learn · connect · succeed jcahpo regional...
TRANSCRIPT

Learn · Connect · Succeed
JCAHPO Regional Meetings
2017

TECHNICIANS AND NURSES PROGRAM ASCRS MAY 2017 Introduction Compounding • TASS • Anesthetics: Topical, Intracameral • Antisepsis • Dilation Phenyl, Shugar, Lidocaine, Combo • Anti-IFIS
William G. Myers, M.D. Northwestern University Chicago, IL
TECHNICIANS AND NURSES PROGRAM ASCRS MAY 2017
• NSAIDs • Stains TA, Blue, Green • Ocular Viscoelastic Devices • IC: Cefuroxime, Moxifloxacin, Vancomycin • Patient Independent Protocols
HISTORICAL OVERVIEW ON INTRAOCULAR INJECTION, GHOLAM PEYMAN M.D. • Intravitreal injection was tried in the 1940s • In 1971, understanding the ocular anatomical barrier to the
medication administered locally or systemically initiated the efforts to manage endophthalmitis via intravitreal injection of antibiotics
• Extensive experimental evaluation was needed to convince its skeptics.
• Investigations related to the toxicity of compounds injected intravitreally , pharmacokinetics of non-toxic doses in the vitreous cavity
• Comparative efficacy with other routes of administration in experimentally induced endophthalmitis.
HISTORICAL OVERVIEW ON INTRAOCULAR INJECTION, GHOLAM PEYMAN M.D.
• The toxicity and efficacy of combinations of drugs were studied.
• Infection stimulates the ocular defense mechanisms • These natural defense responses often are so severe they
impact the recovery of the eye from the infection. • Tolerance and the effect of anti-inflammatory agents were
evaluated

HISTORICAL OVERVIEW ON INTRAOCULAR INJECTION, GHOLAM PEYMAN M.D.
• Intraocular injection as the best choice to reach the intraocular pathology while avoiding the toxic side effects of systemic administration.
• Slow release drug polymers, their pharmacokinetics, and usefulness in acute infective processes.
• In acute infection, the slow release systems were not superior to the single bolus intraocular injection. They are useful in management of chronic disorders.
HISTORICAL OVERVIEW ON INTRAOCULAR INJECTION, GHOLAM PEYMAN M.D.
• Bacterial endophthalmitis originates from the external ocular surface flora, so preoperative preparation included systemic topical and subconjunctival administration of antibiotics.
• Topical application of Povidone iodine is useful in reducing the bacterial load on the conjunctiva and the corneal surface
• We expanded this treatment regimen to include intracameral /intravitreal injections.
• Presently intraocular injections are considered the standard of care for infectious endophthalmitis.
HISTORICAL OVERVIEW ON INTRAOCULAR INJECTION, GHOLAM PEYMAN M.D.
• No technique will completely eliminate all bacteria to prevent infection. • Therefore, there will always be some organisms that may not be sensitive to
the specific antibiotics applied extraocularly or intraocularly. • Presently, we are able to manage the majority of eyes afflicted by
endophthalmitis, if recognized and treated in a timely fashion.
CHEMICAL COMPOSITION OF AQUEOUS PH, OSMOLARITY, CONCENTRATION, STERILITY
James P. Gills, MD Affiliate Professor of Ophthalmology
University of South Florida Consulting Professor of Ophthalmology
Duke University Medical Center
EVOLUTION OF THE INTRACAMERAL REGIMEN
Financial Disclosure: Stockholder in Lenstec & Abbott Medical
Began by using antibiotics in irrigating solution 40 years ago Vancomycin
1/10,000 endophthalmitis Controlled dosage with postop A/C injection
35 years Vancomycin / Ceftazidime
75,000 routine cataract procedures Over 15 years
Each patient received dosage of 0.1cc equal to: Vancomycin 33.3mcg Dexamethasone 99mcg Ceftazidime 20mcg
No topical antibiotics No incidents of endophthalmitis

75,000 consecutive cataract implant procedures Over 14 years Performed by 40 ophthalmologists 30,000 Mackool pts. / 45,000 other surgeons
Each patient received: 0.1mg intracameral vancomycin in 0.1cc of BSS at the end of procedure
No Cases of endophthalmitis
44,554 routine cataract procedures Over 22 years
Each patient received: Bolus of Vancomycin in the bag and AC
4 Cases of presumed but not proved endophthalmitis = 0.0089%
5,000 routine cataract procedures Over 6 years
Each patient received: 0.05ml of Vigamox® in the AC at the close of
cataract surgery No incidents of endophthalmitis
12,192 routine cataract procedures Over 5 years
Each patient received: 0.1ml of 0.5% Moxifloxacin (Vigamox®) in
the AC at the end of cataract surgery No incidents of endophthalmitis No case of TASS or other major reaction
•
David B. Glasser, M.D.
Columbia, MD
BETTER SURGERY THROUGH CHEMICALS COMPOUNDING
REGULATORY CONSIDERATIONS
• USP
• FDA
• Congress
• State/local regulators
• Pharmacy boards
• OSHA/state OSHA
• Medical licensing boards
• Credentials committees
• Payers
• CMS
• TJC
• AAAHC
• AAAASF
• DNVHC
• CAHQ
• IRBs
WHO REGULATES US? USP SECTION 797
• Guidelines for compounded sterile preparations to reduce risk of:
• Microbial contamination
• Excessive bacterial endotoxins
• Variability in concentration
• Chemical and physical contaminants
• Poor quality ingredients
• Affects multi-use of compounded products in ASCs
• Interpreted and enforced by state and federal licensing agencies (TJC, AAAHC, AAAASF, etc.)
EVIDENCE-BASED REGULATION? • “My ASC was inspected by AAAHC as part of our Deemed Status triennial accreditation.
We use the Betadine solution that comes with the cataract eye pack. It turns out the Betadine 10% solution bottle is labeled ‘not for use on the eye’ and ‘not for ocular use.’ We all dilute this solution with saline prior to the skin/eye prep.
• “Getting this product onto the eye (for the sterile prep), even when deliberately diluting the Betadine solution to <5%, is a big CMS violation. ‘Not for use on the eye’ is regardless of its dilution. If you dictate that you place the Betadine into the cul de sac as part of your prep/drape, that would be evidence of a violation, and the inspectors will SHUT YOU DOWN today. That's what they tried to do with me.”
FDA • Regulatory mechanisms: drugs, devices, cells, tissues
• Approval process
• Good manufacturing practices (GMPs)
• Regulate companies rather than practitioners
• Less interested in “practice of medicine” issues
• High-risk, high-profile activities attract attention
• Compounding
• Increased interest: New England Compounding Center
• Fungal meningitis outbreak in 2012
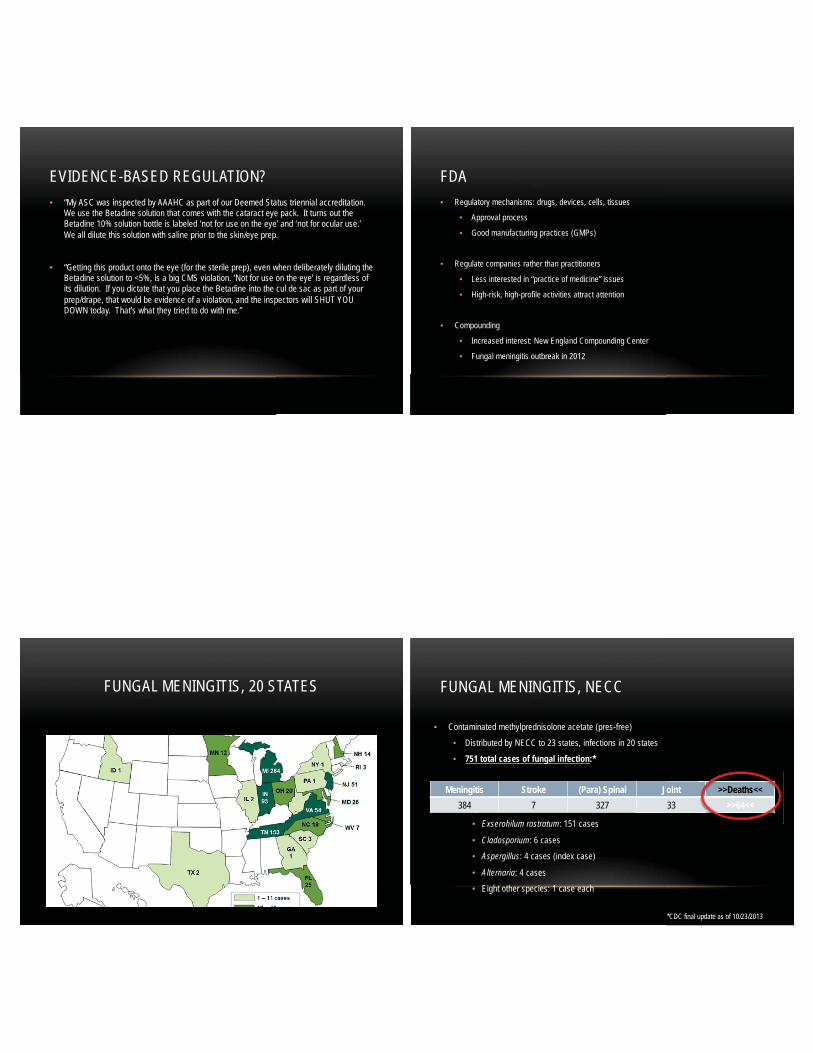
FUNGAL MENINGITIS, 20 STATES FUNGAL MENINGITIS, NECC
• Contaminated methylprednisolone acetate (pres-free)
• Distributed by NECC to 23 states, infections in 20 states
• 751 total cases of fungal infection:*
• Organisms identified
• Exserohilum rostratum: 151 cases
• Cladosporium: 6 cases
• Aspergillus: 4 cases (index case)
• Alternaria: 4 cases
• Eight other species: 1 case each
Meningitis Stroke (Para) Spinal Joint >>Deaths<< 384 7 327 33 >>64<<
*CDC final update as of 10/23/2013
>>Deaths<<>>64<<

NEW FEDERAL LEGISLATION
• Drug Quality and Safety Act (DQSA): empowers FDA
• Sterile compounding
• 503A facilities: “Traditional Compounders”
• Patient-specific prescriptions required
• 503B facilities: “Outsourcing Facilities”
• Subject to GMP-like regulations
• Can sell across state lines
• Can manufacture sterile product in advance of a prescription
• Current focus is on repackaging of bevacizumab (Avastin) and beyond use dates (BUD)
NEW STATE REGULATIONS • Varies by state
• New laws in some states
• Some state pharmacy boards have implemented stricter controls
INCREASED REGULATION
• New legislation: DQSA
• Increased FDA vigilance
• Intensified enforcement of existing regulations
• New pharmacy board regulations
• Inability to stock urgent/emergency medications
• Patient-specific prescription requirement
• Increased costs
• Decreased availability
PAYMENT REGULATIONS
• Cataract surgery drugs: CMS policy • Triamcinolone/moxifloxacin/vancomycin (TriMoxiVanc)
• Trans-zonular intraoperative injection
• Injection bundled into professional fee (66984, 66982)
• Medication cost bundled into facility fee
• Phenylephrine 1%/ketorolac 0.3% (Omidria)
• Placed into irrigating solution • No professional fee
• Awarded pass-through status for 24-36 months
• Facility bills separately
• Patient responsible for 20% co-pay

PAYMENT REGULATIONS • Intravitreal anti-VEGF injections
• Ophthalmologist purchases drug and bills CMS Part B the average sales price (ASP) plus 6%
• Higher earnings on ranibizumab and aflibercept
• Reimbursement publicly reported as Medicare payment
• Payer coverage policies for specific indications may vary
• Often based on FDA-approved indications
• May limit use of less-expensive bevacizumab
WHY DO WE NEED COMPOUNDING? Ophthalmology
What to look for in a compounding pharmacy

