links between macro economics and health in the southeast
TRANSCRIPT

1
Links Between MacroEconomics and Health inthe Southeast Asian (SEA)
Region - A Framework
Abusaleh ShariffNational Council of Applied Economic Research
11, I.P. Estate, New Delhi-110 002
August 18, 2003
© World Health Organization, 2003. All rights reserved.

2
Scheme of Presentation
� Introduction and Objectives� SEAR - Country Profile� Linkage Between Health and Economic
Development� Investment in Health �Public investments Own resources �Public-Private Partnership �Rich & Poor Country Compact� Health Accessibility and Growth

3
SEAR - Study Area
� WHO Southeast Asian Region -10 Countries� Less Developed
– Bangladesh, Bhutan, Maldives, Myanmar andNepal
� Relatively Developed– Thailand, Indonesia, DPR Korea, India and Sri
Lanka

4
Objectives� Monetary and Physical Investment in primary care
essential to achieve HEALTH FOR ALL� High incidence of preventable diseases � disease
profile and assess health deficits in SEAR� Profile of Health Spending and linkages with state of
health� Identify mechanism to enhance the health coverage of
the poor� WTO linked globalization � TRIPS & GATS �
Impact on price and availability of Drugs and Medicines

5
Salient Features of SEAR
0
1
2
3
4
5
6
C o unt rie s
Po pulat io n Gro wth To tal Fertility rate (b irths p er woman)
01 02 03 04 05 06 07 08 09 0
1 00
C o unt rie s
Po p ulat io n with acces s to safe d rinking water Po p ulat io n with acces s to ad eq uate sanitat io n (%)

6
Salient Features of SEAR
0
20
40
60
80
1 00
C o unt rie sLive Bir t hs At t e nde d by t ra ine d pe rsonne lWome n of c hildbe a ring a ge using c ont ra c e pt ive s
0
10
20
30
40
50
60
70
80
90
100
Bang
lades
h
DPR
Kor
ea
Indi
a
Indo
nesia
Mald
ives
Mya
nmar
Nep
al
Sri L
anka
Thail
and
Countries
Adult literacy Rate (2001)Life Expectancy at birth (2001)Infant Mortality Rate (2001)

7
Millennium Development Goals
� Unparalleled importance to Health– 8 Goals, 18 Targets, and 48 Indicators– Health related - 3 Goals, 8 Targets and 18
Indicators - Centrality of Health in MDGs� Health Goals by 2015:
– Reduction of U-5 Mortality by two-thirds– Reduction of MMR by three quarters– Reversing the spread of diseases, especially
HIV/AIDS and malaria.

8
Assessment of MDGs� Mixed Results
– No reversals of MDG indicators in SEAR while lastyear was of many reversals globally
– Good performance by Bangladesh, Bhutan andIndonesia in reducing U-5 mortality rates.
– Moderate performance in DPR Korea, Malaysia andThailand.
– Myanmar's progress in U5 has been not satisfactory– Thailand excelled in preventing the spread of
HIV/AIDS by more than 80 % since early 90’s– Sri Lanka’s achievement on life expectancy front is
especially commendable.� Sub-national level, inter-group disparities and gender
inequalities are all over, especially so in India

9
Direct and Indirect Costs ofill-Health
� Reduction in DALYs� Acute physical pain and suffering.� Increasing medical expenses and contraction
of other essential expenditures.� Loss of valuable work-hours due to disability
and life-years arising out of death.� Loss of personal income and national income
as well.

10
Direct and Indirect Costs ofill-Health
� impoverishment of the household due toreduced income and increasing expenditure.
� Under-investment in children’s education andother basic requirement
� Additional pressure on public funds andgovernment allocations under stress.
� Reduction in sources of resource mobilization(lower number of tax payers).

11
Longevity, Health andDevelopment
Longitivity
Investments
Income
Savings
EconomicGrowth

12
Cost to Firms
� Continuing disease Episodes affectProductivity� productivity of firms
� Firms encounter increase cost of production� Lower and falling profits � fall in National
Income� Better health of labour force improves firms
capacity to compete in international biddingprocess

13
Role of Health inEconomic Development
� High and advanced qualities of Health and educationtrigger economic development from high levels.
� Essential � that ill health aggravates poverty ratherthan adhering to the view � that poverty accentuatesconditions of ill health.
� Healthy individuals are more productive and live longerto generate high levels of income.
� Sri Lanka - a reduction in malaria from its endemiclevels during the second half of 1970s, contributed to a9 percent increase in GDP.

