learning culture: learning from deaths in · women with bipolar disorder and pregnancy: factors...
TRANSCRIPT


Learning culture: Learning from deaths in mental health, learning disabilities and community services Chair: Saffron Cordery, Director of Strategy and Policy, NHS Providers
Speakers: Dr Trudi Seneviratne, Consultant Adult & Perinatal Psychiatrist, South London & Maudsley NHS Foundation Trust Clare Dolman, Research & Patient and Public Involvement Lead, Perinatal Mental Health, Institute of Psychiatry, Psychology & Neuroscience, King's College London Tony Kelly, National Clinical Director for the Maternity and Neonatal Health Safety Collaborative, NHS Improvement Professor Cathy Warwick OBE, Chief Executive, Royal College of Midwives

Perinatal mental: A public
health priority
NHS Provider’s Conference [email protected] @TrudiSene1 08.06.2017



20 %

DETECT
SCREEN
PREVENT
INTERVENE
UK LEADS THE WAY .....
..............BUT WE CAN DO MORE



Key Messages & National Standards •Access to MBU Beds •Each CCG to have Specialist Community Perinatal Mental Health Teams – adequately resourced MDT to meet demand (psychiatrist and specialist nurses Type 1 standard) •Assessment within 24 hours to 2 weeks •Emergency provision •Psychological treatment within 1 month if assessment •Do not offer valproate for acute or long term treatment of mental health problems in women of childbearing potential

Impact of not Intervening: Devastating
• Impact on maternal health: suffering and isolation
• Impact on family
• Small for dates foetus
• Prematurity and longer term physical health problems
• Subsequent Reciprocal attachment with mother disrupted
• Infant temperament & Mother’s ill health
• Emotional neglect
• Physical harm.........suicide /homicide

0
1
2
3
4
5
6
7
8
9
10
1985-1987 1988-1990 1991-1993 1994-1996 1997-1999 2000-2002 2003-2005 2006-2008
Rate
per
100,0
00 m
ate
rnit
ies
Test for trend over period 1985-2008: p<0.001
Direct 4,67 100,000
Indirect 6.72 100,000 Total 11,39/100,000
Maternal death rate



Vulnerability of children < 1 year old
Marks and Kumar, 1995
Age of victim and annual homicide rates
Age of victim in Serious Case Reviews in England
Sidebotham et al, 2011

Conception
Early
childhood
Middle
childhood
Adolescence
Adulthood
Early adversity
Maltreatment
Trauma
Toxic stress
Disrupted neuro-
development
Social, emotional and
cognitive impairment
Adoption of risky
health behaviours
Disease disability
and social problems
Cumulative burden over time
Increased risks
for the next
generation
Conception
Early
childhood
Middle
childhood
Adolescence
Adulthood
Early adversity
Maltreatment
Trauma
Toxic stress
Disrupted neuro-
development
Social, emotional and
cognitive impairment
Adoption of risky
health behaviours
Disease disability
and social problems
Cumulative burden over time
Increased risks
for the next
generation
“Early adversity casts a long shadow” Sir Michael Rutter
Prevention case Why babies matter
£8.1 bn

Performance of Children at 11 years (SLCDS)
z-scores
-1
-0.5
0
0.5
1
IQ
Rea
ding
Mat
hs
Con
duct
Hyp
erac
tivity
Atten
tion
Em
otio
nal
Effect of mother's postnatal depressionMother well
Mother ill

0
10
20
30
40
50
60
70
% o
f a
do
lesc
en
t o
ffsp
rin
g
Never In utero 1st year Early childhood Middle childhood Adolescence
Timing of offspring first exposure to maternal depression
Depressed adolescents
Well adolescents
Adolescent depression at 16 years and first exposure to mother’s depression

