laser eye surgery
TRANSCRIPT

CORNEAL REFRACTIVE SURGERY BY
FEMTO-SECOND LASER
Presented by:
Ajay Singh
Physics Department Indian Institute of Technology Delhi

Heating
Cooling
Imaging
Communicati
on

ANATOMY OF THE EYE

HOW THE EYE WORK
Cornea = Lens Cover
Iris and Pupil = Aperture of
Camera
Lens = Camera’s Lenses
Retina = Camera’s Film

COMMON VISIONS PROBLEMS
Myopia
Nearsightedness
Nearby objects can be seen
perfectly while objects at distance
appear blurry
Light rays occur in front of retina

HYPEROPIA
Opposite of myopia
Farsightedness
Can see distant object more
clearly than nearby objects
Light rays focus behind
retina

ASTIGMATISM
People who suffer myopia
and hyperopia will suffer
astigmastism also
Object both far and near
appear blurry
Light entering the eyeball
focuses on multiple areas
rather than on retina
PRESBYOPIA
Common vision problem for
old age
Dependent with reading
glasses
Human eye loss flexibility of
the lens
Weakening in the muscle

NON-SURGICAL CORRECTION OPTIONS
Glasses
Contact Lenses
Orthokeratology

Refractive Eye Surgery
Refractive eye surgery is eye surgery used to improve the refractive
state of the eye and decrease or eliminate dependency on glasses or
contact lenses. This can include various methods of surgical remodelling
of the cornea or cataract surgery. The most common methods today use
excimer lasers to reshape the curvature of the cornea. Successful
refractive eye surgery can reduce or cure common vision disorders such
as myopia, hyperopia and astigmatism, as well as degenerative
disorders like keratoconus.
In Laser surgery surgery, the curvature of the cornea is altered by
removing a specific amount of corneal tissue with ultraviolet photo-
ablation from the excimer laser.
http://ildenaro.it/blog/2014/02/27/riparazione-della-cornea-al-monaldi-il-laser-supervoloce/

1950’s – Columbian Jose Barraquer developed Microkeratome
& keratomileusis techniques and discovered root causes for eye
trauma
1970’s – Russian Svyatoslav Fyodorov developed Radial
Keratotomy (and posterior chamber implantable contact lenses
in 1980)
1970’s – Development of Excimer Laser (origin of LASEK laser)
1982 – 3 Members of the IBM research team discovered the
laser could be used to remove biological tissue without heat
damage to surrounding tissue
1987 – Dr. Steven Trokel performed the 1st laser surgery on a
patients eye
1996 – Lasik Eye Surgery cecame officially approved by the
U.S. government
BRIEF HISTORY

CLASSIFICATION
REFRACTIVE SURGERIES
CORNEA BASED LENTICULAR BASED COMBINED(BIOPTICS)
-R.K.
-PRK
-LASIK/Intra
LASIK
-EPILASIK
-LASEK
-Conductive
Keratoplasty
-Corneal Inlays
and rings
-Clear Lens
extraction for
myopia
-Phakic IOL
- Prelex Clear
Lens Extraction
with use of
Multifocal IOL’s
Combination
of the two

A) Radial keratotomy (RK)
B) Excimer laser photorefractive keratectomy ( PRK )
C) Laser assisted in situ keratomiliuses (LASIK)
D) Laser assisted subepithelial keratomiliuses ( LASEK )
E) Laser thermokeratoplasty (LTK )
D) Intracorneal ring segments (ICRS)
G) Phakic intraocular lenses (IOLs )

Various types of laser surgery are used to treat refractive error:
LASIK : knife is used to cut a flap in the cornea, and a laser is used
to reshape the layers underneath, to treat refractive error.
IntraLASIK: a variant in which the flap is also cut with a laser
Photorefractive keratectomy (PRK, LASEK), in which the cornea is
reshaped without first cutting a flap
Laser thermal keratoplasty: in which a ring of concentric burns is
made in the cornea, which cause its surface to steepen, allowing
better near vision
Lasers are also used to treat non-refractive conditions, such as:
Phototherapeutic keratectomy (PTK), in which opacities and surface
irregularities are removed from the cornea
Laser coagulation, in which a laser is used to cauterize blood
vessels in the eye, to treat various conditions
Lasers can be used to repair tears in the retina.

