level one screen training september, 2014 level one... · user access is limited by agency, ... to...
TRANSCRIPT
INTRODUCTION TO THE LEVEL ONE SCREEN OCTOBER 2014 Department of Health and Mental Hygiene – Devon Mayer Department of Aging – Teja Rau

Overview
1. Background 2. About the Screen 3. Pilot testing in Maryland 4. Administering the Screen 5. Policy Considerations 6. Implementation and Follow up

1. BACKGROUND

Balancing Incentive Program
Shifting priority from nursing facilities to community-based services Balancing Incentive Program States must increase spending on community-based long term
services and supports to at least 50% Funding
States get time-limited increased federal match on community-based LTSS and
Increased federal match must be reinvested into services Required structural changes under BIP
1. No Wrong Door/Single Entry Point Maryland Access Point 2. Core Standardized Assessment Level One Screen and interRAI 3. Conflict-Free Case Management

Why are MAP sites performing the Screen?
MAP is the Single Entry Point to community Medicaid services in Maryland’s No Wrong Door System.
Built on the strength of existing, community-level agencies that are known and trusted to populations served.
MAP is the only local agency authorized to complete the Screen.
Money Follows the Person and BIP have funded: Statewide MAP toll-free number Staffing support at MDoA MAP website MAP expansion grants Marketing and outreach Level One screen-pilot and tracking system development

What is interRAI?
International non-profit organization whose members are professionals and researchers from 30 different countries.
Developed a suite of evidence-based instruments and tools that are tested for reliability and validity.
http://interrai.org Maryland is using the interRAI:
Level 1 Screen to be performed by MAP staff Home Care Assessment performed by AERS

Core Standardized Assessment
Valid, reliable tool used in 23 states and numerous
countries including Canada, most of Western Europe, and Australia
interRAI collects and analyzes the data from the assessments in order to conduct continuous quality improvement
interRAI has developed a screen and its corresponding algorithm as part of their research
2. About the Screen

What does the Screen do?
The screen helps determine: Service Needs Likelihood of meeting a nursing facility level of care Risk of institutionalization Referral recommendations

How was the Screen Developed?
Subset of questions from the interRAI-Home Care
Based on a scientifically derived algorithm Used interRAI’s algorithm that determines risk of
institutionalization and overlaid it with Maryland-specific level of care criteria
Maryland materials include:
South Dakota’s “Item by Item Guide” New Jersey’s “Item Definitions and Coding”

Where will the Screen live? Online LTSSMaryland Tracking System
MAP staff will use the LTSS Maryland Tracking System to administer the Level One Screen
Web-based tracking system with a daily exchange of information with MMIS.
The tracking system coordinates the eligibility process for: Community Options Waiver Community First Choice Medical Assistance Personal Care Brain Injury Waiver Money Follows the Person-Peer Outreach, Options Counseling,
Developmental Disabilities

LTSSMaryland Tracking System, cont.
User access is limited by agency, jurisdiction, client assignment. Administrator – ideal for supervisors and managers Intake – ideal for I&A staff, MAP-OC Staff – ideal for staff only administering Screen as referred
The system is HIPAA and 508 Compliant
It was built on a platform that allows for additional modules to be added on in the future Next steps are under way to add Medical Day Care Waiver

Screen Logistics
31 questions Average time to complete is between 15-23 minutes
May take longer if a translator is required.
Can be administered over the phone or in-person Can be used with family caregivers, although it is
preferred that the individual participate as well.
Screen Structure 14
Usually 3 day look back (“In the past three days, have you…”) Consider this when administering screen on persons
newly discharged from a hospital or rehab setting.
Four types of items: Ability—could person have done task? Performance—did person do task? Conditions/symptoms—did person have or display? Other—environment, supervision

All Persons
Interest and Info
Assist & Referral
Low Risk
Moderate Risk
High Risk
No
No
No
No
Yes
Yes
Yes
Yes
Screen Logic
3. Pilot Testing in Maryland
Pilot Testing in Maryland
2 pilots held in 2013 Current participants New callers to AAAs
Anne Arundel Baltimore City Baltimore County Calvert Carroll Cecil Charles
Harford Howard MAC Queen Anne’s USA Washington Worcester

• Total screens completed by MAP staff 250 • People who received a Screen and went on to a AERS-
administered interRAI Home Care Assessment (replaced STEPS) 184/250 • Level 4 – moderate risk level • 32%. 80/250 • Level 5 – high risk level • 26.4% 66/250 • Level 3 – low risk level • 20% 50/250 • Level 1 – interest and information. • 13.2% 33/250 • Level 2 – assistance or referral • 8.4% 21/250
Pilot Summary