Economist James Heckman found highest rates of return from early interventions
James Heckman’s analysis of the rates
of return from programmes
across different stages of childhood
suggest the smart investor would focus
her attentions on the early years
*8.1bn

carepathways©GreenMieleProtti
PERINATAL MENTAL HEALTH CARE PATHWAYS. MATERNAL MENTAL HEALTH: PSYCHIATRY
SERVICE LINE STRAND
TIER 0
PRIMARY CARE TIER 1&2
SECONDARY CARE TIER 3
TERTIARY CARE CARE TIER 4
Maternal Mental Health Psychiatry
Primary Care Liaison (based in GP surgery) – Psychiatric
Nurses/Social workers – triage, may hold low risks
cases
Perinatal Psychiatric teams can work jointly with Adult General Mental Health Services (AMHS) or CAMHS for adolescent pregnancies , Drug & Alcohol services, General Liaison Psychiatry, Eating Disorders and Learning Disability services. Named perinatal mental health champion in these teams is responsible for liaising with perinatal psychiatry for preconception advice and at pregnancy recognition.
MOTHER & BABY UNIT
The Perinatal Psychiatric Team works in partnership with: Obstetricians, Specialist Mental Health Midwife and Health Visitor, Child Safeguarding Midwife, Hospital Liaison Health Visitor, Social Workers (Children’s Social Care). Also with Maternal Mental Health psychological therapies and Early Years’ services when these are separated from the perinatal mental health teams.
Accredited Perinatal Psychiatric Service led by an adult psychiatrist with capacity for community outreach, obstetric liaison, case management and coordination of admission to MBU when indicated. The service offers on going advice, regular training and supervision to all tier 1,2,3 services, including midwives, health visitors.

Channi Kumar Mother and Baby Unit
• 13 bedded acute psychiatric unit for local, regional and
national referrals
• Full MDT assessment and treatment of all mental health problems presenting during pregnancy or up to one year post birth
• Staff include psychiatrists, psychologists, RMNs, OTs, nursery nurses, social workers and health care assistants
• Treatment is individualised and reflects the input of whole MDT

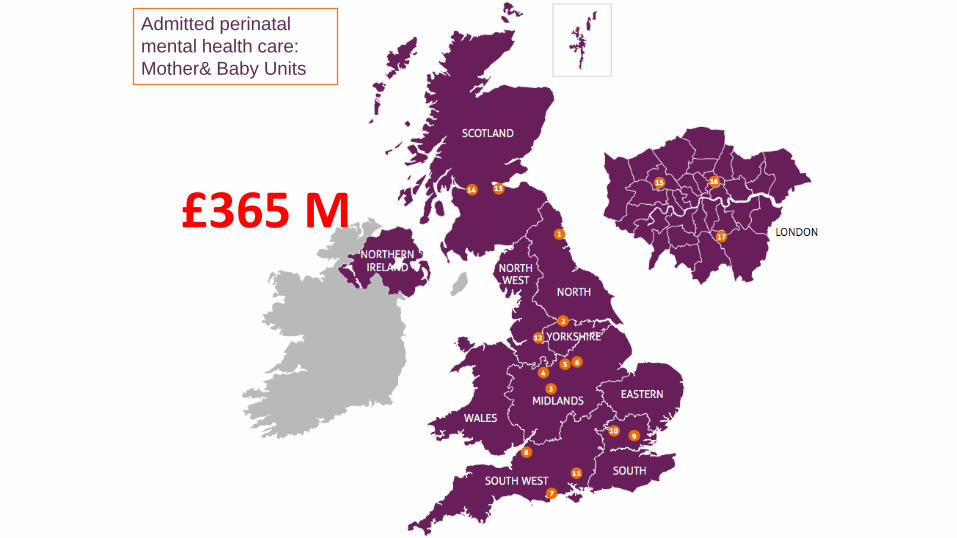
Admitted perinatal
mental health care:
Mother& Baby Units
£365 M
2015
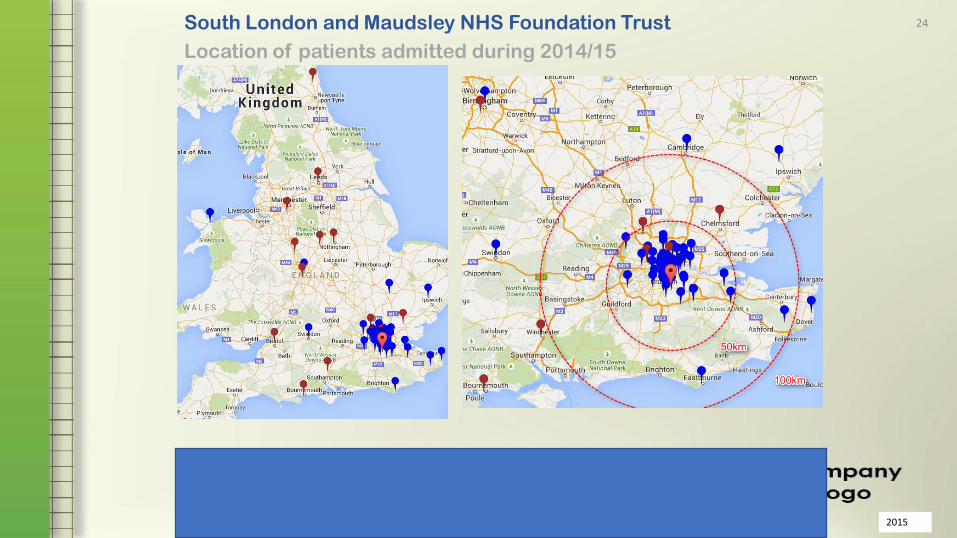
South London and Maudsley NHS Foundation Trust 24
Location of patients admitted during 2014/15

