long-acting risperidone for the treatment ofschizophrenia and schizoaffective disorder.
METHODS
A literature search was performed in two parts.Firstly, an electronic search of English language arti-cles published between January 2000 and October2006 that evaluated the pharmacokinetics, efficacy,safety, and cost-effectiveness of long-acting risperi-done for the treatment of schizophrenia and schizoaf-fective disorder was performed using Medline andEMBASE. The primary search parameters were “long-acting injectable risperidone”, “schizophrenia”,“schizoaffective disorder”, “efficacy”, “tolerability”,“safety”, “quality of life”, “patient satisfaction”, “phar-macokinetics”, cost-effectiveness”, and “phar maco -economic”. Original research articles, reviews, andother articles of interest were reviewed. Secondly,abstracts and posters on long-acting risperidone pre-sented at key psychiatry and schizophrenia congressesduring this period were also reviewed, where availablein the public domain.
RESULTS
Overview of pharmacokinetic properties
TechnologyLong-acting risperidone is synthesized by a
microsphere encapsulation process using static flowmethods to incorporate risperidone inside a glycol-ide/lactide matrix, a commonly used medical poly-mer. In vitro studies have demonstrated that a smallamount of risperidone at the surface of the micros-pheres is released by diffusion within 24 hours. Thisis followed by a latent period of approximately 3weeks, while the majority of the release occurs by ero-sion of the glycolic acid-lacate polymer during weeks4–6 (Ramstack et al 2003). Following administration,the copolymer gradually breaks down in the body,steadily releasing risperidone at a constant rate(Ramstack et al 2003; Eerdekens et al 2004). The finalend products of long-acting risperidone are risperidoneand naturally occurring glycolic and lactic acids, which
Revista Românã de Psihiatrie, seria a III-a, vol. IX, nr. 2-3, 2007
111
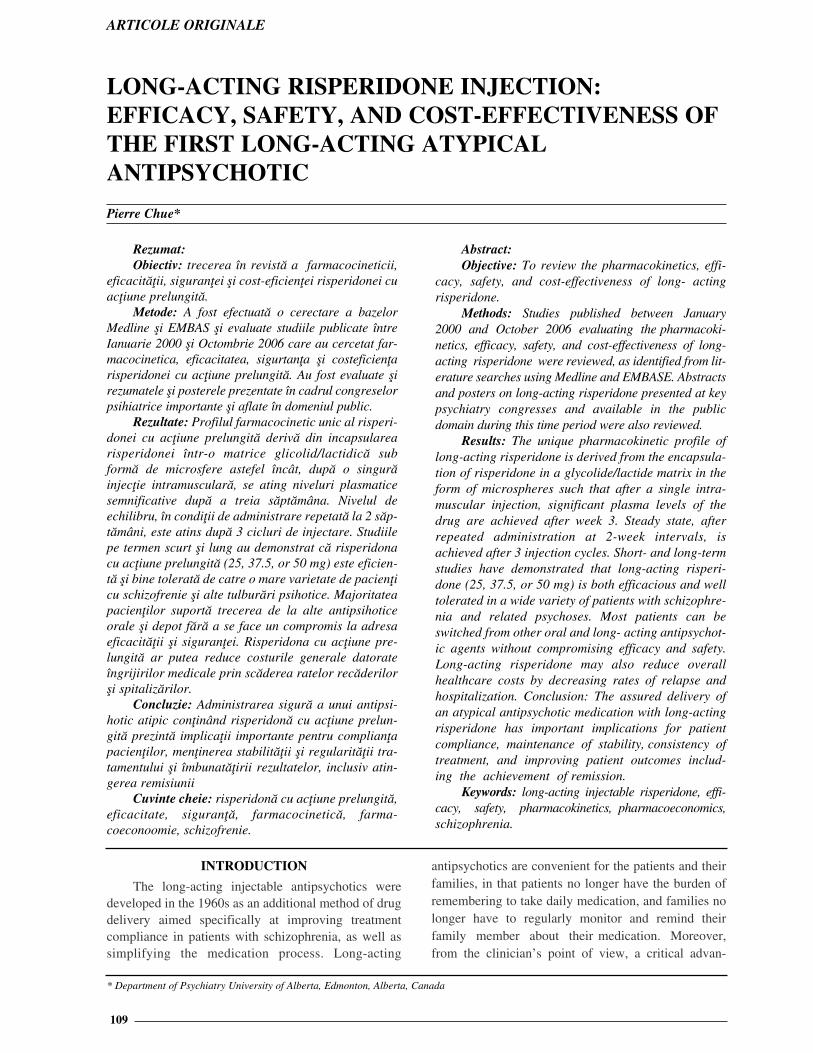
are further metabolized to carbon dioxide and water(Nordstrom et al 1993). It is theorized that the sus-tained release of risperidone from the microspheresresults in consistent and continuous antipsychoticcoverage by reduction of the peaks and troughsobserved with oral medication (Eerdekens et al 2004).The erosion of the microsphere with subsequent disper-sion of risperidone is illustrated in Figure 1.
Figure 1. The dispersion of risperidone from micros-pheres. Reproduced with permission of Wolters Kluwer
Health from Ereshefsky L, Mannaert E. 2005.Pharmacokinetic profile and clinical efficacy of long-acting
risperidone: potential benefits of combining an atypicalantipsychotic and a new delivery system. Drugs R D,
6:129–37. Figure 1 from page 131.
Pharmacokinetic profile
The release profile of risperidone microspheres invitro has been confirmed in a number of clinical stud-ies. Risperidone is metabolized principally by thecytochrome P450 2D6 (CYP) enzyme to the activemetabolite 9-OH-risperidone with the sum of the twobeing frequently modeled for pharmacokinetic pur-poses and labelled the “active moiety”. The results ofpharmacokinetic dose trials support the administra-tion of long-acting risperidone every 2 weeks to main-tain plasma levels of active moiety comparable to lev-els obtained with repeated oral dosing.
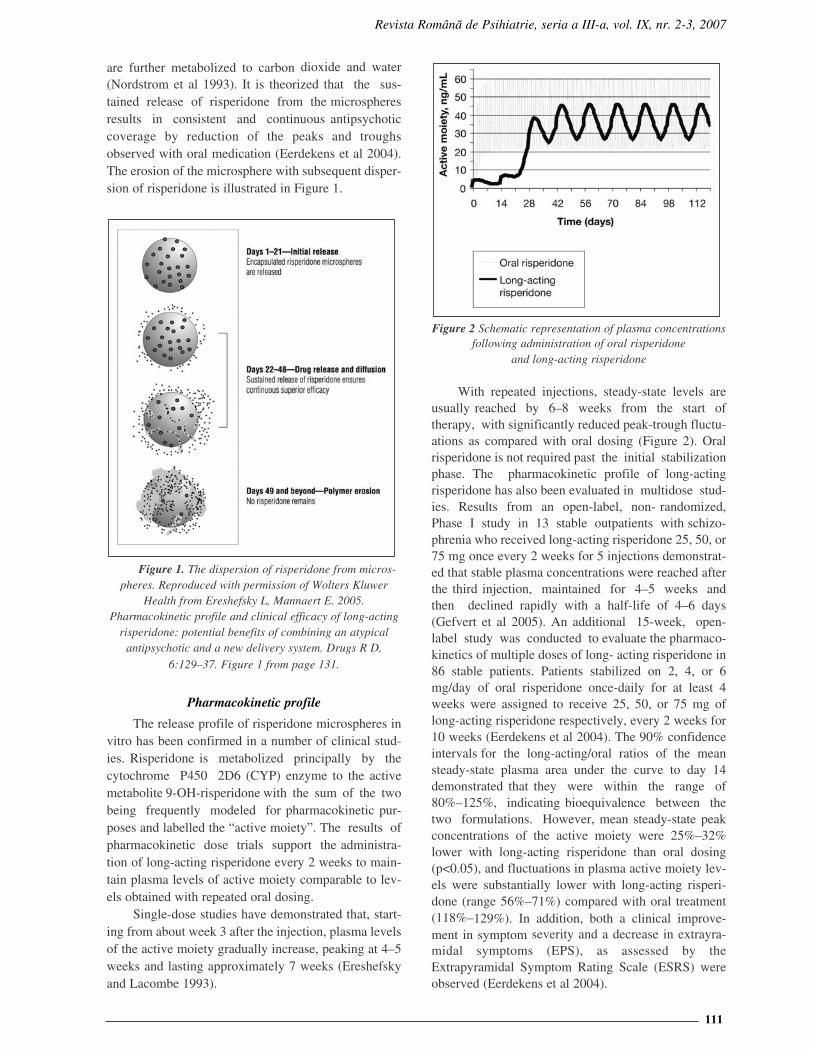
Single-dose studies have demonstrated that, start-ing from about week 3 after the injection, plasma levelsof the active moiety gradually increase, peaking at 4–5weeks and lasting approximately 7 weeks (Ereshefskyand Lacombe 1993).
Figure 2 Schematic representation of plasma concentrationsfollowing administration of oral risperidone
and long-acting risperidone
With repeated injections, steady-state levels areusually reached by 6–8 weeks from the start oftherapy, with significantly reduced peak-trough fluctu-ations as compared with oral dosing (Figure 2). Oralrisperidone is not required past the initial stabilizationphase. The pharmacokinetic profile of long-actingrisperidone has also been evaluated in multidose stud-ies. Results from an open-label, non- randomized,Phase I study in 13 stable outpatients with schizo-phrenia who received long-acting risperidone 25, 50, or75 mg once every 2 weeks for 5 injections demonstrat-ed that stable plasma concentrations were reached afterthe third injection, maintained for 4–5 weeks andthen declined rapidly with a half-life of 4–6 days(Gefvert et al 2005). An additional 15-week, open-label study was conducted to evaluate the pharmaco-kinetics of multiple doses of long- acting risperidone in86 stable patients. Patients stabilized on 2, 4, or 6mg/day of oral risperidone once-daily for at least 4weeks were assigned to receive 25, 50, or 75 mg oflong-acting risperidone respectively, every 2 weeks for10 weeks (Eerdekens et al 2004). The 90% confidenceintervals for the long-acting/oral ratios of the meansteady-state plasma area under the curve to day 14demonstrated that they were within the range of80%–125%, indicating bioequivalence between thetwo formulations. However, mean steady-state peakconcentrations of the active moiety were 25%–32%lower with long-acting risperidone than oral dosing(p<0.05), and fluctuations in plasma active moiety lev-els were substantially lower with long-acting risperi-done (range 56%–71%) compared with oral treatment(118%–129%). In addition, both a clinical improve-ment in symptom severity and a decrease in extrayra-midal symptoms (EPS), as assessed by theExtrapyramidal Symptom Rating Scale (ESRS) wereobserved (Eerdekens et al 2004).

Pierre Chue: Long-acting risperidone injection
112
Dopamine D2-receptor occupancy
Dopamine D2 -receptor occupancy is an impor-tant consideration in determining efficacy and toler-ability. Previous positron emission tomography (PET)studies have indicated that optimal clinical responseoccurs when at least 65% of striatal D2 receptors areoccupied, while the risk of EPS increases notably atD2-receptor occupancy levels above 80% (Kapur et al1999, 2000). To date, available PET data have suggest-ed that dosing long-acting risperidone at 25–50 mgevery 2 weeks is sufficient in attaining clinical responsewith minimal risk of EPS (Farde et al 2002; Gefvert etal 2005; Remington et al 2006).
One such PET study evaluated D2-receptor occu-pancy for long-acting risperidone at doses of 25, 50,or 75 mg administered every 2 weeks in 9 patients withschizophrenia or schizoaffective disorder (Remingtonet al 2006). Patients were scanned twice during the 2-week injection interval: within 3 days after injection(post-injection) and within 5 days before the next injec-tion (pre-injection). Mean post- and pre-injection D2-receptor occupancy levels for the 25, 50, and 75 mgincreased in a dose-dependent fashion and were 71.0%and 54.0%, 74.4%, and 65.4%, and 81.5% and 75.0%,respectively. Although all three doses of long-actingrisperidone demonstrated peak D2-receptor occupancylevels above the 65% threshold associated with optimalclinical response, only the 75-mg dose approximat-ed the 80% threshold linked to increased risk of EPS(Remington et al 2006). A PET study was undertak-en by Gefvert et al to measure D2-receptor occu-pancy at steady state in 8 patients treated with doses of25 (n=3), 50 (n=3), or 75 mg (n=2) of long-actingrisperidone every 2 weeks (Gefvert et al 2005). Dose-proportional individual D2-receptor occupancy was25%–48% in the 25-mg group, 59%–83% in the50-mg group, and 62%–72% in the 75-mg group. Theranges of active moiety concentration were 4.4–8.8ng/mL, 15.0–31.2 ng/mL, and 22.5–26.3 ng/mL forthe three dosages, respectively. Although the D2-receptor occupancy at the 25- mg dose seems somewhatlower than what is considered necessary for an antipsy-chotic effect, it should be taken into account that thedopamine D2-receptor occupancies in this small trialwere trough levels and do not exclude higher occu-pancies at peak plasma concentrations (Gefvert et al2005). However, Farde et al estimated individual D2-receptor occupancy values of long-acting risperidone atboth trough and peak concentrations in a large Phase IIIclinical trial by using plasma concentration and recep-tor binding data from the study by Gefvert et al(Farde et al 2002). Results suggested that mostpatients who responded well to the 25 mg dose hadD2-receptor occupancy values of 50–70% at trough,shifting to values above 70% at peak. Patients in the 50mg group had simulated D2-receptor occupanciescovering the target range of 70–80%, while patientsreceiving the 75 mg dose had D2-receptor occupancies
that were higher than desirable (57% of patients>80% D2- receptor occupancy) with no added clinicalbenefit (Farde et al 2002).
