large cell carcinoma accounts for 5-10% of all lung cancers. strongly associated with cigarette...
TRANSCRIPT


Large cell carcinoma
•Accounts for 5-10% of all lung cancers .
•Strongly associated with cigarette smoking.
• The lesion occurs peripherally and grows
rapidly, with early metastases and a poor
outcome •They lack any diagnosic
features to suggest their diagnosis prior to biopsy .
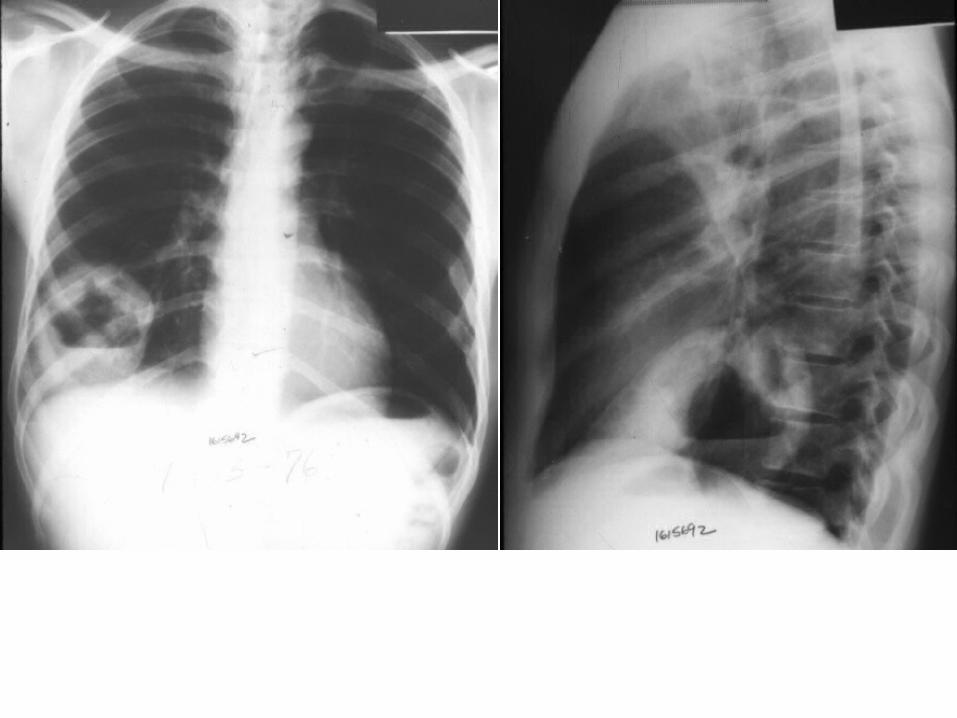

Pancoast tumors
•Represent 1-3% of all lung cancers. •Typically involve the lower trunks of the
brachial plexus, intercostal nerves, stellate ganglion, adjacent ribs, and vertebrae.
• More than 95% are NSCC .•Horner's syndrome, mediastinal and
supraclavicular adenopathy and vertebral body invasion portends a poorer prognosis
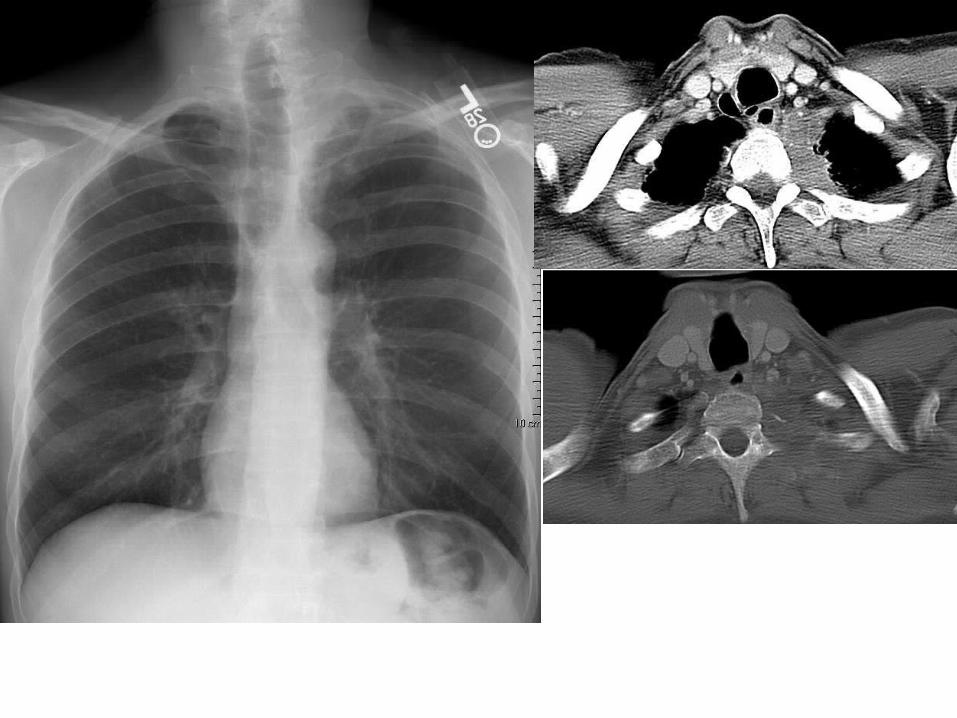

