lecture 3 therapeutic relationship in couples therapy
TRANSCRIPT

LECTURE 3. THE THERAPEUTIC RELATIONSHIP IN A COUPLE CONTEXTCOUPLE COUNSELLING SKILLSKEVIN STANDISH
LEARNING OUTCOMES1. How couple counselling differs from working with individual clients.
2. Building the Therapeutic Alliance in couples (Rait 2000)
3. Explore The Milan Principles (Brown 2010)
4. The Challenge of Creating Dialogical Space for Both Partners in Couple Therapy (Rober 2015)
5. DEVELOPING THE WORKING ALLIANCE IN MARITAL THERAPY A PSYCHODYNAMIC PERSPECTIVE (Patalano 1997; Scharff 2014; Bagnini 2014)
6. Behavioral Couple Therapy: Building a Secure Base for Therapeutic Integration (Gurman 2013)
7. Reflexivity and the use of self in the couple (GRANT & CRAWLEY 2001)
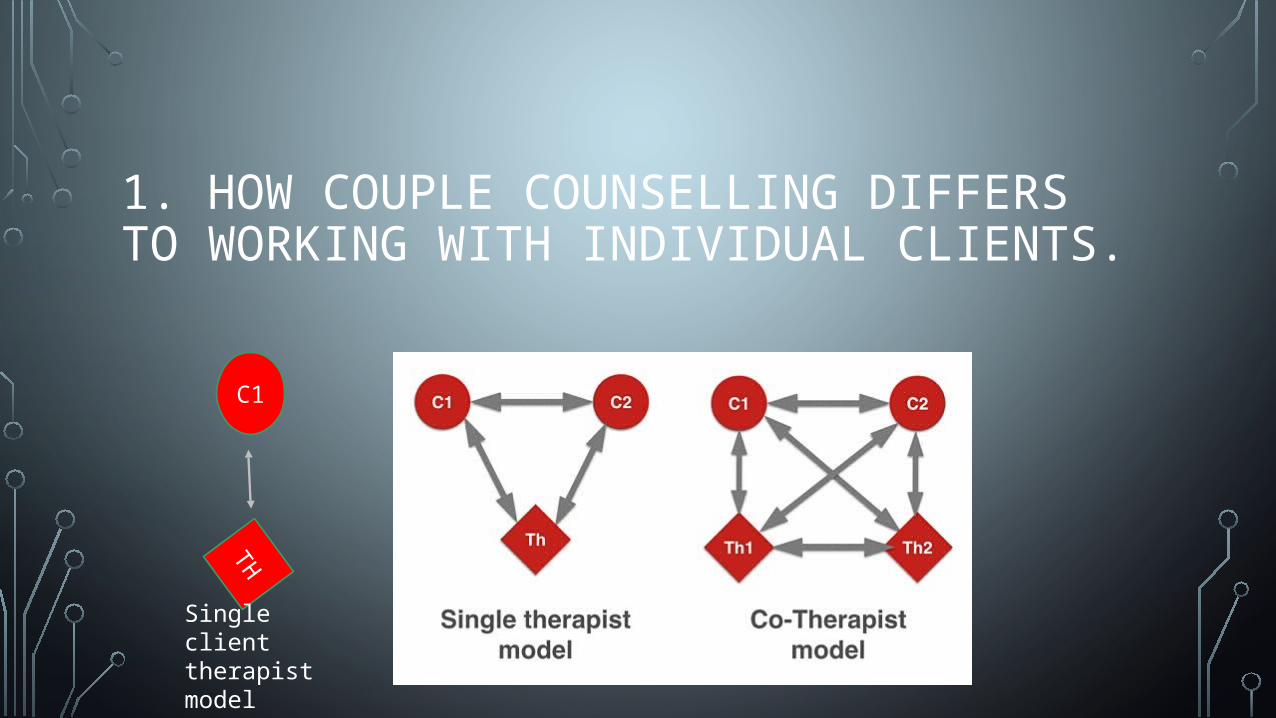
1. HOW COUPLE COUNSELLING DIFFERS TO WORKING WITH INDIVIDUAL CLIENTS.
C1
TH
Single client therapist model
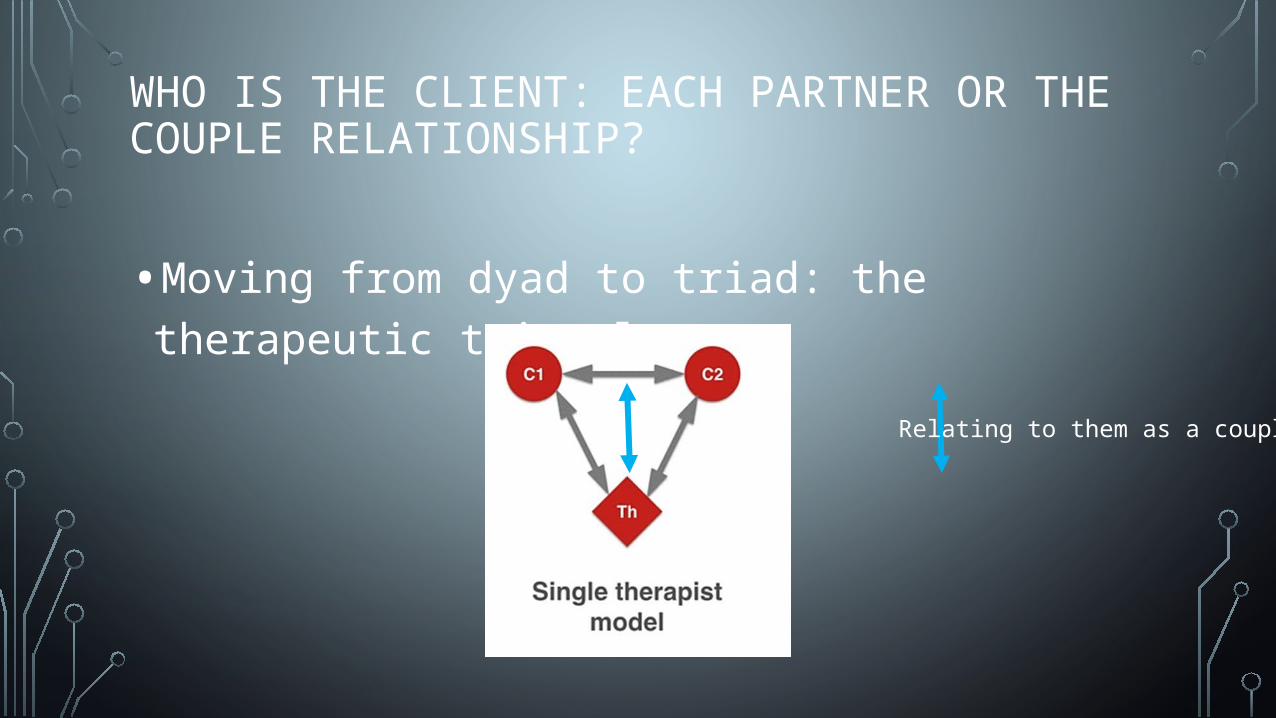
WHO IS THE CLIENT: EACH PARTNER OR THE COUPLE RELATIONSHIP?
•Moving from dyad to triad: the therapeutic triangle
Relating to them as a couple