CLINICAL EFFICACY OF LONG-ACTINGRISPERIDONE
Long-acting risperidone is available in dosagestrengths of 25, 37.5, or 50 mg. Although not commer-cially available, several pivotal studies have also inves-tigated the use of a 75-mg dose. As such, results per-taining to the 75-mg dose are also discussed here. Theshort-term (vs placebo) and long-term clinical benefitsof long-acting risperidone were explored in two largeclinical trials, in which long-acting risperidone wasadministered by intramuscular injection at doses of 25,50, and 75 mg every 2 weeks (Fleischhacker et al 2003;Kane et al 2003). A more recent study has alsoinvestigated the use of a 37.5-mg dose (Möller et al2005).
Pivotal and switch studies with long-acting risperidone
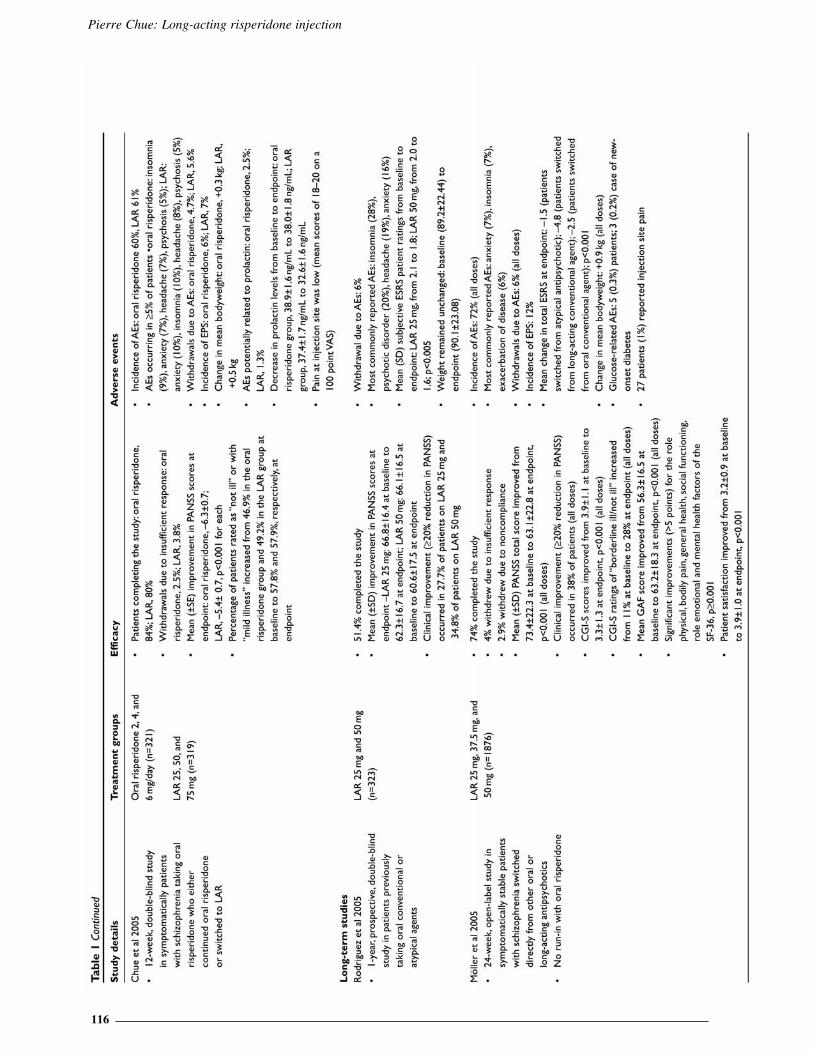
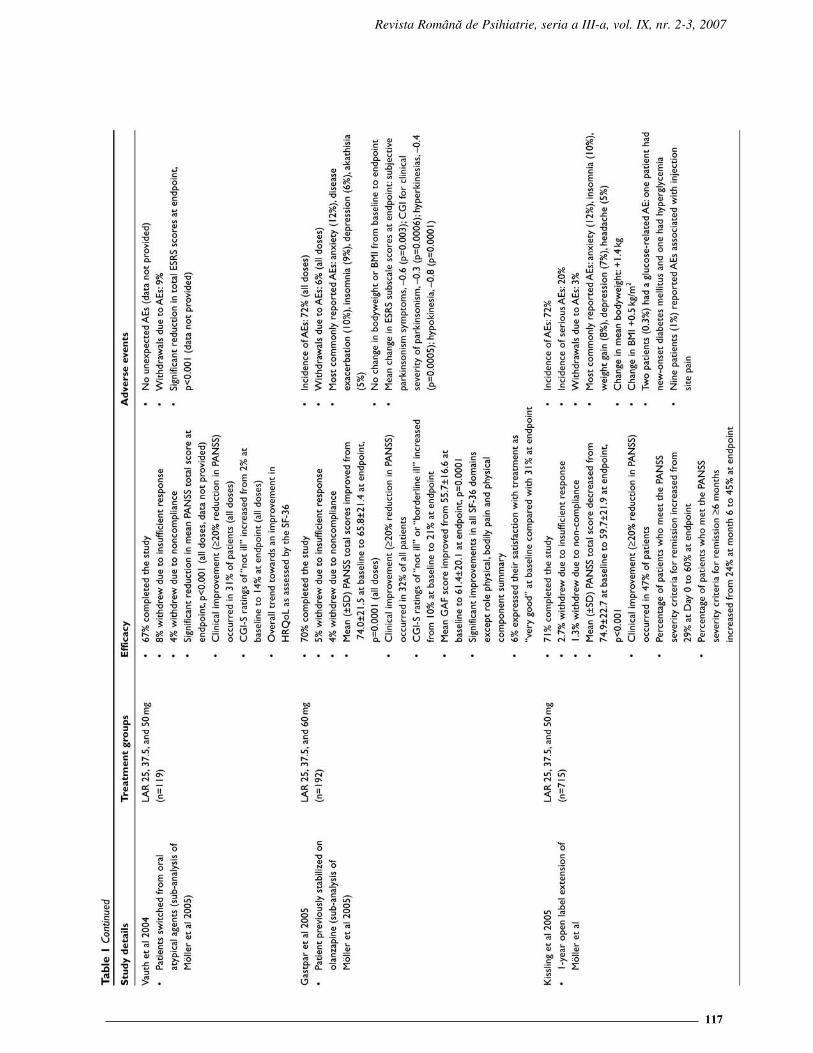
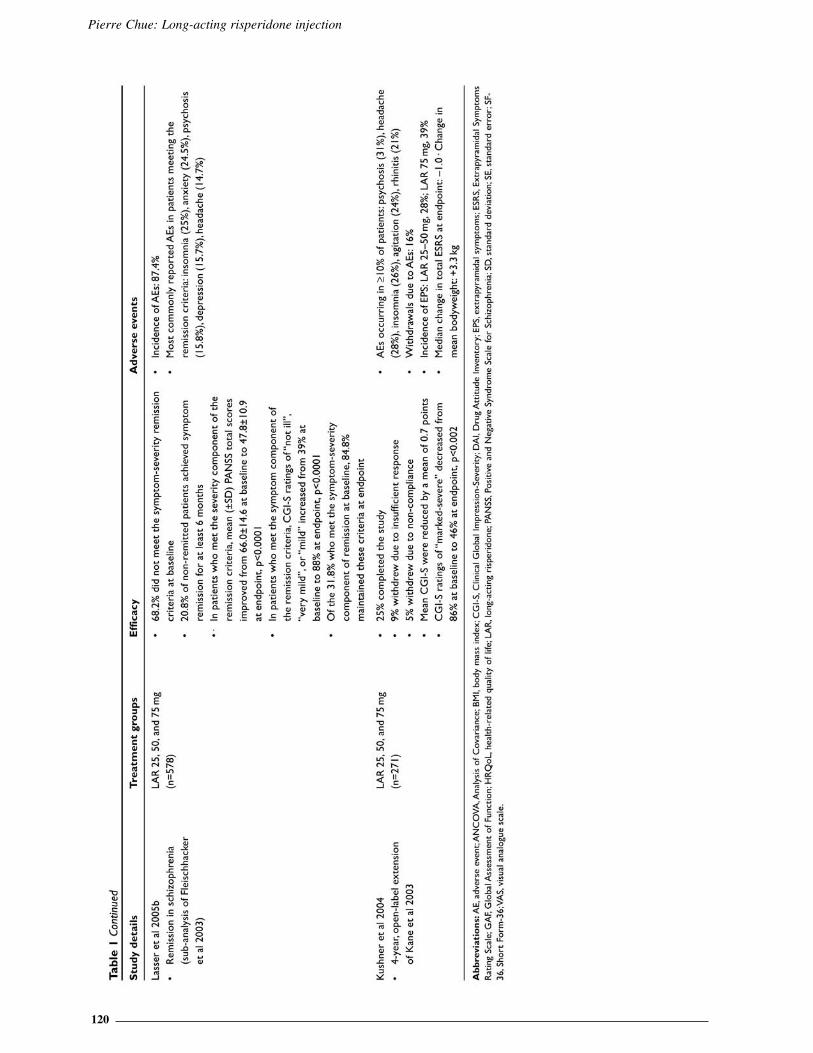
In a 12-week, randomized, placebo-controlled trialby Kane et al, long-acting risperidone was associat-ed with significantly greater improvements inPositive and Negative Syndrome Scale (PANSS) andClinical Global Impression (CGI)-severity scores atendpoint compared with placebo (p<0.001) (Kane et al2003). Significant improvements in total PANSS scores(p<0.01), positive symptoms (p<0.01), and negativesymptoms (p<0.001) were also observed during aninternational, open-label, 1-year study conducted byFleischhacker et al in patients with schizophrenia whowere switched to long-acting risperidone from oral orlong-acting conventional or oral atypical antipsychotics(Fleischhacker et al 2003). Results from a number ofclinical studies and sub-analyses of the 1-year trial havealso reported significant and sustained clinicalimprovement in patients switched, directly or indi-rectly, to long-acting risperidone from oral and long-acting antipsychotic agents. Overall, with the excep-tion of the 4-year open-label extension study byKushner et al, results from the pivotal studiesreported continuation rates with long-acting risperidone(51%–92%) (Chue et al 2005a; Fleischhacker et al2003; Kane et al 2003; Kushner et al 2004;Lindenmayer et al 2004; Turner et al 2004; Emsley etal 2005; Kissling et al 2005; Möller et al 2005).Furthermore, across the pivotal studies, withdrawalsdue to insufficient response (range 1.2%–12.2%) andlack of compliance (range 1.3%–5%) with long-act-ing risperidone were low. An overview of pivotal stud-ies and sub-analyses that have evaluated the efficacy oflong-acting risperidone in patients with schizo-phrenia and schizoaffective disorder is summarizedin Table 1. It is recommended that the original stud-ies be reviewed given the different designs, durations,

Revista Românã de Psihiatrie, seria a III-a, vol. IX, nr. 2-3, 2007
113
and objectives of these studies. For example in thestudies by Chue et al (2005a) and Fleischhacker et al(2003), the dose of long-acting risperidone was basedupon clinical judgement thus, more severe patientstended to receive the higher dose potentially accountingfor treatment failures at this dose. Furthermore, sincethe benefit of a long-acting antipsychotic is accrued inthe longer-term (Gastpar et al 2005; Turner et al 2004;Lee et al 2006; Lindemayer et al 2006,), this may not beapparent initially in short-term studies especiallywhen compared to patients switched from activetreatment to placebo who can show a relative improve-ment to begin with that may be associated, for exam-ple, with the lack of medication side effects (Kaneet al 2003). Switching antipsychotics is not without itscomplexities (Remington et al 2004) and the uniquepharmacokinetics of long-acting risperidone may influ-ence the outcome in short-term studies involvingswitching in stable patients (Lindenmayer et al 2004),or in patients that were previously on high dose or com-bination antipsychotic therapies (Kane et al 2003).