Screen Categories and Level of Care
Total Level 1 -
Interest and Information
Level 2 - Assistance or Referral
Level 3 - Low Risk
Level 4 - Moderate
Risk
Level 5 - High Risk
n % n % n % n % n % n %
Total Number of People 250 100.00 33 13.20 21 8.40 50 20.00 80 32.00 66 26.40
Nursing Facility Level of Care Determination*
Yes 83 45.11 3 13.04 1 6.67 12 31.58 28 49.12 39 76.47
No 95 51.63 19 82.61 14 93.33 24 63.16 26 45.61 12 23.53
Clinical Review 6 3.26 1 4.35 0 0.00 2 5.26 3 5.26 0 0.00
Pilot Summary, cont.
Hilltop Institute analyzed the results Each of the respondents had both the telephone screen
and an interRAI in order to analyze the results across both tools
Each telephone screen respondent was grouped into one of five levels
Each interRAI assessment respondent was assessed for nursing facility level of care (NF LOC)

Pilot Results
The average length of call was 23 minutes
Reasons MAP staff gave for administering the screen: Sense the need for long term services and supports
Need help with ADLs
Recent diagnosis of disease/illness
Bringing a family member home from hospital or NF
Crisis situation
Nearly half of respondents with a full interRAI assessment met Nursing Facility Level of Care criteria
Nursing Facility Level of Care tracked predictably across the telephone screen risk levels, with over 75 percent of individuals in Level 5 meeting Nursing Facility Level of Care criteria
The average number of activities of daily living (ADLs) and instrumental activities of daily living (IADLs) needing more than supervisory assistance tracked predictably across levels, with individuals in Level 5 needing the most assistance
GOAL: By marketing and strengthening the MAP single-entry point system, we can triage people into programs and target use of public resources more effectively
4. Screen Administration
Where does the Screen fit in?
1. CONTACT: Individuals contact the MAP or are referred from another agency/organization 2. TRIAGE: MAP staff triage for those seeking LTSS information 3. MAP staff person conducts Level One Screen 4. OPTIONS COUNSELING: Identify person’s goals, formal and informal supports and
resources, and educates consumer on various programs a) Provide Options Counseling and use information from Screen to guide individual in identifying and setting
goals, planning, and referrals
5. MEDICAID PROGRAMS: a) Waiver Registry: Add individual to registry by submitting completed Screen. b) Financial questions on Screen will provide high-level eligibility determination for Medicaid services. c) Submitting a completed Screen for those eligible for Medicaid programs and scoring at a high risk for
institutionalization may prompt a referral to an AERS interRAI assessment and starts the CFC/MAPC eligibility determination process
d) MAP staff provides support planning agency (SPA) information packets for those eligible for CFC/MAPC
6. NON-MEDICAID PROGRAMS a) May be part of Options Counseling planning and assistance with accessing programs b) Pending MDoA Workgroup: Use information from Level 1 Screen to determine eligibility and gather data.
7. Additional OC may be provided thereafter, as appropriate, if person is ineligible for Medicaid programs.
8. FOLLOW UP, as needed

Person contacts MAP and asks a question or tells their story.
MAP Staff completes the Level One Screen
Once the screen is completed, the person can be added to the registry. Registry to be maintained by date
screened and risk of institutionalization. MA-eligible individuals can be referred to CFC/MAPC
When a Medicaid program is able to provide a service, the person will receive an interRAI-Home Care assessment
MAP staff has access to LTSSMaryland to follow the process and provide updates to the person if they call back.
Answer brief questions
Make initial referrals (e.g., behavioral health, VA,
traumatic brain injury)
Provide MAP Options Counseling and develop Action Plan
Trigger responses: The person needs personal assistance, has stated he/she has functional deficiencies,
or may move because of physical needs.

Before you begin: Considerations when using the Screen
Become familiar with the subject areas and questions
The screen is to be administered as a conversation, not a scripted series of questions
Set a welcoming tone and convey openness
The Screen may come up after an initial opening
conversation with the person where he or she has already related some of their concerns, goals, and needs.