PRESENTING ISSUES
•http://www.psychotherapy.net/video/emotionally-focused-therapy-training
•3:30 min

FEEDBACK
•What did you see the therapist doing to ensure a good therapeutic alliance is built?

2. BUILDING THE THERAPEUTIC ALLIANCE IN COUPLES (RAIT 2000)
https://www.youtube.com/watch?v=rgWnadSi91sJohn Gottman: How to Build Trust 5min

FEEDBACK
•What can you do to help build trust in clients as a couple in therapy?
THE THERAPEUTIC ALLIANCE COUPLES DIFFERS FROM INDIVIDUALS IN THAT THE THERAPIST HAS TO MAINTAIN MULTIPLE ALLIANCES SIMULTANEOUSLY
• 5 important dimensions of the therapeutic alliance that apply to the couples context:
1. The patient’s affective bond with the therapist,
2. the patient’s capacity to work effectively in therapy,
3. the therapist’s empathic understanding and involvement,
4. the agreement of patient and therapist on the tasks and goals of therapy.
5. The couples capacity to mutually invest in, and collaborate on, the therapy
MAINTAIN MULTIPLE ALLIANCES SIMULTANEOUSLY•Because there are multiple participants in couples,
simply meeting with a couple can be challenging, especially for the beginning therapist.
•Couples sessions tend to be noisier and more openly conflictual than the individual psychotherapy.
•Difficulties inmanaging the multi- sourced therapeutic conversation,
•

MAINTAIN MULTIPLE ALLIANCES SIMULTANEOUSLY• recognizes that not every partner comes to treatment with equal
motivation, similar goals, or agreed-upon beliefs about how to change.
• Couples therapy is conducted with individuals who are to some degree, involuntary clients.
• As a result, many couple therapy approaches have paid extensive attention to the beginning phase of treatment, especially given the higher rates of premature termination reported than in individual treatment

MAINTAIN MULTIPLE ALLIANCES SIMULTANEOUSLY• The therapist’s alliance with one or two family members inevitably
affects the alliance with other family members in a circular, reciprocal fashion, no single dyadic or triangular alliance can be considered in isolation.
• In couples the therapist needs to develop different levels of alliance, including an alliance with each individual partner and the couple as a whole.
• The couples therapist must be skilled at developing and maintaining a functional therapeutic milieu that continually balances the therapist’s relationship with each partner, as well as the couple as a whole

THEY MUST ADOPT A CONCEPTUAL FRAMEWORK THAT ACCOUNTS FOR INTERACTIONS IN TRIANGLES AND HOW DIFFERENT MODELS PLACE THE THERAPIST IN DIFFERENT POSITIONS
•dyadic exchanges are viewed within the context of triangular relationships.
•Knowledge of triangles provides the therapist with a way to think beyond the symmetrical and complementary exchanges that characterize dyadic interactions to three-person interactions.
INTERACTIONS IN TRIANGLES•While a two person system may be stable as long as
it is calm, the dyad will immediately involve “the most vulnerable other person to become a triangle” when anxiety increases (Bowen, 1976, p. 76).
• If the emerging tension becomes too great for the threesome, the system then can be expected to engage others in a series of interlocking triangles

INTERACTIONS IN TRIANGLES•Haley (1976) has asserted that the therapist needs to
include himself or herself in the description of the couple:
• “When doing therapy with a couple, it is best for the therapist to consider that whatever the partners do in relation to each other is also in relation to the therapist.”
•Thinking in terms of triangles carries important implications for therapeutic practice.

INTERACTIONS IN TRIANGLES•Unlike the therapist in individual psychotherapy, the couple’s therapist must be able to join and manage skillfully an alliance with each member of the couple, as well as the couple as a unit.
•The therapist needs to be able to move freely back and forth between members of the couple, always attending to invitations to join one against the other.

DIFFICULTIES IN THE THERAPEUTIC ALLIANCE• Whatever the therapist’s model of treatment, understanding of the
couple’s patterns, as well as his or her own participation in them, problems in the therapeutic alliance do arise.
• While these impasses can be both frustrating and demoralizing, they also represent a potential learning opportunity for clinician and couple alike.
• the therapeutic impasse in couple therapy is a deterioration in the therapeutic relationship in which the therapeutic experience has lost its emotional energy.

DIFFICULTIES IN THE THERAPEUTIC ALLIANCE• they also provide the therapist and patient with
“indispensable information” and the opportunity for genuine, corrective learning.
•According to Whitaker (1968), the responsibility to prevent or terminate an impasse lies with the therapist.