14
Role of Health inEconomic Development
� Persistent episodes of ill health diminishes thereturns to business and infrastructure investments.
� Childhood sickness � disability in adulthood,explains one way in which the quality of futurestock of capital is adversely effected.
� Health is a cause rather than a fallout of economicdevelopment.
� Europe, Britain & Japan rapid growth during industrial revolution was supported by the existence of advanced health gains and standards.

15
Health SpendingNational health spending: sources and uses (per cent)
SourceCentral
Govt.State &
Local Govt.Corporate
3rd PartyHouseholds Total
Uses Primary Care 4.3 5.6 0.8 48.0 58.7 Secondary & Tertiary Inpatient Care
0.9 8.4 2.5 27.0 38.8
Nonservice Provision 0.9 1.6 NA NA 2.5 Total 6.1 15.6 3.3 75 100Source: World Bank (1995b).
16
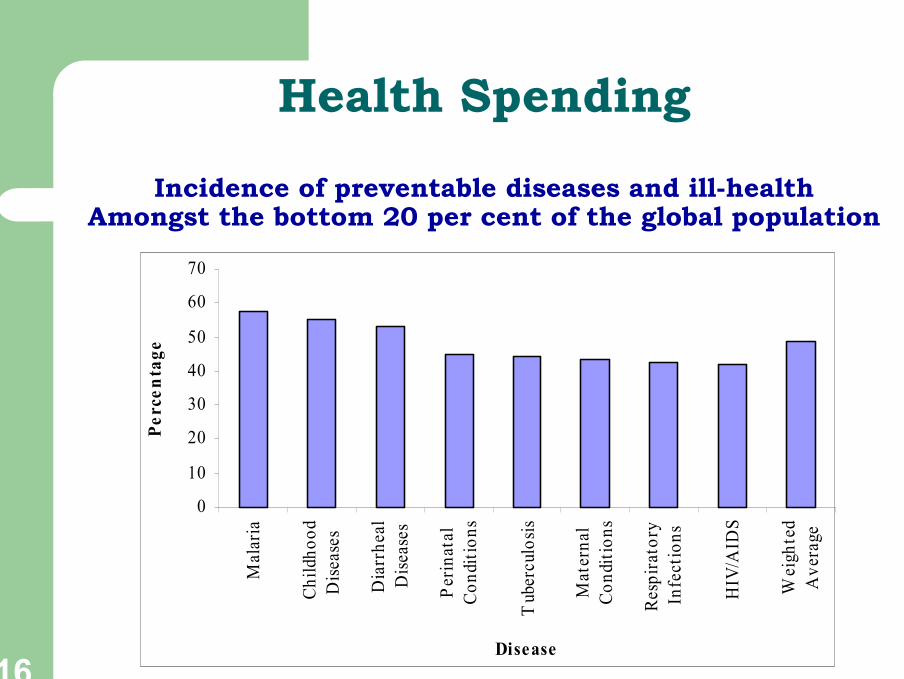
Health Spending
Incidence of preventable diseases and ill-healthAmongst the bottom 20 per cent of the global population
0
10
20
30
40
50
60
70M
alar
ia
Child
hood
Dise
ases
Dia
rrhe
alD
iseas
es
Perin
atal
Cond
ition
s
Tub
ercu
losis
Mat
erna
lCo
nditi
ons
Resp
irato
ryIn
fect
ions
HIV
/AID
S
Wei
ghte
dA
vera
ge
Disease
Perc
enta
ge