Long-acting conventional antipsychotic and long- acting risperidone studies
Few studies have examined the efficacy oflong-acting risperidone compared with a long-actingconventional agent. This likely due to the fact that ran-domization to conventional depot is no longer consid-ered a standard of treatment for patients with schizo-phrenia, and such a study would not be acceptable tothe majority of research ethics boards (certainly inNorth America and Canada) (Quraishi and David2000). Thus, the two studies that have examined long-acting injectable treatments have been open-labelcomparisons in special populations. In the first 6-month study, 115 patients fulfilling the criteria forschizophrenia and substance abuse disorder were allo-cated to receive either long-acting risperidone n=57)or long-acting zuclopenthixol (n=58). Overall, long-acting risperidone (mean dose 47.2 mg q15 days and3.4 mg oral risperidone) was shown to be moreeffective than long-acting zuclopenthixol (mean dose200 mg q21 days and 15 mg oral zuclopenthixol) inimproving the symptoms of schizophrenia (mean[±SD] PANSS total scores improved from 93.79±22.9at baseline to 64.39±19.9 at endpoint for the long-act-ing risperidone group vs 93.69±22.5 at baseline to74.03±20.9 for the long-acting zuclopenthixol group).Long-acting risperidone was also more effective intreating substance abuse (mean [±SD] number of total
positive tests for substance abuse: long-acting risperi-done 8.67±3.0 vs 10.36±3.1 for long-actingzuclopenthixol, p=0.005). More patients receivinglong-acting risperidone attended more than 75% ofaddiction counselling sessions compared with patientsreceiving long-acting zuclopenthixol (92.9% vs67.8%, p=0.001) (Rubio et al 2006). In the secondstudy of chronic hospitalized patients with schizophre-nia followed up for one year, of 40 patients treatedwith long-acting risperidone, 83% were discharged andnone readmitted. In contrast, of 54 patients treated withconventional depot, 58% were discharged and 26% re-admitted (Snaterse et al 2005).
Oral atypical antipsychotics and ong-acting risperidone studies
The large and often contradictory literature exam-ining the efficacy of oral atypical antipsychotics inhead-to-head comparisons illustrates the difficulty indemonstrating substantial differences between effica-cious agents particularly when dosing and titration arecontrolled. A non- inferiority analysis of oral risperi-done and long-acting risperidone found that long-acting risperidone was as efficacious and as well tol-erated as oral risperidone in a 20- week randomized,double-blind, double-dummy study (Chue et al 2005a).It is known from earlier studies with conventionalantipsychotics comparing a long-acting injection to itsoral equivalent, that benefits secondary to improvedcompliance are demonstrated with greater duration ofstudy and maintenance of adequate serum levels(Jayaram et al 1986). Since non-compliant patients,although representing a significant proportion of real-world patients with schizophrenia and other psychoses,are rarely recruited to clinical trials, this poses prob-lems in demonstrating the benefit of a treatment that islikely to be advantageous in that very population. Theonly other study presented to date comparing long-act-ing risperidone injection to an oral atypical antipsy-chotic is being conducted in first-episode patients.Malla et al have shown preliminary data on a 24-month, prospective, open-label, multi-center study inyoung adults (aged 18–30 years) with recentonset schizophreniform disorder, schizophrenia, andschizoaffective disorder (£3 years) (Malla et al 2006).The effectiveness data set is very small (n=15), butmean changes in CGI-S (±SD) and total PANSSscores for long-acting risperidone were –0.7±1.3 and–16.1±16.2 respectively, and for oral atypical antipsy-chotics were –0.2± 0.8 and –5.0±12.9 respectively.

Pierre Chue: Long-acting risperidone injection
114

Revista Românã de Psihiatrie, seria a III-a, vol. IX, nr. 2-3, 2007
115
Pierre Chue: Long-acting risperidone injection
116
Revista Românã de Psihiatrie, seria a III-a, vol. IX, nr. 2-3, 2007
117

Pierre Chue: Long-acting risperidone injection
118

Revista Românã de Psihiatrie, seria a III-a, vol. IX, nr. 2-3, 2007
119
Pierre Chue: Long-acting risperidone injection
120

Revista Românã de Psihiatrie, seria a III-a, vol. IX, nr. 2-3, 2007
121
Achieving and maintaining remission in schizophrenia
Recently, operational criteria for remission inschizophrenia have been proposed by the Remissionin Schizophrenia Working Group (Andreasen et al2005). The consensus definition of remission wasdefined as achieving a score £3 (mild or less) simulta-neously in seven core PANSS items: delusions [P1],conceptual disorganization [P2], hallucinations [P3],unusual thought content [G9], mannerisms and pos-turing [G5], blunted affect [N1], passive/apatheticsocial withdrawal [N4], and lack of spontaneity andflow of conversation [N6], sustained for a minimumduration of 6 months (Andreasen et al 2005).
To date, the consensus remission criteria havebeen retrospectively applied to two clinical studies,which primarily evaluated the efficacy of long-actingrisperidone (Table 1) (Kissling et al 2005; Lasser et al2005b). The first was a sub-analysis of the 1-year trialby Fleischhacker et al (2003) in patients with schizophre-nia who were switched to long-acting risperidone fromoral or long-acting conventional or oral atypical antipsy-chotics. Although all patients in this study were consid-ered clinically “stable” at baseline, 68.2% (394/578) didnot meet the symptom- severity component of remissionat baseline (Lasser et al 2005b). Following treatment withlong-acting risperidone, 20.8% (n=82) of non-remittedpatients achieved symptom remission for at least 6months, with significant decreases in mean PANSS totaland subscale scores (p<0.0001). Finally, out of the184 patients who met the symptom- severity compo-nent of the remission criteria at baseline, 84.8%(n=156) maintained their remitted status after 1 year oftreatment (Lasser et al 2005b).
The second study assessed data from an extensionphase of a 6-month trial in 715 stable psychotic patientswho were transitioned directly from their previousantipsychotic regimen to long-acting risperidone (25,37.5, or 50 mg), without an oral risperidone run-in(Kissling et al 2005). The proportion of patients whomet the PANSS severity criteria for remission increasedfrom 209 (29%) at baseline to 429 (60%) at endpoint.Among those patients who met the severity criteriaat study entry, 84% met them at endpoint. Furthermore,79% of those patients met both the severity and theduration criteria for remission at endpoint. Of the 506patients who did not meet the severity criteria atbaseline, 50% did so at endpoint. At 12 months 31% ofthose patients met both the severity and duration crite-ria and were therefore considered to be in remission(Kissling et al 2005).
Health-related quality of life, patient satisfaction and functioning
The concept of health-related quality of life(HRQoL) has not been a treatment outcome focusedupon in studies until the last few years. Nonetheless,when patients are asked directly what is important to
them in terms of treatment, it is in fact such measuresas improvement in overall happiness, mental healthand functionality (Hufnagel et al 2004). These patientbenefits are not easily shown through standard studiesconducted in the context of drug registration andapproval, which are designed with very specific effica-cy and tolerability perspectives.
Results from the 6-month study by Möller et al(2005) and a number of its sub-analyses have demon-strated that patients experience significant improve-ments in HRQoL and patient satisfaction followingtreatment with long-acting risperidone (Table 1). Inaddition, a number of studies have been specificallyundertaken to examine the effect of long- acting risperi-done on QoL and social functioning. A post- hoc analy-sis by Nasrallah et al measured HRQoL using the SF-36 scale in patients who participated in the 12-weekstudy by Kane et al (2003) (Nasrallah et al 2004). Atweek 12, patients receiving long-acting risperidone 25mg and 50 mg had improved significantly in five of theeight domains of the SF-36 (bodily pain, general health,social functioning, role-emotional, and mental health)compared with patients receiving placebo. No signifi-cant differences in seven of the eight measures wereobserved between the long-acting risperidone 25-mgsubject group and US normal population scores (indi-viduals aged 35–44 years). In contrast, subjects in theplacebo group had a significantly poorer QoL com-pared with the US normal population in all measures(p<0.01). Similarly, a sub-analysis of the data from the1- year study by Fleischhacker et al also found thatlong-acting risperidone resulted in a significantimprovement on the SF-36 Mental ComponentSummary score and on the vitality and social func-tioning scales (Fleischhacker et al 2005).
Recently a 1-year, randomized, double-blind, mul-ticenter study was undertaken to examine the effects oflong-acting risperidone on social functioning usingthe Personal and Social Performance (PSP) Scale(Rodriguez et al 2005). The PSP scale provides a clini-cian rating of personal and social functioning on a 100-point scale based on the assessment of patient’s func-tioning in four important domains: a) socially use-ful activities, including work and study; (b) person-al and social relationships; (c) self-care; and (d) dis-turbing and aggressive behaviors (Morosini 2000).
Results demonstrated significant improvements inthe Personal and Social Performance Scale (PSP) scoresfrom baseline to endpoint (p=0.003). In addition, assess-ments on the Strauss-Carpenter Level of FunctioningScale (LOF) indicated that patients had a greater fre-quency of social contacts, increased quality of relation-ships, and a improved overall level of function duringmaintenance treatment with long-acting risperidone.
Safety and tolerability of long-acting risperidone
On the basis of the results from the studies byKane et al and Fleischhacker et al, long-acting risperi-

Pierre Chue: Long-acting risperidone injection
122
done generally appears to be well tolerated, with anoverall incidence of adverse events similar to that withplacebo in comparative trials. In the study by Kaneet al, similar proportions of patients in the placeboand long-acting groups (80%–83%) reported adverseevents, while serious adverse events were more fre-quent in the placebo group (23.5%) than in the 25, 50,and 75 mg long-acting risperidone groups (13%, 14%,and 15%, respectively) (Kane et al 2003). Likewiselong- acting risperidone was also well tolerated in thelong-term study by Fleischhacker et al with the per-centage of patients reporting adverse events decliningfrom 68% during months 1–3 of the study to 43% dur-ing months 10–12 (Fleischhacker et al 2003). Resultsfrom a number of studies have also reported thatpatients can be safely transitioned from oral conven-tional or atypical therapy and conventional long-acting agents to long-acting risperidone (Lasser et al2004a; Lindenmayer et al 2004; Turner et al 2004; vanOs et al 2004). Furthermore, one such study byMöller et al demonstrated that switching from exist-ing antipsychotic therapy to long-acting risperidone,without an oral risperidone run-in, was well toleratedin a large cohort of patients with schizophrenia orother psychotic disorders (Möller et al 2005). Severalstudies have also reported that patients consideredsymptomatically stable on oral risperidone can besafely switched to long-acting risperidone (Chue et al2005a; Lasser et al 2005a), thereby contradicting theperception of some clinicians and patients that adverseevents are more common with long-acting than withoral formulations.
Overall, relatively few patients have withdrawnin studies with long-acting risperidone due to adverseevents (range 1.2%–16%) (Fleischhacker et al 2003;Kane et al 2003; Kushner et al 2004; Lindenmayer et al2004; Turner et al 2004; Chue et al 2005a; Lasser et al2005a; Möller et al 2005; Emsley 2006). The mostcommon adverse events reported with long-actingrisperidone were headache (range 7%–28%), insomnia(range 7%–28%), anxiety (range 7%–24%), and psy-chosis (range 5%–31%). In the majority of studies theseverity of movement disorders, as assessed by theESRS, was unchanged or further reduced duringtreatment with long-acting risperidone. In addition, asub- analysis of the 1-year study demonstrated thatlong-acting risperidone is associated with a low inci-dence of treatment- emergent dyskinesia (1.2% annu-ally) (Gharabawi et al 2005). Three studies, whichexamined the effect of long- acting risperidone onserum prolactin levels, reported rates of hyperpro-lactinemia of 1.3%–7% (Lindenmayer et al 2004;Turner et al 2004; Chue et al 2005a).
Metabolic side-effects in patients treated withatypical antipsychotic agents are increasingly receiv-ing more attention in the literature, with recent evi-dence suggesting that some atypical antipsychotics mayincrease risk factors for diabetes and cardiovascular
disease, including increased adiposity and adverseeffects on glucose and lipid metabolism (ADA 2004;Citrome 2004). On the basis of the limited evidencepresented here from the pivotal trials, weight gain withlong-acting risperidone was low, being in the range of0.5–2 kg in the short-term (12 weeks) and around 3kg after 1 year of treatment, with no further weight gainapparent in patients receiving long-acting risperidonefor up to 4 years (Kushner et al 2004). In addition,results from a short-term study demonstrated that serumglucose and triglyceride levels were reducing duringtreatment with long-acting risperidone (Lindenmayer etal 2004), while a further study reported a low occur-rence (0.3%) of glucose- related adverse events over 6months (Möller et al 2005).
