left ventricular function in patients with atrial fibrillation before and after cardioversion
TRANSCRIPT

reactive intimal proliferation associated with the aggre- gation and organization of blood clots occurs within the aneurysm. Specific hemodynamic vessel wall-shearing stress is present at the inlet and outlet parts of the aneu- rysm, and this is said to damage endothelial cells and promote stenosis. l 3~14 However, the mechanism by which this stenosis progresses over a long period of time is still not well understood and requires further study.
We have no data concerning the long-term prognosis for children with Kawasaki disease who do not have aneu- rysms or whose aneurysms have regressed. A normal angiogram does not necessarily mean complete recovery by coronary arteries. Arterial damage may persist and there is a possibility of the risk of early arteriosclerosis as a sequela of vasculitis because of the characteristic fea- tures of panarteritis observed in this disease.15
Coronary artery bypass graft surgery was performed in all patients, and the l- to 4-year postoperative courses have been favorable. Arterial grafts, such as from the internal thoracic artery or gastroepiploic artery, which can be expected to retain good patency for a long period of time are currently recommended. However, in cases in which aneurysms are present throughout the entire length of the trunk of the coronary arteries, such as in patients 4 and 5, aneurysms may also be present in the internal thoracic artery, and when this vessel is planed to be used for grafting, it must be thoroughly evaluated to exclude presence of aneurysms preoperatively.
We believe that Kawasaki disease gives rise to long- term complications, such as aneurysms that progress to cause angina pectoris or myocardial infarction. A num- ber of the infants with Kawasaki disease currently being examined in the department of internal medicine may go
on to develop such complications in the future. Thus, long-term follow-up, including regular exercise tests and coronary arteriography, is considered important.
1. Kawasaki T, Kosaki F, Okawa S, Shigematsu I, Yanagawa H. A new infantile mucocutaneous lympho node syndrome (MLNS) prevailing in Japan. Pednxtrics 1914;54:21 l-216. 2. Kato H, Ichinose E, Yoshioka F, Takeshi T, Matunaga S, Suzuki K, Rikitake N. Fate of coronary aneurysms in Kawasaki disease. Serial coronary angiography and long-term follow up study. Am J Cardiol 1982;49:1758-1766. 3. Kamiya T, Suzuki J. Cardiovascular angiographic findings in Kawasaki dis- ease. Jpn J Pediatric Med 1985;17:765-770. 4. Nakano H, Ueda K, Saito A, Nojima K. Repeated angiograms in coronary arterial aneurysms in Kawasaki disease. Am J Cardiol 1985;56:846-851. 5. Flugelman YM, Hashin Y, Bassan MM, Lear R, Gotman SM. Acute myocar- dial infarction 14 years after an acute episode of Kawasaki disease. Am J Cardiol 1983;52:427-428. 6. Ohyagi Y, Hirose K, Tsujimoto S, Doyama K, Watanabe Y, Nakai T. Kawasa- ki disease complicated by acute myocardial infarction 9 years after onset. Am Heart J 1985;110:670-672. 7. Ishiwata S, Nishiyama S, Nakanishi S, Seki A, Watanabe Y, Konishi T, Fuse K. Coronary artery disease and internal mammary artery aneurysms in a young woman: possible sequelae of Kawasaki disease. Am Hear? J 1990;120:213-217, 8. Fujiwara H, Hamashima Y. Pathology of the heart in Kawasaki disease. Pediatrics 1978;61:1Of-107. 9. Wong CK, Cheng CH, Lau CP, Leung WH. Asymptomatic congenital core- nary artery aneurysm in adulthood. Ear Heart J 1989;10:947-949. 10. Landing BM, Larson E. Are infantile periarteritis nodosa with coronary artery involvement and fatal mucocutaneous lymph node syndrome the same? Comparison of 20 patients from Hawaii and Japan. Pediatrics 1977;59:651-662, 11. Tanaka N, Sekimoto K, Naoe S. Kawasaki disease. Relationship with infan- tile periarteritis nodosa. Arch Pathol Lab Med 1976;100:81-86. 12. Fujiwara H, Fujiwara T, Kao TC, Ohshio G, Hamashima Y. Pathology of Kawasaki disease in the healed stage. Relationship between typical and atypical cases of Kawasaki disease. Acta Pathol Jpn 1986;36:857-867. 13. Young DF, Tsai FY. Flow characteristics in models of arterial stenoses-steady flow. J Biomechnnics 1973;6:395-410. 14. Kim BM, Corcoran WH. Experimental measurements of turbulence spectra distal to stenosis. J Biomechanics 1974;7:335-342. 15. Kato H, Inoue 0, Akagi T. Kawasaki disease, cardiac problem and manage- ment. Pediatr Rev 1988;9:209-217.
