liquidos en el paciente septico
TRANSCRIPT

American Journal of Emergency Medicine 33 (2015) 186–189
Contents lists available at ScienceDirect
American Journal of Emergency Medicine
j ourna l homepage: www.e lsev ie r .com/ locate /a jem
Original Contribution
Fluid balance in sepsis and septic shock as a determining factor
of mortalityJosep-Maria Sirvent, MD, PhD a,⁎, Cristina Ferri, MD b, Anna Baró, MD a,Cristina Murcia, MD a, Carolina Lorencio, MD a
a Department of Intensive Care (ICU), University Hospital of Girona Doctor Josep Trueta, IDIBGI, CIBERES, Girona, Spainb Department of Intensive Care (ICU), University Hospital of Tarragona Joan XXIII, Tarragona, Spain
a b s t r a c ta r t i c l e i n f o
⁎ Corresponding author. Department of Intensive CarGirona Doctor Josep Trueta, Avda de França s/n, E-1700940 288; fax: +34 972 940 296.
E-mail address: [email protected] (J.-M. Si
http://dx.doi.org/10.1016/j.ajem.2014.11.0160735-6757/© 2014 Elsevier Inc. All rights reserved.
Article history:
Received 11 October 2014Received in revised form 25 October 2014Accepted 7 November 2014Objective: The objective was to assess whether fluid balance had a determinant impact on mortality rate in acohort of critically ill patients with severe sepsis or septic shock.Design: A prospective and observational study was carried out on an inception cohort.Setting: The setting was an intensive care unit of a university hospital.Patients: Patients admitted consecutively in the intensive care unit who were diagnosed with severe sepsis or
septic shock were included.Interventions: Demographic, laboratory, and clinical data were registered, as well as time of septic shock onset,illness severity (Simplified Acute Physiology Score II, Sepsis-related Organ Failure Assessment), and comorbidi-ties. Daily and accumulated fluid balance was registered at 24, 48, 72, and 96 hours. Survival curves representing28-day mortality were built according to the Kaplan-Meier method.Results:A total of 42patientswere included in the analysis:men, 64.3%;mean age, 61.8±15.9 years. Septic shockwas predominant in 69% of the cases. Positive blood cultures were obtained in 17 patients (40.5%). No age, sex,Sepsis-related Organ Failure Assessment, creatinine, lactate, venous saturation of O2, and troponin differenceswere observed upon admission between survivors and nonsurvivors. However, higher Simplified Acute Physiol-ogy Score II was observed in nonsurvivors, P= .016. Nonsurvivors also showedhigher accumulated positive fluidbalance at 48, 72, and 96 hours with statistically significant differences. Besides, significant differences (P= .02)were observed in the survival curve with the risk of mortality at 72 hours between patients with greater than 2.5L and less than 2.5 L of accumulated fluid balance.Conclusions: Fluid administration at the onset of severe sepsis or septic shock is the first line of hemodynamictreatment. However, the accumulated positive fluid balance in the first 48, 72, and 96 hours is associated withhigher mortality in these critically ill patients.© 2014 Elsevier Inc. All rights reserved.
1. Introduction
In severe sepsis and septic shock, themain elements of treatment areintravenous fluids, appropriate antibiotics, source control, vasopressors,and ventilatory support [1]. For more than 10 years, the administrationof intravenous fluids has been known as a key in the initial stages ofsepsis resuscitation, as proven by a classic article on goal-based treat-ments [2]. Anyway, it is now recognized that the administration ofexcess fluid in sepsis may lead to worsened respiratory function,increased intraabdominal pressure, worsened coagulopathy, andincreased probability of cerebral edema [3]. Some authors observed dif-ficulty in fluid balancemanagement in critically ill patients, and positivefluid balance is associated with increased mortality rates in patients
e (ICU), University Hospital of7 Girona, Spain. Tel.: +34 972
rvent).
with acute lung injury and septic shock [4,5]. For all these reasons, thepresent observational study was designed to assess whether fluidbalance has a determinant impact onmortality in a well-defined cohortof patients with severe sepsis or septic shock.