Introduce the Screen
Sample Introduction I’d like to have a conversation with you to find out how you
do everyday tasks and to learn more about your health. This will take about fifteen minutes.
It’s important that you tell me how things really are going for you, as accurately as possible, so I can make sure you get the kind of assistance that will best meet your needs.
Would you like to have other family members participate in this conversation? We can have this conversation in-person or over the phone. Which do you prefer?
Considerations when using the Screen (cont’d)
Ask if the person would like to conduct the screen face-to-face or with family/others present
Let the person tell their story and prompt them in Screen areas they don’t cover
Listen for underlying issues and concerns Example: Example: Caller requests information about meals
at local senior center and during conversation staff believes person may need assistance with ADLs.
If the person has communication challenges or cognitive issues, it is appropriate to administer the screen to their main helper. When using the screen with the main helper, it is preferable to
include both in the conversation.
When to administer the screen?
The caller needs assistance performing ADLs Multiple or complex needs
The caller indicates they may need to move from their current living situation because of increased need
The caller requests it The caller wants to be added to the registry The caller may benefit from Medicaid community
programs (CFC, MAPC, waiver) As part of MAP Options Counseling, to gather information
to explore formal and informal supports and services. The MAP staff believes it would benefit the caller

What about non-Medicaid clients?
Part of the Screen results includes a high-level determination of financial eligibility for Medicaid community long term care programs.
The Screen may be administered on people accessing non-Medicaid programs. Part of Options Counseling to gather more information to
develop a plan Determine referrals MDoA workgroup development: Triage and determine
eligibility for Senior Care, SALGHS, Congregate Housing MAP staff should contact AERS separately to request
assessments for non-MA clients.
Adding Individuals to the Registry
1. The complete screen will calculate a result from 1-5. 5- High Risk priority to apply for waiver slots when available 4- Moderate Risk 3- Low Risk 2- Assistance and Referral 1- Interest and Info default score for incomplete submitted Screens
2. Individuals can be added to the registry without completing the screen, but they will be placed in the lowest priority category (1)
3. The registry will be ranked first on priority category, then date order will be followed:
An person calling today who is screened as a Category 5 will have priority over individuals in other categories who were already on the registry

Multiple Screen Scores
The Tracking System keeps a record of all Screen scores that are administered and submitted.
The Screen may be administered multiple times on the same person.
There is a pop-up notice if the Screen has been administered more than once in 90-days. You can still administer the Screen if appropriate.

Bypassing the Screen?
What if a person goes directly to the health department for an assessment?
1. Cannot be placed on the waiver registry 2. Misses out on understanding about Medicaid
programs, potential eligibility. 3. Does not get Options Counseling/assistance planning
and navigating

5. Policy and Other Considerations
Limits to Screen
The Screen will never be perfect People may over/underestimate their ability to
perform ADLs, IADLs which could result in: Individuals that are referred on for the interRAI assessment
that won’t meet NF LOC Individuals that are not referred for the assessment, but do
meet LOC
People may disagree with the results of the screen People may request to repeat the screen until they get the
results they want.

Benefit to Caller
Medicaid-eligible individuals can be directly referred to CFC or MAPC through the tracking system Includes referrals for a Supports Planner and AERS referral
Individuals can request to be added to the registry in date order, based on risk of institutionalization
The results will trigger referral recommendations Callers can receive information on the services they may
be eligible for Callers will have a better idea of likelihood of receiving
services, including time frames. This information can help in the Options Counseling process to help plan for the future based on their current available resources.
Benefit to MAP Staff
Staff will be able to see if caller has previously been screened in another county
Staff will be able to view current Medicaid program enrollment, including coverage groups, and supports planner, if assigned
Results can be used during Options Counseling MAP staff will have a clearer sense of when to
refer someone for an AERS assessment

