latest 19 may 2014
DESCRIPTION
year 5TRANSCRIPT

General Surgery Curriculum
FF5126 Module Head :Dr (Ms). Saladina Jaszle Binti Jasmin
Assistant: Dr (Mr).Azlanuddin bin Azman
I.INTRODUCTION
During the 7 week posting, the students will initially be given a week of refresher course which will includeseminars andlectureson specific topics plus demonstrations
on basic surgical procedures (Appendix 1). Following this, they will bedivided into 2 groups; each group will be required to spend a 3 week rotation each in UKMMC and TelukIntan Hospital (Appendix 2). The group at UKMMC will be further divided
based on the 5 units in General surgery consisting of ;
1. Breast and Endocrine Surgery 2. Colorectal Surgery 3. Hepatobiliary Surgery
4. Vascular Surgery 5. Minimally Invasive Surgery
These subgroups will consist of 5-15 students who will be taught by 5-10 lecturers. Each lecturer is required to teach at least weekly for a minimum of an hour.
However,the leaders of these subgroups are responsible to contact the lecturers
themselves, early in the posting, to arrange for these teaching sessions which are usually conducted in the wards. Other additional teaching sessions usually take place
in the operation theatres, clinics and endoscopy suites. Students are exposed to the concept of senior clerkship during their surgical attachment. The senior clerkship
serves to prepare the students to become familiar and competent in handling common surgical cases and perform simple day-to-day procedures as surgical house officers.The current module will give more emphasis in basic surgical emergencies
and procedures. Apart from these, the general surgical posting also impartsthe personal and professional development module in the training. In line with the senior
clerkship concept, the students are required to go on-call and perform as “Junior House Officers”.
All tasks(performed/observed) by the students must be immediately documented in their respective log books(Appendix 3) for verification/grading purposes by the
supervising doctors/staff. At the end of each 3 week posting, the students need to get their supervisors’ report. Each student should at the end of the surgical posting have a total of 2 supervisor’s report; one from Teluk Intan Hospital and one from UKMMC.
The Friday of the 5th week of posting is the dateline to submit a case report to the
office for stamping of date of reception; those submitted thereafter will be rejected & the student will be given a zero for his/her case write-up. The end of posting test will be held in the surgical wards in UKMMC on the last day.Having completed the
surgical posting, the students are expected to have acquired the necessary surgical knowledge and skills to enable them to be proficient house officers.

Year5 UKMMC General Surgery 2012/13
TelukIntan Hospital
Teaching Faculty :-
1) Mr Lewellyn Rajakumar-General Surgeon 2) Mr Mohan Gopalakrishnan – General Surgeon 3) UKM Lecturer from the Surgical Department – One lecturer per week for 2 sessions (1-2hours/session)
Guidelines and Role of Resident Teaching Faculty:
1. Each doctor is required to spend a minimum of four hours of student teaching/supervision per week. 2. Students should be supervised in history taking, physical examination and
management of patients. Procedures that are stated in the log book (Appendix 3) should be supervised/demonstrated to them.
3. Student presentations in the clinics, ward rounds and bedside teaching sessions should be documented by the students in their respective log books. 4. Besides presentations, students are required to record all tasks performed, assisted
or observed immediately in the log book ; these will need endorsement/grading by the supervising doctor/staff.
5. Doctors are required to complete the supervisor’s report (Appendix 4) and hand to The office in UKMMC in a sealed envelope to be given to the student group leader on their last day in Teluk Intan.
He/she will need to return these to the Surgical Department in UKMMC on the same/next working day.
6. Doctors here are most welcomed to provide feedback/contact theYear 5 Module head/Assistant on any relevant issues.
The student leader will need to liase with EncikMarzuki or PuanKhairunnisaat the
Undergraduate Office at UKMMC, in regards to:
1. Thesupply of gloves, aprons, hats & masks
2. Transport between UKMMC &TelukIntan Hospital

