lecture 5 regulation of sodium and water excretion ….. essentially same as….. regulating plasma...
TRANSCRIPT

Lecture 5Regulation of Sodium and Water Excretion
….. essentially same as…..Regulating Plasma Volume and Osmolarity

Kidneys excrete salt and water
Since the amounts of salt and water in body define blood volume & osmolarity,
Kidney’s control blood volume and body fluid osmolarity.

Renal Role in Blood Pressure Regulation
►Short Term BP Control: seconds/minutes classic baroreceptor reflex sympathetic output changes vascular resistance
►Medium Term BP Control: minutes/hours renin release renin promotes angiotensin II formation circulating angiotensin II changes vascular resistance
►Long Term BP Control: hours/days changes in total body salt & H20 changes blood volume
The Kidney’s Role: 1) renin release (min/hrs) 2) controlling blood volume (hrs/days)
• Blood volume changes when H20 moves in or out of the plasma.
• H20 always moves down osmotic gradients.
CONCEPTCONCEPT:: If you control Na, then you control blood volume.
• Most abundant osmotically active particle in plasma is Na+.
• Control of Na = control of H20 movement = Control of volume

Regulation of Na+ & H20 Balance
First a Conceptual Overview
Parallel BulkHandling
DifferentialHormonal
Fine-Tuning
PressureNatriuresis
Aldosterone ….. Na ADH ….. H20

Regulation of Na+ Balance
Pressure NatriuresisDefinitionsDefinitions:: Natriuresis = Na+ excretion in Urine
Pressure Natriuesis is caused by increased blood pressure & associated increase in GFR.
MoreIN
MoreOUT
Simply HemodynamicsSimply Hemodynamics:: More IN = More OUT No independent treatment of Na+ & H20 Good for simple bulk volume control
Some Murky Mechanism DetailsSome Murky Mechanism Details: : Some evidence that increased BP some
how down regulates Na reabsorptionfrom the proximal tubule
Higher hydrostatic pressure in peritubularcapillaries reduces reabsorption fromthe proximal tubule. Pressure Natriuresis:
1) driven by simple hemodynamics 2) proximal nephron phenomenon 3) no sensors or circulating factors
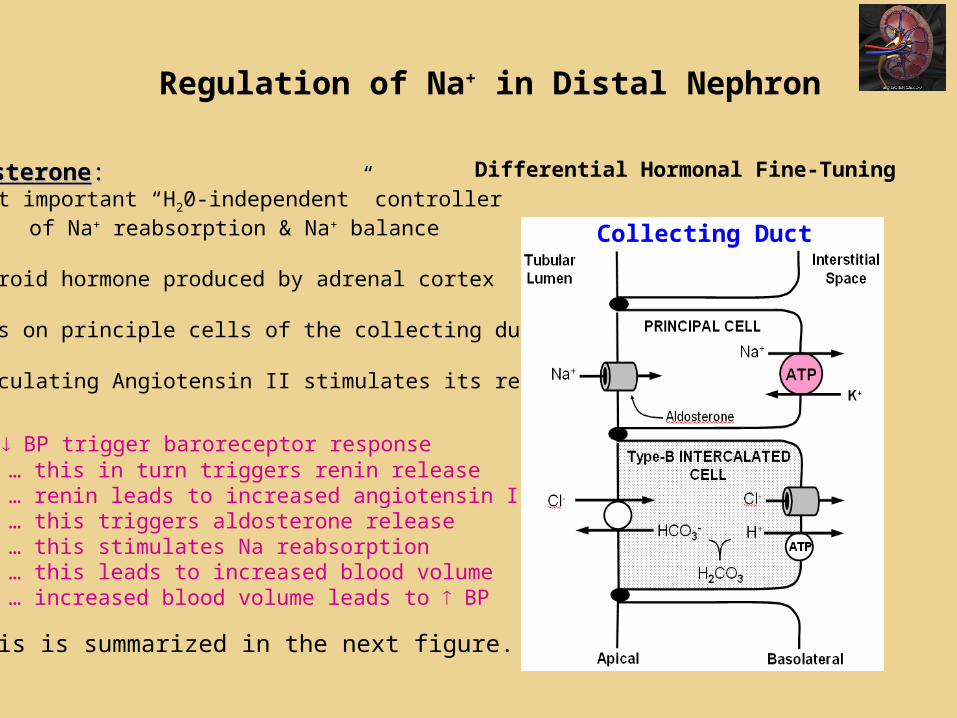
Regulation of Na+ in Distal Nephron
AldosteroneAldosterone:: Most important “H20-independent” controller
of Na+ reabsorption & Na+ balance Steroid hormone produced by adrenal cortex
Acts on principle cells of the collecting duct
Circulating Angiotensin II stimulates its release
So… BP trigger baroreceptor response … this in turn triggers renin release … renin leads to increased angiotensin II levels … this triggers aldosterone release … this stimulates Na reabsorption … this leads to increased blood volume … increased blood volume leads to BP
This is summarized in the next figure.
Differential Hormonal Fine-Tuning
Collecting Duct

