liver transplantation in patients with non-biliary cirrhosis: prognostic value of preoperative...
TRANSCRIPT

Journal of Hepatology 1998; 28: 320–328 Copyright C European Associationfor the Study of the Liver 1998Printed in Denmark ¡ All rights reserved
Munksgaard ¡ Copenhagen Journal of HepatologyISSN 0168-8278
Liver transplantation in patients with non-biliary cirrhosis: prognosticvalue of preoperative factors
Eleazar Gonzalez, Antoni Rimola, Miquel Navasa, Hernan Andreu, Luis Grande,Juan-Carlos Garcıa-Valdecasas, Isabel Cirera, Josep Visa and Juan Rodes
Liver Unit and Department of Surgery, Hospital Clınic i Provincial, University of Barcelona, Barcelona, Spain
Background/Aim: The type of disease indicating livertransplantation is one of the most powerful predictorsof postoperative survival. This may be an importantproblem in evaluating the prognostic significance ofother factors when patients with liver diseases of verydifferent nature are jointly studied. To minimize thisbias, the present study aimed to investigate preopera-tive prognostic factors in liver transplantation only inpatients with non-biliary cirrhosis.Methods: Twenty-three preoperative standard clinicaland laboratory variables were analyzed as possibleprognostic factors in 162 patients receiving liver trans-plantation for non-biliary cirrhosis. Data for sevensplanchnic and systemic hemodynamic variables werealso analyzed in 55 patients.Results: Using univariate analyses followed by amultivariate analysis, only preoperative blood urea ni-trogen (BUN) reached statistical significance as an
A , liver transplantation is considered to bethe therapy of choice for most patients with ad-
vanced liver disease. However, the disproportion be-tween the large number of potential candidates for thistherapeutic modality and the relatively small numberof organ donors makes selection of liver transplantcandidates mandatory. Allocating scarce donor liversto adequate transplant recipients to obtain a reason-ably acceptable survival after transplantation is one ofthe objectives of this selection (1–4), and, thus, theprognostic significance of preoperative factors may beof value in identifying appropriate liver transplant can-didates.
Received 2 June; revised 3 September; accepted 15 September 1997
Correspondence: Antoni Rimola, Liver Unit, HospitalClınic i Provincial, Villarroel 170, 08036 Barcelona, Spain.Tel: 34-3-227-5499. Fax: 34-3-451-5522.e-mail: rimola/medicina.ub.es
320
independent predictor of hospital survival; the survivalrate at the end of hospitalization being 90% in pa-tients with BUNÆ25 mg/dl and 65% in patients withBUN±25 mg/dl (pΩ0.0008). Similarly, preoperativeBUN was the only variable independently predictingcumulative long-term survival, with an 87% survivalprobability at 1 year and 73% at 4 years in patientswith BUNÆ25 mg/dl, and 61% and 49%, respectively,in patients with BUN±25 mg/dl (pΩ0.0014).Conclusions: Renal function parameters are the mostpowerful preoperative predictors of survival after livertransplantation in patients with non-biliary cirrhosis.It is suggested that liver transplantation is indicatedin these patients before marked renal dysfunction de-velops.
Key words: Cirrhosis; Impaired renal function; Livertransplantation; Prognosis.
During the last few years numerous studies have in-vestigated preoperative prognostic factors in livertransplant patients. However, almost all these investi-gations have included patients with liver diseases ofvery different natures. In most of these studies, par-ticularly in those involving large series of patients, thetype of liver disease indicating transplantation hasbeen found to influence postoperative survival (5–9).For instance, patients receiving transplantation for dis-eases of biliary origin, such as primary biliary cir-rhosis, do better than patients with other diseases,while patients transplanted for acute liver failure doworse. Therefore, some concerns may be raised aboutthe prognostic significance of preoperative factorswhen patients with liver diseases of very different na-ture are jointly investigated. In the present study, alarge number of preoperative data have been analyzedas possible factors influencing prognosis after livertransplantation in a population made up of adult pa-

Prognostic factors in liver transplant
tients with cirrhosis of non-biliary etiology, which iscurrently the commonest indication for liver transplan-tation (5,6,10–12).
Materials and MethodsThe study included 162 consecutive adult patients (113males and 49 females; median age: 50 years, range: 20–62 years) with cirrhosis of non-biliary origin whounderwent primary liver transplantation. Indicationsfor liver transplantation were the following: hepatitis Bvirus (HBV)-related cirrhosis in 12 patients (associatedwith hepatitis D virus infection in four), hepatitis Cvirus (HCV)-associated cirrhosis in 75, alcoholic cir-rhosis in 40 (in 19 of these 40 patients serologicalmarkers of HCV infection were not available), autoim-mune hepatitis in three, idiopathic hemochromatosis inone, cirrhosis secondary to alpha-1-antitrypsin de-ficiency in one, Budd-Chiari syndrome in one, cirrhosisdue to different combinations of etiologies in 11 (HBVand HCV infection in four, and HCV infection andalcoholism in seven), and cryptogenic cirrhosis in 18(in 13 cases, serological HCV infection markers couldnot be determined). Twenty-four patients also hadhepatocarcinoma. Fourteen patients belonged toChild-Pugh class A (all these patients had hepatocarci-noma), 74 to class B and 74 to class C. One hundredand forty-four patients were living at home and 18were hospitalized at the time of transplantation (sevenwere in the Intensive Care Unit).