2. Methods
2.1. Population and data collection
Our study includes the patients admitted consecutively in the inten-sive care unit (ICU) of a teaching hospital for 4 months (from October2012 to January 2013) that were diagnosed with severe sepsis or septicshock. It is a prospective and observational study on an inception cohort.Patients with septic shock were identified by a specific team ofintensivists. Demographic, laboratory, and clinical data were registered:age, sex, time of septic shock onset, focus of infection, presence of initialacute kidney injury, severity of illness based on the Simplified AcutePhysiology Score (SAPS) II score [6], the Sepsis-related Organ Failure
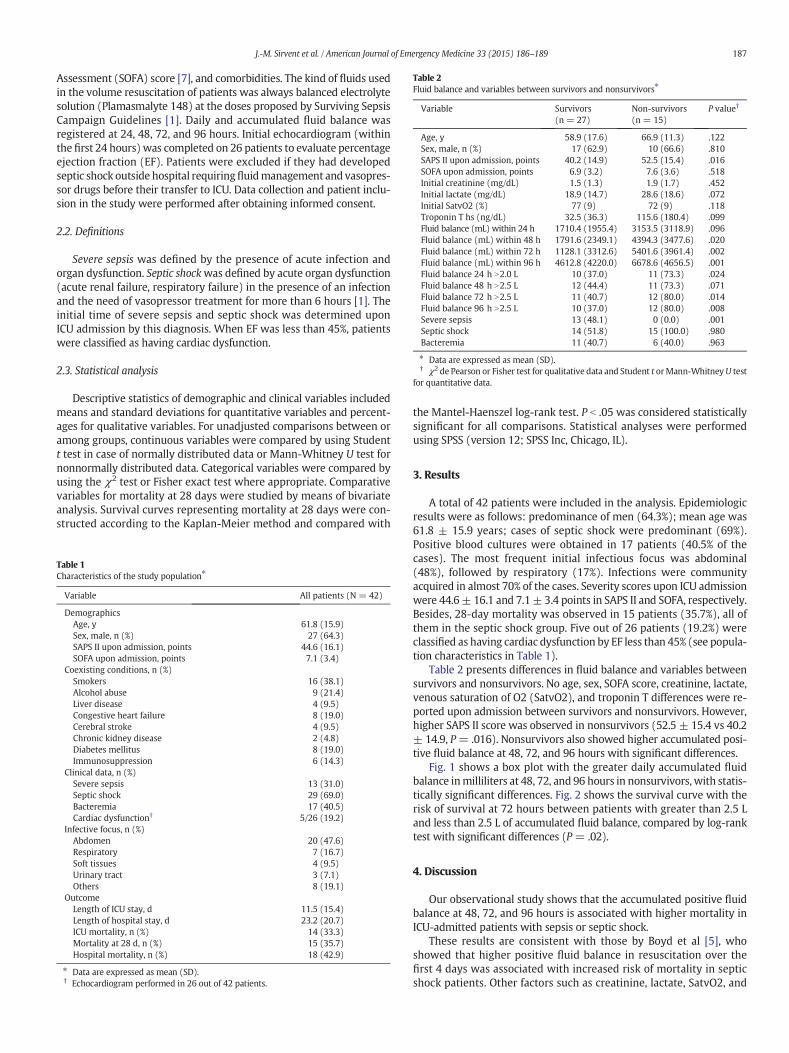
Table 2Fluid balance and variables between survivors and nonsurvivors⁎
Variable Survivors(n = 27)
Non-survivors(n = 15)
P value†
Age, y 58.9 (17.6) 66.9 (11.3) .122Sex, male, n (%) 17 (62.9) 10 (66.6) .810SAPS II upon admission, points 40.2 (14.9) 52.5 (15.4) .016SOFA upon admission, points 6.9 (3.2) 7.6 (3.6) .518Initial creatinine (mg/dL) 1.5 (1.3) 1.9 (1.7) .452Initial lactate (mg/dL) 18.9 (14.7) 28.6 (18.6) .072Initial SatvO2 (%) 77 (9) 72 (9) .118Troponin T hs (ng/dL) 32.5 (36.3) 115.6 (180.4) .099Fluid balance (mL) within 24 h 1710.4 (1955.4) 3153.5 (3118.9) .096Fluid balance (mL) within 48 h 1791.6 (2349.1) 4394.3 (3477.6) .020Fluid balance (mL) within 72 h 1128.1 (3312.6) 5401.6 (3961.4) .002Fluid balance (mL) within 96 h 4612.8 (4220.0) 6678.6 (4656.5) .001Fluid balance 24 h N2.0 L 10 (37.0) 11 (73.3) .024Fluid balance 48 h N2.5 L 12 (44.4) 11 (73.3) .071Fluid balance 72 h N2.5 L 11 (40.7) 12 (80.0) .014Fluid balance 96 h N2.5 L 10 (37.0) 12 (80.0) .008Severe sepsis 13 (48.1) 0 (0.0) .001Septic shock 14 (51.8) 15 (100.0) .980Bacteremia 11 (40.7) 6 (40.0) .963
⁎ Data are expressed as mean (SD).† χ2 de Pearson or Fisher test for qualitative data and Student t orMann-WhitneyU test
for quantitative data.