Non-admitted perinatal
mental health care
Quality: national outcomes framework CROM
• CROM • Maternal mental health HoNOS,
BPRS • Parent Infant relationship CARE Index, PIIOS,CARO • Infant ADBB
• PROM • CORE • Voice- perinatal; POEM • CAN-Mothers ( Hybrid) • PHQ9/GAD 7 ( Primary Care)
• PREM • Voice- perinatal; POEM;FFT
PROCESS
• RCPsych CCQI Process
• Waiting times
• NHSE Benchmarking data
• FACE –Perinatal

Initial severity is inevitably
greater in Acute than in
Community services
Reduction in total score is
significant with a large effect
size in both service samples
67% of inpatient episodes
had a pair of HoNOS
ratings.
Only 39% of community
episodes had a pair of
ratings and these cannot be
representative of service
outcomes.
Method 1
Change in Total HoNOS score
Change in Total HoNOS score provides
minimal information on the outcome of tx.

SLaM Perinatal Psychological Therapies 2015-2016

MBU : Improvements in maternal and infant interactions during
admission

What next ?????
• Intervening in perinatal period
a public health priority
• Access to services makes a difference
• After the 5YFV
• NHSE/STP/Commissioners/Clinical
Services

Learning culture: Learning from deaths in mental health, learning disabilities and community services Speakers: Clare Dolman, Research & Patient and Public Involvement Lead, Perinatal Mental Health, Institute of Psychiatry, Psychology & Neuroscience, King's College London


33

Women with Bipolar Disorder
and Pregnancy:
Factors influencing their
decision-making regarding
treatment
Clare Dolman1, Ian Jones2 Louise M Howard1 1 Section of Women’s Mental Health, Health Service and Population Research Department, Institute
of Psychiatry, Psychology and Neuroscience, King’s College London 2 MRC Centre for Neuropsychiatric Genetics and Genomics, Department of Psychological Medicine
and Neurology, Cardiff University
34
o Problems getting reliable
information and advice
o Need access to a
specialist perinatal
mental health service,
including MBUs
Conclusion
35
o Information
o Continuity of care
o Training of health professionals
o A comprehensive care plan
o Access to an MBU
o Peer support
o More research to help them make decisions
‘What women want from Services’ themes
36