The surgical and anesthesia procedures performedin organ donors and transplant recipients have beendescribed elsewhere (13). All the patients received livergrafts from ABO-identical donors. Conventional post-operative control and treatment were followed (14,15).After discharge from hospital, patients were period-ically followed by members of the liver transplantteam. Initial immunosuppressive therapy consisted ofcorticosteroids, azathioprine and cyclosporine. Aza-thioprine was administered only during the first post-operative month. The dosage of steroids was progress-ively reduced until discontinuation at the 18–24thmonth. Cyclosporine was maintained throughout thestudy period. The doses of these immunosuppressivedrugs were also appropriately modified according tothe possible development of serious adverse effects orrejection. Rejection was diagnosed on the basis of con-sistent histological findings. Episodes of rejection weretreated with short courses of high-dose corticosteroids.Monoclonal antilymphocyte antibodies (OKT3) wereadministered only in patients with steroid resistant re-jection.
In all 162 patients, 23 preoperative clinical and lab-oratory variables were analyzed as prognostic factors
321
after transplantation. These variables included demo-graphic data, etiology of cirrhosis, associated hepato-carcinoma, prior history of abdominal surgery, majorclinical signs of liver disease, nutritional status, stan-dard liver and renal function tests, blood cell count,Child-Pugh classification, and patient location (homeor hospital) at the time of transplantation. All thesevariables were collected on the day of liver transplan-tation.
Fifty-seven of the 162 patients included in the inves-tigation underwent preoperative invasive hemodynamicstudies. The following variables were also investigatedas possible prognostic factors: heart rate, mean arterialpressure (determined by an automatic vital sign moni-tor [Dinamap, Critikon, Tampa, FL, USA]; 57 pa-tients), cardiac index (measured by thermodilutionthrough a Swan-Ganz catheter; 51 patients), systemicvascular resistance (calculated from the mean arterialpressure, right atrial pressure and cardiac output; 51patients), portal pressure (measured as wedge to freehepatic vein pressure gradient; 55 patients), hepaticblood flow (measured by constant indocyanine greeninfusion method; 27 patients), and azygous vein bloodflow (determined by thermodilution method; 38 pa-tients). All these data were obtained within the 6months prior to transplantation. Patients subsequentlyreceiving drugs or surgical techniques (including TIPS)capable of modifying hemodynamic parameters wereexcluded from this part of the analysis.
Statistical analysisThe short-term prognosis was investigated during thein-hospital period. To assess the prognostic significanceof every variable in this period of time, patients whodied during hospitalization after liver transplantationwere compared with patients discharged from the hos-pital. Comparison between these two groups was per-formed by univariate analyses (Mann-Whitney’s testfor quantitative variables and the chi-square test forqualitative variables) followed by a multivariate analy-sis (logistic regression including variables reaching a p-value less than 0.10 in univariate analyses).
To investigate the long-term prognostic value of thedifferent variables, the 162 patients were classified intogroups according to the presence or absence of eachqualitative variable and to the median value of eachquantitative variable. The survival probability of everygroup of patients was subsequently calculated (Kap-lan-Meier method), and the curves obtained were stat-istically compared by the Mantel-Cox method. Vari-ables reaching a p-value ∞0.10 were introduced into amultivariate analysis (Cox’s multiple regression analy-

E. Gonzalez et al.
sis) to identify variables independently correlating withprognosis.
All these statistical analyses were performed usingthe BMDP statistical package (BMDP Statistical Soft-ware, Inc., Los Angeles, CA, USA, 1990) (16). Resultsare expressed as median (and range).
ResultsShort-term survivalDuring the in-hospital period after liver transplan-tation (median: 39 days), 25 (15%) of the 162 patients
TABLE 1
Preoperative clinical and laboratory data in 162 patients undergoing liver transplantation for cirrhosis of non-biliary etiology, classified accordingto whether they died during hospitalization (Group I) or were discharged from the hospital (Group II)
Group I Group II p-value(nΩ25) (nΩ137)
Age (years) 51 (20–58) 50 (21–62) NS**Gender (male/female) 14/11 99/38 NSEtiology of cirrhosis: (no.)