187J.-M. Sirvent et al. / American Journal of Emergency Medicine 33 (2015) 186–189
Assessment (SOFA) score [7], and comorbidities. The kind of fluids usedin the volume resuscitation of patients was always balanced electrolytesolution (Plamasmalyte 148) at the doses proposed by Surviving SepsisCampaign Guidelines [1]. Daily and accumulated fluid balance wasregistered at 24, 48, 72, and 96 hours. Initial echocardiogram (withinthe first 24 hours) was completed on 26 patients to evaluate percentageejection fraction (EF). Patients were excluded if they had developedseptic shock outside hospital requiringfluidmanagement and vasopres-sor drugs before their transfer to ICU. Data collection and patient inclu-sion in the study were performed after obtaining informed consent.
2.2. Definitions
Severe sepsis was defined by the presence of acute infection andorgan dysfunction. Septic shockwas defined by acute organ dysfunction(acute renal failure, respiratory failure) in the presence of an infectionand the need of vasopressor treatment for more than 6 hours [1]. Theinitial time of severe sepsis and septic shock was determined uponICU admission by this diagnosis. When EF was less than 45%, patientswere classified as having cardiac dysfunction.
2.3. Statistical analysis
Descriptive statistics of demographic and clinical variables includedmeans and standard deviations for quantitative variables and percent-ages for qualitative variables. For unadjusted comparisons between oramong groups, continuous variables were compared by using Studentt test in case of normally distributed data or Mann-Whitney U test fornonnormally distributed data. Categorical variables were compared byusing the χ2 test or Fisher exact test where appropriate. Comparativevariables for mortality at 28 days were studied by means of bivariateanalysis. Survival curves representing mortality at 28 days were con-structed according to the Kaplan-Meier method and compared with
Table 1Characteristics of the study population⁎
Variable All patients (N = 42)
DemographicsAge, y 61.8 (15.9)Sex, male, n (%) 27 (64.3)SAPS II upon admission, points 44.6 (16.1)SOFA upon admission, points 7.1 (3.4)
Coexisting conditions, n (%)Smokers 16 (38.1)Alcohol abuse 9 (21.4)Liver disease 4 (9.5)Congestive heart failure 8 (19.0)Cerebral stroke 4 (9.5)Chronic kidney disease 2 (4.8)Diabetes mellitus 8 (19.0)Immunosuppression 6 (14.3)
Clinical data, n (%)Severe sepsis 13 (31.0)Septic shock 29 (69.0)Bacteremia 17 (40.5)Cardiac dysfunction† 5/26 (19.2)
Infective focus, n (%)Abdomen 20 (47.6)Respiratory 7 (16.7)Soft tissues 4 (9.5)Urinary tract 3 (7.1)Others 8 (19.1)
OutcomeLength of ICU stay, d 11.5 (15.4)Length of hospital stay, d 23.2 (20.7)ICU mortality, n (%) 14 (33.3)Mortality at 28 d, n (%) 15 (35.7)Hospital mortality, n (%) 18 (42.9)
⁎ Data are expressed as mean (SD).† Echocardiogram performed in 26 out of 42 patients.
the Mantel-Haenszel log-rank test. P b .05 was considered statisticallysignificant for all comparisons. Statistical analyses were performedusing SPSS (version 12; SPSS Inc, Chicago, IL).