Year5 UKMMC General Surgery 2012/13
III. MODULE LEARNING OUTCOMES
General :
At the end of year V, the students should be able to:
1. Assistas a junior doctor in the surgical wards under direct supervision of a medical officer.
2. Apply basic surgical knowledge and skills effectively, to practice safely and competently.
3. Participate as a team member and assume leadership role in relevant situations.
4. Conduct basic surgical procedures in the wardunder direct supervision of a
medical officer/ staff, as deemed appropriate. 5. Commit to lifelong learning.
Specific Learning Outcomes :
At the end of the 7-week attachment, the student should be able to:
1. Satisfactory obtain a surgical history and perform physical examination.
2. Request basic and specific investigations to assist in diagnosis and management of common surgical problems.
3. Interpret relevant findings to reach a correct diagnosis. 4. Understand and discuss appropriate management of common surgical diseases.
5. Discuss the principles of surgical practice in the management of surgical patients.
6. Understand the ethical and medico-legal issues in the management of surgical patients. 7. Perform simple ward procedures competently. (e.g: phlebotomy, bladder
catheterization, blood taking, setting up an intravenous drip) 8. Assist in simple surgical procedures (e.g: insertion of chest tube, excision of
lumps, toilet and suturing) 9.Participate in the collaborative management involving allied healthcare personnel (e.g: pharmacist, nutritionist, physiotherapist, rehabilitationist,
and social services available) in the management of surgical patients. 10.Understandskills in dealing with uncertainty, death and dying patients.
11.Demonstrate a sense of responsibility in interpersonal and professional conduct.

Year5 UKMMC General Surgery 2012/13
IV. COURSE CONTENT
A. Clinical Topics
General Surgery
( must know)
General Surgery
( should know)
General Surgery
( nice to know )
Trauma - ABC of trauma - primary survey
- secondary survey - types of shock &
management - types of trauma &principle management
- chest injury - head injury: types &
management - genitourinary trauma
Endocrine
-benign thyroid diseases -thyroid malignancies -thyrotoxicosis
-hypercalcaemia and hypocalcaemia
Endocrine