What to look for in a compounding pharmacy
PCAB Accreditation
What to look for in a compounding pharmacy Registered as outsourcing facility
What to look for in a compounding pharmacy
Quality Costs Money
What to look for in a compounding pharmacy
Standards of Compliance

What to look for in a compounding pharmacy
Lab Environment
What to look for in a compounding pharmacy
Certifications
What to look for in a compounding pharmacy
Quality Assurance
TASS
Toxic Anterior Segment Syndrome
Henry F. Edelhauser, PhD Emory University Atlanta, GA Daniel G. Dawson, MD University of Florida Gainesville, FL

• Acute inflammation of the anterior chamber of the eye following cataract surgery.
Toxic Anterior Segment Syndrome Recommendations
TASS task force recommendations For cleaning and sterilization of intraocular surgical
equipment (12/23/06). ASCRS AAO ASORN AORN APIC CDC FDA
TASS Force Data & Surgery Center Visits Highest risk
85%
43%
Inadequate cleaning and flushing of handpieces and instruments (residual of OVD’s)
Enzymatic cleaners and detergents Reusable small gauge cannulas Using preserved epinephrine Inadequate manual cleaning of instruments Re-use of single use surgical devices
TASS Force Data & Surgery Center Visits Causes of TASS lower frequency
Reuse of single use surgical devices No immediate cleaning of OVD’s from instruments Reuse of tubing for flushing, latex bulbs for irrigation Poor instrument maintenance (rust, autoclave residue) Improper use of prep solns, detergents, cleaners (Physohex, hibicliens, Ivory
Snow, etc) Failure to follow DFU, use of non-approved enzymatics Use of post-op ointment in clear cornea cases Touching of IOL or patient contact areas with instruments with gloved hands Wrong concentration of detergent and enzymatic cleaners Lack of routine cleaning and use of ultrasonic cleaners
43%
5%
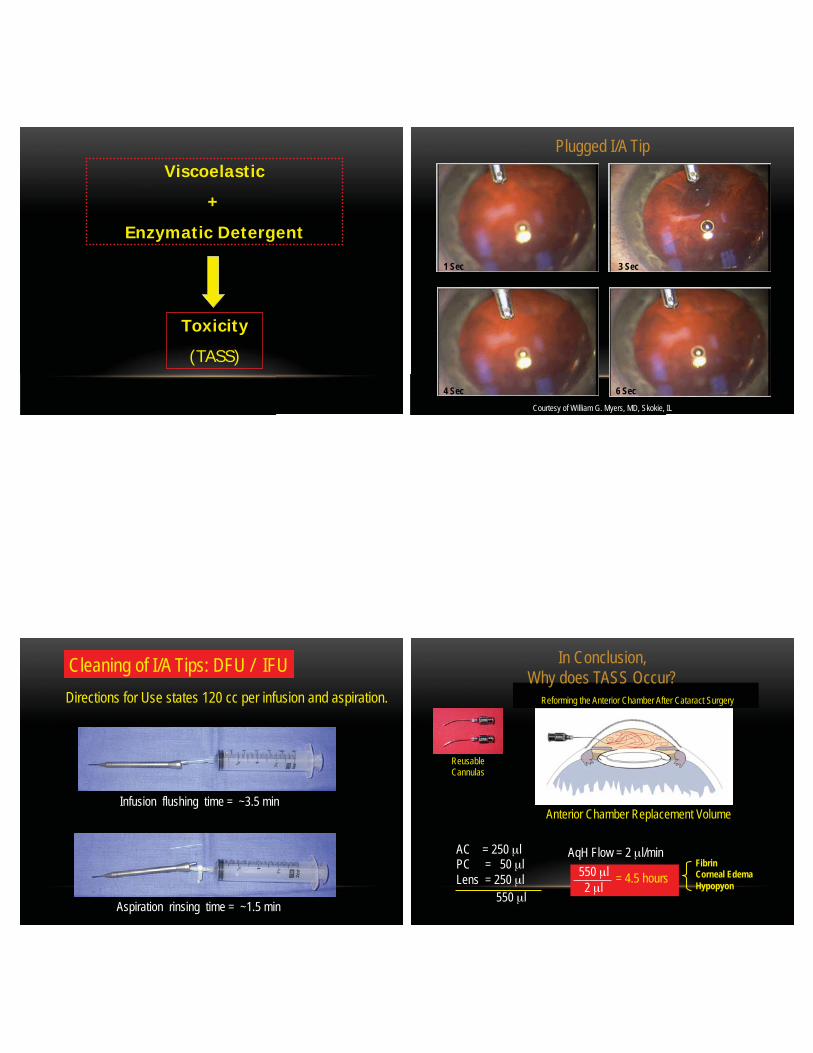
Viscoelastic
+
Enzymatic Detergent
Toxicity
(TASS)
Plugged I/A Tip
1 Sec 3 Sec
4 Sec 6 Sec Courtesy of William G. Myers, MD, Skokie, IL
Infusion flushing time = ~3.5 min
Cleaning of I/A Tips: DFU / IFU
Aspiration rinsing time = ~1.5 min
Directions for Use states 120 cc per infusion and aspiration.
Anterior Chamber Replacement Volume
AC = 250 μl PC = 50 μl Lens = 250 μl
550 μl
Reforming the Anterior Chamber After Cataract Surgery
Reusable Cannulas
In Conclusion, Why does TASS Occur?
AqH Flow = 2 μl/min 550 μl 2 μl
= 4.5 hours Fibrin Corneal Edema Hypopyon

TASS Common Offenders
Inadequate flushing of ophthalmic instruments and handpieces Use of enzymatic detergents Intraocular medications with preservatives Reuse of single use devices
Findings validate the need to follow the recommendations detailed in the TASS Force recommended practices document
Anesthetic Agents
Anesthetic agents block neurologic transmission indiscriminately Key enzymes are blocked resulting in transient lack of innervation Topical anesthetic come as esters and amides Anesthetic allergy is rare Most allergy is from excipients such as preservatives and bisulfites Side effects to contained epinephrine account for most systemic reactions
Anesthetic Agents
Topical length of action: Lidocaine 18 minutes, Tetracaine 45 minutes, Proparcaine 10 minute Intracamerally only lidocaine has been clinically tested 1% OK 15 minutes Care to only use methylparaben free MPF and not more than 1%
William G. Myers, M.D.
OPTIMIZING POVIDONE IODINE ANTISEPSIS OF MUCOUS MEMBRANES
Slides courtesy Jeroen van Roiij Rotterdam, The Netherlands
• 1811: Bernard Courtois: I2 + antiseptic
• iodination of lipids
• oxidation of cytoplasmic/membrane compounds
• Issues: Toxic, discoloration
Introduction
• 1955: Povidone Iodine = PVP Iodine = POIO
• PolyVinylPyrrolidone: a non surfactant carrier
• free I2: antiseptic/disinfectant, no resistance!1
• Surgery: chlorhexidine, alcohol vs 10% POIO2
Introduction What is POIO
• Before 2007: the only significant measure to prevent endophthalmitis after surgery1,2
• ESCRS: Intracameral ABX additional effect3
• Intracameral injection & POIO most important4
POIO in Ophthalmology
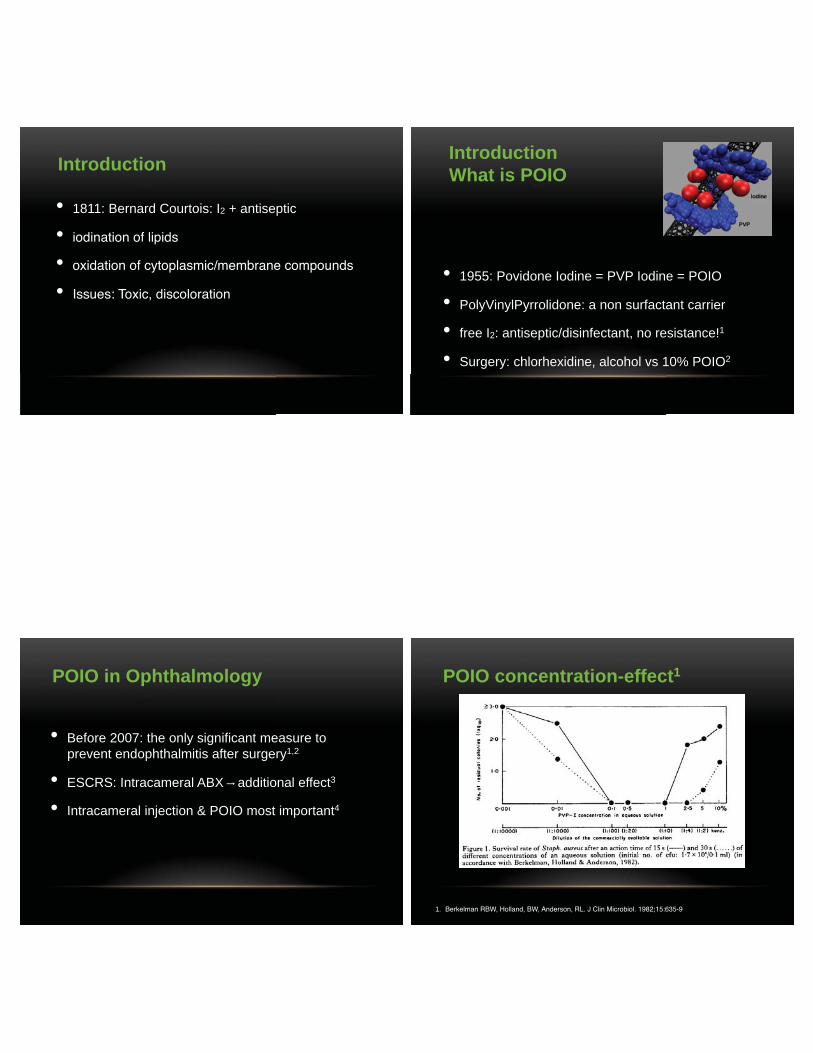
POIO concentration-effect1
1. Berkelman RBW, Holland, BW, Anderson, RL. J Clin Microbiol. 1982;15:635-9
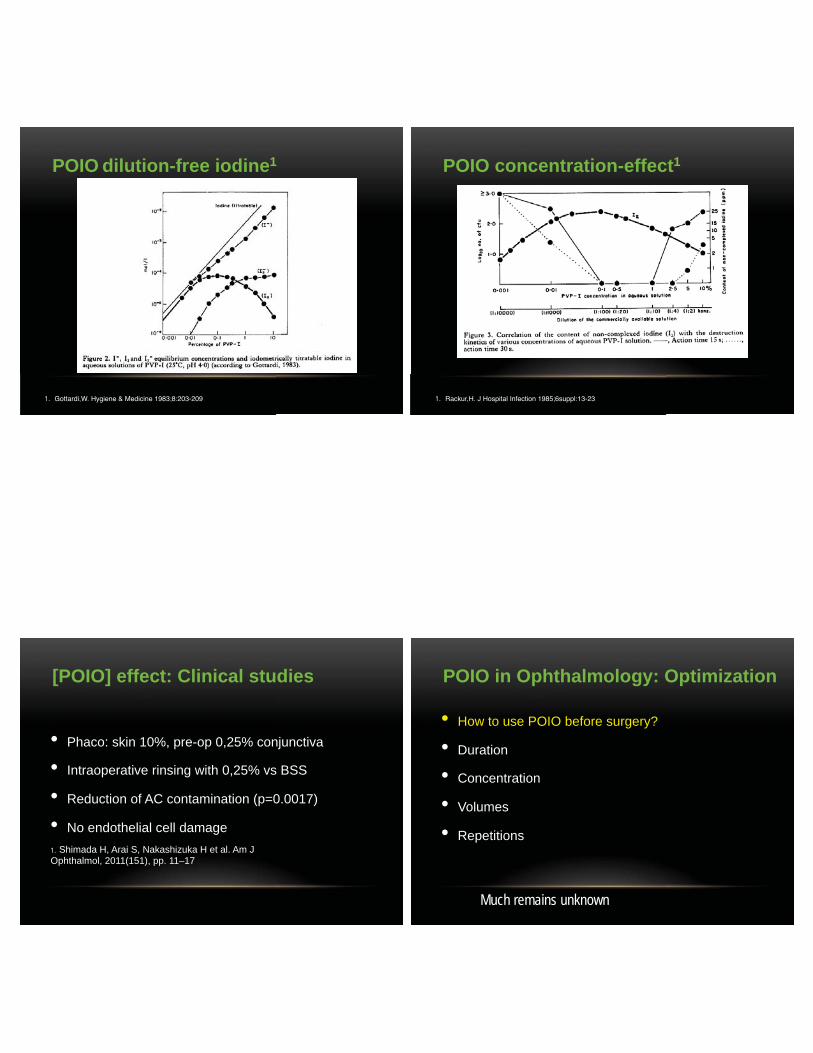
POIO dilution-free iodine1
1. Gottardi,W. Hygiene & Medicine 1983;8:203-209
POIO concentration-effect1
1. Rackur,H. J Hospital Infection 1985;6suppl:13-23
[POIO] effect: Clinical studies
1. Shimada H, Arai S, Nakashizuka H et al. Am J Ophthalmol, 2011(151), pp. 11–17
• Phaco: skin 10%, pre-op 0,25% conjunctiva
• Intraoperative rinsing with 0,25% vs BSS
• Reduction of AC contamination (p=0.0017)
• No endothelial cell damage
• How to use POIO before surgery?
• Duration
• Concentration
• Volumes
• Repetitions
POIO in Ophthalmology: Optimization
Much remains unknown