Finally, in the patient populations studied,including antipsychotic injection-naive patients, theperception of pain at the injection site was rated as mildand decreased over time (Fleischhacker et al 2003;Kane et al 2003; Lindenmayer et al 2004; Turner et al2004; Chue et al 2005a; Lindenmayer et al 2005). Itis postulated that the low incidence of injection sitepain could be related to the fact that long-actingrisperidone is an isotonic water-based suspension hasbeen shown to be easier and less painful to administerthan the oil-based solutions of the conventional long-acting antipsychotic agents (Bloch et al 2001). A fulloverview of the safety data for long-acting risperidoneis also shown in Table 1.
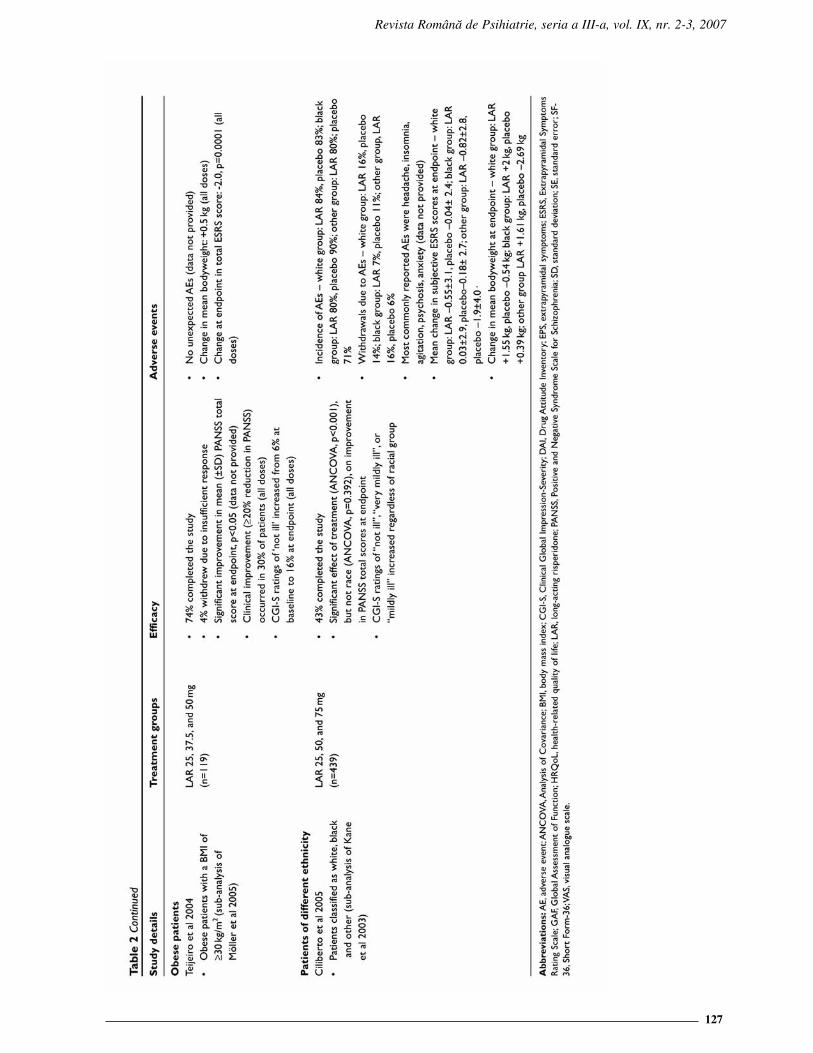
Efficacy and safety of long-acting risperidone in special populations
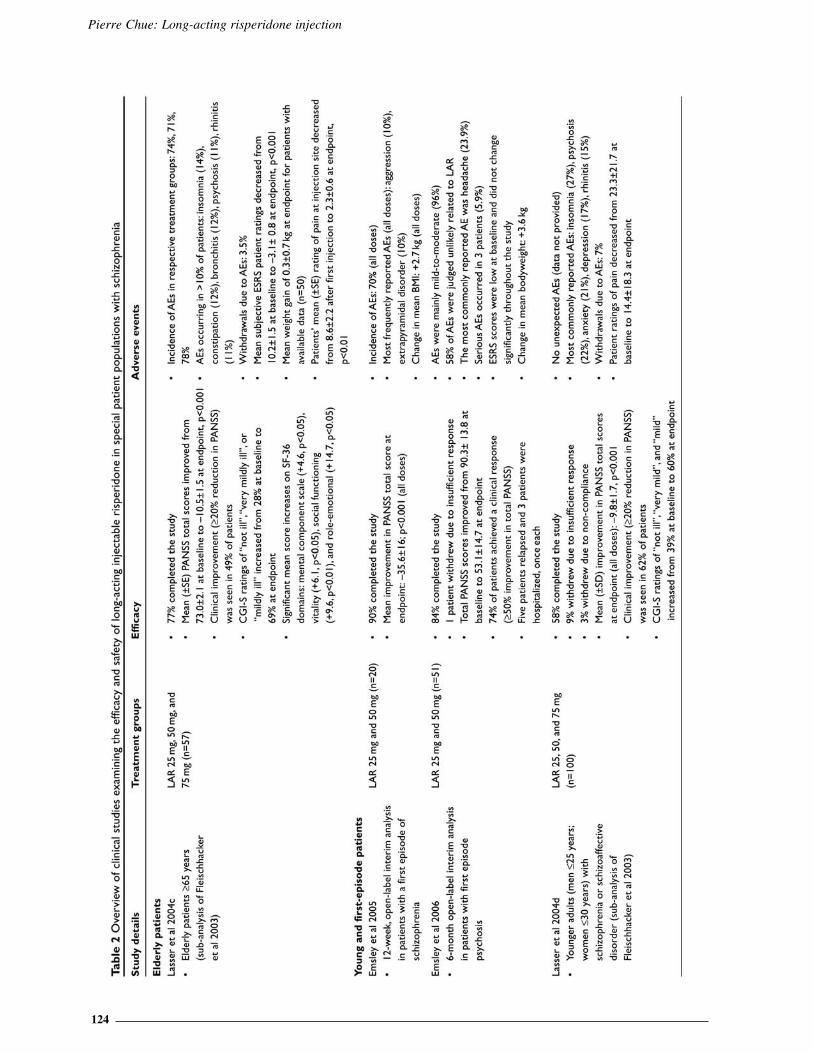
Certain populations such as the elderly, youngadults or those with a first episode of schizophrenia,patients with schizoaffective disorder and patients ofdifferent ethnicity require special consideration henselecting pharmacotherapy. A number of studies havedemonstrated that long-acting risperidone is botheffective and well tolerated in these populations(Table 2). However, it is important to note that theseresults are based solely on sub- analyses and interimanalyses and, as such, further controlled studies oflong-acting risperidone in these vulnerable patientgroups are warranted.
Elderly patients
Elderly patients with schizophrenia have gen-erally been neglected in the research literature, butoften suffer from persistent symptoms and cognitivedeficits (Davidson et al 2000). Elderly patients alsohave a greater sensitivity to treatment-relatedadverse effects, a higher rate of co- morbidities andan increased risk of medication interactions (Masand2000). A sub-analysis of the 12-month study byFleischhacker et al examined the efficacy and safety oflong-acting risperidone in elderly patients ( 65years) with schizophrenia and schizoaffective disor-der (Lasser et al 2004c). Long-acting risperidonewas associated with significant improvements as

Revista Românã de Psihiatrie, seria a III-a, vol. IX, nr. 2-3, 2007
123
determined by PANSS (p<0.001) and CGI-S assess-ment scales. Moreover, despite the age of this popula-tion and high rate of polypharmacy, the incidence ofadverse events of particular concern such as cardiaceffects and movement disorders, was low.
Importantly, no new cases of tardive dyskine-sia were reported in this high-risk group and symptomsof movement disorders were reduced compared to base-line (Lasser et al 2004c).
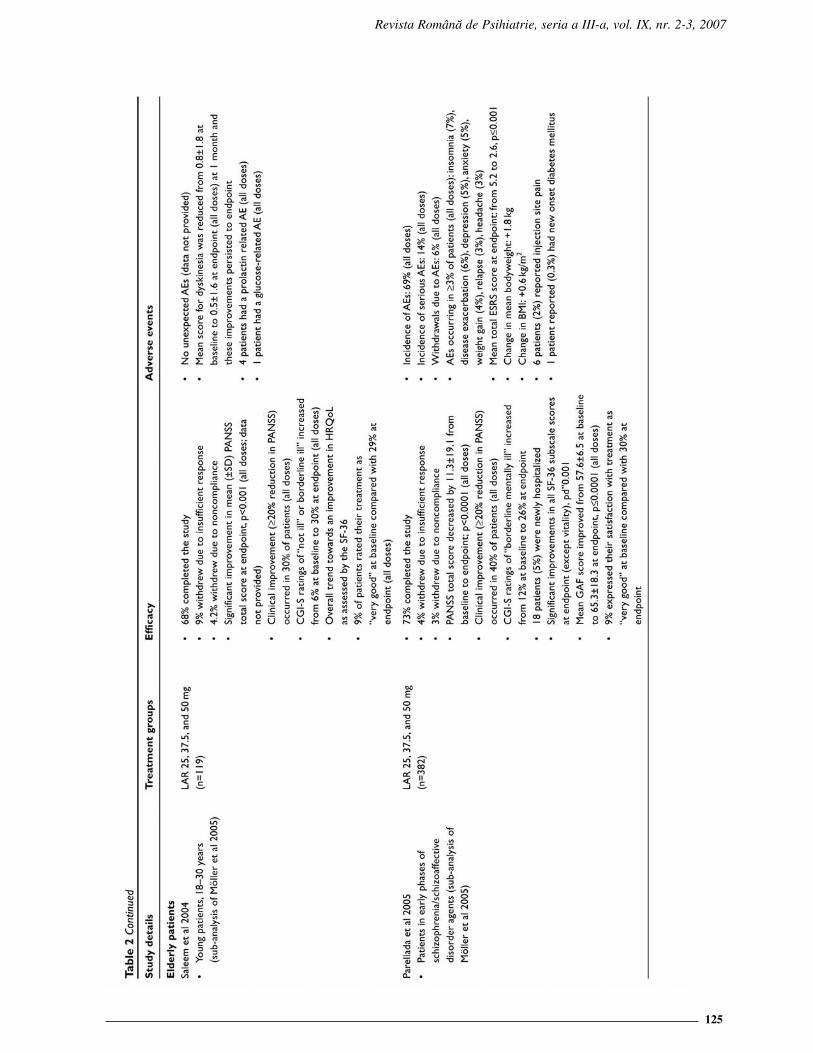
Young patients or patients with a first episode ofschizophrenia
The early recognition and management of first-episode schizophrenia is a challenging task. Althoughthese patients are the most responsive to treatment,they are also very sensitive to adverse events andoften lack “disease insight”, which contribute to poorcompliance and high treatment discontinuation rates(Kasper 1999). A recent subanalysis of the 6-monthstudy by Möller et al examined the efficacy and safetyof long-acting risperidone in patients in the early phas-es of schizophrenia and schizoaffective disorders(Parellada et al 2005). Following initiation of long-act-ing risperidone statistically significant improvementswere seen in the control of symptoms and the severityof schizophrenia (both PANSS and CGI-S), as well asGlobal Assessment of Functioning (GAF), HRQoL,patient satisfaction, and EPS (Parellada et al 2005). Anumber of other sub-analyses have also reported thatlong-acting risperidone was efficacious and wellaccepted in young adults with schizophrenia orschizoaffective disorder (Lasser et al 2004d; Saleem etal 2004) (Table 2). In addition, Emsley et al, has report-ed on the 6-month interim data on 51 patients with firstepisode psychosis with 74% of patients achieving 50% reduction in the PANSS (Emsley et al 2005).