17
Health Spending
� Health (Public) expenditures should be directed towardsdiseases of the poor � Cost Effective.
� Differentiate Primary (public) health care, Essentialclinical services � PUBLIC GOOD vCurative Care � PRIVATE GOOD
� CMH Report � an investment of $4 for public healthand $8 for clinical services are capable of achieving areduction of over 32% of all DALYs amounting to 226million years of DALY in low income countries.
18
Health Spending
� Cost Efficient expenditures benefiting masses.� A total cost per capita worth $15 will reducethe disease burden by 25% or 301 millionDALYs in less developed countries
� Prevailing per capita health expenditures in SEAR arequite low.– Eg. Bangladesh 1.6 per cent of GDP in 1996-98.– In India it is less than 2 per cent and in Nepal less
than 1%.
19
Public Expenditures on healthEssential so is Public-Private
Compact� The significance of the presence of
government in the health sector is tenfold:– health being a public good is subject to market
failure and problem of free riding, which can beresolved by the government.
– financial risk coverage is provided by thegovernment in times of crisis, especially to the poor.
� Promote Public - Private Compact �especially in insurance, production of drugs andmedicines, and training

20
WTO, Globalization and TRIPS� The era of globalization has added to the disease
burden of the people in region under study andsimultaneously broadened the horizons of reducing it.
– disease related to HIV/AIDS, tobacco intake have escalateddue to enhanced economic activities effecting the behavioralpattern of the masses.
– emphasis has been laid on R&D as a means to improve thequality of health care.
� The WTO lead TRIPS and GATS � will they improveavailability of drugs in low income countries? Not Clear
– the low income countries have been more hurt than benefiteddue to the patenting of processes and products related topharmaceuticals, having to pay higher prices.

21
Public-Private Compact
� Weak Public Institutions, lack of resources, poormanagement, and low accountability- Public Provision ofHealth Care � not a enduring solution.
� Experience of Developed countries suggest-basic healthservices should be comprehensively provided by thestate early on, followed by more targeted interventions,and then public-private partnership.
� Recent household surveys of many countries around theworld indicate private providers play a significant role inhealthcare delivery, even to the poor.

22
Public-Private Compact
� Reviews of disease control and child andreproductive health programs have similarly foundthat the private sector will prove to be a contributingfactor in controlling the burden of disease in theSEA region.

23
Public-Private Compact
� Some of the ways to improve the quality ofservices poor patients receive –
– Government can ‘contract / ‘purchase’ from private sources foridentified poor.
– Government may focus their contacting and funds on diseasesthat disproportionately affect the poor, or on services of criticalimportance to the poor such as MCH, family Planning services.
– Improving the health insurance facilities so that the people arenot forced to pay out of their pocket at the time of need.
– Enhancing quality regulations and professional ethics toinformal providers located in rural areas or slums.
– ‘Community financing’ by pooling its own resources and thatwould mainly cover basic curative health services other thanthe package of essential interventions.

24
Rich and Poor Country Compact� High-income donor countries- helping the low-
income countries pursue their health objectivesand bridge the existing gap in health financing.
� Millennium Development Compact: Top andHigh Priority Countries can’t wait untileconomic growth- rather they need largeinjections of donor financing.
� Financing on the eradication of diseases is notthe only objective- A rigorous R & D initiativehas to be undertaken by the donor countries-would help to achieve a healthy world.
25
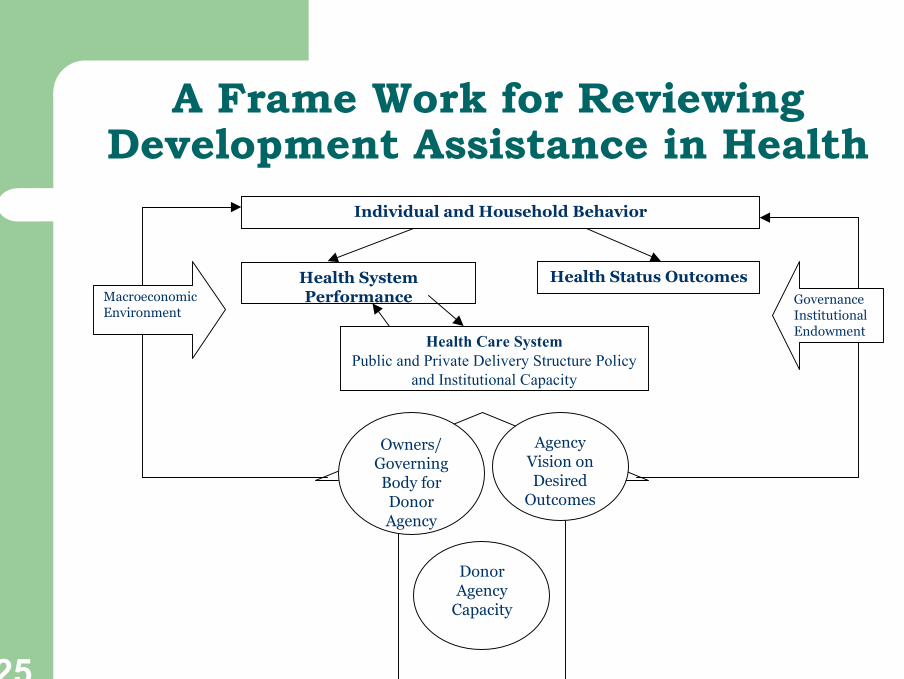
A Frame Work for ReviewingDevelopment Assistance in Health
Individual and Household Behavior
Health SystemPerformance
Health Status Outcomes
Health Care SystemPublic and Private Delivery Structure Policy
and Institutional Capacity
Owners/GoverningBody forDonorAgency
AgencyVision onDesired
Outcomes
DonorAgency
Capacity
GovernanceInstitutionalEndowment
MacroeconomicEnvironment