-complications of thyroid surgery&management -primary and secondary
hyperparathyroidism -Cushing’s syndrome
-Conn’s syndrome -phaechromocytoma
Endocrine
-carcinoidtumour -insulinoma -adrenocortical carcinoma
-anteriormediastinal mass -inflammatory thyroid
diseases
Breast - benign diseases
- malignancies - nipple discharge
Breast -ductal carcinoma in situ
-lobular carcinoma in situ -phyllodestumour
-Paget’s disease -chronic granulomatous mastitis
Breast -reconstruction: types &
indications -management of non
palpablelesions
General
- hernia :inguinal, ventral, femoral, incisional,
paraumbilical& complications - lumpsand bumps;
management - appendicitis
General
- types and management of enterocutaneous
fistulaes
Upper GI
-peptic ulcer disease -gastric carcinoma -oesophageal carcinoma
-reflux
Upper GI
-Barrett’s oesophagus -oesophageal corrosive injuries
-gastric lymphoma
Upper GI
-hiatus hernia
Year5 UKMMC General Surgery 2012/13
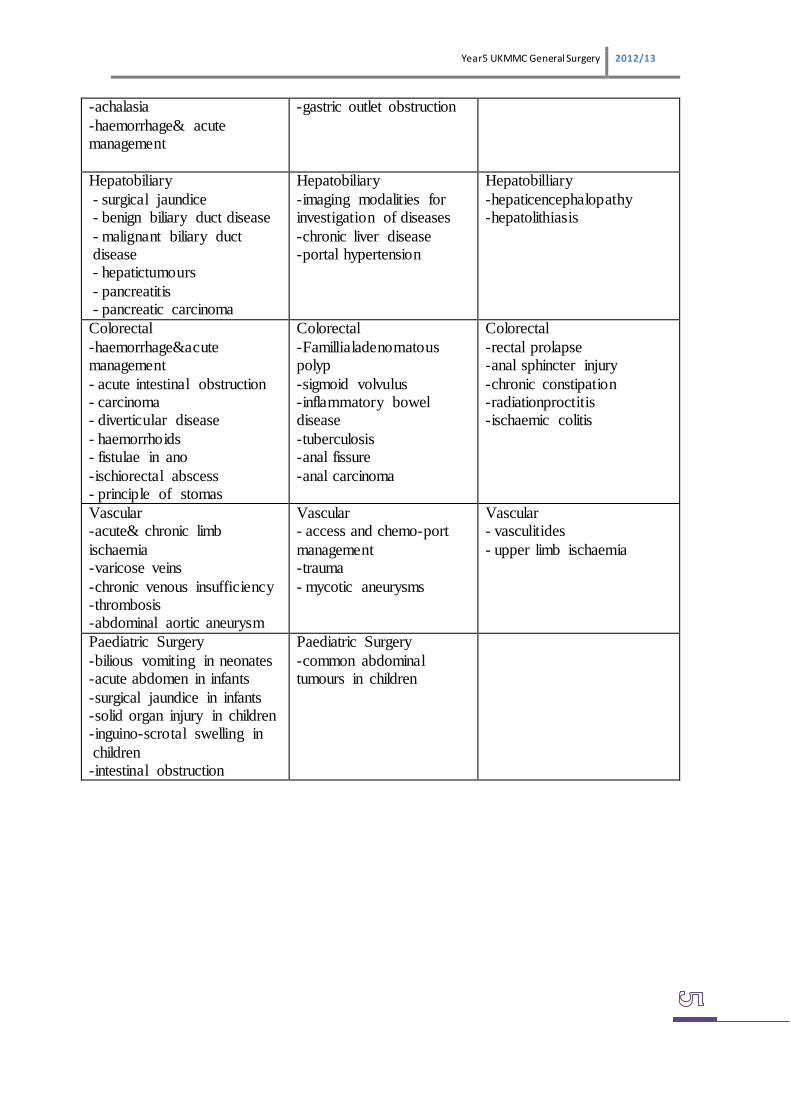
-achalasia
-haemorrhage& acute management
-gastric outlet obstruction
Hepatobiliary
- surgical jaundice - benign biliary duct disease
- malignant biliary duct disease - hepatictumours
- pancreatitis - pancreatic carcinoma
Hepatobiliary
-imaging modalities for investigation of diseases
-chronic liver disease -portal hypertension
Hepatobilliary
-hepaticencephalopathy -hepatolithiasis
Colorectal
-haemorrhage´ management
- acute intestinal obstruction - carcinoma - diverticular disease
- haemorrhoids - fistulae in ano
-ischiorectal abscess - principle of stomas
Colorectal
-Famillialadenomatous polyp
-sigmoid volvulus -inflammatory bowel disease
-tuberculosis -anal fissure
-anal carcinoma
Colorectal
-rectal prolapse -anal sphincter injury
-chronic constipation -radiationproctitis -ischaemic colitis
Vascular -acute& chronic limb
ischaemia -varicose veins
-chronic venous insufficiency -thrombosis -abdominal aortic aneurysm
Vascular - access and chemo-port
management -trauma
- mycotic aneurysms
Vascular - vasculitides
- upper limb ischaemia
Paediatric Surgery
-bilious vomiting in neonates -acute abdomen in infants
-surgical jaundice in infants -solid organ injury in children -inguino-scrotal swelling in
children -intestinal obstruction
Paediatric Surgery
-common abdominal tumours in children