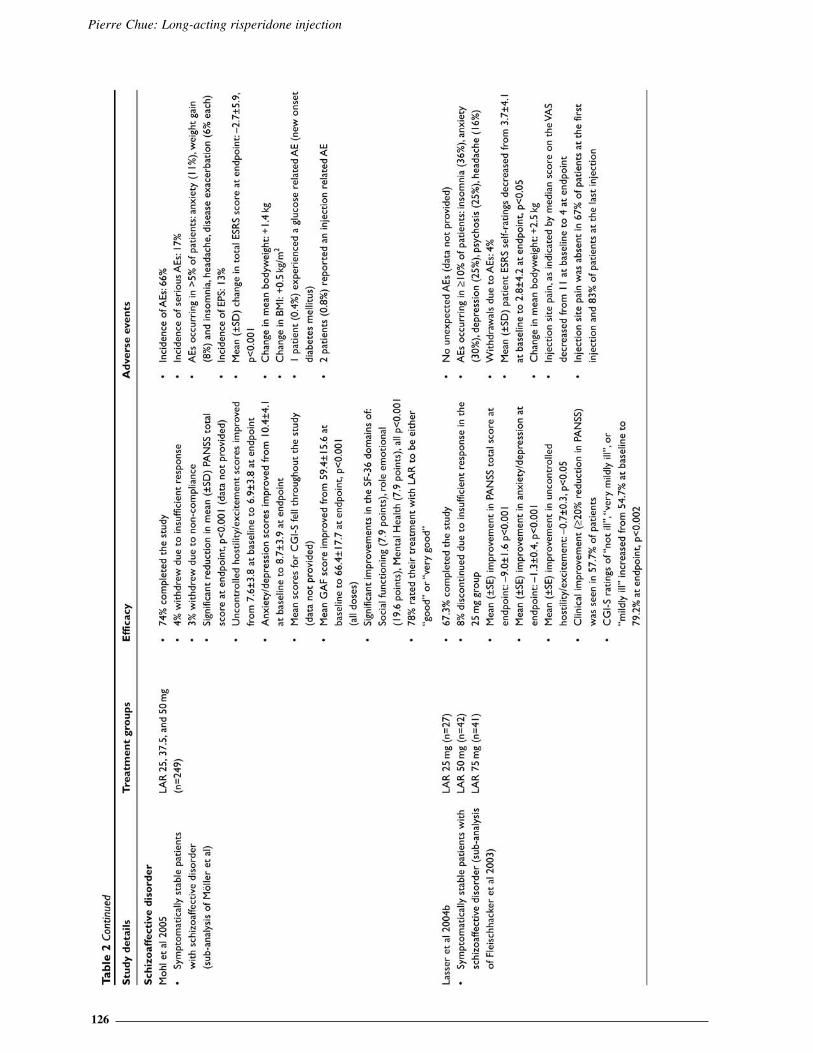
Patients with schizoaffective disorder
Schizoaffective disorder is a complex disorderto both diagnose and successfully treat, often requir-ing a combination of different classes of medicationsincluding an antipsychotic and an antidepressant ormood stabiliser (Levinson et al 1999). Two analyseswere identified which examined the efficacy of long-acting risperidone in stable patients with schizoaffec-tive disorder (Lasser et al 2004b; Mohl et al 2005)(Table 2). Data from these two studies suggest that sig-nificant clinical benefits follow a switch to long-actingrisperidone in symptomatically stable patients withschizoaffective disorder, despite the fact that PANSSscores were low at baseline and further clinicalimprovement would not necessarily be anticipated. Of
particular note for patients with schizoaffective disor-der were the significant improvements in the two symp-tom domains relating to mood – the anxiety/depres-sion factor and the uncontrolled hostility/excitementfactor (Lasser et al 2004b; Mohl et al 2005). The reduc-tion in psychopathology symptoms was also accom-panied by significant improvements in CGI-S scores,GAF scores and improvements in HRQoL, asassessed by the SF-36 (Lasser et al 2004b; Mohl et al2005).
Patients of different ethnicity
Several studies have suggested that African-American patients may respond differently to treatmentthan do other racial or ethnic groups (Emsley et al2002). The nature of these differences is poorlyunderstood but may reflect genetic, pharmacokinetic,cultural, or environmental factors (Frackiewicz et al1997; Poolsup et al 2000). To date, the impact of raceon the efficacy and safety of long-acting risperidonein Caucasian, African-American and other patientswith schizophrenia or schizoaffective disorder has beenexamined in a sub-analysis of the 12-week, placebo-controlled study by Kane et al (Ciliberto et al 2005)(Table 2). Results demonstrated that there was a signif-icant effect of treatment (p<0.001), independent ofrace, on the improvement in mean PANSS total scores.
Obese patients
Weight gain and obesity have been reported inpatients receiving both conventional and atypicalantipsychotics, and are associated with increased risksfor hypertension, stroke, osteoarthritis, and particular-ly for coronary heart disease and type 2 diabetes(Ganguli 1999). To date, one study has been undertak-en to investigate the efficacy of long-acting risperidonein obese patients (body mass index of 30 kg/ m2) withschizophrenia or schizoaffective disorder (Table 2).Results demonstrated that there were significantreductions from baseline in mean total PANSS scores at1 month and these continued throughout the trial.Overall, the efficacy of long-acting risperidone in obesepatients was comparable to that reported for schizo-phrenia patients in general (Marder et al 1997).Importantly, bodyweight remained stable throughoutthe 6-month study period, with a mean increase of 0.5kg. Furthermore, despite the high BMI of thepatients, approximately half of the patients remainedon the starting dose of long-acting risperidonethroughout the study.
Pierre Chue: Long-acting risperidone injection
124
Revista Românã de Psihiatrie, seria a III-a, vol. IX, nr. 2-3, 2007
125
Pierre Chue: Long-acting risperidone injection
126
Revista Românã de Psihiatrie, seria a III-a, vol. IX, nr. 2-3, 2007
127
Pierre Chue: Long-acting risperidone injection
128
The cost-effectiveness of long-acting risperidone
Healthcare costs in schizophrenia are dispro-portionately high. Although the illness affects approxi-mately 1% of the world’s population, it accounts forup to 3% of health expenditure (Knapp 2000). Relap -ses increase refractoriness to future treatment leading tomore frequent and prolonged hospitalization, and con-tribute significantly to the economic burden of schizo -phrenia. Results from a recent study demonstrated afour-fold increase in costs among patients experiencingrelapse, compared to those who did not (Almond etal 2004). Overall, 79% of the direct costs of schizo-phrenia result from hospitalization or other residentialcare, while medications represent only a small fraction(1%–6%) of the total cost of schizophrenia (Foster andGoa 1998; Davies and Drummond 1994; Goeree etal 2005). It is expected that the introduction oflong-acting risperidone with its potential to improvecompliance and decrease relapse should lead to lowerlevels of healthcare resource use.
Hospitalization rates, healthcare resource utilization,and relapse rates with long-acting risperidone
Hospitalization rates were assessed as part ofa 1-year international, open-label trial of long-actingrisperidone in inpatients and outpatients with stableschizophrenia or schizoaffective disorder (Chue et al2005b). Of the 397 patients who received a modaldose of long-acting risperidone 25 mg or 50 mg, 24%
were inpatients and 76% were outpatients at baseline.Results demonstrated that the number of patientsrequiring hospitalization decreased continuously andsignificantly from 38% in the 3 months before treat-ment to 12% during the last 3 months of treatment(p<0.001). Of baseline inpatients, 71% were dis-charged during treatment. Overall, the 1-year re-hospi-talization rate was 17.6%, with a rate of 15.9% for base-line outpatients (Chue et al 2005b). A further analysisof this study examined healthcare resource utilizationduring 1-year treatment with long-acting risperidone(Leal et al 2004). Results demonstrated that meanhospitalization length during the study was 30.5 days(outpatients, 4.9 days; inpatients 110 days). The needfor partial hospitalization (day or night clinics)decreased significantly over the 12-month period, from7% during the 12 weeks before treatment to 3% duringthe last 12 weeks (p=0.002). The need for outpa-tient consultations also decreased significantly from70% in the 12 weeks before treatment to 30%(p<0.0001) during the first 12 weeks of treatment.The need for outpatient consultation remained stablethroughout the remainder of the treatment period.Overall, only 9% of patients required an emergencyroom visit, mostly for non-psychiatric conditions(Leal et al 2004).
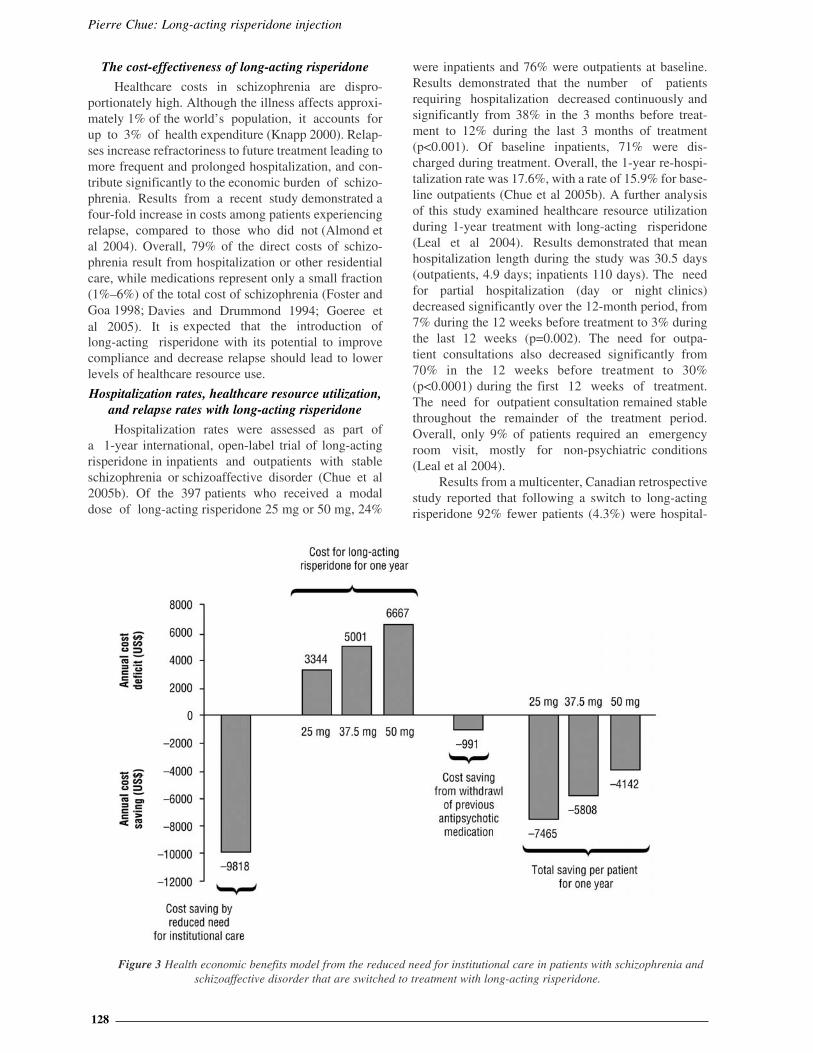
Results from a multicenter, Canadian retrospectivestudy reported that following a switch to long-actingrisperidone 92% fewer patients (4.3%) were hospital-
Figure 3 Health economic benefits model from the reduced need for institutional care in patients with schizophrenia andschizoaffective disorder that are switched to treatment with long-acting risperidone.

Revista Românã de Psihiatrie, seria a III-a, vol. IX, nr. 2-3, 2007
129
ized post-initiation compared with prior (50.7%),(p<0.0001). Furthermore, total duration of hospital-ization days decreased by 99% (p<0.0001) and anti-cholinergic and anxiolytic use fell by 22% (p=0.0719)and 38% (p=0.0252), respectively (Chue et al 2005d).Of note, preliminary data from a Swedish multi-center study in 92 patients have demonstrated that forpatients treated with long-acting risperidone, thetotal number of hospitalizations was reduced by 38%(p=0.0004) compared with the same observational peri-od when treated with their previous antipsychotictherapy (Eriksson et al 2003). Using an empirical eco-nomic model, based on the Swedish costs, the meanannual cost savings can be calculated per patientfollowing a switch to long-acting risperidone withinthe recommended dose range (Figure 3). Finally, a 1-year mirror image observational study was under-taken to investigate predictors of relapse (defined ashospital admission) for patients (n=142) on long-acting risperidone (Patel et al 2006). Results demon-strated that patients who discontinued long-actingrisperidone (0–12 months) were 3 times more likely torelapse than continuers at 1 year (odds ratio [OR] 3.08,95% confidence interval [CI]: 1.39–6.81, p=0.003).Clinically unstable patients (those admitted in theyear preceding long-acting risperidone treatment)were much more likely to relapse than those who wereclinically stable (OR 6.58, 95% CI: 2.77–15.66,p<0.001). No statistically significant differences werefound for relapse in terms of sociodemographic factors,diagnosis and illness duration, medication historyand clinical indication for long-acting risperidone(Patel et al 2006). As such, patients who receive con-sistent and continuous treatment with long-actingrisperidone may be expected to have a lower incidenceof relapse rates and, therefore, an improved long-termprognosis.
Pharmacoeconomic evaluations of long-actingrisperidone
The use of modeling as a means of assessing theeconomics of health interventions has increased consid-erably in recent years. A number of studies haveemployed either discrete event simulation or decisionanalytic models, both of which theoretically addressthe heterogeneous and real-world characteristics ofpatients with schizophrenia, to examine the costs oflong-acting risperidone compared with oral and con-ventional long-acting agents in the US, Canada,Belgium, and Germany (Chue et al 2005c; De Graeveet al 2005; Edwards et al 2005; Laux et al 2005).