Pancoast Tumours Imaging
•MRI is more accurate in identification of the extent of tumor involvement; it is superior to CT scanning in
the detection of invasion of adjacent organs (eg, vertebral bodies, brachial plexus, subclavian vessels).
• CT or MRI of the brain is recommended in the initial evaluation, because distant metastases to the brain
are not infrequent •


Differential Diagnosis of an opacity at the Superior Sulcus
•Mesothelioma.•Lymphoma.•Plasmacytoma.•Metastatic malignancies (thyroid, larynx).•Lymphomatoid granulomatosis.•Cervical rib syndrome.•Tuberculosis.•Fungal infections.

Small Cell Lung Cancer•strong association with smoking
.•Rapid growth.•Early spread to distant sites.•Exquisite sensitivity to chemo
and radiotherapy.•Frequent association with
distinct paraneoplastic syndromes .
•Surgery usually plays no role in its management, except in rare
situations (<5% of patients) in which it presents at a very early
stage as a solitary pulmonary nodule

Small cell lung cancer
•18% of all lung cancers.•Often present with bulky
hila and mediastinal lymph node masses .
•TNM system does not provide important
prognostic information; only useful in <5%.
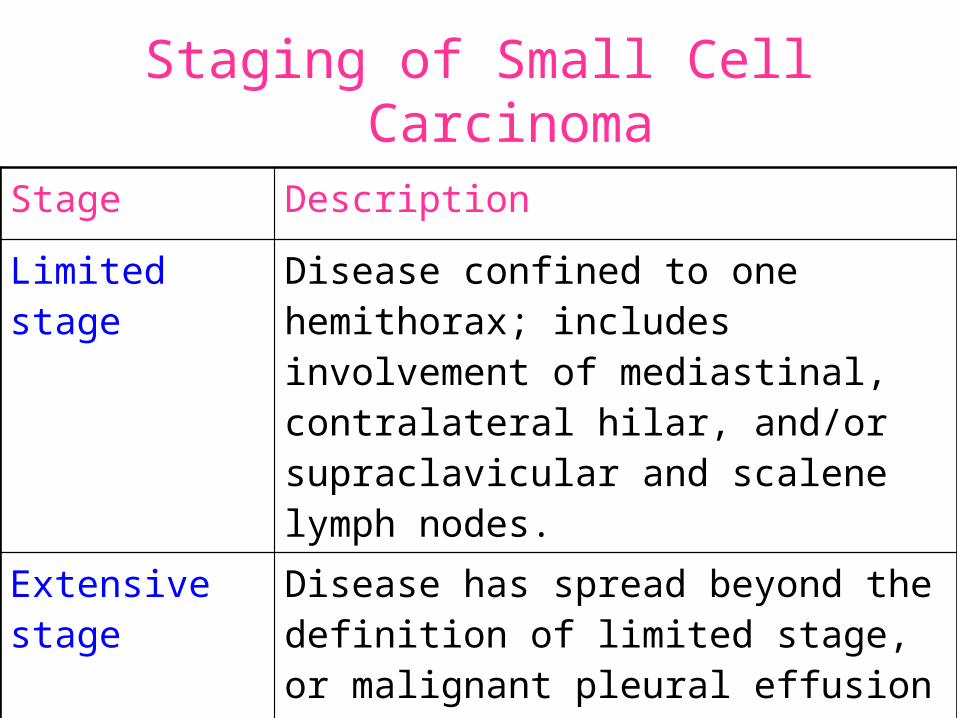
Staging of Small Cell Carcinoma
Stage Description
Limited stage Disease confined to one hemithorax; includes involvement of mediastinal, contralateral hilar, and/or supraclavicular and scalene lymph nodes.
Extensive stage
Disease has spread beyond the definition of limited stage, or malignant pleural effusion is present