Year5 UKMMC General Surgery 2012/13
Urology
-haematuria: causes & management -benign prostatic hyperplasia
-genitourinary calculi -management of testicular
pain
Urology
-management of testicular swelling -Fournier’s Gangrene
Urology
-prostate carcinoma
Plastic Surgery -benign and malignant skin lesions
-benign and malignant oral lesions
-burns& management
Plastic Surgery - parotidtumours
Neurosurgery - brain abscess
Neurosurgery -braintumours
-spinal cord compression -hydrocephalus
B.Clinical procedures
To perform under supervision To observe
-venous blood taking -intravenous drip -insertion/removal of venofix
-blood culture & sensitivity -insertion/removal of urinary catheter
-insertion/removal of nasogastric tube -removal of sutures -wound dressing
-digital per rectal examination -proctoscopy (+/- enema insertion)
-taking informed consent -arterial blood gas -fine needle aspiration cytology ( FNAC)
-core-biopsy -insertion of Sengstaken- Blakemoore tube
-suprapubic catherisation -insertion/removal of chest tube -insertion of central venous line
-banding of haemorrhoids -incision and drainage
-stoma care -endoscopy (OGDS/ERCP/colonoscopy/sigmoidoscopy)

Year5 UKMMC General Surgery 2012/13
V. TEACHING-LEARNING METHODOLOGY
A. Workshop , Lectures &Seminarsin the 1st week
1)A workshop will include briefing and demonstrations on -basic clinical procedures
-asepsis / sterility -handling of basic surgical instruments 2)Seminar& Lectures on core surgical topics
-will be facilitated by designated lecturers
B. Clinical Teaching Rounds Students are expected to attend ward roundseveryday according to their respective teams. They are expected to perform as junior house officer and participate in the
team’s patient care. They are expected to present the cases during the ward rounds.
C. Wardwork
Students are expected to work together with the house officers and medical officers after the clinical teaching rounds. Apart from tagging in the wards, students are also
expected to go to the outpatient clinics, operating theatres and endoscopy suites to clerk patients and to observe procedures.
Whilst in the ward, the students are also expected to observethe work of the allied health providers and provide assistancein the day to day running of the ward (ie; Dietician, Pharmacist, Physiotherapist, etc.) in the co-management of surgical
patients.
D. Bed side teaching The students are expected to arrange the bed side teaching with their respective lecturers/doctors.During these teaching sessions, the students may discuss problem-
based learning, patient management, case presentations or perform clinical examination under supervision.
E. On-calls Students will be allocated on-call duty according to their respective teams, generally
once alternate week. They are expected to tag along the Medical Officer On-call for that particular day as “junior House officer”. They are required to attend to patients at
the Emergency Department, operating theatre, endoscopy suites and the wards. Students are expected to present the cases to the respective Medical officer/ Registrar / Lecturer.
On Call Duties: 1.On-Call will be at UKMMC andTelukIntanHospital from 5pm to 12 midnight
followed bya normal day the following day. 2.On-Call duties must be emphasized parallel as the concept of junior clerkship.
Patients must be seen first-hand together with the house-officer on call, clerked, taken blood investigations and managed accordingly until reviewed by the medical officer/ specialist.
3. Blood investigations will be taken by the student under the supervision of the house officer/ medical officer.
4. All surgical procedures that are required of the Year V students will be under the supervision of the medical officer/specialist.
Year5 UKMMC General Surgery 2012/13
5. If a particular student is unable to do the call, he or she has to find a replacement for that particular day. 6. At any day, these cases could be asked to be presented and discussed in the group
bedside teaching by the supervisor.
F. Operation Theatre Students are encouraged to “Scrub up “ and assist as a second assistant in both the main and day care operation theatres.
G. Continuous Medical Education (CME) activities Students will be introduced to the concept of lifelong learning and are expected to
participate in the department’s regular CMEs ie; Journal Club Presentation, Recap (Revision of clinical case management and presentation), Radiological conferences, Histopathological conferences, Surgical updates, Surgical research
presentations(Surgitract), and Mortality & Morbidity meetings.
H. Clinical Proficiency Test ,CPT At the end of each posting there will be a formal assessment by the lectures. Each student will be given 20 minutes to examine/discuss a patient. The student will be
tested for another 10 minutes on an instrument and/or radiograph.
VI. ABSENCE FROM POSTING ACTIVITIES/SCHEDULE
The students are required to attend all academic and clinical activities pertaining to their course module. The attendance is 100%. If a student is unwell and is absent, a
medical certificate (m.c.) of illnessmust be produced to the respective lecturer on his/her return.
If a student is unable to attend a session due to involvement in any official extra-curricular activities, an official letter stating his/her involvement must be produced to
the respective lecturer on his/her return. The m.c.or letter, whichever may be the case, then needs to be given to the surgical
department office for recording/filing.
VII. ASSESSMENT
Areas of Assessment Percentage
i. Clinical Proficiency test - 50% ii. Supervisor’s reports(2) - 20% iii. Log Book - 20%
iv. Case report - 10% Total 100%
A student will need to acquire a minimum50% ofthetotal marksto be considered to
have passed the surgical posting/module.

Year5 UKMMC General Surgery 2012/13
VIII. REFERENCES
A. Textbooks:
1. Forrest, Carter, Macleod: Principles and Practice of surgery. Churchill
Livingstone, Latest Edition (2005). 2. Cushieri, Hennessy,Greenhalgh, Rowley and Grace; Clinical surgery.
Blackwell science, Latest Edition (2003). 3. Williamson; Scott: An Aid to clinical Surgery. Churchill Livingstone, Latest
Edition (2005).
4. Norman L Browse; An introduction to the Symptoms and Signs of Surgical Diseases. Latest Edition (2005).
B. Reference books:
1. Cushieri, Giles, Moossa; Essential Surgical Practice, Latest Edition(1996). 2. Bailey and Love’s Short Practice of Surgery, Latest Edition (2004).
C. Web:
1. Surgical tutor- surgical-tutor.org.uk 2. International journal of surgery - http://www. theijs.com
UPDATED: March 2012- Dept. of Surgery Year 5 Curriculum Committee
a. Mr. Hairol Othman b. Mr Azlanuddin b. Azman c. Mr. Noor Izham Ismail d. Ms Marjmin bt. Osman
1st Revision on the Updated Year 5 Curriculum, March 2012 - Dr Saladina Jaszle @ 28th April 2014