In the US, a decision analytical model capturedrates of patient compliance, rates, frequency and dura-tion of relapse, incidence of adverse events, andhealthcare resource utilization and associated costswith 7 treatment alternatives (Edwards et al 2005).Primary outcomes were expressed in terms of percent-
age of patients relapsing per year, number of relapsedays per year, and total direct 2003 medical cost perpatient per year. On the basis of model projections,patients receiving long-acting risperidone will have thebest clinical outcomes in terms of the frequency andduration of relapses. Over a period of 1 year, this wouldtranslate into direct medical cost-savings with long-acting risperidone compared with oral risperidone,olanzapine, quetiapine, ziprasidone, aripiprazole, andlong-acting haloperidol of US$161, 1425, 508, 259,1068, and 8224, respectively (Edwards et al 2005).
In Canada, a discrete-event model wasdesigned to evaluate the cost-effectiveness of long-act-ing risperidone for patients with schizophrenia at ahigh risk of non- compliance, compared with 2 stan-dard treatment alternatives (oral risperidone and long-acting haloperidol) over a 5-year period (Chue et al2005c). On the basis of 3000 simulated patient charac-teristics, the model generated individual patient his-tories. Outcomes included the number and durationof psychotic episodes, the cumulative PANSS scoreand direct medical costs. The time horizon of themodel was 5 years and a 5% discount rate was used forcosts and effects. In this model, initiating treatmentwith long-acting risperidone was the dominant strat-egy. After 5 years, treatment with long-acting risperi-done saved Can$6908 and Can$13130 (discounted) andavoided 0.28 and 0.54 relapses per patient, comparedwith long-acting haloperidol and oral risperidone,respectively (Chue et al 2005c).
In the Belgian model, a decision tree model wascreated to compare the cost effectiveness of three first-line treatment strategies in a sample of young schizo-phrenia patients who had been treated for 1 year andwhose disease had not been diagnosed for longer than 5years (De Graeve et al 2005). This model used a timehorizon of 2 years, with health state transition proba-bilities, resource use and cost estimates derived fromclinical trials, expert opinion, and published prices. Theprincipal efficacy measure was the proportion
of patients successfully treated, defined asthose who responded to initial treatment and whohad none to two episodes of clinical deteriorationwithout needing a change of treatment over the 2-yearperiod. A greater proportion of patients were success-fully treated with long-acting risperidone (82.7%) for2 years, compared with those treated with oral olanza-pine (74.8%) or long-acting haloperidol (57.3%).Total mean costs per patient over 2 years were 16406 with long-acting risperidone, 17 074 witholanzapine, and 21 779 with long-acting haloperidol(year of costing 2003) (De Graeve et al 2005).Similarly, the mean cost-effectiveness ratios were 19 839, 22 826, and 38 008 per successfullytreated patient for long-acting risperidone, olanzap-ine, and haloperidol, respectively. Cost savings werealso observed when long-acting risperidone was com-pared with oral olanzapine and long-acting haloperi-

Pierre Chue: Long-acting risperidone injection
130
dol in a German study (Laux et al 2005). In this study adiscrete-event simulation model was developed to com-pare the benefits and costs of three pharmacologi-cal treatment strategies from the perspective of majorthird party payers (sickness funds and social security)over a 5-year period in Germany. The model accountedfor fixed patient characteristics, and on the basis ofthese, simulated patient histories according to severaltime-dependent variables. In accordance with Germanguidelines, costs and effects were discounted bybetween 3% and 10%. Outcomes were expressed interms of the number and duration of psychoticepisodes, cumulative symptom scores, costs, and quali-ty- adjusted-life-years (QALY). The long-actingrisperidone strategy was calculated to avoid 0.23 and0.33 relapses per patient, decrease the cumulativesymptom score by 25 and 33 points, and decrease costsby 2017 and 6096 per patient ( 1608 and 5422discounted), compared with the long- acting haloperi-dol and olanzapine strategies respectively, over 5 years(Laux et al 2005).
Discussion
It is recognized that long-acting antipsychoticsfacilitate compliance with medication, and may help toprevent relapse and improve functional outcomes inpatients with schizophrenia (Gerlach 1994).Accordingly, the guidelines for long-acting antipsy-chotic treatment that were developed by a EuropeanNeuropsychopharmacology Consensus Conferencerecommend that: “any patient for whom long-termantipsychotic treatment is indicated should be con-sidered for depot drugs” (Kane et al 1998). Thedevelopment of long-acting risperidone, which com-bines the benefits of an atypical agent with the advan-tages of a long-acting formulation, represents an impor-tant new option for the long-term management ofpatients with schizophrenia.
Results from the studies presented here havedemonstrated that long-acting risperidone 35, 37.5,or 50 mg, administered once every 2 weeks, is botheffective and well tolerated in patients with schizo-phrenia or schizoaffective disorder (Fleischhacker et al2003; Kane et al 2003; Lindenmayer et al 2004; Turneret al 2004; Chue et al 2005a; Möller et al 2005). Inaddition, several patient groups, including the young,the elderly, patients with schizoaffective disorder, andpatients of different ethnicity have also been shown toderive significant benefit from long- acting risperidone.None of these trials, as with studies of conventionallong-acting antipsychotics (Adams et al 2001), specifi-cally recruited non-compliant patients due to the dif-ficulties in maintaining such patients in a study thus,the positive outcomes reported are potentially subject tosome bias. Nonetheless, the favorable efficacy andtolerability profile of long-acting risperidone is alsoassociated with improvements in quality of life andpatient satisfaction, thereby helping to reduce the bur-
den on family members and caregivers and promotesocial integration (Nasrallah et al 2004; Fleischhackeret al 2005). Recently, The Remission in SchizophreniaWorking Group defined remission as “a state in whichpatients have experienced an improvement in core signsand symptoms to the extent that any remaining sympto-matology is of such low intensity that it no longer inter-feres significantly with behavior, and is below thethreshold typically utilized in justifying an initial diag-nosis of schizophrenia” (Andreasen et al 2005).Although these newly proposed remission criteriarequire further refinement, results from two retro-spective analyses have demonstrated long-actingrisperidone may help patients achieve and maintainremission (Kissling et al 2005; Lasser et al 2005b).Prospective studies utilizing the consensus remissioncriteria as a primary outcome are now eagerly awaited.
Non- and partial compliance with antipsychotictherapy remains widespread (Weiden and Zygmunt1997). The combination of symptomatic improve-ment and better tolerability with long-acting risperi-done is expected to improve compliance with ther-apy. This is of particular relevance to young patientsor patients with a first episode of schizophrenia, whoare particularly sensitive to adverse events and are lack-ing in disease insight, leading to poor compliance andtreatment discontinuation. Indeed, a study of first-episode patients with schizophrenia demonstrated thatpartial compliance increased by nearly five-fold the riskof both first and second relapse (Robinson et al1999). Evidence that long-acting risperidone improvescompliance comes from the finding that across the piv-otal studies only 1.3%–5% of patients discontinuedtreatment with long- acting risperidone because ofpoor compliance. Overall, the high retention rates inthese studies (51%–92%) probably reflects a number offactors: the low incidence of adverse events (only1.2%–16% of patients discontinued as a results ofadverse events), the improvement in symptoms,HRQoL, and patient functioning experienced bypatients with long- acting risperidone treatment, and thefact that long-acting risperidone was well accepted bypatients, supported by the low rating of subjectivepain and absence of objective changes at the injec-tion site (Lindenmayer et al 2005). This is in contrast tothe overall 74% all-cause discontinuation rate recentlyreported from the Clinical Antipsychotic Trial ofIntervention Effectiveness (CATIE) (Lieberman et al2005). Although some clinicians believe that long-act-ing agents are old fashioned, stigmatizing, and lessacceptable to patients (Patel et al 2003), results from asystematic review of patient preference reported that in5 out of the 6 studies analyzed, the majority of patientspreferred to receive their medication via a long-actingformulation than in tablet form (Walburn et al 2001).
Interestingly, in a number of studies with long-act-ing risperidone it has been noted that there has been areduction in concomitant medications including side

Revista Românã de Psihiatrie, seria a III-a, vol. IX, nr. 2-3, 2007
131
effect medications (anticholinergics, anxiolytics,hypnotics, sedatives), antipsychotics used in combina-tion, and other classes of psychotropics such as antide-pressants and mood stabilizers (Fleischhacker et al2003; Taylor et al 2004; Chue et al 2005d; E-STAR2005; Snaterse 2005). This may be regarded as a proxymeasure of both efficacy and tolerability in real-worldpatients and warrants further study.
Medications that can reduce relapse rates andimprove compliance leading to lower levels of health-care resource use, particularly hospitalization, are animportant part of the management of schizophre-nia. A number of pharmacoeconomic models andearly clinical data have consistently demonstratedthat long-acting risperidone reduces the number ofrelapses, compared with oral atypical or conventionallong-acting agents (Eriksson et al 2003; Chue et al2005c; De Graeve et al 2005; Edwards et al 2005; Lauxet al 2005). Applying country-specific economic data,this improvement in the number of relapses has consis-tently translated into various levels of cost savingsdespite very different healthcare systems (Chue et al2005c; De Graeve et al 2005; Edwards et al 2005; Lauxet al 2005). These findings suggest that long-actingrisperidone is potentially a cost-effective first-linestrategy for managing schizophrenia and reducing theburden related to the disease (Annemans 2005).However, it is recognized that for long-acting risperi-done the results drawn from pharma co eco nomic modeldata are limited and must be supported by real-world observational findings before definitive con-clusions can be made, particularly when the cost-effec-tiveness of conventional long-acting antipsychotics forschizophrenia has not been consistently demonstrated(Knapp et al 2002; Kilian and Angemeyer, 2004).Furthermore, an analysis of 22 pharmacoeconomicevaluations of different drug therapies showed thatnon- compliance always resulted in a reduction in effi-cacy, but the impact on costs varied substantially(Hughes et al 2001).
It is acknowledged that this review has sever-al limitations. Firstly, this review includes initial datapublished at international congresses that are not yetsubject to peer review, but nonetheless provide clini-cians with early and important information. In addi-tion, since this review analyzed a large number ofclinical trials, encompassing a wide range of studydesigns from randomized, control to open-label, switchstudies, variable patients numbers, and duration of fol-low-up, it is difficult to make direct comparisonsacross studies. The results of the efficacy of long-actingrisperidone in special populations (young patients,elderly patients, patients with schizoaffective disor-der, and patients of different ethnicity) were basedsolely on sub-analyses. As such, further controlledstudies of long-acting risperidone in these difficult-to-treat populations are warranted. Likewise, thehypothesis that switching patients from oral or long-
acting conventional or oral atypical antipsychoticsmay result in significant improvements also requiresfurther investigation because the majority of theseresults were also based on sub-analyses.
Finally, no head-to-head studies with otheratypical antipsychotic agents have been published todate. However, it remains important to consider alllevels of clinical evidence when evaluating the over-all effectiveness of medication since randomized clin-ical trials in select study populations for registrationpurposes may not always reflect current and relevantclinical practice objectives.
The unique pharmacokinetics of long-actingrisperidone does have implications when initiating andtitrating therapy, particularly when compared to con-ventional long-acting antipsychotics. However, clini-cal recommendations concerning dosing are beyondthe scope of this review, but are discussed in a num-ber of clinical articles and in the Product Monograph(Marder et al 2003; Keith et al 2004; Viner et al 2006).
CONCLUSION
This review indicates that long-acting risperidoneis suitable for a wide range of patients, including thosewho are deemed clinically stable, to further improvesymptom control and enhance tolerability. The combi-nation of improved efficacy and good tolerability mayhave important implications for patient compliance totherapy and subsequent positive long-term outcomesincluding the achievement of remission.
ACKNOWLEDGMENTS
The author would like to thank Frances Gambling,Medicus International, for her editorial assistance.Editorial support was funded by an unrestricted edu-cational grant from Janssen.
ReferencesAdams CE Fenton MK, Quraishi S, David AS. 2001.
Systematic meta- review of depot antipsychotic drugs forpeople with schizophrenia. Br J Psychiatry, 179: 290–9.
American Diabetes Association. 2004. Consensusdevelopment conference on antipsychotic drugs and obesityand diabetes. J Clin Psychiatry, 65:267–72.
Almond S, Knapp M, Francois C. 2004. Relapse inschizophrenia: Costs, clinical outcomes and quality of life. BrJ Psychiatry, 184:346–51.
Andreasen N, Carpenter W, Kane J, et al. 2005.Remission in schizophrenia: Proposed criteria and rationalefor consensus. Am J Psychiatry, 162:441–9.