Stigma
“I do think that amongst some members of staff in the Trust ...it’s
implicit that they view those of us …with bipolar as maybe
...[pause] we wouldn’t have adequate parenting skills” P10
37
“I am scared of getting pregnant again because ... now
that I have been diagnosed, I don't know if I will be deemed fit
to look after a newborn. It scares me so much.” (e-forum)
Fear of Social Services

38

39

www.maternalmentalhealthalliance.org
www.everyonesbusiness.org.uk 40

Call to ACT: overview
Accountability for perinatal mental health care to be clearly set
(including MBU provision)
Community specialist perinatal mental health teams meeting
quality standards to be available for women in every area of the UK
Training in perinatal mental health care to be delivered to all
professionals involved in the care of women during perinatal period
20

The costs of not treating perinatal
mental illnesses effectively are
significant:
• Much avoidable suffering
• Damage to families
• Impact on children
• Death or serious injury
• Economic costs
Report by LSE and the Centre for
Mental Health showed the cost to
the public sector of perinatal
mental health problems is 5 times
the cost of improving services
42

www.bipolaruk.org
www.app-network.org
43

Quality improvement in maternity and
neonatal health:
Tony Kelly, National Clinical Director, NHS Improvement

To improve the safety and outcomes of maternal and neonatal
care by reducing unwarranted variation and provide a high
quality healthcare experience for all women, babies and
families across maternity care settings in England”
What is the aim of the collaborative?
45

• Maternity care in England is of high quality
• Commitment and compassion are excellent
• The system is under huge pressures already
Disclaimer
46
Yes
• All maternity services in England
• All care settings
• All components of the pathway (conception to puerperium)
No
• Elements of care out with the gift of clinical teams
• (limited influence on improvement in maternal mortality)
What is within the scope of the
collaborative?
47
Person
Centred
Clinical
Excellence
Systems
and
Process
Human
Dimensions
48
Human
Dimensions
49
1. Build an infrastructure to support safety and improvement science
by creating the conditions for continuous improvement
2. Create the conditions for a safety culture
3. Create a learning system

Systems &
Processes
50
4. Develop a collaborative measurement strategy that
measures improvement and demonstrates impact
5. Learning from and designing reliable
systems and processes within maternity
services
8. Design and implement highly reliable
and effective pathways of care
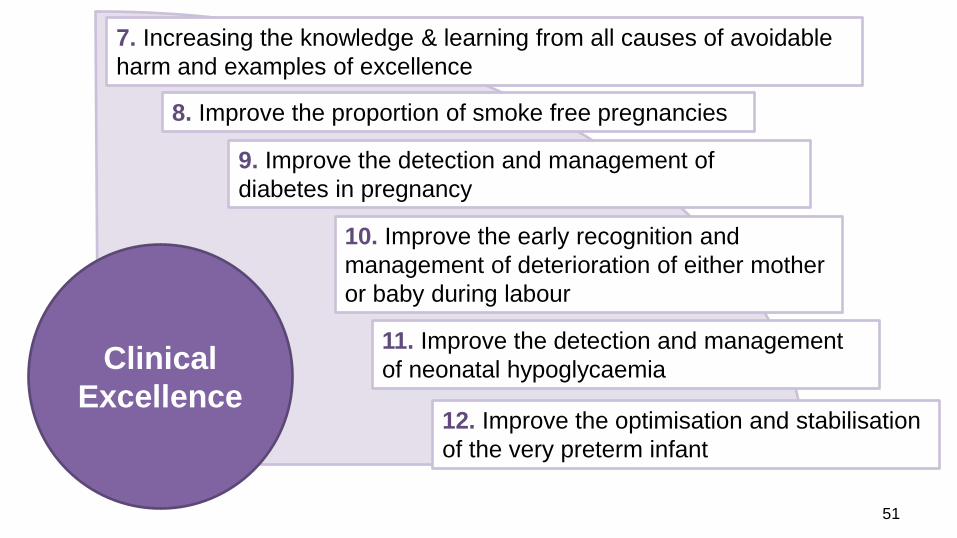
Clinical
Excellence
51
7. Increasing the knowledge & learning from all causes of avoidable
harm and examples of excellence
8. Improve the proportion of smoke free pregnancies
9. Improve the detection and management of
diabetes in pregnancy
10. Improve the early recognition and
management of deterioration of either mother
or baby during labour
11. Improve the detection and management
of neonatal hypoglycaemia
12. Improve the optimisation and stabilisation
of the very preterm infant