Alcoholic 7 (28%) 33 (24%) NSPosthepatitic B 1 (4%) 11 (8%) NSPosthepatitic C 14 (56%) 61 (45%) NSMore than one etiology 0 (0%) 11 (8%) NSOther 3 (12%) 21 (15%) NS
History of abdominal surgery (no.) 12 (48%) 51 (37%) NSData at the time of transplant:
Ascites (no.) 21 (84%) 100 (73%) NSGI bleeding (no.) 2 (8%) 8 (6%) NSHepatic encephalopathy (no.) 7 (28%) 24 (18%) NSNutritional status: (no.) NS
Good 9 (36%) 74 (54%)Regular 10 (40%) 48 (35%)Bad 6 (24%) 15 (11%)
Hepatocarcinoma (no.) 4 (16%) 20 (15%) NSSerum bilirubin (mg/dl) 4.0 (0.7–31.0) 2.6 (0.2–29.0) NSProthrombin activity (%) 50 (23–85) 53 (10–99) NSSerum albumin (g/l) 32 (23–46) 33 (21–53) NSSerum alanine aminotransferase (U/l) 51 (8–175) 54 (10–516) NSSerum alkaline phosphatase (U/l) 236 (152–699) 282 (115–1970) NSHematocrit value (%) 30 (24–50) 35 (20–49) 0.0945White blood cell count (¿1000/mm3) 4.8 (1.9–9.9) 4.0 (1.0–12.4) NSPlatelet count (¿1000/mm3) 69 (47–238) 68 (21–357) NSBUN (mg/dl) 25 (8–80) 16 (6–60) 0.0043Serum creatinine (mg/dl) 1.0 (0.5–2.2) 0.8 (0.5–2.0) NSSerum sodium (mEq/l) 131 (112–156) 135 (107–150) 0.0641Serum potassium (mEq/l) 3.8 (2.7–5.9) 3.6 (2.4–5.8) NSChild-Pugh score 10 (6–15) 9 (5–14) NSPatient location at the time of transplantation: NSAt home 22 (88%) 122 (89%)Hospitalized 3 (12%) 15 (11%)
Hemodynamic data*:Portal pressure (mmHg) 18 (10–25) 18 (8–31) NSHepatic blood flow (l/min) 0.9 (0.5–2.6) 1.0 (0.4–1.9) NSAzygous blood flow (ml/min) 529 (172–971) 683 (58–1205) NSHeart rate (beats/min) 77 (67–92) 77 (59–114) NSMean arterial pressure (mmHg) 82 (59–101) 78 (47–115) NSCardiac index (l ¡minª1 ¡mª2) 4.3 (2.7–6.4) 4.7 (2.8–7.7) NSSystemic vascular resistance (dyn ¡ s ¡cmª5) 763 (488–1671) 679 (357–1421) NS
* Determined in different subsets of patients within 6 months prior to liver transplantation.**NS: not significant; in order to include variables with p∞0.10 in a multivariate analysis, this p-value was selected as the cutoff for statistical
significance.
322
died. In 18 patients the main causes of death were in-fectious complications, mostly associated with multi-organ failure: six pneumonia, four disseminated fungalinfections (candidiasis in two cases, Aspergillus fumi-gatus infection in one case and mucormycosis in one),three cytomegalovirus infections with severe lung in-volvement, three bacteremia, one abdominal abscessand one brain toxoplasmosis. Causes of death in theother seven patients were miscellaneous: primary graftnonfunction (another liver graft was not available),postoperative hemorrhage (the source of the hemor-
Prognostic factors in liver transplant
TABLE 2
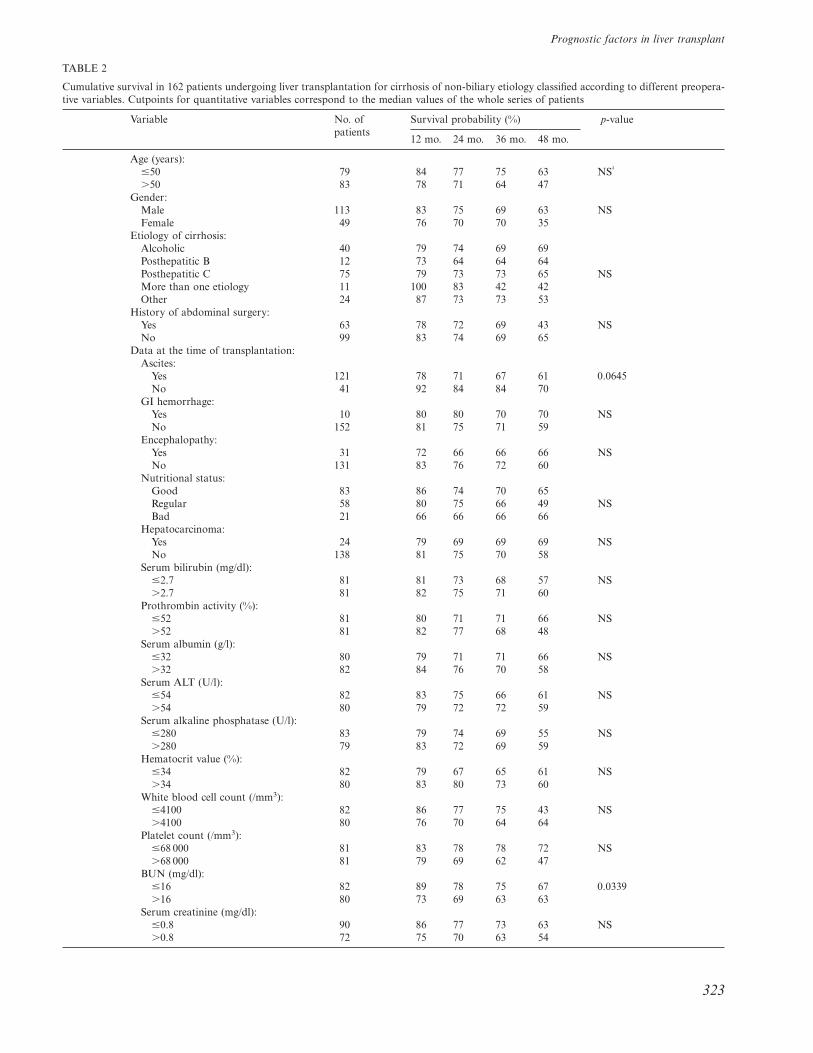
Cumulative survival in 162 patients undergoing liver transplantation for cirrhosis of non-biliary etiology classified according to different preopera-tive variables. Cutpoints for quantitative variables correspond to the median values of the whole series of patients
Variable No. of Survival probability (%) p-valuepatients
12 mo. 24 mo. 36 mo. 48 mo.