POIO IN OPHTHALMOLOGY: OPTIMIZATION • The preoperative conjunctival bacterial load, a well accepted surrogate
parameter for the risk for postoperative endophthalmitis, can be reduced by the use of povidone–iodine.
• The rate of postoperative endophthalmitis has declined over a 20-year period
• This decline in postoperative endophthalmitis coincided with an increase in the volume of povidone–iodine used in the preoperative preparation of the surgical field.
• Multiple factors might have contributed to this decline such as smaller and better corneal incisions.
POIO: how long & how concentrated?
• Lab studies: 15-30 sec; 30 sec; 5-10 min; 2 min.
• Skin: 1% shorter (1 min) than 10% (4 min)
• Microbiology conjunctiva:
10% 5 min. equivalent to 5% for 1 minute
• Lower concentrations work better
[POIO] SAFETY STUDIES
63
• Ocular surface toxicity (concentration dependent) • Allergic contact dermatitis (probably povidone or excipients)
• No cases of anaphylaxis
• Intravitreal injection of POIO: rabbit study
• Trost et al injected 50, 100, 200, 400 mcg of POIO in 16 rabbits
• No retinal damage: slit-lamp, ophthalmoscopy, ERG, histology
POTENTIAL FOR ENDOTHELIAL DAMAGE
• 5% POIO (Lerhaupt and Mauger)
• 1% POIO (Naor et al)
• 0.1% povidone-iodine* (Naor et al)
• (Entire aqueous replaced with POIO) • *Concentrations of PI tolerated by animal endothelium in vitro and in vivo were higher than
the reported bactericidal levels. (Naor)
• 0.025% no damage Nakashizu

Conclusions
• Povidone iodine is key in endophthalmitis prevention
• Lower concentration (0.25 -1%) probably most effective
• May dry the skin after 30 seconds before draping
• Generous volumes of POIO to the ocular surface (flush)
• Removes biofilm
• Increased free iodine if POIO lower
• Increased total free iodine if POIO longer
William G. Myers, M.D.
Assistant Professor
University of Chicago
Associate Professor
NorthShore Uni ersit Health S stem
HYPOCHLOROUS ACID: NOVEL MUCUS MEMBRANE ANTISEPTIC
Financial Interest, Employee of Leiter’s Compounding Pharmacy
Mucous Membrane Disinfection
CHLORINE SPECIES IS PH-DEPENDENT
pH 2
Molar
Per
centa
ge (%
)
7 10
100
0
50
Cl2 (aq)
OCl- HOCl
SEMMELWEIS
• Subsequently shown the key molecule in “bleach effect” is hypochlorous acid • Kills all bacteria, viruses and fungi on contact • Lives saved- maternal mortality rate decreased from 10% to 2% from 1842 to 1851

No wash
Soap wash
Calcium hypochlorite
HENRY DAKIN
Worked with Alexis Carrel to create a solution for the treatment of wounds during
World War I
ISSUES WITH ANTIBIOTICS 1. Frequently prescribed for viral infections
2. Widespread use in agriculture
3. No effect on biofilms- such problems constitute the majority of surgical infections
4. BACTERIAL EVOLUTION LEADING TO ANTIBIOTIC RESISTANCE
BIOFILM

HYPOCHLOROUS ACID DISINTEGRATES THE LIPIDS THAT COMPOSE THE CELL WALL AND THE BACTERIA IS UNABLE TO GENERATE ATP
THE PROTON GRADIENT OF EUKARYOTIC CELLS (ATP GENERATION IN THE MITOCHONDRIA) IS NOT AFFECTED BY HYPOCHLOROUS ACID
BODEN STUDY 2008 • Performed an in vitro study using blood agar plates as a
surrogate for the surface of the conjunctiva • Tested POIO on staph epi as well as other species • Proved that applying lidocaine gel 1% onto blood agar plates
before using POIO allowed bacterial growth • Recommended that POIO go on the conjunctiva first before
lidocaine gel.
Effect of lidocaine gel on povidone–iodine antisepsis and microbial survival John H. Boden, MD et.al. J Cataract Refract Surg 2008; 34:1773–1775
RESULTS • POIO Kills bacteria at high concentrations at 30 seconds
5% POIO
1% POIO
0.25% POIO
0.1% POIO
0.025% POIO

PRELIMINARY RESULTS • Lidocaine gel (1%,2%) applied to plates before POIO allowed for bacterial growth
Akten Gel (2%) + POIO Urojet (1%) + POIO
PRELIMINARY RESULTS HOCl has limited ability to kill staph epidermidis
HOCl .01%
HOCl .03%
30 secs 1 minute 0,3,6 minutes
SUMMARY OF FINDINGS IN THE LITERATURE AND PRESENT STUDY REGARDING EFFECTIVE AND SAFE POVIDONE-IODINE CONCENTRATIONS
PI Concentration 0.001 0.01 0.11.0 10
Vitreous concentration effective for endophthalmitis (rabbit) 0.013-10
Vitreous concentration safe for retina (rabbit) 0.027
Concentration safe for endothelial cells (in vitro) 0.05
Vitreous concentration effective for endophthalmitis and safe for retina (rabbit)
PI concentration used for vitreous irrigation in the present study
0.013-0.027
0.025one tenth of the 0.25% PI used for ocular surface disinfection
Brozou CG et al. Ophthalmic Res 2009
Trost LW et al. J Ocul Pharmaco Ther 2007
Naor J et al. J Cataract Refract Surg 2001
STERILE CONCENTRATE IN A 20 ML SINGLE-DOSE VIAL OF BSS-PLUS
Free iodine [ I2] iodine ion [ I - ]
Oxidized glutathione 4.6mg (C20H32N6O12S6) additives calcium chloride dehydrate (CaCl2 2H2O) magnesium chloride hexahydrate (MgCl2 ) dextrose (C6H12O6)
In BSS-PLUS, oxidized glutathione and other additives have a weak reducing action, which may promote transformation of free iodine to iodine ion with no antibacterial activity.
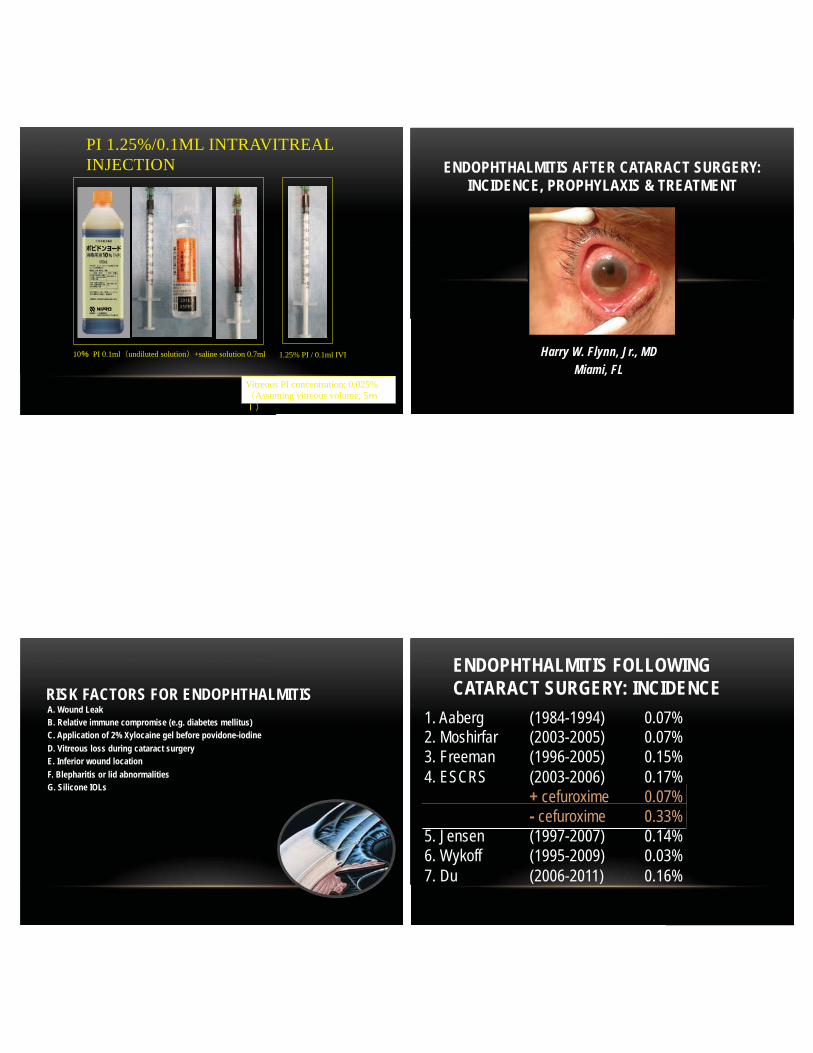
PI 1.25%/0.1ML INTRAVITREAL INJECTION
10 PI 0.1ml undiluted solution +saline solution 0.7ml 1.25% PI / 0.1ml IVI
Vitreous PI concentration; 0.025% Assuming vitreous volume; 5
Harry W. Flynn, Jr., MD Miami, FL
ENDOPHTHALMITIS AFTER CATARACT SURGERY: INCIDENCE, PROPHYLAXIS & TREATMENT
RISK FACTORS FOR ENDOPHTHALMITIS A. Wound Leak B. Relative immune compromise (e.g. diabetes mellitus) C. Application of 2% Xylocaine gel before povidone-iodine D. Vitreous loss during cataract surgery E. Inferior wound location F. Blepharitis or lid abnormalities G. Silicone IOLs
ENDOPHTHALMITIS FOLLOWING CATARACT SURGERY: INCIDENCE
1. Aaberg (1984-1994) 0.07% 2. Moshirfar (2003-2005) 0.07% 3. Freeman (1996-2005) 0.15% 4. ESCRS (2003-2006) 0.17% + cefuroxime 0.07%
- cefuroxime 0.33% 5. Jensen (1997-2007) 0.14% 6. Wykoff (1995-2009) 0.03% 7. Du (2006-2011) 0.16%