Year5 UKMMC General Surgery 2012/13

Year5 UKMMC General Surgery 2012/13
APPENDIX 2: WEEKLY TIME-TABLE/ DEPARTMENT ACTIVITY A. UKMMC
Monday Tuesday Wednesday Thursday Friday
7.30am-8am CWR
8am – 9am Surgitract Recap
CPC Radiology
conference
Census/ HPE
conference/ Surgitract
9am – 10am CWR
10am – 1pm Wardwork/Clinic/OT/Endoscopy
2pm- 3pm CWR
3pm- 5pm Bedside teaching (based on respective lecturer)
5pm-12
midnight On-Call; Once alternate week
B. TELUK INTAN HOSPITAL
Monday Tuesday Wednesday Thursday Friday
8am – 10am CWR
GWR
9am-12am 10am – 1pm Wardwork/Clinic/OT/Endoscopy
2pm- 3pm Wardwork
3pm- 5pm Bedside teaching (based on respective doctor); 4 hrs/week/per doctor&
3hrs/week/UKMMC lecturer
5pm-12
midnight On-Call; Once alternate week
Abbreviation & Venue: CWR Clinical Ward Rounds GWR Grand Ward Round CPC Clinico-pathological conference ;Auditorium HPE conference Histopathologicalexamination conference , last
Friday of the month ; Pathology seminar room Recap Revision of clinical patient management SurgitractSurgical research presentations Radiology conference Radiology seminar room

Year5 UKMMC General Surgery 2012/13
WEEKLY TIME TABLE
Week 1: UKMMC
CME/ CPC ( 1 hr)
Demonstration/Lecture Seminar
Ward Work/ Bedside teaching
On call
Mon Dept CME (1 hr)
Briefing (1 hr)
Surg L1 (2 hrs) Demonstration (2 hrs)
Rad L1 (1 hr)
Tues Recap (1 hr) Surg L2 (2 hrs) SurgL3(1 ½ hrs)
SurgL4(1 ½ hrs) SurgL5(1 ½ hrs)
Wed CPC (1 hr) SurgL6(1 ½ hrs) Sem 1 (2 hrs) Rad L2 (1 hr)
Sem 2 (1 ½ hrs)
Thurs Radiology conf (1 hr) Sem 3 (1 ½ hrs)
SurgL7(1 ½hrs) Sem 4 (2 hrs) Rad L3 (I hr)
Fri Census/HPE/Surgitract (1 hr)
Sem 5(1 ½hrs) Sem 6(1 ½hrs)
Total 6 hrs 6 + 6.5 + 6 + 6 + 3= 27.5 hrs
Week 2-4: UKMMC
CME
Clinic/OT/Endoscopy Ward Work
Bedside Teaching
On call
Mon Dept CME (1 hr) 12 hrs/w eek
2 hrs 1.5 hr
3.5 hrs/w eek (Alternate
w eek on call X1 ie 7 hrs per
call)
Tues Recap (1 hr) 2 hrs 1.5 hr
Wed CPC (1 hr) 2 hrs 1.5 hr
Thurs Radiology conf (1 hr) 2 hrs 1.5hr
Fri Census/HPE/Surgitract (1 hr)
2 hrs 1.5 hr
Per Week 5 hrs 12 hrs 10 hrs 7.5 hrs 3.5 hrs
Week 5-7: TelukIntan Hospital
CME/Others
Clinic/OT/Endoscopy Ward Work/
Bedside Teaching
On call
Mon 12 hrs/w eek
15 hrs/w eek
4 hrs/doctor/
w eek
3hrs/lecturer/w eek
3.5 hrs/w eek
(Alternate
w eek on call X1 ie 7 hrs per
call)
Tues
Wed
Thurs Last Thurs: Return Trip (2-5pm)
Fri GWR (3 hrs) Last Fri: Exam in
UKMMC (9am-1pm)
Per Week 3 hrs 12 hours 15hrs 15 hrs 3.5 hrs
L: Lecture Sem: Seminar Surg: Surgical Rad:Radiology

Year5 UKMMC General Surgery 2012/13
CREDIT HOURS
PROGRAMME UKMMC TELUK INTAN HOSPITAL
GRAND TOTAL
CME 21 6 27.0
Lecture/seminar 27.5 0 27.5
Bedside Teaching 22.5 45 67.5
On call 21
21.0
Case report 1x 6 hrs 6 0 6.0
OT/Clinic/Endoscopy 36 33 69.0
Ward work 30 41 71.0
TOTAL 155hrs 125 hrs 280hrs

Year5 UKMMC General Surgery 2012/13
APPENDIX 3
Year V Log Book (FF5126)
Department of Surgery
Name:
Matric No. :
Session:
Group :
Posting date Begin : End :
Supervisor(s) :
1. 2.