Annemans L. 2005. Cost effectiveness of long-actingrisperidone: what can pharmacoeconomic models teach us?Pharmacoeconomics, 23(Suppl 1):1–2.
Bagnall AM, Jones L, Ginnelly L, et al. 2003. A sys-tematic review of atypical antipsychotic drugs in schizophre-nia. Health Technol Assess, 7:1–193.
Barkic J, Filakovic P, Radanovic-Grguric L, et al. 2003.The influence of risperidone on cognitive functions in schiz-ophrenia. Coll Antropol, 27(Suppl 1):111–8.

Pierre Chue: Long-acting risperidone injection
132
Beasley C, Tollefson G, Tran P, et al. 1996. Olanzapineversus placebo and haloperidol. Acute phase results of theNorth American double- blind olanzapine trial.Neuropsychopharmacology, 14:111–23.
Bilder RM, Goldman RS, Volavka J, et al. 2002.Neurocognitive effects of clozapine, olanzapine, risperidone,and haloperidol in patients with chronic schizophrenia orschizoaffective disorder. Am J Psychiatry, 159:1018–28.
Bloch Y, Mendlovic S, Strupinsky S, et al. 2001.Injections of depot antipsychotic medications in patients suf-fering from schizophrenia: do they hurt? J Clin Psychiatry,62:855–9.
Boyer P, Lecrubier Y, Puech A, et al. 1995. Treatmentof negative symptoms in schizophrenia with amisulpride. BrJ Psychiatry, 166:68–72.
Buckley P. 2004. Efficacy of quetiapine for the treat-ment of schizophrenia: a combined analysis of three placebo-controlled trials. Curr Med Res Opin, 20:1357–63.
Chue P, Eerdekens M, Augustyns I, et al. 2005a.Comparative efficacy and safety of long-acting risperidoneand risperidone oral tablets. Eur Neuropsychopharmacol,15:111–7.
Chue PS, Heeg B, Buskens E, et al. 2005c.Modelling the impact of compliance on the costs andeffects of long-acting risperidone in Canada.Pharmacoeconomics, 23 Suppl 1:62–74.
Chue P, Lam A, Chandra K et al. 2005d. Hospitalizationand medication use in schizophrenia patients receivingrisperidone long-acting injectable or oral atypical antipsty-chotic medication. PA202. Presented at ISPOR 8th AnnualCongress, Florence, Italy.
Chue P, Llorca P, Duchesne I, et al. 2005b.Hospitalization rates in patients during long-term treatmentwith long-acting risperidone injection. J Appl Res, 5:266–74.
Ciliberto N, Bossie CA, Urioste R, et al. 2005. Lack ofimpact of race on the efficacy and safety of long-actingrisperidone versus placebo in patients with schizophrenia orschizoaffective disorder. Int Clin Psychopharmacol,20:207–12.
Citrome LL. 2004. The increase in risk of diabetes mel-litus from exposure to second-generation antipsychoticagents. Drugs Today (Barc), 40:445–64.
Colonna L, Saleem P, Dondey-Nouvel L, et al. 2000.Long-term safety and efficacy of amisulpride in subchronic orchronic schizophrenia. Amisulpride Study Group. Int ClinPsychopharmacol, 15:13–22.
Davidson M, Harvey PD, Vervarcke J, et al. 2000. Along-term, multicenter, open-label study of risperidone inelderly patients with psychosis. On behalf of theRisperidone Working Group. Int J Geriatr Psychiatry,15:506–14.
Davies L, Drummond M. 1994. Economics and schizo-phrenia: the real cost. Br J Psychiatry, 165:18–21.
Davis J, Metalon L, Watanabe M, et al. 1994. Depotantipsychotic drugs. Place in therapy. Drugs, 47:741–73.
De Graeve D, Smet A, Mehnert A, et al. 2005. Long-acting risperidone compared with oral olanzapine andhaloperidol depot in schizophrenia: a Belgian cost-effective-ness analysis. Pharmacoeconomics, 23(Suppl 1):35–47.
Dolder CR, Lacro JP, Dunn LB, et al. 2002.Antipsychotic medication adherence: is there a differencebetween typical and atypical agents? Am J Psychiatry,159:103–8.
Edwards NC, Locklear JC, Rupnow MF, et al. 2005.
Cost effectiveness of long-acting risperidone injection ver-sus alternative antipsychotic agents in patients withschizophrenia in the USA. Pharmacoeconomics,23(Suppl 1):75–89.
Eerdekens M, Karcher K, Remmerie B, et al. 2004.Pharmacokinetics and tolerability of long-acting injectablerisperidone in schizophrenia. Schizophr Res, 70:91–100.
Electronic Schizophrenia Treatment AdherenceRegistry (E-STAR). Janssen-Ortho Inc. Data on file. 2005.
Emsley RA. 1999. Risperidone in the treatment of first-episode psychotic patients: a double-blind multicenterstudy. Risperidone Working Group. Schizophr Bull,25:721–9.
Emsley R, Oosthuizen P, Koem L, et al. 2005. A trial ofrisperidone long- acting injectable in first episode psychosis.Presented at the Annual Meeting of the American PsychiatricAssociation. May 21–26 2005; Atlanta, GA, USA.
Emsley R, Oosthuizen P, Koem L et al. 2006. Safety andefficacy of long- acting risperidone as a first-line treatmentfor first-episode psychosis: 6-month interim analysis[abstract]. Abstracts of the XIIIth Biennial Winter Workshopof Schizophrenia Research. February 4–10 2006; Davos,Switzerland.
Emsley RA, Roberts MC, Rataemane S, et al. 2002.Ethnicity and treatment response in schizophrenia: a compar-ison of 3 ethnic groups. J Clin Psychiatry, 63:9–14.
Ereshefsky L, Lacombe S. 1993. Pharmacological pro-file of risperidone. Can J Psychiatry, 38(Suppl 3):S80–8.
Ereshefsky L, Mannaert E. 2005. Pharmacokineticprofile and clinical efficacy of long-acting risperidone:potential benefits of combining an atypical antipsychoticand a new delivery system. Drugs R D, Ereshefsky L,Mascarenas CA. 2003. Comparison of the effects of differentroutes of antipsychotic administration on pharmacokinet-ics and pharmacodynamics. J Clin Psychiatry, 64(Suppl16):18–23.
Ereshefsky L, Saklad SR, Jann MW, et al. 1984. Futureof depot neuroleptic therapy: pharmacokinetic and pharmaco-dynamic approaches. J Clin Psychiatry, 45:50–9.
Eriksson L, Almqvist A, Mehnert A, et al. 2003. Long-acting risperidone significantly reduces the need for insti-tutional psychiatric care. Presented at American College ofNeuropsychopharmacologists, 42nd Annual meeting.December 7 2003; San Juan, Puerto Rico.
Farde L, Eerdekens M, Eriksson B, et al. 2002.Relationship between plasma concentrations, D2-receptor occu-pancy and efficacy of Risperdal Consta. Presented atAmerican College of Neuropsychopharmacologists,41st Annual Meeting. December 8–12 2002; San Juan, Puerto Rico.
Fleischhacker WW, Eerdekens M, Karcher K, et al.2003. Treatment of schizophrenia with long-actinginjectable risperidone: a 12-month open-label trial of thefirst long-acting second-generation antipsychotic. J ClinPsychiatry, 64:1250–7.
Fleischhacker WW , Lasser R, Mehnert A. 2005.Perceived functioning and well-being and association withpsychiatric symptomatology in clinically stable schizophre-nia patients treated with long-acting risperidone for 1 year.Br J Psychiatry, 187:131–6.
Foster RH, Goa KL. 1998. Risperidone. A pharma-coeconomic review of its use in schizophrenia.Pharmacoeconomics, 14:97–133.
Frackiewicz EJ, Sramek JJ, Herrera JM, et al. 1997.Ethnicity and antipsychotic response. Ann Pharmacother,31:1360–9.
Revista Românã de Psihiatrie, seria a III-a, vol. IX, nr. 2-3, 2007
133
Franz M, Lis S, Pluddemann K, et al. 1997.Conventional versus atypical neuroleptics: subjective qualityof life in schizophrenic patients. Br J Psychiatry, 170:422–5.
Ganguli R. 1999. Weight gain associated with antipsy-chotic drugs. J Clin Psychiatry, 60(Suppl 21):20–4.
Gastpar M, Masiak M, Latif MA, Frazzingaro S, MedoriR, Lombertie ER. 2005. Sustained improvement of clinicaloutcome with risperidone long-acting injectable in psychoticpatients previously treated with olanzapine. JPsychopharmacol, 19:32–8.
Geddes J, Freemantle N, Harrison P, et al. 2000.Atypical antipsychotics in the treatment of schizophrenia:systematic overview and meta- regression analysis. BMJ,321:1371–6.
Gefvert O, Eriksson B, Persson P, et al. 2005.Pharmacokinetics and D2 receptor occupancy of long-actinginjectable risperidone (Risperdal Consta TM ) in patients withschizophrenia. Int J Europsychopharmacol, 8:27–36.
Gerlach J. 1994. Oral versus depot administration ofneuroleptics in relapse prevention. Acta Psychiatr ScandSuppl, 382:28–32.
Gharabawi GM, Bossie CA, Zhu Y, et al. 2005. Anassessment of emergent tardive dyskinesia and existing dysk-inesia in patients receiving long-acting, injectable risperi-done: Results from a long-term study. Schizophr Res,77:129–39.
Glazer WM, Ereshefsky L. 1996. A pharmacoeconomicmodel of outpatient antipsychotic therapy in “revolving door”schizophrenic patients. J Clin Psychiatry, 57:337–45.
Goeree R, Farahati F, Burke N, et al. 2005. Theeconomic burden of schizophrenia in Canada in 2004. CurrMed Res Opinion, 21:2017–28.
Hamilton SH, Edgell ET, Revicki DA, et al. 2000.Functional outcomes in schizophrenia: a comparison of olan-zapine and haloperidol in a European sample. Int ClinPsychopharmacol, 15:245–55.
Hufnagel E, Locklear J, Caruso R, et al. 2004.Treatment goal expectations of physicains and patients withschizophrenia. Presented at the 56th Institute on PsychiatricServices Scientific Meeting. October 6–10 2004; Atlanta, GAUSA.
Jayaram G, Coyle J, Tune L. 1986. Relapse inchronic schizophrenics treated with fluphenazine decanoateis associated with low serum neuroleptic levels. J ClinPsych, 47:247–8.
Kane J. 2001. Progress defined–short-term efficacy,long-term effectiveness. Int Clin Psychopharmacol,16(Suppl 1):S1–8.
Kane JM, Aguglia E, Altamura AC, et al. 1998.Guidelines for depot antipsychotic treatment inschizophrenia. European NeuropsychopharmacologyConsensus Conference in Siena, Italy. EurNeuropsychopharmacol, 8:55–66.
Kane JM, Eerdekens M, Lindenmayer JP, et al.2003. Long-acting injectable risperidone: efficacy and saf-ety of the first long-acting atypical antipsychotics. Am JPsychiatry, 160:1125–32.
Kapur S, Zipursky R, Jones C, et al. 2000. Relationshipbetween dopamine D(2) occupancy, clinical response, andside effects: a double-blind PET study of first-episode schiz-ophrenia. Am J Psychiatry, 157:514–20.
Kapur S, Zipursky RB, Remington G. 1999. Clinicaland theoretical implications of 5-HT2 and D2 receptoroccupancy of clozapine, risperidone, and olanzapine in
schizophrenia. Am J Psychiatry, 156:286–93.Kasper S. 1999. First-episode schizophrenia: the
importance of early intervention and subjective tolerability.J Clin Psychiatry, 60(Suppl 23):5–9.
Keefe RS, Silva SG, Perkins DO, et al. 1999. Theeffects of atypical antipsychotic drugs on neurocognitiveimpairment in schizophrenia: a review and meta-analysis.Schizophr Bull, 25:201–22.
Keith SJ, Pani L, Nick B, et al. 2004. Practicalapplication of pharmacotherapy with long-acting risperi-done for patients with schizophrenia. Psychiatr Serv,55:997–1005.
Kilian R, Angemeyer MC. 2004. [The impact ofantipsychotic medication on the incidence and the costs ofinpatient treatment in people with schizophrenia: resultsfrom a prospective observational study] Psychiatr Prax,31:138–46.
Kissling W, Heres S, Lloyd K, et al. 2005. Direct tran-sition to long-acting risperidone—analysis of long-termefficacy. J Psychopharmacol, 19:15–21.
Knapp M. 2000. Schizophrenia costs and treatmentcost-effectiveness. Acta Psychiatr Scand Suppl:15–8.