3. Results
A total of 42 patients were included in the analysis. Epidemiologicresults were as follows: predominance of men (64.3%); mean age was61.8 ± 15.9 years; cases of septic shock were predominant (69%).Positive blood cultures were obtained in 17 patients (40.5% of thecases). The most frequent initial infectious focus was abdominal(48%), followed by respiratory (17%). Infections were communityacquired in almost 70% of the cases. Severity scores upon ICU admissionwere 44.6± 16.1 and 7.1± 3.4 points in SAPS II and SOFA, respectively.Besides, 28-day mortality was observed in 15 patients (35.7%), all ofthem in the septic shock group. Five out of 26 patients (19.2%) wereclassified as having cardiac dysfunction by EF less than 45% (see popula-tion characteristics in Table 1).
Table 2 presents differences in fluid balance and variables betweensurvivors and nonsurvivors. No age, sex, SOFA score, creatinine, lactate,venous saturation of O2 (SatvO2), and troponin T differences were re-ported upon admission between survivors and nonsurvivors. However,higher SAPS II score was observed in nonsurvivors (52.5 ± 15.4 vs 40.2± 14.9, P= .016). Nonsurvivors also showed higher accumulated posi-tive fluid balance at 48, 72, and 96 hours with significant differences.
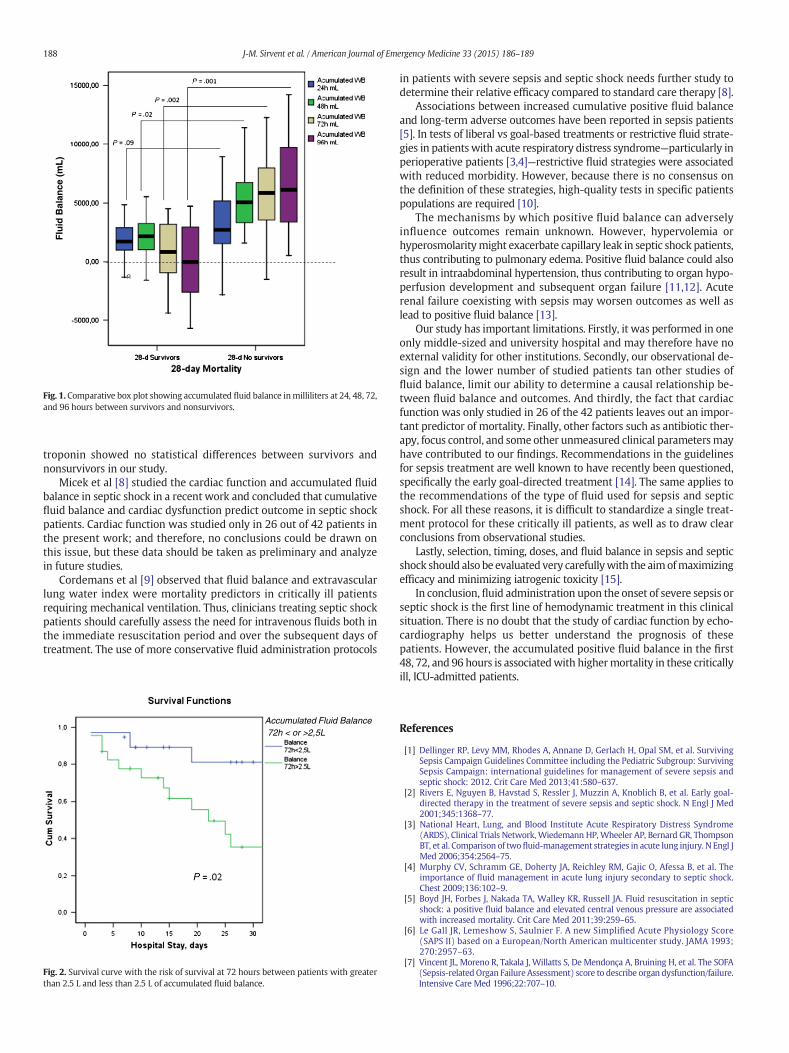
Fig. 1 shows a box plot with the greater daily accumulated fluidbalance inmilliliters at 48, 72, and 96 hours in nonsurvivors, with statis-tically significant differences. Fig. 2 shows the survival curve with therisk of survival at 72 hours between patients with greater than 2.5 Land less than 2.5 L of accumulated fluid balance, compared by log-ranktest with significant differences (P = .02).