ENDOPHTHALMITIS FOLLOWING CATARACT SURGERY AT BASCOM PALMER EYE INSTITUTE
Year # / Total Incidence (%) 2000 1/ 2,949 0.03
2001 1/ 3,162 0.03
2002 0/ 3,434 0.00
2003 3/ 3,531 0.09
2004 1/ 3,082 0.03
2005 1/ 3,475 0.03
2006 1/ 3,699 0.03
2007 1/ 4,066 0.03
2008 1/ 4,219 0.02
2009 1/ 4,884 0.02
2010 0/ 4865 0.00
2011 0/ 5211 0.00
2012 3/ 4861 0.06
13 Year Total 14/ 49,616 0.03
METHODS OF PROPHYLAXIS 1. Preoperative povidone-iodine antisepsis
2. Preoperative topical antibiotics
3. Properly sized and constructed incision
4. Antibiotics in irrigating solution
5. Antibiotics injected into AC (intracameral)
6. Postoperative subconjunctival antibiotics
7. Postoperative topical antibiotics
POVIDONE-IODINE (PI): • Used as an antiseptic agent for the pre-operative
preparation of the skin and mucous membranes
• PI can cause allergic contact or irritant dermatitis (contact hypersensitivity), however this is rare and likely due to the povidone component. Anaphylactic reactions are RARE!
• The only alternative is topical chlorhexidine with risk of corneal endothelial damage
• Can be used at 0.05 to 0.1% per Vote study.
ESCRS STUDY A. 24 Ophthalmology units in Europe
B. Total of 14,000 patients
C. Clear corneal (5.88 X higher) vs. Scleral tunnel
D. Silicone IOL (3.13 X higher) vs acrylic IOL
E. Surgical complications (4.95 X higher) vs none

SHORTCOMINGS OF ESCRS REPORTS
A. Cefuroxime reconstituted from powder B. Short-term stability of mixed powder C. Cefuroxime not ideal for Staphylococcus D. Potential contamination of mixed powder
RISKS OF INTRACAMERAL ANTIBIOTICS
1. TASS - Related to mixing, concentration, buffering errors 2. CME - Reported in the use of intracameral vancomycin 3. Endothelial cell loss/toxicity 4. Retinal toxicity – Aminoglycosides
Vancomycin use discouraged NEWER RISK FACTORS FOR ENDOPHTHALMITIS
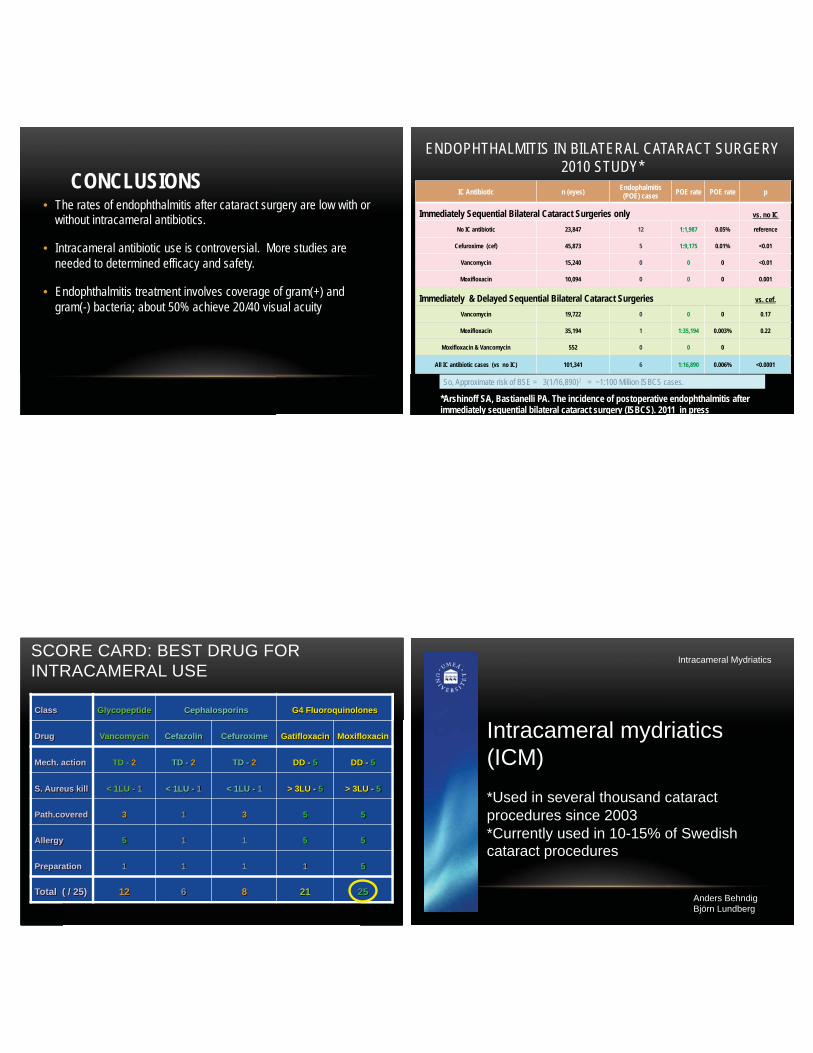
CONCLUSIONS • The rates of endophthalmitis after cataract surgery are low with or
without intracameral antibiotics.
• Intracameral antibiotic use is controversial. More studies are needed to determined efficacy and safety.
• Endophthalmitis treatment involves coverage of gram(+) and gram(-) bacteria; about 50% achieve 20/40 visual acuity
ENDOPHTHALMITIS IN BILATERAL CATARACT SURGERY 2010 STUDY*
IC Antibiotic n (eyes) Endophalmitis (POE) cases POE rate POE rate p
Immediately Sequential Bilateral Cataract Surgeries only vs. no IC
No IC antibiotic 23,847 12 1:1,987 0.05% reference
Cefuroxime (cef) 45,873 5 1:9,175 0.01% <0.01
Vancomycin 15,240 0 0 0 <0.01
Moxifloxacin 10,094 0 0 0 0.001
Immediately & Delayed Sequential Bilateral Cataract Surgeries vs. cef.
Vancomycin 19,722 0 0 0 0.17
Moxifloxacin 35,194 1 1:35,194 0.003% 0.22
Moxifloxacin & Vancomycin 552 0 0 0
All IC antibiotic cases (vs no IC) 101,341 6 1:16,890 0.006% <0.0001
*Arshinoff SA, Bastianelli PA. The incidence of postoperative endophthalmitis after immediately sequential bilateral cataract surgery (ISBCS). 2011 in press
So, Approximate risk of BSE = 3(1/16,890)2 = ~1:100 Million ISBCS cases.
SCORE CARD: BEST DRUG FOR INTRACAMERAL USE
Class Glycopeptide Cephalosporins G4 Fluoroquinolones
Drug Vancomycin Cefazolin Cefuroxime Gatifloxacin Moxifloxacin
Mech. action TD - 2 TD - 2 TD - 2 DD - 5 DD - 5
S. Aureus kill < 1LU - 1 < 1LU - 1 < 1LU - 1 > 3LU - 5 > 3LU - 5
Path.covered 3 1 3 5 5
Allergy 5 1 1 5 5
Preparation 1 1 1 1 5
Total ( / 25) 12 6 8 21 25
96
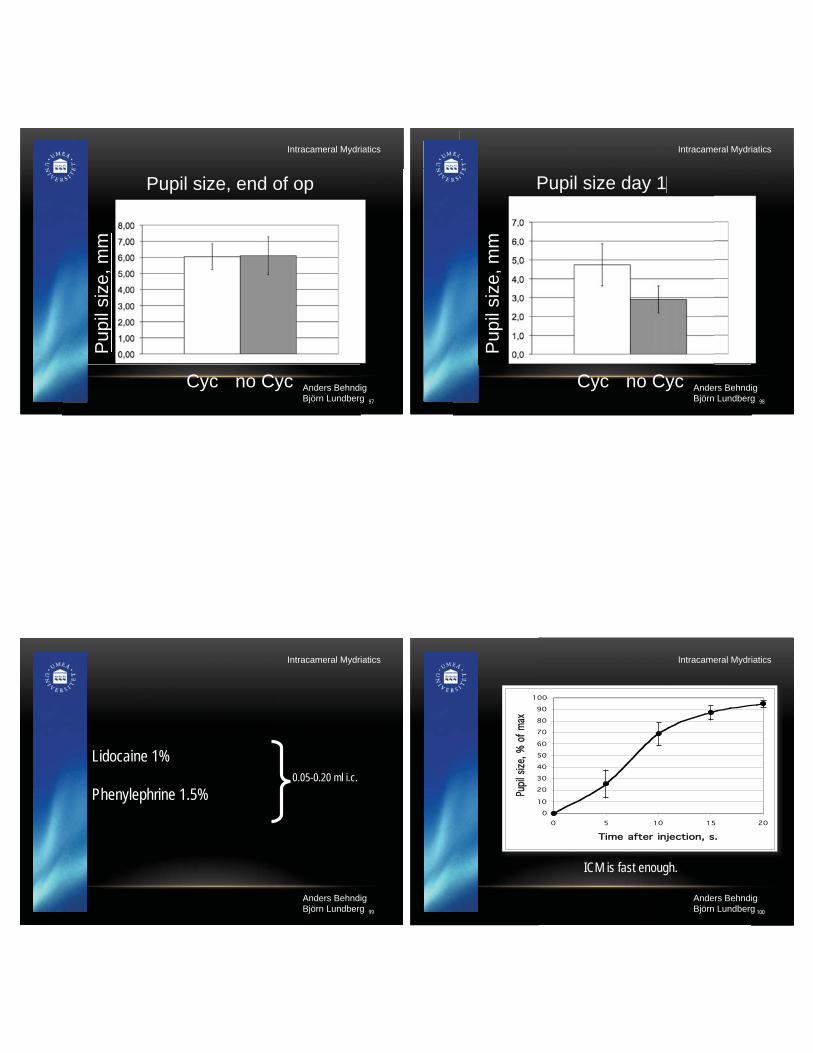
Intracameral mydriatics (ICM) *Used in several thousand cataract procedures since 2003 *Currently used in 10-15% of Swedish cataract procedures
Intracameral Mydriatics
Anders Behndig Björn Lundberg
97
Pupil size, end of op
Cyc no Cyc
Pup
il si
ze, m
m
Pupil size, end of op
Pup
il si
ze, m
m
Intracameral Mydriatics
Anders Behndig Björn Lundberg
98
Pupil size day 1 Pupil size day 1
Pup
il si
ze, m
m
Cyc no Cyc
Intracameral Mydriatics
Anders Behndig Björn Lundberg
99
Lidocaine 1% Phenylephrine 1.5%
0.05-0.20 ml i.c.
Intracameral Mydriatics
Anders Behndig Björn Lundberg
100
ICM is fast enough.
0
10
20
30
40
50
60
70
80
90
100
0 5 10 15 20
Time after injectioon, s.
Pupi
l si
ze,
% o
f m
ax
Intracameral Mydriatics
Anders Behndig Björn Lundberg

101
Corneal endothelial safety *Short term (1 month) *Long term (6 years)
No differences
Intracameral Mydriatics
Anders Behndig Björn Lundberg
102
Intracameral mydriatics, are they safe and effective?
Definitely
Intracameral Mydriatics
Anders Behndig Björn Lundberg
Enough
VISUALIZATION: DYES AND TRIAMCINOLONE
MINAS CORONEO
OUTBACK EYE SERVICE

KNOWING WHERE TO LOOK Before After
AIR INJURES ENDOTHELIUM
NORMAL
AIR
Çekiç, O et al. Am J Ophthalmol 2003;135:641-7
SAFETY
• Trypan blue does NOT decrease CCC tear resistance in human model • There is a considerable safety margin. • These observations are consistent with clinical experience.
• Findings confirmed by Mamalis et al, 2012