DIFFICULTIES IN THE THERAPEUTIC ALLIANCE•couple therapists, regardless of theoretical orientation, may seek to protect themselves through:
•over-involvement,• increasing isolation, •or overreliance on formal technique.
• Indications that the therapist is experiencing a therapeutic impasse include:
• insufficient joining,
• lack of therapeutic intensity,
• lack of pacing,
• inability to challenge the system,
• diffusing conflict,
• being “ahead” of the couple,
• over identifying with one partner member,
• taking too central and directive a position
DIFFICULTIES IN THE THERAPEUTIC ALLIANCE
• In each case, the fit between the therapist and family’s goals, style, and preferences contribute to the quality of the therapeutic alliance.
•While ruptures in the therapeutic alliance can present a serious barrier to therapeutic progress,

THERAPEUTIC ALLIANCE AND PROGRESS IN COUPLETHERAPY: MULTIPLE PERSPECTIVES (GLEBOVA 2011)
• There was very little change in alliance over the early sessions of therapy, and
• changes in alliance did not always account for changes in relationship satisfaction.
• Husbands’ perceptions of satisfaction and alliance seem to play an important role in the dynamics of the therapeutic process.
• Findings suggest a reciprocal relationship between perceptions of alliance and
• progress in therapy when combining perceptions of therapists and couple clients.
3. EXPLORE THE MILAN PRINCIPLES (BROWN 2010)
THE MILAN PRINCIPLES OF HYPOTHESISING CIRCULARITY AND NEUTRALITY IN DIALOGICAL FAMILY THERAPY: EXTINCTION; EVOLUTION; EVICTION... OR EMERGENCE?

COPYRIGHT © ALLYN & BACON 2003
CIRCULAR CAUSALITY: KEY CONCEPT UNDERLYING SYSTEMIC THERAPY
We mutually influence each other via–
• Patterns of Interaction• Family members’
characteristic ways of behaving.
• Centrality of Communication• Patterns of interaction
expressed are both verbal and nonverbal.
• “One cannot not communicate.”
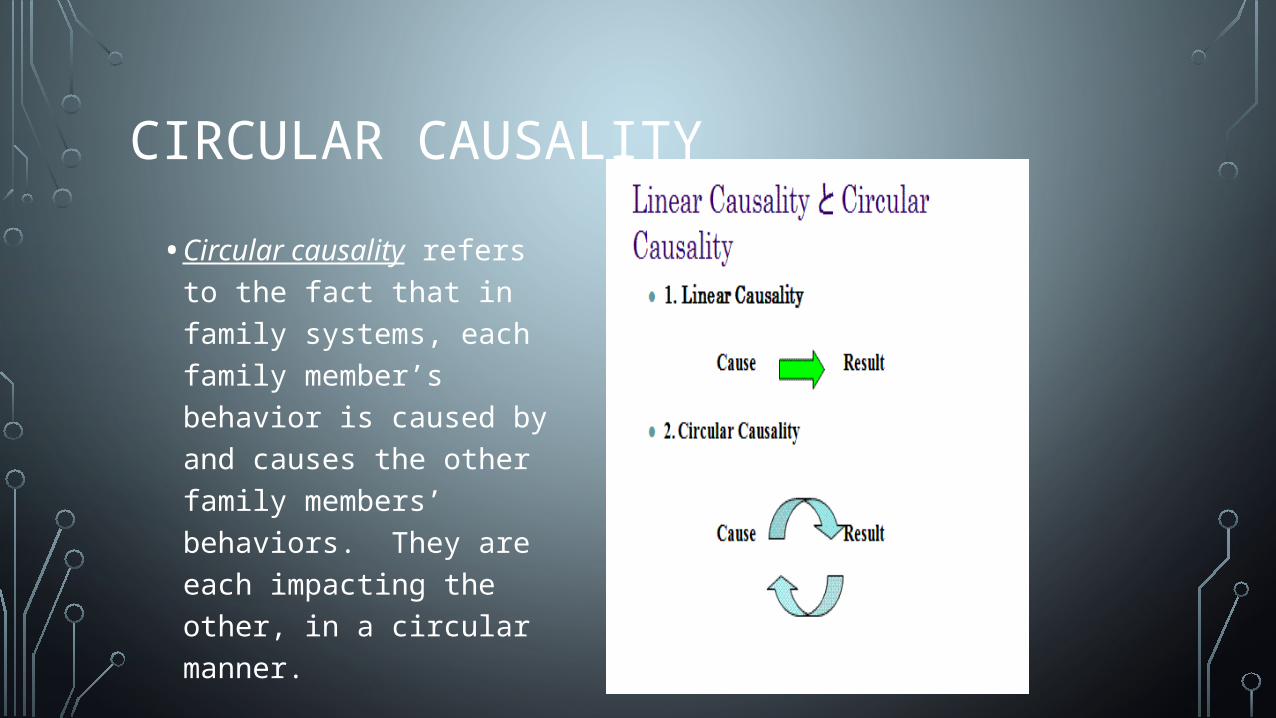
CIRCULAR CAUSALITY• Circular causality refers
to the fact that in family systems, each family member’s behavior is caused by and causes the other family members’ behaviors. They are each impacting the other, in a circular manner.
CIRCULAR CAUSALITY
• The distancer-pursuer and overfunctioner-underfunctioner are just two examples of the sorts of circular patterns that can develop in families. There are many other possibilities.
• A good clue to a “circular” pattern is when people tend to respond in predictable ways to each other, and their responses may become more extreme or even “stubborn” over time.