4. Discussion
Our observational study shows that the accumulated positive fluidbalance at 48, 72, and 96 hours is associated with higher mortality inICU-admitted patients with sepsis or septic shock.
These results are consistent with those by Boyd et al [5], whoshowed that higher positive fluid balance in resuscitation over thefirst 4 days was associated with increased risk of mortality in septicshock patients. Other factors such as creatinine, lactate, SatvO2, and
Flu
id B
alan
ce (
mL
)
Fig. 1. Comparative box plot showing accumulated fluid balance inmilliliters at 24, 48, 72,and 96 hours between survivors and nonsurvivors.
188 J-M. Sirvent et al. / American Journal of Emergency Medicine 33 (2015) 186–189
troponin showed no statistical differences between survivors andnonsurvivors in our study.
Micek et al [8] studied the cardiac function and accumulated fluidbalance in septic shock in a recent work and concluded that cumulativefluid balance and cardiac dysfunction predict outcome in septic shockpatients. Cardiac function was studied only in 26 out of 42 patients inthe present work; and therefore, no conclusions could be drawn onthis issue, but these data should be taken as preliminary and analyzein future studies.
Cordemans et al [9] observed that fluid balance and extravascularlung water index were mortality predictors in critically ill patientsrequiring mechanical ventilation. Thus, clinicians treating septic shockpatients should carefully assess the need for intravenous fluids both inthe immediate resuscitation period and over the subsequent days oftreatment. The use of more conservative fluid administration protocols
Accumulated Fluid Balance72h < or >2,5L
Fig. 2. Survival curve with the risk of survival at 72 hours between patients with greaterthan 2.5 L and less than 2.5 L of accumulated fluid balance.
in patients with severe sepsis and septic shock needs further study todetermine their relative efficacy compared to standard care therapy [8].
Associations between increased cumulative positive fluid balanceand long-term adverse outcomes have been reported in sepsis patients[5]. In tests of liberal vs goal-based treatments or restrictive fluid strate-gies in patients with acute respiratory distress syndrome—particularly inperioperative patients [3,4]—restrictive fluid strategies were associatedwith reduced morbidity. However, because there is no consensus onthe definition of these strategies, high-quality tests in specific patientspopulations are required [10].
The mechanisms by which positive fluid balance can adverselyinfluence outcomes remain unknown. However, hypervolemia orhyperosmolaritymight exacerbate capillary leak in septic shock patients,thus contributing to pulmonary edema. Positive fluid balance could alsoresult in intraabdominal hypertension, thus contributing to organ hypo-perfusion development and subsequent organ failure [11,12]. Acuterenal failure coexisting with sepsis may worsen outcomes as well aslead to positive fluid balance [13].
Our study has important limitations. Firstly, it was performed in oneonly middle-sized and university hospital and may therefore have noexternal validity for other institutions. Secondly, our observational de-sign and the lower number of studied patients tan other studies offluid balance, limit our ability to determine a causal relationship be-tween fluid balance and outcomes. And thirdly, the fact that cardiacfunction was only studied in 26 of the 42 patients leaves out an impor-tant predictor of mortality. Finally, other factors such as antibiotic ther-apy, focus control, and some other unmeasured clinical parametersmayhave contributed to our findings. Recommendations in the guidelinesfor sepsis treatment are well known to have recently been questioned,specifically the early goal-directed treatment [14]. The same applies tothe recommendations of the type of fluid used for sepsis and septicshock. For all these reasons, it is difficult to standardize a single treat-ment protocol for these critically ill patients, as well as to draw clearconclusions from observational studies.