Age (years):Æ50 79 84 77 75 63 NS†
±50 83 78 71 64 47Gender:
Male 113 83 75 69 63 NSFemale 49 76 70 70 35
Etiology of cirrhosis:Alcoholic 40 79 74 69 69Posthepatitic B 12 73 64 64 64Posthepatitic C 75 79 73 73 65 NSMore than one etiology 11 100 83 42 42Other 24 87 73 73 53
History of abdominal surgery:Yes 63 78 72 69 43 NSNo 99 83 74 69 65
Data at the time of transplantation:Ascites:
Yes 121 78 71 67 61 0.0645No 41 92 84 84 70
GI hemorrhage:Yes 10 80 80 70 70 NSNo 152 81 75 71 59
Encephalopathy:Yes 31 72 66 66 66 NSNo 131 83 76 72 60
Nutritional status:Good 83 86 74 70 65Regular 58 80 75 66 49 NSBad 21 66 66 66 66
Hepatocarcinoma:Yes 24 79 69 69 69 NSNo 138 81 75 70 58
Serum bilirubin (mg/dl):Æ2.7 81 81 73 68 57 NS±2.7 81 82 75 71 60
Prothrombin activity (%):Æ52 81 80 71 71 66 NS±52 81 82 77 68 48
Serum albumin (g/l):Æ32 80 79 71 71 66 NS±32 82 84 76 70 58
Serum ALT (U/l):Æ54 82 83 75 66 61 NS±54 80 79 72 72 59
Serum alkaline phosphatase (U/l):Æ280 83 79 74 69 55 NS±280 79 83 72 69 59
Hematocrit value (%):Æ34 82 79 67 65 61 NS±34 80 83 80 73 60
White blood cell count (/mm3):Æ4100 82 86 77 75 43 NS±4100 80 76 70 64 64
Platelet count (/mm3):Æ68 000 81 83 78 78 72 NS±68 000 81 79 69 62 47
BUN (mg/dl):Æ16 82 89 78 75 67 0.0339±16 80 73 69 63 63
Serum creatinine (mg/dl):Æ0.8 90 86 77 73 63 NS±0.8 72 75 70 63 54
323

E. Gonzalez et al.
TABLE 2
Continued.
Variable No. of Survival probability (%) p-valuepatients
12 mo. 24 mo. 36 mo. 48 mo.
Serum sodium** (mEq/l):Æ135 86 76 69 66 59 NS±135 75 86 78 73 62
Serum potassium** (mEq/l):Æ3.6 82 88 76 76 65 0.0816±3.6 79 74 72 63 54
Child-Pugh score:Æ9.0 88 82 76 70 60 NS±9.0 74 80 69 69 58
Patient location at the time oftransplantation:
Home 144 82 74 69 58 NSHospital 18 74 66 66 66
Hemodynamic data*:Portal pressure (mmHg):
Æ18 29 79 71 71 71 NS±18 26 81 76 76 76
Hepatic blood flow (l/min):Æ0.990 14 71 63 63 NA NS±0.990 13 76 76 76 76
Azygous blood flow (ml/min):Æ678 19 73 73 73 NA NS±678 19 78 72 72 72
Heart rate (beats/min):Æ77 28 79 75 75 75 NS±77 29 79 75 70 70
Mean arterial pressure (mmHg):Æ79 31 87 80 70 70 NS±79 26 69 69 69 69
Cardiac index (l ¡minª1 ¡mª2):Æ4.62 26 73 68 68 NA NS±4.62 25 80 75 75 75
Systemic vascular resistance (dyn ¡ s ¡cmª5):Æ695 25 84 79 79 79 NS±695 26 69 64 64 NA
*NA: not assessable since no patient reached this follow-up.**Immediate pre-transplant serum sodium and potassium values were not determined in one patient..Determined within 6 months prior to transplantation.†NS: not significant; in order to include variables with p∞0.10 in a multivariate analysis, this p-value was selected as the cutoff for statisticalsignificance.
rhage was an inferior caval vein lesion related to aveno-venous bypass cannulation), brain anoxia second-ary to cardiorespiratory arrest, intestinal infarctionwith no apparent cause, cardiac arrest in the setting ofpostoperative heart failure, massive bronchial hemor-rhage following tracheostomy, and Kaposi’s sarcomaassociated with graft rejection, respectively.