Types of lasers used-
Excimer-Excited dimer of two atoms
-An inert gas(Argon)
-Halide(Fluoride)
which releases ultraviolet energy at193nm for corneal ablation
Non-Excimer solid state lasers-
210nm Q switched diode pumped laser
213 nm Q switched diode pumped laser(Pulsar)
Advantage of Non-Excimer solid state lasers-
No toxic excimer gases
Wavelength closer to absorption peak of corneal collagen—less
thermal and collateral damage
Better pulse to pulse stability
Not absorbed by air, water, tear fluid-so less sensitive to humidity or
room temperature
No purging with inert gases required.

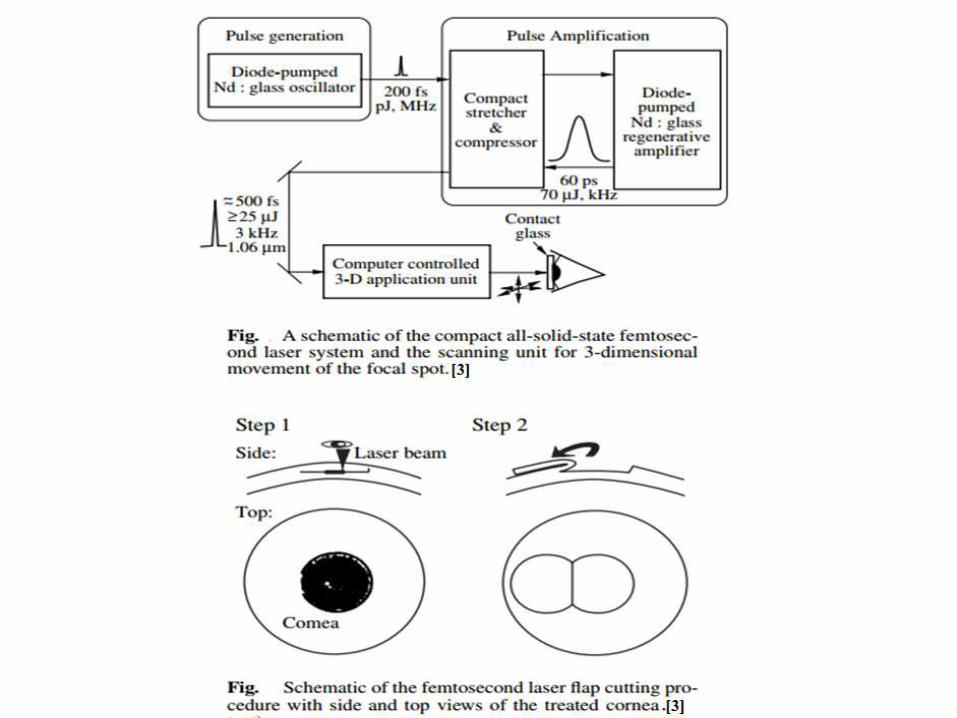
PROCEDURE (FEMTOSECOND LASER SURGERY)
Step 1 : Corneal Flap Cutting Procedure
Step 2 : Femtosecond Laser Keratomileusis (FLK)
Step 3:Femtosecond Laser Intrastromal Vision Correction (FLIVC)
Source:www.ele.uri.edu/courses/bme281/F12/ColtonS_2.ppt



INTERACTION OF FEMTOSECOND LASER PULSES WITH CORNEAL TISSUE
Why femtosecond? Bubbles?/
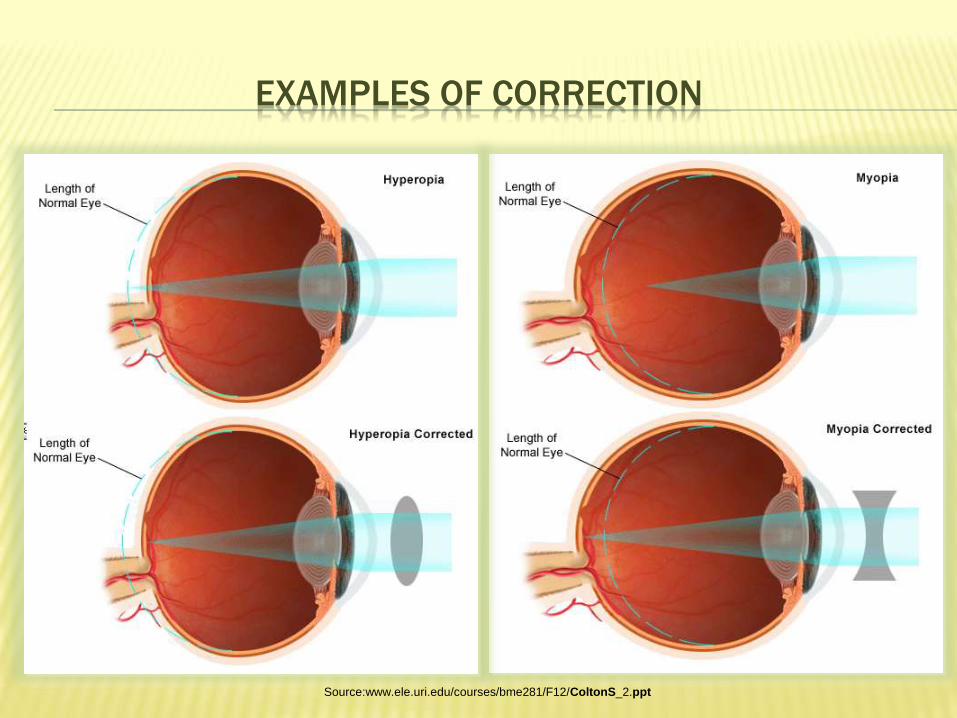
EXAMPLES OF CORRECTION
Source:www.ele.uri.edu/courses/bme281/F12/ColtonS_2.ppt