26
Rich and Poor Country Compact
� Developmental Assistance for Health (DAH): Governments with taxpayer’s money are the fundamental source- delivered through publicagencies in the aid receiving countries.
� 47% of DAH allocated to countries that spend less than US$20 percapita on health and about 28% to those spending less than US$40per capita. The overall amounts of DAH are very small, amounting toless than US$1per capita even in countries with low totalexpenditures.
� Overall international donations grew to US$679 million in 2000, withabout US$109 million or 16% allocated for health purposes of alltypes.
� DAH � objectives have shifted from single purpose efforts toexpanding health system capacity and strengthen national healthpolicy framework through systemic reforms.

27
Rich and Poor Country Compact
Diseases Support(in million
US$)
Percentage
HIV/AIDS includingsexually transmitted disease
337 20
Vaccine preventablechildhood disease
250 15
Maternal and prenatalconditions
180 10
Malaria 87 5 Tuberculosis 81 4.5 Non communicablediseases
47 3
Disease and Health Sub-Sector Specific DonorFunding
Source: summarized from p17 of the Report of the Working Group 6 ofthe CMH.

28
Rich and Poor Country Compact
� As trading partners it is beneficial to donor countries toprotect the interest of low cost labour force in low-income countries.
� Monterrey Consensus of Millennium Declaration:developed countries that have not done so to makeconcrete efforts towards the target of 0.7 per cent ofGNP as official development assistance (ODA) todeveloping countries � as opposed to only 0.15 -0.20 per cent.
� ODA @ 0.7 per cent of GNP � aid would be $165billion a year that is three times the current level andadequate to achieve Millennium Development Goals.

29
Health Access to the Poor
� Donors reluctant due to absence of dependableassurance that funds are spent prioritized sectors andand that transparent monitoring and evaluationmechanisms are put in place to assist the sustainability inoutside funding.
� Recipient countries to evolve implimentative platforms,institutions, procedures and inventory control systemsthat bring utmost amounts of transparency andaccountability.� It is important that creditable output measures are
agreed upon to undertake annual or regular evaluationof the programs being implemented.

30
Health Access to the Poor
� Increasing Physical Access to Servicesessential
� Increase number of health centres and small health posts in rural areas. � Improve Outreach � regularly visiting health workers to distant villages to provide preventive and promotive care is a simple but effective means of increasing the coverage of services for the poor.� Providing adequate travel allowances and other
incentives can act as a powerful motivation for healthworkers to visit the remote areas regularly.

31
Health Access to the Poor� Increasing the Resources Available for Health
Facilities Frequented by the Poor– Identify key public health services relevant for the poor.
– Decentralized provisioning and involvement of thecommunity creates the possibility of mobilizingadditional resources for the health sector at the locallevel.
– Carefully planned user-fee and cost recoverymechanism
– Attempt health risk pooling through social healthinsurance schemes � not easy but high returns ifsucceeded.

32
Health Access to the Poor
� An important means for improving the health ofthe poor is to regularly measure the extent towhich they benefiting from health services.
� Since most governments in this region arelikely to continue their role as health provider,the strategy should involve identifying ways toimprove the quality and efficiency of thegovernment health services so that poor canoptimize their use of these services.