Person
Centred
52
13. Work with Mothers and families to improve their
experience of safer care
14. Work with staff to improve the work
environment to support staff to deliver safer care
15. Work effectively with local network and
commissioning organisations to develop effective
local maternity systems
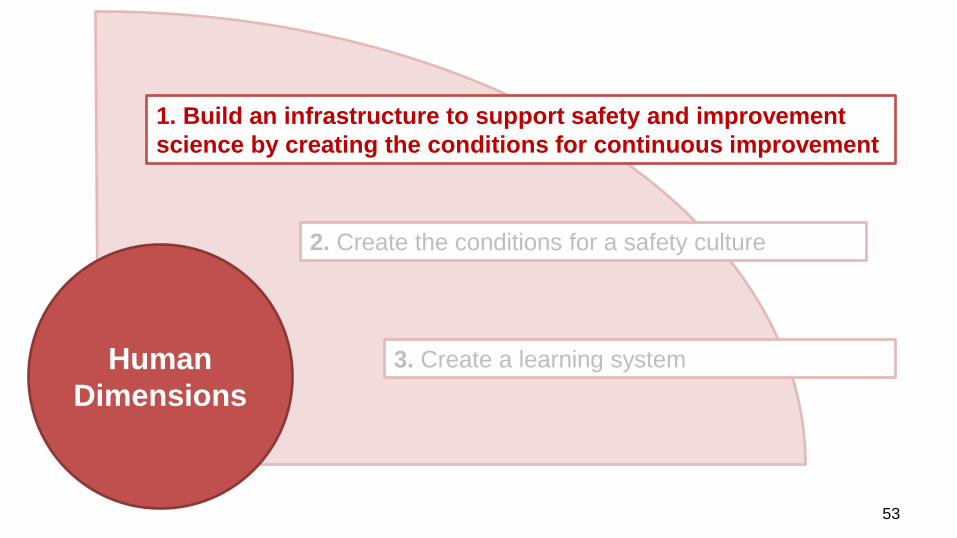
Human
Dimensions
53
1. Build an infrastructure to support safety and improvement
science by creating the conditions for continuous improvement
2. Create the conditions for a safety culture
3. Create a learning system

This is the ‘how’ in the conversation
54
• Capability (& capacity) for effective quality improvement is
low
• Often the focus is on assurance through process
• Retrospective rather than forward focused
• Need capability at all levels of the system
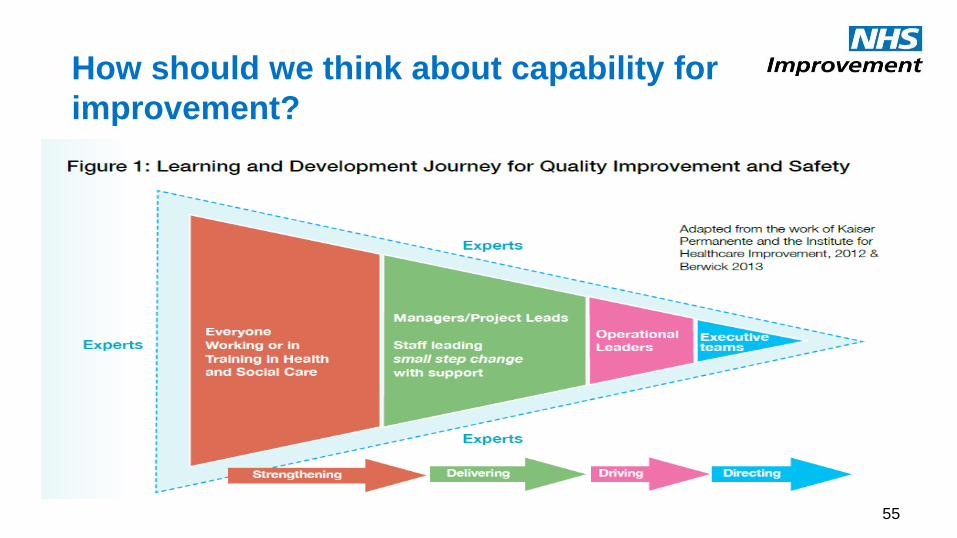
How should we think about capability for
improvement?
55