… BP triggers baroreceptor response … BP & sympathetic inputs trigger renin release from granular cells … renin enters circulation and leads to increased angiotensin II levels … angiotensin II triggers aldosterone release from adrenal cortex … aldosterone stimulates Na reabsorption from collecting duct … the retained Na leads to increased blood volume which raises BP
Aldosterone is not the only hormone that regulates the body’s Na+ balance.

Atrial Natriuretic Peptide
Atrial Natriuretic PeptideAtrial Natriuretic Peptide
→ released from heart when atria stretch due to high blood volume ( BP)
→ vasodilates afferent arteriole increasing GFR
→ inhibits Na reabsorption in from collecting duct
→ inhibits renin-angiotensin
Now….
Let’s look at hormonal control H20 balance

Regulation of H20 Balance
Key Hormone = Antidiuretic Hormone (ADH) sometimes called vasopressin
Collecting DuctADHADH : :
Peptide hormoneCys-Tyr-Phe-Gln-Asn-Cys-Pro-Arg-Gly
Released from posterior pituitary
Increases H20 Permeability of apicalmembrane by promoting the fusion
of vesicles containing an aquaporin
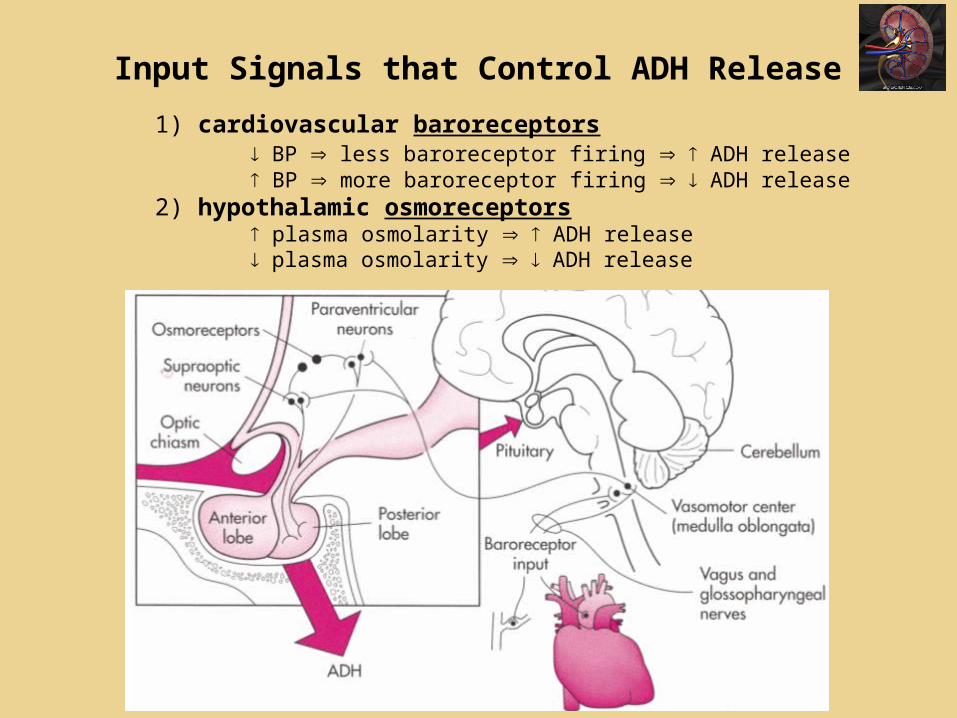
Input Signals that Control ADH Release
1) cardiovascular baroreceptors BP less baroreceptor firing ADH release BP more baroreceptor firing ADH release
2) hypothalamic osmoreceptors plasma osmolarity ADH release plasma osmolarity ADH release
Input Signals that Control ADH Release
1) cardiovascular baroreceptors BP less baroreceptor firing ADH release BP more baroreceptor firing ADH release
2) hypothalamic osmoreceptors plasma osmolarity ADH release plasma osmolarity ADH release
Baroreceptors