TRIAMCINOLONE USE IN ANTERIOR SEGMENT VITRECTOMY
Robert J Cionni MD
TRIAMCINOLONE USE IN ANTERIOR SEGMENT
VITRECTOMY
Kenalog injection into the anterior chamber provides better visualization of the
vitreous.
Visualizing vitreous using Kenalog suspension. Burk SE, Da Mata AP, Snyder ME, Schneider S, Osher RH, Cionni RJ. J Cataract Refract Surg. 2003 Apr;29(4):645-51.
TRIAMCINOLONE PREPARATION
• Aspirate 0.2cc Kenalog.
• Pass through filter.
• Captures Kenalog granules in filter.
• Push 5cc BSS through filter to rinse Kenalog.
• Re-suspend in 6cc syringe with BSS.
• Pass BSS through filter to capture Kenalog.
• Re-suspend in 6cc syringe with BSS again.
• Place in TB syringe (shake before use)
TRIESCENCE® NOW AVAILABLE
• Triamcinolone acetonide injectable suspension 40 mg/mL
• Recommended dose for visualization: 1 to 4 mg (25 to 100 microliters of 40 mg/mL suspension) intravitreally.
• Prefers to dilute 3:1 • Reduces post-op inflammation
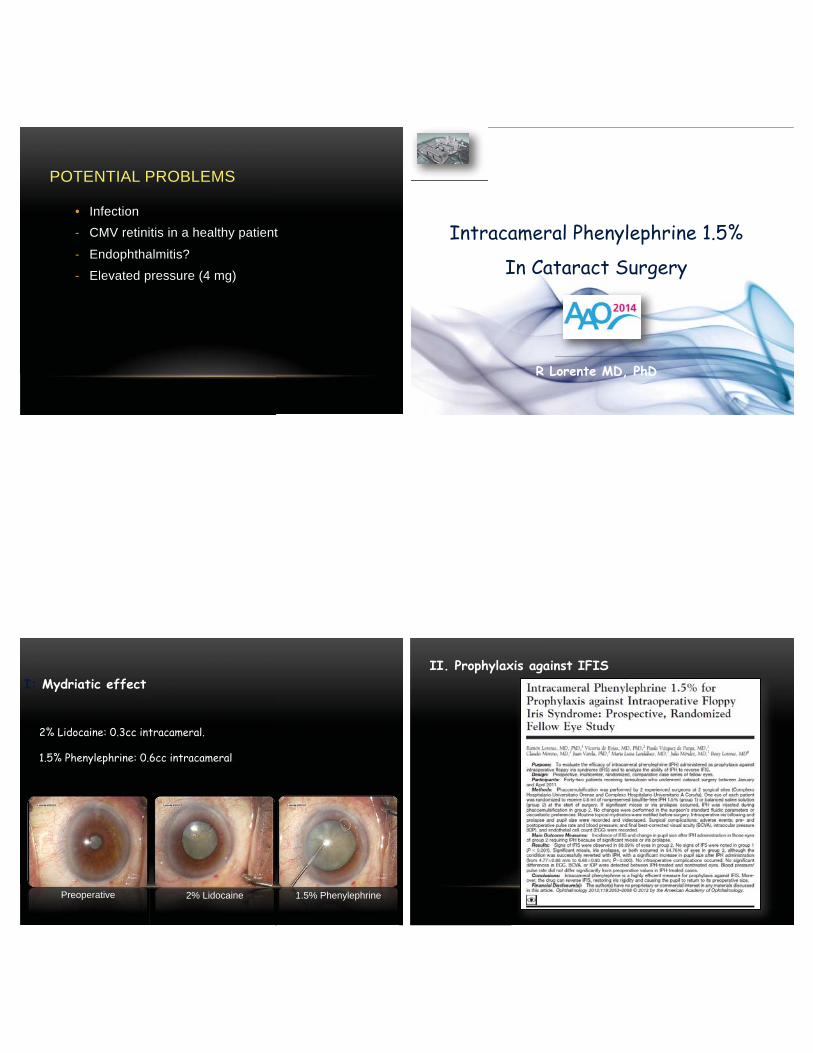
POTENTIAL PROBLEMS
• Infection - CMV retinitis in a healthy patient
- Endophthalmitis?
- Elevated pressure (4 mg)
Intracameral Phenylephrine 1.5%
In Cataract Surgery
R Lorente MD, PhD
Authors have no financial interest
2% Lidocaine: 0.3cc intracameral.
1.5% Phenylephrine: 0.6cc intracameral.
Preoperative 2% Lidocaine 1.5% Phenylephrine
I: Mydriatic effect II. Prophylaxis against IFIS

Results:
Signs of IFIS:
88% in group without phenylephrine
0% in group with phenylephrine
Significant miosis or iris prolapse or both:
54.7% in group without.
II. Prophylaxis against IFIS
54.76% were succesfully reversed with intracameral phenylephrine.
Increase in pupil size:
From 4.77 ± 0.88mm to 6.68 ± 0.93.
No signs of IFIS.
III. ABILITY TO REVERSE IFIS
No mydriatic drops are necessary to dilate the pupil.
IPH 1.5% is a highly effective measure for prophylaxis against IFIS.
Ability to restore the iris rigidity, causing the pupil to return to its
preoperative size.
CONCLUSION WHAT DOES IFIS LOOK LIKE?
T Yousef, accessed on YouTube 2012
122
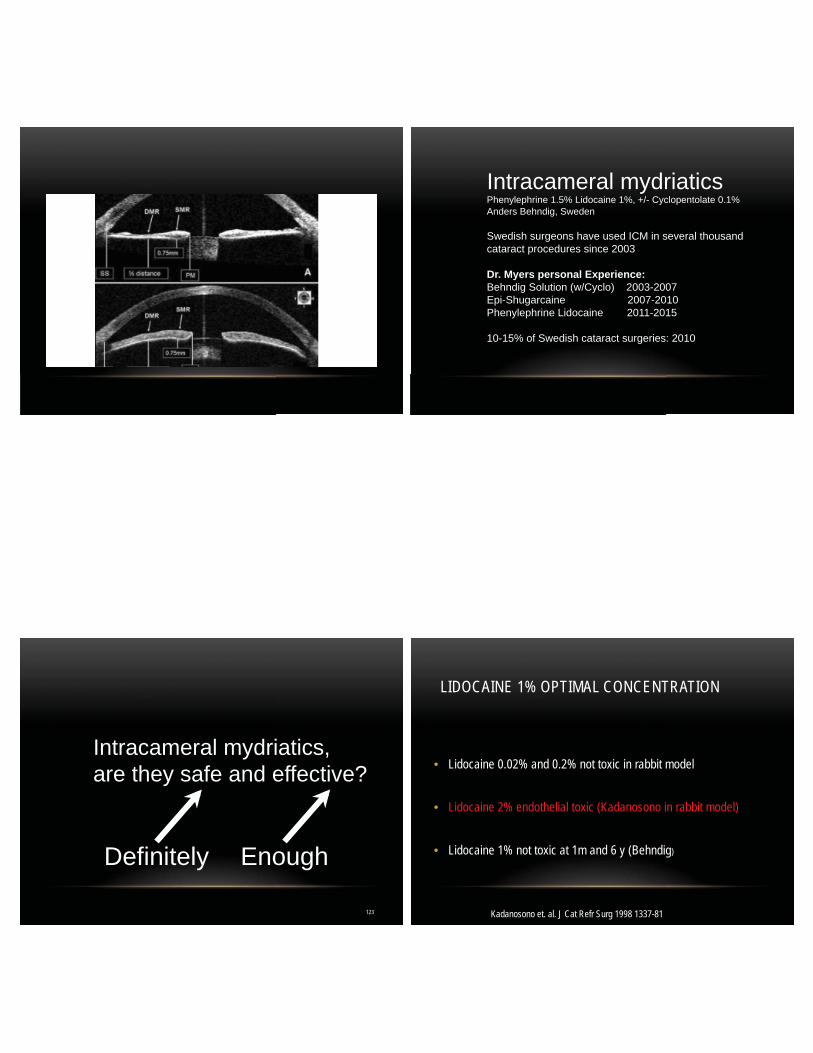
Intracameral mydriatics Phenylephrine 1.5% Lidocaine 1%, +/- Cyclopentolate 0.1% Anders Behndig, Sweden Swedish surgeons have used ICM in several thousand cataract procedures since 2003 Dr. Myers personal Experience: Behndig Solution (w/Cyclo) 2003-2007 Epi-Shugarcaine 2007-2010 Phenylephrine Lidocaine 2011-2015
10-15% of Swedish cataract surgeries: 2010
123
Intracameral mydriatics, are they safe and effective?
Definitely
Enough
LIDOCAINE 1% OPTIMAL CONCENTRATION
• Lidocaine 0.02% and 0.2% not toxic in rabbit model
• Lidocaine 2% endothelial toxic (Kadanosono in rabbit model) • Lidocaine 1% not toxic at 1m and 6 y (Behndig)
Kadanosono et. al. J Cat Refr Surg 1998 1337-81
125
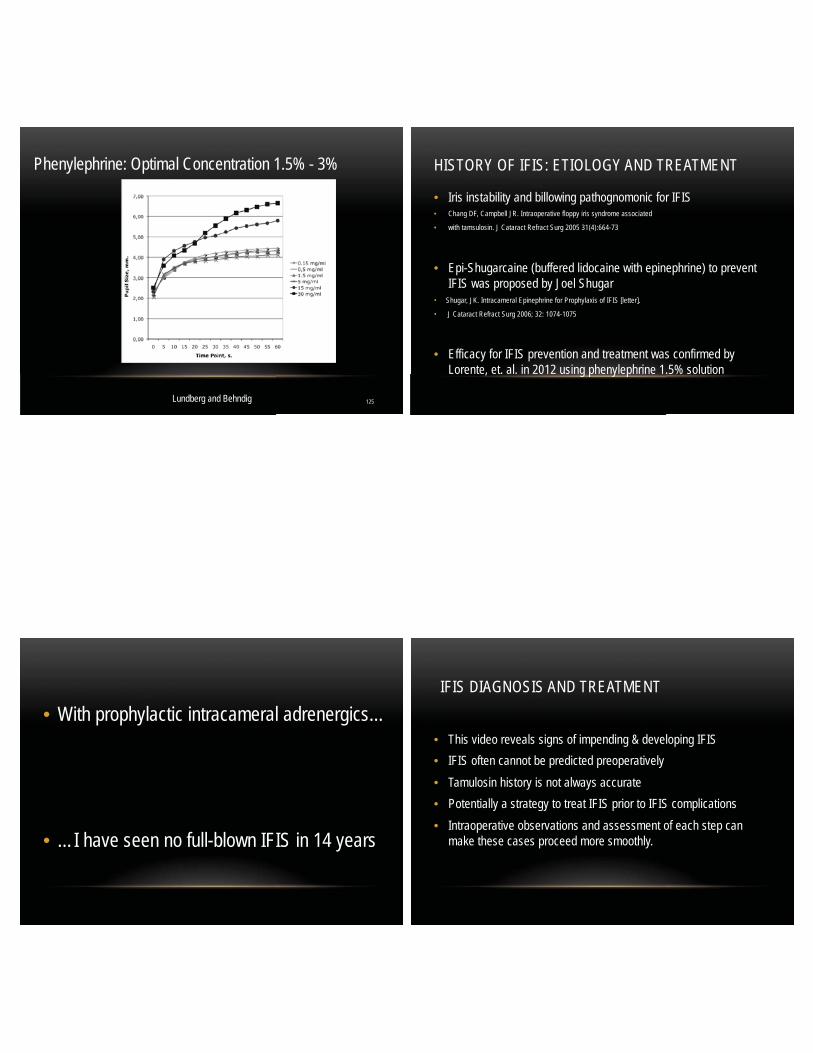
Phenylephrine: Optimal Concentration 1.5% - 3%
Lundberg and Behndig
HISTORY OF IFIS: ETIOLOGY AND TREATMENT
• Iris instability and billowing pathognomonic for IFIS • Chang DF, Campbell JR. Intraoperative floppy iris syndrome associated
• with tamsulosin. J Cataract Refract Surg 2005 31(4):664-73
• Epi-Shugarcaine (buffered lidocaine with epinephrine) to prevent IFIS was proposed by Joel Shugar
• Shugar, JK. Intracameral Epinephrine for Prophylaxis of IFIS [letter].
• J Cataract Refract Surg 2006; 32: 1074-1075
• Efficacy for IFIS prevention and treatment was confirmed by Lorente, et. al. in 2012 using phenylephrine 1.5% solution
• With prophylactic intracameral adrenergics…
• …I have seen no full-blown IFIS in 14 years
IFIS DIAGNOSIS AND TREATMENT
• This video reveals signs of impending & developing IFIS • IFIS often cannot be predicted preoperatively • Tamulosin history is not always accurate • Potentially a strategy to treat IFIS prior to IFIS complications • Intraoperative observations and assessment of each step can
make these cases proceed more smoothly.

IFIS INTRACAMERAL PHENYLEPHRINE LIDOCAINE DIAGNOSIS SIGNS TREATMENT THEORY OF IFIS
• This patient had a low risk of IFIS based on history alone: Female, No DM, PXF, nor previous IFIS meds
• Ectropion uveae and posterior bowing of the mid- peripheral iris is seen best supine, not at the slit lamp
• Dilator atrophy has been shown by histopathology • Lack of iris stiffness: gravitational sag of the mid- peripheral iris • Small intra-ocular pressure currents easily billow the flaccid iris
THEORY OF IFIS SIGNS
• Iris pointing toward the incision is an early intra-operative sign of IFIS, showing lack of Anterior Posterior rigidity
• Vermiform iris billowing movements with infusion of intracameral adrenergic agent in an undilated pupil as a stream
• Posterior bowing of the mid peripheral iris identified in undilated pupil
• This triad of signs gives advance warning of impending IFIS
• Early signs of IFIS can best be identified with an undilated pupil
• IFIS can be demonstrated early enough in the case to allow for proper management with PE, hooks or rings
STEPS TO MINIMIZE IFIS COMPLICATIONS
• Two paracenteses allow for chamber decompression
• Inject Intracameral phenylephrine 1.5% and lidocaine 1% slowly
• Infuse small aliquots to prevent AC over-pressurization and iris prolapse
• Perform capsulorhexis through a paracentesis with 23G or 20G micro-incisional capsule forceps or with a cystotome
• Insertion and removal of continuous-loop iris expansion devices can be difficult due to the lack of iris rigidity, hooks may be better
STEPS TO MINIMIZE IFIS COMPLICATIONS
• Do not overfill the eye with fluids • Keep the cannula in the eye • Decompress via the second paracentesis
• Allow time for the iris to stiffen: ~ 2 min
• Decision on iris hooks 2 min (pupil>4.8 mm)
• Enjoy the case as if no IFIS occurred!
IFIS CASE
Jeffrey T. Liegner, M.D.
Major Shareholder Imprimis
INTRAVITREAL ANTIBIOTICS AND STEROID
FOR DROP-LESS CATARACT SURGERY
Topical Antibiotics: Prophylaxis against most common organisms Broad spectrum coverage Fluoroquinolones and Gram Positive Penetration varies: drug concentration in eye Compliance issues (including accuracy) Cost issues: generic vs trade name drugs Treating Ocular Surface: Threat is inside eye
Vitreous is where the infection takes hold

Intraocular Antibiotics for Infection Prophylaxis
Combination drugs yield broadest spectrum: • Different antibiotics require different pH
• Concentrations vary based on target therapy
• Binders and stabilizers critical to avoid precipitation • Osmolarity and tonicity different for each drug
Intracameral Injection vs Intravitreal Placement • Anterior Chamber Volume Turnover: Washout Rate
• Two hours max retention in anterior chamber (250 µl at 2.5 µl/min)
• Trabecular Meshwork: outflow altered by drug
• Corneal Endothelium: drug concentration and toxicity • Intravitreal Depot: Bound into protein matrix • Drug retention and release gradually
• Transparent nature of ABX combination: not visualized
• Dexamethasone
• Soluble steroid in clear solution: minimum floaters • Short acting: clears intraocular space within four hours • Preservative Free is expensive (Single Dose Vials) • Not reimbursed by Medicare or insurance
• Triamcinolone acetonide • Suspension in buffered preservative free solution • Small particulate size required to transfer through cannula • Long acting drug: several weeks of immunosuppression • Suspends easily into vitreous • Reimbursed by insurance companies and Medicare (J3300)
Intraocular Medications to Reduce Inflammation
Intraocular Medications & Proactive Control: Anterior Chamber Placement of Steroid • Anterior chamber particulate creates pseudo-hypopyon • Particulate clogs trabecular meshwork: IOP spikes
• Intra-Vitreal Placement: Trans-Zonular Injection • 27ga or 30ga Cannula: Very tiny particulate size • Vitreous holds particulate for slow release • Floaters seen: 80% POD1, 20% POW1
• High safety, no zonular damage, easy to learn, quick delivery

INTRAVITREAL ANTIBIOTICS AND STEROID FOR DROP-LESS CATARACT SURGERY
Statistics: Endophthalmitis Rates and Inflammation Control • 3% to 7% require supplemental topical steroids:
• Usually 10-14 days postop, typical symptoms, quick to respond to topical
• No IOP elevation with <4mg triamcinolone • Endophthalmitis rate <0.005%, 10x lower than topical
• One infection in >20,000 cataract procedures
• CME rate (OCT): 1.8% in healthy eyes with cataract
• Compared to 5.79% (2010 Study, Law)
• NSAIDs not used unless clinically significant edema noted
CATARACT SURGERY PROPHYLAXIS
Neal Shorstein
COMPLICATIONS – PHACO • Endophthalmitis
• Rare
• 20% blindness
• Cystoid Macular Edema • Common (1-3%)
• Mild vision loss • Cost $
• Loss of faith
COMPLICATIONS – PHACO • Endophthalmitis
• Intracameral cefuroxime or moxifloxacin
• Cystoid Macular Edema • Subconjunctival triamcinolone
• NSAID • Epiretinal membrane
• Macular diabetic retinopathy
• Posterior capsular rupture

DROPS - RISKS • Expensive • Failure to:
• Order
• Pick up
• Instill
• Contamination
• Abrasion
• Trauma • Wound gape increases risk of endophthalmitis
ADVANTAGES – NO DROPS
• Definitive drug delivery • Where it counts (antibiotic)
• Peaks and Troughs • High peak – intracameral antibiotic • Sustained levels – subconjunctival triamcinolone
• Avoids contamination • Avoids trauma to eye
INTRACAMERAL – LARGE SERIES Author Time Period Surgeries Endoph Rate
(Intracameral) Rate Agent
Gimbel US
1990-1993 4,684 0/4,684 - vancomycin
Montan Sweden
1996-2000 32,180 1/1,609 4x cefuroxime
ESCRS 9 Countries
2003-2006 16,211 1/2,000 5x cefuroxime
Barreau France
2003-2008 5,115 1/2,289 28x cefuroxime
Friling Sweden
2005-2010 464,996 1/4,000 14x cefuroxime
Shorstein US
2007-2011 16,264 1/7,108 22x cefuroxime, moxifloxacin, vanc
Rodriguez-Caravaca Spain
2005-2012 19,463 1/2,574 15x cefuroxime
Matsuura Japan
2009-2012 18,794* 1/6,265 3x moxifloxacin
*Culture confirmed; conducted by survey
RESULTS – MODALITY
N – number of eyes
OR – odds ratio; Adjusted for calendar year, patient age, Charlson comorbidity, ocular comorbidity and posterior capsular rupture
CI – confidence interval
Endo - endophthalmitis
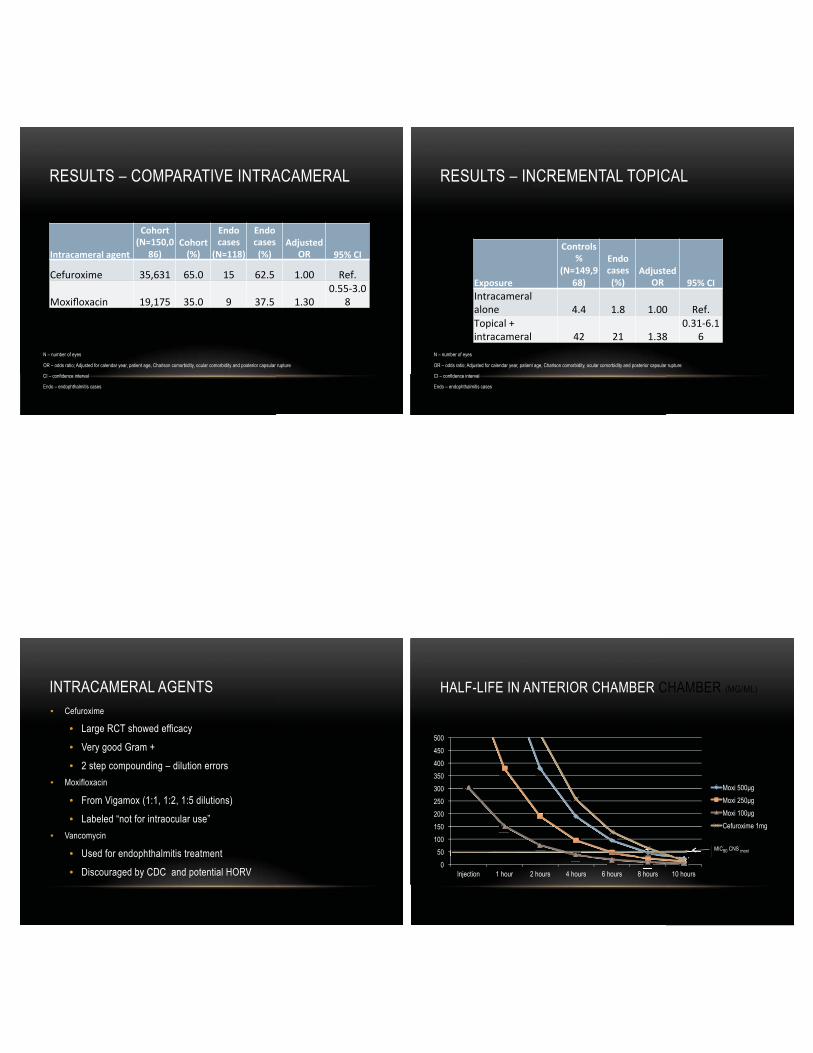
RESULTS – COMPARATIVE INTRACAMERAL
N – number of eyes
OR – odds ratio; Adjusted for calendar year, patient age, Charlson comorbidity, ocular comorbidity and posterior capsular rupture
CI – confidence interval
Endo – endophthalmitis cases
RESULTS – INCREMENTAL TOPICAL
N – number of eyes
OR – odds ratio; Adjusted for calendar year, patient age, Charlson comorbidity, ocular comorbidity and posterior capsular rupture
CI – confidence interval
Endo – endophthalmitis cases
INTRACAMERAL AGENTS • Cefuroxime
• Large RCT showed efficacy
• Very good Gram +
• 2 step compounding – dilution errors • Moxifloxacin
• From Vigamox (1:1, 1:2, 1:5 dilutions)
• Labeled “not for intraocular use” • Vancomycin
• Used for endophthalmitis treatment
• Discouraged by CDC and potential HORV
HALF-LIFE IN ANTERIOR CHAMBER CHAMBER (ΜG/ML)
0 50
100 150 200 250 300 350 400 450 500
Injection 1 hour 2 hours 4 hours 6 hours 8 hours 10 hours
Moxi 500μg Moxi 250μg Moxi 100μg Cefuroxime 1mg
MIC90 CNS moxi

ANTIBIOTICS • Use intracameral antibiotics 100% of the time • May not matter which one you use • Topical drops may not add effectiveness
• Especially with well constructed wounds
INJECTIONS – STEROID • Subconjunctival triamcinolone
• 2mg 5mm inferior to limbus
• Accessible, Visible location
• Painless
• Goal dissolving in 1-2 months
STEROID CONCENTRATION (2MG)
0.05mL of 40mg/mL 0.2mL of 10mg/mL
RESULTS • 2013 (ASCRS)
• 1000 non-glaucoma patients
• CME Incidence 0.85%
• Quiet eyes
• IOP spike 1% (30-40mmHg); resolved with drops or excision
• 2014 (preliminary results)
• Adjusted Odds Ratio similar to topical prednisolone
• Diclofenac and flurbiprofen reduced Odds Ratio by ½
• Ketorolac not effective
• Subgroup analysis of ERM, PCR, Macular DR, AMD
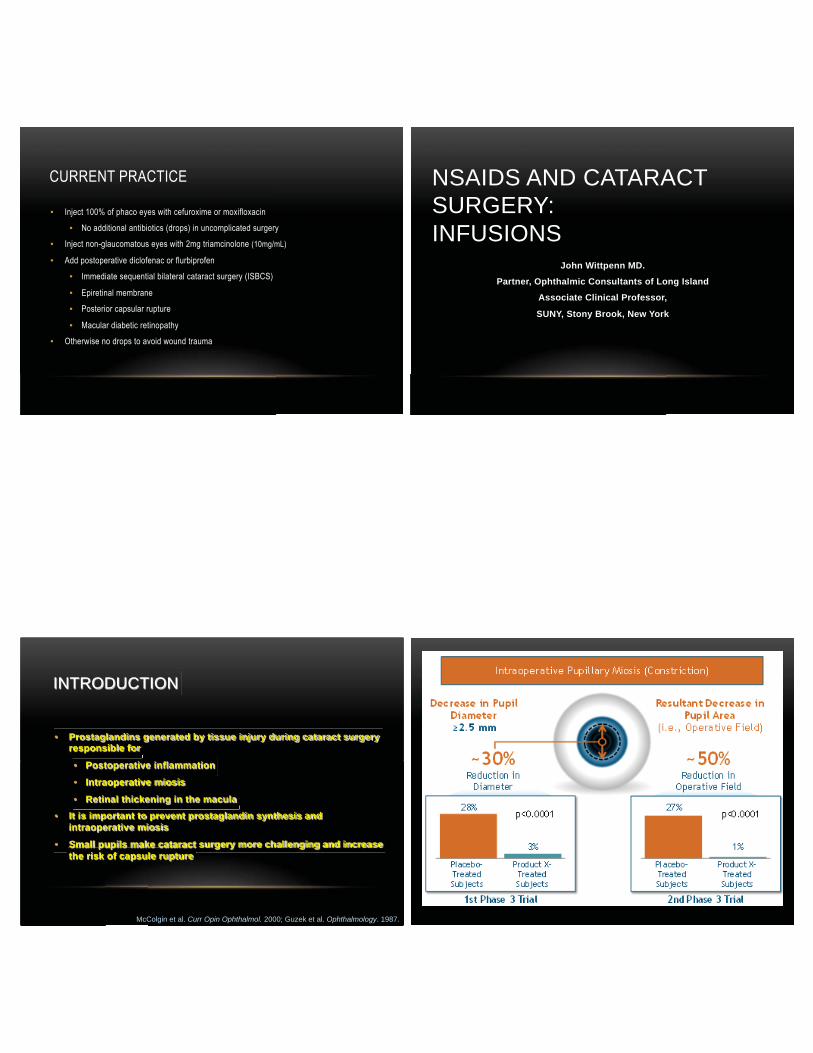
CURRENT PRACTICE
• Inject 100% of phaco eyes with cefuroxime or moxifloxacin
• No additional antibiotics (drops) in uncomplicated surgery
• Inject non-glaucomatous eyes with 2mg triamcinolone (10mg/mL)
• Add postoperative diclofenac or flurbiprofen
• Immediate sequential bilateral cataract surgery (ISBCS)
• Epiretinal membrane
• Posterior capsular rupture
• Macular diabetic retinopathy
• Otherwise no drops to avoid wound trauma
NSAIDS AND CATARACT SURGERY: INFUSIONS
John Wittpenn MD.
Partner, Ophthalmic Consultants of Long Island
Associate Clinical Professor,
SUNY, Stony Brook, New York
INTRODUCTION
• Prostaglandins generated by tissue injury during cataract surgery responsible for
• Postoperative inflammation
• Intraoperative miosis
• Retinal thickening in the macula • It is important to prevent prostaglandin synthesis and
intraoperative miosis
• Small pupils make cataract surgery more challenging and increase the risk of capsule rupture
McColgin et al. Curr Opin Ophthalmol. 2000; Guzek et al. Ophthalmology. 1987.
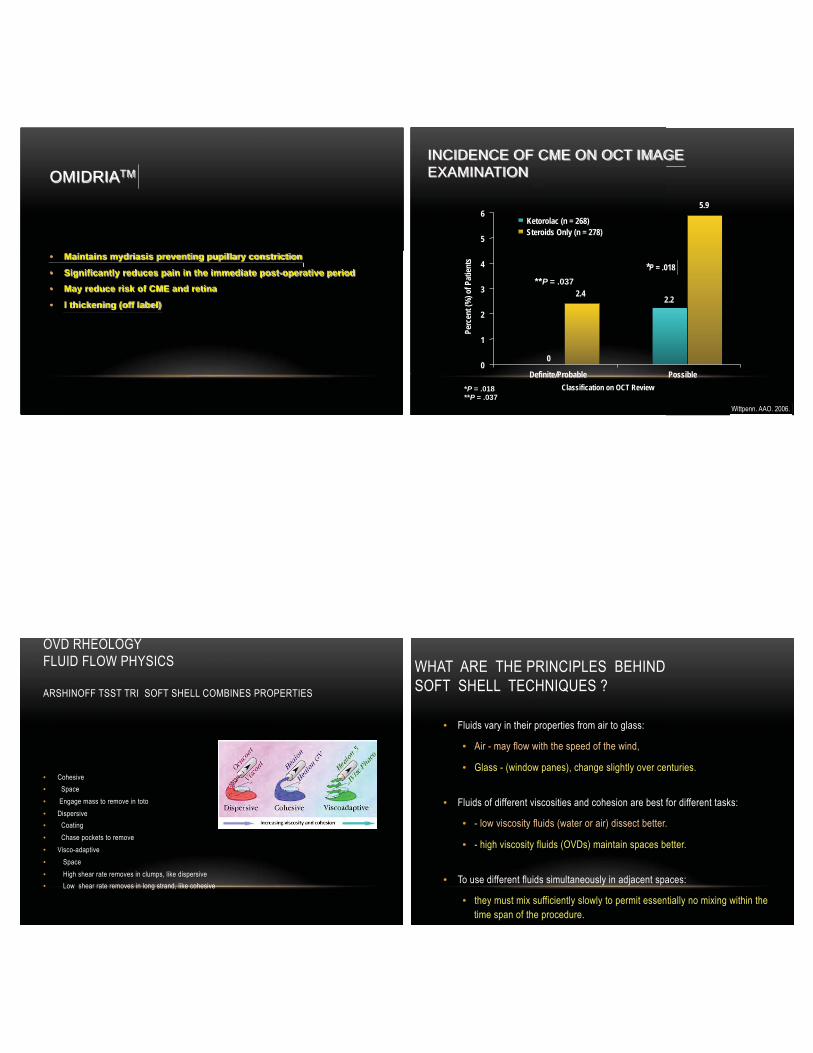
OMIDRIATM
• Maintains mydriasis preventing pupillary constriction
• Significantly reduces pain in the immediate post-operative period
• May reduce risk of CME and retina
• l thickening (off label)
INCIDENCE OF CME ON OCT IMAGE EXAMINATION
*P = .018 **P = .037
Wittpenn. AAO. 2006.
Perc
ent (
%) o
f Pat
ients
Classification on OCT Review
**P = .037
0
2.4 2.2
5.9
0
1
2
3
4
5
6
Definite/Probable Possible
*P = .018
Ketorolac (n = 268) Steroids Only (n = 278)
OVD RHEOLOGY FLUID FLOW PHYSICS ARSHINOFF TSST TRI SOFT SHELL COMBINES PROPERTIES
• Cohesive • Space • Engage mass to remove in toto • Dispersive • Coating • Chase pockets to remove • Visco-adaptive • Space • High shear rate removes in clumps, like dispersive • Low shear rate removes in long strand, like cohesive
WHAT ARE THE PRINCIPLES BEHIND SOFT SHELL TECHNIQUES ?
• Fluids vary in their properties from air to glass:
• Air - may flow with the speed of the wind,
• Glass - (window panes), change slightly over centuries.
• Fluids of different viscosities and cohesion are best for different tasks:
• - low viscosity fluids (water or air) dissect better.
• - high viscosity fluids (OVDs) maintain spaces better.
• To use different fluids simultaneously in adjacent spaces:
• they must mix sufficiently slowly to permit essentially no mixing within the time span of the procedure.
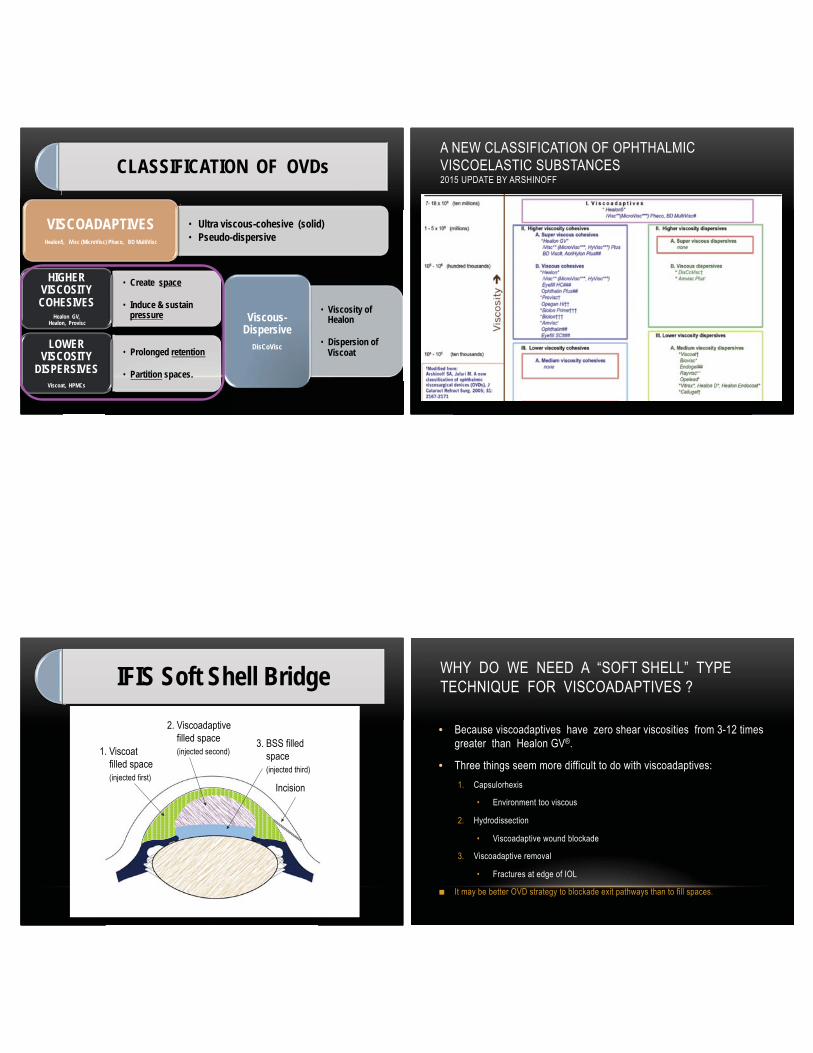
CLASSIFICATION OF OVDs
• Create space
• Induce & sustain pressure
HIGHER VISCOSITY COHESIVES
Healon GV,
Healon, Provisc
• Prolonged retention
• Partition spaces.
LOWER VISCOSITY
DISPERSIVES
Viscoat, HPMCs
• Viscosity of Healon
• Dispersion of Viscoat
Viscous- Dispersive
DisCoVisc
• Ultra viscous-cohesive (solid) • Pseudo-dispersive
VISCOADAPTIVES
Healon5, iVisc (MicroVisc) Phaco, BD MultiVisc
A NEW CLASSIFICATION OF OPHTHALMIC VISCOELASTIC SUBSTANCES 2015 UPDATE BY ARSHINOFF
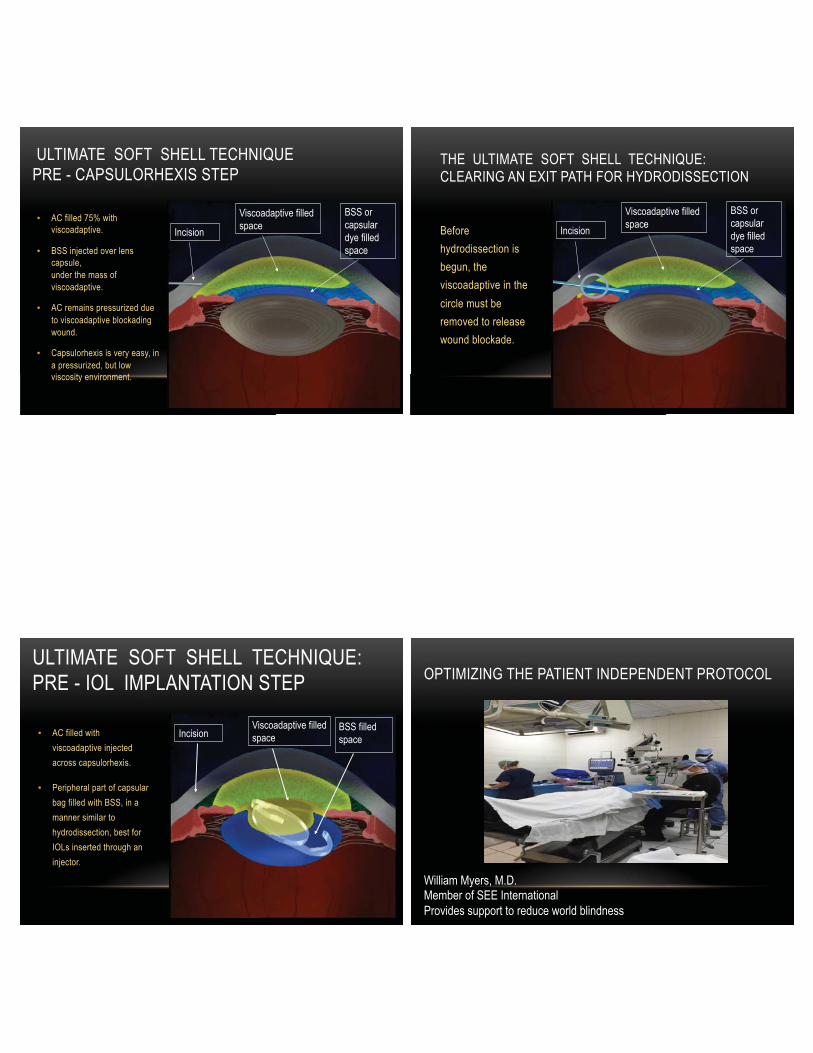
Incision
1. Viscoat filled space (injected first)
2. Viscoadaptive filled space (injected second) 3. BSS filled
space (injected third)
IFIS Soft Shell Bridge WHY DO WE NEED A “SOFT SHELL” TYPE TECHNIQUE FOR VISCOADAPTIVES ?
• Because viscoadaptives have zero shear viscosities from 3-12 times greater than Healon GV®.
• Three things seem more difficult to do with viscoadaptives: 1. Capsulorhexis
• Environment too viscous
2. Hydrodissection
• Viscoadaptive wound blockade
3. Viscoadaptive removal
• Fractures at edge of IOL
■ It may be better OVD strategy to blockade exit pathways than to fill spaces.
ULTIMATE SOFT SHELL TECHNIQUE PRE - CAPSULORHEXIS STEP
• AC filled 75% with viscoadaptive.
• BSS injected over lens capsule, under the mass of viscoadaptive.
• AC remains pressurized due to viscoadaptive blockading wound.
• Capsulorhexis is very easy, in a pressurized, but low viscosity environment.
Incision
Viscoadaptive filled space
BSS or capsular dye filled space
Incision
Viscoadaptive filled space
BSS or capsular dye filled space
THE ULTIMATE SOFT SHELL TECHNIQUE: CLEARING AN EXIT PATH FOR HYDRODISSECTION
Before hydrodissection is begun, the viscoadaptive in the circle must be removed to release wound blockade.
ULTIMATE SOFT SHELL TECHNIQUE: PRE - IOL IMPLANTATION STEP
• AC filled with viscoadaptive injected across capsulorhexis.
• Peripheral part of capsular bag filled with BSS, in a manner similar to hydrodissection, best for IOLs inserted through an injector.
BSS filled space Incision
Viscoadaptive filled space
OPTIMIZING THE PATIENT INDEPENDENT PROTOCOL
William Myers, M.D. Member of SEE International Provides support to reduce world blindness

MOTIVATION FOR PATIENT INDEPENDENT PROTOCOLS
• World burden of functional blindness • Cataract major cause of treatable blindness • Antibiotics, medications often not available • Cost a real issuer in developing world • Patients are burden to family • Surgical treatments are a one time intervention • We want to provide a turnkey process
WHAT DO WE EXPECT THE PATIENT TO DO?
• Preoperative Antibiotic Drops: • buy, pay, use, evidence for use? • Arrive an hour prior for dilation: 9+ additional drops • Tolerate the prep with 5% Povidone Iodine • sting, burn, frequent blinking • Not touch their eyes and lids: bacterial release • tight wad of facial tissue
All of these factors contradict each other
WHAT DO WE EXPECT THE PATIENT TO DO?
• Look at the light: • Have you ever looked at the light yourself? • Hold Still: • fear, pressure, pain, anxiety • Postoperative Drops: • buy, pay, use, taper • Do not press on eye: • but desire to wipe the eye • GoodRx PT $4 V 166, Generic vs brand
All of these factors contradict each other
WHAT DO WE EXPECT OUR STAFF TO DO?
• Large portion of counseling time involves drops • Patients call in questions about drops • “Doctor, do you know what they want for the drops?” • “Could you change these to generics?” • “The drops sting”, especially with generic alternatives
Time Time Time … is on our side …NOT
WHAT DO WE EXPECT OUR NURSES TO DO?
• Give 3 sets of drops several minutes apart • Prep the patient after initial anesthetics • Gels vs drops for anesthesia • Patient complains of pain of the prep
• Advise the patient about the things they will perceive
Time Time Time …is on our side … NOT WHAT ARE DOCTORS CONCERNED WITH ?
• Infection: what works: topical, • Wounds, draping, intracameral antibiotics • Dilation: what is sufficient, IFIS • Sedation: over/under, anesthesia care • Immobility: dementia, RLS, Sleep apnea • Pain: topical, intracameral, block
Evidence Based Decisions
WHAT CAN WE GIVE?
• Antibiotics: drape, gel, IC v BAK toxicity • Antiseptics: Betadine: %, chlorhexidine 0.1% • NSAIDs: preop / postop Cost to treat? • Steroids: routes, dose, steroid responses • Sedatives: routes, options
Drugs and Antiseptics OPTIONS:
• Antibiotics: • Preop, intraop, postop and routes • HORV, MICs, compliance issues • Steroids: • Subconjunctival, intracameral, intravitreal, topical • Complications: glaucoma, iritis, duration, cloud • NSAIDS: • Oral, topical, intraocular, which agent, toxicity
Infection and Inflammation

OPTIONS
• Dilation: • Topical, intracameral, IFIS prophylaxis • Topical cycloplegic: toric lens • Omidria: • Cost, Duration: Cascade or Suppress Theory
Dilation and IFIS COMBINATIONS
• 503a or 503b • Combo drops • Gatifloxacin, Nepafenac, Prednisolone acetate • Intracameral • Triamcinolone acetate, moxifloxacin, +/- vancomycin • Ideally validated for: stability, interactions • Less RN time to dispense, less BAK, wiping • Routes: Transzonular, Intravitreal via pars plana
503a and 503b Compounders
ADVANTAGES OF NO DROPS
• Are post op drops needed? • Wounds suck (Ian Francis) • Defined dose given above MBC • No patient charging allowed • CMS bans added patient fees
DISADVANTAGES OF INTRAVITREAL
• Patient sees a cloud for days • Surgeon visualization is impaired • Intravitreal pressure effects: iris, lens • Steroid response treatment options • Solitary peer reviewed article
Steroid issues

ADVANTAGES OF 503B COMPOUNDING
• Each batch must be tested for: • Sterility and Endotoxin testing • Stability testing to BUD • BUD (beyond use dating, similar to expiration date) • Pre-shipment quarantine 14 days • FDA monitoring of facilities • ISO 5 level environment
Product provenance and testing WHAT I DO
• No preoperative drops • Patient arrival <30 min prior • Nurses give no dilating drops • Topical lidocaine, no gels • Betadine 1% 30 seconds flush • Repeat last 2 steps on call to OR • Repeat last 2 steps once speculum is in
Preoperative
MY ASC ORDERS
• In Preop • Lidocaine drops on cornea • Paint eyelid area with Alcon 5% povidone iodine • Leave Povidone Iodine on skin to dry. • Povidone iodine 1% 10 seconds flushing
• Repeat entering OR and after speculum placed
OR ORDERS
• OPERATING ROOM • Instill several drops of MPF 2% lidocaine on eye • Vigorous flush with 1% povidone Iodine solution • Anesthetic + povidone iodine flush after speculum • 0.25% povidone iodine in small BSS bottle • Apply to cornea every few seconds instead of BSS

WHAT I DO
• Paracentesis • Phenylephrine 1.5% and Lidocaine 1% • 0.3 mL, after shallowing the AC • Intraoperative wetting with 0.25% Povidone iodine • replaces BSS squeeze bottle 0.8 mL in 15 mL BSS
• Recent Japanese work topical PVI 0.025% effective eradicating AC CFUs
Intraoperative, near beginning of case WHAT I DO
• Subconjunctival 3mg Triamcinolone acetate • bulbar subconjunctival inferior to lower lid margin
• Moxifloxacin 3mL bottle • Diluted in 7mL BSS in hood by pharmacist • Dosed QS (<1mL) to fill, seal the eye: mid-stromal hydration • Alternatively, 1mL vial 0.15% moxifloxacin from compounder
• Reapply lidocaine 1% • Povidone iodine 1% flush
Intraoperative, near end of case
WHAT I DO
• No patch • No shield except night for 3 days • No post operative drops • NSAID drops, only if ERM,DME,PCR • Oral NSAID option, if GI ok and OSD
Postoperative simplified COLLEAGUES AND MENTORS
• Hank Edelhauser • Joel Shugar • Minas Coroneo • Sam Masket • Steve Arshinoff • Anders Behndig • Ramon Lorente • Hiroyuki Shimada • Hiroyuki Nagashizaka • David Glasser • Jim Gills • Gholam Peyman • Steve Charles • Harry Flynn • Jeroen van Roiij • Chuck Leiter • And all the others who have participated in Better Surgery through Chemicals over the years
THANK YOU FOR YOUR ATTENDANCE PLEASE REVIEW THIS COURSE