How will the collaborative ‘plug this gap’
56
National Learning Set
Trust
Trust
Trust
Trust
Trust Trust Trust
Local Community of
Practice
Trust Trust
Trust
Trust
LMS

How will the collaborative ‘plug this gap’
57
Exec champion
Local improvement teams
Main workforce
Local Trust
Champions
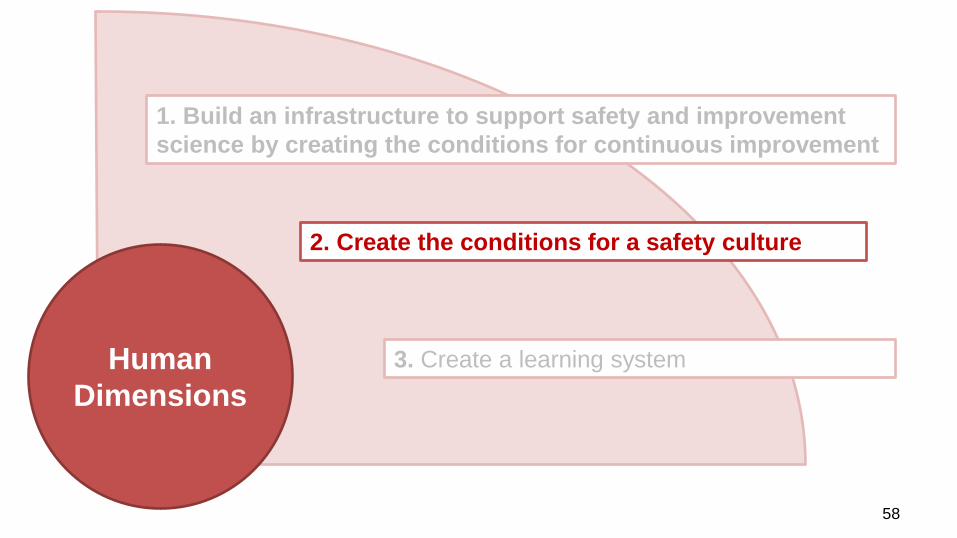
Human
Dimensions
58
1. Build an infrastructure to support safety and improvement
science by creating the conditions for continuous improvement
2. Create the conditions for a safety culture
3. Create a learning system
What is culture?
59
“How the Organisation behaves
when nobody is watching”
“How the Team behaves
when nobody is watching”

What is culture?
60

What can make safety culture assessment
work or fail?
61
Enablers
• Voluntary engagement
• Good local promotion
• Staff engagement
• Psychological safety
• Meaningful debriefing
• Opportunity to learn
High positive responses
seen in organisations with:
• Open just culture
• Organisational values
• Open communication
• Teamwork
• Planning

Trust
AHSN NM&N
HSC
MCN ODN
62
How will the collaborative ‘plug this gap’

LMS
AHSN NM&N
HSC
MCN ODN
63
How will the collaborative ‘plug this gap’
By 2020 each Trust, local maternity system and network should have:
• significant capability (& capacity) for improvement
• detailed knowledge of local cultural issues
• developed a locally sensitive improvement plan
• made significant improvement to local service quality and safety
• data to share with their board, staff and commissioners that reflect
these improvements
…to create the conditions for a safety culture and a national maternal
and neonatal learning system
What is the ambition of the collaborative?
64