Table 1 shows preoperative clinical and laboratorydata of the 25 patients who died during hospitalizationafter transplantation and the 137 patients dischargedfrom hospital. Three preoperative variables analyzedwere found to be associated with a bad post-transplantprognosis with a p-value less than 0.10: increased bloodurea nitrogen (BUN), and decreased plasma sodiumand hematocrit values. After introducing these three
324
variables into a logistic regression analysis, only BUNreached statistical significance as an independent pre-dictor of hospital survival (pΩ0.0013). The hospitalsurvival rate was 90% in patients with preoperativeBUNÆ25 mg/dl (the upper normal limit in our labora-tory), whereas only a 65% survival was obtained in pa-tients with BUN ±25 mg/dl (pΩ0.0008).
Preoperative BUN was also related to the develop-ment of renal dysfunction during the in-hospital periodafter transplantation. One hundred and twelve patientsdeveloped significant postoperative renal impairment(arbitrarily defined as BUN ±50 mg/dl and/or serumcreatinine ±1.5 mg/dl, with an increase of ±50% inrelation to preoperative values) and 15 of these patientsrequired artificial renal support (hemodialysis and/or

Prognostic factors in liver transplant
hemofiltration). Cyclosporine administration waseither delayed or discontinued in 25 patients becauseof serious renal dysfunction. Preoperative BUN valueswere significantly greater in patients who developedpostoperative renal impairment than in those who didnot (18 [6–80] versus 14 [7–29] mg/dl; pΩ0.0021) andin patients requiring hemodialysis/hemofiltration thanin those who did not require this therapy (25 [8–80]versus 16 [6–60] mg/dl; pΩ0.0482). Postoperative renalimpairment and necessity of artificial renal supportwere associated with a significantly lower short-termsurvival: the hospital survival rate was 79% versus 96%in patients with and without renal impairment (pΩ0.0141), and 47% versus 88% in patients who did anddid not require artificial renal support (pΩ0.0001).
Long-term survivalIn addition to the 25 patients who died during hospi-talization after transplantation, 19 more patients diedafter discharge. The causes of death in these 19 patientswere infectious complications in six patients (two Pneu-mocystis carinii pneumonia, two bacteremia withmultiorganic failure, one disseminated Aspergillus fu-migatus infection, and one pneumonia in which thecausative organism could not be isolated), HBV infec-tion in five patients (four infection recurrences and oneprimary infection following a fulminant course), denovo malignant disease in three patients (one intestinallymphoma, one brain lymphoma and one colon aden-
Fig. 1. Survival probability in 162 patients undergoing livertransplantation for cirrhosis of non-biliary origin classifiedaccording to whether their preoperative BUN was normal(Æ25 mg/dl; Group A, nΩ128) or increased (±25 mg/dl;Group B, nΩ34). pΩ0.0014.
325
ocarcinoma), and miscellaneous disorders in the re-maining five patients (perioperative wound hemor-rhage during re-transplantation for chronic rejection,brain hemorrhage, diaphragmatic paralysis secondaryto diabetic neuropathy, recurrent cholangitis related tomultiple biliary tract strictures, and chronic rejection,respectively).
The overall mortality rate during the whole periodof the study (median: 17 months; range: 0.1–59) was27%. The survival probability in the 162 patients was81%, 74%, 69% and 59% at 12, 24, 36 and 48 months,respectively (patients remaining at risk in each of thesetimes were 97, 65, 39 and 11). The presence of ascitesand increased BUN and serum potassium values at thetime of transplantation were associated with poor post-transplant survival with a significance level of p∞0.10(Table 2). After introducing these three variables into amultivariate analysis (Cox’s multiple regression model),only BUN was found to correlate independently withsurvival (pΩ0.010). Figure 1 shows the cumulative sur-vival of the 162 patients classified according to whethertheir preoperative BUN was normal or increased (Æ25mg/dl or ±25 mg/dl, respectively).