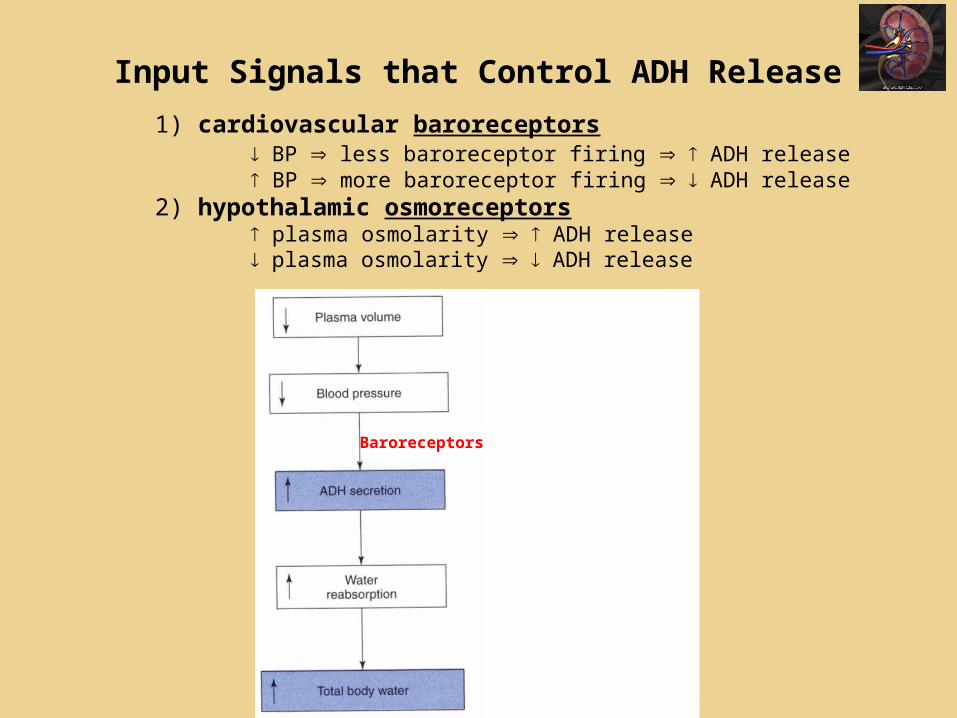
Input Signals that Control ADH Release1) cardiovascular baroreceptors
BP less baroreceptor firing ADH release BP more baroreceptor firing ADH release
2) hypothalamic osmoreceptors plasma osmolarity ADH release plasma osmolarity ADH release
Osmoreceptors
The cells thatrelease ADH integratethe 2 input signals.
“2 heads are better than 1”

Input Signals that Control ADH Release1) cardiovascular baroreceptors
BP less baroreceptor firing ADH release BP more baroreceptor firing ADH release
2) hypothalamic osmoreceptors plasma osmolarity ADH release plasma osmolarity ADH release
Generally, osmolarity usually dominates unless there arevery large changes in volume.
Certain other brain level inputs can alter short-term ADH release (fear, pain, alcohol).
Diabetes insipidus is due to abnormal ADH regulation. Origin could be brain problem or bad renal ADH receptors.

Free Water Clearance (CH20)means to access renal H20 handling, not the usual clearance calculation
The CH20 determination considers urine as having 2 parts:UrineVolume
solute-free H20
H20 withsolute
Can be calculate as Osmolar Clearance
COSM =
UOSM · V
POSM
solute-free H20
H20 withsolute
This is the H20 “cleared”
Volume in which solutes present would be iso-osmotic compared to plasma.
v

Free Water Clearance (CH20)means to access renal H20 handling, not the usual clearance calculation
The CH20 determination considers urine as having 2 parts:UrineVolume
solute-free H20
H20 withsolute
Can be calculate as Osmolar Clearance
COSM =
UOSM · V
POSM
Thus…. CH20 = V - COSM
solute-free H20
H20 withsolute
This is the H20 “cleared”
Volume in which solutes present would be iso-osmotic compared to plasma.
v

Free Water Clearance (CH20)means to access renal H20 handling, not the usual clearance calculation
The CH20 determination considers urine as having 2 parts:UrineVolume
solute-free H20
H20 withsolute
Can be calculate as Osmolar Clearance
COSM =
UOSM · V
POSM
Thus…. CH20 = V - COSM
solute-free H20
H20 withsolute
This is the H20 “cleared”
Volume in which solutes present would be iso-osmotic compared to plasma.
v
Note: CH20 could be negative !! This is when veryconcentrated urine is being produced.