Year5 UKMMC General Surgery 2012/13
Lecturer(s) in charge :
1. 2.
Clinician(s) in charge :
Registrar: 1. 2.
Medical Officer: 1. 2.
House Officer: 1. 2.

Year5 UKMMC General Surgery 2012/13
Procedures performed
No. Type Date Diagnosis Supervisor’s Name
Signature
1 Insertion of a venofix
( 5 cases)
2 Removal of a venofix
( 5 cases)
3 Insertion of a
nasogastric tube
( 3 cases)

Year5 UKMMC General Surgery 2012/13
4 Removal of a
nasogastric tube
( 3 cases)
5 Insertion of a urinary
catheter (2 cases)
6 Removal of aurinary catheter (2 cases)
7 Wound dressing
(3 cases)
8 Removal of sutures/
R.O.S
(3 cases)

Year5 UKMMC General Surgery 2012/13
9 Venepuncture
( 5 cases)
10 Digital rectal examination
& proctoscopy
( 3 cases)
11 Setting up an intravenous drip
( 3 cases)
12 Blood culture & sensitivity (3 cases)

Year5 UKMMC General Surgery 2012/13
Procedures observed
No. Type Date Diagnosis Supervisor’s name
Signature
1 Arterial blood gas
/puncture
2 Insertion of a central venous line
3 Insertion of a chest tube
4 Removal of a chest
tube
5 Insertion of an enema
6 Core biopsy
7 Fine needle aspiration cytology
8 Rubber banding of
piles
9 Suprapubic
catheterization
10 Stoma care
11 Taking an informed
consent
12 Toilet & suturing

Year5 UKMMC General Surgery 2012/13
Endoscopic observations
No. Type Date Diagnosis Supervisors’s name
Signature
1 OGDS
2
Colonoscopy
3 ERCP

Year5 UKMMC General Surgery 2012/13
On call duty
No. Type of Procedure
Date Diagnosis Supervisor’s Name
Signature

Year5 UKMMC General Surgery 2012/13
Case Presentation
a) Clinic No. Patient’s name RN Date Diagnosis Supervisor’s
name Signature Marks
Pass: 5-10
Fail: 0-4
1
2
3
4
5

Year5 UKMMC General Surgery 2012/13
b) Ward round
No. Patient’s name RN Date Diagnosis Supervisor’s name
Signature Marks Pass: 5-10 Fail: 0-4
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
C) Bedside Teaching

Year5 UKMMC General Surgery 2012/13
No. Patient’s name RN Date Diagnosis Supervisor’s name
Signature Marks Pass: 5-10 Fail: 0-4
1
2
3
4
5
6
7
8
9
10
Operation Theatre:
Students are encouraged to “Scrub up “ and assist as a second assistant.

Year5 UKMMC General Surgery 2012/13
a)Main / General
No. Patient’s Name
RN Date Diagnosis Type of Surgery Surgeon’s Name
Signature
1
2
3
4
5
b) Daycare
No. Patient’s RN Date Diagnosis Type of Surgeon’s Signature