DiscussionThe results of the present study show that preoperativerenal function is a powerful indicator of early andlong-term postoperative prognosis in adult patients re-ceiving liver transplantation for cirrhosis of non-biliaryorigin. Of 23 preoperative variables analyzed in thisinvestigation, only BUN reached statistical significanceas an independent prognostic factor in these patients.This finding agrees with the results reported in almostall the previous studies investigating prognostic factorsin liver transplantation in which preoperative renalfunction parameters were found to strongly correlatewith survival after transplantation (17–21), the onlyexception being one recently published study (22). Ourfindings agreed with these results in spite of the factthat some of these investigations included patients witha very variable degree of renal dysfunction (rangingfrom normal renal function to severe renal failure re-quiring hemodialysis) (17,18), whereas our investiga-tion included only patients with normal renal functionor mild to moderate renal impairment (the maximalvalues of preoperative BUN and serum creatinine were80 and 2.2 mg/dl, respectively). This indicates that pre-operative renal function has a very sensitive prognosticsignificance in liver transplant recipients, which can bemaintained even in the setting of a relatively narrowrange of renal function variability.
Although the reasons for the correlation betweenpreoperative BUN and survival after liver transplan-

E. Gonzalez et al.
tation cannot be ascertained from the results of thepresent study, several possible explanations may besuggested. First, renal function parameters have beenfound to be the most powerful prognostic factors inseveral populations of patients with cirrhosis, such asthose with tense ascites or severe infectious compli-cations (23–26). The relationship between renal dys-function and poor prognosis in patients with cirrhosissuggests that tolerance to adverse events complicatingthe course of the disease (for instance, a serious infec-tion or a very aggressive surgical operation such asliver transplantation) is lower in patients with impairedrenal function than in those with preserved renal func-tion. Mechanisms for this intolerance are not yetclearly understood. An alternative explanation couldbe based on the development of postoperative renalfailure which, while it occurred more frequently in pa-tients with higher preoperative BUN, could have play-ed a contributory role in the death of our patients sinceit was associated with a low hospital survival rate. Fi-nally, an increased risk of postoperative sepsis has beenreported in liver transplant recipients with preoperativerenal dysfunction (19,27). The findings of a recentstudy (28), that renal failure, together with age, Child’sclass and UNOS status, are strongly correlated withsevere complications after transplant (mostly infec-tions) in patients with biliary cirrhosis give additionalsupport to the idea that patients with preoperative re-nal dysfunction are predisposed to post-transplant in-fectious complications. Since the main causes of deathin our series were infections, a link between renal im-pairment, serious infection and death may also be sug-gested in our patients. An additional deleterious factorcould be the use of nephrotoxic antimicrobial agents(such as aminoglycosides and amphotericin B), withthe possibility of worsening a previously impaired renalfunction which, in turn, may contribute to poor sur-vival.
All patients with preoperative renal dysfunction inour series showed renal function parameters suggestingthat the renal impairment was of functional nature(low urinary sodium excretion, normal fresh urinesediment and no significant proteinuria). Therefore,since patients with relevant nephropathy were not in-cluded in our study, the possibility that pre-transplantkidney disease may have influenced the postoperativeoutcome can reasonably be ruled out.
Since the existence of renal dysfunction prior to livertransplantation is associated with a poor prognosis inliver transplant recipients for non-biliary cirrhosis, itmay be concluded that these patients should be trans-planted before the development of renal impairment.In this context it is important to note the results of a
326
recent study reporting that patients with cirrhosis, as-cites and either reduced liver size, low serum sodiumconcentration or high plasma renin activity are at greatrisk of developing renal failure (29). Therefore, it canbe suggested that in ascitic patients with cirrhosisshowing these abnormalities, liver transplantation isindicated as soon as possible to avoid the developmentof renal failure which could impair the post-transplantprognosis in these patients.
One important question is whether liver transplan-tation should be offered or denied to patients withnon-biliary cirrhosis and increased preoperative BUNlevels, since their prognosis is worse than patients with-out renal dysfunction. In our opinion, and accordingto the recommendations published by the Council onEthical and Judicial Affairs of the American MedicalAssociation (30), although the survival disparity be-tween patients with and without renal dysfunction(hospital survival rate of 65% versus 90%, and 4-yearsurvival probability of 49% versus 63%, respectively),is statistically significant, it is not substantial enoughto be relevant in making the clinical decision to acceptor reject these patients for liver transplantation. Fur-thermore, patients with preoperative renal dysfunction(whose survival expectancy without transplantation isvery poor: 35% hospital survival rate and less than25% cumulative survival probability at 4 years)(23,28,31) seem likely to receive sufficient benefit fromthis therapy for them not to be rejected for liver trans-plantation.
Another important issue is the possibility of increas-ing survival expectancy after transplantation in pa-tients with cirrhosis and renal impairment by eitherpreoperatively improving kidney function or perform-ing combined liver-kidney transplantation. However,although both alternatives are attractive from a theor-etical point of view, at present no effective therapy isavailable for ameliorating renal function in these pa-tients, and the potential usefulness of concomitant kid-ney grafting (as a ‘‘pre-emptive’’ procedure for reduc-ing the risk of serious postoperative renal impairment)has never been assessed. Nevertheless, this last possi-bility does not seem very appropriate for patients withonly mild to moderate preoperative renal dysfunction,specially in the current setting of organ donorshortage.