CIRCULAR CAUSALITY:DISTANCER-PURSUER

MILAN SYSTEMIC FAMILY THERAPYKEY CONCEPTS
1. Hypothesizing2. Circular questioning 3. Neutrality

1. HYPOTHESIZING
• Systemic hypothesizing is the Milan therapist’s way of confirming or disconfirming necessary information regarding how the family functions and how the therapist conceptualizes their functioning.
• Hypothesizing begins with the initial telephone call from the family.
• Prior to the first session, the Milan team exhausts all possible hypotheses about the family’s symptoms and functioning based on the telephone conversation.
HYPOTHESIZING• reflecting team members inform the therapist halfway through the
session of the new developed hypothesis.
• A new therapeutic direction may develop based on the consensus of the reflecting team
• As the session comes to a close, the team arrives at a final neutral hypothesis : the most systemic and powerful hypothesis for the family.
• The final hypothesis not ascribe blame to any single family member; often results in a prescription or ritual developed by the reflecting team.
• Later, after the family leaves, the reflecting team and therapist discuss how the family reacted to the intervention and plan for the next session.
• In some cases, a therapeutic letter is written

CIRCULAR QUESTIONING• Circular questioning is an interviewing method used
to gain descriptive assessments and deliver interventions through questioning of the family members
• Circular questioning is to expand the family’s beliefs beyond the meanings that they currently hold.
• This is often done by asking questions to individuals that probe how others view the situation.

CIRCULAR QUESTIONING
• Meaning formulation is an important component of this approach to develop context. “Without context, there is no meaning” (Campbell, 2003, p. 19).
• to examine their belief systems and the Meanings that they attached to their behaviours.
• based on inquiries about the differences within the relationships of family members and their perceptions

CIRCULAR QUESTIONING• The therapist continually searches for patterns, feedback loops,
differences in beliefs among family members (called openings), and the covert rules that support family interactions.
• openings allow a place during the session to begin questioning, , and exploring differences
• Circular questioning is an attempt for the therapist to see each person’s point of view. This later changed to curiosity (Cecchin 1987)
• What is the symptom that the patient presents? What is it there for? What function might it serve?
• What is the context of the symptom, i.e. what is happening when the symptom occurs?
• Why now? Why this symptom? Who can make it better, who can make it worse?
• Who is affected by the symptom? How? How does the symptom affect the family and how does the family deal with it?