Lastly, selection, timing, doses, and fluid balance in sepsis and septicshock should also be evaluated very carefullywith the aimofmaximizingefficacy and minimizing iatrogenic toxicity [15].
In conclusion, fluid administration upon the onset of severe sepsis orseptic shock is the first line of hemodynamic treatment in this clinicalsituation. There is no doubt that the study of cardiac function by echo-cardiography helps us better understand the prognosis of thesepatients. However, the accumulated positive fluid balance in the first48, 72, and 96 hours is associatedwith highermortality in these criticallyill, ICU-admitted patients.
References
[1] Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach H, Opal SM, et al. SurvivingSepsis Campaign Guidelines Committee including the Pediatric Subgroup: SurvivingSepsis Campaign: international guidelines for management of severe sepsis andseptic shock: 2012. Crit Care Med 2013;41:580–637.
[2] Rivers E, Nguyen B, Havstad S, Ressler J, Muzzin A, Knoblich B, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med2001;345:1368–77.
[3] National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome(ARDS), Clinical Trials Network, Wiedemann HP,Wheeler AP, Bernard GR, ThompsonBT, et al. Comparison of twofluid-management strategies in acute lung injury. N Engl JMed 2006;354:2564–75.
[4] Murphy CV, Schramm GE, Doherty JA, Reichley RM, Gajic O, Afessa B, et al. Theimportance of fluid management in acute lung injury secondary to septic shock.Chest 2009;136:102–9.
[5] Boyd JH, Forbes J, Nakada TA, Walley KR, Russell JA. Fluid resuscitation in septicshock: a positive fluid balance and elevated central venous pressure are associatedwith increased mortality. Crit Care Med 2011;39:259–65.
[6] Le Gall JR, Lemeshow S, Saulnier F. A new Simplified Acute Physiology Score(SAPS II) based on a European/North American multicenter study. JAMA 1993;270:2957–63.
[7] Vincent JL, Moreno R, Takala J, Willatts S, De Mendonça A, Bruining H, et al. The SOFA(Sepsis-relatedOrgan FailureAssessment) score to describe organ dysfunction/failure.Intensive Care Med 1996;22:707–10.
189J.-M. Sirvent et al. / American Journal of Emergency Medicine 33 (2015) 186–189
[8] Micek ST, McEvoy C, McKenzie M, Hampton N, Doherty JA, Kollef MH. Fluid balanceand cardiac function in septic shock as predictors of hospital mortality. Crit Care2013;17:R246.
[9] Cordemans C,De Laet I, VanRegenmortelN, SchoonheydtK, DitsH, HuberW, et al. Fluidmanagement in critically ill patients: the role of extravascular lung water, abdominalhypertension, capillary leak, andfluid balance. Anaesth Intensive Care 2012;2(Suppl. 1).
[10] Corcoran T, Rhodes JE, Clarke S, Myles PS, Ho KM. Perioperative fluid managementstrategies inmajor surgery: a stratifiedmeta-analysis. Anesth Analg 2012;114:640–51.
[11] Myburgh JA. Fluid resuscitation in acute illness-time to reappraise the basics. N EnglJ Med 2011;364:2543–4.
[12] Ke L, Ni HB, Sun JK, Tong ZH, Li WQ, Li N, et al. Risk factors and outcome of intra-abdominal hypertension in patients with severe acute pancreatitis. World J Surg2012;36:171–8.
[13] Payen D, de Pont AC, Sakr Y, Spies C, Reinhart K, Vincent JL, SOAP investigators. Apositive fluid balance is associated with a worse outcome in patients with acuterenal failure. Crit Care 2008;12(3):R74.
[14] Coen D, Cortellaro F, Pasini S, Tombini V, Vaccaro A, Montalbetti L, et al. Towards aless invasive approach to the early goal-directed treatment of septic shock in theED. Am J Emerg Med 2014;32:563–8.
[15] Myburgh JA, Mythen MG. Resuscitation fluids. N Engl J Med 2013;369:1243–51.