Left Ventricular Function in Patients with Atrial Fibrillation Before and After Cardioversion Mahbubul Alam, MD, PhD, and Curt Thorstrand, MD, PhD
A trial fibrillation (AF) is a clinically important ar- rhythmia with important therapeutic and prognostic
implications. The disorganized electrical and mechanical activity causes loss of active atria1 contraction. This in turn results in insufficient atria1 emptying and impaired ventricular filling. l AF may be converted to sinus rhythm by means of direct-current countershock. Hemodynamic studies before and after cardioversion of AF to normal sinus rhythm report conflicting results regarding im- provement in hemodynamic function.2-4 Some studies suggested that normal atria1 contraction may not occur immediately after successful cardioversion of AF to sinus rhythm.lT3 The purpose of this study was to evaluate, using echocardiography and Doppler, the mechanical ac- tivity of the left atrium and its effect on left ventricular (LV) function after electrocardioversion of AF to sinus rhythm.
From the Department of Medicine I, Cardiology Section, Karolinska Institute at South Hospital (SMersjukhuset), 11883 Stockholm, Swe- den. Manuscript received July 16, 1991; revised manuscript received and accepted November 4,199l.
The study was begun with 19 patients with electro- cardiographic evidence of AF and without history of coronary artery disease or cardiomyopathy. The study was designedfor 1 -month follow-up. Seven patients were excluded: 5 owing to reversion to AF before the final echocardiographic examination, and 2 owing to unsuc- cessful cardioversion. Left atria1 dimension was not used as an exclusionary criterion. Thus, 12 patients (aged 57 f 9 years) were converted to normal sinus rhythm by means of direct-current cardioversion. Demographic data on the patients are listed in Table I. Digoxin was withdrawn 2 days before cardioversion. Patients were receiving anticoagulation therapy (warfarin sodium) for 12 weeks, with prothrombin time being within the thera- peutic range. Inpatients receivingsotalol medication, the drug was continued at the time of cardioversion.
Patients were examined before, and 4 hours, 2 weeks and 1 month after cardioversion. All patients underwent complete M-mode and 2-dimensional echocardiogra- phy, including pulsed-wave Doppler. An Aloka SSD- 870 echocardiographic machine with a 2.5 MHz trans-
694 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 69 MARCH 1, 1992
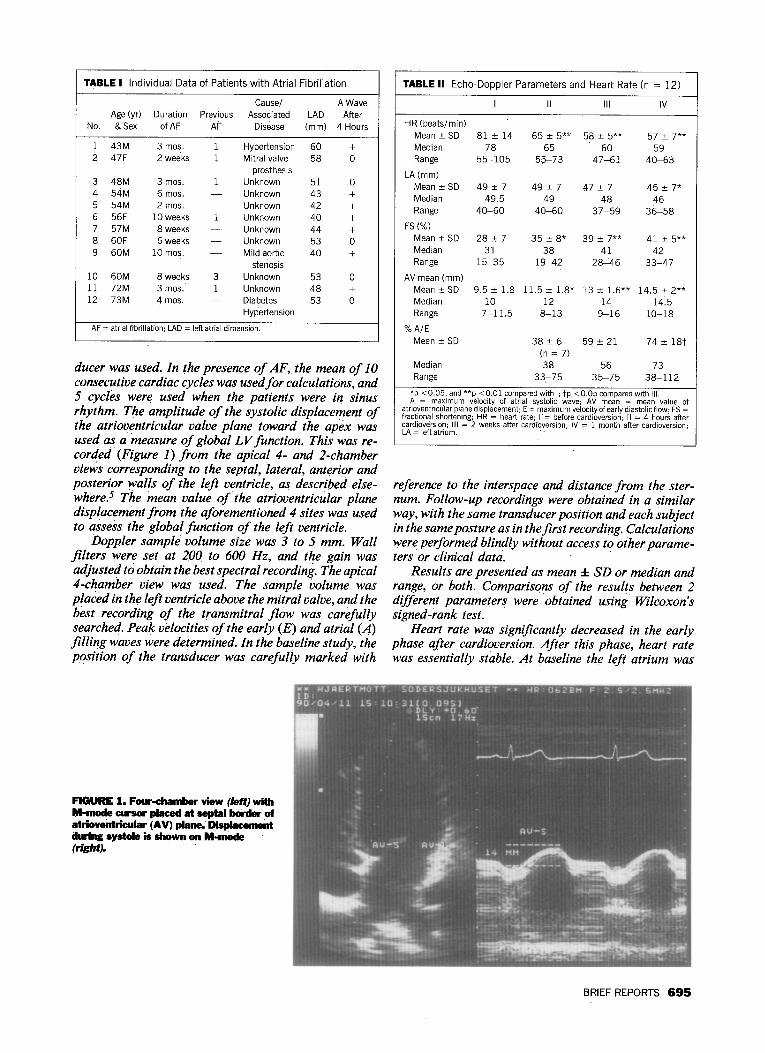
TABLE I Individual Data of Patients with Atrial Fibrillation
Cause/ A Wave Age (yr) Duration Previous Associated LAD After
No. & Sex of AF AF Disease (mm) 4 Hours
1 43M 3 mos. 1 Hypertension 60 + 2 47F 2 weeks 1 Mitral valve 58 0
prosthesis 3 48M 3 mos. 1 Unknown 51 0 4 54M 6 mos. - Unknown 43 + 5 54M 2 mos. - Unknown 42 + 6 56F lOweeks 1 Unknown 40 + 7 57M 8 weeks - Unknown 44 + 8 60F 6 weeks - Unknown 53 0 9 60M 10 mos. - Mild aortic 40 +
stenosis 10 60M 8 weeks 3 Unknown 53 0 11 72M 3 mos. 1 Unknown 48 t 12 73M 4 mos. - Diabetes 53 0
Hypertension
AF = atrial fibrillation; LAD = Matrial dimension.
ducer was used. In the presence of AF, the mean of 10 consecutive cardiac cycles was usedfor calculations, and 5 cyclks were used when the patients were in sinus rhythm. The amplitude of the systolic displacement of the atrioventricular valve plane toward the apt& was used as a measure of global LVfunction. This was re- corded (Figure I) from the apical 4- and 2-chamber vie& corresponding to the septal, lateral, anterior and posterior walls of the left ventricle, as described else- where.5 The mean value of the atrioventricuiar plane displacement from the aforementioned 4 sites was used to assess the global function of the left ventricle.
Doppler sample volume size was 3 to $ mm. Wall filters were set at 200 to 600 Hz, and the gain was adjqted to obtain the best spectral recording. The apical I&amber view was used. The sample volume was placed in the left ventricle above the mitral valve, and the b&t recording of the transmitral flow was cartifully searched. Peak velocities of the early (E) and atria1 (A) $lling waves were determined. In the baseline study, the position of the transducer was carefully marked with
- TABLE II Echo-Doppler Parameters and Heart Rate (n = 12)
I II Ill IV - -
HR (beats/min) Mean + SD 81 f 14 65 +- 5** 58 k 5** 57 * 7** Median 78 65 60 59 Range 55-105 55-73 47-61 40-63
LA (mm) Mean f SD 49 + 7 49 2 7 47 2 7 45 2 7* Median 49.5 49 48 46 Range 40-60 40-60 37-59 36-58
FS (%) Mean f SD 28 2 7 35 + 8* 39 k 7** 41 t 5** Median 31 38 41 42 Range 15-35 1942 28-46 33-47
AV mean (mm) Mean 2 SD 9.5 k 1.8 11.5 -t 1.8” 13 2 1.6** 14.5? 2** Median 10 12 14 14.5 Range 7-11.5 8-13 9-16 lo-18
%A/E Mean + SD 38 * 6 59 + 21 74 f 18t
(n = 7) Median 38 56 73 Range 33-75 35-75 38-l 12
- *p ~0.05, and **p ~0.01 compared with I; tp <0.05campared with Ill. A = maximum velocity of atrial systolic wave; AV mean = mean value of
atrioventricular plane displacement; E = maximum velocity of early diastolic flow; FS = fractional shortening; HR = heart rate; I’= before cardioversion; II = 4 hours after cardnversion; Ill = 2 weeks after cardioversion; IV = 1 month after cardloversion; LA = left &urn.
reference to the interspace and distance from the ster- num. Follow-up recordings were obtained in a similar way, with the same transducer position and each subject in the same posture as in the first recording. Calculations were performed blindly without access to other parame- ters or clinical data.
Results are presented as mean f SD or median and range, or both. Comparisons of the results between 2 different parameters were obtained using Wilcoxon’s signed-rank test.
ireart rate was significantly decreased in the early phase after cardioversitin. After this phase, heart rate was essentially stable. At baseline the left atrium was
FIGURE l.Fovzhamberview(/eff)tith MmodecursorDlacsdatssDtalborderot
Wing systole is shown on (right).
BRIEF REPORTS 696

enlarged, but I month after cardioversion the dimension was signiftcantly reduced. Both fractional shortening and mean value of atrioventricular plane displacement were significantly increased 4 hours after cardioversion. Further improvement was noticed after 2 weeks and 1 month (Table ZZ).
Patients were divided into 2 groups: those with left atria1 dimension GO mm (43 f 3, range 40 to 48; group Z [n = a), and those with 150 mm (55 f 3, range 52 to 60; group ZZ [n = 6j) at baseline. Four hours after car- dioversion, all patients in group Z, and only 1 in group ZZ showed evidence of Doppler-recorded A waves (Table Z). After 2 weeks, all patients had A waves. Doppler A-wave signals increased further, and after 1 month the A/E ratio was significantly increased compared with that at 2 weeks.
During LV filling, the atrium goes through phases of passive atria1 emptying, diastasis and active atria1 empty- inge6 Most investigators agree that loss of atria1 systole, as in AF, results in a 20 to 30% decrease in stroke volume and cardiac output.7 The decrease is even more pro- nounced in patients with reduced ventricular compliance. It has been suggested that the return of normal atria1 mechanical function may not occur immediately after successful cardioversion.3 Underlying rheumatic heart disease or duration of AF may play a role in the return of left atria1 mechanical activity.’ Pulsed Doppler echocar- diography provides a noninvasive method for the quanti- fication of blood flow across the mitral valve, thereby allowing measurement of the contribution of the left atri- al systolic flow to the total LV filling.8 Using this tech- nique we found that patients with a relatively small left atria1 dimension showed A waves (i.e., evidence of me- chanical atria1 activity) 4 hours after cardioversion, con- trasting with those with large left atria who had no A waves.
Conflicting results have been reported regarding he- modynamic function after cardioversion of AF to sinus rhythm.2-4 Recent studies5p9 demonstrated that the atrio- ventricular plane displacement toward the apex (i.e., sys- tolic descent of the base) is a simple and reliable method for assessing LV systolic function. In patients with a mean atrioventricular plane displacement 210 mm, a normal LV ejection fraction could be predicted with high sensitivity and specificity.9 In the present study, the base- line value was 9.5 mm. The increase in myocardial func- tion 4 hours after cardioversion may be explained by a decrease in heart rate, as well as by the addition of active atria1 function in most patients.
The relation of the height of the Doppler-recorded A wave to that of the E wave of the transmitral flow was
used to express the contribution of atria1 contraction to LV tilling. The height of the A wave is dependent on the pressure gradient across the mitral valve at end-diastole. Because a major change in LV compliance in individual patients during the study is unlikely, the height of the A wave may be used to reflect the force of atria1 contrac- tion. In accordance with Starling’s law of the heart,lO the characteristics of ventricular contraction are a function of the ventricular end-diastolic fiber length and pressure. Thus, each heart needs a specific end-diastolic pressure and fiber length to contract during systole. The atrium, through its effects on LV end-diastolic pressure and fiber length, is thus capable of modifying ventricular perfor- mance. In agreement with the above concept, the contin- ued increase in atria1 systole resulted in a concomitant improvement in LV function up to 1 month without any further decrease in heart rate.
In conclusion, patients with AF showed improved, but not completely restored, LV function at an early phase after cardioversion to normal sinus rhythm. The increase of LV function is probably due to a reduction in heart rate, as well as to the addition of active atria1 systole. Patients with a relatively small left atrium showed evi- dence of atria1 systole in an early phase after cardiover- sion. A subsequent improvement in LV function may be explained by a continued increase in atria1 pumping ac- tivity.
1. Manning WJ, Leeman DE, Gotch PJ, Come PC. Pulsed Doppler evaluation of atrial mechanical function after electrical cardioversion of atria1 fibrillation. JAm Coli Cardiol 1989;13:617-623. 2. Orlando JR, van Henrick R, Aronow WS, Olson HG. Hemodynamics and echocardiograms before and after cardioversion of atria1 fibrillation to normal sinus rhythm. Chest 1979;76:521-526. 3. Rowlands DJ, Logan WFWE, Hewitt G. Atria1 function after cardioversion. Am Heart J 1967;74:149-160. 4. DeMaria AN, Lies JE, King JF, Miller RR, Amsterdam EA, Mason DT. Echographic assessment of atria1 transport, mitral movement, and ventricular performance following elcctroversion of supraventricular arrhythmias. Circula- tion 1975;51:273-282. 5. Hijglund C, Alam M, Thorstrand C. The atrioventricular valve plane displace- ment in healthy persons. An echocardiographic study. Acta Med Stand 1988;224: 557-562. 6. Alam M, Rosenhamer G, Hiiglund C. Comparability of echocardiography and chest x-ray following myocardial infarction. J Intern Med 1989;226:171-175. 7. Sanfilippo, Abascal VM, Sheehan M, Oertel LB, Harrigan P, Hughes RA, Weyman AE. Atrial enlargement as a consequence of atria1 fibrillation. A pro- spective echocardiographic study. Circulation 1990;82:792-797. 8. Rekey R, Quinones MA, Zoghbi WA, Kuo LC, Abinader EG. Influence of left atria1 systolic emptying on left ventricular early filling dynamics by Doppler in patients with sequential atriaventricular pacemakers. Am J Cardiol 1988;62: 968-971. 9. Alam M. The atrioventricular plane displacement as a means to evaluate left ventricular systolic function in acute myocardial infarction. C/in Cardiol 1991; 14:58X-594. 10. Starling EH. The Linacre Lecture on the Laws of the Heart (Cambridge, 1915). London: Longmans, Green and Co., 1918.
696 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 69 MARCH 1, 1992