NEUTRALITY/CURIOSITY• neutrality was that if every family member were asked at the end
of a session, ‘Whose side was the therapist on during the session?’ they would all say, ‘My side’”
• neutrality has been misunderstood and challenged as implying cold or aloof (Cecchin, 1987)
• A curious therapist allows all family members a voice
• Therefore, adhering to neutrality, the curious therapist is more likely to be open to numerous hypotheses about the system and invite the family members to explore those hypotheses, increasing the number of options for change

THE MILAN PRINCIPLES (BROWN 2010)• The primary aim of the three Milan principles of hypothesising,
circularity and neutrality• was to proffer an effective methodology for interviewing families, • with a secondary aim of casting off the stereotypical personal
therapist qualities such as intuition, charisma and concern• The relevance of the three principles to the therapeutic process, the
therapeutic role and the therapeutic relationship is considered.• seeks to conceptualise a vague 'knowing' that there is continual
learning and growth in grappling with the tensions in this field, in remaining ever curious, in asking the questions ...
JOIN THE COUPLE SYSTEM
•The therapist engages the couple and becomes empathically and emotionally connected to each person
•Partners must experience the therapist empathy and support for each of them individually and as a couple if they working alliance is to be established

JOIN THE COUPLE SYSTEM
•A holding environment and blame free context for the therapeutic work must be established with an atmosphere of safety prevailing to allow risk taking an exploration of vulnerabilities
•Joining with the couple involves collaborating with them
JOIN THE COUPLE SYSTEM
• The therapist must be an active participant, structuring and guiding the work while at the same time, conveying the belief that the couple possess the power, strength and resources to facilitate change
• Adequate and continuous joining is the glue that holds a couple and therapist together


4. THE CHALLENGE OF CREATING DIALOGICAL SPACE FOR BOTH PARTNERS IN COUPLE THERAPY (ROBER 2015)

THE CHALLENGE OF CREATING DIALOGICAL SPACEFOR BOTH PARTNERS IN COUPLE THERAPY (ROBER 2015)
• Dialogue in marital and family therapy (MFT) is by definition a multi-actor dialogue the conversation is often tension filled and can have dramatic real life consequences for family members
• the therapeutic relationship and the concept of not knowing• marital and family therapist cannot escape the uncomfortable
position of being responsible to find ways to actively contribute to a helpful dialogue with clients;
• a dialogue that is not a natural given, but rather a project that needs the therapist’s constant consideration and care

CONCEPT OF NOT KNOWING
• Described as a general attitude in which the therapist’s actions communicate a genuine curiosity
• In order to really listen to the client’s story, and to really understand what the client means, the therapist needs to be not knowing in the sense that he/she has to suspend his/her own assumptions and preconceptions, and be open to what the client wants to convey.
• The therapist is not the expert, but rather the client is seen as such.• HOWEVER The notion of the client as an expert does not deny that
a therapist has expertise!

KEY POINTS CREATING DIALOGICAL SPACE FOR BOTH PARTNERS 1. The therapeutic relationship in a multi-actor setting is complex.
2. Free and spontaneous dialogue, in which mutual understanding and intimacy can grow, is the exception rather than the rule as tension is at the core of dialogue.
3. As a therapist who adopts a receptive stance too early in the first marital therapy session can reinforce an already existing imbalance in the couple, the therapist cannot escape the uncomfortable position of having the responsibility to find ways to actively contribute to a helpful dialogue with the clients.
4. A couple therapist needs to find a way to transform the antagonism in the relationship into an agonism, in which tension and conflict are accepted and talked about, and in which the partner can sometimes be seen as an opponent or an adversary, but never as an enemy.

5. DEVELOPING THE WORKING ALLIANCE IN MARITAL THERAPY A PSYCHODYNAMIC PERSPECTIVE (PATALANO 1997; SCHARFF 2014; BAGNINI 2014)

DEVELOPING THE WORKING ALLIANCE IN MARITAL THERAPY; A PSYCHODYNAMIC PERSPECTIVE (PATALANO 1997)
• A good working alliance in marital therapy is one in which the partners are actively collaborating with their therapist to work through conflicts.
• The therapist begins to develop the alliance by setting the frame of therapy and helping the couple understand the guidelines of treatment.
• The partners gradually identify with and emulate the therapist's working style and use of self as a reflective instrument.
• The working alliance can be weakened by empathic failures and strengthened by increased feelings of trust in the therapist and the process of treatment
ESTABLISHING A THERAPEUTIC RELATIONSHIP IN ANALYTIC COUPLE THERAPY (SCHARFF 2014)
• The therapist approaches the couple, not as two individuals meeting the therapist, but as a couple.
• The patient is the couple relationship, not the two spouses who comprise it.
• To deal with the couple, the therapist must enter a couple state of mind as she addresses the task of the first interview and hopes to move beyond assessment into couple therapy.