•With central tumors, distinguishing primary tumor from lymph node
metastasis may be impossible

International Staging System for Lung Cancer
•This is the common evaluation framework,because, patient treatment
options and prognosis are directly related to their tumor stage at presentation.
•Derived from a TNM classification scheme with four separate stage groups from I to IV.
Stage I reflects the best prognosis, stage IV the worst .

Tumor (T)
–TX - Positive malignant cytology, no lesion seen –T1 - Diameter smaller than or equal to 3 cm –T2 - Diameter larger than 3 cm –T3 - Extension to pleura, chest wall, diaphragm,
pericardium, within 2 cm of carina, or total atelectasis –T4 - Invasion of mediastinal organs (eg, esophagus,
trachea, great vessels, heart), malignant pleural effusion, or satellite nodules within the primary lobe

T1 Tumor
•Diameter of 3 cm or smaller ,
surrounded by lung or visceral
pleura.
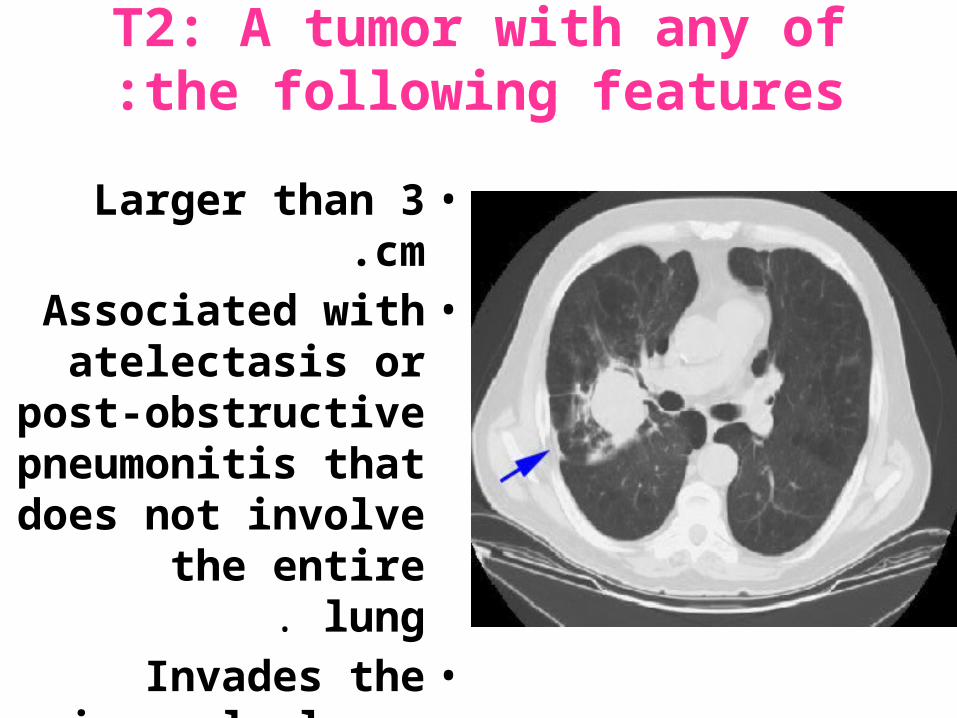
T2: A tumor with any of the following features:
•Larger than 3 cm.•Associated with
atelectasis or post-obstructive
pneumonitis that does not involve the entire
lung. •Invades the visceral
pleura.
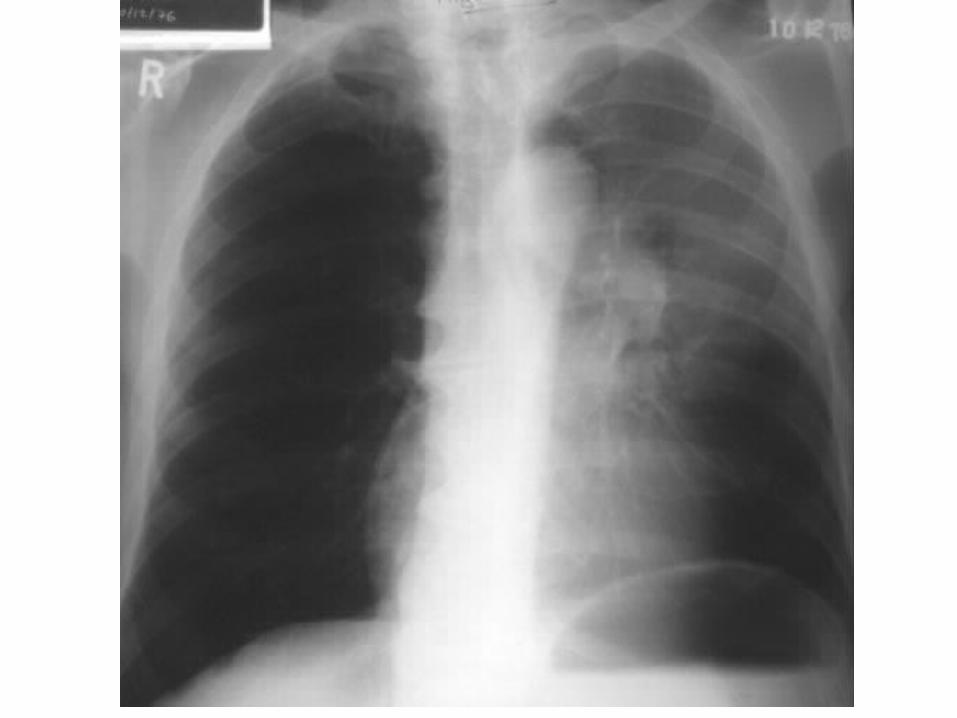