Benefit to State
Community-Medicaid eligible individuals can be directly referred to HCBS from MAP sites, decentralizing the referral process. State staff will be freed up to focus on technical assistance,
training, and monitoring for the enrollment process. Target scarce resources (waiver slots) to those most at risk of
institutionalization MDoA is exploring the use of the screen to prioritize for
state-funded programs, alleviating the Health Departments from full assessments
Data collection can be analyzed to determine cost-effectiveness of NF diversion, proving impact of state-funded programs Makes the case for increased future funding.
IMPLEMENTATION
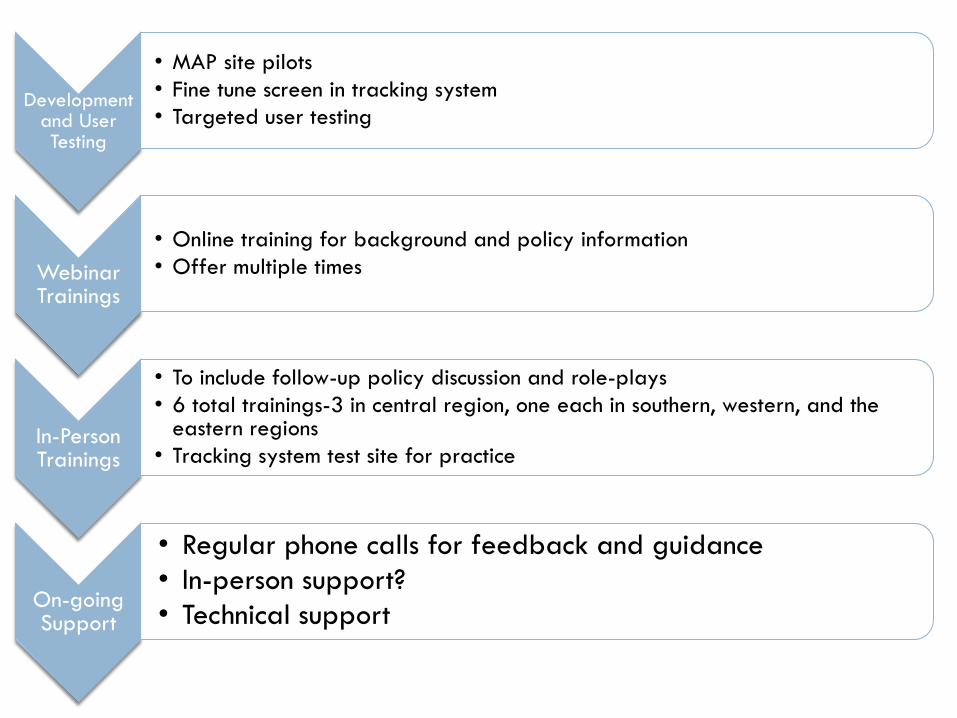
Development and User Testing
• MAP site pilots • Fine tune screen in tracking system • Targeted user testing
Webinar Trainings
• Online training for background and policy information • Offer multiple times
In-Person Trainings
• To include follow-up policy discussion and role-plays • 6 total trainings-3 in central region, one each in southern, western, and the
eastern regions • Tracking system test site for practice
On-going Support
• Regular phone calls for feedback and guidance • In-person support? • Technical support

Follow up from MAP Staff
We welcome constructive feedback on the training and materials to be used with the Screen
As with any new process, we expect the need to make changes based on your experiences after implementation
FYI-Current tracking system contract ends in October, new
contract starts November 1. No system changes are likely to be made until after the new
contract begins. MAP sites can request follow up training from DHMH/MDoA

FFP Time Study
1 FTE or 20% of your staff, whichever is more
Only staff who manage and/or provide I&A services, MAP Options Counseling, and MAP website directory maintenance can participate in the FFP time study.
Please do not include staff who provide-or spend time on case management, supports planning, and MFP-nursing facility Options Counseling.

FFP Time Study Trainings Work load and time frame: Pilot dates: October 27th to November 14th. 5-20 minutes per day depending on the activities
performed and how familiar the individual is with the coding system.
Participants will receive an email twice per day containing a link to a quick survey.

FFP Time Study: How to Sign Up
1. Attend at least one of the following trainings:
In Person: Monday, October 20th, 11:00 AM to 1:00 PM
Anne Arundel County, Independence Room
2664 Riva Road, Suite 170, Annapolis, MD 21401
In Person: Tuesday, October 21st, 1:00 PM to 3:00 PM
Havre de Grace Activity Center
351 Lewis Lane, Havre de Grace, MD 21078
Webinar: Wednesday, October 22nd, 1:00 PM to 3:00 PM
https://global.gotomeeting.com/join/205615013,
Call In: 1-(571) 317-3131, Access Code: 205-615-013
Webinar: Thursday, October 23nd, 10:00 AM to 12:00 PM https://global.gotomeeting.com/join/950930757,
Call In: 1-(408) 650-3112 , Access Code: 950-930-757
2. Sign-up for training by Monday, October 6th using the following link:
http://www.signupgenius.com/go/20f0d4aa5aa2ba4fa7-ffptime

Questions???
Additional training requests Ami Vyas, MDoA [email protected] Rebecca Oliver, DHMH-Medicaid [email protected]
Future training topic suggestions Emily Miller, MDoA – [email protected] Tiffani Nibbs, DHMH-Medicaid [email protected]
General questions or concerns about policy or the Screen Teja Rau, MDoA [email protected] Tiffani Nibbs, DHMH-Medicaid [email protected]
LTSS Tracking System Rebecca Oliver, DHMH-Medicaid [email protected]