Knapp M, Ilson S, David A. 2002. Depot antipsychoticpreparations in schizophrenia: the state of the economicevidence. Int ClinPsychopharmacol, 17:135–40.
Kushner S, Khan A, Eerdekens M et al. 2004. Treatmentwith long-acting risperidone in patients with schizophreniafor up to four years. Presented at Institute on PsychiatricServices. October 6–10, 2004; Atlanta, GA, USA.
Lambert M, Naber D. 2004. Current issues in schizo-phrenia: overview of patient acceptability, functioning capac-ity and quality of life. CNS Drugs, 18(Suppl 2):5–17; discus-sion 41–3.
Lasser R, Bossie C, Gharabawi G, et al. 2004a. Patientswith schizophrenia previously stabilized on conventionaldepot antipsychotics experience significant clinical improve-ments following treatment with long-acting risperidone. EurPsychiatry, 19:219–25.
Lasser R, Bossie CA, Gharabawi G, et al. 2004b.Efficacy and safety of long-acting risperidone in stablepatients with schizoaffective disorder. J Affect Disord,83:263–75.
Lasser R, Bossie C, Gharabawi G, et al. 2005a. Clinicalimprovement in 336 stable chronically psychotic patientschanged from oral to long-acting risperidone: A 12-monthopen trial. Int J Neuropsychopharmacol, 8:1–12.
Lasser R, Bossie CA, Gharabawi GM, et al. 2005b.Remission in schizophrenia: Results from a 1-year study oflong-acting risperidone injection. Schizophr Res, 77:215–27.
Lasser R, Bossie CA, Zhu Y, et al. 2004c. Efficacy andsafety of long-acting risperidone in elderly patients withschizophrenia and schizoaffective disorder. Int J GeriatrPsychiatry, 19:898–905.
Lasser R, Bossie CA, Zhu Y, et al. 2004d. Long-acting risperidone in young adults with schizophrenia orschizoaffective disorder. Presented at American PsychiatricAssociation, 1–6 May 2004; New York, USA.
Laux G, Heeg B, van Hout B, et al. 2005. Costs andeffects of long-acting risperidone compared with oral atyp-ical and conventional depot formulations in Germany.Pharmacoeconomics, 23:49–61.
Lauriello J, McEvoy JP, Rodriquez S et al. 2005. Long-acting risperidone vs. placebo in the treatment of hospitalinpatients with schizophrenia. Schizophr Res, 72:249–58.
Pierre Chue: Long-acting risperidone injection
134
Leal A, Rosillon D, Mehnert A, et al. 2004. Healthcareresource utilization during 1-year treatment with long-act-ing, injectable risperidone. Pharmacoepidemiol Drug Saf,13:811–6.
Lee MS, Ko YH, Lee SH, et al. 2006. Long-term treat-ment with long- acting risperidone in Korean patients withschizophrenia. Hum Psychopharmacol, 21:399–407.
Leucht S, Pitschel-Walz G, Abraham D, et al. 1999.Efficacy and extrapyramidal side-effects of the newantipsychotics olanzapine, quetiapine, risperidone, andsertindole compared to conventional antipsychotics andplacebo. A meta-analysis of randomized controlled trials.Schizophr Res, 35:51–68.
Levinson DF, Umapathy C, Musthaq M. 1999.Treatment of schizoaffective disorder and schizophrenia withmood symptoms. Am J Psychiatry, 156:1138–48.
Lieberman JA, Stroup TS, McEvoy JP, et al. 2005.Effectiveness of antipsychotic drugs in patients with chronicschizophrenia. N Engl J Med, 353:1209–23.
Lindenmayer JP, Eerdekens E, Berry SA, et al. 2004.Safety and efficacy of long-acting risperidone in schizophre-nia: a 12-week, multicenter, open-label study in stablepatients switched from typical and atypical oral antipsy-chotics. J Clin Psychiatry, 65:1084–9.
Lindenmayer JP, Grochowski S, Mabugat L. 1994.Clozapine effects on positive and negative symptoms: asix-month trial in treatment- refractory schizophrenics. JClin Psychopharmacol, 14:201–4.
Lindenmayer JP, Jarboe K, Bossie CA, et al. 2005.Minimal injection site pain and high patient satisfactionduring treatment with long-acting risperidone. Int ClinPsychopharmacol, 20:213–21.
Lindenmayer JP, Khan A, Eerdekens M, Van Hove I,Kushner S. 2006.in patients with schizophrenia or schizo-affective disorder. Eur Neuropsychopharmacol, 16; [Epubahead of print]
Malla A, Binder C, Chue P. 2006. Comparison of long-acting injectable risperidone and oral novel antipsychoticdrugs for treatment in early phase of schizophrenia spectrumpsychosis. Presented at 61st Annual Convention Society ofBiological Psychiatry. May 18–20, 2006; Toronto. Canada.
Marder SR, Conley R, Ereshefsky L, Kane JM, TurnerMS. 2003. Clinical guidelines: Dosing and switchingstrategies for long-acting risperidone. J Clin Psychiatry,64(Suppl 16):41–6.
Marder SR, Davis JM, Chouinard G. 1997. The effectsof risperidone on the five dimensions of schizophreniaderived by factor analysis: combined results of the NorthAmerican trials. J Clin Psychiatry, 58:538–46.
Marder S, Meibach R. 1994. Risperidone in the treat-ment of schizophrenia. Am J Psychiatry, 151:825–35.
Masand PS. 2000. Side effects of antipsychotics inthe elderly. J Clin Psychiatry, 61(Suppl 8):43–9; discussion50–1.
Meltzer H, Beurnett S, Bastani B. 1990. Effects of sixmonths clozapine treatment of quality of life of chronic schiz-ophrenic patients. Hosp Community Psychiatry, 41:892–7.
Meyer-Lindenberg A, Gruppe H, Bauer U, et al. 1997.Improvement of cognitive function in schizophrenic patientsreceiving clozapine or zotepine: results from a double-blindstudy. Pharmacopsychiatry, 30:35–42.
Mohl A, Westlye K, Opjordsmoen S, et al. 2005. Long-acting risperidone in stable patients with schizoaffectivedisorder. J Psychopharmacol, 19:22–31.
Möller H, Llorca PM, Sachetti E, et al. 2005. Efficacyand safety of direct transition to risperidone long-actinginjectable in patients treated with various antipsychotic ther-apies. Int Clin Psychopharmacol , 20:121–30.
Morosini PL. 2000. Development, reliability andacceptability of a new version of the DSM-IV Social andOccupational Functioning Assessment Scale (SOFAS) toassess routine social functioning. Acta Psychiatr Scand,101:323–9.
Nasrallah H, Duchesne I, Mehnert A, et al. 2004.Health-related quality of life with schizophrenia duringtreatment with long-acting risperidone injection. J ClinPsychiatry, 65:531–6.
Nordstrom AL, Farde L, Wiesel FA, et al. 1993. CentralD2-dopamine receptor occupancy in relation to antipsychoticdrug effects: a double- blind PET study of schizophrenicpatients. Biol Psychiatry, 33:227–35.
Parellada E, Andrezina R, Milanova V, et al. 2005.Patients in the early phases of schizophrenia and schizoaf-fective disorders effectively treated with risperidone long-acting injectable. J Psychopharmacol, 19:5–14.
Patel MX, Nikolaou V, David AS. 2003.Psychiatrists’ attitudes to maintenance medication forpatients with schizophrenia. Psychol Med, 33:83–9.
Patel MX, Young C, David A, et al. 2006.Risperidone long-acting injection: predictors of relapse atone year. Abstracts of the XIIIth Biennial Winter Workshopon Schizophrenia Research. February 4–10, 2006; Davos,Switzerland.
Peuskens J, Moller HJ, Puech A. 2002. Amisulprideimproves depressive symptoms in acute exacerbations ofschizophrenia: comparison with haloperidol and risperido-ne. Eur Neuropsychopharmacol, 12:305–10.
Peuskens J, Van Baelen B, De Smedt C, et al. 2000.Effects of risperidone on affective symptoms in patientswith schizophrenia. Int Clin Psychopharmacol, 15:343–9.
Poolsup N, Li Wan Po A, Knight TL. 2000.Pharmacogenetics and psychopharmacotherapy. J ClinPharm Ther, 25:197–220.
Quraishi S, David A. 2000. Depot haloperidol for schiz-ophrenia. Cochrane Database Syst Rev, 2:CD001361.
Ramstack J, Grandolfi G, D’Hoore P, et al. 2003. Long-acting risperidone: Prolonged-release injectable delivery ofrisperidone using Medisorb® microsphere technology.Schizophr Research, 60:314.
Remington G, Chue P, Kopala L, Stip E. 2004.Switching atypical antipsychotics: a review. ActaNeuropsychiatrica, 16:301–13.
Remington G, Mamo D, Labelle A, et al. 2006. A PETstudy evaluating dopamine D2 receptor occupancy forlong-acting injectable risperidone. Am J Psychiatry,163:396–401.
Revicki DA, Genduso LA, Hamilton SH, et al. 1999.Olanzapine versus haloperidol in the treatment of schizo-phrenia and other psychotic disorders: quality of life andclinical outcomes of a randomized clinical trial. Qual LifeRes, 8:417–26.
Robinson D, Woerner MG, Alvir JM, et al. 1999.Predictors of relapse following response from a firstepisode of schizophrenia or schizoaffective disorder. ArchGen Psychiatry, 56:241–7.
Rodriguez S, Locklear J, Turkoz I, et al. 2005.Maintenance therapy with long-acting risperidone: function-ing and quality of life in patients with schizophrenia and

Revista Românã de Psihiatrie, seria a III-a, vol. IX, nr. 2-3, 2007
135
schizoaffective disorder. Presented at American PsychiatricAssociation. 22–26 May, 2005; Atlanta, GA, USA.
Rubio G, Martinez I, Ponce G, et al. 2006. Long-acting injectable risperidone versus zuclopenthixol in thetreatment of schizophrenia with substance abuse comorbidity.Can J Psychiatry, 51:35-43.
Saleem P, Firmino H, Parellada E, et al. 2004. Youngpatients (18-30 years) with schizophrenia and schizoaffec-tive disorder: results of direct switching to long-actinginjectable risperidone (StoRMi trial). Presented at the 12thBiennial Winter Workshop on Schizophrenia. 7–13 February2004, Davos, Switzerland.
Snaterse M, Welch R, Chue P. effectiveness and tolera-bility outcomes of a risperidone long-acting injection com-pared to conventional depot antipsychotics in a Canadianteaching hospital. Presented at 44th American College ofNeuropsychopharmacology Annual Meeting. 11–15December 2005; Hawaii, USA.
Taylor DM, Young CL, Mace S, Patel MX. 2004. Earlyclinical experience with risperidone long-acting injection: aprospective, 6-month follow- up of 100 patients. J ClinPsychiatry, 65:1076-83.
Teijeiro R, Turner M, Bouhours P et al. Obese patientswith schizophrenia and schizoaffective disorder: efficacy ofrisperidone long-acting injectable. Presented at the 12thBiennial Winter Workshop on Schizophrenia. 7–13February 2004; Davos, Switzerland, 2004.
Tollefson GD, Sanger TM, Lu Y, et al. 1998.Depressive signs and symptoms in schizophrenia: a pro-
spective blinded trial of olanzapine and haloperidol. Arch GenPsychiatry, 55:250–8.
Turner M, Eerdekens E, Jacko M, et al. 2004.Long-acting injectable risperidone: safety and efficacy instable patients switched from conventional depot antipsy-chotics. Int Clin Psychopharmacol, 19:241–9.
Valenstein M, Copeland LA, Owen R, et al. 2001.Adherence assessments and the use of depot antipsychotics inpatients with schizophrenia. J Clin Psychiatry, 62:545–51.
van Os J, Bossie C, Lasser R. 2004. Improvements instable patients with psychotic disorders switched from oralconventional antipsychotics therapy to long-acting risperi-done. Int Clin Psychopharmacol, 19:229–32.
Vauth R, Justers J, Braendle D, et al. Direct switchfrom atypical antipsychotic to long-acting injectable risperi-done in schizophrenia and schizoaffective disorders[abstract]. 2004. Abstracts of the Biennial WinterWorkshop of Schizophrenia Research. 7–13 February; Davos,Switzerland.
Viner MW, Matuszak JM, Knight LJ. 2006. Initial dos-ing strategies for long-acting injectable risperidone. J ClinPsychiatry, 67:1310–1. Walburn J, Gray R, Gournay K, et al.2001. Systematic review of patient and nurse attitudes todepot antipsychotic medication. Br J Psychiatry, 179:300–7.
Weiden P, Zygmunt A. 1997. Medication noncompli-ance in schizophrenia. Part I. Assessment. J PracticalPsychiatry and Behavioural Health, 3:106–10.
***