T3: A tumor of any size that directly invades any of the following:
•The chest wall (including superior
sulcus tumors), diaphragm,
mediastinal pleura, parietal pericardium.
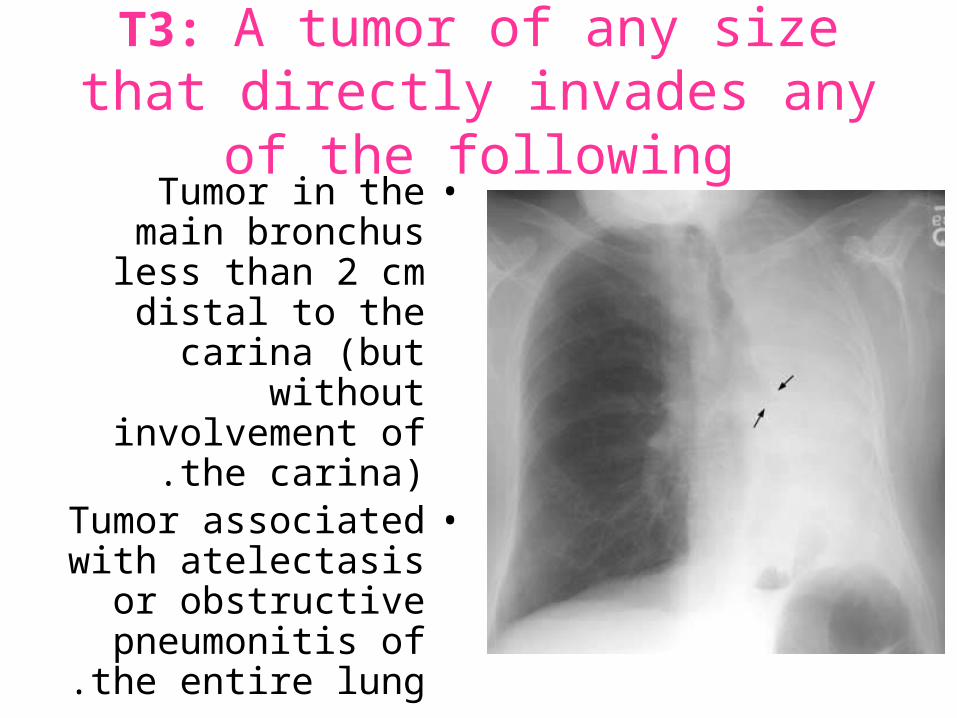
T3: A tumor of any size that directly invades any of the following
•Tumor in the main bronchus less than 2 cm distal to the carina (but without involvement of
the carina).•Tumor associated with
atelectasis or obstructive pneumonitis
of the entire lung .