LMS
MCN ODN
AHSN NM&N
HSC
65
Women,
Babies &
Families

Where are we now?
66
• All maternity services allocated to waves
• 44 Trusts in wave 1
– Covering 77 sites
– 166 local improvement leads
• Effective coverage of all AHSNs
• 7 entire local maternity systems in wave 1

How will the waves be structured?
• Establish national network
of all maternity units in
England
• Supported at national level
to enable local delivery
• 44 organisations to form
first national learning set
• Develop local communities
of practice at LMS level (to
meet once a quarter)
• Further 46 Trusts across
England to form second
national learning set
• Supported at national and
local level
• Wave 1 and 2
organisations to provide
local leadership
Wave 1
• Remaining 46 Trusts
across England to form
third national learning set
• Will join first and second
wave organisations in local
COP
• Supported at national and
local level
April 2017 – March 2018
Wave 2
April 2018 – March 2019
Wave 3
April 2019 – March 2020
67
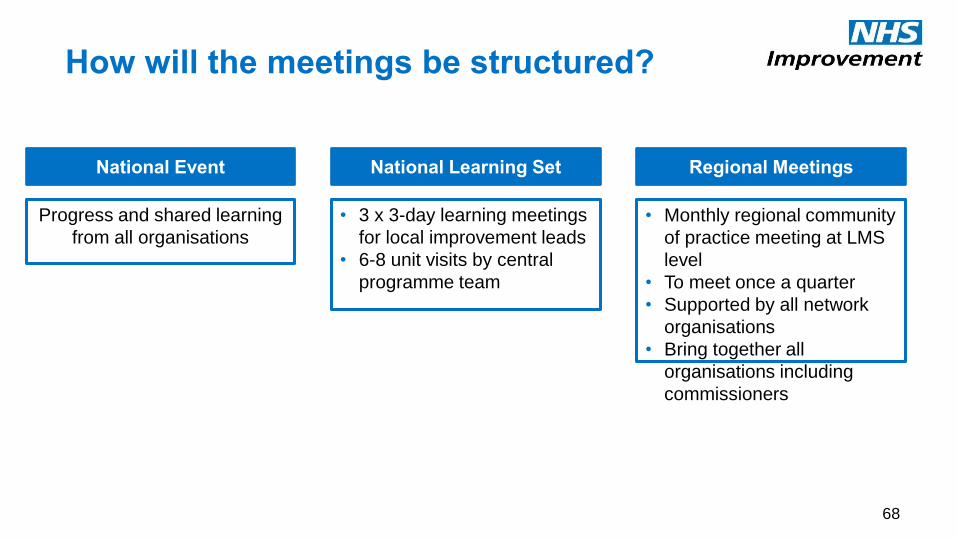
How will the meetings be structured?
National Event
Progress and shared learning
from all organisations
• 3 x 3-day learning meetings
for local improvement leads
• 6-8 unit visits by central
programme team
National Learning Set
• Monthly regional community
of practice meeting at LMS
level
• To meet once a quarter
• Supported by all network
organisations
• Bring together all
organisations including
commissioners
Regional Meetings
68


Activity of an individual unit
70
April to June July to September October to March
Diagnostic Phase Good Practice / Case Studies
Team
Data
Culture
Current / Future Pathway
Local priority setting
Develop improvement plan
Testing Phase
Unit level mobilisation
Identify change ideas
PDSA cycles
Measurement for improvement
Implementation Phase
Refine PDSA cycles
Extract & share learning
Support next wave
What additional support will organisations
in the national learning set receive?
71
Annual national learning event
Access to LIFE improvement
platform
Measurement for improvement
support
Tailored resources and
networks
community of practice meetings
Improvement & capability
development
(per wave)
Monthly unit visits
(per wave)
Wave learning sessions
(per wave)

Thank you
@tonykellyuk
www.improvement.nhs.uk
#MatNeoQI

Learning culture: Learning from deaths in mental health, learning disabilities and community services Speakers: Professor Cathy Warwick OBE, Chief Executive, Royal College of Midwives