Several authors have reported that other preopera-tive factors, apart from renal dysfunction, mainlythose indicating the existence of severe liver failureand very bad general clinical status, also correlatewith mortality after liver transplantation (2,7–9,18,19,21,32). None of these variables was identifiedas a prognostic factor in our study. This was possibly

Prognostic factors in liver transplant
due to the characteristics of the patients included inthe current investigation. All our patients were adultswith cirrhosis of non-biliary origin and only a smallnumber required intensive care because of critical sta-tus. On the other hand, it has recently been reportedthat sensitive, objective nutritional and metabolic par-ameters are associated with outcome after liver trans-plantation (33). In our study, no relationship was ob-served between preoperative nutritional status andpost-transplant survival, although nutrition in our pa-tients was only clinically (and, therefore, subjectively)assessed. Finally, several authors have reported thatpatients undergoing liver transplantation for cirrhosisrelated to HBV infection or cirrhosis associated withhepatocellular carcinoma show poorer long-term prog-nosis than patients transplanted for other diseases,mainly due to virus infection and tumor recurrence(34–36). This was not observed in our study, probablybecause of the relatively small number of patients withHBV-related cirrhosis in our series and because of thelow tumor recurrence rate (5%; data not shown in theResults) due to the restrictive policy followed in theselection of liver transplant candidates with hepatocel-lular carcinoma, by which only patients with small andnon-extended tumors were accepted for transplan-tation (37).
In summary, among a large number of variables de-termined before surgery, renal function parameters,particularly BUN, were the most important predictorsof survival after liver transplantation in patients withnon-biliary cirrhosis. In these patients, liver transplan-tation should be performed before marked renal dys-function develops.
AcknowledgementsThe study was supported in part by the grant FIS 92/0804 from the Fondo de Investigaciones Sanitarias dela Seguridad Social, Spain.
References1. Neuberger J, Shorrock CS. General considerations. In: Neu-
berger J, Lucey MR, editors. Liver transplantation: practiceand management. London: BMJ Publishing Group; 1994. p.11–24.
2. Donovan JP, Zetterman RK, Burnett DA, Sorrell MF. Pre-operative evaluation, preparation, and timing of orthotopicliver transplantation in the adult. Semin Liver Dis 1989; 9:168–75.
3. Shaw BW, Jr. Exclusion criteria for liver transplantation.Transplant Proc 1989; 21: 3484–6.
4. Rosen HR, Shackleton CR, Martin P. Indications for andtiming of liver transplantation. Med Clin N Am 1996; 80:1069–102.
5. Kilpe VE, Krakauer H, Wren RE. An analysis of liver trans-
327
plant experience from 37 transplant centers as reported toMedicare. Transplantation 1993; 56: 554–61.
6. European Liver Transplant Registry. Data analysis 05/1968–06/1995. Hopital Paul Brousse, Villejuif, France.
7. Adler M, Gavaler J, Duquesnoy R, Fung JJ, Svanas G, StarzlTE, et al. Relationship between diagnosis, preoperative evalu-ation, and prognosis after orthotopic liver transplantation.Ann Surg 1988; 208: 196–202.
8. Gordon RD, Todo S, Tzakis AG, Fung JJ, Stieber A, Stas-chak SM, et al. Liver transplantation under cyclosporine: adecade of experience. Transplant Proc 1991; 23: 1393–6.
9. Doyle HR, Marino I, Morelli F, Doria C, Aldrighetti L,McMichael J, et al. Assessing risk in liver transplantation.Special reference to the significance of a positive crossmatch.Ann Surg 1996; 224: 168–77.
10. Rimola A, Navasa M, Rodes J, Elias E, Neuberger J, LuceyMR, et al. Specific indications. In: Neuberger J, Lucey MR,editors. Liver Transplantation: Practice and Management.London: BMJ Publishing Group, 1994; p. 34–104.
11. Lake JR. Changing indications for liver transplantation.Gastroenterol Clin N Am 1993; 22: 213–29.
12. Tuttle-Newhall JE, Rutledge R, Johnson M, Fair J. A state-wide, population-based, time series analysis of access to livertransplantation. Transplantation 1997; 63: 255–62.
13. Gonzalez FX, Rimola A, Grande L, Antolin M, Garcıa-Val-decasas JC, Fuster J, et al. Predictive factors of early post-operative graft function in human liver transplantation.Hepatology 1994; 20: 565–73.
14. Sher LS, Pan SH, Hoffman AL, Villamil FG, Howard TK,Podesta LG, et al. Liver transplantation. In: Makowka L,editor. The Handbook of Transplantation Management. Au-stin: R.G. Landes Co.; 1991. p. 192–253.
15. Buckels JA. Problems before discharge. In: Neuberger J, Lu-cey MR, editors. Liver Transplantation: Practice and Man-agement. London: BMJ Publishing Group, 1994; p. 151–65.
16. Dixon WJ. BMDP Statistical Software Manual. Berkeley:University of California Press; 1985.
17. Rimola A, Gavaler JS, Schade RR, El-Lakany S, Starzl TE,Van Thiel DH. Effects of renal impairment on liver trans-plantation. Gastroenterology 1987; 93: 148–56.
18. Cuervas-Mons V, Millan I, Gavaler JS, Starzl TE, Van ThielDH. Prognostic value of preoperatively obtained clinical andlaboratory data in predicting survival following orthotopicliver transplantation. Hepatology 1986; 6: 922–7.
19. Baliga P, Merion RM, Turcotte JG, Ham JM, Henley KS,Lucey MR, et al. Preoperative risk factor assessment in livertransplantation. Surgery 1992; 112: 704–11.
20. Mendoza A, Fernandez F, Mutimer DJ. Liver transplan-tation for fulminant hepatic failure: importance of renal fail-ure. Transplant Int 1997; 10: 55–60.
21. Eckhoff DE, Pirsch JD, D’Alessandro AM, Knetchle SJ,Young CJ, Geffner SR, et al. Pretransplant status and patientsurvival following liver transplantation. Transplantation1995; 60: 920–5.
22. Gonwa TA, Klintmalm GB, Levy M, Jennings LS, GoldsteinRM, Husberg BS. Impact of pretransplant renal function onsurvival after liver transplantation. Transplantation 1995; 59:361–5.
23. Llach J, Gines P, Arroyo V, Rimola A, Tito L, BadalamentiS, et al. Prognostic value of arterial pressure, endogenousvasoactive systems, and renal function in cirrhotic patientsadmitted to the hospital for the treatment of ascites. Gastro-enterology 1988; 94: 482–7.

E. Gonzalez et al.
24. Toledo C, Salmeron JM, Rimola A, Navasa M, Arroyo V,Llach J, et al. Spontaneous bacterial peritonitis in cirrhosis:predictive factors of infection resolution and survival in pa-tients treated with cefotaxime. Hepatology 1993; 17: 251–7.
25. Follo A, Llovet JM, Navasa M, Planas R, Forns X, Franci-torra A, et al. Renal impairment after spontaneous bacterialperitonitis in cirrhosis: incidence, clinical course, predictivefactors and prognosis. Hepatology 1994: 20: 1495–501.
26. Cabrera J, Arroyo V, Ballesta AM, Rimola A, Gual J, ElenaM, et al. Aminoglycoside nephrotoxicity in cirrhosis: valueof urinary b2-microglobulin to discriminate functional renalfailure from acute tubular damage. Gastroenterology 1982;82: 97–105.
27. Mora NP, Cofer JB, Solomon H, Goldstein RM, Gonwa TA,Husberg BS, et al. Analysis of severe infections (INF) after180 consecutive liver transplants: the impact of amphotericinB prophylaxis for reducing the incidence and severity offungal infections. Transplant Proc 1991; 23: 1528–30.
28. Ricci P, Thernau TM, Malinchoc M, Benson JT, Petz, JLKlintmalm GB, et al. A prognostic model for the outcome ofliver transplantation in patients with cholestatic liver disease.Hepatology 1997; 25: 672–77.
29. Gines A, Escorsell A, Gines P, Salo J, Jimenez W, IngladaL, et al. Incidence, predictive factors, and prognosis of thehepatorenal syndrome in cirrhosis with ascites. Gastroenter-ology 1993; 105: 229–36.
30. Council on Ethical and Judicial Affairs, American MedicalAssociation. Ethical considerations in the allocation of or-gans and other scarce medical resources among patients.Arch Intern Med 1995; 155: 29–40.
328
31. Rodes J, Bosch J, Arroyo V. Clinical types and drug therapyof renal impairment in cirrhosis. Postgrad Med J 1975; 51:492–7.
32. Mora NP, Klintmalm GB, Solomon H, Goldstein RM, Gon-wa TA, Husberg BS. Survival after liver transplantation in300 consecutive patients: the influence of age, clinical status,and pretransplant disease. Transplant Proc 1992; 24: 156–7.
33. Selberg O, Bottcher J, Tusch G, Pichlmayr R, Henkel E,Muller M-J. Identification of high- and low-risk patients be-fore liver transplantation: a prospective cohort study of nu-tritional and metabolic parameters in 150 patients. Hepa-tology 1997; 25: 652–7.
34. Todo S, Demetris AJ, Van Thiel DH, Teperman L, Fung JJ,Starzl TE. Orthotopic liver transplantation for patients withhepatitis B virus-related liver disease. Hepatology 1991; 13:619–26.
35. Samuel D, Muller R, Alexander G, Fassati L, Ducot B,Benhamou JP, et al., and the Investigators of the EuropeanConcerted Action on Viral Hepatitis Study. Liver transplan-tation in European patients with the hepatitis B surface anti-gen. N Engl J Med 1993; 329: 1842–7.
36. Gores GJ. Liver transplantation for malignant disease.Gastroenterol Clin N Am 1993; 22: 285–99.
37. Castells A, Bruix J, Bru C, Fuster J, Vilana R, Navasa M, etal. Treatment of small hepatocellular carcinoma in cirrhoticpatients: a cohort study comparing surgical resection andpercutaneous ethanol injection. Hepatology 1993; 18: 1121–6.