THE TRIANGULAR FIELD OF COUPLE CONTAINMENT(BAGNINI 2014)
• search for clinical ideas that reveal the unconscious pathological matrix of couple relating (projections and introjections; transference and countertransference)
• and provide therapeutic guidelines for ameliorating their destructive hold on couple life
• Containment of the couple’s primitive defences and anxieties is essential to establishing a safe working alliance,
• but containment and its rupture reveals how therapists get inevitably caught in the web of triangular transferences

6. BEHAVIORAL COUPLE THERAPY: BUILDING A SECURE BASE FOR THERAPEUTIC INTEGRATION (GURMAN 2013)
HTTPS://WWW.PSYCHOTHERAPY.NET/VIDEO/BEHAVIORAL-COUPLES-THERAPY-VIDEO4 MIN

FEEDBACK
•Reflections on therapist approach?

BEHAVIORAL COUPLE THERAPY: BUILDING A SECURE BASEFOR THERAPEUTIC INTEGRATION (GURMAN2013)
• Integrative behavioral couple therapy (IBCT), the most visible and influential of the several BCT approaches, is examined, with particular attention to its functional–contextual base and the nature and role of functional analysis in clinical case conceptualization.
• It is argued that continuing enhancement and refinement of IBCT as an integrative therapeutic method will require greater flexibility in the techniques that are used and increased
• attention to the self of the IBCT therapist.
ENGAGING MEN IN COUPLES' THERAPY
• https://www.youtube.com/watch?v=nP0N0UIkPEY• 2min21
7. REFLEXIVITY AND THE USE OF SELF IN THE COUPLE THERAPY(GRANT & CRAWLEY 2001)

REFLEXIVITY AND THE USE OF SELF.
•The loss of reflective space.• Countertransference and reactions •Alliance with one partner versus the other partner

THE SELF IN THE COUPLE RELATIONSHIP: PART 1 JAN GRANT AND JIM CRAWLEY (2001)
• the importance of the ‘goodenough’ development of the core self in the couple relationship
• It argues that difficulties in the development of the self lie behind a significant number of troubled couple relationships.
• individual therapy, by assisting in the development of a more cohesive sense of self in the individual, inevitably has an impact on the individual’s relationships, especially their relationship with a partner

THE SELF IN THE COUPLE RELATIONSHIP: PART 2JIM CRAWLEY AND JAN GRANT (2001)
• focuses on the significance of ‘the self’ for couples therapy,
•argues that couples therapy may sometimes need to include therapeutic work with one partner to facilitate change in the relationship.
•Conceptualization of the couple relationship as ‘a transitional space’ is central.
•Links to the idea of “containment” in couples

SUMMARY1. Couple counselling differs from working with individual clients. It
involves working with triangles of relationships.2. Building the Therapeutic Alliance in couples involves joining with both
individuals who make up the couple as well as the couple as a unit3. Systemic principles inform the feedback loops and the circularity of
interactions.4. It is important to create Dialogical Space for Both Partners 5. Your therapeutic approach will determine the kind of working alliance
you develop6. Reflexivity and the use of self in the couple is vital to understanding
the process of healing both individual and the couple in couple therapy

SUE JOHNSON EMOTIONALLY FOCUSED COUPLES THERAPY (EFT) IN ACTION VIDEO
• https://www.youtube.com/watch?v=xaHms5z-yuM&ebc=ANyPxKrrw1smza8vU0370VX2xcOrvc1pXijShxyXOMvn1AmFs0vBUFpxYqDWaXF0Xgj8qhStZkNP
• 3:49 min
CORE READINGS

EXTRA READINGS