The surgery is typically done within 30 minutes or less-quick & painless
Most people achieve 20/20 vision (or even better) afterwards (90% reachdesired vision after LASIK)
May still need glasses/contact lenses, but prescription is much lowerthan before
A small percentage of people have an enhancement (minor touch up)surgery later for further improved vision
Requires no bandages or stitches
Research conducted by the Magill Research Center for VisionCorrection, Medical University of South Carolina, showed that the overallpatient satisfaction rate after primary LASIK surgery was 95.4%. Theyfurther differentiated between myopic LASIK (95.3%) and hyperopicLASIK (96.3%). They concluded that the vast majority (95.4%) of patientswere satisfied with their outcome after LASIK surgery.
ADVANTAGES OVER NON-LASER SURGERIES

LASIK LASEK
Name Detail: Laser-Assisted In Situ Keratomileusis Laser Assisted Sub-Epithelial
Keratomileusis
Corrective Uses: Refractive error correction for
nearsightedness, farsightedness,
astigmatism and presbyopia.
Refractive error correction for
nearsightedness,
farsightedness, astigmatism
and presbyopia.
Procedure Length: Outpatient procedure. Laser treatment
requires less than one minute for each
eye; total procedure lasts about 15
minutes per eye.
Outpatient procedure. Laser
treatment requires less than
one minute for each eye; total
procedure lasts about 15
minutes per eye.
Procedural Notes: Uses a microkeratome knife and
excimer laser in procedure. The
epithelium and stroma are cut to a
thickness of 100-180 microns, then an
excimer laser ablates corneal tissue
under the epithelial/corneal tissue flap.
An alcohol solution helps lift the
epithelium.
The epithelium is cut to a
thickness of 50 microns while
the stroma is left uncut. Uses a
trephine, a finer blade than that
used in LASIK. An excimer
laser ablates corneal tissue
under the epithelial flap. An
alcohol solution helps lift the
epithelium.
Main difference Between LASIK and LASEK is thickness of the flap
which includes corneal stroma tissue in LASIK and only epithelial tissue
in LASEK.

Healing &
Recovery:
2 days – 1 week; faster than LASEK. Allowed to drive 1-3
days after surgery.
Flap edges heal within a day. Can drive in about
a week with crisp vision in about 6-8 weeks.
Recovery slightly longer than LASIK - about 4-7
days.
Benefits: Appropriate for people who have more corneal tissue, less
discomfort than LASEK, almost no pain, 20/20 vision or
better is typically achieved, corneal haze very rare,
immediate clear vision, follow-up enhancements are
easier if needed.
Better choice for poor LASIK candidates
including people with less corneal tissue, fewer
haze outcomes than LASIK, preserves more
corneal tissue than LASIK, less risk of dry eye
than LASIK.
Potential
Drawbacks:
Those with thinner corneas may suffer less than ideal
results, flap may dislodge with trauma, increases higher
order aberrations (HOA)**, uneven flap edges may lead to
astigmatism, flap may result in scars, ** Higher order
aberrations (HOA) affect the contrast sensitivity and fine
detail of vision, such as night vision, glare, contrast.
More discomfort than LASIK, takes longer to heal
than LASIK, medications, and conditions are
contraindications, trauma, such as being hit in
the eye may cause flap to dislodge, as a fairly
new technique, long-term outcomes are not well
established, increases HOA, blade can create
uneven flap edges leading to astigmatism.
Indications
for
Procedure:
Required thickness of corneal tissue achieved,
requirement for painless procedure and/or extremely fast
recovery, probably best for correcting over 6.00 diopters of
refractive error.
Corneas too thin or flat for LASIK.
For both of the procedures, extensive screening is required for qualification. Participants must be between
the ages of 18 and 40, vision must be less than -14.00 diopters of nearsightedness, less than +6.00 diopters
of farsigntedness, and less than 6.00 diopters of astigmatism, must not have a history of eye disease or
abnormality.
Contradiction
s to
Procedure:
Thin cornea, not within age limit,uncorrectable range of
vision, unstable prescription, eye disease or abnormality,
diabetic retinopathy, cataracts, glaucoma, ocular
hypertension, autoimmune disorders, contradictory
medication, pregnancy, nursing, large pupils, dry eye, prior
eye surgery, naturally elevated HOA.
Possible inability to maintain thin flap (resulting in
removal of epithelium), not within age limit,
uncorrectable range of vision, unstable
prescription, eye disease or abnormality, diabetic
retinopathy, cataracts, glaucoma, ocular
hypertension, dry eye, prior eye surgery, naturally
elevated HOA.

Acronyms not clarified in the chart include:
– BCV = Best Corrected Vision
– BCVA = Best Corrected Visual Acuity (same as BCV)
– DLK = Diffuse Lamellar Keratitis
– HOA = Higher Order Aberrations
– LOA = Lower Order Aberrations
– ASA =Advanced Surface Ablation (Used in PRK and LASEK)
– ICL = Implantable Contact Len
– IOL = Intra-Ocular Lens.
Per the Council for Refractive Surgery Quality Assurance (CRSQA)
Standards for refractive surgery:
– Minimum of 90% of patients achieve at least 20/40 uncorrected vision.
– Minimum of 50% of patients achieve at least 20/20 uncorrected vision.
– Minimum of 85% of patients achieve within 1± diopter of target.
– Minimum of 50% of patients achieve within 0.5± diopter of target.
– Maximum of 3% of patients experience complications unresolved by 6
months postop.
– Maximum of 0.5% of patients experience serious (vision-threatening)
complications at 6 months post op requiring extensive maintenance or
invasive intervention.

The surgery is typically done within 30 minutes or less-quick & painless
Most people achieve 20/20 vision (or even better) afterwards (90% reachdesired vision after LASIK)
May still need glasses/contact lenses, but prescription is much lowerthan before
A small percentage of people have an enhancement (minor touch up)surgery later for further improved vision
Requires no bandages or stitches
Research conducted by the Magill Research Center for VisionCorrection, Medical University of South Carolina, showed that the overallpatient satisfaction rate after primary LASIK surgery was 95.4%. Theyfurther differentiated between myopic LASIK (95.3%) and hyperopicLASIK (96.3%). They concluded that the vast majority (95.4%) of patientswere satisfied with their outcome after LASIK surgery.
RESULTS

Some patients lose vision.
Some patients develop debilitating visual symptoms.
You may still need eyeglasses after surgery.
Some patients may develop severe dry eye syndrome.
For some farsighted patients, results may diminish with age.
Long-term data is not available.
Potentials Risks
Also The LASER eye surgery is not for you if you are
You required a change in your contact lens or glasses prescription in the
past year. This is called refractive instability.
You have a disease or are on medications that may affect wound healing.
You actively participate in contact sports. You participate in boxing,
wrestling, martial arts or other activities in which blows to the face and
eyes are a normal occurrence.
But Still the success rate > 95%, further
improvements going on

http://en.wikipedia.org/wiki/Refractive_surgery
http://minecrafterfield.deviantart.com/art/Human-Eye-test-sketch-320704758
http://en.wikipedia.org/wiki/Refractive_surgery
http://www.worldoflasers.com/laserapplindustrial.htm
http://en.wikipedia.org/wiki/LASIK
http://en.wikipedia.org/wiki/Laser_surgery#Eye_surgery
http://www.powershow.com
http://www.allaboutvision.com/visionsurgery/lasik.htm
http://www.dlxguard.com/history-laser-eye-surgery
http://www.lasik-eye-surgery.info/history.htm
http://www.medicinenet.com/lasik_eye_surgery/article.htm
http://www.webmd.com/eye-health/lasik-laser-eye-surgery
Reference Links