Free Water Clearance (CH20)means to access renal H20 handling, not the usual clearance calculation
The CH20 determination considers urine as having 2 parts:UrineVolume
solute-free H20
H20 withsolute
Can be calculate as Osmolar Clearance
COSM =
UOSM · V
POSM
Thus…. CH20 = V - COSM
If… V = COSM
Then… CH20
is zero
If… V < COSM
Then… CH20
is negative
solute-free H20
H20 withsolute
This is the H20 “cleared”
Volume in which solutes present would be iso-osmotic compared to plasma.
v
If… V > COSM
Then… CH20
is positive
Note: CH20 could be negative !! This is when veryconcentrated urine is being produced.


Renal Physiology Quiz for Lecture 5:
Note that this and other Renal Physiology quizzes are simply provided to you to help you self-test your understanding of each lecture. They are not a substitute for studying the other learning
materials presented to you. These questions are not intended to reflect the style or level of difficulty of questions on the Final Exam.

True/False Questions:
1. The looping configuration of the vasa recta is important to preserving the hypo-osmotic interstitium of the renal medulla.
F 2. Renin is a proteolytic enzyme that cleaves the angiotensinogen produced by the liver. T3. The kidney rapidly changes the body’s blood volume in pace with short-term
(seconds/minutes) fluctuations in blood pressure. F4. Pressure natriuresis is largely a proximal nephron phenomenon that does not
involving any pressure sensing receptors. T 5. Aldosterone is a peptide hormone released from the adrenal medulla. F 6. Antidiuertic hormone (ADH) causes the water permeability of the collecting duct to
decrease. F 7. Atrial Natriuretic Peptide (ANP) promotes the excretion of Na+ into the renal tubular
fluid. T 8. A negative free water clearance means that the urine is dilute and excess water is
being excreted in the urine. F

Multiple Choice Questions9. Which of the following will result in triggering more renin release? a. decrease in renal afferent arteriolar pressure b. increase in sympathetic neural activity c. abnormally low NaCl level in the tubular fluid passing through the distal tubule d. answers a, b and c are all correct e. .none of the above
10. Which of the following will result in triggering more aldosterone release? a. a decrease in plasma K+ levels b. a reduction in circulating angiotensin II levels c. block of angiotensin converting enzyme d. stimulation of renin release e. an elevation in mean arterial pressure
11. Which of the following will result in triggering more ADH release? a. an increase in blood osmolarity b. an increase in blood volume c. an increase in blood pressure d. answers a, b and c are all correct e. none of the above12. What is the free water clearance considering the follow lab values? Urine volume = 2 ml/min Urine Osmolarity = 600 mOsm Plasma Osmolarity = 300 mOsm a. -2 b. +6 c. 0 d. -1 e. +3


The main goal of visualization and rendering is to effectively convey information to the viewer. For scientific visualization, this goal translates into determining which portions of data to highlight and how to render these portions to concisely convey
the appropriate information to the specific audience. These are the tasks that medical and technical illustrators have undertaken for centuries. We have developed a system that builds upon and extends recent work in volume
illustration to produce images that simulate pictorial representations for scientific and biomedical visualizations. Our system is designed in collaboration with a trained biomedical illustrator whose work focuses on visualization for clinical research and resident surgical training. The system combines traditional and
novel volume illustration techniques. A high-level interface enables the user to specify the type of illustration and visualization goals to produce effective,
illustrative rendering on commodity graphics hardware at nearly interactive rates. .This work has been published in IEEE Computer Graphics & Applications Journal, special issue "Smart Depiction in Visual Communication", May/June 2005. [PDF]. The demostration of the system has been included in SIGGRAPH 2005 conference
half-day course, course #31 "Computer-Generated Medical, Technical, and Scientific Illustration".