Year5 UKMMC General Surgery 2012/13
Name Surgery Name
1
2
3
4
5
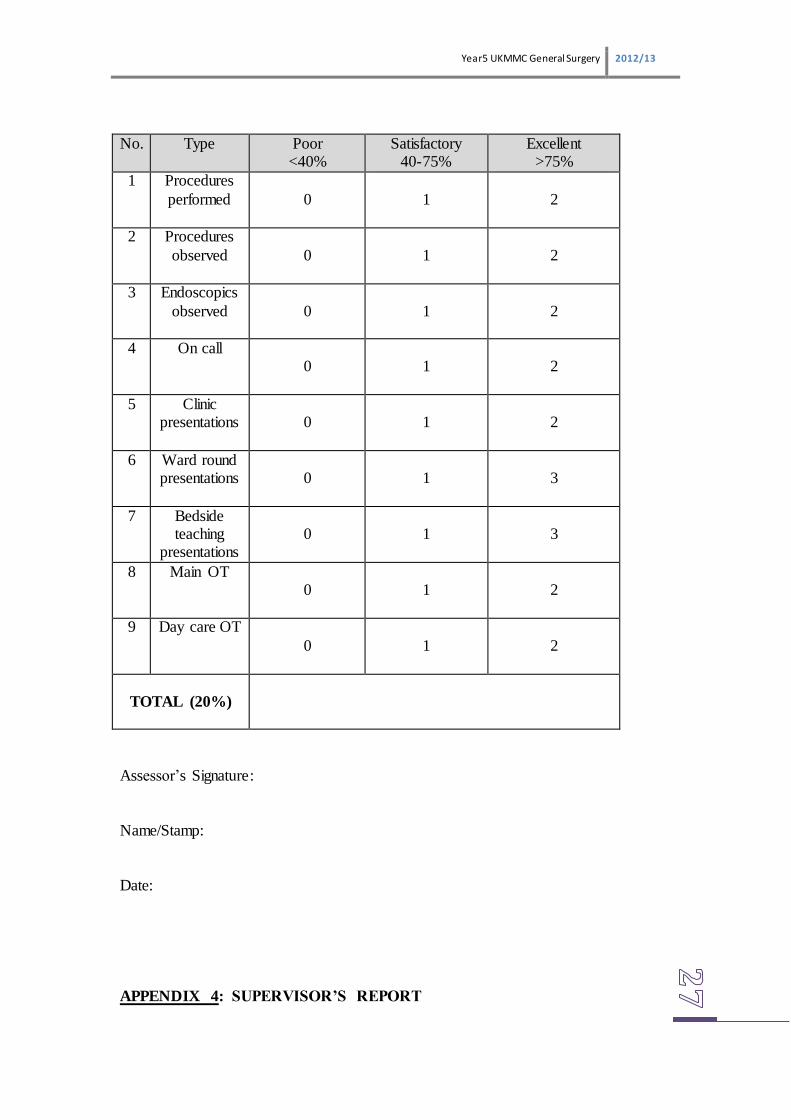
LOG BOOK ASSESSMENT
Year5 UKMMC General Surgery 2012/13
No. Type Poor <40%
Satisfactory 40-75%
Excellent >75%
1 Procedures
performed
0
1
2
2 Procedures
observed
0
1
2
3 Endoscopics
observed
0
1
2
4 On call
0
1
2
5 Clinic presentations
0
1
2
6 Ward round presentations
0
1
3
7 Bedside teaching
presentations
0
1
3
8 Main OT 0
1
2
9 Day care OT
0
1
2
TOTAL (20%)
Assessor’s Signature:
Name/Stamp:
Date:
APPENDIX 4: SUPERVISOR’S REPORT

Year5 UKMMC General Surgery 2012/13
Name : Matric No. : Year : Date of Posting:
Clinical Assessment
Component Excellent (5) Good ( 4) Fair (3) Borderline(2) Fail ( 1)
1 History
2 Examination
3 Diagnostic skill
4 Investigation
5 Management
6 Clinical knowledge
Professional Assessment
Component Excellent (5) Good ( 4) Fair (3) Borderline (2) Fail ( 1)
7 Appearance
8 Bedside manners
9 Attitude
10 Attendance TOTAL SCORE
Total final score ( Clinical + Professional Assessment score ) = /50
Comment :
______________________________________________________________________________
_______________________________________________________________________
-------------------------------------------
Date: Supervisor’s Signature & Stamp
APPENDIX 5:CLINICAL PROFICIENCY TEST

Year5 UKMMC General Surgery 2012/13
Student Name: Matric No.:
Examiner 1: Examiner 2:
CASE 1 (Modified Long / Short Case)
Diagnosis:
Component Assessed
__________________________________________________________________________________________________________________________________________________________________________________________
_____________________________________________________________________
Marks: /10
Lecturer’s Comment:
_____________________________________________________________________________________________
_____________________________________________________________________________
CASE 2 (Instrument / Radiograph)
Diagnosis:
Component Assessed
_______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Marks: /10
Lecturer’s Comment:
__________________________________________________________________________________________________________________________________________________________________________
__________________ ___________________
Signature & StampSignature & Stamp
Date: