liver involvement in hematological malignancy liver involvement in... · linical presentation of...
TRANSCRIPT

Liver involvement in Hematologic malignancy
Dr Taya Kitiyakara
Ramathibodi hospital
Mahidol University
For THASL, 21-23 Mar 2013

Hematologic malignancy
Lymphoma
Leukaemia
Myeloma
Myeloproliferative diseases

Grouping of liver involvement
Diagnosis
(Pre-Rx) Treatment Long-term
post Rx

Diagnosis Treatment Post-treatment long-term
Liver infiltration Infections Chronic GVH
Acute liver failure Drugs Fe overload
Amyloidosis Sinusoidal
obstruction syndrome
NRH; FNH
Primary hepatic lymphoma
Acute Graft-versus-Host disease (GVH)
Others: Infections
Haem recurrence PTLD
Splanchnic venous thrombosis
Biliary tract obstruction/
infection Cirrhosis, HCC

Diagnosis Treatment Post-treatment long-term
Liver infiltration Infections Chronic GVH
Acute liver failure Drugs Fe overload
Amyloidosis Sinusoidal
obstruction syndrome
NRH; FNH
Primary hepatic lymphoma
Acute Graft-versus-Host disease (GVH)
Others: Infections
Haem recurrence PTLD
Splanchnic venous thrombosis
Biliary tract obstruction/
infection Cirrhosis, HCC

Direct and indirect infiltration of the liver in hematologic malignancy
• All leukaemia, lymphoma, myeloma can cause infiltration of the liver
• Problems include abnormal LFT (AlkP and γGT), biliary obstruction, hepatomegaly and liver failure
• Myeloma can produce amyloid
• Primary hepatic lymphoma
• (Hepato-splenic T cell lymphoma)

Liver infiltration by lymphoma

Infiltration of the liver by hematologic cells is common
• Hodgkin’s Lymphoma: 5% of patients have infiltration at diagnosis, 50% at autopsy
(Jaundice more from tissue infiltration> biliary obstruction)
• NHL: 20-45% of patients have liver
infiltration (Jaundice from biliary obstruction>
infiltration)
• Myeloma: 25-40% infiltration on autopsy
Infiltration into sinusoids (vs portal area in autoimmune hepatitis)
Immunoperoxidase staining for lambda light chains of sinusoidal plasma cells C Barth et al. Z Gastroenterol 2005 MJ Birrer et al Semin Liver Dis 1987 KI Lei et al Leuk Lymph 1998

Biliary obstruction from infiltration
Patient with Lymphoma in Ramathibodi hospital
Hematologic malignancy as cause of liver failure
• Costa F et al, Chronic lymphocytic leukemia Leuk Lymphoma 1998 • Esfahani K et al Chronic lymphocytic leukemia Current Oncol 2011 • Padilla GF et al non-Hodgkin lymphoma Acta Gastroenterol Latinoam 2008. • Dellon ES et al natural killer–like T-cell leukemia/ Lymphoma World JGastroenterol 2006;
• Kojima H, et al Lennert’s lymphoma Leuk Lymphoma 2003.
• Santos ES et al Primary hepatic non-Hodgkin’s lymphomas Am J Gastroenterol 2003 • Lettieri CJ et al non-Hodgkin’s lymphoma Am J Gastroenterol 2003. • Thompson DR, malignant lymphoma Clin Lymphoma 2001
• Yeshurun M et al low-grade NHL transformation into large-cell lymphoma Leuk Lymphoma 2001 • Morali GA et al relapsing non-Hodgkin’s lymphoma Eur J Gastroenterol Hepatol 2001 • Anderson SH et al acute leukaemia Liver 2001 • Stewart KS, et al. Non-Hodgkin lymphoma in pregnancy Obstet Gynecol 1999. • Suzuki N et al. Ki-1 lymphoma Am J Gastroenterol 1998
• Souto P haematological malignancy Eur J Gastroenterol Hepatol 1997;
• Yoshikawa M, hepatosplenic B-cell non-Hodgkin’s lymphoma J Gastroenterol 1996
• Woolf GM et al. Lymphoma Dig Dis Sci 1994 • Zafrani ES et al Primary lymphoma of the liver Liver 1993. • Salo J et al. non-Hodgkin’s lymphoma. Am J Gastroenterol 1993 • Rahhal FE et al Myeloma. World J Gastroenterol 2009

Liver failure from hematologic malignancy
• Rare
• Time-scale from presentation to liver failure varies (from days to weeks)
• Jaundice, coagulopathy, encephalopathy
• Elevated LDH, lactic acidosis and recurrent hypoglycaemia also seen
• Urgent Transjugular liver biopsy needed for rapid diagnosis and treatment (if other tissue can not be obtained) K Esfahani et al Current Oncol 2011

Diagnosis Treatment Post-treatment long-term
Liver infiltration Infections Chronic GVH
Acute liver failure Drugs Fe overload
Amyloidosis Sinusoidal
obstruction syndrome
NRH; FNH
Primary hepatic lymphoma
Acute Graft-versus-Host disease (GVH)
Others: Infections
Haem recurrence PTLD
Splanchnic venous thrombosis
Biliary tract obstruction/
infection Cirrhosis, HCC

Amyloidosis (AL) associated with multiple myeloma
• Manifestation of hepatic amyloidosis: – Hepatosplenomegaly – ALKP ↑ – Splenomegaly – Ascites – PT prolong (acquired
factor X deficiency) – Cholestasis – Jaundice – Acute liver failure – Spontaneous rupture
Heart failure Renal failure Neuropathy rash
JH Pinney et al Ann Clin Biochem 2012 T Cross et al Postgrad Med J 2006

Diagnosis: Histology showing Amyloid deposition: fat pad
aspiration, rectal biopsy, liver biopsy Imaging Scintigraphy with 123I-human serum amyloid P
(SAP) component TREATMENT: Suppression of B cells/underlying clonal disease Autologous stem cell transplantation OUTCOME: Untreated: <5% survival in 10yrs Variable survival with treatment, Related to extent organ damage Reported 42% survival in 4 years
Kumar SK et al Mayo Clin Proc 2011 Pinney JH et al Ann Clin Biochem 2012

Diagnosis Treatment Post-treatment long-term
Liver infiltration Infections Chronic GVH
Acute liver failure Drugs Fe overload
Amyloidosis Sinusoidal
obstruction syndrome
NRH; FNH
Primary hepatic lymphoma
Acute Graft-versus-Host disease (GVH)
Others: Infections
Haem recurrence PTLD
Splanchnic venous thrombosis
Biliary tract obstruction/
infection Cirrhosis, HCC
Primary Hepatic lymphoma
• DEFINITION:
• PHL as a lymphoma localized and limited to the liver without extrahepatic involvement.
• Symptoms should be explainable by involvement of the liver.
• Furthermore, superficial lymphadenopathy, splenomegaly, abnormal hematological parameters, spleen or bone marrow localization cannot be present for at least 6 mo after appearance of the hepatic lesion
EJA Steller et al World J Radiol 2012

Clinical presentation of 1⁰ hepatic lymphoma
• Clinical presentation of PHL is nonspecific.
• Most often fever, loss of weight and night sweats (also known as ‘B’ symptoms) occur.
• Alternative symptoms described are: right upper abdominal pain, epigastric pain, abdominal distension, nausea- vomiting, anorexia, asthenia or itch.
• Jaundice and hepatomegaly (rarely ascites) can be found in some patients.
• Blood tests can show abnormal AST, ALT, AlkP, total and direct bilirubin and LDH
Common cell types: B-cell NHL (63%) and T-cell lymphoma (25%)

• Solitary liver nodule • Multiple nodules • Diffuse infiltrating
On CT: • hypo- or iso-
attenuating • Hypointense on
contrast injection or rim enhancement
On MRI: • Hypointense T1 • Slight enhancement
of signal T2
1/3 each
Noronha V et al Crit Rev Oncol/Hematol 2005

Treatment for 1⁰ Hepatic lymphoma
• Chemotherapy is the treatment of choice
• Many will have had surgery, and chemotherapy should be used adjunctively
• No randomised controlled trials
• However, outcomes were not good in case series.
EJA Steller et al World J Radiol 2012

Diagnosis Treatment Post-treatment long-term
Liver infiltration Infections Chronic GVH
Acute liver failure Drugs Fe overload
Amyloidosis Sinusoidal
obstruction syndrome
NRH; FNH
Primary hepatic lymphoma
Acute Graft-versus-Host disease (GVH)
Others: Infections
Haem recurrence PTLD
Splanchnic venous thrombosis
Biliary tract obstruction/
infection Cirrhosis, HCC

Clinical presentation
• Budd-chiari syndrome: ascites, abdominal pain, encephalopathy, upper GI bleeding
• Abnormal AST/ALT
• Portal vein thrombosis: abdominal pain, nausea, dyspepsia, loose stool. Less commonly: small bowel infarction
• Severity of symptoms depends on extent and speed of thrombus
• Diagnosis often by Doppler, CT contrast scan, MRI
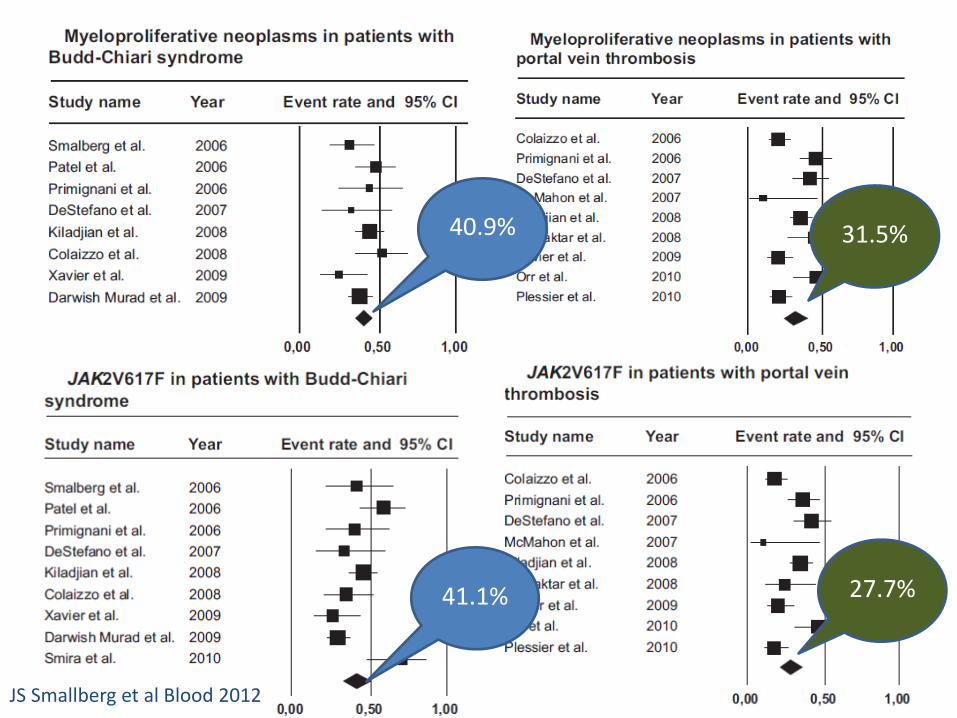
40.9%
27.7% 41.1%
31.5%
JS Smallberg et al Blood 2012

Distribution of Myeloproliferative disorder subtypes in non-cirrhotic
Splanchnic Thrombosis
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Budd-Chiari Portal V thrombosis
JAK2V617F+ only
unclassified MPN
MF
ET
PV
JS Smallberg et al Blood 2012

Treatment
• Anticoagulation • Angioplasty/ shunt/ stent • TIPS when angioplasty and medical treatment
fails • Liver transplantation
• Treatment of MPN disorder • Unclear whether any MPN-specific treatment
should be given to solitary JAK2 patients other than close observation
Baveno V consensus workshop on portal hypertension. J Hepatol 2010
JS Smallberg et al Blood 2012

A common problem for hepatologists: ….abnormal LFT’s /jaundice after stem
cell transplantation?!? 1. Sepsis related cholestasis 2. Acute graft versus host
disease 3. Sinusoidal obstruction
syndrome 4. Tumour infiltration 5. Liver infection 6. Cardiac failure 7. Antibiotics/antifungals 8. Ciclosporin 9. TPN 10. Biliary obstruction/infection

Timetable for common complications after stem cell transplantation for
hematologic malignancies
HH Tuncer et al World J Gastroenterol 2012

Diagnosis Treatment Post-treatment long-term
Liver infiltration Infections Chronic GVH
Acute liver failure Drugs Fe overload
Amyloidosis Sinusoidal
obstruction syndrome
NRH; FNH
Primary hepatic lymphoma
Acute Graft-versus-Host disease (GVH)
Others: Infections
Haem recurrence PTLD
Splanchnic venous thrombosis
Biliary tract obstruction/
infection Cirrhosis, HCC

Liver infections
Bacteria
mycobacterium
Non-opportunistic /
Biliary tract
Virus
CMV
HSV
HHV-6
VZV
adenovirus
EBV
(PTLD)
HBV
HCV
Fungus
Aspergillosis
Candida
(krusei, galbrata)
Molds:
Scopulariopsis
Trichosporon
Pseudallescharia
Fusarium
mucor

CMV and Herpes family virus
นพ. วชัรศกัดิ์ โชติยะปตุตะ
Acute viral infection: Dengue and Herpes infection

Adenovirus hepatitis
Extensive liver necrosis can occur with adenovirus.
Patients often have
combinations of: fever, respiratory distress,
diarrhea, and liver dysfunction.
Note the "smudgy" appearance of the nucleus(arrows), they are characterized by a crowding of chromatin towards the nuclear membrane. Immunohistochemical staining are confirmatory
Diagnosis with DNA blood test or immunohistochem’. Treatment is with cidofovir
Neofytos D et al Biol Blood Marrow Transplant 2007

On the left, a sterile healing abscess with a
necrotic center devoid of fungal elements, surrounded by inflammatory cells and a pseudo-capsule (asterisk) On the right, an acute abscess with a small focus of red-staining fungal elements (arrow) in a field of degenerative neutrophils, surrounded by a pseudo-capsule
Fungal infections: •Fever with tender enlarged hepatomegaly •Micro-abscesses may be missed by CT scan •Liver biopsy often needed •Prophylaxis antifungal treatment often select triazole resistant fungi and molds •Restoration of granulocyte count is the most important factor in recovery
GB MacDonald Hepatology 2010

Diagnosis Treatment Post-treatment long-term
Liver infiltration Infections Chronic GVH
Acute liver failure Drugs Fe overload
Amyloidosis Sinusoidal
obstruction syndrome
NRH; FNH
Primary hepatic lymphoma
Acute Graft-versus-Host disease (GVH)
Others: Infections
Haem recurrence PTLD
Splanchnic venous thrombosis
Biliary tract obstruction/
infection Cirrhosis, HCC

Commonly used and reported drugs
Hepatitic picture
• cyclophosphamide infusions,
• liposomal amphotericin,
• trimethoprim-sulfamethoxazole,
• itraconazole, voriconazole
• imatinib
Cholestatic picture
• Cyclosporin
• Tacrolimus
• trimethoprim-sulfamethoxazole,
• itraconazole, voriconazole, fluconazole, posaconazole
• TPN
“..in many cases, attribution to a single drug is mostly guesswork because every patient receives multiple drugs”.
GB MacDonald et al Hepatology 2010

Diagnosis Treatment Post-treatment long-term
Liver infiltration Infections Chronic GVH
Acute liver failure Drugs Fe overload
Amyloidosis Sinusoidal
obstruction syndrome
NRH; FNH
Primary hepatic lymphoma
Acute Graft-versus-Host disease (GVH)
Others: Infections
Haem recurrence PTLD
Splanchnic venous thrombosis
Biliary tract obstruction/
infection Cirrhosis, HCC

Sinusoidal obstruction syndrome (SOS) aka. Hepatic veno-occlusive disease
• Early onset after starting myeloablative therapy for stem cell transplantation
• Clinical features: tender hepatomegaly, hyperbilirubinaemia, fluid retention with weight gain
• Diagnostic criteria by investigators in Seattle and Baltimore
• Risk factors related mainly to myeloablative therapy

Diagnostic criteria for SOS Seattle group criteria Baltimore group criteria
Diagnosis requires 2 out of 3, within 20 days of transplantation
Hyperbilirubinemia (>2mg/dl) plus 2 or more of:
Bilirubin >2mg/dl Hepatomegaly, usually painful
Hepatomegaly or RUQ pain from liver
≥5% weight gain
>2% weight gain due to fluid accumulation
Ascites
McDonald GB et al Ann Intern Med 1993 Jones RJ et al Transplantation 1987

Risk factors for SOS Liver disease at base line Specific conditioning regimens Other drugs during
conditioning
HBV or HCV Cyclophosphamide(CY) based Itraconazole
NASH Cy 120mg/kg + TBI (esp with
higher TBI doses)
Sirolimus
(rapamycin)
Alcoholic hepatitis BCV (Cy+ BCNU+ VP-16) Norethisterone
Fibrosis/cirrhosis Cy+ BU
Extramedullary hemapoiesis
with sinusoidal fibrosis Mephalan (Mel) based
Intrahepatic cholestasis with
jaundice Mel + BU
Prior History Other regimens
Prior SOS BU + TBI
Prior liver irradiation
Gemtuzumab ozogamicin-
containing myeloablative
regimens
TBI= total body irradiation BU= busulfan
Prior myeloablative
hematopoietic cell transplant
High dose radiolabelled antibody
myeloablative regimen
HH Tuncer et al World J Gastroenterol 2012

Pathogenesis of Sinusoidal obstruction syndrome
Chemotherapy Irradiation other drugs

Pathogenesis of Sinusoidal obstruction syndrome
•Intrahepatic coagulation not thought to be main cause of disease •Other biochemical changes: NO, glutathione, matrix metalloproteinase-9, F-actin

Histology of SOS
• A. Zone 3 of the liver acinus in an early phase of SOS, with disruption of sinusoidal anatomy, red blood cells extending through the space of Disse, hepatocyte necrosis, and subendothelial edema in a patent central vein (CV) (H&E).
• B. Extensive hepatocyte necrosis and dropout, disruption of sinusoids, extravasation of red blood cells throughout zone 3, and subendothelial fibrosis (Masson trichrome).
GB MacDonald Hepatology 2010

Sinusoidal obstruction Syndrome
Evaluation
• Clinical (rapidity of symptom development)
• Level of abnormal LFT (bilirubin, AST>750u/l)
• USS doppler (reverse flow in PV, thrombosis)
• HVPG >20mmHg
• Other organ failure
Treatment
• Supportive
• No effective treatment
• Prophylaxis with Heparin does NOT work
• Prophylactic Defibrotide?
• PREVENTIVE- by avoiding high risk myeloablative regimens

Outcome
• 70% of patients resolve spontaneously
• Death usually from renal and cardiopulmonary failure
• “Reverse” cirrhosis can occur in survivors
‘Normal’ cirrhosis: fibrosis occurring around portal tracts and spreading to other portal tracts
CV

Histology of chronic SOS
• F. confluent fibrosis in and around adjacent central veins, with central to central bridges forming a picture of “reverse” cirrhosis two months after transplant.
Trichrome : Intimal and perisinusoidal fibrosis
GB MacDonald Hepatology 2010 Photo courtesy of Dr N Angkathunyakul

Diagnosis Treatment Post-treatment long-term
Liver infiltration Infections Chronic GVH
Acute liver failure Drugs Fe overload
Amyloidosis Sinusoidal
obstruction syndrome
NRH; FNH
Primary hepatic lymphoma
Acute Graft-versus-Host disease (GVH)
Others: Infections
Haem recurrence PTLD
Splanchnic venous thrombosis
Biliary tract obstruction/
infection Cirrhosis, HCC

Acute Graft-versus-Host disease (aGVH)
• Arises when donor T cells respond to genetically different proteins on host cells (so starts at engraftment)
• Frequency directed related to the degree of mismatch in HLA proteins
• Non-HLA proteins also involved
• (30-40% incidence in HLA matched related donors , 60-80% incidence with one HLA Ag mismatch unrelated donors)
• 3 main organs: Skin, Gastrointestinal tract and Liver
JLM Ferrara et al Lancet 2009

aGVH: a common sequence
Skin
Maculopapular rash
Bullous lesions
GI tract
Watery diarrhoea
Abdominal pain
Liver
Cholestatic LFT
Jaundice
Hepatitic variant After donor lymphocyte
infusion JLM Ferrara et al Lancet 2009

Evaluating aGVH Staging of acute Graft versus Host disease
(modified Keystone criteria)
stage Skin GI tract Liver
0 No rash Diarrhea <500mL/d Bilirubin <2.0mg/dL
1 Maculopapular rash <25% of
body surface
Diarrhea 501-
1000mL/d or nausea
(+/- vomiting)
Bilirubin 2.0-
3.0mg/dL
2 Maculopapular rash 25-50% of
body surface
Diarrhea 1001-
1500mL/d
Bilirubin 3.1-
6.0mg/dL
3 Generalized erythroderma Diarrhea >1501mL/d Bilirubin 6.1-
15mg/dL
4 Generalized erythroderma
with blister/bullous formation
and desquamation
Severe abdominal
pain +/- ileus Bilirubin >15mg/dL
Grade: Severe Grade: life-threatening

Diagnosis
• Clinical symptoms with associated histopathology
• Often histopathology difficult to obtain from the liver (low platelet count)
• Easier to obtain tissue from skin or upper/lower GI tract
• Important findings: – lymphocytic infiltration and – apoptosis in crypts

Diffuse cholestasis with bile duct damage (lymphocytic infiltrate, Nuclear pleomorphism and Vacuolization of bile duct epithelium )
Histology of hepatic Acute GVHD
Important features (simplified): 1. lymphocytic infiltration of bile duct 2. Bile duct epithelial damage 3. bile duct degeneration and 4.cholestatis
Photo courtesy of Dr N Angkathunyakul

Treatment
• Ursodeoxycholic acid improves bilirubin level
• High dose corticosteroids is the mainstay of treatment (complete response in 30-50%)
• Other immunosuppressive regimens for non-responders
• Many progress to become cGVHD

Modified from S Aria et al J Hematotherapy Stem cell Res 2002
Mini-summary and algorithm in peri-transplant period
Liver dysfunction
Bili>2.5
AST/ALT>200
ALP>300
hepatomegaly
Symptoms
Weight
Drugs?
Blood for testing/smear
Restrict Na 2g/g
TPN holiday
ciclosporin→tacro’
Cultures
Viral DNA
Imaging:
Normal
Imaging: Biliary tract
disease
Imaging:
Focal mass/lesion
Imaging:
Hepatomegaly
(ascites)
VOD? Micro-
abscesses biopsy
Rx Surgical consult
Infection?: Rx. Follow LFT 3 days-worse?
Worse :biopsy If not worse:
observe, …assess in 3
days: better?
If not:biopsy

Phew! The immediate stem cell transplant period is over…

Diagnosis Treatment Post-treatment long-term
Liver infiltration Infections Chronic GVH
Acute liver failure Drugs Fe overload
Amyloidosis Sinusoidal
obstruction syndrome
NRH; FNH
Primary hepatic lymphoma
Acute Graft-versus-Host disease (GVH)
Others: Infections
Haem recurrence PTLD
Splanchnic venous thrombosis
Biliary tract obstruction/
infection Cirrhosis, HCC

Chronic GVHD • Definition: arbitary cut-off at 100 days
• Major cause of late non-relapse death
• Risk factors: old age and acute GVHD
• Hepatic manifestations:
– Abnormal ALT ALP γGT
– Slowly progressive jaundice
– Acute hepatitic picture
• Liver biopsy often needed
• Treatment with
– UDCA
– Immunosuppression
JLM Ferrara et al Lancet 2009

Liver histology in chronic GVHD
• E. A portal space showing absence of recognizable bile duct epithelium in a patient with longstanding refractory chronic GVHD (H&E).
Important features: Lobular hepatitis Portal inflammation Loss of small bile ducts
MacDonald GB Hepatology 2010

Diagnosis Treatment Post-treatment long-term
Liver infiltration Infections Chronic GVH
Acute liver failure Drugs Fe overload
Amyloidosis Sinusoidal
obstruction syndrome
NRH; FNH
Primary hepatic lymphoma
Acute Graft-versus-Host disease (GVH)
Others: Infections
Haem recurrence PTLD
Splanchnic venous thrombosis
Biliary tract obstruction/
infection Cirrhosis, HCC

Nodular Regenerative hyperplasia
NRH: Nodular architecture without intervening fibrosis A response to vascular injury from malignancy or its treatment Clinically silent but may produce portal hypertension
Photo courtesy of Dr N Angkathunyakul

Central fibrous scar Reported to be up to 12% of survivors
Focal nodular hyperplasia
Photo courtesy of Dr N Angkathunyakul

Diagnosis Treatment Post-treatment long-term
Liver infiltration Infections Chronic GVH
Acute liver failure Drugs Fe overload
Amyloidosis Sinusoidal
obstruction syndrome
NRH; FNH
Primary hepatic lymphoma
Acute Graft-versus-Host disease (GVH)
Others: Infections
Haem recurrence PTLD
Splanchnic venous thrombosis
Biliary tract obstruction/
infection Cirrhosis, HCC

Fever
Tender hepatomegaly
Predominantly Elevated ALP (Jaundice)
Summary
Sepsis Biliary disease
Fungus Abscess
Viral infection
SOS
Infiltration cGVHD
Cardiac failure
Budd-Chiari
Mycobacterial infection
Drugs aGVHD
Fe overload NRH FNH Cirrhosis/HCC